Embed Size (px)
Citation preview
8. Pharmacologic Approaches toGlycemic Treatment: Standards ofMedical Care in Diabetesd2018Diabetes Care 2018;41(Suppl. 1):S73–S85 | https://doi.org/10.2337/dc18-S008
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes”includes ADA’s current clinical practice recommendations and is intended to providethe components of diabetes care, general treatment goals and guidelines, and toolsto evaluate quality of care. Members of the ADA Professional Practice Committee, amultidisciplinary expert committee, are responsible for updating the Standardsof Care annually, or more frequently as warranted. For a detailed description ofADA standards, statements, and reports, as well as the evidence-grading systemfor ADA’s clinical practice recommendations, please refer to the Standards of CareIntroduction. Readers who wish to comment on the Standards of Care are invited todo so at professional.diabetes.org/SOC.
PHARMACOLOGIC THERAPY FOR TYPE 1 DIABETES
Recommendations
c Most people with type 1 diabetes should be treated with multiple daily in-jections of prandial insulin and basal insulin or continuous subcutaneousinsulin infusion. A
c Most individuals with type 1 diabetes should use rapid-acting insulin analogs toreduce hypoglycemia risk. A
c Consider educating individuals with type 1 diabetes onmatching prandial insulindoses to carbohydrate intake, premeal blood glucose levels, and anticipatedphysical activity. E
c Individuals with type 1 diabetes who have been successfully using continuoussubcutaneous insulin infusion should have continued access to this therapy afterthey turn 65 years of age. E
Insulin TherapyInsulin is the mainstay of therapy for individuals with type 1 diabetes. Generally,the starting insulin dose is based on weight, with doses ranging from 0.4 to1.0 units/kg/day of total insulin with higher amounts required during puberty.The American Diabetes Association/JDRF Type 1 Diabetes Sourcebook notes0.5 units/kg/day as a typical starting dose in patients with type 1 diabetes whoare metabolically stable, with higher weight-based dosing required immediatelyfollowing presentation with ketoacidosis (1), and provides detailed informationon intensification of therapy to meet individualized needs. The American DiabetesAssociation (ADA) position statement “Type 1 Diabetes Management Throughthe Life Span” additionally provides a thorough overview of type 1 diabetestreatment (2).
Suggested citation: American Diabetes Associ-ation. 8. Pharmacologic approaches to glyce-mic treatment: Standards of Medical Care inDiabetesd2018. Diabetes Care 2018;41(Suppl. 1):S73–S85
© 2017 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
American Diabetes Association
Diabetes Care Volume 41, Supplement 1, January 2018 S73
8.PHARMACOLO
GIC
APPROACHES
TOGLYCEM
ICTR
EATM
ENT

Education regarding matching prandialinsulin dosing to carbohydrate intake,premeal glucose levels, and anticipatedactivity should be considered, and se-lected individuals who have masteredcarbohydrate counting should be edu-cated on fat and protein gram estimation(3–5). Although most studies of multipledaily injections versus continuous subcu-taneous insulin infusion (CSII) have beensmall and of short duration, a systematicreview and meta-analysis concluded thatthere are minimal differences betweenthe two forms of intensive insulin therapyin A1C (combined mean between-groupdifference favoring insulin pump therapy–0.30% [95% CI –0.58 to –0.02]) and se-vere hypoglycemia rates in children andadults (6). A 3-month randomized trial inpatients with type 1 diabeteswith noctur-nal hypoglycemia reported that sensor-augmented insulin pump therapy withthe threshold suspend feature reducednocturnal hypoglycemia without increas-ing glycated hemoglobin levels (7). TheU.S. Food and Drug Administration (FDA)has also approved the first hybrid closed-loop system pump. The safety and effi-cacy of hybrid closed-loop systems hasbeen supported in the literature in ado-lescents and adults with type 1 diabetes(8,9).Intensive management using CSII and
continuous glucose monitoring should beencouraged in selected patients whenthere is active patient/family participa-tion (10–12).The Diabetes Control and Complica-
tions Trial (DCCT) clearly showed that in-tensive therapy with multiple dailyinjections or CSII delivered by multidisci-plinary teams of physicians, nurses, dieti-tians, and behavioral scientists improvedglycemia and resulted in better long-termoutcomes (13–15). The study was carriedout with short-acting and intermediate-acting human insulins. Despite better mi-crovascular, macrovascular, and all-causemortality outcomes, intensive therapywas associated with a high rate of severehypoglycemia (61episodesper100patient-yearsof therapy). Since theDCCT, anumberof rapid-acting and long-acting insulin an-alogs have beendeveloped. These analogsare associated with less hypoglycemia,less weight gain, and lower A1C than humaninsulins in people with type 1 diabetes(16–18). Longer-acting basal analogs(U-300 glargine or degludec) may addi-tionally convey a lower hypoglycemia risk
compared with U-100 glargine in patientswith type 1 diabetes (19,20).
Rapid-acting inhaled insulin used be-fore meals in patients with type 1 diabe-tes was shown to be noninferior whencomparedwith aspart insulin for A1C low-ering, with less hypoglycemia observedwith inhaled insulin therapy (21). How-ever, the mean reduction in A1C wasgreater with aspart (–0.21% vs. –0.40%,satisfying the noninferiority margin of0.4%), and more patients in the insulinaspart group achieved A1C goals of#7.0% (53 mmol/mol) and #6.5% (48mmol/mol). Because inhaled insulin car-tridges are only available in 4-, 8-, and12-unit doses, limited dosing incrementsto fine-tune prandial insulin doses in type 1diabetes are a potential limitation.
Postprandial glucose excursions maybe better controlled by adjusting the tim-ing of prandial (bolus) insulin dose admin-istration. The optimal time to administerprandial insulin varies, based on the typeof insulin used (regular, rapid-acting ana-log, inhaled, etc.), measured blood glucoselevel, timing of meals, and carbohydrateconsumption. Recommendations for pran-dial insulin dose administration shouldtherefore be individualized.
PramlintidePramlintide, an amylin analog, is an agentthat delays gastric emptying, blunts pan-creatic secretion of glucagon, and en-hances satiety. It is FDA-approved for usein adults with type 1 diabetes. It has beenshown to induce weight loss and lower in-sulin doses. Concurrent reduction of pran-dial insulin dosing is required to reduce therisk of severe hypoglycemia.
Investigational Agents
Metformin
Adding metformin to insulin therapy mayreduce insulin requirements and improvemetabolic control in patients with type 1diabetes. In one study, metformin wasfound to reduce insulin requirements(6.6 units/day, P , 0.001), and led tosmall reductions in weight and total andLDL cholesterol but not to improved gly-cemic control (absolute A1C reduction0.11%, P5 0.42) (22). A randomized clin-ical trial similarly found that, among over-weight adolescents with type 1 diabetes,the addition of metformin to insulin didnot improve glycemic control and in-creased risk for gastrointestinal adverseevents after 6 months compared with
placebo (23). TheReducingWithMetforminVascular Adverse Lesions in Type1Diabetes(REMOVAL) trial investigated the additionof metformin therapy to titrated insulintherapy in adults with type 1 diabetes atincreased risk for cardiovascular diseaseand found that metformin did not signifi-cantly improve glycemic control beyondthe first 3 months of treatment and thatprogression of atherosclerosis (measuredby carotid artery intima-media thickness)was not significantly reduced, althoughother cardiovascular risk factors such asbody weight and LDL cholesterol im-proved (24). Metformin is not FDA-approved for use in patients with type 1diabetes.
Incretin-Based Therapies
Due to their potential protection of b-cellmass and suppressionof glucagon release,glucagon-like peptide 1 (GLP-1) receptoragonists (25) and dipeptidyl peptidase4 (DPP-4) inhibitors (26) are being studiedin patients with type 1 diabetes but arenot currently FDA-approved for use in pa-tients with type 1 diabetes.
Sodium–Glucose Cotransporter 2 Inhibitors
Sodium–glucose cotransporter 2 (SGLT2)inhibitors provide insulin-independentglucose lowering by blocking glucose re-absorption in theproximal renal tubule byinhibiting SGLT2. These agents providemodest weight loss and blood pressurereduction in type 2 diabetes. There arethree FDA-approved agents for patientswith type 2 diabetes, but none are FDA-approved for the treatment of patientswith type 1 diabetes (2). SGLT2 inhibitorsmay have glycemic benefits in patientswith type 1 or type 2 diabetes on insulintherapy (27). The FDA issued a warningabout the risk of ketoacidosis occurringin the absence of significant hyperglyce-mia (euglycemic diabetic ketoacidosis)in patients with type 1 or type 2 diabe-tes treated with SGLT2 inhibitors.Symptoms of ketoacidosis include dysp-nea, nausea, vomiting, and abdominalpain. Patients should be instructed tostop taking SGLT2 inhibitors and seekmedical attention immediately if theyhave symptoms or signs of ketoacidosis(28).
SURGICAL TREATMENT FORTYPE 1 DIABETES
Pancreas and Islet TransplantationPancreas and islet transplantation havebeen shown to normalize glucose levels
S74 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 41, Supplement 1, January 2018

but require life-long immunosuppressionto prevent graft rejection and recurrenceof autoimmune islet destruction. Giventhe potential adverse effects of immuno-suppressive therapy, pancreas transplan-tation should be reserved for patientswith type 1 diabetes undergoing simulta-neous renal transplantation, following re-nal transplantation, or for those withrecurrent ketoacidosis or severe hypogly-cemia despite intensive glycemic man-agement (29).
