Embed Size (px)
Citation preview

8. Pharmacologic Approaches toGlycemic TreatmentDiabetes Care 2017;40(Suppl. 1):S64–S74 | DOI: 10.2337/dc17-S011
PHARMACOLOGIC THERAPY FOR TYPE 1 DIABETES
Recommendations
c Mostpeoplewith type1diabetes shouldbe treatedwithmultiple daily injections ofprandial insulin and basal insulin or continuous subcutaneous insulin infusion. A
c Most individuals with type 1 diabetes should use rapid-acting insulin analogsto reduce hypoglycemia risk. A
c Consider educating individuals with type 1 diabetes on matching prandialinsulin doses to carbohydrate intake, premeal blood glucose levels, and antic-ipated physical activity. E
c Individuals with type 1 diabetes who have been successfully using continuoussubcutaneous insulin infusion should have continued access to this therapyafter they turn 65 years of age. E
Insulin TherapyInsulin is the mainstay of therapy for individuals with type 1 diabetes. Generally, thestarting insulin dose is based on weight, with doses ranging from 0.4 to 1.0 units/kg/day of total insulin with higher amounts required during puberty. The American DiabetesAssociation/JDRF Type 1 Diabetes Sourcebook notes 0.5 units/kg/day as a typical startingdose in patients who are metabolically stable, with higher weight-based dosing requiredimmediately following presentation with ketoacidosis (1), and provides detailed informa-tion on intensification of therapy to meet individualized needs. The American DiabetesAssociation (ADA) position statement “Type 1 Diabetes Management Through the LifeSpan” additionally provides a thorough overview of type 1 diabetes treatment and asso-ciated recommendations (2).Education regarding matching prandial insulin dosing to carbohydrate intake, pre-
meal glucose levels, and anticipated activity should be considered, and selected indi-viduals who have mastered carbohydrate counting should be educated on fat andprotein gram estimation (3–5). Although most studies of multiple daily injections(MDI) versus continuous subcutaneous insulin infusion (CSII) have been small and ofshort duration, a systematic review andmeta-analysis concluded that there areminimaldifferences between the two forms of intensive insulin therapy in A1C (combinedmeanbetween-group difference favoring insulin pump therapy 20.30% [95% CI 20.58to 20.02]) and severe hypoglycemia rates in children and adults (6). A 3-month ran-domized trial in patients with type 1 diabetes with nocturnal hypoglycemia reportedthat sensor-augmented insulin pump therapy with the threshold suspend feature re-duced nocturnal hypoglycemia without increasing glycated hemoglobin levels (7). In-tensive management using CSII and continuous glucose monitoring (CGM) should beencouraged in selected patientswhen there is active patient/family participation (8–10).The Diabetes Control and Complications Trial (DCCT) clearly showed that intensive
therapy with MDI or CSII delivered by multidisciplinary teams of physicians, nurses, dieti-tians, and behavioral scientists improved glycemia and resulted in better long-term out-comes (11–13). The study was carried out with short-acting and intermediate-actinghuman insulins. Despite better microvascular, macrovascular, and all-causemortalityoutcomes, intensive therapy was associated with a high rate of severe hypoglycemia(61 episodes per 100 patient-years of therapy). Since the DCCT, a number of rapid-acting and long-acting insulin analogs have been developed. These analogs are as-sociated with less hypoglycemia in type 1 diabetes, while matching the A1C loweringof human insulins (14,15).
Suggested citation: American Diabetes Associa-tion. Pharmacologic approaches to glycemictreatment. Sec. 8. In Standards of MedicalCare in Diabetesd2017. Diabetes Care 2017;40(Suppl. 1):S64–S74
© 2017 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
American Diabetes Association
S64 Diabetes Care Volume 40, Supplement 1, January 2017
8.PHARMACOLO
GIC
APPROACHES
TOGLYCEM
ICTR
EATM
ENT

Rapid-acting inhaled insulin used be-fore meals in type 1 diabetes was shownto be noninferior when compared withaspart insulin for A1C lowering, with lesshypoglycemia observed with inhaled in-sulin therapy (16). However, the meanreduction in A1C was greater with aspart(20.21% vs. 20.40%, satisfying the non-inferiority margin of 0.4%), and more pa-tients in the insulin aspart groupachieved A1C goals of #7.0% (53mmol/mol) and #6.5% (48 mmol/mol).Because inhaled insulin cartridges areonly available in 4, 8, and 12 unit doses,people with type 1 diabetes may havelimited dosing increments to fine-tuneprandial insulin doses when using thistherapy.Postprandial glucose excursions may be
better controlled by adjusting the timingof prandial (bolus) insulin dose adminis-tration. The optimal time to administerprandial insulin varies, based on thetype of insulin used (regular, rapid-actinganalog, inhaled, etc.), the measuredblood glucose level, timing of meals,and carbohydrate consumption. Rec-ommendations for prandial insulindose administration should thereforebe individualized.
PramlintidePramlintide, an amylin analog, is anagent that delays gastric emptying,blunts pancreatic secretion of glucagon,and enhances satiety. It is U.S. Food andDrug Administration (FDA)–approvedfor use in adults with type 1 diabetes. Ithas been shown to induce weight lossand lower insulin doses. Concurrent re-duction of prandial insulin dosing is re-quired to reduce the risk of severehypoglycemia.
Pancreas and Islet TransplantationPancreas and islet transplantation havebeen shown to normalize glucose levelsbut require lifelong immunosuppressionto prevent graft rejection and recurrenceof autoimmune islet destruction. Giventhe potential adverse effects of immuno-suppressive therapy, pancreas transplan-tation should be reserved for patientswith type 1 diabetes undergoing simulta-neous renal transplantation, followingrenal transplantation, or for those withrecurrent ketoacidosis or severe hypogly-cemia despite intensive glycemic manage-ment (17). Islet transplantation remainsinvestigational. Autoislet transplantationmay be considered for patients requiring
total pancreatectomy for medically refrac-tory chronic pancreatitis.
Investigational Agents
Metformin
Adding metformin to insulin therapy mayreduce insulin requirements and improvemetabolic control in overweight/obese pa-tients with poorly controlled type 1 diabe-tes. In ameta-analysis,metformin in type1diabetes was found to reduce insulin re-quirements (6.6 units/day, P, 0.001) andled to small reductions in weight and totaland LDL cholesterol but not to improvedglycemic control (absolute A1C reduction0.11%, P 5 0.42) (18). Metformin is notFDA-approved for use in patients withtype 1 diabetes.
