-
8/13/2019 A Cell-based Model of Coagulation and the Role of
Factor VIIa - Blood Review 2003
1/5
A cell-based model ofcoagulation and the role offactor
VllaMaureane HoffmanDepartment of Pathology, Duke University
Medical Center, Durham. NorthCarol ina. USA
Abstract Our cell-based m odel of haemostasis replaces
thetraditi onal cascade hypothesis, and proposes that coagul
ationtakes place on different cell surfaces in three ov erlapping
steps:initiation, amplification, and propagation. In highlighting
the im-portance of cellular co ntrol during coagula tion, the
cell-basedmodel allows a more thorough understanding of how
haemosta-sis works in vivo, and sheds light on the pathoph
ysiologica l mech-anisms behin d certain coagulation disorders. For
instance, thismodel proposes that haemophilia involves a failure of
platelet-surface FXa generati on, lead ing to a lack of
platelet-surfacethrombin production. Our data suggest that
high-dose FVlla isable to bind weakly to activated platelets,
independently of tissuefactor, in otder to generate sufficient
amounts of FXa to supporta burst bf thrombin generation in the
absence of FIXa/FVllla.The considerable success of high-dose
recombina nt FVll a (rFVlla;NovoSeven@, Novo Nordisk, Copenh agen,
Denmark) as a ther-apy for patients with haemophilia and inhibitors
has led to its usein a growing number of alternative indications.
We believe thateven in the presence of the FIXa/FVllla complex,
rFVlla may beable to enhance both FXa and FlXa levels on the
surface of acti-vated platelets , thus increasing the production of
thrombin .0 2003 Elsevie r Science Ltd. Al l rights reserved.
KEY WORDS: coagulation; cell-based m odel; haemostasis;
re-combinant factor Vll a; haemophilia
INTRODUCTION **$Q
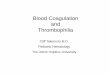
he classical model of coagulation descr ibes a cas-cade of
reactions involving activation of var ious clot-a ting factors
along either an extrinsic or an intrinsic
pathway. According to this model, st imulation of ei ther
ofthese two pa thways can resul t in the production of a
largeamount of thrombin and subsequent formation of a f ibrinclot
(Fig. 1).
Howeve r, al though this cascade paradigm supp orts labo-ratory
evaluation of coagulation disorders and demon stratesthe
interactions between coagulation factors, i t does notadequately
explain the mecha nisms leading to haem ostasisin viva.
Furthermore, i t does not provide a great deal ofinformation
regarding the pathophysiology of the haemo-static system. In part
icular , the model does not explain whycertain categor ies of
patients demonstrate a haemorrhagictendency; nor does i t faci l
itate accurare prediction of whichpatients wi l l actual ly bleed.
For instance, patients with a defi -ciency of factor XII @X II) ,
high-molecular-weight kininogen,or prekallikrein do not presen t w
ith a bleeding tende ncy de-
Intrinsic p8thW8yfactor XIIHMWK4factor Xl- factor XIa
ifactor IX- factor tXi3factor VllIa
Extrinsic pathway
factor VitaTissue facbr
factor X 1 = 4factor xa - facmr xfactor Va
fibrinogen --+ fibrinFig. I. The cascade hypothesis: intr insic
and extr insic pathways.
: spi te a prolonged part ial thromboplastin t ime (FIT), which:
indicates a disturbance in the functional activ i ty of the in-: tr
insic pathw ay.* In contrast, an increased predisposit ion to:
haemorrhagic r isk may be present in patients deficient in_ FXI.
The degree of prolongation of the FIT in this disor-i der, however,
does not necessar i ly predict the extent of the; bleeding
tendency, which is typical ly less severe than that: observed in
haemophi l ia.