PHARMACOLOGIC THERAPY FORTYPE 2 DIABETES
Recommendations
c Metformin, if not contraindicatedand if tolerated, is the preferred ini-tial pharmacologic agent for thetreatment of type 2 diabetes. A
c Long-term use of metformin may beassociated with biochemical vitaminB12 deficiency, and periodic mea-surementofvitaminB12 levels shouldbe considered in metformin-treatedpatients, especially in those with ane-mia or peripheral neuropathy. B
c Consider initiating insulin therapy(with or without additional agents)in patients with newly diagnosedtype 2 diabetes who are symptom-atic and/or have A1C $10% (86mmol/mol) and/or blood glucoselevels$300mg/dL (16.7mmol/L). E
c Consider initiating dual therapy inpatients with newly diagnosedtype 2 diabetes who have A1C$9% (75 mmol/mol). E
c In patients without atheroscleroticcardiovascular disease, if mono-therapy or dual therapy does notachieve or maintain the A1C goalover 3 months, add an additionalantihyperglycemic agent based ondrug-specific and patient factors(Table 8.1). A
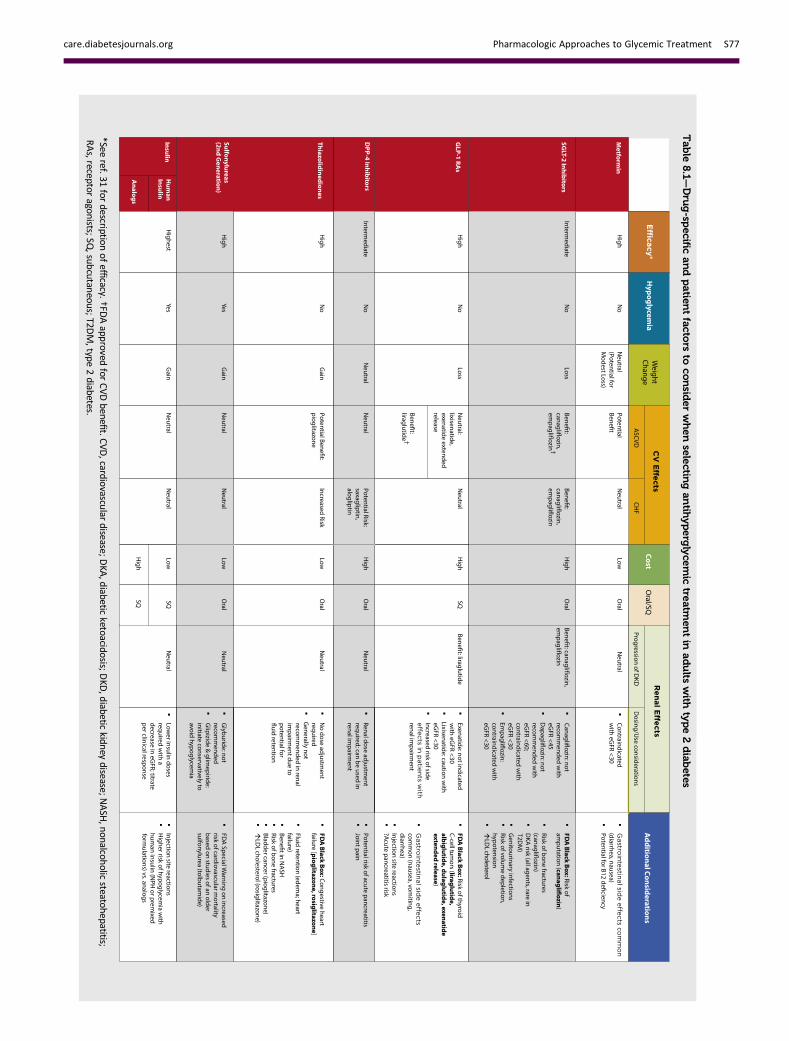
c A patient-centered approach shouldbe used to guide the choice ofpharmacologic agents. Consider-ations include efficacy, hypoglyce-mia risk, history of atheroscleroticcardiovascular disease, impact onweight, potential side effects, re-nal effects, delivery method (oralversus subcutaneous), cost, andpatient preferences. E
c In patients with type 2 diabetes andestablished atherosclerotic cardio-vascular disease, antihyperglycemic
therapy should begin with lifestylemanagement and metformin andsubsequently incorporate an agentproven to reduce major adverse car-diovascular events and cardiovascu-lar mortality (currently empagliflozinand liraglutide), after consideringdrug-specific and patient factors(Table 8.1). A*
c In patients with type 2 diabetes andestablished atherosclerotic cardiovascu-lar disease, after lifestyle managementand metformin, the antihyperglycemicagent canagliflozin may be consideredto reduce major adverse cardiovascularevents, based on drug-specific and pa-tient factors (Table 8.1). C*
c Continuous reevaluationof themed-ication regimen and adjustment asneeded to incorporate patient fac-tors (Table 8.1) and regimen com-plexity is recommended. E
c For patients with type 2 diabeteswhoarenot achieving glycemic goals,drug intensification, including consid-eration of insulin therapy, should notbe delayed. B
c Metformin should be continuedwhenused in combinationwithotheragents, including insulin, if not contra-indicated and if tolerated. A
See Section 12 for recommendationsspecific for children and adolescentswith type 2 diabetes. The use of metfor-min as first-line therapywas supported byfindings from a large meta-analysis, withselection of second-line therapies basedon patient-specific considerations (30).An ADA/European Association for the Studyof Diabetes position statement “Manage-ment of Hyperglycemia in Type 2 Diabe-tes, 2015: A Patient-Centered Approach”(31) recommended a patient-centered ap-proach, including assessment of efficacy,hypoglycemia risk, impact on weight, sideeffects, costs, and patient preferences. Re-nal effects may also be considered whenselecting glucose-loweringmedications forindividual patients. Lifestyle modificationsthat improvehealth (see Section4 “LifestyleManagement”) should be emphasizedalong with any pharmacologic therapy.
Initial TherapyMetformin monotherapy should bestarted at diagnosis of type 2 diabetes un-less there are contraindications. Metfor-min is effective and safe, is inexpensive,
and may reduce risk of cardiovascularevents and death (32). Compared withsulfonylureas, metformin as first-linetherapy has beneficial effects on A1C,weight, and cardiovascular mortality(33). Metformin may be safely used inpatients with estimated glomerular filtra-tion rate (eGFR) as low as 30 mL/min/1.73 m2, and the FDA recently revisedthe label for metformin to reflect itssafety in patients with eGFR $30 mL/min/1.73 m2 (34). Patients should be ad-vised to stop the medication in cases ofnausea, vomiting, or dehydration. Met-formin is associated with vitamin B12deficiency, with a recent report from theDiabetes Prevention Program OutcomesStudy (DPPOS) suggesting that periodictesting of vitamin B12 levels should beconsidered in metformin-treated pa-tients, especially in those with anemiaor peripheral neuropathy (35).
In patients with metformin contrain-dications or intolerance, consider an ini-tial drug from another class depicted inFig. 8.1 under “Dual Therapy” and pro-ceed accordingly. When A1C is $9% (75mmol/mol), consider initiating dual com-bination therapy (Fig. 8.1) to more expe-ditiously achieve the target A1C level.Insulin has the advantage of being effec-tive where other agents may not be andshould be considered as part of any com-bination regimen when hyperglycemia issevere, especially if catabolic features(weight loss, ketosis) are present. Con-sider initiating combination insulin in-jectable therapy (Fig. 8.2) when bloodglucose is$300 mg/dL (16.7 mmol/L) orA1C is$10% (86 mmol/mol) or if the pa-tient has symptoms of hyperglycemia(i.e., polyuria or polydipsia). As the pa-tient’s glucose toxicity resolves, the regi-men may, potentially, be simplified.