Incretin-Based Therapies
Due to their potential protection of b-cellmass and suppression of glucagon release,glucagon-like peptide 1 (GLP-1) receptoragonists and dipeptidyl peptidase 4 (DPP-4)inhibitors are being studied in patients withtype 1 diabetes but are not currently FDA-approved for use in patients with type 1diabetes.
Sodium–Glucose Cotransporter
2 Inhibitors
Sodium–glucose cotransporter 2 (SGLT2)inhibitors provide insulin-independent glu-cose lowering by blocking glucose reab-sorption in the proximal renal tubule byinhibiting SGLT2. These agents providemodest weight loss and blood pressurereduction in type 2 diabetes. There arethree FDA-approved agents for patientswith type 2 diabetes, but none are FDA-approved for the treatment of patientswith type 1 diabetes (2). The FDA issued awarning about the risk of ketoacidosis oc-curring in the absence of significant hyper-glycemia (euglycemic diabetic ketoacidosis)in patients with type 1 and type 2 diabetestreatedwith SGLT2 inhibitors. Symptomsofketoacidosis includedyspnea, nausea, vom-iting, and abdominal pain. Patients shouldbe instructed to stop taking SGLT2 inhibi-tors and seek medical attention immedi-ately if they have symptoms or signs ofketoacidosis (19).
PHARMACOLOGIC THERAPY FORTYPE 2 DIABETES
Recommendations
c Metformin, if not contraindicatedand if tolerated, is the preferred ini-tial pharmacologic agent for thetreatment of type 2 diabetes. A
c Long-term use of metformin maybe associated with biochemicalvitamin B12 deficiency, and peri-odic measurement of vitamin B12levels should be considered inmetformin-treated patients, es-pecially in those with anemia orperipheral neuropathy. B
c Consider initiating insulin therapy(with or without additional agents)in patients with newly diagnosedtype 2 diabetes who are symptom-atic and/or have A1C $10% (86mmol/mol) and/or blood glucoselevels$300 mg/dL (16.7 mmol/L). E
c If noninsulin monotherapy atmaximum tolerated dose does notachieve or maintain the A1C targetafter 3 months, add a second oralagent, a glucagon-like peptide 1 re-ceptor agonist, or basal insulin. A
c A patient-centered approach shouldbe used to guide the choice of phar-macologic agents. Considerations in-clude efficacy, hypoglycemia risk,impact on weight, potential side ef-fects, cost, and patient preferences. E
c For patients with type 2 diabeteswho are not achieving glycemicgoals, insulin therapy should notbe delayed. B
c In patients with long-standingsuboptimally controlled type 2 di-abetes and established athero-sclerotic cardiovascular disease,empagliflozin or liraglutide shouldbe considered as they have beenshown to reduce cardiovascularand all-cause mortality whenadded to standard care. Ongoingstudies are investigating the cardio-vascular benefits of other agents inthese drug classes. B
The use of metformin as first-line ther-apy was supported by findings froma large meta-analysis, with selectionof second-line therapies based onpatient-specific considerations (20).An ADA/European Association for theStudy of Diabetes position statement(21) recommended a patient-centeredapproach, including assessment of ef-ficacy, hypoglycemia risk, impact onweight, side effects, costs, and patientpreferences. Renal effectsmayalsobe con-sidered when selecting glucose-loweringmedications for individual patients. Life-style modifications that improve health
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S65

(see Section 4 “Lifestyle Management”)should be emphasized along with anypharmacologic therapy.
Initial TherapyMetforminmonotherapy should be startedat diagnosis of type 2 diabetes unlessthere are contraindications. Metforminis effective and safe, is inexpensive, andmay reduce risk of cardiovascular eventsand death (22). Metforminmay be safelyused in patients with estimated glo-merular filtration rate (eGFR) as low as30 mL/min/1.73 m2 (23), and the U.S.label for metformin was recently re-vised to reflect its safety in patientswith eGFR $30 mL/min/1.73 m2 (24).Patients should be advised to stop the
medication in cases of nausea, vomiting,or dehydration. Metformin is associatedwith vitamin B12 deficiency, with a recentreport from the Diabetes Prevention Pro-gram Outcomes Study (DPPOS) suggestingthat periodic testing of vitamin B12 levelsshould be considered inmetformin-treatedpatients, especially in those with anemia orperipheral neuropathy (25).
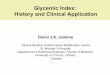
In patients with metformin contrain-dications or intolerance, consider an ini-tial drug from another class depicted inFig. 8.1 under “Dual Therapy” and pro-ceed accordingly. When A1C is $9%(75 mmol/mol), consider initiating dualcombination therapy (Fig. 8.1) to moreexpeditiously achieve the target A1Clevel. Insulin has the advantage of being
effective where other agents may not beand should be considered as part of anycombination regimen when hyperglycemiais severe, especially if symptoms are pre-sent or any catabolic features (weightloss, ketosis) are present. Consider ini-tiating combination insulin injectabletherapy (Fig. 8.2) when blood glucoseis $300 mg/dL (16.7 mmol/L) or A1Cis$10% (86 mmol/mol) or if the patienthas symptoms of hyperglycemia (i.e.,polyuria or polydipsia). As the patient’sglucose toxicity resolves, the regimenmay, potentially, be simplified.
Combination TherapyAlthough there are numerous trials com-paring dual therapywithmetformin alone,
Figure 8.1—Antihyperglycemic therapy in type 2 diabetes: general recommendations. The order in the chart was determined by historical availability andthe route of administration, with injectables to the right; it is not meant to denote any specific preference. Potential sequences of antihyperglycemictherapy for patients with type 2 diabetes are displayed, with the usual transition moving vertically from top to bottom (although horizontal movementwithin therapy stages is also possible, depending on the circumstances). DPP-4-i, DPP-4 inhibitor; fxs, fractures; GI, gastrointestinal; GLP-1 RA, GLP-1receptor agonist; GU, genitourinary; HF, heart failure; Hypo, hypoglycemia; SGLT2-i, SGLT2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione. *See ref. 21 fordescription of efficacy and cost categorization. §Usually a basal insulin (NPH, glargine, detemir, degludec). Adapted with permission from Inzucchi et al. (21).
