Embed Size (px)
Citation preview
Case ReportRare Appendicitis-Like Syndrome: The Case ofthe Obstructing Broccoli
Stephen Jones, Patrick Narh-Martey, Mitun Patel, Amanpreet Dhaliwal,Jessica Persson, and Denis Orr II
Department of Surgery, Western Reserve Health Education, USA
Correspondence should be addressed to Stephen Jones; [email protected]
Received 1 January 2014; Accepted 31 March 2014; Published 22 April 2014
Academic Editor: Johny Verschakelen
Copyright © 2014 Stephen Jones et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The diagnosis of acute appendicitis can be somewhat obscure in a patient that presents with right lower quadrant abdominal pain.The advancement and ease of imaging have made CT scanning readily available in the emergency department. Management can bechallenging when the patient has a high likelihood of appendicitis based on clinical suspicion and negative CT scan. The purposeof this case report is to demonstrate how an obstructing bezoar caused an appendicitis-like syndrome in a patient with negativeCT scan and clinical diagnosis of acute appendicitis. This case report will discuss the appendicitis-like syndrome of an obstructingbezoar and an approach at management.
1. Introduction
The diagnosis of acute appendicitis can be somewhat obscurein a patient that presents with right lower quadrant abdom-inal pain. Pyrexia, pain localized to McBurney’s point, andnausea can be a common occurrence in the emergencydepartment. A good history and physical exam often makethe diagnosis and negate the need for radiologic imaging.However, the advancement and ease of imaging have madeCT scanning readily available in the emergency department.The sensitivity of CT scans for identifying acute appendicitisreaches approximately 97% and the negative predictive value(NPV) reaches 99% by some reports [1, 2]. Managementcan be challenging when the patient has a high likelihoodof appendicitis based on clinical suspicion and negative CTscan. The purpose of this case report is to demonstrate howobstructing bezoars can cause an appendicitis-like syndromein a patient with negative CT scan and clinical diagnosisof acute appendicitis. Foreign body ingestion is commonand typically passed without intervention [3]. Depending onthe type of foreign body, presentation can vary. Impaction,
bowel obstruction, and perforation are the most commonpresentations described [3]. This report will discuss theappendicitis-like syndrome of an obstructing bezoar and anapproach at management.
2. Case Report
2.1. Case Presentation. A 32-year-old otherwise healthy malepresents to the emergency department with a history ofacute onset right lower quadrant abdominal pain which is10 hours in duration. He describes the pain as throbbingin nature, 7 out of 10 on the pain scale with no radiation.No alleviating or exacerbating factors were described. Thepatient also complains of nausea and vomiting for this timeperiod as well. In addition, he reports subjective fever andchills. He has no sick contacts. The patient states that his lastmeal was the past night and he reports having broccoli fordinner. He reports no difficulty in chewing food. He deniesany significant past medical or surgical history includingany gastric surgery or gastrointestinal resection. There is nohistory of Crohn’s disease or ulcerative colitis in his family.
Hindawi Publishing CorporationCase Reports in MedicineVolume 2014, Article ID 764869, 4 pageshttp://dx.doi.org/10.1155/2014/764869

2 Case Reports in Medicine
125 7.916.7
48.1236
140 17
3.9 0.9
103
28
Neutrophils: 88%
Figure 1
2.2. Physical Exam
General Appearance.He is alert and oriented times 3, in milddistress.
Vital Signs. Temperature was 98.2 F. Blood pressure was112/65mmHg. Pulse was 96 bpm. Respirations were 16. SPO2was 99% on room air.
Skin. Skin was warm and dry. HEENT indicated the follow-ing: normocephalic/atraumatic, PERRL, moist oral mucosa,and healthy dentition. Lungs were clear to auscultationbilaterally with no wheezes, rales, or rhonchi. Heart hadregular rate and rhythm and no murmurs, rubs, or gallops.