Combination TherapyAlthough there are numerous trialscomparing dual therapy with metforminalone, few directly compare drugs as add-on therapy. A comparative effectivenessmeta-analysis (36) suggests that eachnew class of noninsulin agents added toinitial therapy generally lowers A1C ap-proximately 0.7–1.0%. If the A1C targetisnotachievedafterapproximately3monthsand patient does not have atheroscleroticcardiovascular disease (ASCVD), considera combination of metformin and any oneof the preferred six treatment options:sulfonylurea, thiazolidinedione, DPP-4
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S75
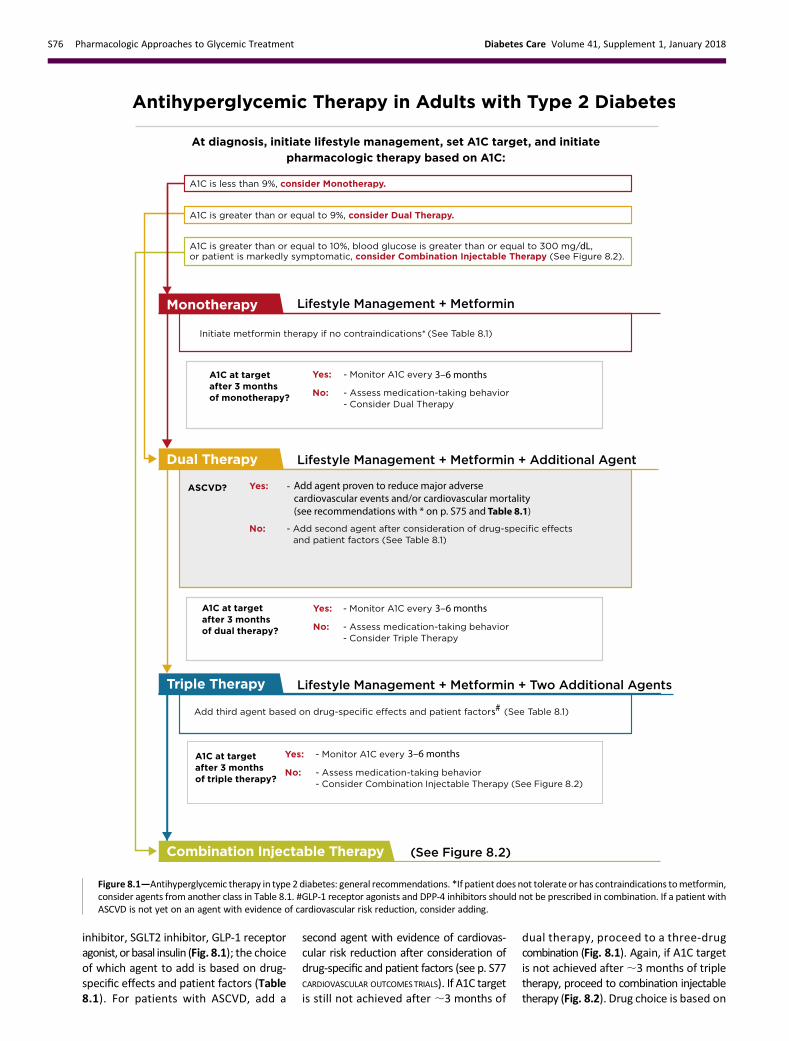
inhibitor, SGLT2 inhibitor, GLP-1 receptoragonist, orbasal insulin (Fig. 8.1); the choiceof which agent to add is based on drug-specific effects and patient factors (Table8.1). For patients with ASCVD, add a
second agent with evidence of cardiovas-cular risk reduction after consideration ofdrug-specific and patient factors (see p. S77CARDIOVASCULAR OUTCOMESTRIALS). If A1C targetis still not achieved after ;3 months of
dual therapy, proceed to a three-drugcombination (Fig. 8.1). Again, if A1C targetis not achieved after;3 months of tripletherapy, proceed to combination injectabletherapy (Fig. 8.2). Drug choice is based on
Figure 8.1—Antihyperglycemic therapy in type 2 diabetes: general recommendations. *If patient does not tolerate or has contraindications tometformin,consider agents from another class in Table 8.1. #GLP-1 receptor agonists and DPP-4 inhibitors should not be prescribed in combination. If a patient withASCVD is not yet on an agent with evidence of cardiovascular risk reduction, consider adding.
S76 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 41, Supplement 1, January 2018
Tab
le8.1—Dru
g-sp
ecificandpatien
tfacto
rsto
consid
erwhensele
ctingan
tihyperglyce
mic
treatm
entin
adults
with
type2diab
etes
*Seeref.31
fordescriptio
nofefficacy.
†FDAapp
rovedfor
CVDbene
fit.CVD,cardio
vascular
disease;DKA
,diabetic
ketoacidosis;DKD
,diabetic
kidney
disease;NASH
,nonalcoh
olicsteatohepatitis;
RAs,receptor
agonists;SQ,sub
cutaneous;T2D
M,type
2diabetes.
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S77

patient preferences (37), as well as variouspatient, disease, and drug characteristics,with the goal of reducing blood glucoselevelswhileminimizing side effects, espe-cially hypoglycemia. If not already in-cluded in the treatment regimen, additionof an agent with evidence of cardiovas-cular risk reduction should be consid-ered in patients with ASCVD beyond
dual therapy, with continuous reevalu-ation of patient factors to guide treat-ment (Table 8.1).
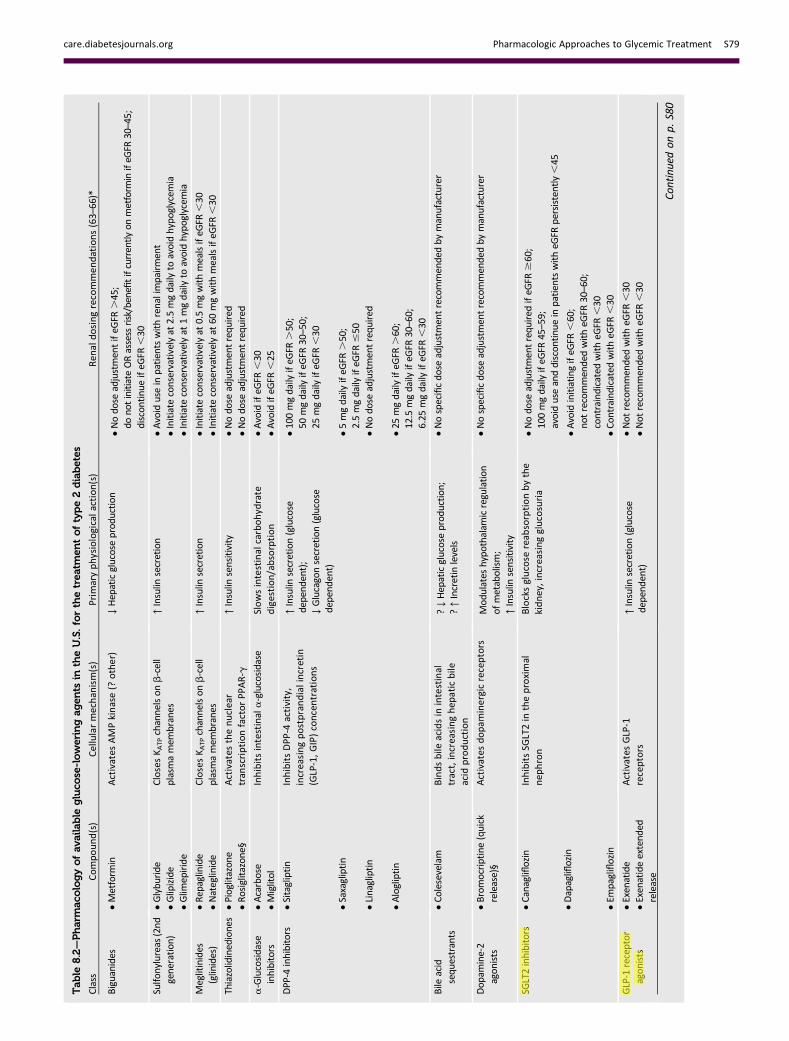
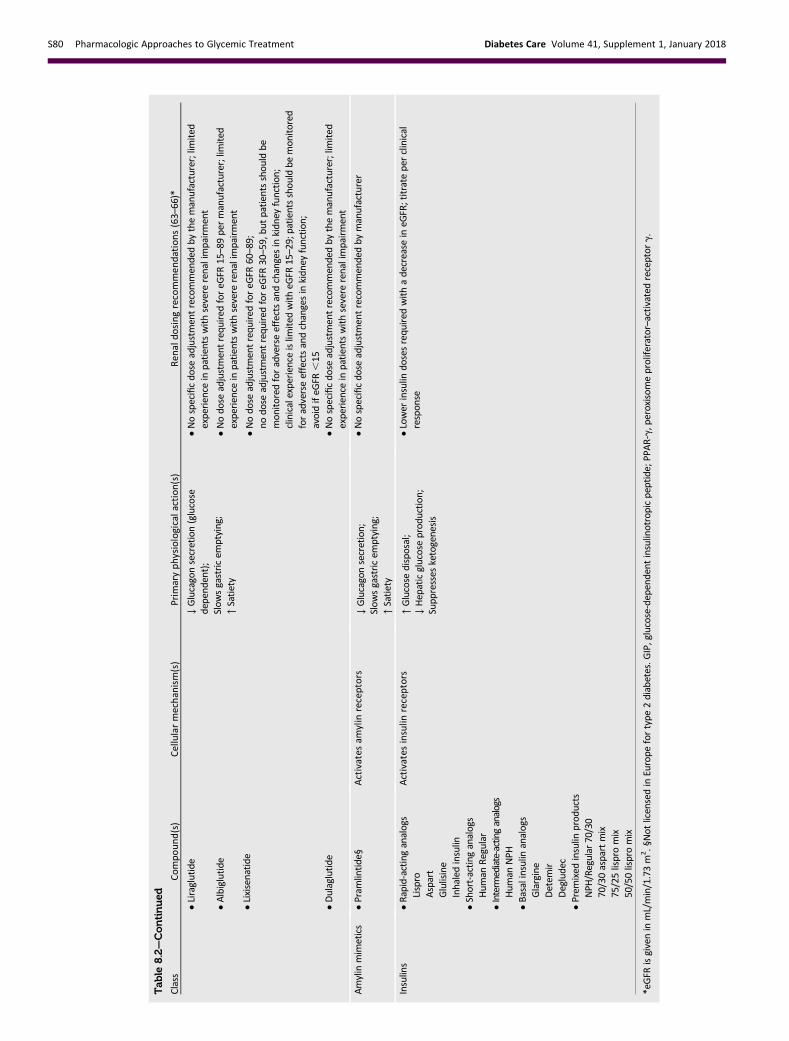
Table 8.2 lists drugs commonly used inthe U.S. Cost-effectiveness models of thenewer agents based on clinical utility andglycemic effect have been reported (38).Table 8.3 provides cost information forcurrently approved noninsulin therapies.
