Embed Size (px)
Citation preview
NATURE MEDICINE • VOLUME 7 • NUMBER 7 • JULY 2001 775
NEWS & VIEWS
Nicotine has been well established as theaddictive component of cigarette
smoke. Nicotine-releasing devices, such aspatches, gums, inhalers and nasal sprays,are used increasingly to aid smoking cessa-tion. In addition, nicotine is being investi-gated to treat pathologies such as Alzheimerdisease, Parkinson disease, ulcerative colitisand sleep disorders. In this issue, Heeschenet al.1 show that in the absence of smoking,nicotine stimulates angiogenesis in murinemodels of inflammation, ischemia, athero-sclerosis and cancer. Morever, nicotine ac-celerates the growth of atheroscleroticplaques and lung cancer and restores bloodflow to ischemic limbs in mice.Considering the critical role that angiogen-esis has in many diseases2 and the increas-ing therapeutic use of nicotine, the study byHeeschen et al. is significant and timely.
The findings build on earlier work byVillablanca, which showed that nicotine,at concentrations found in the plasma ofsmokers, stimulates DNA synthesis in andproliferation of endothelial cells in vitro vianicotinic acetylcholine receptors (nAChR)on endothelial cells3. At the time,Villablanca proposed that the “results maybe important in tumor angiogenesis,atherogenesis and vascular dysfunction insmokers.” Heeschen et al. now provide thefirst in vivo data to support this hypothesis.
The authors first show that in addition tobeing mitogenic, nicotine is a survival fac-tor for endothelial cells in vitro (that is, it re-duces apoptosis of cells under hypoxia),and induces endothelial cells to form capil-
lary-like networks in collagen gels. Thesefunctions of nicotine, reminiscent of thoseof the vascular endothelial growth factor(VEGF), a critical angiogenic molecule2,can be blocked by hexamethonium, a spe-cific antagonist of nAChR (Fig. 1).
Heeschen et al. then tested the angio-genic capacity of nicotine in four in vivomurine models, all of which had interest-ing results. First, nicotine increased angio-genesis in polymer discs implanted in theflanks of mice. Second, nicotine increasedthe capillary density as well as the numberand diameter of collateral vessels in is-chemic hind limbs; the structural changeswere accompanied by functional improve-ments in blood flow. Third, nicotine in-creased vascularization in Lewis lungcarcinomas grown subcutaneously and inthe lungs. The increase in angiogenesis was
Clearing the smoke on nicotine and angiogenesisNicotine is widely used as an aid to smoking cessation and is being evaluated to treat non-smoking related disorders. Stimulation
of angiogenesis by nicotine raises many questions about its mechanism of action and use in therapy. (pages 833-839)
RAKESH K. JAIN
and CD40L– apoptotic cells and vinculin-specific CD8+ T cells in HIV-infected pa-tients. They demonstrate in a panel ofHIV-infected patients a strong correlationbetween the presence of circulatingCD40L+ apoptotic cells and the ability ofCD8+ T cells to express vinculin-specific cy-tolytic activity. Based on this finding, theauthors argue that the development of thisself-reactive CD8+ T-cell response duringHIV infection is regulated by the availabil-ity of CD40L+ apoptotic cells, which arepresumably the source of vinculin taken upand presented by dendritic cells to CD8+ Tcells in vivo. They speculate further that theCD40L– apoptotic cells generated duringHIV-infection could suppress the autoreac-tive response. As uptake of these apoptoticcells by immature dendritic cells would notprovide a dendritic cell maturation signal,the immature dendritic cells displayingvinculin peptides would deliver an anergic(tolerizing) signal to autoreactive CD8+ Tcells, rendering them unresponsive to asubsequent activating stimulus (Fig. 1).Thus, the balance between CD40L+ andCD40L– apoptotic cells during HIV infec-tion would dictate the presence and mag-nitude of an autoreactive T-cell response
