Embed Size (px)
Citation preview

THE EFFECT OF ADRENOCORTICOTROPHICHORMONEONCHILDREN WITH THE NEPHROTICSYNDROME. II.
PHYSIOLOGIC OBSERVATIONSON DISCRETEKIDNEY FUNCTIONSANDPLASMA
VOLUME1
By HENRYL. BARNETT, CAROLYNW. FORMAN,2 HELEN McNAMARA,AND WALLACEW. McCRORY8
(From The New York Hospital and the Department of Pediatrics, Cornell University MedicalCollege, New York City)
AND
By MILTON RAPOPORT,ALEXANDERJ. MICHIE, AND GUILIO BARBERO
(From The Children's Hospital of Philadelphia and the Department of Pediatrics, and HarrisonDepartment of Surgical Research, School of Medicine, University of Pennsylvania,
Philadelphia)
(Submitted for publication September 12, 1950; accepted, December 4, 1950)
INTRODUCTION
Inability to predict the time of occurrence ofspontaneous diureses in the nephrotic syndromehas retarded investigations of the physiologicchanges which may precede, accompany, and fol-low these heartening but enigmatic events. It hasbeen demonstrated recently that several agents(1-5) are capable of inducing diureses at a pre-dictable time in a far higher percentage of trialsthan could be attributed to chance. Adrenocorti-cotrophic hormone (ACTH) is one such agent,and the abrupt, profuse, and sustained diureseswhich may accompany or follow its administrationare clinically similar to the dramatic diureses whichoccur spontaneously. Clinical observations on theeffect of ACTH4 on a group of children with thenephrotic syndrome is the subject of a separate re-port (6) in which the possible clinical significanceof the results is also discussed. Serial physiologicmeasurements were made on selected patients be-fore, during, and after administration of ACTH.These observations were directed toward an in-creased understanding of the syndrome itself andespecially of the mechanism of diuresis rather than
1 Presented in part before the Society of Pediatric Re-search at French Lick, Indiana, on May 9, 1950.
2 Public Health Service Postdoctorate Fellow, 1949-51.3 Lewis Cass Ledyard, Jr. Fellow in Pediatrics, 1949-50.
Present address: Children's Hospital of Philadelphia.'We wish to thank Dr. John R. Mote of the Armour
Laboratories for allocating the ACTH used in theseobservations.
toward evaluation of possible relationships be-tween the disease and pituitary or adrenocorticalfunction. As an integral part of the approach,an attempt was made to disclose, if possible,consistent changes which might precede theoutset of diuresis and, to this end, as manyrelevant physiologic measurements as practica-ble were made. These included: blood volume;discrete kidney functions; concentrations of elec-trolytes and nitrogenous constituents of serum;metabolic balances of electrolytes and nitrogen;serum lipid fractions; and urinary protein andsediment.
It has not been possible from any one or com-bination of changes to predict when diuresis wouldoccur in relation to administration of ACTH.The most striking changes observed after the out-set of diuresis were increases in plasma volume andunexpectedly large increases in glomerular filtra-tion rate (GFR). These changes together withobservations on other discrete kidney functionsare described in the present paper. Observationson other measurements will be the subject of asubsequent report (7).
SUBJECTSANDMETHODS
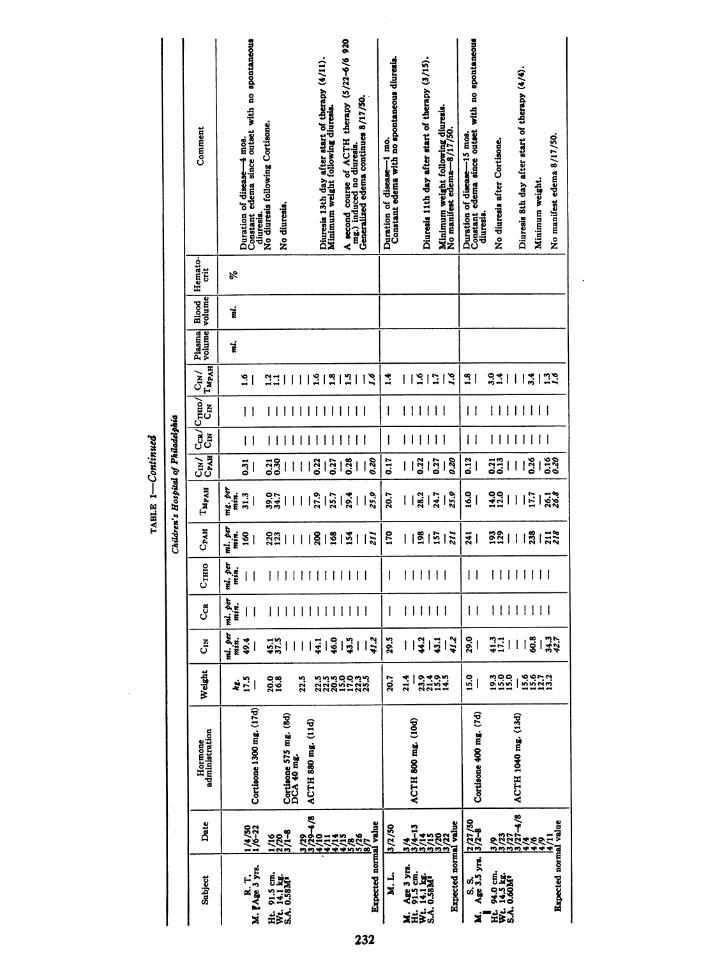
Observations were made on eight children with thenephrotic syndrome whose clinical status and course dur-ing ACTHadministration is described in a separate re-port (6). Clinical data relevant to the observationspresented here are included in Table I.
