Embed Size (px)
DESCRIPTION
The postsurgical stability of two groups of patients treated with different fixation techniques after mandibular advancement was evaluated retrospectifvely.
Citation preview

A comparative study advancement surgery
of stabitity after mandibular
Ekaterina Douma,* M. M. Kuftinec,** and Farhad M6shiri*** Louisville, Ky., and Athens, Greece.
The postsurgical stability of two groups of patients treated with different fixation techniques after mandibular advancement was evaluated retrospectively. Sixteen patients (group 1) underwent rigid osseous fixation, and another group of 16 patients (group 2) underwent intraosseous wiring fixation. Our findings suggested that skeletal and dental changes occurred in both groups as a result of adaptation to the altered functional equilibrium. Relapse resulting in a percentage loss of the initial advancement occurred primarily 6 to 8 weeks postsurgically. No statistically significant difference was found to exist in,the short-term and long-term rates between the two groups. For the population studied, relative stability after mandibular advancement surgery was affected more by individual variability than by the fixation technique. (AM J ORTHOD DENTOFAC ORTHOP 1991 ;100:141-55.)
T h e application of combined surgical- orthodontic procedures for the treatment of major facial deformities and associated malocclusions has become an increasingly prevalent treatment modality over the past 2 decades. Development of sound conjoint treat- ment principles made possible the correction of skeletal and dental dysplasias that were unyielding to either surgical or orthodontic treatment alone? "2 The orthog- natbic surgery option gives a clinician the ability to correct skeletal dysplasias in nongrowing patients, as well as to treat severe progressive deformities in ado- lescents and young adults. 3 Skeletal Class II malocclu- sions resulting from mandibular retrognathism often re- quire a combined orthodontic-surgical approach for op- timal function and best esthetic results. The sagittal split ramus osteotomy is currently one of the most favored surgical techniques for the management of mandibular retrognathism. 2 The technique has been successfully used by many clinicians over the years. Despite its popularity, however, one factor still remains a major concern in the surgical correction of mandibular ret- rognathism: its potential for relapse3 In fact, several investigations have shown that skeletal relapse is the most often encountered sequela of mandibular advance- ment surgery; it usually occurs early in the postsurgical period.
*Former resident, now in practice in Athens, Greece. **Professor of Orthodontics, Director of Postgraduate Program, University of Louisville, Louisville, Ky. ***Clinical Professor of Orthodontics, University of Louisville, Louisville, Ky. 8/1/21619
Although skeletal relapse seems to be a multifac- torial phenomenon, according to short-term and long- term follow-up of clinical cases, different.studies have suggested a link between certain etiologic factors. Po- sitional change of the proximal segment was found to be the most important parameter in determining stability of the advanced mandible. According to recent stud- ies,58 intraoperative distraction of the mandibular con- dyles from their functional position in the glenoid fossae results in a dramatic skeletal relapse immediately on release of intermaxillary fixation. The relapse occurs because a large discrepancy between the functional oc- clusal position and the terminal hinge position is cre- ated. Paramandibular connective tissue tension from the skin, interstitial connective tissue components, and en- veloping periosteum have also been reported as etio- logic factors in relapse. Recent reports indicate that the relapse seen after mandibular advancement surgery is a result of paramandibular connective tissue tension, lack of control of the proximal segment during surgery, condylar distraction, inadequate fixation periods, mag- nitude of advancement, t/nfavorable growth postsurgi- cally, and preexisting internal derangement of the tem- poromandibular joints. 9'2 To minimize relapse, intraos- seous fixation of the bone segments with stainless steel wires was used for a period of 6 to 8 weeks after surgery. Histologic studies have shown that wiring of the prox- imal and distal segments provide semirigid fixation at best. 13~7 The patient with an osteotomy is at risk of relapse for as long as 25 weeks after surgery. In an effort to prevent intersegment movement and to promote primary bone healing, a technique for rigid approxi-
141

142 Douma, Kttftinec, atzd Moshiri Am. J. Orthod. Dentofac. Orthop. August 1991
Po
(3 Or
G~
Me
Fig. 1. Hard tissue cephalometric landmarks used in study.
mation and fixation of the bony segments has evolved. The objective was tO prevent a major source of relapse while simultaneously reducing the length of intermax- illary dental fixation. Rigid fixation after sagittal split osteotomy for mandibular advancement was accom- plished by means of compression screws, usually in- serted through a small skin incision at a 90 ° angle to the osteotomy site. z8-2~
Recent investigations of rigid fixation reported a good postsurgical stability, with a capability o f e a r l y masticatory function, improved nutrition, and a faster rate of recovery. When the relapse rates in intermax- illary and rigid fixation groups were compared, skele- tal changes in the rigid fixation group were statistically smaller than those in the intermaxillary group. The rel- atively new technique was thus reported to be effec- tive and stable. However, sufficient clinical documen- tation to support the theoretical concepts is not readily available.
The purpose o f this study was to investigate any significant differences between rigid and intraosseous wiring fixation techni~tues in patients treated with bi-
lateral sagittal split ramus osteotomy for mandibular advancement. Comparisons were to be made of any short-term and long-term skeletal and dental changes between the two groups.
