Embed Size (px)
Citation preview

5. Common and rare alleles
Mutation means 1. the process by which a gene undergoes a structural change, 2. a modified gene resulting from mutation
Mutations:-gene mutations-„point“ mutation – only one nucleotide qualitative change-in regulatory sequences quantitative change-compound mutations-chromosomal mutations-numerical-structural

Fig. 1: Destiny of gene mutations (alleles) in populations. How common and rare alleles originate
1

Fig.2
2

A fresh allele (point mutation) is subject to changes in its relative frequency according to the circumstances (its adaptive value in the environment). A polymorphism may be totally neutral, slightly different or (rarely) very different. Rare alleles may produce serious diseases easily
4000 Mendelean conditions, 1/3 of proteins polymorphic, virtually any locus polymorphic regarding DNA
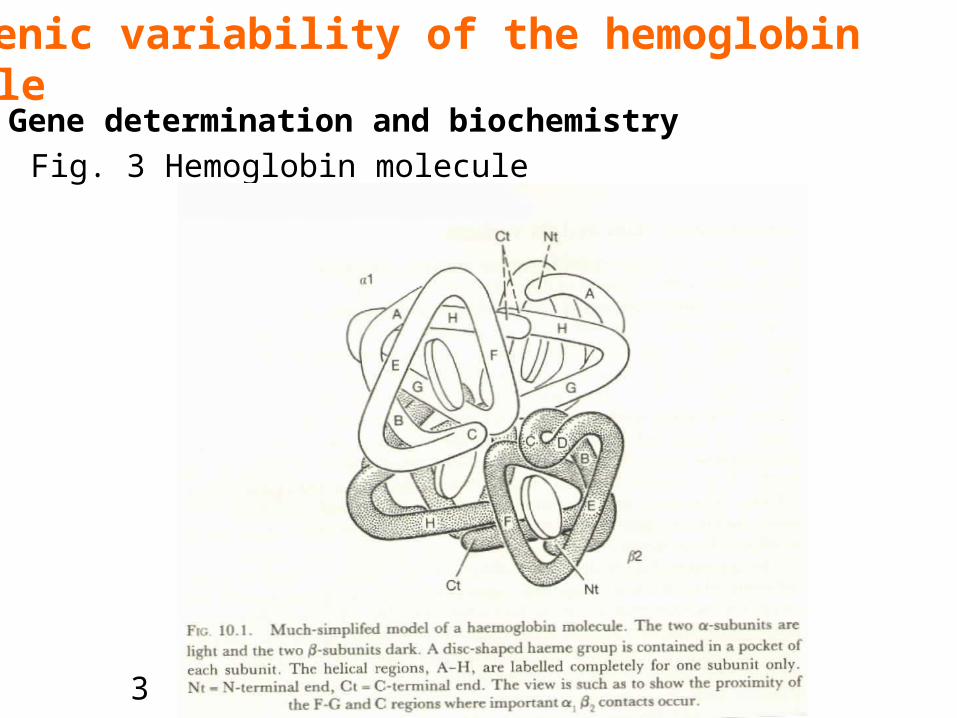
6. Genic variability of the hemoglobin molecule6.1 Gene determination and biochemistry
Fig. 3 Hemoglobin molecule
3

Fig. 4 Genetic detemination of human hemoglobins

Fig. 5 Disposition of Hb genes along chromosomes
Different Hb genes resulted from gene duplications. 1 and 2 the same polypeptide
5

Several hundreds, the majority of them rareFig. 6
6.2 Point mutations of Hb molecule

Hereditary methemoglobinemiasFig. 7 Several alleles – point mutations in the vicinity of heme group. Fe3+ bound to the inappropriate AA methemoglobin reductase unable to reduce it(Mutations of methemoglobin reductase the same „distant“ phenotype)
NeutralDeleterious: doubtless when heterozygotes are diseased, problematic when heterozygotes are not manifestly ill (recessive mutations)