Various combinations of the following measurements
227
BARNETT, FORMAN, MCNAMARA,MCCRORY,RAPOPORT, MICHIE, AND BARBERO
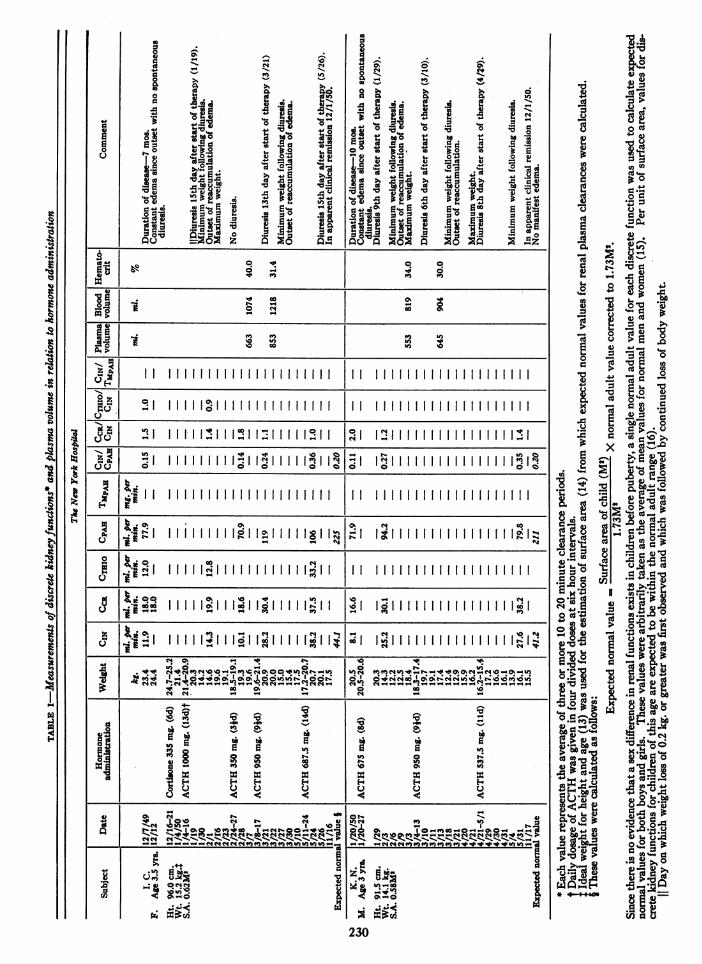
were made before, during, and after administration ofACTH: daily weight; plasma volume and hematocrit;clearances of inulin (CIN); endogenous creatinine (Cco);thiosulfate (CTHIO) and p-aminohippurate (CPAI); andmaximum tubular excretion of PAH (TMPAH). In threechildren (I. C., K. N., J. S.), 24-hour clearances of en-dogenous creatinine (Cc1-u4) were measured. Thesechildren were on low salt (20 meq. per day) but other-wise normal diets. Most of the time they were ambulatoryand normally active.
Methods for inulin, p-aminohippurate, urea (8) andendogenous creatinine (9), in blood and urine, and thecatheterization and infusion technic used for short-termsimultaneous clearances have been described (8). Serumand urine thiosulfate concentrations were determined bythe method of Newman, Gilman, and Phillips (10).CCit_ was calculated using 24-hour creatinine excretionand mid-point serum values interpolated from creatininedeterminations made one to three days apart. Plasmavolume was measured with T-1824 using a single 10-minute blood sample and the acetone extraction methodof Chinard and Eder (11) for lipemic sera. Blood volumewas calculated from plasma volume and hematocrit (12).