Abdomen. Abdomen was soft. He is not distended. He istender to palpation in the right lower quadrant with positiverebound at McBurney’s point, positive Rovsing sign, andpositive Obturator sign. No hernias were identified. Rectalexam revealed good anal sphincter tone, no external hemor-rhoids/skin tags, and hemoccult negative stool.
2.3. Labs. See Figure 1.
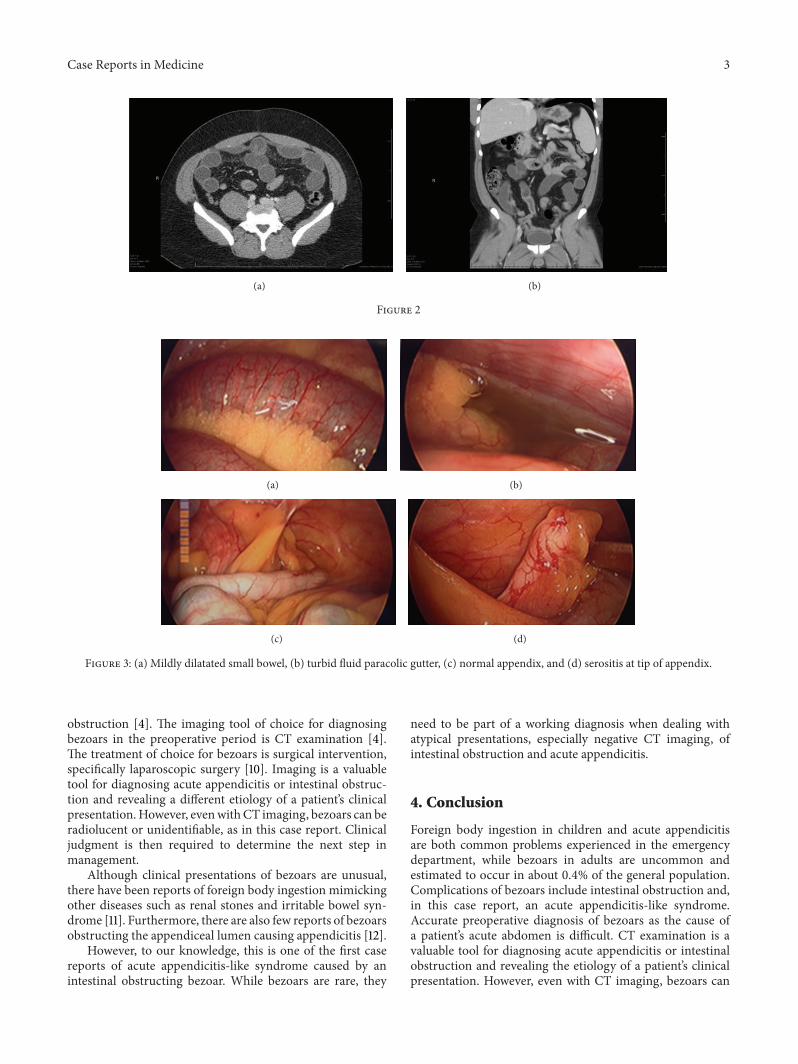
2.4. CT Findings. See Figures 2(a) and 2(b).
2.5.The Operation. Needle was inserted at the umbilicus andpneumoinsufflation was obtained. Using OptiView guidance,the laparoscope was inserted through a trocar into theabdominal cavity. Next, the area was inspected for injury,failing to reveal any. Additional ports were placed. Thediagnostic laparoscopy immediately revealed exudative fluidin the abdominal cavity. This was yellow-green. It wassuctioned and the specimen was sent for Gram stain cultureand sensitivity. The fluid was washed out. The appendixwas identified and found to be relatively normal with min-imal serositis at the tip. The small bowel had serositis andinflammation throughout the majority of the small bowelaffecting the proximal bowel more than the distal bowel. Theterminal ileum was then identified from the ileocecal valveproximally and identification of a mass in the small bowelwas made. The mass was firm and impacted and not able tobe significantly milked in either direction. The stomach wasinspected along with the duodenum and the gallbladder. Thegallbladder was distended, but no signs of acute cholecystitiswere appreciated. Next, anesthesia administered air to thestomach as well as methylene blue and neither of these testsrevealed a leak in the stomach or duodenum. Therefore,the small bowel was then addressed just distally to theimpaction and enterotomy was made. This was done by
scoring the small bowel laparoscopically. The decision wasmade to open the fascia slightly at the umbilical port siteand withdraw the small bowel. In doing so, the impactedforeign body had been milked away from the site. The bowelholding the foreign body was unable to be extracted throughthe enlarged port site, and, therefore, towel clamps wereapplied. Pneumoinsufflation was reobtained. The bowel wasgrasped with the grasper and extracted at the umbilical portsite. The small bowel was opened with monopolar cauteryvia the Bovie cautery extracorporeally and then droppedback into the abdominal cavity. Towel clamps were appliedto the skin and the impacted foreign body was milkedtowards the enterotomy (Figure 4).This technique revealed alarge unchewed and undigested piece of broccoli measuringapproximately 5-6 centimeters in diameter at widest point(Figure 5). The food piece was then scooped up with abag through the midline port site, which was held in placewith the towel clamps and extracted extracorporeally. Thebowel was then extracted extracorporeally and the bowel wasclosed using running 0 Vicryl. After testing the integrity ofthe enterotomy site, additional Lembert interrupted verticalsutures were placed to reinforce the area. Next, the abdominalcavity was washed out with approximately 1.5 liters of warmsaline. The fascia was closed using running 0 PDS sutures,and the skinwas closedwith subcuticular stitches.Thepatienttolerated the procedure well (Figure 3).