The findings in this report provide aplausible explanation for the developmentof vinculin-specific, autoreactive CD8+ T-cell responses during HIV infection bycross-priming. However, a number of criti-cal issues remain unresolved and call into
question the general applicability of cross-priming in the development of autoim-mune diseases or even in the generation ofCD8+ T-cell responses to foreign proteins,such as viral antigens. First and foremost isthe issue of the quantity of foreign or selfprotein that must be delivered by the apop-totic cells. Is it simply a numbers game,where protein expression by the apoptoticcell has to be above a set threshold, or dothe apoptotic cells deliver the protein toimmature dendritic cells through a unique,highly efficient and highly regulated, butas yet undefined, presentation pathway?Also, the role of CD4+ T-cell ‘help’ in the in-duction of CD8+ T-cell responses by cross-priming is unclear. The results in thisreport imply that activated CD4+ T cellssimply serve as an alternative source ofCD40L necessary for dendritic-cell matura-tion. Prapato et al. also suggest that the up-take of apoptotic cells (regardless of CD40Lstatus) by dendritic cells in the presence ofan ongoing inflammatory stimulus, suchas virus infection, might result in the si-multaneous induction of both an antiviraland an autoreactive CD8+ T-cell response.However, whether autoimmune responsesduring microbial infection represent thespontaneous activation of genuine self-re-active T cells or reflect the cross-reactivitybetween microbial and self proteins re-mains subject of debate.
It is clear that self-reactive T cells are nor-mally present in our bodies. Cell death by
apoptosis might represent one stimulus bywhich these potentially self-destructive Tcells are awakened and returned to life.
1. Townsend, A.R., Gotch, F.M. & Davey, J. Cytotoxic Tcells recognize fragments of the influenza nucleopro-tein. Cell 42, 457–467 (1985).
2. Kaech, S.M. & Ahmed, R. Memory CD8+ T cell differ-entiation: Initial antigen encounter triggers a develop-mental program in naive cells. Nat. Immunol. 2,415–422 (2001).
3. Braciale, T.J. et al. Antigen presentation pathways toclass I and class II MHC-restricted T lymphocytes.Immunol. Rev. 98, 95–114 (1987).
4. Watts, C. & Powis, S. Pathways of antigen processingand presentation. Rev. Immunogenet. 1, 60–74.(1999).
5. Propato, A. et al. Apoptotic cells overexpress vinculinand induce vinculin-specific cytotoxic T cell cross-priming, depending on their capacity to activate den-dritic cells. Nature Med. 7, 807–813 (2001).
6. Bevan, M.J. Cross-priming for a secondary cytotoxicresponse to minor H antigens with H-2 congenic cellswhich do not cross-react in the cytotoxic assay. J. Exp.Med. 143, 1283–1288 (1976).
7. Albert, M.L., Sauter, B. & Bhardwaj, N. Dendritic cellsacquire antigen from apoptotic cells and induce classI-restricted CTLs. Nature 392, 86–89 (1998).
8. Banchereau, J. & Steinman, R.M. Dendritic cells andthe control of immunity. Nature 392, 245–252(1998).
9. di Marzo Veronese, F. et al. Autoreactive cytotoxic Tlymphocytes in human immunodeficiency virus type1-infected subjects. J. Exp. Med. 183, 2509–2516(1996).
10. Heath, W.R. & Carbone, F.R. Cross-presentation, den-dritic cells, tolerance and immunity. Annu. Rev.Immunol. 19, 47–64 (2001).