RESULTS5
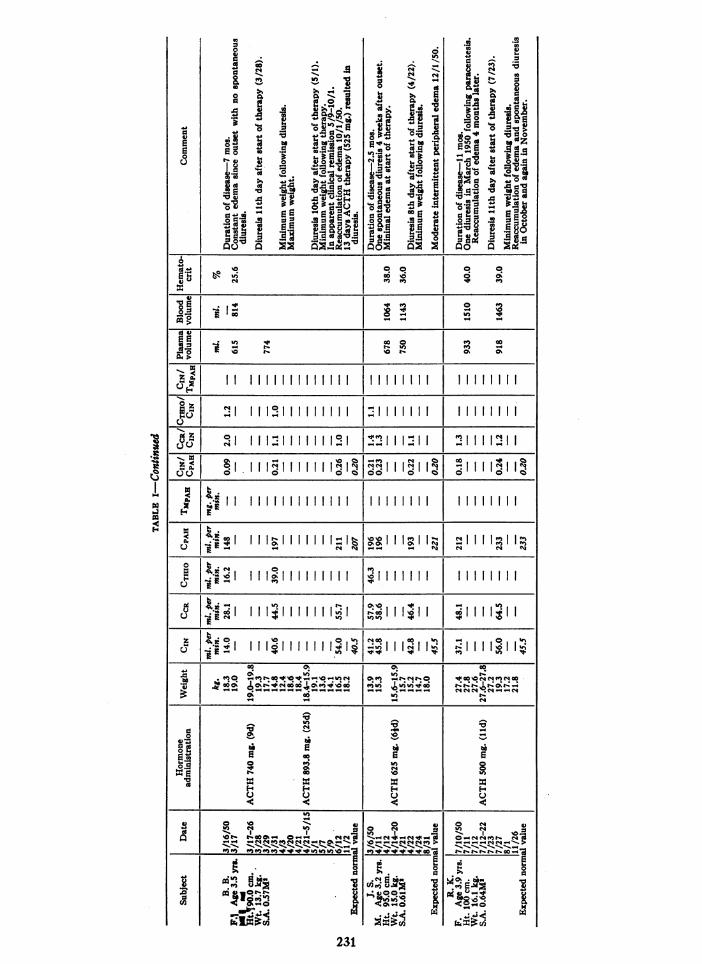
Changes observed in discrete kidney functionsand plasma volume in relation to hormone adminis-tration are given in Table I. Data from B. B. andI. C. are shown graphically in Figures 1 and 2.
Glomerular filtration rateThe most striking changes observed during or
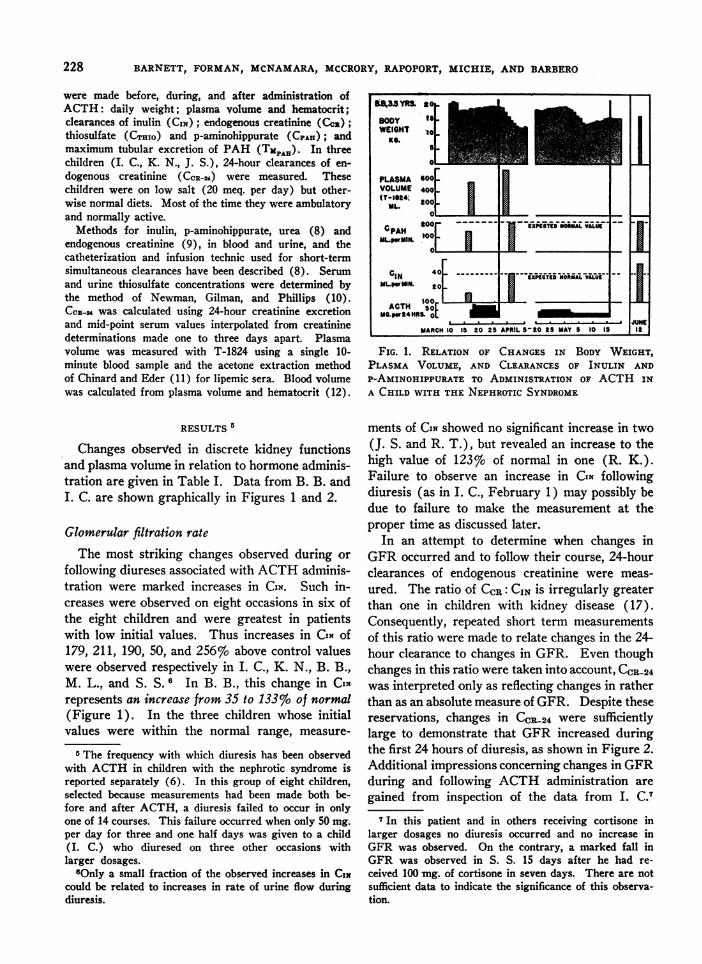
following diureses associated with ACTHadminis-tration were marked increases in CIN. Such in-creases were observed on eight occasions in six ofthe eight children and were greatest in patientswith low initial values. Thus increases in CIN of179, 211, 190, 50, and 256% above control valueswere observed respectively in I. C., K. N., B. B.,M. L., and S. S. 6 In B. B., this change in IN-represents an increase from 35 to 133%o of normal(Figure 1). In the three children whose initialvalues were within the normal range, measure-
5 The frequency with which diuresis has been observedwith ACTH in children with the nephrotic syndrome isreported separately (6). In this group of eight children,selected because measurements had been made both be-fore and after ACTH, a diuresis failed to occur in onlyone of 14 courses. This failure occurred when only 50 mg.per day for three and one half days was given to a child(I. C.) who diuresed on three other occasions withlarger dosages.
6Only a small fraction of the observed increases in CINcould be related to increases in rate of urine flow duringdiuresis.
FIG. 1. RELATION OF CHANGES IN BODY WEIGHT,PLASMA VOLUME, AND CLEARANCES OF INULIN ANDP-AMINOHIPPURATE TO ADMINISTRATION OF ACTH INA CHILD WITH THE NEPHROTICSYNDROME