METHOD AND MATERIALS
Two groups of 16 patients each who underwent mandib- ular advancement by means of bilateral sagittal split ramus osteotomy for correction of mandibular retrognathism were selected for this study. Patients who had any additional sur- gery (e.g., genioplasty or two jaw procedures) were not in- cluded in our sample. All the surgical procedures were per- formed by two "members of the same oral surgery group in an attempt to eliminate major technical differences. No max- illary surgical procedures were performed in any of the pa- tients. The cephalograms were taken in norma lateralis, on the same cephalometers, so that magnification factors would remain constant, and reasonable comparisons could be made.22.23
Group 1 consisted of 14 females and 2 males with a mean age of 30.68 years (range, 14 to 50 years). Stabilization of the segments was achieved postsurgically by means of bone compression screws, which were consistently placed through

Volume 100 Stability after mandibular advancement surgery 143 Number 2
o
\
L~L
I
1 UFH
:L
Fig. 2. Soft tissue landmarks and constructed parameters (after Moshiri F. J Clin Orthod 1982;16:37- 59): UFH, upper face height; NLA, nasolabial angle; ULL, upper lip length; LLL, lower lip length; FCA, facial contour angle.
Table I. P e r c e n t a g e s o f r e l a p s e
Short-term relapse (Ar - PgT,) - (Ar - PgT0 *100 (Ar - PgT2) - (Ar - PgT0
Long-term relapse (Ar - PgT3) - (Ar - PgT4)*100 (Ar - PgT2) - (Ar - PgT0
Total relapse (Ar - PgT2) - (Ar - PgT4) *100 (Ar - PgTz) - (Ar - PgTO
Group 1 (rigid fi.ration)
Mean (SD)
Group 2 (wire firation)
Mean (SD)
t tests
Group 1 to group 2
20.7 (21.6) 17.6 (20.2) 0.70 (NS)
10.1 (17.8) 6.1 (20.4) 0.62 (NS)
31.4 (30.4) 23.0 (31.5) 0.49 (NS)
No'rE: For explanation of T, - T4, see Fig. 3.
an intraoral approach. Interdental fixation with an occlusal
spl int in place was used for up to 2 weeks . 2'
Group 2 cons i s ted o f 13 female and 3 male patients who
also underwen t mand ibu la r a d v a n c e m e n t through bilateral
sagit tal split r a m u s os teo tomy. In this group, inferior border
in t raosseous wir ing o f the bony s egmen t s was emp loy ed to
assure stabil i ty and ensu re aga ins t major skeletal relapse. 2~
In addit ion, interdental fixation with an acrylic occlusal
splint was rout ine ly main ta ined for a period o f 6 to 8
weeks .
144 Dottma, Kt~inec, and Moshiri Am. J. Orthod. Dentofac. Orthop. August 1991
G R O U P
RIGID FIXATION
A
I JI¢
SURGICAL CHANGE -I
FIXATION CHANGE I
POSTFIXATION I" CHANGE "1
4 NET POSTSURGICAL CHANGE 'l
NET LONG-TERM CHANGE
T1 T2 T3 T4
PRESURGERY IMMEDIATE SHORT-TERM LONG-TERM
POSTSURGERY
MEAN [S.DI 3.3 DAYS 11.541 2.15 MOSII.071 11.15 MOSI3.601
MINIMUM 2 1 7
MAXIMUM 8 4 1 8
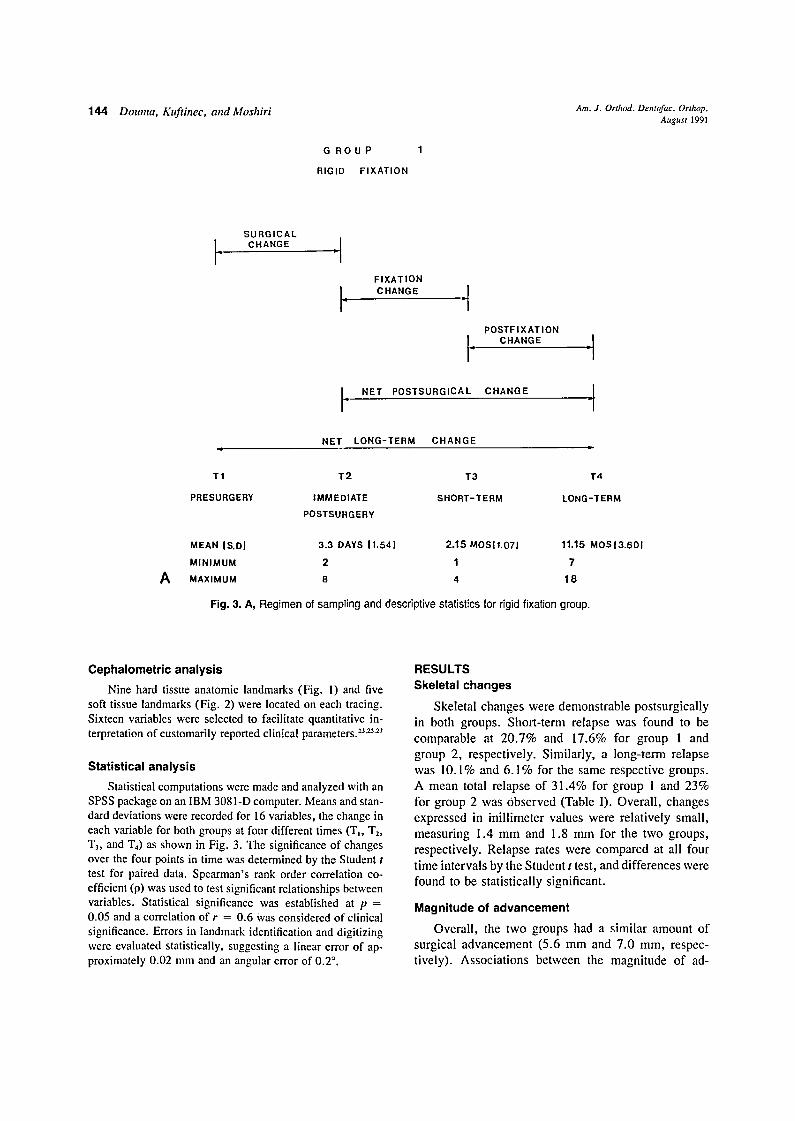
Fig. 3. A, Regimen of sampling and descriptive statistics for rigid fixation group.
