Embed Size (px)
Citation preview

525
Bilateral Posterior Cerebral Artery Strokesin a Young Migraine Sufferer
Margaret Moen, MD, Steven R. Levine, MD, Daniel S. Newman, MD,
Anne Dull-Baird, PhD, Gregory G. Brown, PhD, and K.M.A. Welch, MD
We report a young migraine sufferer who developed bilateral posterior cerebral artery territoryinfarcts during the course of his classic migraines, the second of which was associated with intraluminalclot in the posterior cerebral artery. To our knowledge, bilateral posterior cerebral artery stroke fromspontaneous migraine has not been reported. Head computed tomographic, magnetic resonanceimaging, and angiographic correlation is presented. The mechanism of migrainous infarction may bein part explained by caliber changes in arterioles and capillaries leading to flow reduction in the moreproximal conduit arteries combined with the associated coagulopathy that has been previouslydocumented during migraine attacks. (Stroke 1988; 19:525-528)
Ischemic cerebral infarction that occurs during theprogress of a migraine attack is rare and themechanisms are uncertain.1"* Although the neu-
rologic symptoms associated with migraine are mostcommonfy visual,7 localized to the cerebral cortexsupplied by the posterior cerebral artery (PCA),8
ischemic strokes attributed to migraine most commonlyoccur within the territory of the middle cerebralartery.1*"11 Only rarely is arterial occlusion demon-strated on angiography and, paradoxically, most oftenin a single PCA.1"312'13 To our knowledge, bilateral PCAstroke from spontaneous migraine has not been re-ported. We describe a young migraine sufferer withbilateral PCA infarcts, the second of which wasassociated with an intraluminal clot in the PCA. Theangiographic findings in this patient support recentlypostulated novel mechanisms of migrainous stroke,14
which we discuss.
Case ReportA 37-year-old man had suffered from confusional
migraine since the age of 20 years. His attacks alwaysbegan with the acute onset of visual images "shifting"in front of him, associated with scotoma and confusionfor the memory of recent events. These symptomslasted from minutes to hours and were then alwaysfollowed by a mild to moderate bifrontal throbbingheadache, photophobia, and malaise. They generallyoccurred once to twice a month but recently hadincreased in frequency, accompanied by a bifrontalheadache. However, on one occasion his alteredmemory and vision did not disappear. Head computedtomography (CT scan) revealed a left temporo-occipitalinfarct. Catheter vertebral angiography revealed an
From the Center for Cerebrovascular Disease Research, Depart-ment of Neurology (M.M., S.R.L., D.S.N., K.M.A.W.) andDivision of Neuropsychology (A.D-B., G.G.B.), Henry FordHospital, Detroit, Michigan.
Supported in part by National Institutes of Health Grant NS23393and the American Heart Association of Michigan (to S.R.L.).
Address for reprints: Steven R. Levine, MD, Center for Cerebro-vascular Disease Research, Department of Neurology, K- l l , HenryFord Hospital, 2799 Wfest Grand Boulevard, Detroit, MI 48202.
Received July 16, 1987; accepted October 21, 1987.
occluded left PCA (Figure 1). Bilateral carotid angiog-raphy was normal. He was placed on aspirin anddipyridamole. One week later he again noted shiftingvisual images, severe trouble recollecting recentevents, and a more diffuse throbbing headache.
Medical history was unremarkable for head injury,loss of consciousness, cardiac disease, rheumaticfever, coagulopathy, chiropractic manipulation, dys-lipidemia, diabetes mellitus, or hypertension. He hadsmoked 20 cigarettes/day for 10 years.
A sister had suffered from migraines associated withright orbital swelling and blurred vision. A maternaluncle went blind suddenly after a severe headache. Thepatient's mother also had severe migraines.
General physical, neurovascular, and cardiac exam-inations were normal. Neurologic examination re-vealed absent anterograde memory and moderatelyimpaired retrograde memory.
Cognitive function testing conducted 2-3 weeksafter the initial onset of symptoms suggested a severeamnestic syndrome without global cognitive impair-ment. Testing also revealed substantial but incompletedisorientation to time, place, and person, and mildimpairment of digit span and mental tracking. Imme-diately after presentation, the patient reproduced someof the themes and details from paragraph-long passagesand nonverbal designs; 30 minutes later he could recallnone of the content from either set of materials, eventhough strong cues were provided. He obtained aWechsler memory quotient of 64, > 2 SD below hisfull-scale Wechsler intelligence quotient. Althoughtesting revealed him to have mild to moderate impair-ment in verbal fluency, speech-sound perception,visual-motor coordination, and constructional praxis,he displayed normal to superior performance onconcept formation, tactile problem solving, rhythmdiscrimination, and motor speed tests. Adequate scoreson visual search and oral reading tests indicate thathis visual field deficit did not interfere substantiallywith registration of stimuli presented in the memorytests.