Of note, prices listed are average whole-sale prices (AWP) (39) and National Aver-age Drug Acquisition Costs (NADAC) (40)and do not account for discounts, re-bates, or other price adjustments ofteninvolved in prescription sales that affectthe actual cost incurred by the patient.While there are alternative means to esti-mate medication prices, AWP and NADAC
Figure 8.2—Combination injectable therapy for type 2 diabetes. FBG, fasting blood glucose; hypo, hypoglycemia. Adapted with permission from Inzucchiet al. (31).
S78 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 41, Supplement 1, January 2018
Tab
le8.2—Pharmac
ologyofav
ailable
gluco
se-loweringag
ents
intheU.S.forthetrea
tmen
toftype2diabetes
Class
Compound(s)
Cellularmechanism(s)
Prim
aryphysiologicalaction(s)
Ren
aldosingrecommen
dations(63–66)*
Biguanides
cMetform
inActivates
AMPkinase(?
other)
↓Hepaticglucoseprod
uction
cNodo
seadjustmentifeG
FR.45;
donotinitiateORassessrisk/benefitifcurrently
onmetform
inifeG
FR30–45;
discon
tinu
eifeG
FR,30
Sulfo
nylureas
(2nd
generation
)cGlybu
ride
ClosesK A
TPchannelson
b-cell
plasmamem
branes
↑Insulin
secretion
cAvoiduseinpatientswithrenalimpairment
cGlipizide
cInitiate
conservativelyat
2.5mgdaily
toavoidhypo
glycem
iacGlim
epiride
cInitiate
conservativelyat
1mgdaily
toavoidhypo
glycem
ia
Meglitinides
(glinides)
cRepaglinide
ClosesK A
TPchannelson
b-cell
plasmamem
branes
↑Insulin
secretion
cInitiate
conservativelyat
0.5mgwithmealsifeG
FR,30
cNateglinide
cInitiate
conservativelyat
60mgwithmealsifeG
FR,30
Thiazolidinediones
cPioglitazon
eActivates
thenuclear
tran
scriptionfactorPP
AR-g
↑Insulin
sensitivity
cNodo
seadjustmentrequ
ired
cRosiglitazon
e§cNodo
seadjustmentrequ
ired
a-Glucosidase
inhibitors
cAcarbose
Inhibitsintestinala-glucosidase
Slowsintestinalcarbohydrate
digestion/absorption
cAvoidifeG
FR,30
cMiglitol
cAvoidifeG
FR,25
DPP-4
inhibitors
cSitagliptin
InhibitsDPP
-4activity,
increasingpostprandialincretin
(GLP-1,GIP)concentrations
↑Insulin
secretion(glucose
depend
ent);
↓Glucagonsecretion(glucose
depend
ent)
c100mgdaily
ifeG
FR.50;
50mgdaily
ifeG
FR30–50;
25mgdaily
ifeG
FR,30
cSaxagliptin
c5mgdaily
ifeG
FR.50;
2.5mgdaily
ifeG
FR#50
cLinagliptin
cNodo
seadjustmentrequ
ired
cAlogliptin
c25
mgdaily
ifeG
FR.60;
12.5mgdaily
ifeG
FR30–60;
6.25
mgdaily
ifeG
FR,30
Bile
acid
sequ
estrants
cColesevelam
Bindsbile
acidsin
intestinal
tract,increasinghep
aticbile
acid
production
?↓Hepaticglucoseprod
uction
;?↑Incretinlevels
cNospecificdo
seadjustmentrecommendedby
manufacturer
Dop
amine-2
agon
ists
cBromocriptine(quick
release)§
Activates
dopam
inergicreceptors
Mod
ulates
hypo
thalam
icregulation
ofmetabolism;
↑Insulin
sensitivity
cNospecificdo
seadjustmentrecommendedby
manufacturer
SGLT2inhibitors
cCanagliflozin
InhibitsSG
LT2in
theproximal
nep
hron
Blocksglucose
reab
sorptionbythe
kidney,increasingglucosuria
cNodo
seadjustmentrequ
ired
ifeG
FR$60;
100mgdaily
ifeG
FR45–59;
avoiduseanddiscon
tinu
einpatientswitheG
FRpersistently,45
cDapagliflozin
cAvoidinitiating
ifeG
FR,60;
notrecommendedwitheG
FR30–60;
contraindicatedwitheG
FR,30
cEm
pagliflozin
cCon
traind
icated
witheG
FR,30
GLP-1
receptor
agon
ists
cExenatide
Activates
GLP-1
receptors
↑Insulin
secretion(glucose
depend
ent)
cNot
recommendedwitheG
FR,30
cExenatideextend
edrelease
cNot
recommendedwitheG
FR,30
Continuedon
p.S80
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S79
Tab
le8.2—Continued
Class
Compound(s)
Cellularmechanism(s)
Prim
aryphysiologicalaction(s)
Ren
aldosingrecommen
dations(63–66)*
↓Glucagonsecretion(glucose
depend
ent);
Slow
sgastricem
ptying;
↑Satiety
cLiraglutide
cNospecificdo
seadjustmentrecommendedby
themanufacturer;lim
ited
experience
inpatientswithsevere
renalimpairment
cAlbiglutide
cNodo
seadjustmentrequ
ired
foreG
FR15–89permanufacturer;lim
ited
experience
inpatientswithsevere
renalimpairment
cLixisenatide
cNodo
seadjustmentrequ
ired
foreG
FR60–89;
nodo
seadjustmentrequ
ired
foreG
FR30–59,bu
tpatientsshou
ldbe
mon
itored
foradverseeffectsandchangesinkidn
eyfunction
;clinicalexperience
islim
ited
witheG
FR15–29;patientsshou
ldbe
mon
itored
foradverseeffectsandchangesinkidn
eyfunction
;avoidifeG
FR,15
cDulaglutide
cNospecificdo
seadjustmentrecommendedby
themanufacturer;lim
ited
experience
inpatientswithsevere
renalimpairment
Amylinmimetics
cPram
lintide§
Activates
amylin
receptors
↓Glucagonsecretion;
Slow
sgastricem
ptying;
↑Satiety
cNospecificdo
seadjustmentrecommendedby
manufacturer
Insulins
cRapid-actinganalogs
Activates
insulin
receptors
↑Glucose
disposal;
↓Hepaticglucoseprod
uction
;Supp
resses
ketogenesis
cLower
insulin
dosesrequ
ired
withadecrease
ineG
FR;titrate
perclinical
respon
seLispro
Aspart
Glulisine
Inhaledinsulin
cShort-acting
analogs
Hum
anRegular
cInterm
ediate-actinganalogs
Hum
anNPH
cBasalinsulin
analogs
Glargine
Detem
irDegludec
cPrem
ixed
insulin
prod
ucts
NPH
/Regular
70/30
70/30aspartmix
75/25lispromix
50/50lispromix
*eGFR
isgiveninmL/min/1.73m
2.§Not
licensedinEurope
fortype
2diabetes.G
IP,glucose-dependent
insulinotropicpeptide;PPAR-g,peroxisom
eproliferator–activatedreceptor
g.
