Embed Size (px)
Citation preview
British Joumal ofPIastic Surgery (1991). 44,142-146 fjCJ 1991 The Trustees of British Association of Plastic Surgeons
A bilayer “artificial skin” capable of sustained release of an antibiotic
K. Matsuda, S. Suzuki, N. Isshiki, K. Yoshioka, T. Okada, S.-H. Hyon and Y. Ikada
Department of Plastic Surgery, Faculty of Medicine, and Research Center for Medical Polymers and Biomaterials, Kyoto University, Kyoto, Japan
SUMMARY. The most frequent complication of the bilayer “artikial skin”, composed of a silicone sheet and collagen sponge described in a previous paper, was infection beneath it. This paper describes a new type of %rtificial skin” in which microspheres containing antibiotics were installed beneath the silicone sheet, allowing a continuous release of antibiotics.
A bilayer “artificial skin”, stage 1 membrane, which is composed of an upper silicone sheet and a lower sponge sheet of a collagen and glycosaminoglycan (GAG), was first developed by Yannas, Burke and their colleagues (Dagalakis et al., 1980; Yannas and Burke, 1980; Yannas et al., 1980, 1981, 1982; Burke et al., 1981; Burke, 1983; Yannas, 1984, 1988). Modifying their technique, we produced a bilayer “artificial skin” similar to stage 1 membrane (Suzuki et al., 199Oa). The “artificial skin” was used in experimental animals and clinically, both with success (Suzuki et al., 1990a, b).
The “artificial skin” had the following advantages : (1) The lower sponge sheet of collagen has an affinity to tissue and little antigenicity. (2) It is unnecessary to peel it off at the time of secondary skin grafting because the original network of collagen is biode- graded with infiltration of fibroblasts and capillaries, producing a synthesised connective tissue matrix. (3) Since the lower sheet is spontaneously converted into new connective tissue, the secondary skin graft takes
easily and postoperative contracture is not significant even though the graft is thin. It would therefore be possible to take the skin repeatedly from the same donor site at intervals. (4) The water vapour permea- bility of the upper silicone sheet is comparable to that of normal skin.
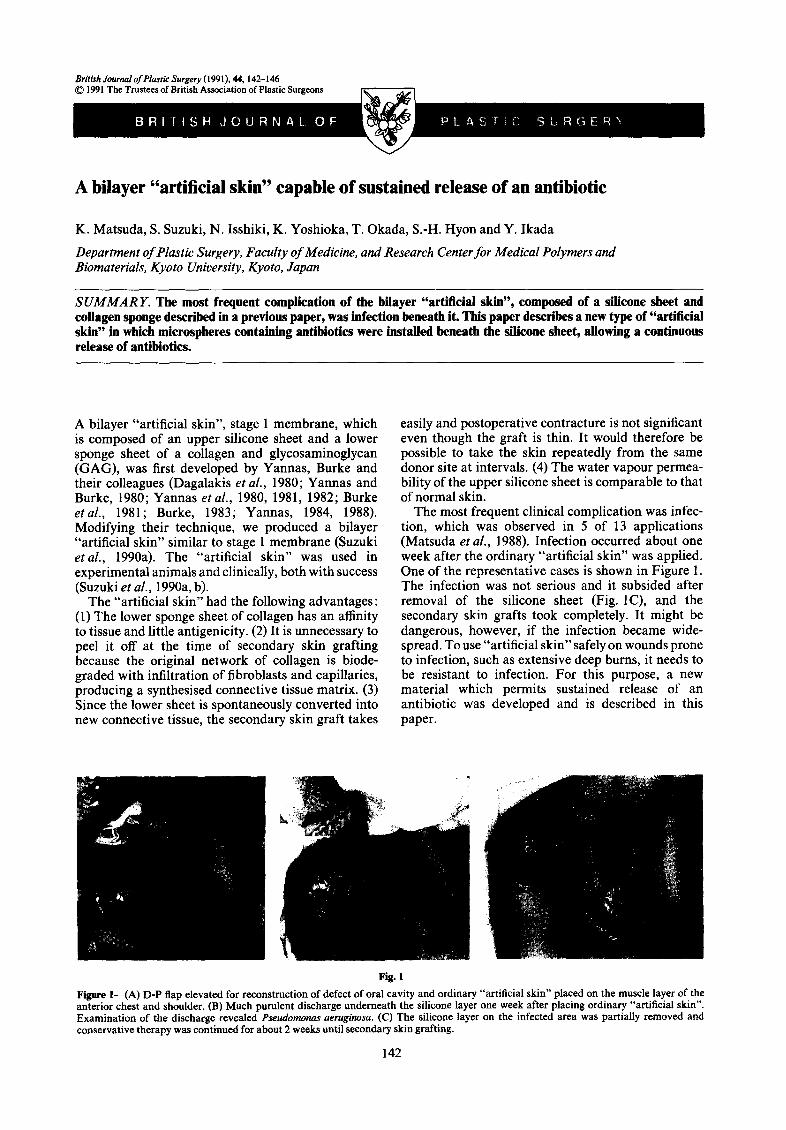