Cephalometric analysis Nine hard tissue anatomic landmarks (Fig. 1) and five
soft tissue landmarks (Fig. 2) were located on each tracing. Sixteen variables were selected to facilitate quantitative in- terpretation of customarily reported clinical parameters. 23'~27
Statistical analysis
Statistical computations were made and analyzed with an SPSS package on an IBM 3081-D computer. Means and stan- dard deviations were recorded for 16 variables, the change in each variable for both groups at four different times (TI, T2, T3, and 'I"4) as shown in Fig. 3. The significance of changes over the four points in time was determined by the Student t test for paired data. Spearman's rank order correlation co- efficient (p) was used to test significant relationships between variables. Statistical significance was established at p = 0.05 and a correlation of r = 0.6 Was considered of clinical significance. Errors in landmark identification and digitizing were evaluated statistically, suggesting a linear error of ap- proximately 0.02 mm and an angular error of 0.2".
RESULTS Skeletal changes
Skeletal changes were demonstrable postsurgically in both groups. Short-term relapse was found to be comparable at 20.7% and 17.6% for group 1 and group 2, respectively. Similarly, a long-term relapse was 10.1% and 6.1% for the same respective groups. A mean total relapse of 31.4% for group 1 and 23% for group 2 was Observed (Table I). Overall , changes expressed in inill imeter values were relatively small , measuring 1.4 mm and 1.8 mm for the two groups, respectively. Relapse rates were compared at all four time intervals by the Student t test, and differences were found to be statistically significant.
Magnitude of advancement
Overall , the two groups had a similar amount of surgical advancement (5.6 mm and 7.0 mm, respec- tively). Associations between the magnitude of ad-
Volume I00 Number 2
G R O U P
INTERMAXIL LARY
Stability after mandibular advancenzent s,+rgery
2
FIXATION
145
B
SURGICAL CHANGE "1
I- FIXATION CHANGE I-
POSTF|XAT|ON 14 CHANGE ii I
t + NET POSTSURGICAL CHANGE "1
NET LONG-TERM CHANGE
T1 T2 T3 T4
PR ESURGERY IMMEDIATE SHORT-TERM LONG-TERM POSTSURGERY
MEAN IS.D.I 6.06 DAYS 13.711 2.43 MOS I1.111 22.85 MOS 111.091
MINIMUM 2 1 12 MAXIMUM 18 5 46
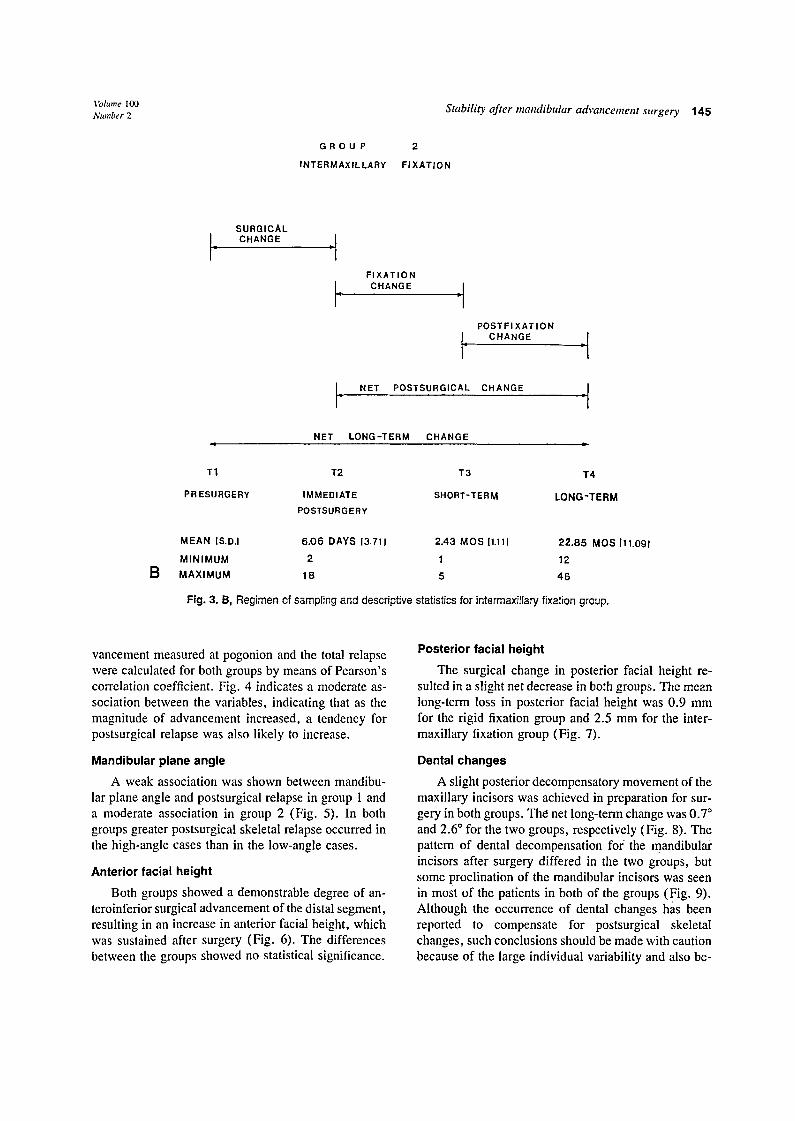
Fig. 3. B, Regimen of sampling and descriptive statistics for intermaxi~lary fixation group.
vancement measured at pogonion and the total relapse were calculated for both groups by means of Pearson's correlation coefficient. Fig. 4 indicates a moderate as- sociation between the variables, indicating that as the magnitude of advancement increased, a tendency for postsurgical relapse was also likely to increase.