S66 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 40, Supplement 1, January 2017

fewdirectly comparedrugs as add-on ther-apy. A comparative effectiveness meta-analysis (23) suggests that each new classof noninsulin agents added to initial ther-apy generally lowers A1C approximately0.9–1.1%. If the A1C target is not achievedafter approximately 3 months, consider acombination of metformin and one of
the six available treatment options: sul-fonylurea, thiazolidinedione, DPP-4 in-hibitor, SGLT2 inhibitor, GLP-1 receptoragonist, or basal insulin (Fig. 8.1). If A1Ctarget is still not achieved after ;3months of dual therapy, proceed tothree-drug combination (Fig. 8.1). Again,if A1C target is not achieved after
;3 months of triple therapy, proceedto combination injectable therapy(Fig. 8.2).
Drug choice is based on patient pref-erences (26), as well as various patient,disease, and drug characteristics, withthe goal of reducing blood glucose levelswhile minimizing side effects, especially
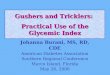
Figure 8.2—Combination injectable therapy for type 2 diabetes. FBG, fasting blood glucose; GLP-1 RA, GLP-1 receptor agonist; hypo, hypoglycemia.Adapted with permission from Inzucchi et al. (21).
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S67

Table
8.1—Pro
pertiesofava
ilable
gluco
se-loweringagents
intheU.S.thatmayguideindividualize
dtreatm
entch
oicesin
patients
withtype2diabetes(21)
Class
Compound(s)
Cellularmechanism(s)
Prim
aryphysiological
action(s)
Advantages
Disadvantages
Cost*
Biguanides
cMetform
inActivates
AMP-kinase
(?other)
c↓Hep
aticglucose
production
cExtensive
experience
cRarehypoglycem
iac↓CVDeven
ts(UKPD
S)cRelativelyhigher
A1C
efficacy
cGastrointestinalsideeffects
(diarrhea,abdo
minalcram
ping,nausea)
cVitam
inB12
deficiency
cCo
ntraindications:eG
FR,30
mL/min/1.73m
2,acidosis,hypoxia,
dehydration,etc.
cLacticacidosisrisk
(rare)
Low
Sulfonylureas
2ndgeneration
cGlyburide
cGlipizide
cGlim
epiride
ClosesKATPchan
nelsonb-cell
plasm
amem
branes
c↑Insulin
secretion
cExtensive
experience
c↓Microvascularrisk
(UKPD
S)cRelativelyhigher
A1C
efficacy
cHypoglycem
iac↑Weight
Low
Meglitinides
(glinides)
cRep
aglin
ide
cNateglinide
ClosesKATPchan
nelsonb-cell
plasm
amem
branes
c↑Insulin
secretion
c↓Po
stprandialglucose
excursions
cDosingflexibility
cHypoglycem
iac↑Weight
cFreq
uen
tdosingsched
ule
Moderate
TZDs
cPioglitazone‡
cRosiglitazone§
Activates
thenuclear
transcriptionfactor
PPAR-g
c↑Insulin
sensitivity
cRarehypoglycem
iacRelativelyhigher
A1C
efficacy
cDurability
c↓Triglycerides
(pioglitazone)
c?↓CVDeven
ts(PROactive,p
ioglitazone)
c↓Risk
ofstroke
andMIin
patientswithoutdiabetes
andwith
insulin
resistance
andhistoryof
recent
stroke
orTIA
(IRISstudy[42],pioglitazone)
c↑Weight
cEdem
a/heartfailure
cBonefractures
c↑LD
L-C(rosiglitazone)
Low
a-Glucosidase
inhibitors
cAcarbose
cMiglitol
Inhibitsintestinal
a-glucosidase
cSlow
sintestinalcarbohydrate
digestion/absorption
cRarehypoglycem
iac↓Po
stprandialglucose
excursions
c?↓CVDeven
tsin
prediabetes
(STO
P-NIDDM)
cNonsystem
ic
cGen
erallymodestA1C
efficacy
cGastrointestinalsideeffects
(flatulence,d
iarrhea)
cFreq
uen
tdosingsched
ule
Lowto
moderate
DPP
-4inhibitors
cSitagliptin
cSaxagliptin
cLinaglip
tin
cAlogliptin
InhibitsDPP-4activity,increasing
postprandialincretin(GLP-1,G
IP)
concentrations
c↑Insulin
secretion
(glucose
dep
enden
t)c↓Glucago
nsecretion
(glucose
dep
enden
t)
cRarehypoglycem
iacWelltolerated
cAngioedem
a/urticariaandother
immune-mediatedderm
atologicaleffects
c?Acute
pancreatitis
c↑Heartfailure
hospitalizations
(saxagliptin;?alogliptin
)
High
Bile
acid
sequestran
tscColesevelam
Bindsbileacidsinintestinaltract,
increasing
hepatic
bileacid
production
c?↓Hep
aticglucose
production
c?↑Incretin
levels
cRarehypoglycem
iac↓LD
L-C
cModestA1C
efficacy
cConstipation
c↑Triglycerides
cMay
↓absorptionofother
med
ications
High
Con
tinu
edon
p.S69
S68 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 40, Supplement 1, January 2017

Table
8.1—Continued
Class
Compound(s)
Cellularmechanism(s)
Prim
aryphysiological
action(s)
Advantages
Disadvantages
Cost*
Dopam
ine-2
agonists
cBromocriptine
(quickrelease)§
Activates
dopam
inergic
receptors
cModulateshypothalam
icregu
lationofmetabolism
c↑Insulin
sensitivity
cRarehypoglycem
iac?↓CVDeven
ts(CyclosetSafety
Trial)
cModestA1C
efficacy
cDizziness/syncope
cNau
sea
cFatigue
cRhinitis
High
SGLT2
inhibitors
cCan
aglifl
ozin
cDap
aglifl
ozin‡
cEm
paglifl
ozin
InhibitsSG
LT2in
the
proximalnep
hron
cBlocksglucose
reab
sorption
bythekidney,increasing
glucosuria
cRarehypoglycem
iac↓Weight
c↓Bloodpressure
cAssociatedwithlower
CVDevent
rate
andmortalityinpatientswith
CVD(empagliflozinEM
PA-REG
OUTCOME)
cGen
itourinaryinfections
cPo
lyuria
cVolum
edepletion/hypotension/dizziness
c↑LDL-C
c↑Creatin
ine(transient)
cDKA
,urinarytractinfections
leading
tourosepsis,pyelonephritis
High
GLP-1
receptor
agonists
cExen
atide
cExen
atideextended
release