S80 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 41, Supplement 1, January 2018
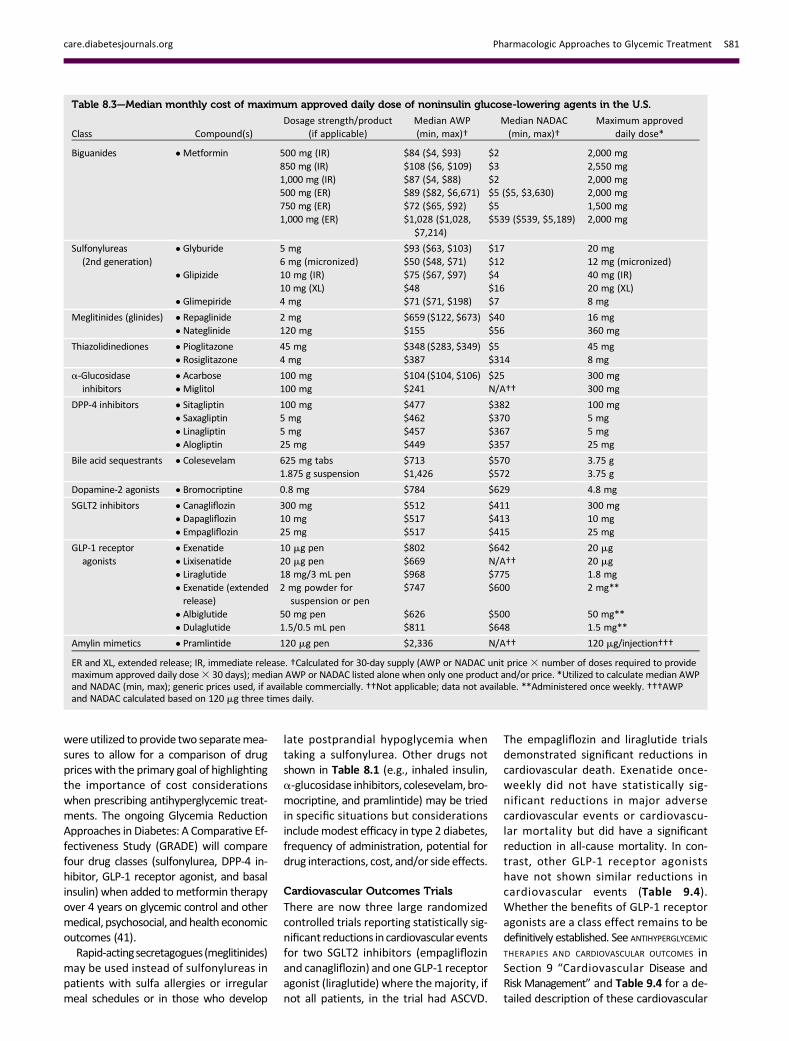
were utilized to provide two separatemea-sures to allow for a comparison of drugprices with the primary goal of highlightingthe importance of cost considerationswhen prescribing antihyperglycemic treat-ments. The ongoing Glycemia ReductionApproaches in Diabetes: A Comparative Ef-fectiveness Study (GRADE) will comparefour drug classes (sulfonylurea, DPP-4 in-hibitor, GLP-1 receptor agonist, and basalinsulin) when added tometformin therapyover 4 years on glycemic control and othermedical, psychosocial, and health economicoutcomes (41).Rapid-actingsecretagogues (meglitinides)
may be used instead of sulfonylureas inpatients with sulfa allergies or irregularmeal schedules or in those who develop
late postprandial hypoglycemia whentaking a sulfonylurea. Other drugs notshown in Table 8.1 (e.g., inhaled insulin,a-glucosidase inhibitors, colesevelam,bro-mocriptine, and pramlintide) may be triedin specific situations but considerationsincludemodest efficacy in type 2 diabetes,frequency of administration, potential fordrug interactions, cost, and/or side effects.
Cardiovascular Outcomes Trials
There are now three large randomizedcontrolled trials reporting statistically sig-nificant reductions in cardiovascular eventsfor two SGLT2 inhibitors (empagliflozinand canagliflozin) and one GLP-1 receptoragonist (liraglutide) where themajority, ifnot all patients, in the trial had ASCVD.
The empagliflozin and liraglutide trialsdemonstrated significant reductions incardiovascular death. Exenatide once-weekly did not have statistically sig-nificant reductions in major adversecardiovascular events or cardiovascu-lar mortality but did have a significantreduction in all-cause mortality. In con-trast, other GLP-1 receptor agonistshave not shown similar reductions incardiovascular events (Table 9.4).Whether the benefits of GLP-1 receptoragonists are a class effect remains to bedefinitively established. See ANTIHYPERGLYCEMIC
THERAPIES AND CARDIOVASCULAR OUTCOMES inSection 9 “Cardiovascular Disease andRisk Management” and Table 9.4 for a de-tailed description of these cardiovascular
Table 8.3—Median monthly cost of maximum approved daily dose of noninsulin glucose-lowering agents in the U.S.
Class Compound(s)Dosage strength/product
(if applicable)Median AWP(min, max)†
Median NADAC(min, max)†
Maximum approveddaily dose*
Biguanides c Metformin 500 mg (IR) $84 ($4, $93) $2 2,000 mg850 mg (IR) $108 ($6, $109) $3 2,550 mg1,000 mg (IR) $87 ($4, $88) $2 2,000 mg500 mg (ER) $89 ($82, $6,671) $5 ($5, $3,630) 2,000 mg750 mg (ER) $72 ($65, $92) $5 1,500 mg1,000 mg (ER) $1,028 ($1,028,
$7,214)$539 ($539, $5,189) 2,000 mg
Sulfonylureas(2nd generation)
c Glyburide 5 mg $93 ($63, $103) $17 20 mg6 mg (micronized) $50 ($48, $71) $12 12 mg (micronized)
c Glipizide 10 mg (IR) $75 ($67, $97) $4 40 mg (IR)10 mg (XL) $48 $16 20 mg (XL)
c Glimepiride 4 mg $71 ($71, $198) $7 8 mg
Meglitinides (glinides) c Repaglinide 2 mg $659 ($122, $673) $40 16 mgc Nateglinide 120 mg $155 $56 360 mg
Thiazolidinediones c Pioglitazone 45 mg $348 ($283, $349) $5 45 mgc Rosiglitazone 4 mg $387 $314 8 mg
a-Glucosidaseinhibitors
c Acarbose 100 mg $104 ($104, $106) $25 300 mgc Miglitol 100 mg $241 N/A†† 300 mg
DPP-4 inhibitors c Sitagliptin 100 mg $477 $382 100 mgc Saxagliptin 5 mg $462 $370 5 mgc Linagliptin 5 mg $457 $367 5 mgc Alogliptin 25 mg $449 $357 25 mg
Bile acid sequestrants c Colesevelam 625 mg tabs $713 $570 3.75 g1.875 g suspension $1,426 $572 3.75 g
Dopamine-2 agonists c Bromocriptine 0.8 mg $784 $629 4.8 mg
SGLT2 inhibitors c Canagliflozin 300 mg $512 $411 300 mgc Dapagliflozin 10 mg $517 $413 10 mgc Empagliflozin 25 mg $517 $415 25 mg
GLP-1 receptoragonists
c Exenatide 10 mg pen $802 $642 20 mgc Lixisenatide 20 mg pen $669 N/A†† 20 mgc Liraglutide 18 mg/3 mL pen $968 $775 1.8 mgc Exenatide (extendedrelease)
2 mg powder forsuspension or pen
$747 $600 2 mg**
c Albiglutide 50 mg pen $626 $500 50 mg**c Dulaglutide 1.5/0.5 mL pen $811 $648 1.5 mg**
Amylin mimetics c Pramlintide 120 mg pen $2,336 N/A†† 120 mg/injection†††
ER and XL, extended release; IR, immediate release. †Calculated for 30-day supply (AWP or NADAC unit price3 number of doses required to providemaximum approved daily dose3 30 days); median AWP or NADAC listed alone when only one product and/or price. *Utilized to calculate median AWPand NADAC (min, max); generic prices used, if available commercially. ††Not applicable; data not available. **Administered once weekly. †††AWPand NADAC calculated based on 120 mg three times daily.
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S81
outcomes trials. Additional large random-ized trials of other agents in these classesare ongoing.Of note, these studies examined the
drugs in combination with metformin(Table 9.4) in the great majority of pa-tients for whom metformin was not con-traindicated or not tolerated. For patientswith type 2 diabetes who have ASCVD, onlifestyle and metformin therapy, it is rec-ommended to incorporate an agent withstrong evidence for cardiovascular risk re-duction especially those with proven ben-efit on both major adverse cardiovascularevents and cardiovascular death after con-sideration of drug-specific patient factors(Table 8.1). See Fig. 8.1 for additional rec-ommendations on antihyperglycemictreatment in adults with type 2 diabetes.
Insulin TherapyMany patients with type 2 diabetes even-tually require and benefit from insulintherapy. The progressive nature of type 2diabetes shouldbe regularly andobjectivelyexplained to patients. Providers should
avoid using insulin as a threat or de-scribing it as a sign of personal failureor punishment.
Equipping patientswith an algorithm forself-titration of insulin doses based on self-monitoring of blood glucose improvesglycemic control in patients with type 2 di-abetes initiating insulin (42). Comprehen-sive education regarding self-monitoringof blood glucose, diet, and the avoidanceof and appropriate treatment of hypogly-cemia are critically important in any pa-tient using insulin.