The most frequent clinical complication was infec- tion, which was observed in 5 of 13 applications (Matsuda et al., 1988). Infection occurred about one week after the ordinary “artificial skin” was applied. One of the representative cases is shown in Figure 1. The infection was not serious and it subsided after removal of the silicone sheet (Fig. lC), and the secondary skin grafts took completely. It might be dangerous, however, if the infection became wide- spread. To use “artificial skin” safely on wounds prone to infection, such as extensive deep burns, it needs to be resistant to infection. For this purpose, a new material which permits sustained release of an antibiotic was developed and is described in this paper.
Figure l--(A) D-P flap elevated for reconstruction of defect of oral cavity and ordinary “artificial skin” placed on the muscle layer of the anterior chest and shoulder. (B) Much purulent discharge underneath the silicone layer one week after placing ordinary “artificial skin”. Examination of the discharge revealed Psedornonus aeruginosa. (C) The silicone layer on the infected area was partially removed and conservative therapy was continued for about 2 weeks until secondary skin grafting.
142
A Bilayer “Artificial Skin” Capable of Sustained Release of an Antibiotic 143
released amount/contained amount (%)
/
o--+ microsphere
z
I I I I I I 1 3 5 7 9 11 13 (days)
Fig. 2
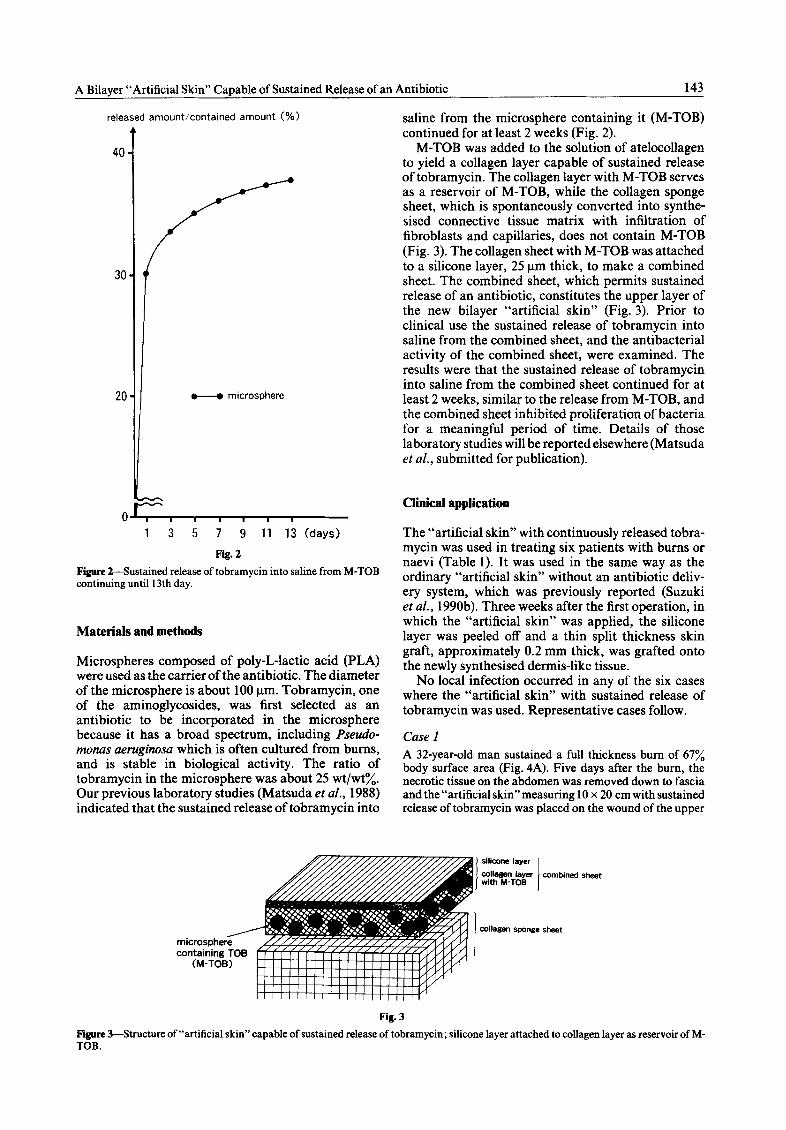
Figure 2-Sustained release. of tobramycin into saline from M-TOB continuing until 13th day.
Materials and methods
Microspheres composed of poly-L-lactic acid (PLA) were used as the carrier of the antibiotic. The diameter of the microsphere is about 100 pm. Tobramycin, one of the aminoglycosides, was lirst selected as an antibiotic to be incorporated in the microsphere because it has a broad spectrum, including Pseudo- monas aeruginosa which is often cultured from bums, and is stable in biological activity. The ratio of tobramycin in the microsphere was about 25 wt/wt%. Our previous laboratory studies (Matsuda et al., 1988) indicated that the sustained release of tobramycin into
saline from the microsphere containing it (M-TO@ continued for at least 2 weeks (Fig. 2).