3. Discussion
Foreign body ingestion is a common problem experienced inthe emergency department. The ingestion of foreign objectsis most commonly seen in children, while, on the other hand,adult presentations of foreign body ingestion are more likelyto be due to bezoars. A bezoar is defined as a swallowed massof undigested material found within the gastrointestinal tract[4].Themost typical compositions of bezoars include hair (asseen in trichophagia), vegetable fibers, or, interestingly, per-simmon fruit. Bezoars are uncommon and estimated to occurin about 0.4% of the general population [5]. At least 80% ofingested foreign objects are passed spontaneously throughthe gastrointestinal tract without complication [3]. Althoughrare, bezoars are a recognized cause of intraluminal bowelobstruction [6]. Other complications associated with bezoarsand foreign body ingestion include bleeding, impaction,obstruction, and perforation [3]. These complications tendto occur at areas of angulation or narrowing of the gas-trointestinal tract [7]. Therefore, patients at increased risk ofbezoar formation include those with reduced gastrointestinalmotility or altered anatomy status after gastric surgery, mostnotably for treatment of peptic ulcer disease [4, 8].
Accurate preoperative diagnosis of bezoars as the causeof a patient’s acute abdomen symptoms is difficult [9]. Due tolow incidence, bezoars are naturally on the bottom of the listfor differential diagnoses [4].Variousmethods of imaging canbe utilized to aid in making a diagnosis. Radiologic optionssuch as abdominal X-ray, barium studies, and abdominalultrasound may be useful to diagnose intestinal obstruction,but they are not helpful in identifying a specific cause for
Case Reports in Medicine 3
(a) (b)
Figure 2
(a) (b)
(c) (d)
Figure 3: (a) Mildly dilatated small bowel, (b) turbid fluid paracolic gutter, (c) normal appendix, and (d) serositis at tip of appendix.
obstruction [4]. The imaging tool of choice for diagnosingbezoars in the preoperative period is CT examination [4].The treatment of choice for bezoars is surgical intervention,specifically laparoscopic surgery [10]. Imaging is a valuabletool for diagnosing acute appendicitis or intestinal obstruc-tion and revealing a different etiology of a patient’s clinicalpresentation.However, evenwithCT imaging, bezoars can beradiolucent or unidentifiable, as in this case report. Clinicaljudgment is then required to determine the next step inmanagement.