cLiraglutide
cAlbiglutide
cLixisenatide
cDulaglutide
Activates
GLP-1
receptors
c↑Insulin
secretion
(glucose
dep
enden
t)c↓Glucago
nsecretion
(glucose
dep
enden
t)cSlowsgastricem
ptying
c↑Satiety
cRarehypoglycem
iac↓Weight
c↓Po
stprandialglucose
excursions
c↓Somecardiovascular
risk
factors
cAssociatedwithlower
CVDevent
rate
andmortalityinpatientswith
CVD(liraglutideLEADER)(30)
cGastrointestinalsideeffects
(nau
sea/vomiting/diarrhea)
c↑Heartrate
c?Acute
pancreatitis
cC-cellh
yperplasia/med
ullary
thyroid
tumors
inanim
als
cInjectab
lecTrainingrequirem
ents
High
Amylinmimetics
cPram
lintide§
Activates
amylin
receptors
c↓Glucago
nsecretion
cSlowsgastricem
ptying
c↑Satiety
c↓Po
stprandialglucose
excursions
c↓Weight
cModestA1C
efficacy
cGastrointestinalsideeffects
(nau
sea/vomiting)
cHypoglycem
iaunless
insulin
dose
issimultan
eouslyreduced
cInjectab
lecFreq
uen
tdosingsched
ule
cTrainingrequirem
ents
High
Insulins
cRapid-actinganalogs
-Lispro
-Aspart
-Glulisine
-Inhaled
insulin
cShort-acting
-Human
Regular
cInterm
ediate-acting
-Human
NPH
Activates
insulin
receptors
c↑Glucose
disposal
c↓Hep
aticglucose
production
cSuppresses
ketogenesis
cNearlyuniversalresponse
cTheo
retically
unlim
ited
efficacy
c↓Microvascularrisk
(UKPD
S)
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cPatien
tandprovider
reluctan
cecInjectab
le(excep
tinhaled
insulin)
cPu
lmonarytoxicity
(inhaled
insulin)
High#
Con
tinu
edon
p.S70
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S69

hypoglycemia. Table 8.1 lists drugs com-monly used in the U.S. Cost-effectivenessmodels have suggested that some of thenewer agents may be of relatively lowerclinical utility based on high cost andmoderate glycemic effect (27). Table 8.2provides cost information for currently ap-proved noninsulin therapies. Of note, pri-ces listed are average wholesale prices(AWP) and do not account for discounts,rebates, or other price adjustments ofteninvolved in prescription sales that affectthe actual cost incurred by the patient.While there are alternative means to esti-mate medication prices, AWP was utilizedto provide a comparison of list prices withthe primary goal of highlighting the impor-tance of cost considerations when pre-scribing antihyperglycemic treatments. Theongoing Glycemia Reduction Approachesin Diabetes: A Comparative EffectivenessStudy (GRADE) will compare four drugclasses (sulfonylurea, DPP-4 inhibitor,GLP-1 receptor agonist, and basal insulin)when added to metformin therapy over4 years on glycemic control and othermedical, psychosocial, and health eco-nomic outcomes (28).
Rapid-acting secretagogues (megliti-nides) may be used instead of sulfonyl-ureas in patients with sulfa allergies,irregularmeal schedules, or thosewho de-velop late postprandial hypoglycemiawhen taking a sulfonylurea. Other drugsnot shown in Fig. 8.1 (e.g., inhaled insulin,a-glucosidase inhibitors, colesevelam, bro-mocriptine, and pramlintide) may be triedin specific situations but are not often useddue to modest efficacy in type 2 diabetes,the frequency of administration, the po-tential for drug interactions, and/or sideeffects.
Cardiovascular Outcome TrialsSeveral recently published cardiovascularoutcome trials (CVOTs) have provideddata on patients with type 2 diabeteswith cardiovascular disease or at highrisk for cardiovascular disease. The BI10773 (Empagliflozin) CardiovascularOutcome Event Trial in Type 2 DiabetesMellitus Patients (EMPA-REG OUTCOME)was a randomized, double-blind trial thatassessed the effect of empagliflozin, aSGLT2 inhibitor, versus placebo and stan-dard care, on cardiovascular outcomes inpatients with type 2 diabetes and existingcardiovascular disease. Study participantshad a mean age of 63 years, 57% had di-abetes for more than 10 years, and 99%
Table
8.1—Continued
Class
Compound(s)
Cellularmechanism(s)
Prim
aryphysiological
action(s)
Advantages
Disadvantages
Cost*
cBasalinsulin
analogs
-Glargine
-Detem
ir-Degludec
cPrem
ixed
insulin
products
-NPH
/Regular70/30
270/30aspartmix
275/25lispromix
250/50lispromix
CVD,cardiovasculardisease;EM
PA-REG
OUTC
OME,
BI10
773(Empaglifl
ozin)CardiovascularOutcomeEven
tTrialinType2Diabetes
MellitusPatien
ts(29);GIP,glucose-dep
enden
tinsulinotropicpep
tide;
HDL-C,H
DLcholesterol;IRIS,Insulin
Resistance
Interven
tionAfter
Stroke
Trial;LD
L-C,LDLcholesterol;PP
AR-g,peroxisomeproliferator–activatedreceptorg;PROactive,Prospective
PioglitazoneClinicalTrialin
MacrovascularEven
ts(43);STO
P-NIDDM,Studyto
Preven
tNon-Insulin-Dep
enden
tDiabetes
Mellitus(44);TIA,transien
tischem
icattack;TZD
,thiazolidined
ione;UKP
DS,UKProspective
Diabetes
Study(45,46
).Cyclosettrialofq
uick-releasebromocriptine(47).*Costisbased
onlowest-pricedmem
ber
oftheclass(21).‡lnitialconcernsregardingbladder
cancerrisk
aredecreasingaftersubsequen
tstudy.§N
otlicen
sedin
Europefortype2diabetes.#C
ostishighlydep
enden
tontype/brand(analogs
.human
insulins)anddosage.Adap
tedwithpermissionfrom
Inzucchietal.(21).