University of Virginia Health Science CenterCarter Immunology CenterDepartments of Pathology and MicrobiologyCharlottesville, Virginia, USAEmail: [email protected]
©20
01 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://m
edic
ine.
nat
ure
.co
m© 2001 Nature Publishing Group http://medicine.nature.com
776 NATURE MEDICINE • VOLUME 7 • NUMBER 7 • JULY 2001
NEWS & VIEWS
chorio-allantoic membranes to nicotine so-lution (1 × 10–4 to 1 × 10–8 M) did not affectangiogenesis or extracellular matrix depo-sition6, nor did a two-year exposure ofhealthy rats to inhaled nicotine result ingross vascular or cardiac pathology7. Andtransdermal nicotine administration didnot increase the number of primary coro-nary events in patients with cardiac dis-ease8. To reconcile their results with theseearlier findings, Heeschen et al. propose,without providing experimental evidence,that nicotine stimulates angiogenesis onlyin pathological and not physiological set-tings. Although this conclusion suggeststhat nicotine-induced angiogenesis mightbe useful in treating certain conditions,two findings caution against the long-termuse of nicotine for therapeutic angiogene-sis: Hecht et al.9 showed that certainmetabolites of nicotine are carcinogenicand Gullino10 showed that angiogenic ca-pacity is acquired during neoplastic trans-formation. It is likely that the balancebetween beneficial and detrimental effectsof nicotine will depend upon the dose,schedule, duration of exposure, target tis-sue/cells and genetic profile of the host.
Finally, how does this study affect ourunderstanding of smoking-related vasculardiseases? Nicotine is only one of nearly4,000 chemicals in cigarette smoke.Although nicotine might have an angio-genic effect in some contexts, there are sev-eral molecules in cigarette smoke, such ascadmium and reactive oxygen species,which are toxic to endothelial cells anddetrimental to health. Hence, the net effectof cigarette smoke is anti-vascular, as nu-merous studies have indicated11. Rapidlydeveloping genomics and proteomics tech-nologies should provide insight into the ef-fect of different chemicals in smoke ongene expression and function.
1. Heeschen, C. et al. Nicotine stimulates angiogene-sis: A pathophysiolgical link to cancer and athero-sclerosis. Nature Med. 7, 833–839 (2001).
2. Carmeliet, P. & Jain, R.K. Angiogenesis in cancer andother diseases. Nature 407, 249–257 (2000).
3. Villablanca, A.C. Nicotine stimulates DNA synthesisand proliferation in vascular endothelial cells in vitro. J.Appl. Physiol. 84, 2089–2098 (1998).
4. Pratico, D., Tillmann, C., Zhang, Z.B., Li, H. &FitzGerald, G.A. Acceleration of atherogenesis byCOX-1-dependent prostanoid formation in low den-sity lipoprotein receptor knockout mice. Proc. Natl.Acad. Sci. USA 98, 3358–3363 (2001).
5. Cucina, A. et al. Nicotine-induced smooth muscle cellproliferation is mediated through bFGF and TGF-β1.Surgery 127, 316–322 (2000).
6. Melkonian, G., Le, C., Zheng, W., Talbot, P. &Martins-Green, M. Normal patterns of angiogenesisand extracellular matrix deposition in chick chorioal-lantoic membranes are disrupted by mainstream andsidestream cigarette smoke. Toxicol. Appl. Pharmacol.163, 26–37 (2000).
7. Waldum, H.L. et al. Long-term effects of inhaled nico-
accompanied by increases in tumor growthrate and VEGF production, although nico-tine had no direct effect on the Lewis lungcancer cells. Finally, nicotine increased thevascularization and growth of atheroscle-rotic plaques in the aortic sinus of ApoE-de-ficient mice. Collectively, these findings ofnicotine-induced angiogenesis in differentpathological settings raise several questionsabout nicotine’s mechanism of action andpossible clinical implications.