The cascade hypothesis cannot account for the varying: degrees
of haemorrhagic tendency and diverse cl inical obser-: vations that
resul t from deficiencies of di fferent compone nts: of the two
pathwa ys. In an attemp t to explore the process: of haem ostasis
from new angles, we developed exper imental
and conceptual models that would al low us to test hy-potheses
in a biochemical or Ed r&o system . This, in turn,f would
increase understanding of how the normal haemo-
: static sy stem actual ly wo rks in &JO. In addi t ion, we
wished: to explore the mechan ism of haem ostasis in haemophi l
iac: patients. Such patients have a normal prothrombin t ime: (FT),
which measures activi ty o f the extr insic pathway, de-: spi te a
prolonged FIT and a pronounced bleeding tendency.: W hy, then, does
the extr insic pathway fai l to compen sate forI the dysfunctional
intr insic pathway? In other words, why doj haem ophiliacs
bleed?
We have developed a cel l-based model of haemo stasis that: wi l
l replace the classical model of the coagulation cascade.3: This
cel l -based model empha sises the interaction of clott ing:
factors with speci f ic cel l surfaces4 and appears to be able to:
shed light on many of the unresolved issues highlighted by: the
tradit ional cascade theory.
; THE CELL-BASED MODEL OF HAEMOSTASIS
The f i rst step in our investigation was to establ ish an in
vitroexper imental syste m incorporating platelets and plasma
con-centrations of var ious clott ing factors and coagulation
in-hibi tors. A cel lular source of t issue factor (TF ) was
consid-ered to be essential , and inclusion of TF-bear ing mon
ocytes
0 20 03 Elsevler Sdence Ltd. All r ights reserved. Blood Reviews
(2003) 17, 51-55
-
8/13/2019 A Cell-based Model of Coagulation and the Role of
Factor VIIa - Blood Review 2003
2/5
-
8/13/2019 A Cell-based Model of Coagulation and the Role of
Factor VIIa - Blood Review 2003
3/5
Ila
(4 IXa
b)
TF
+ FreevWF
IIIII--_______ ATFPI = t issue factor pathway inhibitor.
Fig. 3. The ceil-based mode l of haemostasis: (a) init iation,
(b) amplif ication , (c) propagation .
coagu lation, as initially postulate d by the original cas
cadehypothesis.Al though insuff ic ient to resul t in clot
formation by i tsel f,the smal l amount of thrombin generated at
the surface ofTF-bearing cells during the initiation phase is essen
tial inampl i fy ing the procoagulant signal . At ;he end of the
ampl i -f ication p hase, platelets activated by this l imited
amount ofthrombin are clad in activated cofactors and FXIa, and
theprocess of haemo stasis move s into the propagation phase.
PropagationDuring propagation, FlXa combines with i ts cofactor,
FV IIIa,on the surface of activated platelets. Some of the
requiredFIXa is produced on the surface of TF-bear ing cel ls
byTF/FV IIa, and can di ffuse to the activated platelets as i t
isnot inhibi ted by t issue factor pathway inhibi tor (TPPI) ,
andis only slowly inhibi ted by anti thrombln III (ATIII) . Facto
rIXa can also be produced on the platelet surface by FXIa.
Once formed, the FIXa/FV IIIa complex activates FX to
0 200 3 Elsevier Science ltd. All r ights reserved. Blood
Reviews (2003) I7, S/-S5
-
8/13/2019 A Cell-based Model of Coagulation and the Role of
Factor VIIa - Blood Review 2003
4/5
FXa, which immediately combines with i ts cofactor (Fig. 3~).The
FXa/FVa com plex then converts large amoun ts of pro-thrombin to
thrombin, resul ting in the cleavage of f ibrinogento f ibrin m
onom ers, which polymerise to consol idate the ini-tial platelet
plug into a stable fibrin clot.The cel l -based model therefore
places an empha sis onthe cellular con trol o f coagu lation, and
is subse quen tly ableto explain some cl inical aspects of haemo
stasis that theclassical cascade hypothesis cannot.4 It al lows a
more thor-ough understanding of how the coagulation process worksin
viva, and provides a greater degree of consistency withclinical
observation s of various coagulation disorders,
WHY DO HAEMOPHILIACS BLEED?When compared to the tradi tional
cascade theory, the cel l -based model faci l i tates a greater
understanding of the patho-physiological mecha nisms leading to
haemophi l ia. For in-stance, the cascade model does not explain
why the extr in-sic pathway appears unable to produce suff ic ient
amoun ts ofFX to at least part ially compen sate for a deficiency
of FVIIIor FIX. In other words, why does activation of FX by
theTP/FV IIa complex fai l to substi tute for the FXa that
wouldnormal ly be generated by FIXa/PVIIIa?