There were bilateral superior quadrantanopsias andimpaired vertical saccades in both directions.
by guest on June 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
526 Stroke Vol 19, No 4, April 1988
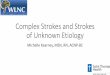
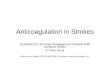
LFIGURE 1. Selective left vertebral angiogram, anterior-posterior view. There is occlusion of left posterior cerebralartery (PCA) (arrow) and paucity of arterial filling distal tooccluded PCA. Right PCA appears normal.
Echocardiography, electrocardiogram, Holter car-diac monitor, complete blood count, platelet count,prothrombin time, activated partial thromboplastintime, factor VIII, factor V, antithrombin HI, protein C,protein S, plasminogen activity and antigen,a-antiplasmin activity, Westergren erythrocyte sedi-
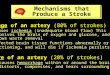
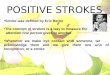
FIGURE 2. Head computed tomogram after contrast infusion.There is low-attenuation region (infarct) in left mesial temporo-occipital area (arrowhead). Contrast-enhancing infarct is seenin right occipital region (arrows).
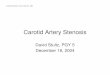
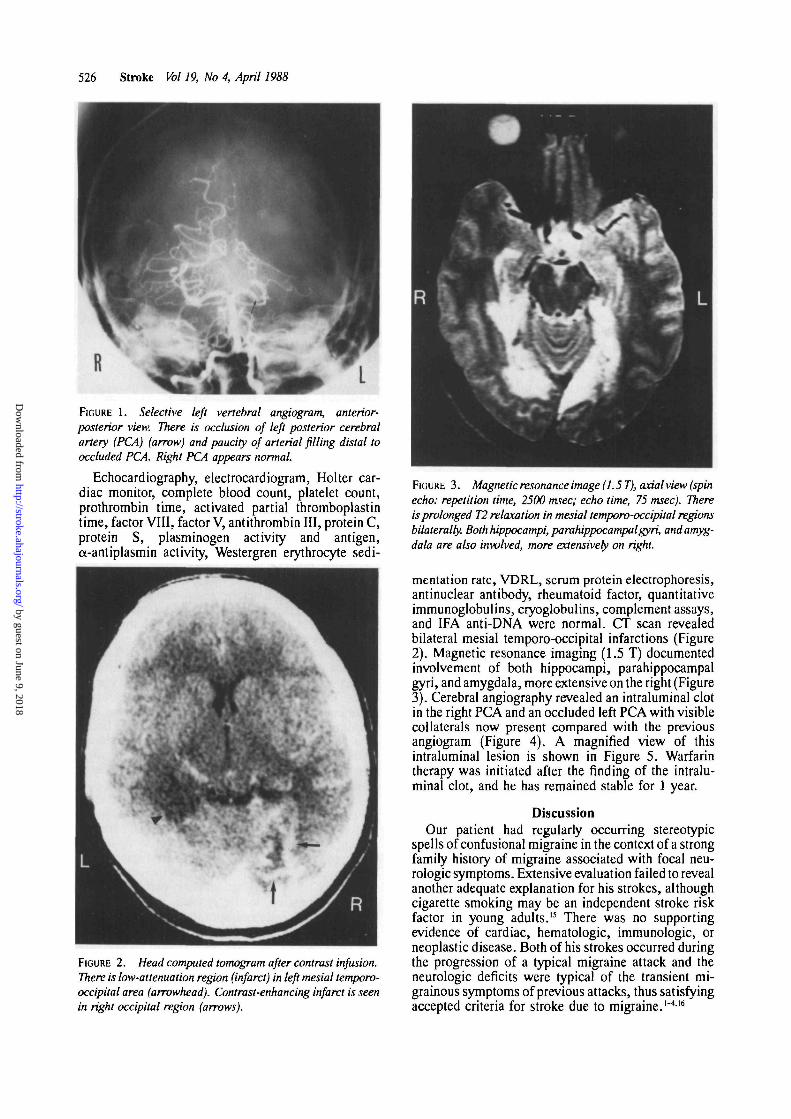
FIGURE 3. Magnetic resonance image (1.5 T), axial view (spinecho: repetition time, 2500 msec; echo time, 75 msec). Thereis prolonged T2 relaxation in mesial temporo-occipital regionsbilaterally. Both hippocampi, parahippocampalgyri, and amyg-dala are also involved, more extensively on right.