ments of CIN showed no significant increase in two(J. S. and R. T.), but revealed an increase to thehigh value of 123%o of normal in one (R. K.).Failure to observe an increase in CIN followingdiuresis (as in I. C., February 1) may possibly bedue to failure to make the measurement at theproper time as discussed later.
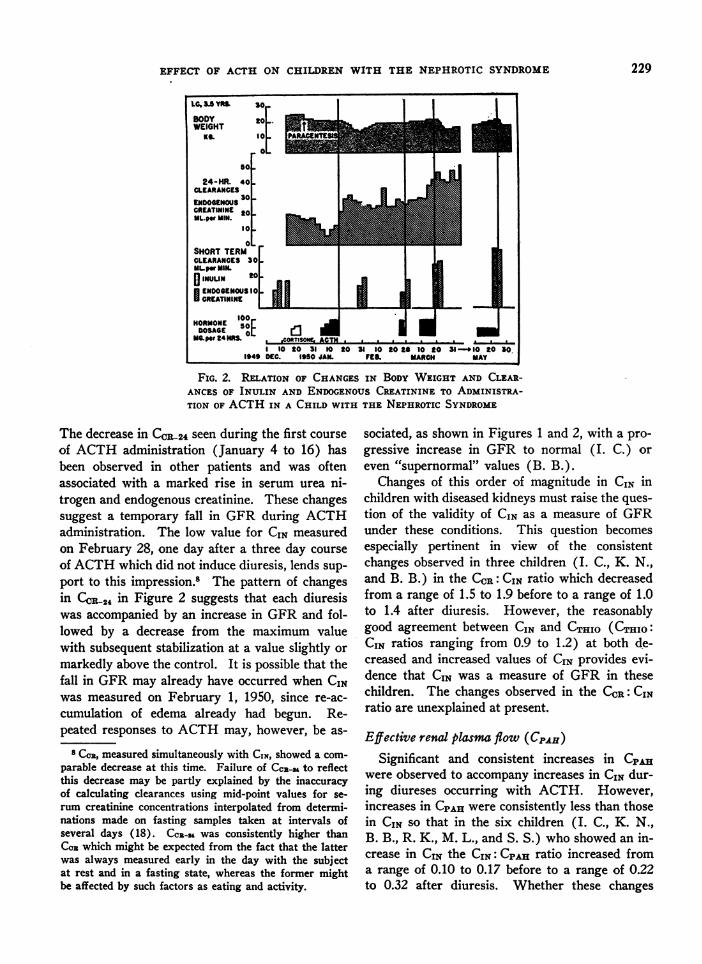
In an attempt to determine when changes inGFRoccurred and to follow their course, 24-hourclearances of endogenous creatinine were meas-ured. The ratio of CCR: CIN is irregularly greaterthan one in children with kidney disease (17).Consequently, repeated short term measurementsof this ratio were made to relate changes in the 24-hour clearance to changes in GFR. Even thoughchanges in this ratio were taken into account, CCR-24was interpreted only as reflecting changes in ratherthan as an absolute measure of GFR. Despite thesereservations, changes in CCR-24 were sufficientlylarge to demonstrate that GFR increased duringthe first 24 hours of diuresis, as shown in Figure 2.Additional impressions concerning changes in GFRduring and following ACTH administration aregained from inspection of the data from I. C.7
7 In this patient and in others receiving cortisone inlarger dosages no diuresis occurred and no increase inGFR was observed. On the contrary, a marked fall inGFR was observed in S. S. 15 days after he had re-ceived 100 mg. of cortisone in seven days. There are notsufficient data to indicate the significance of this observa-tion.