The cel l-based model does not sugg est that FXa genera-t ion by
the TF/FV IIa complex is insuff ic ient in haemophi l ia,but that i
t occurs on the wrong cel l surface. The FIXa/FV IIIacomplex
activates FX on the surface of platelets dur ing thepropagation
phase, whereas TF/PV IIa can only produce FXaon the surface of the
TF-bear ing cel l . The FXa producedon the TF-bearing cel l is
unable to move to the activatedplatelet surface, as there exist two
very eff ic ient inhibitors ofFXa in the plasma: TFPI and ATIII. At
normal plasma levels,both TFPI and ATIII inhibi t FXa so rapidly
and effectivelythat the hal f- li fe of FXa is 1 minute or less in
the f luidphase.2 Therefore, FXa that remains at the TF-bear ing
cel lis relatively protected from inhibit ion, whereas any FXa
thatdi ffuses from the surface is rapidly inhibited.
Accordingly, the cel l -based model proposes thathaem ophilia is
spec ifically a failure of platelet-surfac e FXageneration, which
resul ts in a lack of platelet-surface throm-bin production.
Haemophi l iac patients demonstrate rela-tively normal initiation
and amp lification phase s of coagula-tion, and so are able to form
an initial platelet plug a t thebleeding si te, but they cannot
generate the burst of throm-bin at the platelet surface that is
necessary to stabi l ise theinitial plug into a fibrin clot.
HOW DOES HIGH-DOSE FVBa ENHANCEHAEMOSTASIS IN HAEMOPHJLIA?As
discussed above, the cel l -based model of coagulationsuggests that
the total amou nt of FXa produced is lessimportant than the
location in which i t is generated.* Webel ieve that FXa mu st be
formed on the platelet surfaceby FIXa/PV IIIa, in close proximity
to w, in order to beincorporated into prothrombinase complexe s.
This meansthat the TF/FV IIa complex cannot compensa te for a lack
of
FIX/F VIII, as i t make s FXa in the wrong place. If this is
thecase, then eff ic ient haemophi l ia treatment mus t involve
therestoration of FXa generation on the platelet surface.
Our data imply that high-dose FVIIa is able to do just that- i t
can enhance haem ostasis in haemophi l iacs by activatingsuff ic
ient PX on the surface of activated platelets to supporta burst o f
thrombin generation.
Or iginaIly, our group favoured a TFdependent mecha nismin which
high doses of FVIIa could dr ive the TF pathwayin haemophi l iacs,
enhancing the performance of the extr in-sic pathway and therefore
producing haem ostasis. I t is wel lrecognised that PVIIa exhibi ts
very l i tt le proteolyt ic activ i tyin the absence of TE Howeve
r, the doses of FVIIa required toachieve coagulation in haemophi l
iacs produced plasma lev-els that were several orders of magnitude
greater than the &for binding of PVIIa to TF, leading some
researchers to sug-gest that FVIIa is unl ikely to work through a
TFdependentmechanism.
We used our exper imental model to determine howhigh-dose FVIIa
supports haem ostasis in patients withhaemophi l ia. I t was found
that FVIIa binds weak ly to ac-t ivated platelets, even though
platelets do not carry TEOnce bound to the platelet, PVIIa
generates a smal l amountof PXa, leading to the production of a l
imited amount ofthrombin on the platelet surface. These f indings
are alsoconsistent wi th our conceptual model of coagulation,
whichpostulates that platelet-surface FXa generation is requiredfor
the assemb ly of the prothrombinase complex and subse-quent
thrombin generation. Furthermore, the concentrationof FVIIa
required to produce detectable thrombin generationcorrelates with
the lowest concentration of PVIIa necessaryfor clinical eff icacy
in haem ophilia patien ts. loWhen compared to the amount of FXa
that would usu-al ly be produced by the FIXa/FV IIIa complex, the
quanti tygenerated by platelet-bound FVIIa is low. However, i t is
sig-ni f icantly higher than the level of FXa normal ly producedon
platelets of haemophi l iacs, and is certainly suff ic ient
toenhance thrombin generation in exper imental models of FIXand
FVIII deficiency.