Although clinical presentations of bezoars are unusual,there have been reports of foreign body ingestion mimickingother diseases such as renal stones and irritable bowel syn-drome [11]. Furthermore, there are also few reports of bezoarsobstructing the appendiceal lumen causing appendicitis [12].
However, to our knowledge, this is one of the first casereports of acute appendicitis-like syndrome caused by anintestinal obstructing bezoar. While bezoars are rare, they
need to be part of a working diagnosis when dealing withatypical presentations, especially negative CT imaging, ofintestinal obstruction and acute appendicitis.
4. Conclusion
Foreign body ingestion in children and acute appendicitisare both common problems experienced in the emergencydepartment, while bezoars in adults are uncommon andestimated to occur in about 0.4% of the general population.Complications of bezoars include intestinal obstruction and,in this case report, an acute appendicitis-like syndrome.Accurate preoperative diagnosis of bezoars as the cause ofa patient’s acute abdomen is difficult. CT examination is avaluable tool for diagnosing acute appendicitis or intestinalobstruction and revealing the etiology of a patient’s clinicalpresentation. However, even with CT imaging, bezoars can
4 Case Reports in Medicine
(a) (b)
(c) (d)
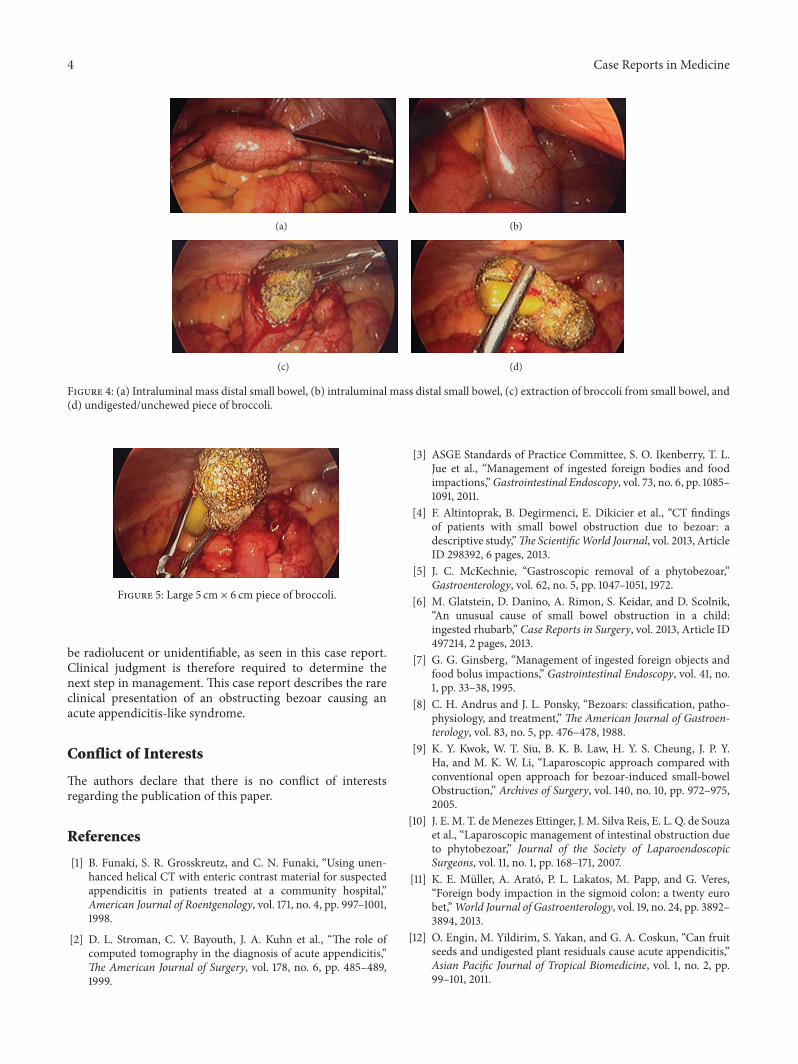
Figure 4: (a) Intraluminal mass distal small bowel, (b) intraluminal mass distal small bowel, (c) extraction of broccoli from small bowel, and(d) undigested/unchewed piece of broccoli.