M-TOB was added to the solution of atelocollagen to yield a collagen layer capable of sustained release of tobramycin. The collagen layer with M-TOB serves as a reservoir of M-TOB, while the collagen sponge sheet, which is spontaneously converted into synthe- sised connective tissue matrix with infiltration of fibroblasts and capillaries, does not contain M-TOB (Fig. 3). The collagen sheet with M-TOB was attached to a silicone layer, 25 pm thick, to make a combined sheet. The combined sheet, which permits sustained release of an antibiotic, constitutes the upper layer of the new bilayer “artificial skin” (Fig. 3). Prior to clinical use the sustained release of tobramycin into saline from the combined sheet, and the antibacterial activity of the combined sheet, were examined. The results were that the sustained release of tobramycin into saline from the combined sheet continued for at least 2 weeks, similar to the release from M-TOB, and the combined sheet inhibited proliferation of bacteria for a meaningful period of time. Details of those laboratory studies will be reported elsewhere (Matsuda et al., submitted for publication).
clinical application
The “artificial skin” with continuously released tobra- mycin was used in treating six patients with bums or naevi (Table 1). It was used in the same way as the ordinary “artificial skin” without an antibiotic deliv- ery system, which was previously reported (Suzuki et al., 1990b). Three weeks after the first operation, in which the “artificial skin” was applied, the silicone layer was peeled off and a thin split thickness skin graft, approximately 0.2 mm thick, was grafted onto the newly synthesised dermis-like tissue.
No local infection occurred in any of the six cases where the “artificial skin” with sustained release of tobramycin was used. Representative cases follow.
Case 1
A 32-year-old man sustained a full thickness bum of 67% body surface area (Fig. 4A). Five days after the bum, the necrotic tissue on the abdomen was removed down to fascia and the “artificial skin”measuring 10 x 20 cm with sustained release of tobramycin was placed on the wound of the upper
/ microsphere containing TOB
CM-TOB)
sheet
Fig. 3
Figure 3-Structure of “artificial skin” capable of sustained release of tobramycin; silicone layer attached to collagen layer as reservoir of M- TOB.