01 40111------- ---CIN 4F zXPEcTI NORIMAL VALUEMLpWrMM. to [I U
ACTH sotH UIMG.pw24HRSt 01
MARCH10 15 20 25 APRIL S-20 2S MAY 5 10 1I
228
EFFECT OF ACTH ON CHILDREN WITH THE
Lc. .5 Rs. 30
BODY 201WEIGHT
Ko 0_
24-HR. 40 .-CLEARANCES
ENDOGENOUS30 -
CREATININE so LUL.pr MIN.
O_
.. 0SHORTTERCLEARANCESMLwMIN.
D INUUN
HORMONEDOSAGE
MG.per 24HRS
1
IOslo oi100
4 1 120fTIS0W-AOTfi-e ._ _. 1-
I 1o tO 31 Et tO 31 30tO2 10 20 31-1949 DC. 1950 JAM. FE. MARCH
LJ-
_ 10 to 30.MAY
FIG. 2. RELATION OF CHANGESIN BODY WEIGHT AND CLEAR-ANCES OF INULIN AND ENDOGENOUSCREATININE TO ADMINISTRA-TION OF ACTHIN A CHILD WITH THE NEPHROTICSYNDROME
The decrease in CCR-24 seen during the first courseof ACTHadministration (January 4 to 16) hasbeen observed in other patients and was oftenassociated with a marked rise in serum urea ni-trogen and endogenous creatinine. These changessuggest a temporary fall in GFR during ACTHadministration. The low value for CIN measuredon February 28, one day after a three day courseof ACTHwhich did not induce diuresis, lends sup-port to this impression.8 The pattern of changesin CC024 in Figure 2 suggests that each diuresiswas accompanied by an increase in GFRand fol-lowed by a decrease from the maximum valuewith subsequent stabilization at a value slightly ormarkedly above the control. It is possible that thefall in GFRmay already have occurred when CINwas measured on February 1, 1950, since re-ac-cumulation of edema already had begun. Re-peated responses to ACTHmay, however, be as-
8 Cm, measured simultaneously with CIN, showed a com-parable decrease at this time. Failure of CC_-S to reflectthis decrease may be partly explained by the inaccuracyof calculating clearances using mid-point values for se-rum creatinine concentrations interpolated from determi-nations made on fasting samples taken at intervals ofseveral days (18). CcN-H was consistently higher thanCo2 which might be expected from the fact that the latterwas always measured early in the day with the subjectat rest and in a fasting state, whereas the former mightbe affected by such factors as eating and activity.
sociated, as shown in Figures 1 and 2, with a pro-gressive increase in GFR to normal (I. C.) oreven "supernormal" values (B. B.).
Changes of this order of magnitude in CIN inchildren with diseased kidneys must raise the ques-tion of the validity of CIN as a measure of GFRunder these conditions. This question becomesespecially pertinent in view of the consistentchanges observed in three children (I. C., K. N.,and B. B.) in the CGR: CIN ratio which decreasedfrom a range of 1.5 to 1.9 before to a range of 1.0to 1.4 after diuresis. However, the reasonablygood agreement between CIN and CTHIO (CTHIO:CIN ratios ranging from 0.9 to 1.2) at both de-creased and increased values of CIN provides evi-dence that CIN was a measure of GFR in thesechildren. The changes observed in the CCR: CINratio are unexplained at present.
