Embed Size (px)
Citation preview

A case of Conn’s syndrome revealed after oral sodiumphosphate (fleet) preparation for colonoscopy
Ralph LEE, Martin STORR & Noel B. HERSHFIELD
Division of Gastroenterology, University of Calgary, Alberta, Canada
Oral sodium phosphate solutions (Fleet Mcneil Con-sumer Healthcare, Guelph, Ontario, Canada) are com-monly used as bowel cleansing agents in preparationfor colonoscopic exams; however, serious electrolytedisorders associated with oral sodium phosphateuse have been described in case reports includinghyperphosphatemia, hypocalcemia, hypomagnese-mia, hypernatremia, and hypokalemia. We describe a57-year-old patient with a past history of resistanthypertension who experienced severe symptomatichypokalemia following colonic cleansing with an oralsodium phosphate solution. Further investigationsrevealed a serum aldosterone of 691 pmol/L and a
serum renin level of 0.02 ng/L/s with a correspondingaldosterone-to-renin ration of 34550:1. The patientwas subsequently diagnosed with primary aldoster-onism secondary to an adenoma of the adrenal gland.Bilateral adrenal venous sampling revealed excessivelevels of aldosterone in the left adrenal vein prior todefinitive surgery. This case indicates that an oralsodium phosphate bowel preparation, though safe formost patients, can be complicated by a previously notdiagnosed endocrine disease like the primary aldos-teronism (Conn’s syndrome) reported here. This is thefirst report of a Conn’s syndrome diagnosed afterbowel cleansing with a sodium phosphate solution.
KEY WORDS: colonoscopy, Fleet, hyperaldosteronism, hypokalemia, sodium phosphate.
INTRODUCTIONcdd_425 111..114
Oral sodium phosphate solutions are commonly usedas bowel cleansing agents in preparation for colono-scopic exams. Each 45 mL dose contains 21.6 g ofmonobasic sodium phosphate monohydrate and 8.1 gof dibasic sodium phosphate heptahydrate in bufferedaqueous solution. Our most effective regimen is theadministration of one dose at 48 h plus one dose at24 h prior to colonoscopy. Sodium phosphate solu-tions have generally been found to be cheaper, more
effective and better tolerated by patients than othercolorectal cleansing regimens.1,2
In March 2002 Health Canada released a safety alertregarding sodium phosphate solutions.3 It warnedthat ‘electrolyte shifts could occur in patients withor without risk factors for electrolyte shifts if themaximum recommended dose of 45 mL [phosphorus5760 mg] in a 24-hour period was exceeded’. It wasalso advised that these solutions should not be used inpatients with congenital megacolon, bowel obstruc-tion, ascites, or congestive heart failure, and should beused with caution in patients with impaired renalfunction, heart disease, acute myocardial infarction,unstable angina, pre-existing electrolyte imbalances,patients taking drugs that could affect their electrolytelevels, and in elderly or debilitated patients. It recom-mended measurements of baseline electrolyte levelsand ensuring adequate pre-prep hydration in people
Correspondence to: Noel B. HERSHFIELD, Division ofGastroenterology, University of Calgary, Calgary, Alberta, Canada T2N4N1. Email: [email protected]© 2010 The AuthorsJournal compilation © 2010 Chinese Medical AssociationShanghai Branch, Chinese Society of Gastroenterology, RenjiHospital Affiliated to Shanghai Jiaotong University School ofMedicine and Blackwell Publishing Asia Pty Ltd.
Journal of Digestive Diseases 2010; 11; 111–114 doi: 10.1111/j.1751-2980.2010.00425.x
111

at risk for electrolyte imbalances or in cases where>45 mL of oral phosphate solution was used over a24-h period.
Love2 proposed that, given the superior cleansingaction of sodium phosphates, and their superiorpatient acceptance, the benefits of the solutions clearlyoutweighed the risks in normal healthy adults.However, renal failure and serious electrolyte dis-orders associated with oral sodium phosphate usehave been described in case reports including hyper-phosphatemia, hypocalcemia, hypomagnesemia,hypernatremia and hypokalemia. This seems often tobe associated with pre-existing and/or undiagnosedrenal impairment but other contributors like mucosalinflammation and impaired bowel motility were alsoimplicated,4 suggesting that patients with pre-existingmucosal damage should not receive oral sodiumphosphate solutions.
