-
7/29/2019 88862534 Brain Herniation
1/64
Cerebral Herniation Syndromes
Imaging findings and clinical correlation
-
7/29/2019 88862534 Brain Herniation
2/64
Definition of Cerebral
Herniation:
Herniation of brain tissue from one
compartment (separated by calvarial
and /or dural boudaries) to another
-
7/29/2019 88862534 Brain Herniation
3/64
Compartments
Supratentorial
Right
Left
Infratentorial
Spinal
-
7/29/2019 88862534 Brain Herniation
4/64
Intracranialcompartments
Brain tissue in each compartment is
contained by (relative) intracranial
boundaries:
Falx cerebri
Tentorium cerebelli
Skull base (foramen magnum)
-
7/29/2019 88862534 Brain Herniation
5/64
Intracranialcompartments
Neurocranium
Falx cerebri
TentoriumCerebelli
Skull Base
(Foramen Magnum)
-
7/29/2019 88862534 Brain Herniation
6/64
IntracranialCompartments
For each compartment there are laws of
Intracranial volume en pressure
Each compartment abides these laws as
good as possible
-
7/29/2019 88862534 Brain Herniation
7/64
Intracranialvolume
Intracranial volume is constant and describedby Monro-Kelly
Doctrine:
Vol. Intracranial = V. Brain + V. CSF + V. Blood
Intracranial components are (almost) non-
compressible Increase in one volume leads to decrease
inanother
-
7/29/2019 88862534 Brain Herniation
8/64
IntracranialPressure
Normal intracranial pressure: 5-15 mmHg
http://www.trauma.org/archive/neuro/icp.html
-
7/29/2019 88862534 Brain Herniation
9/64
IntracranialPressure
Pressure components:
Cerebral Perfusion Pressure (CPP)
Mean Arterial Pressure (MAP)
Intracranial Pressure (ICP)
CPP = MAP - ICP
To maintain CPP: If ICP increases, MAP must
increase (autoregulation)
-
7/29/2019 88862534 Brain Herniation
10/64
IntracranialPressure
When MAP cannot increase:
Increased ICP decreases CPP
Decreased CPP leads to tissue ischemia Tissue ischemia leads to
edema
Edema leads to increased ICP
Further increased ICP leads to:
Tissue death
-
7/29/2019 88862534 Brain Herniation
11/64
When compartmental
volume increases and
pressure increases, braintissue moves from one
compartment to another
-
7/29/2019 88862534 Brain Herniation
12/64
Causesofvolumeincrease
Tumour
Blood Subdural
Epidural
Parenchymous
Ischemia
Infection
-
7/29/2019 88862534 Brain Herniation
13/64
Typesofherniation:
Subfalcine
Transtentorial Descending
Ascending
Tonsillar / Foramen Magnum
Transcranial / Fungus Cerebri
Miscellaneous Transalar/ Transsphenoidal
Middle ear encephalocele
-
7/29/2019 88862534 Brain Herniation
14/64
SubfalcineHerniation
Mass effect in cerebral hemisphere
forces brain tissue under the falx to
opposite side
-
7/29/2019 88862534 Brain Herniation
15/64
Subfalcine Herniation:Structures involved
Falx
Cingulate Gyrus
Pericallosal Artery Anterior Cerebral
Artery
Corpus Callosum
S f
-
7/29/2019 88862534 Brain Herniation
16/64
Subfalcine Herniation:Imaging findings
Ipsilateral cingulate gyrus is pushed down andunder midline
falx
Contralateral cingulate gyrus is compressed
Depression of ipsilateral corpus callosum andelevation /
compression of contralateral corpuscallosum
Acquired intracranail Herniation: MR Findings, Laine et al. AJR
1995;165: 967-973
-
7/29/2019 88862534 Brain Herniation
17/64
SubfalcineHerniation
Falx meningioma with extensive surrounding edema
-
7/29/2019 88862534 Brain Herniation
18/64
SubfalcineHerniation
Displacedpericallosalartery
Contralateralcingulate gyruscompressed
Compression
of frontal hornsof lateralventricles
Ipsilateralcingulate gyrusherniates underfalx
Depression /displacement ofcorpuscallosum
Subfalcine Herniation:
-
7/29/2019 88862534 Brain Herniation
19/64
Subfalcine Herniation:
Complications and Clinical Signs
Compression of the parafalcine cortex may lead tocontralateral
leg paresis
Anterior cerebral artery infarction may lead to
ipsilateralfrontal infarcts
Increased ICP leads to somnolence
http://missinglink.ucsf.edu/lm/ids_104_cerebrovasc_neuropath/Case4/CerebralArteryDistribution.htm
S bf l i H i ti
-
7/29/2019 88862534 Brain Herniation
20/64
Subfalcine Herniation:Complications
CT Angiogram of
patient with subdural
hematoma on the right
shows displacement of
anterior cerebral artery
without evidence of
infarction
S bf l i H i ti
-
7/29/2019 88862534 Brain Herniation
21/64
Subfalcine Herniation:Complications
Right sided mass
effect was treated by
craniotomy.