144 British Journal of Plastic Surgery
Table 1 Clinical uses of the “artificial skin” with sustained release of tobramycin
Extent of area grafted
Case Age Sex Site Cause (cm) Donor site
1 32 M Chest Bum 10x20 Scalp 2 23 F Thigh Naevus 20 x 30 Thigh 3 1 M Abdomen Bum 5x7 Inguinal 4 18 F Lower limb Naevus 25 x 15 Thigh, buttock 5 5 F Upper limb Naevus 18 x 15 Back 6 1 M Lower limb Bum 7x 10 Back
The take of secondary skin graft in all cases was perfect
abdomen (Fig. 4B). Three weeks later the silicone layer was peeled off (Fig. 4C). No infection occurred in newly synthesised connective tissue, though it was adjacent to uncovered burn. Thin patches of split skin graft taken from the scalp were placed on the connective tissue. One week later the secondary grafting had taken completely (Fig. 4D). Three weeks postoperatively, epithelialisation in the gaps between the patched skin grafts was complete. A postoper- ative view at 4 months indicates that contracture of the secondary skin grafts is minimal, with the thinness of the skin grafts taken into consideration (Fig. 4E).
Case 2
A 23-year-old woman suffered from a giant naevus of the left hip and thigh. The lesion of the lateral thigh had previously been treated with meshed skin grafts (Fig. 5A). The naevus of the hip was resected down to fat and the “artificial skin” without sustained release of tobramycin was placed on the wound with tie-over fixation. When this was removed one week later there was a partially purulent discharge underneath the silicone sheet (Fig. 5b). The
silicone sheets over the infected area were immediately peeled off and the infection subsided. Four months after the previous operation, the “artificial skin” with sustained release of tobramycin was used to resurface the anterior thigh (Fig. SC). Though the operation was performed in the same manner as the previous one, no infection occurred this time on the area covered with the “artificial skin” for 3 weeks until secondary grafting (Fig. SD). Meshed skin was placed on the newly synthesised connective tissue as the secondary skin graft and took perfectly. The postoperative appearance at 6 months is satisfactory, considering the meshed skin graft (Fig. 5E).