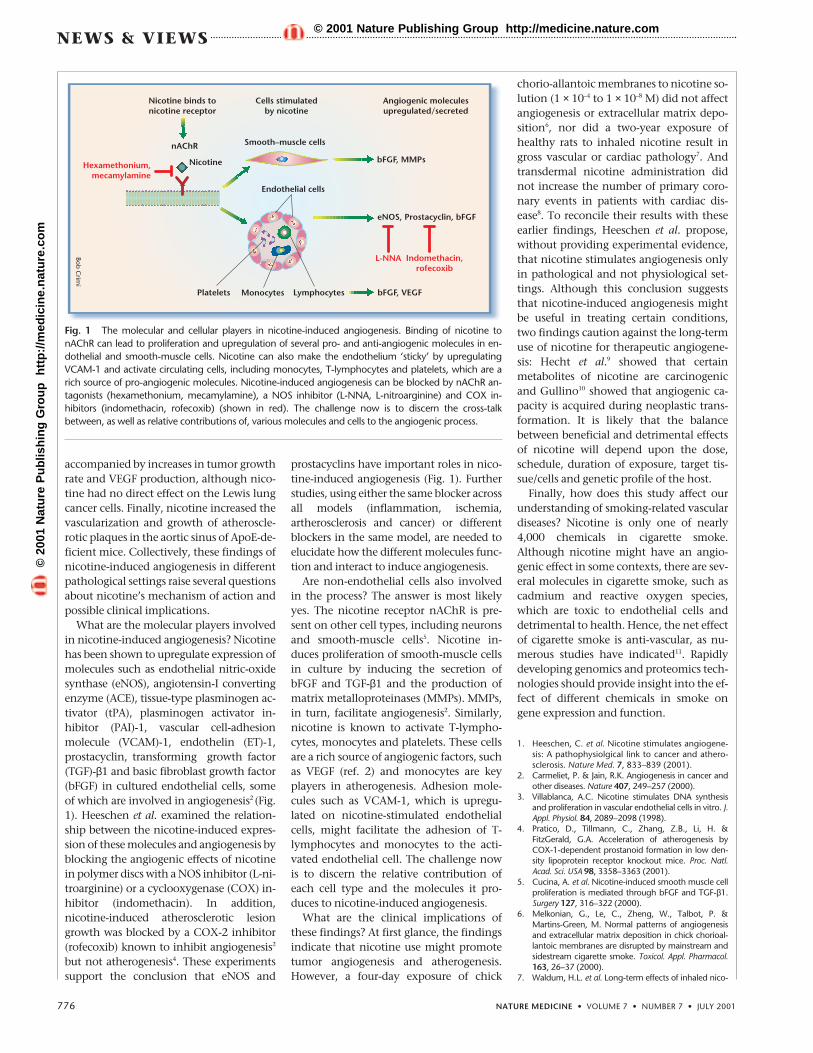
What are the molecular players involvedin nicotine-induced angiogenesis? Nicotinehas been shown to upregulate expression ofmolecules such as endothelial nitric-oxidesynthase (eNOS), angiotensin-I convertingenzyme (ACE), tissue-type plasminogen ac-tivator (tPA), plasminogen activator in-hibitor (PAI)-1, vascular cell-adhesionmolecule (VCAM)-1, endothelin (ET)-1,prostacyclin, transforming growth factor(TGF)-β1 and basic fibroblast growth factor(bFGF) in cultured endothelial cells, someof which are involved in angiogenesis2 (Fig.1). Heeschen et al. examined the relation-ship between the nicotine-induced expres-sion of these molecules and angiogenesis byblocking the angiogenic effects of nicotinein polymer discs with a NOS inhibitor (L-ni-troarginine) or a cyclooxygenase (COX) in-hibitor (indomethacin). In addition,nicotine-induced atherosclerotic lesiongrowth was blocked by a COX-2 inhibitor(rofecoxib) known to inhibit angiogenesis2
but not atherogenesis4. These experimentssupport the conclusion that eNOS and
prostacyclins have important roles in nico-tine-induced angiogenesis (Fig. 1). Furtherstudies, using either the same blocker acrossall models (inflammation, ischemia,artherosclerosis and cancer) or differentblockers in the same model, are needed toelucidate how the different molecules func-tion and interact to induce angiogenesis.