Hypodensity in theright frontal lobe
exemplifies anterior
cerebral artery
infarct afterprolonged subfalcine
herniation
-
7/29/2019 88862534 Brain Herniation
22/64
TranstentorialHerniation
Descending
Ascending
-
7/29/2019 88862534 Brain Herniation
23/64
Descending
Transtentorial Herniation
Supratentorial mass effect forces
cerebral structures downward through
the opening (incisura) of thetentorium
-
7/29/2019 88862534 Brain Herniation
24/64
Descending Transtentorial Herniation:Structures Involved
Tentorium
Uncus
Parahippocampal gyrus
Perimesencephalic cistern
Mesencephalon
Posterior cerebral artery(-branches)
Anterior Choroidal Artery
Oculomotor Nerve (NIII)
-
7/29/2019 88862534 Brain Herniation
25/64
Descending Transtentorial Herniation:Imaging Findings
Asymmetry of ambient cistern (ipsilateral widening
/contralateral effacement)
Widening of contralateral temporal horn of lateral ventricle
Herniated brain is forced medially and inferiorly
beneathtentorium, into perimesencephalic cistern
Compression of ipsilateral cerebral peduncle by uncus
Compression of contralateral cerebral peduncle against
tentorialedge (Kernohans Notch)
Acquired intracranail Herniation: MR Findings, Laine et al. AJR
1995;165: 967-973
-
7/29/2019 88862534 Brain Herniation
26/64
DescendingTranstentorialHerniation
Chronic (hypodens) rightsided subdural hematoma with
unilateral descending transtentorial herniation
-
7/29/2019 88862534 Brain Herniation
27/64
Descendingtranstentorialherniation
Shift of midline structures
Blood
Compression of lateralventricles
Widened temporal horn
Medial, downwarddisplacement of uncusover right tentorial
edge
-
7/29/2019 88862534 Brain Herniation
28/64
Descendingtranstentorialherniation
Herniated uncus in
perimesencephalic
cistern
Ipsilateral midbrain
compression
Asymmetric ambientcistern
-
7/29/2019 88862534 Brain Herniation
29/64
Descendingtranstentorialherniation
Subdural collection on the left with massive
descendingtranstentorial herniation
Descending transtentorial herniation
-
7/29/2019 88862534 Brain Herniation
30/64
Descending transtentorial herniationClinical Findings
Oculomotor (NIII) nerve palsy by compression of thirdcranial
nerve against tentorial edge:
Exotropic, hypotropic eye position
(down and outward)
Ipsilateral ptosis
Ipsilateral fixed, dilated pupil
http://www.bartleby.comhttp://scalpelorsword.blogspot.com/2007/01/droopy-eye.html
Descending transtentorial herniation
-
7/29/2019 88862534 Brain Herniation
31/64
Descending transtentorial herniationClinical Findings
Classic localizing sign: Damage tothe pyramidal tracts
causes
contralateral hemiparesis
Kernohans (Notch) phenomenon:compression of contralateral
cerebral peduncle against tentorial
edge may result in ipsilateral
hemiparesis: False localizing
sign
Kernohan, J.W., & Woltman, H.W. (1929). Incisura of the crus
due to contralateral brain tumor. Archives of Neurology and
Psychiatry,
21, 274-287
Descending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
32/64
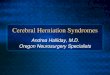
Descending Transtentorial HerniationComplications
Focal infarction of uncus / parahippocampal gyrus
Infarction by compression of posterior cerebral
artery (-branches) against the tentorial edge
Infarction by direct compression of the anterior
choroidal artery by the uncus
Brainstem (Duret) hemorrhage
Complications:
-
7/29/2019 88862534 Brain Herniation
33/64
Complications:Vascular structures at risk
MRI images of the vascular structures around the uncus(posterior