S70 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 40, Supplement 1, January 2017

had established cardiovascular disease.EMPA-REG OUTCOME showed that over amedian follow-up of 3.1 years, treatmentreduced the composite outcome of MI,stroke, and cardiovascular death by 14%(absolute rate 10.5% vs. 12.1% in the pla-cebo group) and cardiovascular death by38% (absolute rate 3.7%vs. 5.9%) (29). TheFDA recently added a new indication forempagliflozin, to reduce the risk of cardio-vascular death in adults with type 2 diabe-tes and cardiovascular disease. Whetherother SGLT2 inhibitors will have the sameeffect in high-risk patients and whetherempagliflozin or other SGLT2 inhibitorswill have a similar effect in lower-risk pa-tients with diabetes remains unknown.The Liraglutide Effect and Action in Di-
abetes: Evaluation of Cardiovascular Out-come Results: A Long Term Evaluation
(LEADER) trial was a randomized double-blind trial that assessed the effect ofliraglutide, a GLP-1 receptor agonist, ver-sus placebo and standard care, on cardio-vascular outcomes in patients with type 2diabetes at high risk for cardiovascular dis-ease or with cardiovascular disease. Studyparticipants had a mean age of 64 yearsand amean duration of diabetes of nearly13 years. Over 80% of study participantshad established cardiovascular diseaseinclusive of a prior myocardial infarction(MI), prior stroke or transient ischemicattack, prior revascularization procedure,or $50% stenosis of coronary, carotid,or lower-extremity arteries. LEADERshowed that the composite primary out-come (MI, stroke, or cardiovascular death)occurred in fewer participants in the treat-ment group (13.0%) when compared with
the placebo group (14.9%) after a medianfollow-up of 3.8 years (30). Whether otherGLP-1 receptor agonists will have the sameeffect inhigh-riskpatientsor if thisdrugclasswill havesimilareffects in lower-riskpatientswith diabetes remains unknown.
CVOT data for the DPP-4 inhibitorssitagliptin (31), saxagliptin (32), andalogliptin (33) have also been reported,with no significant difference in rates ofmajor cardiovasculareventsnotedbetweentreatment and placebo groups in any ofthese trials.
Insulin TherapyMany patients with type 2 diabetes even-tually require and benefit from insulintherapy. The progressive nature of type2 diabetes should be regularly and objec-tively explained to patients. Providers
Table 8.2—Median monthly cost of maximum approved daily dose of noninsulin glucose-lowering agents in the U.S. (48)
Class Compound(s)Dosage strength/product
(if applicable)Median AWP(min, max)†
Maximum approveddaily dose*
Biguanides c Metformin 500 mg (IR) $84 ($5, $94) 2,000 mg
850 mg (IR) $108 ($5, $108) 2,550 mg
1,000 mg (IR) $86 ($4, $87) 2,000 mg
500 mg (ER) $90 ($82, $6,672) 2,000 mg
750 mg (ER) $72 ($65, $92) 1,500 mg
1,000 mg (ER) $1,028 ($1,010, $7,213) 2,000 mg
Sulfonylureas (2nd Gen) c Glyburide 5 mg $94 ($64, $103) 20 mg6 mg (micronized) $50 ($48, $71) 12 mg (micronized)
c Glipizide 10 mg (IR) $74 ($67, $97) 40 mg (IR)10 mg (XL) $97 20 mg (XL)
c Glimepiride 4 mg $74 ($71, $198) 8 mg
Meglitinides (glinides) c Repaglinide 2 mg $799 ($163, $878) 16 mgc Nateglinide 120 mg $156 360 mg
TZDs c Pioglitazone 45 mg $349 ($348, $349) 45 mgc Rosiglitazone 4 mg $355 8 mg
a-Glucosidase inhibitors c Acarbose 100 mg $104 ($104, 105) 300 mgc Miglitol 100 mg $241 300 mg
DPP-4 inhibitors c Sitagliptin 100 mg $436 100 mgc Saxagliptin 5 mg $436 5 mgc Linagliptin 5 mg $428 5 mgc Alogliptin 25 mg $436 25 mg
Bile acid sequestrant c Colesevelam 625 mg tabs $679 3.75 g1.875 g suspension $1,357 3.75 g
Dopamine-2 agonists c Bromocriptine 0.8 mg $719 4.8 mg
SGLT2 inhibitors c Canagliflozin 300 mg $470 300 mgc Dapagliflozin 10 mg $470 10 mgc Empagliflozin 25 mg $470 25 mg
GLP-1 receptor agonists c Exenatide 10 mg pen $729 20 mgc Exenatide(extended-release)
2 mg powder for suspension or pen $692 2 mg**
c Liraglutide 18 mg/3 mL pen $831 1.8 mgc Albiglutide 50 mg pen $527 50 mg**c Dulaglutide 1.5/0.5 mL pen $690 1.5 mg**
Amylin mimetics c Pramlintide 120 mg pen $2,124 120 mg/injection††
ER and XL, extended release; IR, immediate release; TZD, thiazolidinedione. †Calculated for 30 day supply (AWP unit price3 number of doses required toprovidemaximum approved daily dose3 30 days); median AWP listed alonewhen only one product and/or price. *Utilized to calculatemedian AWP(min, max); generic prices used, if available commercially. **Administered once weekly. ††AWP calculated based on 120 mg three times daily.
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S71

should avoid using insulin as a threat ordescribing it as a sign of personal failureor punishment.Equipping patients with an algorithm for
self-titration of insulin doses based on self-monitoring of blood glucose (SMBG) im-proves glycemic control in patients withtype 2 diabetes initiating insulin (34). Com-prehensive education regarding SMBG,diet, and the avoidance of and appropriatetreatment of hypoglycemia are criticallyimportant in any patient using insulin.
Basal Insulin
Basal insulin alone is the most convenientinitial insulin regimen, beginning at 10 unitsper day or 0.1–0.2 units/kg/day, dependingon the degree of hyperglycemia. Basal in-sulin is usually prescribed in conjunctionwith metformin and sometimes one addi-tional noninsulin agent. While there is evi-dence for reduced risk of hypoglycemiawith newer, longer-acting basal insulinanalogs, people with type 2 diabetes
without a history of hypoglycemia mayuse NPH insulin safely and at much lowercost (27,35). Table 8.3 provides averagewholesale price information (cost per1,000 units) for currently available insulinproducts in the U.S. There have been sub-stantial increases in the price of insulin overthe past decade and the cost-effectivenessof different antihyperglycemic agents is animportant consideration when selectingtherapies (36). A follow-on U-100 (100units/mL) glargine product (basaglar) isnow available in the U.S. This product wasapproved through an abbreviated FDA ap-proval pathway based, in part, on the FDA’sfinding of safety and effectiveness for thereference U-100 glargine product.