Effective renal plasma flow (CpAH)Significant and consistent increases in CpAH
were observed to accompany increases in CIN dur-ing diureses occurring with ACTH. However,increases in CPAHwere consistently less than thosein CIN so that in the six children (I. C., K. N.,B. B., R. K., M. L., and S. S.) who showed an in-crease in CIN the CIN: CpAH ratio increased froma range of 0.10 to 0.17 before to a range of 0.22to 0.32 after diuresis. Whether these changes
-
NEPHROTIC SYNDROME 229
I
L
I I
3ca
06
C4 *T: co
icu' ]3U )
_ :g gJ
P
11111 I11 11
IluIlolo II II
in C11811 1 1
e111-21 1l l
l1ll 1z l3 Iwif U)
U).0.4M'*
F la la a41114 El 1-4 1-
A" S s e; 1
1 9 St Go t.
0 m:U $ U
4 -.4:.4¢¢ ¢
0
U)
0
U)
0*
U)
1111111
111111l
1111I1 I
W111 1 11
111111l
II I I I
sI I I I
C) l W'4 _
I " "0 10
.v4o0
.2:
. 4wfi
4 E
I0 I i
0
U)
li I
11
1111
liii
IIII
l l
1111111
1111111
II''
0.U)
0%(.4U~.4
0%
It
04X% .0t 4 '
LI
iz v
ga 0~~~
.
co4)
0
c1'4
W)~~~~~~~~4
I4 I I
"4
U
X- 4)
C.)
I I c1q fl
II IIII I b
UpV)W)~ ba
o'
a1111 _X4)U)SWif'_._ NIS
] qa. S.S4X *,,
230
I)u4)4
4U'4d."4
:3Us .
cn4)
'CI
4)
O cd
4I4)
0
Aa
.
F
,o
'm C.1.
3E S
8 p
11111111
lIIi I°l
1111I I
11111111I1111111
i iI III II
I I I 1 11 1
0V
4o
4'@3 |
at1 °l
a a:
o 0
4).
0It
0 z
U
co G
At*~0UU
Cl
E fioS.o:3
0*
o Cl
_) U
11111111
ol1 IolI I I
111111111
I1 I,- *-I I IoI II I II
G1 lI I I
I I I" I I I
..
4?
I
*40
%be
*s
.4
1
S..-
I-
-00U)U.F
0%'.O4.:34
I-;m :u3
i:1
0
1aoa
ts e!
g.0
co
:iJ
'0
N4
I I
_ 1
I I'l eIII I oI I o I I I I o I I o
c IIIIIIIIIIIII II I I I I I I -, IIIIboa
o t.f |X i ° I I 1e111111111 |eIii |11 I II IIIII
.s 4 00 ~~io0b"0O Q¢0 e)Juvq ort_I t
eq eqt
, ~~ ~ ~ ~ UUs.
*U,0 ~~~~~'oU N Oi'Nt0 4OOU,O
~~4~~~4 NNN.N~~~~~~~Cco~~~~~~U
co '4
44
o 'o _ ,1 I'l=
o02 t-o_k- o__ "M__ _.'NN NNNOr',__MM .
Iaa11Ei
.4,U
a. 0Nf :2
'0Z . 4.4NNN4* .
NZ-4
U5Il d jj laenN
!Z N,
I-. 'ZM I-N- v,
--t -t .1 4l
~z~z$c,5
231
Vi
0u
I.
a°l 5 10
M>
_ ,
uUcIq
.4
w1V
:aU2
I . -- .1_0 -a- wl wl - 0--a II
0-Q23
-
E _
oz Go ov v
44.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
.z1^ NNN
.~ Il
I
I" l-
a__
I@ i%waV 4i
9i 3 3 igE
I
0
g
o.oi .5e E
o0.
0g
Xa -
..t3O_
4i
txo!0
B* AW) 9
Io
o 0r13-c.
ciC:
t- 10 1 c+owo.~nR I I I,e l!aorO -4 m_ &nrtt Os V) V &n VaN M" N "f_ _ __ ___- 4-4"" 4-
.; n q cq n nnnqqnn-ft 1-1 0.0 N ""Cant-Nin
..4 " 1-4 "
232
-st
'o
c:§
E .2 0
z3.g
1-
O
41COEa .w a
f @ -G:- o
.2a1%:9.34vla'%t
114It4%.Zt
EFFECT OF ACTH ON CHILDREN WITH THE NEPHROTIC SYNDROME
in the CIN: CPAHratio are associated with vascularchanges or alterations in the permeability of theglomerular membrane cannot be assessed atpresent.
Maximum tubular excretion of PAH
Increases in TMPAH accompanied increases inCIN in two children (M. L. and S. S.) in whomitwas measured before and during diuresis. Thechanges in TMPAHwere less than those in CIN SOthat the CIN: TMPAHratios increased from initiallylow values before to higher values. In the remain-ing child in whom repeated measurements ofTMPAHwere made, no change in CIN was observedand the changes in TMPAHwere irregular.