cerebral artery and anterior choroidal artery). The
latteroriginates from the anterior cerebral artery and traverses
along
the uncus dorsally (arrows)
Wiesmann et al. Identification and Anatomic Description of the
Anterior Choroidal Artery by Use of 3D-TOF Source and 3D-CISS MR
Imaging AJNR Am J Neuroradiol 2001; 22: 305-310
Complications:
-
7/29/2019 88862534 Brain Herniation
34/64
Complications:Vascular structures at risk
Anterior choroidal arterycompression may lead toinfarcts in the
posteriorlimb of the internalcapsule and the lateralaspect of the
thalamus
Posterior cerebral arterycompression leads to
cerebellar and occipitallobe infarction but mayalso cause
thalamicinfarcts
Complications:
-
7/29/2019 88862534 Brain Herniation
35/64
Complications:Duret Hemorrhage
Prolonged andprogressive
transtentorial
herniation leads tostretching andeventually rupture
ofperforating arteries and
venules in thebrainstem causingpunctate hemorrhage
http://rad.usuhs.mil/rad/herniation/herniation.html#intro
Complications:
-
7/29/2019 88862534 Brain Herniation
36/64
Complications:Duret Hemorrhage
Extensive descending transtentorial herniation resulting
from
gunshot wound to the head; Initial CT scan shows Duret
hemorrhage
-
7/29/2019 88862534 Brain Herniation
37/64
Ascending
Transtentorial Herniation
Posterior fossa mass forcescerebellar structures upwards
through tentorial incisura
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
38/64
sce d g a ste to a e at oStructures involved
As in descending transtentorial herniation
Quadrigeminal plate cistern can be involved
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
39/64
gImaging findings
Upward displacement of upper cerebellar surface
Asymmetry/ effacement of ambient cisterns
Compression of mesencephalon
Asymmetry/ effacement of quadrigeminal plate cistern
Often bilateral changes
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
40/64
AscendingTranstentorialHerniation
Hemorrhagic arteriovenous malformation in the left
cerebellar
hemisphere with bilateral ascending transtentorial
herniation
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
41/64
AscendingTranstentorialHerniation
Effacement ofperimesencephaliccistern
Upper surface ofcerebellar hemisphereascends throughtentorial
incisura
Hemorrhagic lesion
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
42/64
AscendingTranstentorialHerniation
Effacement ofquadrigeminal plate
cisterns
Herniation of
cerebellum through
tentorial incisura
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
43/64
AscendingTranstentorialHerniation
Right sided hemorrhagic contusions with mass effect in theright
cerebellum causing unilateral ascending
transtentorial herniation
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
44/64
AscendingTranstentorialHerniation
Unilateral ascendingtranstentorialherniation on theright side
with
compression of theright cerebralpeduncle
Dilated temporalhorn of left ventricleindicating onset
ofhydrocephalus
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
45/64
special notes
Subtle imaging changes
Less frequent (-ly noted?) than descendingherniation
Often bilateral (no asymmetry)
Differing appearance of perimesencephaliccisterns with different
gantry angles in CT maycomplicate imaging findings
Ascending Transtentorial Herniation
-
7/29/2019 88862534 Brain Herniation
46/64
Clinical findings and Complications
Slowly evolving posterior fossa mass effect will oftenpresent
with signs of hydrocephalus: Headache, nausea,vomiting etc.