Are non-endothelial cells also involvedin the process? The answer is most likelyyes. The nicotine receptor nAChR is pre-sent on other cell types, including neuronsand smooth-muscle cells5. Nicotine in-duces proliferation of smooth-muscle cellsin culture by inducing the secretion ofbFGF and TGF-β1 and the production ofmatrix metalloproteinases (MMPs). MMPs,in turn, facilitate angiogenesis2. Similarly,nicotine is known to activate T-lympho-cytes, monocytes and platelets. These cellsare a rich source of angiogenic factors, suchas VEGF (ref. 2) and monocytes are keyplayers in atherogenesis. Adhesion mole-cules such as VCAM-1, which is upregu-lated on nicotine-stimulated endothelialcells, might facilitate the adhesion of T-lymphocytes and monocytes to the acti-vated endothelial cell. The challenge nowis to discern the relative contribution ofeach cell type and the molecules it pro-duces to nicotine-induced angiogenesis.
What are the clinical implications ofthese findings? At first glance, the findingsindicate that nicotine use might promotetumor angiogenesis and atherogenesis.However, a four-day exposure of chick
Fig. 1 The molecular and cellular players in nicotine-induced angiogenesis. Binding of nicotine tonAChR can lead to proliferation and upregulation of several pro- and anti-angiogenic molecules in en-dothelial and smooth-muscle cells. Nicotine can also make the endothelium ‘sticky’ by upregulatingVCAM-1 and activate circulating cells, including monocytes, T-lymphocytes and platelets, which are arich source of pro-angiogenic molecules. Nicotine-induced angiogenesis can be blocked by nAChR an-tagonists (hexamethonium, mecamylamine), a NOS inhibitor (L-NNA, L-nitroarginine) and COX in-hibitors (indomethacin, rofecoxib) (shown in red). The challenge now is to discern the cross-talkbetween, as well as relative contributions of, various molecules and cells to the angiogenic process.
eNOS, Prostacyclin, bFGF
Nicotine binds tonicotine receptor
Cells stimulatedby nicotine
Angiogenic moleculesupregulated/secreted
nAChR
NicotineHexamethonium,mecamylamine
Platelets Monocytes Lymphocytes
Smooth–muscle cells
Endothelial cells
bFGF, MMPs
bFGF, VEGF
L-NNA Indomethacin,rofecoxib
Bob C
rimi
©20
01 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://m
edic
ine.
nat
ure
.co
m© 2001 Nature Publishing Group http://medicine.nature.com
NATURE MEDICINE • VOLUME 7 • NUMBER 7 • JULY 2001 777
NEWS & VIEWS
When a virus infects a host cell, thehost’s immune system swings into
action. Antiviral immunity is mediated di-rectly both by CD8+ cytotoxic T lympho-cytes (CTLs), which kill infected cellsexpressing viral peptides bound to majorhistocompatibility complex (MHC) class Imolecules on their surface, as well as byneutralizing antibodies.
Viruses that persist in the face of this im-mune onslaught have evolved many eva-sion mechanisms. For example, viruseswith large DNA genomes encode proteinsthat can subvert the presentation of viralpeptide antigens on the infected cell sur-face. In contrast, RNA viruses with muchsimpler genomes are restricted in their abil-ity to encode such decoy molecules, butsuccessfully escape immune attack in otherways.
Although viral escape from host CTL re-sponses through antigenic mutation hasbeen documented1, in this issue, Ciurea etal.2 report the first systematic attempt tosearch for the emergence of new viral vari-ants that evade the activity of CD4+ lym-phocytes, which are responsible for theactivation of neutralizing antibodiesand the maintenance of CTL re-sponses.