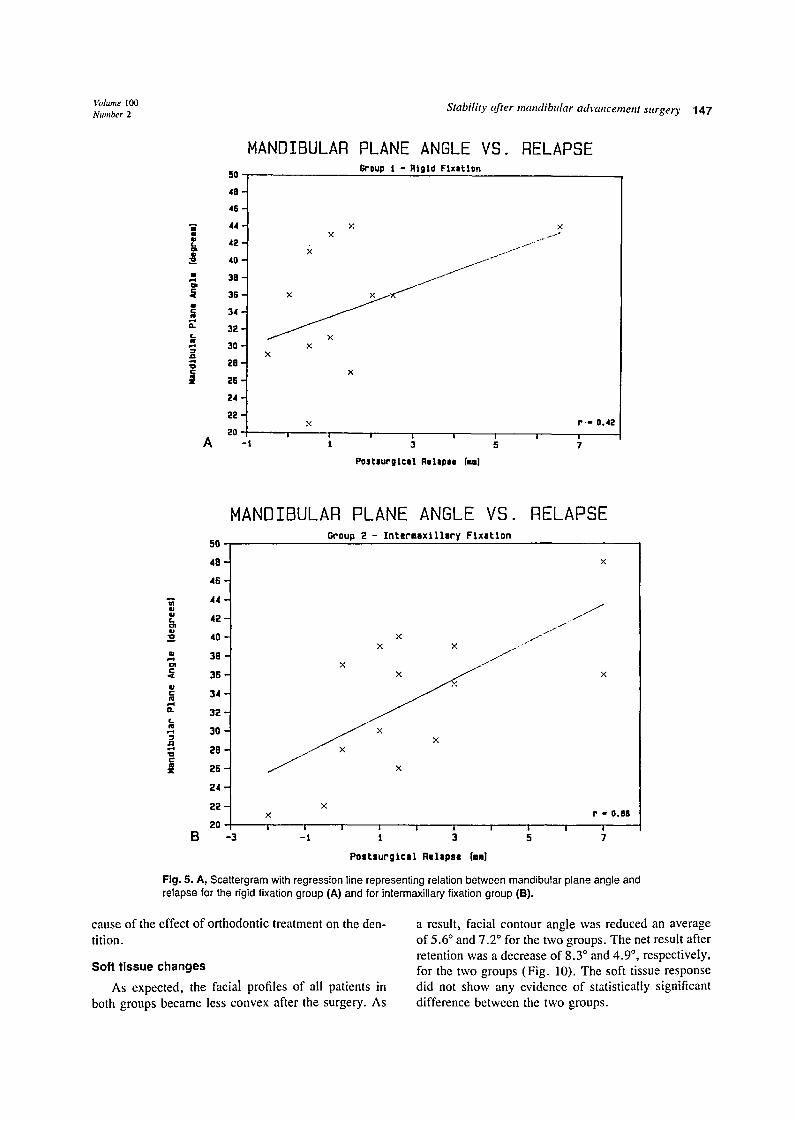
Mandibular plane angle
A weak association was shown between mandibu- lar plane angle and postsurgical relapse in group 1 and a moderate association in group 2 (Fig. 5). In both groups greater postsurgical skeletal relapse occurred in the high-angle cases than in the low-angle cases.
Anterior facial height
Both groups showed a demonstrable degree of an- teroinferior surgical advancement of the distal segment, resulting in an increase in anterior facial height, which was sustained after surgery (Fig. 6). The differences between the groups showed no statistical significance.
Posterior facial height
The surgical change in posterior facial height re- sulted in a slight net decrease in both groups. The mean long-term loss in posterior facial height was 0.9 mm for the rigid fixation group and 2.5 mm for the inter- maxillary fixation group (Fig. 7).