We bel ieve that haemophi l ia is character ised pr imar ilyby a
faihrre o f platelet-surface thrombin generation. If thisis the c
ase, then resul ts from our studies in exper imentalmodels suggest
that high levels of FVIIa may part ially restoreFXa generation on
the platelet surface, leading to enhancedthrombin production in the
absence of FIX or FVIII (Pig. 4) .
We have tentatively made two extrapolations of our invi tro data
to the in vivo effects of high-dose FVIIa therapyin haemophi l ia.
First, OUT data suggest that a high dose isneeded because PVIIa
binds to platelets w ith a low aff ini tyo(d of 50-100 nM, rather
than 5 1 nM or less for FVIIabinding to TF).2 As a resul t, a high
concentration of FVIIais required to achieve even a mode st degree
of plateletbinding. At the concentrations of PVIIa attained in
z&o,binding to platelets is not saturated. This observation led
usto predict that an escalation of FVIIa dose should
thereforeincrease platelet-surface thrombin generation. Several
groUpshave confi rmed this theory by demonstrating that cl
inicaleff icacy may be attained by increasing the dose of FVIIa
inthose haemophikac patients who fai l to respond to ini tialdose
recommendations.
m Blood Reviews (2003) 17, S -55 0 2003 Elsevier Science Ltd.
All r ights reserved.
-
8/13/2019 A Cell-based Model of Coagulation and the Role of
Factor VIIa - Blood Review 2003
5/5
Fig. 4. High-dose FVlla partially restores platelet-surface
thrombin gen-eration in haem ophil ia . (Reproduced from Hoffman
M., Monroe D.M.3rd, Roberts H.R. Activated factor V II activates
factors IX and X on thesurface of activated platelets: thoughts on
the mechanism of action ofhigh-dose activated factor VII. Blood Co
agul Fibrinolysis 1998; 9 (Suppl.I): S6 IS65, with permission.)
The second extrapolation from studies of FVIIa in theexper
imental model is that the action o f high-dose FVIIain vivo is not
directly dependent on n, but is insteadplateletdepe ndent. Earlier
theories postulating a TFdep en-dent mode of action for FVIIa
explain the local isation ofFVIIa a$ti$i ty to the injury si te,
which may account for therelative lack of thrombotic compl ications
observed dur inghighdose FVIIa therapy, but do not adequately justi
fy therequirement for high do ses. lo Howeve r, a
platelet-dependentmecha nism in which FVIIa binds to platelets w
ith low aflin-i ty al lows not only foe the local isation of FVIIa
activi ty, butalso explains why high dos es are required to attain
clinicallyeffective levels of thrombin generation. Whi le this
theoryof platelet dependence does not preclude other actions
andeffects of FVIIa, i t is consistent wi th empir ical ly
determineddosing requirements. Howev er, i t is important to be
awarethat this mechanism is not truly TF- independent, as TF is st
i l lrequired for the initiation of coagu lation. The theory of
aplateletdependent mechan ism of action simply impl ies thatthe pr
imary effect of FVIIa occurs on the platelet surface.