Compression of arteries (posterior cerebral, superiorcerebellar)
may lead to cerebral / occipital or cerebellarinfarction
Rapidly expanding lesions present with emergency
clinical findings due to compression of brainstem
nuclei:respiratory failure, coma and death (often coexistent
withforamen magnum herniation)
-
7/29/2019 88862534 Brain Herniation
47/64
Tonsillar / Foramen Magnum
Herniation
Posterior fossa mass effect forces
cerebellar tonsils downward through
the foramen magnum
Tonsillar Herniation
-
7/29/2019 88862534 Brain Herniation
48/64
Structures involved
Skull base / foramen magnum
Cerebellar tonsils
Posterior inferior cerebellar artery
Tonsillar Herniation
-
7/29/2019 88862534 Brain Herniation
49/64
TonsillarHerniation
Right sided tonsillar herniation
Tonsillar Herniation
-
7/29/2019 88862534 Brain Herniation
50/64
TonsillarHerniation
Anteriorly displaced
cervical myelum
Inferiorly displaced
right cerebellar tonsil
Tonsillar Herniation
-
7/29/2019 88862534 Brain Herniation
51/64
Special notes
(Subtle) extension of cerebellar tonsils in thespinal canal may
be seen in normal individuals orin Chiari I malformation
Extension of 5 mm or more below the foramenmagnum is considered
abnormal
Often coexisting with ascending transtentorial
herniation
Aboullez etal. Position of cerebellar tonsils in the normal
population and in patients with Chiari I malformation:
A quantative approach with MR Imaging. J Comp Assist Tomogr
1985;9: 1033-1036
Tonsillar Herniation
-
7/29/2019 88862534 Brain Herniation
52/64
TonsillarHerniation
Chiari I malformation with extension of the cerebellum in
theupper cervical spinal canal in a patient with a frontal mass
Tonsillar Herniation
-
7/29/2019 88862534 Brain Herniation
53/64
Clinical findings / Complications
Compression of brain stem nuclei causesrespiratory / cardiac
failure, coma, death
Compression of posterior inferior cerebellar artery
(PICA) may cause cerebellar infarcts
Patients with Chiari I malformation can be
symptom free but may experience dysesthesiawith cervical
flexion: Lhermitte phenomenon
-
7/29/2019 88862534 Brain Herniation
54/64
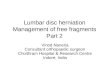
Transcranial Herniation
Fungus Cerebri
Intracranial mass effect forces
cerebral structures outward through
(iatrogenic) calvarial defect
TranscranialHerniation
-
7/29/2019 88862534 Brain Herniation
55/64
Decompressive right frontal craniotomy in two patients
withsevere right sided mass effect. Cerebral structures
herniatethrough calvarial defect. Note that there is no midline
shift.
Mass effect is orientated away from contralateral
hemisphere.
Transcranial HerniationC li ti
-
7/29/2019 88862534 Brain Herniation
56/64
Complications
Decompression usually improves patientsurvival by lowering
intracranial pressureand preventing / undoing
intracranialherniations
Herniation may lead to infarction ofherniated tissue
Exposed brain / dura is prone to infection
-
7/29/2019 88862534 Brain Herniation
57/64
Miscellaneous
Transalar / Sphenoidal Herniation
Middle Ear Encephaloceles
-
7/29/2019 88862534 Brain Herniation
58/64
Transalar / Sphenoidal
Herniation
Anterior cranial fossa mass effect forces
cerebral structures over the edge of the
sphenoid bone into the middle cranial fossa
Transalar / SphenoidalHerniation
-
7/29/2019 88862534 Brain Herniation
59/64
Herniation
Coexisting with other forms of herniation
Rarely recognized; Imaging may show
displacement of middle cerebral artery
No specific clinical signs.
Complications include (rarely) middle cerebralartery infarct
-
7/29/2019 88862534 Brain Herniation
60/64
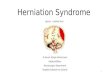
Middle ear (Skull base)
encephalocele
Cerebral structures bulge through
(acquired) skull base defect
NO PRESSURE COMPONENTS
MiddleEarEncephalocele
-
7/29/2019 88862534 Brain Herniation
61/64
Left temporal bone defect with protruding cerebraltissue
Papanikolaou et al. Skull Base. 2007 September; 17(5):
311-316
MiddleEarEncephalocele
-
7/29/2019 88862534 Brain Herniation
62/64
Cerebral tissue
protruding in left
temporal bone
MiddleEarEncephalocele
-
7/29/2019 88862534 Brain Herniation
63/64
Focal osseous defectin left tegmen
Protrusion of cerebralstructures in
epitympanic spacesurrounding the
ossicles
Skullbaseencephalocele
-
7/29/2019 88862534 Brain Herniation
64/64
May occur anywhere along the skull base
Osseous defects may be iatrogenic or
congenital
No specific clinical findings