Basal Insulin
Basal insulin alone is themost convenientinitial insulin regimen, beginning at 10unitsper day or 0.1–0.2 units/kg/day, depend-ing on the degree of hyperglycemia. Basalinsulin is usually prescribed in conjunc-tion with metformin and sometimes oneadditional noninsulin agent. When basalinsulin is added to antihyperglycemicagents in patients with type 2 diabetes,long-acting basal analogs (U-100 glargineor detemir) can be used instead of NPH
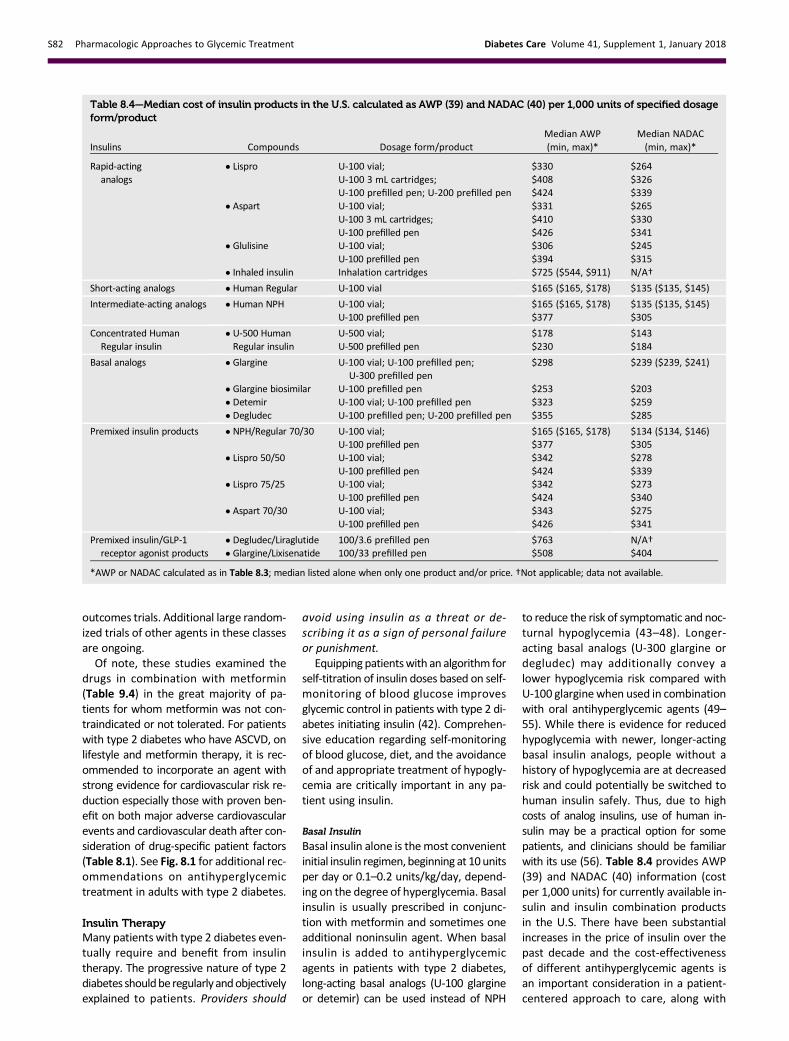
to reduce the risk of symptomatic and noc-turnal hypoglycemia (43–48). Longer-acting basal analogs (U-300 glargine ordegludec) may additionally convey alower hypoglycemia risk compared withU-100 glargine when used in combinationwith oral antihyperglycemic agents (49–55). While there is evidence for reducedhypoglycemia with newer, longer-actingbasal insulin analogs, people without ahistory of hypoglycemia are at decreasedrisk and could potentially be switched tohuman insulin safely. Thus, due to highcosts of analog insulins, use of human in-sulin may be a practical option for somepatients, and clinicians should be familiarwith its use (56). Table 8.4 provides AWP(39) and NADAC (40) information (costper 1,000 units) for currently available in-sulin and insulin combination productsin the U.S. There have been substantialincreases in the price of insulin over thepast decade and the cost-effectivenessof different antihyperglycemic agents isan important consideration in a patient-centered approach to care, along with
Table 8.4—Median cost of insulin products in the U.S. calculated as AWP (39) and NADAC (40) per 1,000 units of specified dosageform/product
Insulins Compounds Dosage form/productMedian AWP(min, max)*
Median NADAC(min, max)*
Rapid-actinganalogs
c Lispro U-100 vial; $330 $264U-100 3 mL cartridges; $408 $326U-100 prefilled pen; U-200 prefilled pen $424 $339
c Aspart U-100 vial; $331 $265U-100 3 mL cartridges; $410 $330U-100 prefilled pen $426 $341
c Glulisine U-100 vial; $306 $245U-100 prefilled pen $394 $315
c Inhaled insulin Inhalation cartridges $725 ($544, $911) N/A†
Short-acting analogs c Human Regular U-100 vial $165 ($165, $178) $135 ($135, $145)
Intermediate-acting analogs c Human NPH U-100 vial; $165 ($165, $178) $135 ($135, $145)U-100 prefilled pen $377 $305
Concentrated HumanRegular insulin
c U-500 HumanRegular insulin
U-500 vial; $178 $143U-500 prefilled pen $230 $184
Basal analogs c Glargine U-100 vial; U-100 prefilled pen;U-300 prefilled pen
$298 $239 ($239, $241)
c Glargine biosimilar U-100 prefilled pen $253 $203c Detemir U-100 vial; U-100 prefilled pen $323 $259c Degludec U-100 prefilled pen; U-200 prefilled pen $355 $285
Premixed insulin products c NPH/Regular 70/30 U-100 vial; $165 ($165, $178) $134 ($134, $146)U-100 prefilled pen $377 $305
c Lispro 50/50 U-100 vial; $342 $278U-100 prefilled pen $424 $339
c Lispro 75/25 U-100 vial; $342 $273U-100 prefilled pen $424 $340
c Aspart 70/30 U-100 vial; $343 $275U-100 prefilled pen $426 $341
Premixed insulin/GLP-1receptor agonist products
c Degludec/Liraglutide 100/3.6 prefilled pen $763 N/A†c Glargine/Lixisenatide 100/33 prefilled pen $508 $404
*AWP or NADAC calculated as in Table 8.3; median listed alone when only one product and/or price. †Not applicable; data not available.
S82 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 41, Supplement 1, January 2018

efficacy, hypoglycemia risk, weight, andother patient and drug-specific factors(Table 8.1) (57).
Bolus Insulin
Many individuals with type 2 diabetesmay require mealtime bolus insulin dos-ing in addition to basal insulin. Rapid-acting analogs are preferred due to theirprompt onset of action after dosing. InSeptember 2017, the FDA approved a newfaster-acting formulation of insulin aspart.The recommended starting dose of meal-time insulin is 4 units, 0.1 units/kg, or 10%of the basal dose. If A1C is,8% (64 mmol/mol) when starting mealtime bolus in-sulin, consideration should be given todecreasing the basal insulin dose.
Premixed Insulin
Premixed insulin products contain both abasal and prandial component, allowingcoverage of both basal and prandial needswith a single injection. NPH/Regular 70/30insulin, for example, is composed of 70%NPH insulin and30% regular insulin. Theuseof premixed insulin products has its advan-tages and disadvantages, as discussed be-low in COMBINATION INJECTABLE THERAPY.
Concentrated Insulin Products
Several concentrated insulin preparationsare currently available. U-500 regular insu-lin, by definition, is five times as concen-trated as U-100 regular insulin and has adelayed onset and longer duration of ac-tion than U-100 regular, possessing bothprandial and basal properties. U-300 glar-gine and U-200 degludec are three andtwo times as concentrated as their U-100formulationsandallowhigherdosesofbasalinsulin administration per volume used.U-300 glargine has a longer duration of ac-tion than U-100 glargine. The FDA has alsoapproved a concentrated formulation ofrapid-acting insulin lispro, U-200 (200units/mL). These concentrated preparationsmay be more comfortable for the patientand may improve adherence for patientswith insulin resistance who require largedoses of insulin.While U-500 regular insulinis available in both prefilled pens and vials (adedicated syringe was FDA approved in July2016), other concentrated insulins are avail-able only in prefilled pens to minimize therisk of dosing errors.
Inhaled Insulin
Inhaled insulin is available for prandial usewithamore limiteddosing range. It is contra-indicated in patients with chronic lung dis-ease such as asthma and chronic obstructive
pulmonarydisease and is not recommendedinpatientswho smokeorwho recently stop-ped smoking. It requires spirometry (FEV1)testing to identifypotential lungdisease inallpatients prior to and after starting therapy.
Combination Injectable TherapyIf basal insulin has been titrated to an ac-ceptable fasting blood glucose level (or ifthedose is.0.5 units/kg/day) andA1C re-mains above target, consider advancingto combination injectable therapy (Fig.8.2). When initiating combination inject-able therapy, metformin therapy shouldbe maintained while other oral agentsmay be discontinued on an individual ba-sis to avoid unnecessarily complex orcostly regimens (i.e., adding a fourth anti-hyperglycemic agent). In general, GLP-1receptor agonists should not be discon-tinued with the initiation of basal insulin.Sulfonylureas, DPP-4 inhibitors, and GLP-1 receptor agonists are typically stoppedonce more complex insulin regimens be-yond basal are used. In patients with sub-optimal blood glucose control, especiallythose requiring large insulin doses, adjunc-tive use of a thiazolidinedione or SGLT2inhibitor may help to improve controland reduce the amount of insulin needed,though potential side effects should beconsidered. Once an insulin regimen is ini-tiated, dose titration is important with ad-justments made in both mealtime andbasal insulins based on the blood glucoselevels and an understanding of the phar-macodynamic profile of each formulation(pattern control).
Studies have demonstrated the non-inferiority of basal insulin plus a singleinjectionof rapid-acting insulin at the larg-est meal relative to basal insulin plus aGLP-1 receptor agonist relative to twodaily injections of premixed insulins(Fig. 8.2). Basal insulin plus GLP-1 recep-tor agonists are associated with less hy-poglycemia and with weight loss insteadof weight gain but may be less tolerableand have a greater cost (58,59). In No-vember 2016, the FDA approved two dif-ferent once-daily fixed-dual combinationproducts containing basal insulin plus aGLP-1 receptor agonist: insulin glargineplus lixisenatide and insulin degludecplus liraglutide. Other options for treat-ment intensification include adding a sin-gle injection of rapid-acting insulin analog(lispro, aspart, or glulisine) before thelargest meal or stopping the basal insulinand initiating a premixed (or biphasic)
insulin (NPH/Regular 70/30, 70/30 aspartmix, 75/25 or 50/50 lispro mix) twicedaily, usually before breakfast and beforedinner. Each approach has its advan-tages and disadvantages. For example,providers may wish to consider regimenflexibility when devising a plan for the ini-tiation and adjustment of insulin therapyin people with type 2 diabetes, with rapid-acting insulin offering greater flexibility interms of meal planning than premixed in-sulin. If one regimen is not effective (i.e.,basal insulin plus GLP-1 receptor agonist),consider switching to another regimen toachieve A1C targets (i.e., basal insulin plussingle injectionof rapid-acting insulinorpre-mixed insulin twice daily) (60,61). Regularhuman insulin and human NPH/Regularpremixed formulations (70/30) are lesscostly alternatives to rapid-acting insulinanalogs and premixed insulin analogs,respectively, but their pharmacody-namicprofilesmaymake them lessoptimal.