Genetic variability in RNA virusesstems primarily from a lack of errorcorrection mechanisms in RNA repli-cases3. However, much of the result-ing variation is detrimental to thevirus. Occasional mutations can con-fer a survival advantage if they alterantigens targeted by the immunesystem4. The first demonstration ofviral escape from host CTL responsesthrough antigenic mutation was pro-vided by studies of mice which havea single T-cell–receptor transgenethat recognizes a MHC class I-restricted peptide from lympho-cytic choriomeningitis virus(LCMV)1. In this model, the CTL re-sponse is monoclonal and restrictedto one viral epitope. After infection
with high doses of LCMV, mutations in theepitope-encoding region that abrogatedrecognition by the transgenic CTL wereprevalent in the persisting viral population.Subsequent studies have validated the useof transgenic systems to investigate im-mune selection pressures by showing thatvariants carrying CTL escape mutationscan have an evolutionary advantage in nat-ural RNA virus infections of hosts with un-manipulated T-cell receptor repertoires4.Similar reports have demonstrated muta-tional escape from polyclonal neutralizing-antibody–mediated pressure in accessibleviral proteins6.
CD4+ T lymphocytes are generally re-garded as ‘helper’ cells. These cells are acti-vated when they engage antigenic peptidesbound to MHC class II molecules on thesurface of specialized antigen-presentingcells (APCs)5. CD4+ T-cell help is requiredfor both the induction of mature B-cell re-sponses, leading to the production of neu-
tralizing antibodies, and the maintenanceof effective virus-specific CTL responses.Thus, CD4+ T cells often have an indirectrole in antiviral immunity.
Mutations can arise within MHC class II-restricted epitopes that diminish recogni-tion by virus-specific CD4+ T cells7, but it isuncertain whether such mutations confer aselection advantage in the host environ-ment. If viral mutation caused sustainedloss of CD4+ T-cell responses, then thiscould seriously impair humoral and CTL-mediated effector mechanisms.
Ciurea et al. used two models of LCMVinfection designed to limit virus-specific T-cell responses to the CD4+ population.Mice depleted of CD8+ T lymphocytes wereinoculated with low doses of LCMV.Although infection persisted under viremiccontrol for 100 days, LCMV recrudesced inthe blood of two mice. This was associatedwith a single non-synonymous nucleotidemutation located within a dominant MHCclass II-restricted CD4+ T-cell epitope in theenvelope glycoprotein GP-1 (residues61–80) in all virus isolates. There was novariation within regions of GP-1 typically
targeted by neutralizing antibodies.These preliminary findings indi-
cated that mutations within domi-nant CD4+ T-cell epitopes mightcontribute to loss of viremic con-trol. However, the presence of neu-tralizing antibody activity and thepolyclonal nature of the CD4+ T-cellresponse precluded definitive inter-pretation of this result. Hence, toaddress the effects of focused CD4+
T-cell activity on the viral popula-tion in relative isolation, spleno-cytes from SMARTA mice, in whichCD4+ T-cell activity is restricted tothe immunodominant GP61-80epitope, were injected into neona-tally infected B6 LCMV-carrier mice.Persistent virus in this recipientstrain is recognized as ‘self’, and in-duces both CD8+ and CD4+ T-celltolerance through thymic deletion.