Figure 5: Large 5 cm × 6 cm piece of broccoli.
be radiolucent or unidentifiable, as seen in this case report.Clinical judgment is therefore required to determine thenext step in management. This case report describes the rareclinical presentation of an obstructing bezoar causing anacute appendicitis-like syndrome.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] B. Funaki, S. R. Grosskreutz, and C. N. Funaki, “Using unen-hanced helical CT with enteric contrast material for suspectedappendicitis in patients treated at a community hospital,”American Journal of Roentgenology, vol. 171, no. 4, pp. 997–1001,1998.
[2] D. L. Stroman, C. V. Bayouth, J. A. Kuhn et al., “The role ofcomputed tomography in the diagnosis of acute appendicitis,”The American Journal of Surgery, vol. 178, no. 6, pp. 485–489,1999.
[3] ASGE Standards of Practice Committee, S. O. Ikenberry, T. L.Jue et al., “Management of ingested foreign bodies and foodimpactions,”Gastrointestinal Endoscopy, vol. 73, no. 6, pp. 1085–1091, 2011.
[4] F. Altintoprak, B. Degirmenci, E. Dikicier et al., “CT findingsof patients with small bowel obstruction due to bezoar: adescriptive study,”The ScientificWorld Journal, vol. 2013, ArticleID 298392, 6 pages, 2013.
[5] J. C. McKechnie, “Gastroscopic removal of a phytobezoar,”Gastroenterology, vol. 62, no. 5, pp. 1047–1051, 1972.
[6] M. Glatstein, D. Danino, A. Rimon, S. Keidar, and D. Scolnik,“An unusual cause of small bowel obstruction in a child:ingested rhubarb,” Case Reports in Surgery, vol. 2013, Article ID497214, 2 pages, 2013.
[7] G. G. Ginsberg, “Management of ingested foreign objects andfood bolus impactions,” Gastrointestinal Endoscopy, vol. 41, no.1, pp. 33–38, 1995.
[8] C. H. Andrus and J. L. Ponsky, “Bezoars: classification, patho-physiology, and treatment,” The American Journal of Gastroen-terology, vol. 83, no. 5, pp. 476–478, 1988.
[9] K. Y. Kwok, W. T. Siu, B. K. B. Law, H. Y. S. Cheung, J. P. Y.Ha, and M. K. W. Li, “Laparoscopic approach compared withconventional open approach for bezoar-induced small-bowelObstruction,” Archives of Surgery, vol. 140, no. 10, pp. 972–975,2005.
[10] J. E. M. T. deMenezes Ettinger, J. M. Silva Reis, E. L. Q. de Souzaet al., “Laparoscopic management of intestinal obstruction dueto phytobezoar,” Journal of the Society of LaparoendoscopicSurgeons, vol. 11, no. 1, pp. 168–171, 2007.
[11] K. E. Muller, A. Arato, P. L. Lakatos, M. Papp, and G. Veres,“Foreign body impaction in the sigmoid colon: a twenty eurobet,”World Journal of Gastroenterology, vol. 19, no. 24, pp. 3892–3894, 2013.
[12] O. Engin, M. Yildirim, S. Yakan, and G. A. Coskun, “Can fruitseeds and undigested plant residuals cause acute appendicitis,”Asian Pacific Journal of Tropical Biomedicine, vol. 1, no. 2, pp.99–101, 2011.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com