Discussion
Various materials may be used to carry an antibiotic and release it in a controlled manner. In our previous study (Matsuda ef al., 1988), we compared the manner of sustained release of tobramycin from three different materials (1) poly-L-lactic acid (PLA); (2) silicone to which polyvinyl alcohol (PVA) is added; and (3) hydrophilic polyurethane. Our previou,s studies indi- cated that sustained release of tobramycin from a microsphere composed of PLA continued for about 2 weeks, while no release of the antibiotic was observed from the silicone sheet containing PVA. In contrast, almost all the tobramycin was released at once on the first day when the hydrophilic polyurethane was used as a drug carrier. The results suggested that the two polymers other than PL-A were unsuitable as a carrier of tobramycin. PLA is a synthetic polymer which is harmlessly degraded to Hz0 and CO2 by water (Hyon et al., 1987). Tobramycin may be released mostly by
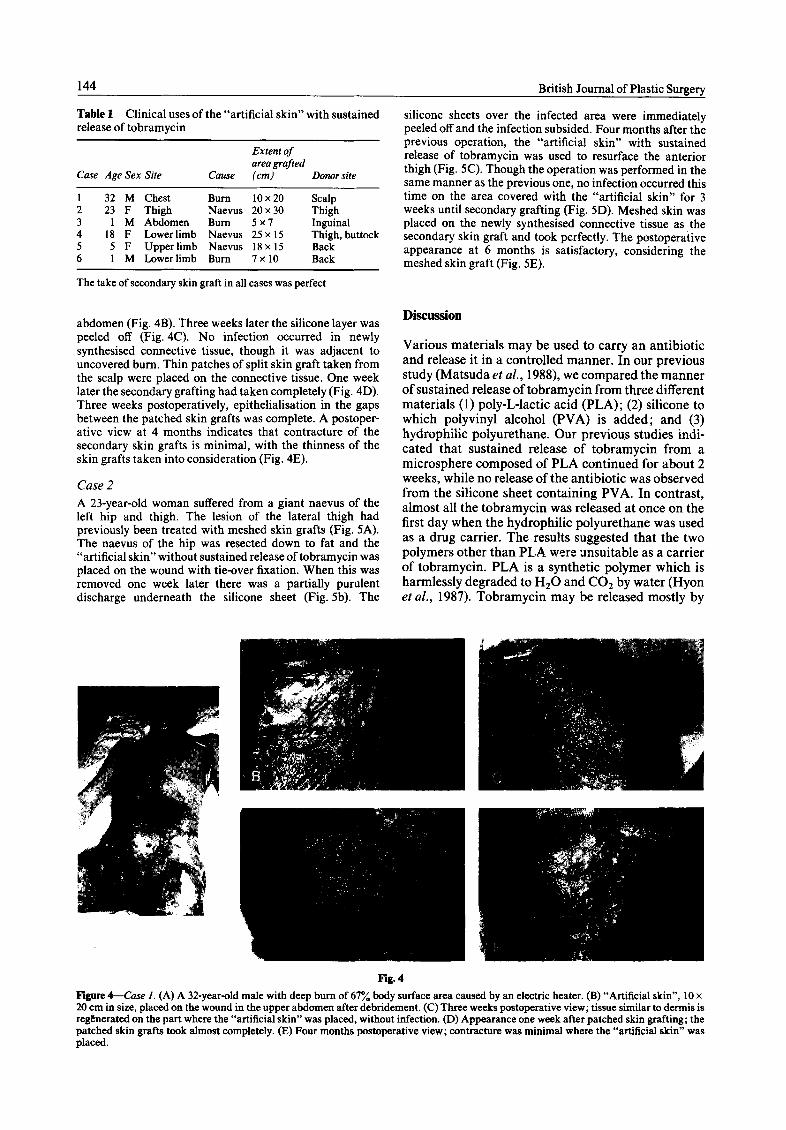
Figure 4-Case 1. (A) A 32-year-old male with deep bum of 67% body surface area caused by an electric heater. (B) “Artificial skin”, 10 x 20 cm in size, placed on the wound in the upper abdomen after debridement. (C)Three weeks postoperative view; tissue similar to dermis is regkierated on the part where the “artificial skin” was placed, without infection. (D) Appearance one week after patched skin grafting; the patched skin grafts took almost completely. (E) Four months postoperative view; contracture was minimal where the “artificial skin” was placed.
A Bilayer “Artificial Skin” Capable of Sustained Release of an Antibiotic
Fig. 5
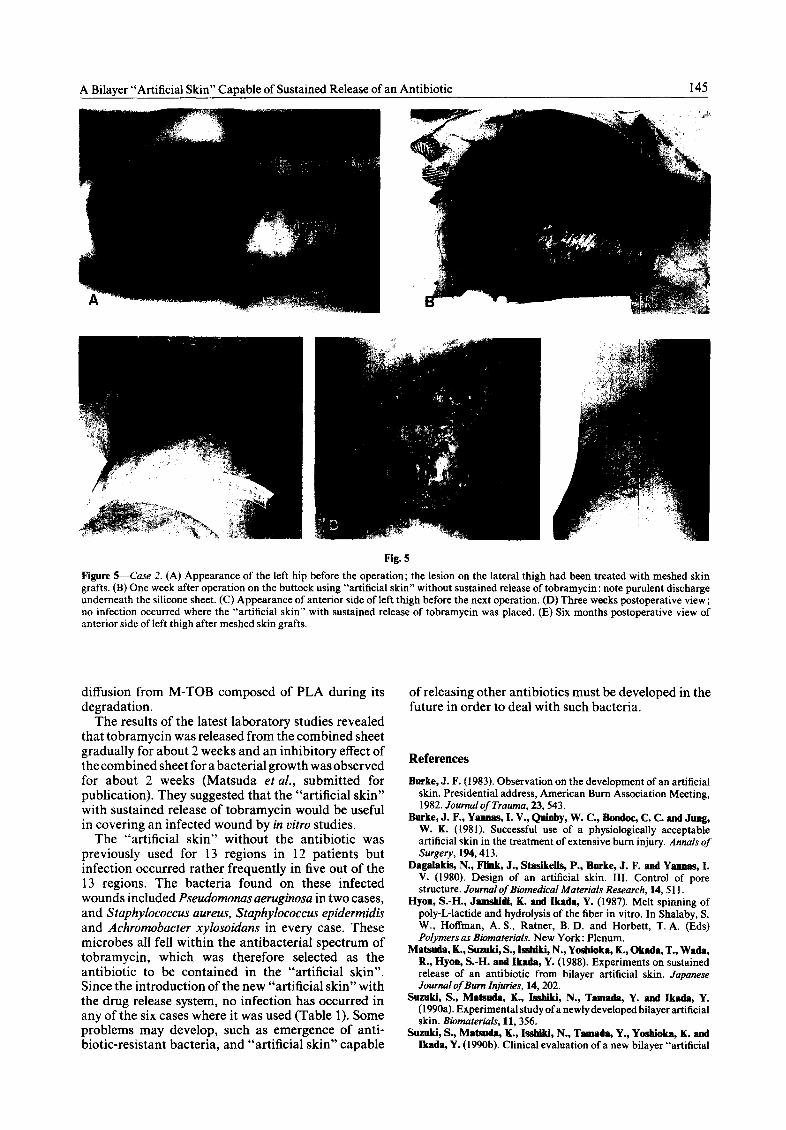