Bolus Insulin
Many individuals with type 2 diabetesmayrequire mealtime bolus insulin dosing inaddition to basal insulin. Rapid-actinganalogs are preferred due to theirprompt onset of action after dosing. The
recommended starting dose of mealtimeinsulin is 4 units, 0.1 U/kg, or 10% of thebasal dose. If A1C is ,8% (64 mmol/mol)when starting mealtime bolus insulin, con-sideration should be given to decreasingthe basal insulin dose.
Premixed Insulin
Premixed insulin products contain both abasal and prandial component, allowingcoverage of both basal and prandial needswith a single injection. NPH/Regular 70/30insulin, for example, is composed of70% NPH insulin and 30% regular insulin.The use of premixed insulin products hasits advantages and disadvantages, asdiscussed below in COMBINATION INJECTABLE
THERAPY.
Concentrated Insulin Products
Several concentrated insulin preparationsare currently available. U-500 regular insu-lin, by definition, is five times as concen-trated as U-100 regular insulin and has adelayed onset and longer duration of
Table 8.3—Median cost of insulins in the U.S. calculated as average wholesale price per 1,000 units of specified dosageform/product (48)
Insulins Compounds Dosage form/productMedian AWP packageprice (min, max)*
Rapid-acting analogs
c Lispro U-100 vial $306U-100 3 mL cartridges $306 ($306, $379)U-100 prefilled pen; U-200 prefilled pen $394
c Aspart U-100 vial $306U-100 3 mL cartridges $380U-100 prefilled pen $395
c Glulisine U-100 vial $283U-100 prefilled pen $365
c Inhaled insulin Inhalation cartridges $557 ($453, $754)
Short-acting
c Human Regular U-100 vial $165
Intermediate-acting
c Human NPH U-100 vial $165U-100 prefilled pen $350
Concentrated Human Regular insulin
c U-500 Human Regular insulin U-500 vial $165U-500 prefilled pen $213
Basal analogs
c Glargine U-100 vial; U-100 prefilled pen; U-300 prefilled pen $298
c Detemir U-100 vial; U-100 prefilled pen $323
c Degludec U-100 prefilled pen; U-200 prefilled pen $355
Premixed products
c NPH/Regular 70/30 U-100 vial $165U-100 prefilled pen $350
c Lispro 50/50 U-100 vial $317U-100 prefilled pen $394
c Lispro 75/25 U-100 vial $317U-100 prefilled pen $394
c Aspart 70/30 U-100 vial $318U-100 prefilled pen $395
AWP listed alone when only one product and/or price.
S72 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 40, Supplement 1, January 2017

action thanU-100 regular, posessing bothprandial and basal properties. U-300glargine and U-200 degludec are threeand two times as concentrated as theirU-100 formulations, have longer dura-tions of action, and allow higher dosesof basal insulin administration per volumeused. The FDA has also approved a concen-trated formulation of rapid-acting insulinlispro, U-200 (200 units/mL). These concen-trated preparations may be more comfort-able for the patient and may improveadherence for patients with insulin resis-tance who require large doses of insulin.While U-500 regular insulin is available inboth prefilled pens and vials (a dedicatedsyringe was FDA approved in July 2016),other concentrated insulins are availableonly in prefilled pens to minimize the riskof dosing errors.
Inhaled Insulin
Inhaled insulin is available for prandialuse with a more limited dosing range.It is contraindicated in patients withchronic lung disease such as asthmaand chronic obstructive pulmonarydisease and is not recommended inpatients who smoke or who recentlystopped smoking. It requires spirometry(FEV1) testing to identify potential lungdisease in all patients prior to and afterstarting therapy.
Combination Injectable TherapyIf basal insulin has been titrated to anacceptable fasting blood glucose level(or if the dose is .0.5 units/kg/day)and A1C remains above target, consideradvancing to combination injectabletherapy (Fig. 8.2). When initiating com-bination injectable therapy, metformintherapy should be maintained whileother oral agents may be discontinuedon an individual basis to avoid unneces-sarily complex or costly regimens (i.e.,adding a fourth antihyperglycemicagent). In general, GLP-1 receptor ago-nists should not be discontinued with theinitiation of basal insulin. Sulfonylureas,DPP-4 inhibitors, and GLP-1 receptor ago-nists are typically stopped oncemore com-plex insulin regimens beyond basal areused. In patients with suboptimal bloodglucose control, especially those requiringlarge insulin doses, adjunctive use of a thia-zolidinedione or SGLT2 inhibitor may helpto improve control and reduce the amountof insulin needed, though potential sideeffects should be considered. Once an in-sulin regimen is initiated, dose titration is
important with adjustments made in bothmealtime and basal insulins based on theblood glucose levels and an understandingof the pharmacodynamic profile of eachformulation (pattern control).
Studies have demonstrated the non-inferiority of basal insulin plus a singleinjection of rapid-acting insulin at thelargest meal relative to basal insulinplus a GLP-1 receptor agonist relativeto two daily injections of premixed insulins(Fig. 8.2). Basal insulin plus GLP-1 receptoragonists are associated with less hypogly-cemia and with weight loss instead ofweight gain but may be less tolerableand have a greater cost (37,38). In No-vember 2016, the FDA approved twodifferent once-daily combination productscontaining basal insulin plus a GLP-1 recep-tor agonist: insulin glargine plus lixisenatideand insulin degludec plus liraglutide. Otheroptions for treatment intensification includeadding a single injection of rapid-acting in-sulin analog (lispro, aspart, or glulisine) be-fore the largest meal or stopping the basalinsulin and initiating a premixed (or bi-phasic) insulin (NPH/Regular 70/30, 70/30aspartmix, 75/25 or 50/50 lispromix) twicedaily, usually before breakfast and beforedinner. Each approach has its advantagesand disadvantages. For example, providersmay wish to consider regimen flexibilitywhen devising a plan for the initiation andadjustment of insulin therapy in peoplewith type 2 diabetes, with rapid-acting in-sulin offering greater flexibility in termsof meal planning than premixed insulin. Ifone regimen is not effective (i.e., basal in-sulin 1 GLP-1 receptor agonist), considerswitching to another regimen to achieveA1C targets (i.e., basal insulin1 single in-jection of rapid-acting insulin or premixedinsulin twice daily) (39,40). Regular humaninsulin and human NPH/Regular premixedformulations (70/30) are less costly alter-natives to rapid-acting insulin analogs andpremixed insulin analogs, respectively,but their pharmacodynamic profiles maymake them less optimal.