Dental changes
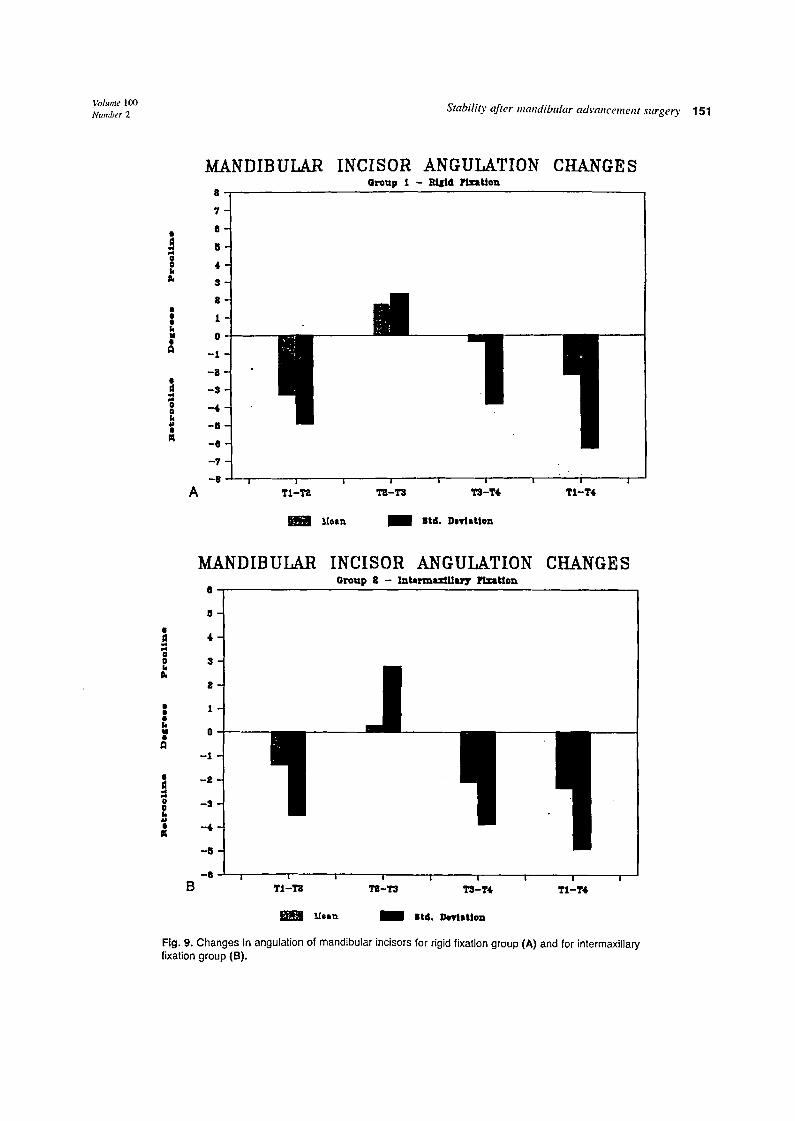
A slight posterior decompensatory movement of the maxillary incisors was achieved in preparation for sur- gery in both groups. The net long-term change was 0.7 ° and 2.6 ° for the two groups, respectively (Fig. 8). The pattern of dental decompensation for the mandibular incisors after surgery differed in the two groups, but some proclination of the mandibular incisors was seen in most of the patients in both of the groups (Fig. 9). Although the occurrence of dental changes has been reported to compensate for postsurgical skeletal changes, such conclusions should be made with caution because of the large individual variability and also be-

146 Douma, Kuftinec, and Moshiri Am. J. Orthod. Dentofac. Orthop. August 1991
i 8 -
i 5 -
i i4 o
c m I t "D
< i0
g
L 8
~ 7
5
~ s
g 4
2 ,
i
A
SURGICAL ADVANCEMENT VS. Group i - R ig id F i x a t i o n
/ " o f
i
X ~ x X
X i i i i i
I 3
Postsungica l Relapse [,,-1
RELAPSE
J /
.1
j . -
X
P " 0.73
I I 5 7
SURGICAL ADVANCEMENT VS. RELAPSE Group 2 - I n t e r = s x l l l a r y F i x a t i o n
iB
i 7 -
i 6 -
i 5 - x
i 4 - c
i 3 -
¢ 1 2 - x x 11 > i t - J " " "u ~'"
iO - ..- J f ~ x ,,K
'~ 9 - ! " /
8 " x
ul 7-
s - / x
.,~ 4 - X ×
~ 3 - X • X
2 "
t l ,~ P - o.01
0 ' i J I l I i i i | I I -3 - 1 3 5 7
B P o s t s u r g i c e l R e l a p s e (ram}
Fig. 4. Scattergram with regression line representing relation between magnitude of mandibular ad- vancement and amount of postsurgical relapse for rigid fixation group (A) and for intermaxillary fixation group (B).
Volume I00 Number 2
|
g "o c
A
50
HANDIBULAR
Stability after mandibular advancement surgery
PLANE ANGLE VS. RELAPSE Group I - Rtgld Flxatlan
48
45
44
42
40
38
36
34
32
3 0
2e
2 6 "
2 4 -
2 2 "
20 - t
x x x t ~°
x
.',,: r - 0.42 i | i ! i i i /
t 3 5 7
Pos t l u ro l ca l Relepee [ inl
147
50
MANDIBULAR PLANE ANGLE VS. RELAPSE Group 2 - Intermaxi l lory Ftxet lon
,¢[ ILl ¢- ¢l
rt .,-e ID
Z
48
46
44
42
40
38
36
34
32
30
26
26
24
22
2O -3
. j J X . i -
X X j r -
X t
x × r ,, 0.00
I it. ] ; i I I s I I B - 1 3 5 7
P o s t s u r g t c a l R e l a p s e [alm]
Fig. 5. A, Scat tergram with regression l ine represent ing relation between mandibular p lane angle and relapse for the rigid f ixat ion group (A) and for intermaxi l lary f ixat ion group (B).
cause of the effect of orthodontic treatment on the den- tition.
Soft t issue changes
As expected, the facial profiles of all patients in both groups became less convex after the surgery. As
a result, facial contour angle was reduced an average of 5.6 ° and 7.2 ° for the two groups. The net result after retention was a decrease of 8.3 ° and 4.9 °, respectively, for the two groups (Fig. 10). The soft tissue response did not show any evidence of statistically significant difference between the two groups.

148 Douma, Kuftinec, and Moshiri Am. J. Orthod. Dentofac. Orthop. Augztst 1991
ANTERIOR FACIAL HEIGHT Group 1 - Rigid FlxuUon
CHANGES
|
l -1
- 2
- - ~ I i I I I ~ I I
A T1--T2 "r2 -1"J T3--T4 TI -T4
IJ©an ~ Std. Deviddon
ANTERIOR FACIAL HEIGHT CHANGES G r i p 2 - Interrnaxlllary Fixation
| 0
0 _c
E E 0
| - I
- 3
~ ! | | I ! I | I I
B T1-T2 T2-T3 1"3-1"4 TI -T4
IJaon ~ 1 Std. DevlaUon
Fig. 6. Changes in anterior facial height for rigid fixation group (A) and for intermaxillary fixation group (B). (Note large standard deviations calculated for both groups of parameters on these and the ensuing figures.)