Figure %&se 2. (A) Appearance of the left hip before the operation; the lesion on the lateral thigh had been treated with meshed skin grafts. (B) One week after operation on the buttock using “artificial skin” without sustained release of tobramycin: note purulent discharge underneath the silicone sheet. (C) Appearance of anterior side of left thigh before the next operation. (D) Three weeks postoperative view; no infection occurred where the “artificial skin” with sustained release of tobramycin was placed. (E) Six months postoperative view of anterior side of left thigh after meshed skin grafts.
diffusion from M-TOB composed of PLA during its of releasing other antibiotics must be developed in the degradation. future in order to deal with such bacteria.
The results of the latest laboratory studies revealed that tobramycin was released from the combined sheet gradually for about 2 weeks and an inhibitory effect of the combined sheet for a bacterial growth was observed for about 2 weeks (Matsuda ef al., submitted for publication). They suggested that the “artificial skin” with sustained release of tobramycin would be useful in covering an infected wound by in vitro studies.
References
Burke, J. F. (1983). Observation on the development of an artificial skin. Presidential address, American Bum Association Meeting, 1982. Joumal of Trauma, 23,543.
The “artificial skin” without the antibiotic was previously used for 13 regions in 12 patients but infection occurred rather frequently in five out of the 13 regions. The bacteria found on these infected wounds included Pseudomonas aeruginosa in two cases, and Staphylococcus aureus, Staphylococcus epidermidis and Achromobacter xylosoidans in every case. These microbes all fell within the antibacterial spectrum of tobramycin, which was therefore selected as the antibiotic to be contained in the “artificial skin”. Since the introduction of the new “artificial skin” with the drug release system, no infection has occurred in any of the six cases where it was used (Table 1). Some problems may develop, such as emergence of anti- biotic-resistant bacteria, and “artificial skin” capable
Burke, J. F., Yannas, 1. V., Quinby, W. C., Bondoc, C. C. and Jung, W. K. (1981). Successful use of a physiologically acceptable artificial skin in the treatment of extensive bum injury. Annals of Surgery, 194,413.