i
0 2003 Elsevier Science Ltd. All r ights mserved. Blood Reviews
(2003) 17, 5 l-55 m
CONCLUSIONS
When compared to the tradit ional cascade hypothesis, webel ieve
that the cel l -based conceptual model of haemosta-sis al lows a
more fundam ental understanding of the cl inicalproblems observed
in some coagulation disorders by focus-ing on the cen tral role of
spec ific cell surfac es in controll ingand directing the haemo
static process.Our cel l -based model bui lds upon the foundations
laid bythe tradi tional cascade theory, but places greater empha
sison the roles of speci f ic receptors present on the surfaces
ofthe cel ls involved. Importantly, the cel l -based model sug
geststhat understanding the structure and function of coagula-t ion
proteins is necessary, but not suff ic ient, to understandhaemo
stasis in vivo. Accordingly, this more recent modelprovides a
potential ly more accurate representation of the
haemo static process in vivo, and facil i tates a greater
un-derstanding of the pathophysiological mecha nisms
behindcoagulation disorders such as haemophi l ia.
Haemophi l ia may be chamcter ised by a fai lure of
platelet-surface thrombin generation in the f inal propagation
stageof the haem ostatic process. High-dose recombinant
FVIIa(rFVIIa; NovoSeven@ , Novo Nordisk, Copenhagen, Denma rk)has
shown considerable succe ss as a therapy for haemophi l-iacs and
inhibi tor patients, and this success may be due toa mechan ism of
action involving platelet-surface FXa gener-ation. This resul ts in
enhanced thrombin production, andmay part ial ly compensa te for
the deficiency of FIX or FVIII.The eff icacy of high-dose rFVIIa in
haemophi l ia and Inhibi torpatients has led to i ts use in a
growing number of al ternativeindications, and data regarding i ts
mechan ism of action insuch circumstance s are scarce. However, we
bel ieve tha teven in the presence of the FIXa/FV IIIa complex,
FVIIa maybe able to enhance both FXa and FIXa levels on the
plateletsurface, thus augmenting the production of vi tal
thrombin.
References
I. Davie EW, Ratnoff OD. Waterfall sequence for intr insic blood
c lot-t ing. Science 1964; 145: I 3 IO- I 3 12.
2. Hoffman M. Mechanism of action of NovoSeven@using a
cell-basedmode l. B loodli ne Reviews 2002; I : 5-6.
3. Veldman A. Hoffman M, Ehrenforth S. New insights into the
coag-ulation system and implications for new therapeutic options
withrecombinant factor Vlla. Curr Med Chem 2003; IO: 797-81 I.
4. Hoffman M, Monroe DM 3rd. A cell-based mode l of
hemostasis.Thromb Haemost 2001; 85: 958-965.
5. Monroe DM. Roberts H R. Hoffman M. Platele t procoagulant
com-plex assembly in a t issue factor- init iated system. Br J Haem
atol 1994;88: 364-37 I.
6. Mann KG. Poten tial analytes for the diagnosis of thrombosis.
Anoverv iew. Ann Ep idemiol 1992; 2: 365-370.
7. Bag lia FA, Bad ell ino KO. Li CQ, Lopez JA, Walsh PN. Factor
Xl bind-ing to the platelet glycoprotein lb-IX-V complex promotes
factorXl activation by thrombin. J Biol Chem 2002; 277: I662- 16
68.
8. Oliver ]A, Monroe DM, Roberts HR. Hoffman MR. Feedback
acti-vation of factor XI on platelets in the absence of factor XII.
Arte-r ioscler Thromb Vast Biol 1999; 19: 170-l 77.
9. Hoffma n M, Monroe DM 3rd. Roberts HR. Activated factor VII
acti-vates factors IX and X on the surface of activated platelets:
thoughtson the mechanism of action of high-dose activated factor
VII. Bloo dCoagu l Fibrinolysis 1998; 9 (Suppl I): S6 I-S65.
IO. Monroe DM, Hoffman M. Oliver ]A, Roberts HR. Platele t activ
ity ofhigh-dose factor Vlla is indepen dent of t issue factor. Br J
Haema tol1997; 99: 542-547.


























![Abnormalities of Blood Coagulation[1]](https://img.pdfslide.net/doc/110x75/577cce2b1a28ab9e788d80ee/abnormalities-of-blood-coagulation1.jpg)