~,blume I00 Number 2 Stability after mandibular adrancenmnt surgery 149
§ i
I 4 ~ -
3 -
| -
1 -
I}
_~ -
. - 4 -
.-5 A
POSTERIOR FACIAL HEIGHT I - ~ e m~m~Qa
CHANGES
I J I I I I J
TI-T~ T~-T3 T'J-T4 TI-T4
i },.[etn ~ 1 ~ St.d. Dev'JaUon
POSTERIOR FACIAL HEIGHT GrOup 2 -- Inbwn~dll~'y
CHANGES
| -1 0
-3
!1 B " ' 4 i i I i I I i i i
T1 -T2 12-1"3 T3--T4 TI -T4
J !Joan ~ Stzt. Devl~on
Fig. 7. Changes in posterior facial height for rigid fixation group (A) and for intermaxillary fixation group (B).

150 Domna, Kuftinec, and Moshiri Am. J. Orthod. Dentofac. Orthop. August 1991
! | k M
o
A
MAXILLARY y ,
8
8 -
$
|
1
0
- 1
- I
- 6
- 5
- 8
- 7 !
T 1 - T a
MAXILLARY 8
INCISOR ANGULATION CHANGES O r o u p I - It18id Y t . z ~ t t ~
!1
I I I 1 I I
'r2-T3 TS-T4, TI -T4,
Moth i Std. D e v i a t i o n
INCISOR ANGULATION Group 2 - Im~armaxlUary FIxltlom
CHANGES
0 0 b
7 ~
6 -
5 -
4 -
3 -
a -
| t - k v O - w
- - l -
- - t - • i
! -a- " 4 1 -
B ~ l l I I I I I I I I
TI-TI~ T S - T 3 ~ - T 4 T I - T 4
i m m L[osn ~ s td . l ) ev i s t lon
Fig. 8. Changes in angulation of maxillary incisors for rigid fixation group (A) and for intermaxillary fixation group (B).
Voh,me 100 Stabilit)" after mandibular advancement surgery 151 Number 2
0 0 k P,
k M
d 0 k ,p
m
MANDIBULAR
'1 7 -
O -
U -
4 -
3 -
1 -
0 -
-1
A
-0
-7
-0
INCISOR ANGULATION CHANGES OFoUp ! - RiIld ~ : I t iOn
I I J " I I I i
T1-TI1 TSI-T3 ~J-T4. TI-T4
Moth i Btd. Deyiation Bi,
MANDIBULAR
0
INCISOR ANGULATION Group B -- ~ s , ~ t l t z ' 7 Fl.zll:ton,
CHANGE S
5
3
2
• I
h u 0
-1
• - 2 - d
o - 3 - o
• - 4 III
-§
- a i i i , i i i
B TI-TB TS-T3 T3-T4, T1-T4
~esn i Std. Devlstlon m
Fig. 9. Changes in angulation of mandibular incisors for rigid fixation group (6,) and for intermaxillary fixation group (B).

152 Dozmza, Kztftinec, and Moshiri Am. J. Orzhod. Dentofac. Orthop. August 1991
| 3 O
o 2 C
1
i °
- 1 | o --2 E 0
6
5
4
- 4
--5
- 6 i
FACIAL CONTOUR ANGLE CHANGES Group 1 - Rlgld Flx~don
!1 I I I I I I I
A T1 -T2 1"2-i"3 T3-T4 T1 -T4
~.,°oo I Std. Deviation m
| 0
0 c
J J 0
8 ! 8
5 -
4-
3-
2-
I
-1 i - 2 -
- 3 -
--6
- 7
- 8
FACIAL CONTOUR ANGLE Croup 2 - Interma~llo~ Fixation
l
CHANGES
i I ! ! | ! | i
D 1"I -T2 TZ-T3 T3 -'['4 TI -T4.
L[,~cn 1 Std. D~latlon
Fig. I0. Changes in facial contour angle for rigid fixation group (A) and for intermaxiHary fixation group (8).

Volume 100 Number 2
DISCUSSION
In patients treated surgically for mandibular retro- gnathism, several investigators documented relapse by composite serial cephalometric tracings. According to many studies, relapse rates varied from 10% to more than 75%, with an average relapse of about 30% of the surgical correction .7,28 The greater percentage of relapse occurred in the early postsurgical period, corresponding to pur T2-T3 period. The reported patients usually un- derwent intraosseous wiring, plus intermaxillary fixa- tion with a splint for a period of 6 to 8 weeks.
Recently, two studies gave reports on postsurgi- cal stability in patients stabilized by means of cortical compression screws or bone plates (rigid fixation), zg-~° These studies reported good'skeletal stability. When a group of patients with rigid skeletal fixation was com- pared with a group with intermaxillary fixation, the skeletal changes of.the former (rigid fixation) were re- ported to be smaller than those seen in the latter group. 3~
In this study skeletal relapse was found to be a frequent and yet unpredictable sequela of the surgical correction. The results indicated that the duration, ex- tent, and direction of skeletal changes were unpredict- able, with large individual variations in response to surgical treatment without an apparent close correlation with the severity of the original malocclusion.
Our results support many previous reports that have found skeletal instability to be an important factor in the majority of treated patients.Z8"32-35 No significant dif- ference in the relapse rates between the two groups was found in either the short-term or the long-term follow- up. Of significant and noteworthy magnitude is the total relapse measured at pogonion (31.4% for the rigid fix- ation group and 23% for the intermaxillary fixation group), which corresponds well with that reported in earlier studies. Comparisons of composite serial ceph- alometric tracings show that skeletal changes occurred for most patients during the first 4 to 8 weeks after surgery.