CD4+ T cells: The great escapeMutation is one way in which RNA viruses evade the destructive actions of CD8+ cytotoxic lymphocytes. New
research shows that they employ the same method to escape attack by CD4+ T cells. (pages 795–800)
RODNEY E. PHILLIPS, GILLIAN C.HARCOURT & DAVID A. PRICE
B cell +
Loss of help
Loss of help
Loss of antiviral effectorfunction (mainly non-lytic)
Antigen presenting cell
CD4+ cell
cell+
Infected target cell
CD8
Viral mutation within the infected host
Failure of neutralizingantibody
Viron
Loss of antiviraleffector function(lytic & non-lytic)
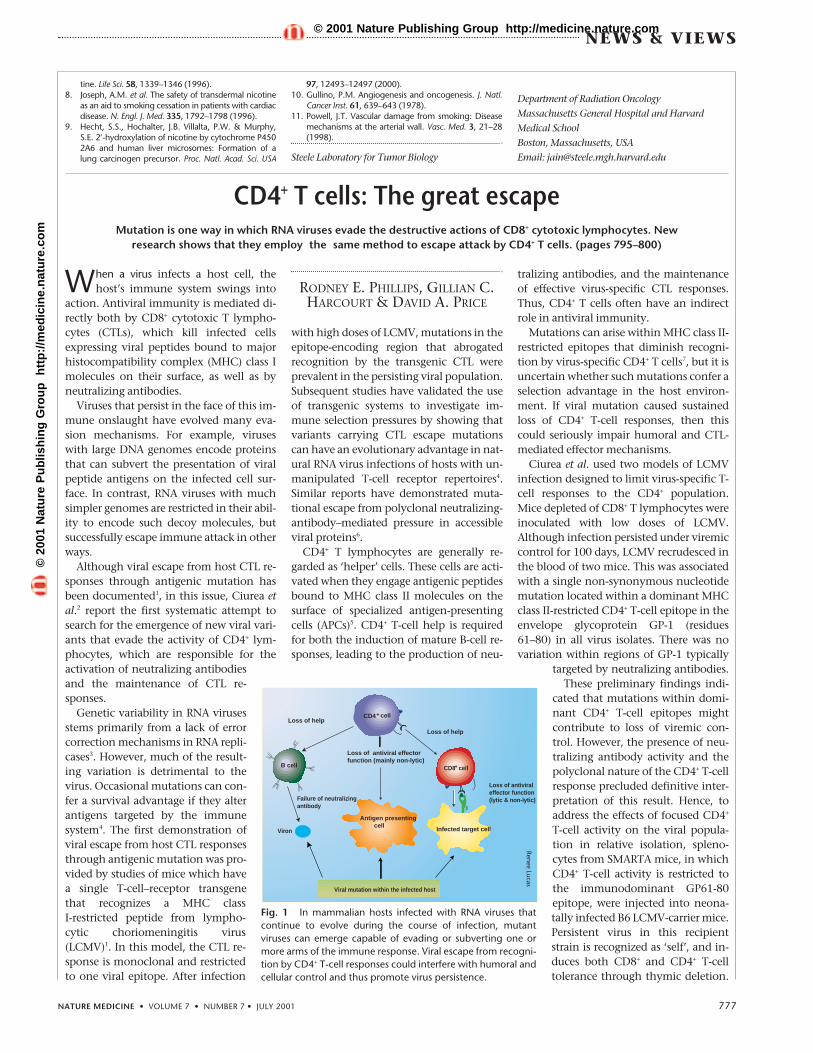
Fig. 1 In mammalian hosts infected with RNA viruses thatcontinue to evolve during the course of infection, mutantviruses can emerge capable of evading or subverting one ormore arms of the immune response. Viral escape from recogni-tion by CD4+ T-cell responses could interfere with humoral andcellular control and thus promote virus persistence.
tine. Life Sci. 58, 1339–1346 (1996).8. Joseph, A.M. et al. The safety of transdermal nicotine
as an aid to smoking cessation in patients with cardiacdisease. N. Engl. J. Med. 335, 1792–1798 (1996).
9. Hecht, S.S., Hochalter, J.B. Villalta, P.W. & Murphy,S.E. 2′-hydroxylation of nicotine by cytochrome P4502A6 and human liver microsomes: Formation of alung carcinogen precursor. Proc. Natl. Acad. Sci. USA
97, 12493–12497 (2000).10. Gullino, P.M. Angiogenesis and oncogenesis. J. Natl.
Cancer Inst. 61, 639–643 (1978).11. Powell, J.T. Vascular damage from smoking: Disease
mechanisms at the arterial wall. Vasc. Med. 3, 21–28(1998).
Steele Laboratory for Tumor Biology
Department of Radiation OncologyMassachusetts General Hospital and HarvardMedical SchoolBoston, Massachusetts, USAEmail: [email protected]
Renee Lucas
©20
01 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://m
edic
ine.
nat
ure
.co
m© 2001 Nature Publishing Group http://medicine.nature.com