7

Unstable hemoglobinsMutation conformation change instability of
the molecule chronichemolytic anemia. RBC: Heinzbodies, stiffness life span
Changed affinity to oxygenEnhanced affinity shift of the dissociation curve to the left delivering of oxygen to tissues erythrocytosisLowered affinity mild anemiaSmall stereochemical changes in a molecule drastic changes in function
8
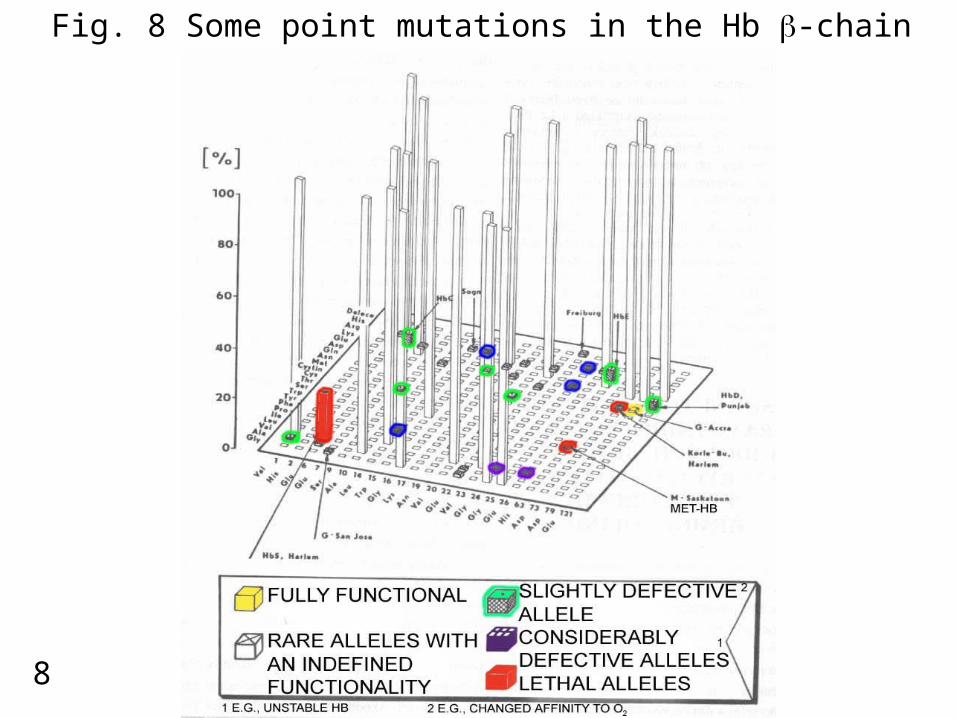
Fig. 8 Some point mutations in the Hb -chain
Hb polymorphismsSickle cell anemia (HbS)
-chain, position 6, Glu Val SCA = homozygosity for HbS - life span, virtually
no descendantsSickle cell trait heterozygosity for HbS - sickle RBC in hypoxic conditions Oxygen affinity Hb oxigenation gelling of Hb sickling of RBC and lowered deformability obturation of capillaries local ischemia etc (Fig. 9
Other polymorphisms: HbC, HbE, HbD, HbK, HbO, HbJ Tongariki – mild problems

9

Adaptive significance of Hb polymorphismsDozens of % in (sub)tropical regions, about 5% in the border localitiesStrong directed selection against HbS its maintaining cannot be caused by drift Plasmodium falciparum stabilizing selection and balanced polymorphism (resistence in small children, blocking of penetration through placenta fertility of heterozygotic women)Other polymorphisms – only probability of enhanced resistance

Compound mutations: Hb HarlemDeletions and additionsConstant Spring Hb: mutation in a stop codon additional 31 AA in the -chain
The same effect as gene deletionLe Pore Hb: mixed chains / and /. Cause: unequal crossing over in meiosis
6.3 Other types of Hb mutations