Fig. 8.2 outlines these options, as wellas recommendations for further intensifi-cation, if needed, to achieve glycemicgoals. If a patient is still above the A1Ctarget on premixed insulin twice daily,consider switching to premixed analog in-sulin three times daily (70/30 aspart mix,75/25 or 50/50 lispro mix). In general,three times daily premixed analog insu-lins have been found to be noninferiorto basal-bolus regimens with similar ratesof hypoglycemia (62). If a patient is stillabove the A1C target on basal insulinplus single injection of rapid-acting insulinbefore the largest meal, advance to abasal-bolus regimen with $2 injectionsof rapid-acting insulin before meals. Con-sider switching patients from one regimento another (i.e., premixed analog insulinthree times daily to basal-bolus regimenor vice-versa) if A1C targets are not beingmet and/or depending on other patientconsiderations (60,61).Metformin shouldbe continued in patients on combinationinjectable insulin therapy, if not contra-indicated and if tolerated, for further gly-cemic benefits.
References1. Peters AL, Laffel L, Eds. American DiabetesAssociation/JDRF Type 1 Diabetes Sourcebook.Alexandria, VA, American Diabetes Association,20132. Chiang JL, Kirkman MS, Laffel LMB, Peters AL;Type 1 Diabetes Sourcebook Authors. Type 1 di-abetes through the life span: a position statementof the American Diabetes Association. DiabetesCare 2014;37:2034–2054
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S83

3. Wolpert HA, Atakov-Castillo A, Smith SA, SteilGM. Dietary fat acutely increases glucose con-centrations and insulin requirements in pa-tients with type 1 diabetes: implications forcarbohydrate-based bolus dose calculationand intensive diabetes management. DiabetesCare 2013;36:810–8164. Bell KJ, Toschi E, Steil GM, Wolpert HA. Opti-mized mealtime insulin dosing for fat and proteinin type 1 diabetes: application of a model-basedapproach to derive insulin doses for open-loopdiabetes management. Diabetes Care 2016;39:1631–16345. Bell KJ, Smart CE, Steil GM, Brand-Miller JC,King B, Wolpert HA. Impact of fat, protein, andglycemic index on postprandial glucose control intype 1 diabetes: implications for intensive diabetesmanagement in the continuous glucosemonitoringera. Diabetes Care 2015;38:1008–10156. Yeh H-C, Brown TT,Maruthur N, et al. Compar-ative effectiveness and safety of methods of in-sulin delivery and glucosemonitoring for diabetesmellitus: a systematic review and meta-analysis.Ann Intern Med 2012;157:336–3477. Bergenstal RM, Klonoff DC, Garg SK, et al.;ASPIRE In-Home Study Group. Threshold-basedinsulin-pump interruption for reduction of hypo-glycemia. N Engl J Med 2013;369:224–2328. Bergenstal RM, Garg S, Weinzimer SA, et al.Safety of a hybrid closed-loop insulin delivery sys-tem in patients with type 1 diabetes. JAMA 2016;316:1407–14089. Garg SK, Weinzimer SA, TamborlaneWV, et al.Glucose outcomes with the in-home use of a hy-brid closed-loop insulin delivery system in adoles-cents and adults with type 1 diabetes. DiabetesTechnol Ther 2017;19:155–16310. Wood JR, Miller KM, Maahs DM, et al.; T1DExchange Clinic Network. Most youth with type 1diabetes in the T1D Exchange Clinic Registry do notmeet American Diabetes Association or InternationalSociety for Pediatric and Adolescent Diabetes clinicalguidelines. Diabetes Care 2013;36:2035–203711. Kmietowicz Z. Insulin pumps improve controland reduce complications in children with type 1diabetes. BMJ 2013;347:f515412. Phillip M, Battelino T, Atlas E, et al. Nocturnalglucose control with an artificial pancreas at a di-abetes camp. N Engl J Med 2013;368:824–83313. Nathan DM, Genuth S, Lachin J, et al.; Diabe-tes Control and Complications Trial ResearchGroup. The effect of intensive treatment of dia-betes on the development and progression oflong-term complications in insulin-dependentdiabetes mellitus. N Engl J Med 1993;329:977–98614. Nathan DM, Cleary PA, Backlund J-YC, et al.;Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Com-plications (DCCT/EDIC) Study Research Group. In-tensive diabetes treatment and cardiovasculardisease in patients with type 1 diabetes. N Engl JMed 2005;353:2643–265315. Diabetes Control and Complications Trial(DCCT)/Epidemiology of Diabetes Interventionsand Complications (EDIC) Study Research Group.Mortality in type 1 diabetes in the DCCT/EDICversus the general population. Diabetes Care2016;39:1378–138316. Tricco AC, Ashoor HM, Antony J, et al. Safety,effectiveness, and cost effectiveness of long act-ing versus intermediate acting insulin for patients
with type 1 diabetes: systematic review and net-work meta-analysis. BMJ 2014;349:g545917. Bartley PC, BogoevM, Larsen J, Philotheou A.Long-term efficacy and safety of insulin detemircompared to Neutral Protamine Hagedorn insulinin patients with type 1 diabetes using a treat-to-target basal-bolus regimen with insulin aspart atmeals: a 2-year, randomized, controlled trial. Dia-bet Med 2008;25:442–44918. DeWitt DE, Hirsch IB. Outpatient insulin ther-apy in type 1 and type 2 diabetes mellitus: scien-tific review. JAMA 2003;289:2254–226419. LaneW, Bailey TS, Gerety G, et al.; SWITCH 1.Effect of insulin degludec vs insulin glargine U100on hypoglycemia in patients with type 1 diabetes:the SWITCH 1 Randomized Clinical Trial. JAMA2017;318:33–4420. Home PD, Bergenstal RM, Bolli GB, et al. Newinsulin glargine 300 units/mL versus glargine100 units/mL in people with type 1 diabetes: arandomized, phase 3a, open-label clinical trial(EDITION 4). Diabetes Care 2015;38:2217–2225
21. Bode BW, McGill JB, Lorber DL, Gross JL,Chang PC, Bregman DB; Affinity 1 Study Group.Inhaled technosphere insulin compared with in-jected prandial insulin in type 1 diabetes: a ran-domized 24-week trial. Diabetes Care 2015;38:2266–227322. Vella S, Buetow L, Royle P, Livingstone S,Colhoun HM, Petrie JR. The use of metformin intype 1 diabetes: a systematic review of efficacy.Diabetologia 2010;53:809–82023. Libman IM,Miller KM,DiMeglio LA, et al.; T1DExchange Clinic Network Metformin RCT StudyGroup. Effect of metformin added to insulin onglycemic control among overweight/obese ado-lescents with type 1 diabetes: a randomized clin-ical trial. JAMA 2015;314:2241–225024. Petrie JR, Chaturvedi N, Ford I, et al.;REMOVAL Study Group. Cardiovascular and met-abolic effects ofmetformin in patientswith type 1diabetes (REMOVAL): a double-blind, rando-mised, placebo-controlled trial. Lancet DiabetesEndocrinol 2017;5:597–60925. Dejgaard TF, Frandsen CS, Hansen TS, et al.Efficacy and safety of liraglutide for overweightadult patients with type 1 diabetes and insufficientglycaemic control (Lira-1): a randomised, double-blind, placebo-controlled trial. Lancet DiabetesEndocrinol 2016;4:221–23226. Guo H, Fang C, Huang Y, Pei Y, Chen L, Hu J.The efficacy and safety of DPP4 inhibitors in pa-tients with type 1 diabetes: a systematic reviewand meta-analysis. Diabetes Res Clin Pract 2016;121:184–19127. Yang Y, Chen S, Pan H, et al. Safety and effi-ciency of SGLT2 inhibitor combiningwith insulin insubjects with diabetes: systematic review andmeta-analysis of randomized controlled trials.Medicine (Baltimore) 2017;96:e694428. U.S. Food and Drug Administration. SGLT2inhibitors: drug safety communication - labels toinclude warnings about too much acid in the bloodand serious urinary tract infections [Internet], 2015.Available from http://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/ucm475553.htm. Accessed 3October 201629. Robertson RP, Davis C, Larsen J, Stratta R,Sutherland DER; American Diabetes Association.Pancreas and islet transplantation in type 1 dia-betes. Diabetes Care 2006;29:935