The surgical lengthening of the mandible in both groups was achieved primarily by an anteroinferior ad- vancement of the distal mandibular segment. 36 This re- suited in an increase in the anterior facial height that was sustained postsurgicalty. Confirming previous stud- ies, a surgical increase in anterior facial height occurred in almost all cases, and a modest net long-term gain was observed.
The posterior facial height was somewhat reduced postoperatively in both groups and remained decreased throughout fixation. Empirical clinical experience in- dicates that surgical increase in posterior vertical di- mensions is unstable and correlates with relapse. 37,3s
Stability after mandibular advancement surgery 153
For this reason, results of our study are positive and indicative of less relapse than observed in earlier re- porl~.
The preoperative mandibular plane angle as a single parameter of facial form is not a reliable predictor of tile amount of p0stsurgical relapse, z,39 It has been spec- ulated that some degree of relapse is observed because of the triangulation phenomenon. If and when this phe- nomenon occurs, the observed relapse should correlate highly with a decreased mandibular plane angle. That did not appear to be the case in this study. In our study, the rigid fixation group showed a weak association be- tween the mandibular plane angle and the total relapse; the correlation between the two vhriables was slightly higher in the wire fixation group.
Although some investigators deny any association between preoperative mandibular plane angle and skel- etal relapse, a number of studies found less relapse in patients with low mandibular plane angles? °'z8 A suggested explanation, which is different from the de- scribed triangulation after surgery, is that the conver- gent skeletal pattern freqtiently was associated with a strong vertical component of masticatory muscle func- tion in support of the new mandibular position, with the posteriorly directed tensor forces unable to effect a large change.
Changes in the maxillary and mandibular dentition seen postoperatively in all patients were greater than skeletal differences. Compensatory changes in the den- tition are said to occur as the skeletal equilibrium is being reestablished. :°.3s In this sample, both the max- illary and the mandibular incisors showed an acceptable proclination, on average, at the time of fixation. How- ever, wide individual variations were observed.
SUMMARY AND CONCLUSIONS
A sample of 32 patients with significant retrognath- ism was evaluated after mandibular advancement sur- gery. Sixteen patients were stabilized by means of bi- cortical bone screws (rigid fixation), and 16 patients had standardized intraosseous wiring of the bony seg- ments. Analysis of longitudinal cephalometric mea- surements demonstrated skeletal and dental adaptations to the altered functional equilibrium. Multiple param- eters were analyzed to determine factors contributing to postoperative changes and to compare the results between the two groups. Findings from this study can be summarized as follows:
1. Skeletal changes were seen after surgery in both groups, resulting in some loss of the initial mandibular advancement. The percentages of short-term and long-term relapse between the

154 Dottma, Kuftinec, and Moshiri Am. J. Orthod. Dentofac. Orthop. August 1991
groups were not found to be s ignif icantly dif-
ferent . 2. The magni tude o f advancement was found to
be a factor in postsurgical mandibular stability
fn both groups. As the magni tude o f advance-
ment increased, there was a tendency for the fiet
amount o f relapse to increase.
3. A weak associat ion be tween the preopera t ive
mandibular plane angle and the total amount o f
relapse was found in the rigid fixation group.
Patients wi th h igh mandibular plane angles
s eemed to show m o r e relapse than patients with
e i ther normal or low angles.
4. Al tera t ions o f the relat ionships be tween max-
i l lary and n~andibular segments occurred post-
opera t ive ly as a result o f adaptat ion to the func-
t ional equ i l ib r ium and or thodont ic mechano-
therapy.
5. No statist ically significant d i f ferences be tween
the rigid fixation and intermaxi l lary fixation
groups were found in the skeletal and den-
tal changes obse rved at the four t ime intervals
studied.
We thank Dr. Kenneth Rotskoff of St. Louis, Missouri, for graciously allowing us to peruse his cases for this study.
REFERENCES 1. Kiyak HA, West RA, Hohl T, McNeil RW. The psychological
impact of orth~nathic surgery: a nine-month follow-up. AM J ORTHOD 1982;81:404-12.
2. Obwegeser H. The indications for surgical correction of man- dibular deformity by the sagittal splitting technique. Br J Oral Surg 1964;1:i57-66.
3. Dal Pont G. Retromolar osteotomy for the correction of prog- nathism. J Oral Surg 1961;26:249-52.
4. Kundert M, Hadjianghelou O. Condylar displacement after sag- ittal splitting of the mandibular rami. J Oral Maxillofac Surg 1980;8:278-97.
5. Booth DF. Control of the proximal segment by lower border wiring in the sagittal split osteotomy. J Oral Maxillofae Surg 1981;9:126-8.
6. Ellis E, Gallo WJ. Relapse following mandibular advancement with dental plus skeletal maxillomandibular fixation. J Oral Max- illofac Surg 1986;44:509-15.
7. Epker BN, Wessberg GA. Mechanisms of early skeletal relapse following surgical advancement of the mandible. Br J Oral Surg 1982;20:175-82.
8. Jeter TS, Van Sickels JE, Dolwick MF. Modified techniques for internal fixation of sagittal ramus osteotomies. J Oral Maxillofac Surg 1984;42:270-2.
9. Fish LC, Epker BN. Prevention of relapse in surgical-orthodontic treatment. Part I. Mandibular procedures. J Clin Orthod 1986; 20:826-41.
10. Kohn MW. Analysis of relapse after mandibular advancement surgery. J Oral Surg 1978;36:676-84.
!1. Martis CS. Complications after mandibular sagittal split oste- otomy. J Oral Maxillofac Surg 1987;42:101-7.
12. Van Sickels JE, Flanary CM. Stability associated with mandib- ular advancement treatment by rigid osseous fixation. J Oral Maxillofac Surg 1985;43:338-41.