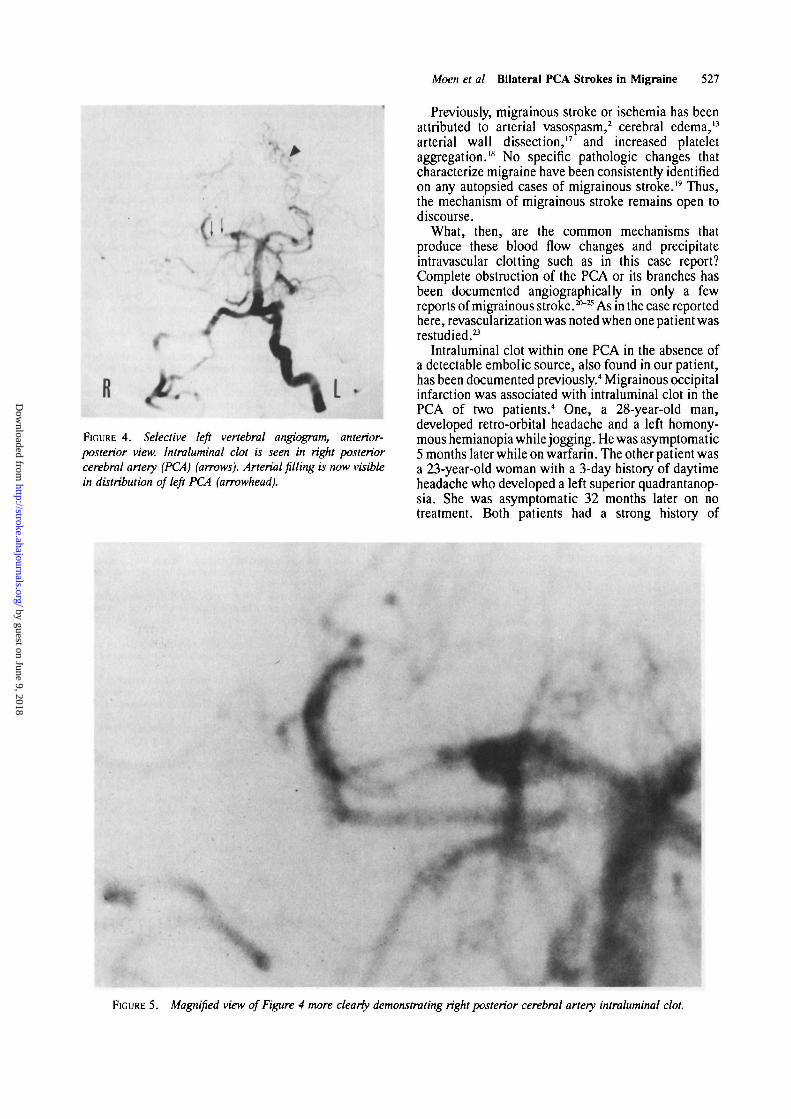
mentation rate, VDRL, serum protein electrophoresis,antinuclear antibody, rheumatoid factor, quantitativeimmunoglobulins, cryoglobulins, complement assays,and IFA anti-DNA were normal. CT scan revealedbilateral mesial temporo-occipital infarctions (Figure2). Magnetic resonance imaging (1.5 T) documentedinvolvement of both hippocampi, parahippocampalgyri, and amygdala, more extensive on the right (Figure3). Cerebral angiography revealed an intraluminal clotin the right PCA and an occluded left PCA with visiblecollaterals now present compared with the previousangiogram (Figure 4). A magnified view of thisintraluminal lesion is shown in Figure 5. Warfarintherapy was initiated after the finding of the intralu-minal clot, and he has remained stable for 1 year.
DiscussionOur patient had regularly occurring stereotypic
spells of confusional migraine in the context of a strongfamily history of migraine associated with focal neu-rologic symptoms. Extensive evaluation failed to revealanother adequate explanation for his strokes, althoughcigarette smoking may be an independent stroke riskfactor in young adults.15 There was no supportingevidence of cardiac, hematologic, immunologic, orneoplastic disease. Both of his strokes occurred duringthe progression of a typical migraine attack and theneurologic deficits were typical of the transient mi-grainous symptoms of previous attacks, thus satisfyingaccepted criteria for stroke due to migraine.1"416
by guest on June 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Moen et al Bilateral PCA Strokes in Migraine 527
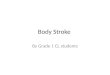
•FIGURE 4. Selective left vertebral angiogram, anterior-posterior view. Intraluminal clot is seen in right posteriorcerebral artery (PCA) (arrows). Arterial filling is now visiblein distribution of left PCA (arrowhead).