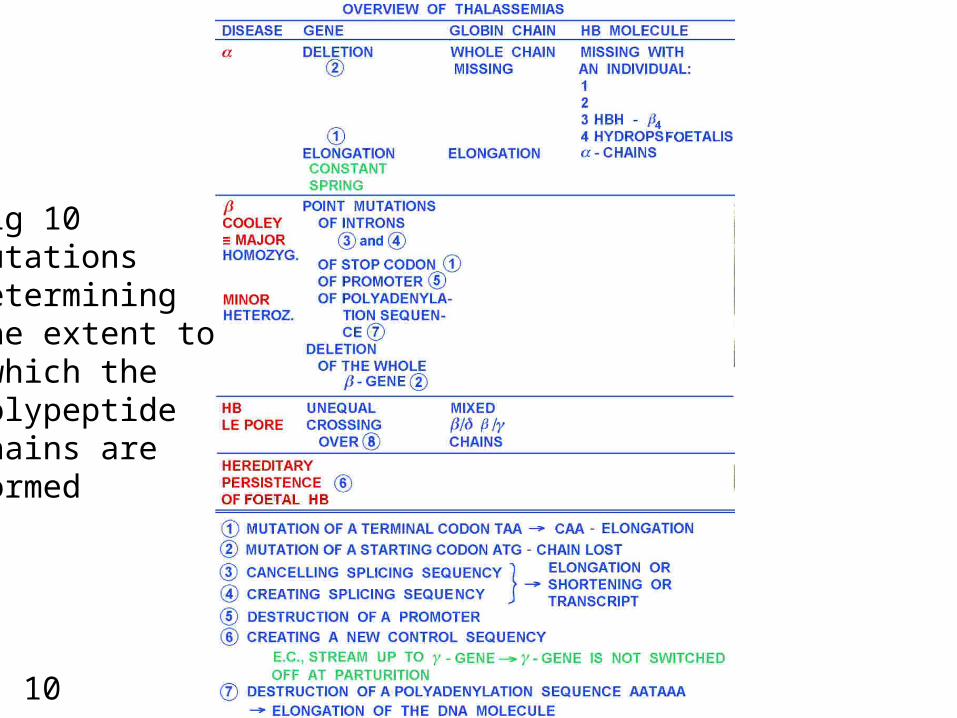
6.4 Thalassemias
10
Fig 10 Mutations determining the extent to which the polypeptide chains are formed

-thalassemia interference with -chain production.Thalassemia major = Cooley´s anemia: Homozygosity for alleles of -chain gene grossly abnormal RBC, unused -chains precipitate RBC destructionThalassemia minor:Heterozygotes, many pathological alleles heterogeneity of the disease (between homozygotes and norm)

Etiology of -thalassemias:- intron mutations - new splicing sequencies GT, AT shortening of the transcript- cancelling of splicing sequencies or destruction of the polyadenylation sequence prolongation of the transcript- mutation of a stop codon chain elongation- mutation of a starting codon or destruction of a promoter complete deletion of the -gene
-thalassemia interference with -chain productionEtiology: -chain gene deletion, 1 – 4

Majority of point mutations are rare, from neutral to grossly pathologicIn non-malaric regions: a single „normal“ Hb - HbA1
(possibly HbA2 with -chains). These alleles are fixed and optimal (neutral)
In malaric regions: a whole array of polymorphisms (balanced polymorphisms) maintained by stabilizing selection
Nearly neutral polymorphisms – a common situation in many genes. Disadvantageous polymorphic alleles must be compensated for, typically by heterozygote advantage
6.5 A survey of adaptive (health) significance of Hb mutations

Izoenzymes: in most cases no known functional explanation of the existence of variants
Pentose shunt pathway NADPH reduced glutathione protection of Hb against oxidationFig.11
Deficiency of the G6PD hemolytic crises after ingestion of Vicia fava (bean), anti-malarials, sulphonamides etc. Fig.12
6.6 Glucose-6-phosphate dehydrogenase G6PD polymorphisms

11

A - acute hemolytic Anemia (AHA)FavismDrugsActivity 0.16 T Africa 0.202 mutat.
2
1
A + asymptom.Activity 0.84Africa 0.25
B – (mediter.)AHA, favismAct. 0.00 – 0.07 TMediter. 0.15 – 0.20Kurdistan Jews 0.55
2
1
B + “normal” G6PD
12

Gd(A+) – 20% in Africa slightly reduced activityGd(A-) – 20% in Africa 8-20% activity drug sensitivityMediterranean (Gd(B-)) – 15 to 20% in Greece, Sardinia, Middle East, India activity less than 7% of norm In all forms the enzyme is unstable (e.g., T1/2 = 13 days instead of 62 days)

Rare diseases- one major gene and allele- Mendelean heredity- severe, in childhood- rare- environmental influences weak
Common diseases- several genes, only slightly deleterious alleles- only enhanced disposition in families- chronic, in adults and elderly- common (mostly „civilization“ diseases)- environmental conditions decisive
Fig. 13 Genetic architecture of essential hypertension
6.7. Common and rare diseases

13





