13. Ellis E, Carlson DS. Stability two years after mandibular ad- vancement with and without suprahyoid myotomy: an experi- mental study. J Oral Maxillofac Surg 1983;41:426-37.
14. Gingrass DJ, Messer El. Rigid noncompressive pin fixation of the mandibular sagittal split osteotomy. J Oral Maxillofac Surg 1986;44:413-6.
15. Greebe FC, Tuinzing DB. Mandibular advancement procedures: predictable stability and relapse. Oral Surg Oral Med Oral Pathol 1984;57: ! 3-6.
16. Paulus GW, Steinhauser EW. A comparative study of wire os- teosynthesis versus bone screws in the treatment of mandibular prognathism. Oral Surg Oral Med Oral Pathol 1982;54:2-6.
17. Reitzik M, Schoorl W. Bone repair in themandible: a histologie and biometric comparison between rigid and semi-rigid fixation. J Oral Maxillofac Surg 1983;41:215-8.
18. Epker BN. Modifications in the sagittal osteotomy of the man- dible. J Oral Surg 1977;35:157-9.
19. Epker BN, Wolford LM, Fish LC. Mandibular deficiency syn- drome: surgical considerations for mandibular advancement. Oral Surg Oral Med Oral Pathol 1978;45:349-63.
20. Thomas PM, Tucker MR, Prewin JR, Proffit WR. Early skele- tal and dental changes following mandibular advancement and rigid internal fixation. Int J Adult Orthod Orth~n Surg 1986; 1:171-8.
21. Van Sickels JE, Larsen AJ, Thrash WJ. Relapse after rigid fix- ation of mandibular advancement, J Oral Maxillofac Surg 1986; 44:698-702.
22. lye J, McNeil RW, ",,Vest RA. Mandibular advancement: skeletal and dental changes during fixation. J Oral Surg 1977;35:881-6.
23. Moshiri F. Orthognathie and craniofacial surgical diagnosis and treatment planning: a visual approach. J Clin Orthod 1982;16:37- 59.
24. Behrman SJ. Complications of sagittal osteotomy of the man- dibular ramus. J Oral Surg 1972;30:554-61.
25. Lake SL, McNeil RW, Little RM, West RA. Surgical mandibular advancement: a cephalometric analysis of treatment response. AM J ORTHOD 1981;80:376-94.
26. Singer RS, Bays RA. A comparison between superior and in- ferior border wiring techniques in sagittal split ramus osteotomy. J Oral Maxillofac Surg 1985;43:321-37.
27. White RP, Proffit WR, Crammer JR, Kohn MW. A study of facial height changes after mandibular osteotomy in 46 patients. J Oral Surg 1971;29:858-61.
28. McDonnell JP, McNeil RW, \Vest RA. Advancement genio- plasty: a retrospective cephalometric analysis of osseous and soft tissue changes. J Oral Surg 1977;35:640-7.
29. Reitzik M. Mandibular advancement surgery: stability following a modified fixation technique. J Oral Surg 1980;38:893-7.
30. Souyris F. Sagittal splitting and bicortical screw fixation of the ascending ramus. J Oral Maxillofac Surg 1978;6:198-203.
31. Schendel SA, Epker BN. Results after mandibular advancement surgery: an analysis of 87 cases. J Oral Surg 1980;38:265-82.
32. Fox GL, Tilson HB. Mandibular retrognathia: a review of lit- erature and selected cases. J Oral Surg 1976;34:53-61.
33. Freihofer HP, Petresevic D. Late results after advancing the man- dible by sagittal splitting of the rami. J Oral Maxillofac Surg 1975;3:250-7.
34. Guernsey LH. Stability of treatment results in Class II maloc- clusion corrected by full mandibular advancement surgery. J Oral Surg 1974;37:668-87.

Volume tO0 Stability after mandibular advancement surge D, 155 Number 2
35. Worms FW, Speidel TM, Bevis RR, Waite DE. Post-treatment stability and esthetics of orthognathic surgery. Angle Orthod 1980;50:251-73.
36. Stoelinga PJW, Leenen RJ. Class It anomalies: a coordinated approach to the management of skeletal, dental, and soft tissue problems. J Oral Surg 1981;39:827-41.
37. Poulton DR, Ware WH. Increase in mandibular and chin pro- jection with orthognathic surgery. AM J ORrnOD 1985;87:363- 76.
38. Proffit WR, White RP. Treatment of severe malocclusions by correlated orthodontic-surgical procedures. Angle Orthod 1970; 40:1-10.
39. McNeil RW, West RA. Severe mandibular retrognathism: ortho- dontic versus surgical orthodontic treatment. AM J ORxrtoo 1977; 72:176-82.
Reprint requests to: Dr. M. M. Kuftinec Department of Growth and Special Care School of Dentistry University of Louisville Louisville, KY 40292
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of the AMERICAN JOURNAL OF ORTHODONTICS AND DENTO- FACIAL ORTHOPEDICS arc available to subscribers (only) for the 1991 issues from the Publisher, at a cost of $48.00 ($62.36 Canada and $59.00 inte.rnational) for Vol. 99 (January-June) and Vol. 100 (July-December). Shipping charges are in- cluded. Each bound volume contains a subject and author index and all advertising is removed. Copies are shipped within 60 days after publication o f the last issue in the volume. The binding is durable buckram with the journal name, volume number, and year stamped in gold on the spine. Payment must accompany all orders. Contact M o s b y - Y e a r Book, Inc. , Circulation Department, 11830 Westline Industrial Drive, St. Louis, MO 63146-3318, USA; telephone (800)325-4177, ext. 4351.
Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular Journal subscription.