Plasma and blood volume
Increases in plasma volume during or after diu-resis were observed in four out of five children inwhomsuch observations were made. The changesin I. C., K. N., B. B., and J. S. were 29, 17, 26, and11 o respectively, above the control values. Cor-responding increases in blood volume in I. C.,K. N., and J. S. were observed but the changeswere proportionately less because of decreases inhematocrit values. Failure to observe an increasein plasma volume in R. K. may possibly be ex-plained again by a failure to make the measure-ment at the proper time.
DISCUSSION
Prompt increases above initially reduced ratesof glomerular filtration are commonly seen duringthe early stages of acute nephritis in children.On the other hand, reduced clearances in childrenwith the nephrotic syndrome of several months'duration have been interpreted as indicating a lessreversible process. The rapid increases in glo-merular filtration rate reported here in childrenwho had reduced kidney function and who were
given ACTHdemonstrate, therefore, a potential-ity for improvement in function beyond that com-
monly considered possible in children with thenephrotic syndrome.
There is no evidence and it is not implied thatthese results are peculiar to diureses induced byACTH. Although the magnitude of the changeswas somewhat greater than those previously re-
ported with other agents (1, 4, 19), it is entirely
possible and probable that quantitatively similarchanges may accompany spontaneous or induceddiureses.
The results described have no bearing on thequestion of whether pituitary or adrenal corticalhormones have any direct relationship to the ne-phrotic syndrome. They do indicate that ACTHadministration may induce repeated diureses atpredictable times permitting serial measurementsof changes which may accompany and be involvedin the mechanism of diuresis. Thus large in-creases in glomerular filtration rate and significantincreases in plasma volume were observed duringdiureses in these children. These observationslend support to the concept (20) that increases inplasma volume and in glomerular filtration rateaccompany and may be involved in the mechanismof diuresis in children with the nephrotic syndrome.
SUMMARY
Profuse, sustained diureses occurring at pre-dictable times in a high percentage of trials dur-ing or following administration of ACTHto chil-dren with the nephrotic syndrome permitted obser-vations on changes which may accompany and beinvolved in the mechanism of diuresis. Serialmeasurements of discrete kidney functions andplasma volume are reported before, during andafter 13 such diureses in eight children. The re-sults indicate:
1. In five children with initially reduced ratesof glomerular filtration, increases in inulin clear-ances ranging from 50 to 256%o above controlvalues were observed during or following diureseson five out of six occasions. In three observationson three children with rates of glomerular filtra-tion initially within the normal range, an increaseof 54%o was observed in one. Thus in nine obser-vations where inulin clearances were measuredbefore and after the outset of diuresis, significantincreases were observed in six.
2. Daily 24-hour creatinine clearances, meas-ured in one of the three instances in which nomarked increase in inulin clearance was observedafter diuresis, suggest that glomerular filtrationrate did increase during diuresis. In addition, the24-hour clearances suggest that a marked increasein glomerular filtration rate during diuresis maybe followed by a decrease from the maximum
233
BARNETT, FORMAN, MCNAMARA,MCCRORY,RAPOPORT, MICHIE, AND BARBERO
value, but with subsequent stabilization at a valueslightly or markedly above the control. Repeatedresponses in children with reduced function maythen be associated with a progressive increase tonormal or even "supernormal" values.
3. A consistent decrease in the endogenous cre-atinine: inulin clearance ratio was observed asglomerular filtration rate increased. However,clearances of thiosulfate and inulin showed reason-ably good agreement at both high and low ratesof glomerular filtration.
4. Clearances and maximum tubular excretionof p-aminohippurate increased during diuresisbut proportionately less than inulin clearances.Consequently, increases in the CIN: CpAH and theCIN: TMPAHratios were observed as rates of glo-merular filtration increased.
5. In four of five observations on five children,increases in plasma volume (T-1824) rangingfrom 11 to 29%-above control values were ob-served during diureses.
CONCLUSIONS
1. Diureses occurring during or following ad-ministration of ACTH to children with the ne-phrotic syndrome are usually associated withmarked improvement in kidney function. Re-peated diureses in children with initially reducedfunction may be associated with progressive in-creases in rates of glomerular filtration to normalvalues. These observations demonstrate a po-tentiality for improvement in function beyond thatcommonly considered possible in the nephroticsyndrome of many months' duration. It is be-lieved that these changes are not peculiar to diu-reses associated with- ACTH administration butmay accompany spontaneous or other types of in-duced diureses.