CASE REPORT
A 57-year-old woman was referred because of a historyof intermittent non-acute bright red rectal bleedingand occasional constipation. A flexible sigmoidoscopyperformed by a family practitioner approximately 2months before reported ulcerative proctitis and anadenomatous polyp. Subsequent biopsies confirmedthe presence of a tubular adenoma, but no patholo-gical findings were present at the apparent area ofinflammation.
Past medical history included a 6-year period of essen-tial hypertension which had proved difficult tocontrol. Apparently no secondary cause for her hyper-tension had been identified and the doses of herhypertensive medications had steadily increased overthe previous 5 years. Medications for this includedlisinopril 20 mg per oral once daily (OD), hydrochlo-rothiazide 12.5 mg per oral b.i.d. and Verapamil180 mg per oral OD. Other medications includedoccasional ibuprofen, a multivitamin and etidronatedisodium with calcium carbonate.
Prior to the colonoscopy her physical examinationwas normal. As per protocol the patient received 2doses of an oral sodium phosphate solution over thetwo consecutive nights prior to her procedure. She wasalso placed on clear fluids the day before her proce-dure and instructed to refrain from eating and drink-ing after midnight on the same day. Immediatelybefore her investigation her blood pressure was 150/90 mmHg with normal physical and rectal examina-
tions. The colonoscope was inserted and advanced tothe cecum. Findings included a sessile rectal polyp anda polypectomy was performed. The scope was with-drawn and the procedure was terminated.
Following completion of the colonoscopy the pati-ent complained of numbness and tingling in herlips, hands and feet. A repeat physical examinationrevealed a blood pressure of 140/85 mmHg withno other physical findings. Electrolyte values werepotassium <1.5 mmol/L, bicarbonate 32 mmol/Land sodium 142 mol/L. Repeat potassium was1.6 mmol/L. An electrocardiogram revealed a normalsinus rhythm of 72 beats per min with T-wave flatten-ing in leads V4 to V6 and U-waves visible across theleads. She was admitted to the hospital for evaluationand treatment of her electrolyte disturbance.
Further questioning of the patient uncovered an inter-mittent 2-month history of paresthesias in her face,left arm, hands, legs, and feet. A review of the patient’spast lab work revealed potassium of 3.4 mmol/L(sodium 143 mmol/L, carbon dioxide 27 mmol/L)and 3.1 mmol/L (sodium 143 mmol/L, carbondioxide 28 mmol/L), 6.5 months and 3 monthsbefore the procedure, respectively.
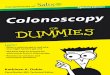
Aggressive i.v. therapy was initiated, which increasedthe patient’s potassium to 2.9 mmol/L (carbondioxide, 23 mmol/L), over a 48-hour period with thesubsequent resolution of her symptoms (see Fig. 1).Additional lab investigations exposed a serum aldos-terone of 691 pmol/L and a serum renin level of0.02 ng/L/s with a subsequent aldosterone-to-reninration of 34550:1. This clinical picture was highly sug-gestive of primary aldosteronism. She was dischargedhome on oral potassium, but she continued to havedifficulties maintaining her potassium levels. Shewas therefore started on amiloride hydrochloric acid10 mg per oral OD which stabilized her potassium at>3.8 mmol/L and she was able to safely discontinueher potassium supplements. A computed tomographyscan of her abdomen and pelvis confirmed the pres-ence of a well-circumscribed 1.5 cm ¥ 1.2 cm lesionarising from the medial limb of her left adrenal gland.Thus, she was referred to an endocrine surgeon. Bilat-eral adrenal venous sampling revealed excessive levelsof aldosterone in the left adrenal vein. This confirmedthe suspect diagnosis of Conn’s syndrome (primaryaldosteronism). The patient underwent an adrenalec-tomy with resulting normal blood pressure 6 monthslater.
Journal of Digestive Diseases 2010; 11; 111–114112 R Lee et al.
© 2010 The AuthorsJournal compilation © 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai
Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.

DISCUSSION
To allow a successful and satisfactory colonoscopywith perfect visualization of the mucosa, a completeand exhaustive bowel cleansing is imperative. Theperfect colonoscopy preparation is therefore effective,convenient, easy to perform and safe. Nowadayseither polyethylene glycol containing electrolyte solu-tions or sodium phosphate solutions are used forbowel cleansing. Trials comparing both regimenssuggest that sodium phosphate solutions are safe andmore or at least equally effective than polyethyleneglycol.5,6 Though sodium phosphate solutions are gen-erally safe, several cases of renal failure or seriouselectrolyte changes have occurred in healthy individu-als and patients with risk factors. If diagnosed in atimely manner, electrolyte imbalances are typicallyreversible and clinically insignificant.6
The case reported here of symptomatic hypokalemiathat developed in a patient after colonic preparationwith oral phosphate solutions indicates that inpatients without pre-existing renal impairment and
without ongoing diuretic treatment severe electrolytechanges may also occur. Our patient had a past historyof minor electrolyte disturbances, but none of theaforementioned medical contraindications to sodiumphosphate solution. Such an incidence should notonly result in the stabilization of the patient but alsoin timely additional investigations aiming to identifyconfounders to this derailment. Our patient was suc-cessfully stabilized with potassium chloride and sub-sequent investigations found primary aldosteronismto be the underlying cause of her hypokalemia andhypertension.