Previously, migrainous stroke or ischemia has beenattributed to arterial vasospasm,2 cerebral edema,13
arterial wall dissection,17 and increased plateletaggregation.18 No specific pathologic changes thatcharacterize migraine have been consistently identifiedon any autopsied cases of migrainous stroke." Thus,the mechanism of migrainous stroke remains open todiscourse.
What, then, are the common mechanisms thatproduce these blood flow changes and precipitateintravascular clotting such as in this case report?Complete obstruction of the PCA or its branches hasbeen documented angiographicalry in only a fewreports of migrainous stroke.20"25 As in the case reportedhere, revascularization was noted when one patient wasrestudied.23
Intraluminal clot within one PCA in the absence ofa detectable embolic source, also found in our patient,has been documented previously.4 Migrainous occipitalinfarction was associated with intraluminal clot in thePCA of two patients.4 One, a 28-year-old man,developed retro-orbital headache and a left homony-mous hemianopia while jogging. He was asymptomatic5 months later while on warfarin. The other pat ient wasa 23-year-old woman with a 3-day history of daytimeheadache who developed a left superior quadrantanop-sia. She was asymptomatic 32 months later on notreatment. Both patients had a strong history of
NFIGURE 5. Magnified view of Figure 4 more clearly demonstrating right posterior cerebral artery intraluminal clot.
by guest on June 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
528 Stroke Vol 19, No 4, April 1988
common migraine. Vasospasm was not seen. Coagu-lopathy and cardiac or other embolic sources wereextensively searched for and not found. Only one othercase of migrainous infarction has been reported to haveintraluminal clot.5
O'Brien26 first demonstrated global oligemia thatoutlasted the brief time associated with focal symptomsof the migraine aura. Olesen et al27 has shown thisspreading oligemia during attacks to be analogous tothe spreading depression of Leao. More recent evalu-ations have reported regional cerebral blood flows tobe in the ischemic range during an attack.28 Caliberchange in arterioles and capillaries can in part bemediated by local factors in the vascular wall, inde-pendent of blood flow,29 and by neurogenic factors.30 Ifthe smaller resistance vessels are involved in theputative spreading depolarization of the migrainousprocess, flow reduction in the more proximal, largerconduit arteries such as the proximal PCA could beexplained by altered downstream resistance. This,combined with the previously reported serum plateletfactor abnormalities in young adults with cerebralinfarction secondary to migraine,18 may produce bloodflow stasis leading to intraluminal clot.
Note added in proof. Since submission of thismanuscript, three additional reports of migrainousstroke have appeared, none with documented bilateralPCA strokes.31"33 Bogousslavsky et al31 reported 22patients, 19 with normal angiograms; 9 had PCAinfarcts. Rothrock et al32 reported 22 patients, 5 of 12with abnormal angiograms, primarily "spasm." Onepatient had PCA "beading." Broderick and Swanson33
reported 20 patients. Five of 12 had abnormal angio-grams including one each with intraluminal clot andfilling defect.
AcknowledgmentsWe thank Ms. Hairy Phelps for secretarial assistance
and Mr. Jim Latif for photographic assistance.