2. The changes observed in plasma volume andglomerular filtration rate support the concept thatincreases in plasma volume and glomerular filtra-tion rate are associated with the mechanism ofdiuresis in children with the nephrotic syndrome.
ACKNOWLEDGMENTS
Weare indebted to Flora Hurwitz, R.N., Marie Ragni,B.A., Jean Tracy, R.N., and Josephine Codis, R. N., fornursing and technical assistance.
REFERENCES
1. Luetscher, J. A., Jr., Hall, A. D., and Kremer, V. L.,Treatment of nephrosis with concentrated humanserum albumin. II. Effects on renal function andon excretion of water and some electrolytes. J.Clin. Invest., 1950, 29, 896.
2. Rosenblum, A. H., Lander, H. B., and Fisher, R. M.,Measles in the nephrotic syndrome. J. Pediat.,1949, 35, 574.
3. Fox, C. L., Jr., and McCune, D. J., Electrolyte changesin nephrosis. Occurrence of diuresis following ad-ministration of sodium and potassium salts. Am.J. M. Sc., 1948, 216, 1.
4. Chasis, H., Goldring, W., and Baldwin, D. S., Effectof febrile plasma, typhoid vaccine, and nitrogenmustard on renal manifestations of human glo-merulonephritis. Proc. Soc. Exper. Biol. & Med.,1949, 71, 565.
5. Farnsworth, E. B., Metabolic changes associated withadministration of adrenocorticotropin in the ne-phrotic syndrome. Proc. Soc. Exper. Biol. & Med.,1950, 74, 60.
6. Rapoport, M., Michie, A., Barbero, G., Barnett, H. L.,Forman, C. W., McNamara, H., and McCrory,W. WV., The effect of adrenocorticotrophic hormoneon children with the nephrotic syndrome. I. Clini-cal observations. In preparation.
7. McNamara, H., Barnett, H. L., Forman, C. W.,McCrory, W. W., and Lauson, H. D., The effectof ACTHon children with the nephrotic syndrome.III. Observations on distribution and excretion ofwater, electrolytes, and nitrogen. In preparation.
8. Barnett, H. L., Hare, K., McNamara, H., and Hare,R., Measurement of glomerular filtration rate inpremature infants. J. Clin. Invest., 1948, 27, 691.
9. Hare, R. S., Endogenous creatinine in serum andurine. Proc. Soc. Exper. Biol. & Med., 1950, 74,148.
10. Newman, E. V., Gilman, A., and Philips, F. S., Therenal clearance of thiosulfate in man. Bull. JohnsHopkins Hosp., 1946, 79, 229.
11. Chinard, F. P., and Eder, H. A., The determinationof the concentration of the dye T-1824 in normaland lipemic plasmas. J. Exper. Med., 1948, 87, 473.
12. Smith, C. H., A method for determining the sedi-mentation rate and red cell volume in infantsand children with the use of capillary blood. Am.J. M. Sc., 1936, 192, 73.
13. Woodbury, R. M., Statures and weights of childrenunder six years of age. U. S. Labor Dept. Child-ren's Bureau Publication, No. 87, 1922.
14. DuBois, E. F., Basal Metabolism in Health and Dis-ease. Lea & Febiger, Philadelphia, 3rd edition,1936, p. 135.
15. Smith, H. W., Kidney: Structure and Function inHealth and Disease. Oxford University Press,New York. In press.
234
EFFECT OF ACTH ON CHILDREN WITH THE NEPHROTIC SYNDROME
16. Barnett, H. L., Kidney function in young infants.Pediatrics, 1950, 5, 171.
17. Hare, K., Goldstein, H., Barnett, H. L., McNamara,H., and Hare, R. S., Renal excretion of creatininein man. Federation Proc., 1949, 8, 67.
18. Sirota, J. H., Baldwin, D. S., and Villarreal, H., Di-urnal variations of renal function in man. J. Clin.Invest., 1950, 29, 187.
19. Cargill, W. H., Effect of the intravenous administra-
tion of human serum albumin on renal function.Proc. Soc. Exper. Biol. & Med., 1948, 68, 189.
20. Eder, H. A., Chinard, F. P., Greif, R. L., Cotzias,G. C., Hiller, A., Van Slyke, D. D., and Lauson,H. D., A study of the changes in plasma volume,renal function, and water and salt balance inducedby repeated administration of human plasma al-bumin to patients with the nephrotic syndrome.J. Clin. Invest., 1948, 27, 532.
235





