Dagalakis, N., FBnk, J., StaaIkeBs, P., Burke, J. F. and Yannas, I. V. (1980). Design of an artificial skin. III. Control of pore structure. Journal of Biomedical Materials Research, 14,s 11.
Hyon, S.-H., Jamskidi, K. and Ikada, Y. (1987). Melt spinning of poly-L-lactide and hydrolysis of the fiber in vitro. In Shalaby, S. W., Hoffman, A. S., Ratner, B. D. and Horbett, T. A. (Eds) Polymers as Biamaterials. New York : Plenum.
Matsoda, K., Suzuki, S., hhiki, N., Yosbioka, K., Okada, T., Wada, R., Hyon, S.-H. and Ikada, Y. (1988). Experiments on sustained release of an antibiotic from bilayer artificial skin. Japanese Journal of Burn Injuries, 14,202.
Suzuki, S., Matsmda, K., J&&i, N., Tamada, Y. and ikada, Y. (1990a). Experimental study of a newly developed bilayer artificial skin. Biomaterials, 11,356.
Suzuki, S., Matsoda, K., Issbiki, N., Tamada, Y., Yosbioka, K. and Ikada, Y. (1990b). Clinical evaluation of a new bilayer “artificial

146 British Journal of Plastic Surgery
skin” composed of collagen sponge and silicone layer. British JournaIof Plastic Surgery, 43,47.
Yanoas, I. V. (1984). What criteria should be used for designing artificial skin replacements and how well do the current grafting materials meet these criteria? Journalof Trauma, 24,293.
Ya~as,I. V. (1988). Synthesisofapolymericmatrixforregeneration of skin and peripheral nerve. 3rd International Conference on Polymers in Medicine, Port0 Cervo, Italy, 1987. New York: Elsevier Press, p. 12.
Yannas, I. V. and Burke, J. F. (1980). Design of an artificial skin. I. Basic design principles. Journal of Biomedical Materials Research, 14,65.
Yannas, I. V., Burke, J. F., Gordon, P. L., Hoang, C. and Rubenstein, R. H. (1980). Design of an artificial skin. II. Control of chemical composition. Journal of Biomedical Materials Research, 14,107.
Yannas, I. V., Burke, J. F., Wnrpekoski, M., Staskeiis, P., Skrabut, E. M., Orgiii, D. and Giard, D. J. (1981). Prompt, long-term functional replacement of skin. Transactions of the American Society for Artifkial Internal Organs, 27, 19.
Ya~as, I. V., Burke, J. F., Orgili, D. P. and Skrabut, E. M. (1982). Wound tissue can utilize a polymeric template to synthesize a functional extension of skin. Science, 215,174.
The Authors
Kazuya Matsuda, MD, Research Fellow, Department of Plastic Surgery, Kyoto University.
ShigehIko BnxnItI, MD, Instructor, Department of Plastic Surgery, Kyoto University.
Nobubiko Issbiki, MD, Professor, Department of Plastic Surgery, Kyoto University.
Kazuo Yosbioka, PbD, Research Fellow, Research Center for Medical Polymers and Biomaterials, Kyoto University.
ToahIyuki Okada, PhD, Research Fellow, Research Center for Medical Polymers and Biomaterials, Kyoto University.
S.-H. Hymn, PhD, Research Fellow, Research Center for Medical Polymers and Biomaterials, Kyoto University.
Yoahlto Ikada, PbD, Professor, Research Center for Medical Polymers and Biomaterials, Kyoto University.
Requests for reprints to: Dr Kazuya Matsuda, Department of Plastic Surgery, Kyoto University, Shogoin, Sakyo-ku, Kyoto, 606 Japan.
Paper received 1 December 1989. Accepted 30 July 1990 after revision.



![antibiotic treatment reveals sustained effect against antimicrobial … · 1 Introduction 2 Bacterial antibiotic resistance has become a serious threat to human health 3 [1–3]](https://img.pdfslide.net/doc/110x75/5f51dbe291992003dd72a4ed/antibiotic-treatment-reveals-sustained-effect-against-antimicrobial-1-introduction.jpg)