Primary aldosteronism is a pathological conditionwhere aldosterone production exceeds the body’snatural requirements, leading to increased sodiumreabsorption as well as urinary loss of sodium andbicarbonate at the distal nephron. Interestingly, mostpatients (>50%) do not present with hypokalemia.7
Even when precautions are taken, severe electrolyteimbalances can occur in patients receiving oralsodium phosphate solution and post-colonoscopy
0
1
2
Pot
assi
um L
evel
3
4
Time (24 h) & date of potassium measurement
6 monthsprior
6 daysprior
11:12 amDay 2
11:00am 12:20 00:10 amDay 2
10:05 pmDay 2
7:05 amDay 2
9:45 amDay 3
9:35 amDay 5
8:30 amDay 6
10:20Day 15
3.4
3.1
1.5 1.6
1.9
2.4 2.2
2.4
2.5
2.8 2.9
3.8
1
2
3
4 5
6
7
Figure 1. Potassium trends in the patient over time along with the various treatment modalities which were initiatedshowing; (1) oral sodium phosphate solution administered for colonic preparation; (2) the colonoscopy is performed; (3) i.v.normal saline drip with 40 milliequivalents (meq) potassium chloride (KCl)/L is initiated for the management of severehypokalemia; (4) regular oral KCl is initiated; (5) four sequential boluses of i.v. KCl are given; (6) the regular dose of oral KClis increased; (7) oral amiloride is started with the subsequent normalization of potassium levels. BID, b.i.d.; IV, i.v; OD, oncedaily; po, per oral.
Journal of Digestive Diseases 2010; 11; 111–114 Conn’s syndrome revealed after oral sodium phosphate 113
© 2010 The AuthorsJournal compilation © 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to ShanghaiJiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.

observation seems necessary, including electrolytecontrol when the patient presents symptoms. This caseshould serve as a reminder that when electrolyteimbalances, like the hypokalemia reported here, occura timely and thorough workup is imperative. This isthe first report of a Conn’s syndrome diagnosed afterbowel cleansing with a sodium phosphate solutionand this case report aims to raise awareness of unex-pected pre-existing conditions that contribute to com-plications when preparing patients for colonoscopy.
REFERENCES
1 Curran MP, Plosker GL. Oral sodium phosphate solution: areview of its use as a colorectal cleanser. Drugs 2004; 64:P1697–P1714.
2 Love J. The appropriate use of sodium phosphates oralsolutions. Can J Gastroenterol 2003; 17: 531.
3 Swann J. Important safety information regarding fleetphospho-soda (sodium phosphates oral solution). HealthCanada, 2005. Cited: 01.02.2009. Available from URL:http://www.hc-sc.gc.ca/dhp-mps/medeff/advisories-avis/prof/_2005/phosphate_solutions_3_hpc-cps-eng.php
4 Fass R, Do S, Hixson LJ. Fatal hyperphosphatemia followingFleet phospo-soda in a patient with colonic ileus. Am JGastroenterol 1993; 88: 929–32.
5 Hsu TW, Imperiale TF. Meta-analysis and cost comparison ofpolyethylene glycol lavage versus sodium phosphate forcolonoscopy preparation. Gastrointest Endosc 1998; 48:276–82.
6 Hookey LC, Depew WT, Vanner S. The safety profile of oralsodium phosphate for colonic cleansing before colonoscopyin adults. Gastrointest Endosc 2002; 56: 895–902.
7 Stowasser M, Gordon MD. Primary aldosteronism. Best PractRes Clin Endocrinol Metab 2003; 17: 501–605.
Journal of Digestive Diseases 2010; 11; 111–114114 R Lee et al.
© 2010 The AuthorsJournal compilation © 2010 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology, Renji Hospital Affiliated to Shanghai
Jiaotong University School of Medicine and Blackwell Publishing Asia Pty Ltd.