30. Palmer SC,MavridisD,Nicolucci A, et al. Com-parison of clinical outcomes and adverse eventsassociated with glucose-lowering drugs in patientswith type 2 diabetes: a meta-analysis. JAMA 2016;316:313–32431. Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of hyperglycemia in type 2 diabe-tes, 2015: a patient-centered approach: updateto a position statement of the American Diabe-tes Association and the European Associationfor the Study of Diabetes. Diabetes Care 2015;38:140–14932. Holman RR, Paul SK, Bethel MA, MatthewsDR, Neil HAW. 10-year follow-up of intensive glu-cose control in type2diabetes.N Engl JMed2008;359:1577–158933. Maruthur NM, Tseng E, Hutfless S, et al. Di-abetesmedications asmonotherapy ormetformin-based combination therapy for type 2 diabetes: asystematic review and meta-analysis. Ann InternMed 2016;164:740–75134. U.S. Food and Drug Administration. Metformin-containing drugs: drug safety communication -revised warnings for certain patients withreduced kidney function [Internet], 2016. Availablefrom http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm494829.htm?source5govdelivery&utm_medium5email&utm_source5govdelivery.Accessed 3 October 201635. Aroda VR, Edelstein SL, Goldberg RB, et al.;Diabetes Prevention Program Research Group.Long-term metformin use and vitamin B12 defi-ciency in the Diabetes Prevention Program Out-comes Study. J Clin Endocrinol Metab 2016;101:1754–176136. Bennett WL, Maruthur NM, Singh S, et al.Comparative effectiveness and safety of medica-tions for type 2 diabetes: an update including newdrugs and 2-drug combinations. Ann Intern Med2011;154:602–61337. Vijan S, Sussman JB, Yudkin JS, Hayward RA.Effect of patients’ risks and preferences on healthgains with plasma glucose level lowering in type 2diabetes mellitus. JAMA Intern Med 2014;174:1227–123438. Institute for Clinical and Economic Review.Controversies in the management of patients withtype 2 diabetes [Internet], 2014. Available fromhttps://icer-review.org/wp-content/uploads/2015/03/CEPAC-T2D-Final-Report-December-22.pdf. Accessed 2 November 201739. Truven Health Analytics. Red Book: A Com-prehensive, Consistent Drug Pricing Resource[Internet], 2016. Available from: http://www.micromedexsolutions.com/micromedex2/librarian.Accessed 18 July 201740. Centers for Medicare & Medicaid Services.Pharmacy pricing: national average drug acquisi-tion cost [Internet], 2017. Available from https://www.medicaid.gov/medicaid/prescription-drugs/pharmacy-pricing/index.html. Accessed 19 July201741. Nathan DM, Buse JB, Kahn SE, et al.; GRADEStudy Research Group. Rationale and design ofthe Glycemia Reduction Approaches in Diabetes:A Comparative Effectiveness Study (GRADE). Di-abetes Care 2013;36:2254–226142. Blonde L, Merilainen M, Karwe V, Raskin P;TITRATE Study Group. Patient-directed titra-tion for achieving glycaemic goals using a once-daily basal insulin analogue: an assessment of
S84 Pharmacologic Approaches to Glycemic Treatment Diabetes Care Volume 41, Supplement 1, January 2018

two different fasting plasma glucose targets - theTITRATE study. Diabetes Obes Metab 2009;11:623–63143. Singh SR, Ahmad F, Lal A, Yu C, Bai Z, BennettH. Efficacy and safety of insulin analogues for themanagementof diabetesmellitus: ameta-analysis.CMAJ 2009;180:385–39744. Horvath K, Jeitler K, Berghold A, et al. Long-acting insulin analogues versus NPH insulin (hu-man isophane insulin) for type2diabetesmellitus.Cochrane Database Syst Rev 2007;2:CD00561345. MonamiM,Marchionni N,Mannucci E. Long-acting insulin analogues versus NPH human insu-lin in type 2 diabetes: a meta-analysis. DiabetesRes Clin Pract 2008;81:184–18946. Owens DR, Traylor L, Mullins P, Landgraf W.Patient-level meta-analysis of efficacy and hypo-glycaemia in peoplewith type 2 diabetes initiatinginsulin glargine 100U/mL or neutral protamineHagedorn insulin analysed according to concomi-tant oral antidiabetes therapy. Diabetes Res ClinPract 2017;124(Suppl. C):57–6547. RiddleMC,Rosenstock J,Gerich J; InsulinGlar-gine 4002 Study Investigators. The treat-to-targettrial: randomized addition of glargine or humanNPH insulin to oral therapy of type 2 diabeticpatients. Diabetes Care 2003;26:3080–308648. Hermansen K, Davies M, Derezinski T,Martinez Ravn G, Clauson P, Home P. A 26-week,randomized, parallel, treat-to-target trial compar-ing insulin detemir with NPH insulin as add-ontherapy to oral glucose-lowering drugs in insulin-naive people with type 2 diabetes. Diabetes Care2006;29:1269–127449. Bolli GB, Riddle MC, Bergenstal RM, et al.;EDITION 3 Study Investigators. New insulin glar-gine 300 U/ml compared with glargine 100 U/mlin insulin-naıve people with type 2 diabetes onoral glucose-lowering drugs: a randomized con-trolled trial (EDITION 3). Diabetes Obes Metab2015;17:386–39450. Terauchi Y, Koyama M, Cheng X, et al. Newinsulin glargine 300U/ml versus glargine 100U/ml
in Japanese people with type 2 diabetes usingbasal insulin and oral antihyperglycaemic drugs:glucose control and hypoglycaemia in a random-ized controlled trial (EDITION JP 2). Diabetes ObesMetab 2016;18:366–37451. Yki-Jarvinen H, Bergenstal RM, Bolli GB, et al.Glycaemic control and hypoglycaemia with newinsulin glargine 300 U/ml versus insulin glargine100 U/ml in people with type 2 diabetes usingbasal insulin and oral antihyperglycaemic drugs:the EDITION2 randomized 12-month trial including6-month extension. Diabetes Obes Metab 2015;17:1142–114952. Marso SP, McGuire DK, Zinman B, et al. Effi-cacy and safety of degludec versus glargine intype 2 diabetes. N Engl J Med 2017;377:723–73253. RodbardHW,CariouB, ZinmanB, et al.; BEGINOnce Long trial investigators. Comparison of insu-lin degludec with insulin glargine in insulin-naivesubjects with Type 2 diabetes: a 2-year random-ized, treat-to-target trial. Diabet Med 2013;30:1298–130454. WyshamC,BhargavaA, Chaykin L, et al. Effectof insulin degludec vs insulin glargine U100 onhypoglycemia in patients with type 2 diabetes:the SWITCH 2 Randomized Clinical Trial. JAMA2017;318:45–5655. Zinman B, Philis-Tsimikas A, Cariou B, et al.;NN1250-3579 (BEGIN Once Long) Trial Investiga-tors. Insulin degludec versus insulin glargine ininsulin-naive patients with type 2 diabetes: a1-year, randomized, treat-to-target trial (BEGINOnce Long). Diabetes Care 2012;35:2464–247156. Lipska KJ, Hirsch IB, RiddleMC.Human insulinfor type 2 diabetes: an effective, less-expensiveoption. JAMA 2017;318:23–2457. Hua X, Carvalho N, TewM, Huang ES, HermanWH, Clarke P. Expenditures and prices of antihy-perglycemic medications in the United States:2002-2013. JAMA 2016;315:1400–140258. DiamantM, NauckMA, Shaginian R, et al.; 4BStudyGroup. Glucagon-like peptide 1 receptor ag-onist or bolus insulin with optimized basal insulin
in type 2 diabetes. Diabetes Care 2014;37:2763–277359. Eng C, Kramer CK, Zinman B, Retnakaran R.Glucagon-like peptide-1 receptor agonist andbasal insulin combination treatment for themanagement of type 2 diabetes: a systematicreview and meta-analysis. Lancet 2014;384:2228–223460. Dieuzeide G, Chuang L-M, Almaghamsi A,Zilov A, Chen J-W, Lavalle-Gonzalez FJ. Safetyand effectiveness of biphasic insulin aspart 30 inpeople with type 2 diabetes switching from basal-bolus insulin regimens in the A1chieve study. PrimCare Diabetes 2014;8:111–11761. Mathieu C, Storms F, Tits J, VenemanTF, ColinIM. Switching from premixed insulin to basal-bolus insulin glargine plus rapid-acting insulin:the ATLANTIC study. Acta Clin Belg 2013;68:28–3362. Giugliano D, Chiodini P, Maiorino MI,Bellastella G, Esposito K. Intensification of insulintherapy with basal-bolus or premixed insulin reg-imens in type 2 diabetes: a systematic review andmeta-analysis of randomized controlled trials. En-docrine 2016;51:417–42863. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetickidney disease: a report from an ADA ConsensusConference. Diabetes Care 2014;37:2864–288364. Neumiller JJ, Alicic RZ, Tuttle KR. Therapeuticconsiderations for antihyperglycemic agents in di-abetic kidney disease. J Am Soc Nephrol 2017;28:2263–227465. U.S. Food and Drug Administration. Cycloset[bromocriptine] prescribing information [In-ternet], 2017. [Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020866s006s007lbl.pdf. Accessed 22 September201766. U.S. Food and Drug Administration. Welchol[Colesevelam] prescribing information [Internet],2014. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/022362s007lbl.pdf. Accessed 22 September 2017
care.diabetesjournals.org Pharmacologic Approaches to Glycemic Treatment S85





