References1. Featherstone HJ: Clinical features of stroke in migraine. A
review. Headache 1986;26:128-1332. Mas JL, Baron JC, Bousser MG, Chiras J: Stroke, migraine and
intracranial aneurysm. A case report. Stroke 1986;17:1019-1021
3. Bousser MG, Baron JC, Chiras J: Ischemic strokes andmigraine. Neuroradiology 1985;27:583-587
4. Pessin MS, Lathi ES, Cohen EB, Kwan ES, Hedges TR,Caplan LR: Clinical features and mechanisms of occipitalinfarction. Ann Neurol 1987;21:29O-299
5. Rascol A, Caubier J, Guiraud B, Manelfe C, David J, ClanetM: Accidents s ische"miques ce're'braux au cours de crisesmigraineuses. A propos des migraines compliqu6es. Rev Neurol1979;135:867-884
6. Edmeads J: Stroke in migraine (editorial). Headache1986;26:149-150
7. Manzoni GC, Farina S, Lanfranchi M, Solari A: Classicmigraine: Clinical findings in 164 patients. Eur Neurol1985;24:163-169
8. Fisher CM: The posterior cerebral artery syndrome. Can JNeurol Sci 1986;13:232-239
9. Cola LA, Mastaglia FL: CT findings in patients with migrain-nous headaches. Br Med J 1976;2:149-150
10. Hungerford GD, DuBoulay GH, Zikha KJ: Computerized axialtomography in patients with severe migraine: A preliminaryreport. J Neurol Neurosurg Psychiatry 1976;39:990-994
11. Guest LA, Woolf AL: Fatal infarction of brain in migraine. BrMedJ 1964;l:225-226
12. Dukes HT, Vieth RG: Cerebral arteriography during migrainesyndrome and headache. Neurology 1964;14:636-639
13. Wolff HG: Headache and Other Head Pain. New York, OxfordUniversity Press, 1972, pp 270-271
14. Welch KMA: Migraine: A biobehavioral disorder. Arch Neurol1987;44:323-327
15. Bonita R, Scragg R, Stewart A, Jackson R, Beaglehole R:Cigarette smoking and risk of premature stroke in men andwomen. Br Med J 1986;293:6-8
16. Fisher CM: Cerebral ischemia. Less familiar types. ClinNeurosurg 1971;18:267-335
17. Sinclair W: Dissecting aneurysm of the middle cerebral arteryassociated with migraine syndrome. Am J Pathol 1953;29:1083-1091
18. Shah AB, Coull BM, Beamer NB: In vivo platelet activationand strokes in young adults with migraine (abstract). Neurology1983;33(suppl 2):206
19. Tatemichi TK, Mohr JP: Migraine and stroke, in Barnett HJM,Mohr JP, Stein BM, Yatsu FM (eds): Stroke, Pathophysiology,Diagnosis, and Management. New York, Churchill Living-stone, 1986, vol 2, ch 42, pp 845-868
20. Brain Sir R: Cerebral vascular disorders. Lancet 1954;1:831-833
21. Buckle RM, DuBoulay G, Smith B: Death due to cerebralvasospasm. / Neurol Neurosurg Psychiatry 1964;27:440-444
22. Dorfman LJ, Marshall WH, Enzmann DR: Cerebral infarctionand migraine; clinical and radiologic correlations. Neurology1979;29:317-322
23. Connor RCR: Complicated migraine. A study of permanentneurological and visual defects caused by migraine. Lancet1962;2:1072-1075
24. Kaul SN, DuBoulay GH, Kendall BE, Russel WR: Relation-ship between visual field defect and arterial occlusion in theposterior cerebral circulation. J Neurol Neurosurg Psychiatry1974;37:1022-1030
25. Ment LR, Duncan CC, Parsells PR, Collins FC: Evaluation ofcomplicated migraine in childhood. Childs Brain 1980;7:261-266
26. O'Brien MD: The relationship between aura symptoms andcerebral blood flow changes in the prodrome of migraine, inProceedings of the International Headache Symposium. Elsi-nore, March 16-18, 1971, pp 141-143
27. Olesen J, Larsen B, Lauritzen M: Focal hyperemia followed byspreading oligemia and impaired activation of rCBF in classicmigraine. Ann Neurol 1981;9:344-352
28. Olsen TS, Friberg L, Lasen NA: Ischemia may be the primarycause of the neurologic deficits in classic migraine. Arch Neurol1987;44:156-161
29. Segal SS, Duling BR: Flow control among microvesselscoordinated by intracellular conduction. Science 1986;234:868-870
30. Burnstock G: Neurogenic control of cerebral circulation.Cephalalgia 1985;5(suppl 2):25-33
31. Bogousslavsky J, Regli F, Van Melle G, Payot M, Uske A:Migraine stroke. Neurology 1988;38:223-227
32. Rothrock JF, Walicke P, Swenson MR, Lyden PD, Logan WR:Migrainous stroke. Arch Neurol 1988;45:63-67
33. Broderick JP, Swanson JW: Migraine-related strokes. ArchNeurol 1987;44:868-871
KEY WORDS • cerebrovascular disordersvertebrobasilar circulation
migraine
by guest on June 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from
M Moen, S R Levine, D S Newman, A Dull-Baird, G G Brown and K M WelchBilateral posterior cerebral artery strokes in a young migraine sufferer.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1988 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.19.4.525
1988;19:525-528Stroke.
http://stroke.ahajournals.org/content/19/4/525World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 9, 2018http://stroke.ahajournals.org/
Dow
nloaded from