Figure 8.2 outlines these options, aswell as recommendations for further in-tensification, if needed, to achieve gly-cemic goals. If a patient is still above theA1C target on premixed insulin twicedaily, consider switching to premixedanalog insulin three times daily (70/30aspartmix, 75/25 or 50/50 lispromix). Ingeneral, three times daily premixed an-alog insulins have been found to be non-inferior to basal-bolus regimens with
similar rates of hypoglycemia (41). If apatient is still above the A1C target onbasal insulin1 single injection of rapid-acting insulin before the largest meal, ad-vance to a basal-bolus regimen with $2injections of rapid-acting insulin beforemeals. Consider switching patients fromone regimen to another (i.e., premixedanalog insulin three times daily to basal-bolus regimen or vice-versa) if A1C targetsare not being met and/or depending onother patient considerations (39,40).
References1. American Diabetes Association, JDRF. AmericanDiabetes Association/JDRF Type 1 DiabetesSourcebook. Peters AL, Laffel L, Eds. Alexandria,VA, American Diabetes Association, 20132. Chiang JL, KirkmanMS, Laffel LMB, Peters AL.Type 1 diabetes through the life span: a positionstatement of the American Diabetes Associa-tion. Diabetes Care 2014;37:2034–20543. Wolpert HA, Atakov-Castillo A, Smith SA,Steil GM. Dietary fat acutely increases glucoseconcentrations and insulin requirements inpatients with type 1 diabetes: implications forcarbohydrate-based bolus dose calculation andintensive diabetes management. Diabetes Care2013;36:810–8164. Bell KJ, Toschi E, Steil GM, Wolpert HA.Optimized mealtime insulin dosing for fat andprotein in type 1 diabetes: application of amodel-based approach to derive insulin dosesfor open-loop diabetes management. DiabetesCare 2016;39:1631–16345. Bell KJ, Smart CE, Steil GM, Brand-Miller JC,King B, Wolpert HA. Impact of fat, protein, andglycemic index on postprandial glucose controlin type 1 diabetes: implications for intensive diabe-tes management in the continuous glucose moni-toring era. Diabetes Care 2015;38:1008–10156. YehH-C, Brown TT,Maruthur N, et al. Compar-ative effectiveness and safety of methods of in-sulin delivery and glucosemonitoring for diabetesmellitus: a systematic review and meta-analysis.Ann Intern Med 2012;157:336–3477. Bergenstal RM, Klonoff DC, Garg SK, et al.;ASPIRE In-Home Study Group. Threshold-basedinsulin-pump interruption for reduction of hypo-glycemia. N Engl J Med 2013;369:224–2328. Wood JR, Miller KM, Maahs DM, et al.; T1DExchange Clinic Network. Most youth withtype 1 diabetes in the T1D Exchange Clinic Reg-istry do not meet American Diabetes Associa-tion or International Society for Pediatric andAdolescent Diabetes clinical guidelines. Diabe-tes Care 2013;36:2035–20379. Kmietowicz Z Insulin pumps improve controland reduce complications in children withtype 1 diabetes. BMJ 2013;347:f515410. Phillip M, Battelino T, Atlas E, et al. Nocturnalglucose control with an artificial pancreas at a di-abetes camp. N Engl J Med 2013;368:824–83311. The Diabetes Control and ComplicationsTrial Research Group. The effect of intensivetreatment of diabetes on the developmentand progression of long-term complications ininsulin-dependent diabetes mellitus. N Engl JMed 1993;329:977–986
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S73

12. Nathan DM, Cleary PA, Backlund J-YC, et al.;Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions andComplications (DCCT/EDIC) Study ResearchGroup. Intensive diabetes treatment and car-diovascular disease in patients with type 1 di-abetes. N Engl J Med 2005;353:2643–265313. Diabetes Control and Complications Trial(DCCT)/Epidemiology of Diabetes Interventionsand Complications (EDIC) Study ResearchGroup. Mortality in type 1 diabetes in theDCCT/EDIC versus the general population. Dia-betes Care 2016;39:1378–138314. DeWitt DE, Hirsch IB. Outpatient insulintherapy in type 1 and type 2 diabetes mellitus:scientific review. JAMA 2003;289:2254–226415. Rosenstock J, Dailey G, Massi-Benedetti M,Fritsche A, Lin Z, SalzmanA. Reduced hypoglycemiarisk with insulin glargine: a meta-analysis compar-ing insulin glargine with human NPH insulin intype 2 diabetes. Diabetes Care 2005;28:950–95516. BodeBW,McGill JB, LorberDL,Gross JL, ChangPC, Bregman DB; Affinity 1 Study Group. Inhaledtechnosphere insulin comparedwith injected pran-dial insulin in type 1 diabetes: a randomized24-week trial. Diabetes Care 2015;38:2266–227317. American Diabetes Association. Pancreasand islet transplantation in type 1 diabetes. Di-abetes Care 2006;29:93518. Vella S, Buetow L, Royle P, Livingstone S,Colhoun HM, Petrie JR. The use of metforminin type 1 diabetes: a systematic review of effi-cacy. Diabetologia 2010;53:809–82019. –U.S. Food and Drug Administration. SGLT2Inhibitors: Drug Safety Communication - Labelsto Include Warnings About Too Much Acid inthe Blood and Serious Urinary Tract Infections[Internet]. Available from http://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/ucm475553.htm. Accessed 3 October 201620. Palmer SC, Mavridis D, Nicolucci A, et al.Comparison of clinical outcomes and adverseevents associated with glucose-lowering drugsin patients with type 2 diabetes: a meta-analysis.JAMA 2016;316:313–32421. Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of hyperglycemia in type 2 diabetes,2015: a patient-centered approach: update to aposition statement of the American Diabetes Asso-ciation and the European Association for the Studyof Diabetes. Diabetes Care 2015;38:140–14922. HolmanRR, Paul SK, BethelMA,MatthewsDR,Neil HAW. 10-year follow-up of intensive glucosecontrol in type 2 diabetes. N Engl J Med 2008;359:1577–158923. Bennett WL, Maruthur NM, Singh S, et al.Comparative effectiveness and safety of medi-cations for type 2 diabetes: an update includingnew drugs and 2-drug combinations. Ann InternMed 2011;154:602–61324. U.S. Food and Drug Administration. Metformin-containing Drugs: Drug Safety Communication -Revised Warnings for Certain Patients WithReduced Kidney Function [Internet]. Availablefrom http://www.fda.gov/Safety/MedWatch/
SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm494829.htm?source5govdelivery&utm_medium5email&utm_source5govdelivery.Accessed 3 October 201625. Aroda VR, Edelstein SL, Goldberg RB, et al.;Diabetes Prevention Program Research Group.Long-term metformin use and vitamin B12 defi-ciency in the Diabetes Prevention Program Out-comes Study. J Clin Endocrinol Metab 2016;101:1754–176126. Vijan S, Sussman JB, Yudkin JS, Hayward RA.Effect of patients’ risks and preferences onhealth gains with plasma glucose level loweringin type 2 diabetes mellitus. JAMA Intern Med2014;174:1227–123427. Institute for Clinical and Economic Review.Controversies in the Management of Patientswith Type 2 Diabetes [Internet]. Available fromhttp://icer-review.org/wp-content/uploads/2015/03/CEPAC-T2D-Final-Report-December-22.pdf.Accessed 17 November 201628. Nathan DM, Buse JB, Kahn SE, et al.; GRADEStudy Research Group. Rationale and design ofthe Glycemia Reduction Approaches in Diabetes: AComparative Effectiveness Study (GRADE). Diabe-tes Care 2013;36:2254–226129. Zinman B, Wanner C, Lachin JM, et al.;EMPA-REG OUTCOME Investigators. Empagli-flozin, cardiovascular outcomes, and mortalityin type 2 diabetes. N Engl JMed 2015;373:2117–212830. Marso SP, Daniels GH, Brown-Frandsen K,et al.; LEADER Steering Committee; LEADER TrialInvestigators. Liraglutide and cardiovascularoutcomes in type 2 diabetes. N Engl J Med2016;375:311–32231. Green JB, Bethel MA, Armstrong PW, et al.;TECOS Study Group. Effect of sitagliptin on car-diovascular outcomes in type 2 diabetes. N EnglJ Med 2015;373:232–24232. Scirica BM, Bhatt DL, Braunwald E, et al.;SAVOR-TIMI 53 Steering Committee and Investiga-tors. Saxagliptin and cardiovascular outcomes inpatients with type 2 diabetes mellitus. N Engl JMed 2013;369:1317–132633. White WB, Cannon CP, Heller SR, et al.;EXAMINE Investigators. Alogliptin after acutecoronary syndrome in patients with type 2 di-abetes. N Engl J Med 2013;369:1327–133534. Blonde L, Merilainen M, Karwe V, Raskin P;TITRATE Study Group. Patient-directed titrationfor achieving glycaemic goals using a once-dailybasal insulin analogue: an assessment of twodifferent fasting plasma glucose targets - theTITRATE study. Diabetes Obes Metab 2009;11:623–63135. Tricco AC, Ashoor HM, Soobiah C, et al.Safety, effectiveness, and cost of long-actingversus intermediate-acting insulin for type 1 di-abetes: protocol for a systematic review andnetwork meta-analysis. Syst Rev 2013;2:7336. Hua X, Carvalho N, Tew M, Huang ES,Herman WH, Clarke P. Expenditures and pricesof antihyperglycemic medications in theUnited States: 2002-2013. JAMA 2016;315:1400–1402
37. Diamant M, Nauck MA, Shaginian R, et al.; 4BStudy Group. Glucagon-like peptide 1 receptoragonist or bolus insulin with optimized basal in-sulin in type 2 diabetes. Diabetes Care 2014;37:2763–277338. Eng C, Kramer CK, Zinman B, Retnakaran R.Glucagon-like peptide-1 receptor agonist andbasal insulin combination treatment for themanagement of type 2 diabetes: a systematicreview and meta-analysis. Lancet 2014;384:2228–223439. Dieuzeide G, Chuang L-M, Almaghamsi A,Zilov A, Chen J-W, Lavalle-Gonzalez FJ. Safetyand effectiveness of biphasic insulin aspart30 in people with type 2 diabetes switching frombasal-bolus insulin regimens in the A1chieve study.Prim Care Diabetes 2014;8:111–11740. Mathieu C, Storms F, Tits J, Veneman TF,Colin IM. Switching from premixed insulin tobasal-bolus insulin glargine plus rapid-acting in-sulin: the ATLANTIC study. Acta Clin Belg 2013;68:28–3341. Giugliano D, Chiodini P, Maiorino MI,Bellastella G, Esposito K. Intensification of insu-lin therapy with basal-bolus or premixed insulinregimens in type 2 diabetes: a systematic reviewand meta-analysis of randomized controlledtrials. Endocrine 2016;51:417–42842. Kernan WN, Viscoli CM, Furie KL, et al.; IRISTrial Investigators. Pioglitazone after ischemicstroke or transient ischemic attack. N Engl JMed 2016;374:1321–133143. Dormandy JA, Charbonnel B, Eckland DJA,et al.; PROactive Investigators. Secondary pre-vention of macrovascular events in patientswith type 2 diabetes in the PROactive Study(PROspective pioglitAzone Clinical Trial InmacroVascular Events): a randomised controlledtrial. Lancet 2005;366:1279–128944. Chiasson J-L, Josse RG, Gomis R, HanefeldM, Karasik A, Laakso M; STOP-NIDDM Trial Re-search Group. Acarbose for prevention of type 2diabetesmellitus: the STOP-NIDDM randomisedtrial. Lancet 2002;359:2072–207745. UK Prospective Diabetes Study (UKPDS)Group. Intensive blood-glucose control with sul-phonylureas or insulin compared with conven-tional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33). Lan-cet 1998;352:837–85346. UK Prospective Diabetes Study (UKPDS)Group. Effect of intensive blood-glucose controlwith metformin on complications in overweightpatients with type 2 diabetes (UKPDS 34). Lan-cet 1998;352:854–86547. Gaziano JM, Cincotta AH, O’Connor CM,et al. Randomized clinical trial of quick-releasebromocriptine among patients with type 2diabetes on overall safety and cardiovascu-lar outcomes. Diabetes Care 2010;33:1503–150848. Truven Health Analytics. Red Book: A Com-prehensive, Consistent Drug Pricing Resource[Internet], 2016. Available from http://micromedix.com/products/product-suites/clinical-knowledge/redbook. Accessed 29 July 2016
S74 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 40, Supplement 1, January 2017