Embed Size (px)
Citation preview


Beginning a JourneyI have been immersed in trying to develop a brain stimulationmethod in the central thalamus to improve cognitive function. I can tell a sequential story of when segments of the work werepublished, but the research has had an ongoing life of parallelevents. The same set of problems has taken me from my initialfascination as an undergraduate researcher through medicalschool research, my residency—which crystallized my ideas afterobserving patients—and the stated long-term goal in the firstNational Institutes of Health (NIH) grant I received, to my work to date.
As an undergraduate, I did historical research at the MontrealNeurological Institute, working with the collected archives of neurosurgeon Wilder Penfield. The institute’s director recognizedmy interest and said, “Not a lot of people are interested in con-sciousness any more, but there is one neurologist who is stilldoing it. His name is Fred Plum, and he’s at Cornell University.”That stuck in my mind. I came to Cornell, and on the first day of medical school at the white coat ceremony, I met Fred Plum(professor emeritus, Neurology and Neuroscience). He has been a mentor ever since.
Consciousness in the Brain—Acquiring Skill Sets for the JourneyHow do some areas of the central part of the upper brain stemand the thalamus participate in establishing and maintaining consciousness in the brain? It is a compelling question. After my third year of medical school at Cornell, I received a HowardHughes grant, and I focused on absence seizures and the organi-zational aspects of consciousness in the brain. How can we learnabout the circuit mechanisms underlying this type of seizure? Iwanted to obtain a new set of skills—to understand how to domathematical modeling of electrical signals and to think aboutwhat the relationship was to consciousness. I went to work onapplied mathematics in the lab of Jonathan Victor, now the FredPlum Professor of Neurology.
After my internship in Chicago, I returned to Cornell to do myresidency, during which I figured out a way to take the model Ihad been pursuing for seizure problems and turn it into a deepbrain stimulation question: how might deep brain stimulationmodulate perceptual function?
I began writing grant proposals to fund the research that could bethe foundation for setting up models to develop new therapeutics.Fred Plum, however, made another recommendation, saying, “This
A CompellingQuestion Drivesa Long-TermPassionHow Do We Develop a Brain Stimulation Method to ImproveCognitive Function in Patients after Serious Brain Injury?NICHOLAS D. SCHIFF, NEUROLOGY AND NEUROSCIENCE
Photos in the article: Patricia Kuharic unless otherwise noted

40
is great, but I don’t want you to work onlyin the lab. I have another project I’m tryingto get started. I’m working with RodolfoLlinás downtown at New York University(NYU) with magneoencephalographic tech-nology, and I want to restart a programthat we worked on in the mid-’80s. I wantyou to come and work with me on that, as well.”
Plum and I evaluated patients in nursingfacilities and other places throughout thetri-state area. It was one of the most inter-esting periods in my training.
Tough on teaching and pursuing funding,Plum said, “You must know how you’regetting funded. You should write your NIHgrant as soon as you have preliminarydata.” I wrote at least six grants my firstyear as a senior resident. As I finished myresidency, I was funded with grants and theconceptualizations of two concurrent post-docs. Working with Victor, I got preliminarydata and wrote my first NIH grant sevenmonths out of residency. And I got it! Itwas a training grant that set me on a path.
“Words without Mind”We went back and examined patients inthe chronic vegetative state. We reestab-lished an earlier benchmark created inPlum’s lab—the first evidence that the vegetative brain functioned at such a lowlevel, 30 percent of normal function, andthat it was apparently anaesthetized basedon a resting metabolism—and correlated it with the new technologies. We worked,particularly with Llinás at NYU using mag-netoencephalography, technology thatmeasures magnetic signals in the brain. As Plum and Llinás joined forces, I becamethe point person for the study.
We eventually enrolled patients in thetrial. The first patient we studied had beencoming to the clinic every day for about20 years. The patient was known to be in
a vegetative state, but every now and thenwould say single words. I said, “Wait asecond, that can’t happen. That’s not theway it works—you don’t say words ifyou’re in a vegetative state!” We examinedthe patient, got the history, and talked tothe family. They were very clear—thispatient showed absolutely no evidence ofawareness of anybody. But every now and
then the patient would blurt out a singleword, usually an expletive in one of twolanguages, and it did not appear to be relatedto anything.
It was a remarkable case, an unusual storyof a patient who had an abnormality ofblood vessels in the center of the brain.Over a two- to three-year period, the bloodclot had continuously ruptured and destroyedalmost the entire brain. The parts of the brainthat it had not destroyed were like a littlemodel of the human language system—islands that preserved the expressivelanguage, cortical regions, the underlyingparts of the basal ganglia, and some verysmall part of the thalamus that we couldnot identify anatomically or metabolically.We knew these parts were still there becausewe could identify them using magnetoen-cephalography, which showed us that asignal was going to the right part of thebrain in the auditory regions.
This became our first insight that had notbeen established in the literature into theexistence of modular preservation, islandsof functions—even where there is almost nobrain remaining—that could produce a clini-cally visible feature, a fragment of behavior.In this case the fragment of behavior was aword. A sentence, not a word, is the unit ofmeaning in language. A word could be likea reflex, given that one can speak so muchfaster than one can think. We concluded ina paper—“Words without Mind,” by RodolfoLlinás, Urs Ribary, Fred Plum, and me—thatwhat we were looking at was a modular
If we knew a patient was able to talk every nowand then, perhaps we could get the patient intothat state and hold the brain in that state. Butcould we get the brain to function in that state?
Fascinating!
This patient showed absolutely no evidenceof awareness of anybody. But every now andthen the patient would blurt out a singleword, usually an expletive in one of two lan-guages, and it did not appear to be relatedto anything.
A sentence, not a word, is the unit of meaningin language. A word could be like a reflex,given that one can speak so much fasterthan one can think.
We found that turning on the brain stimulator,at first gradually and then effectively, restoredspoken language, the ability to eat, and theability to control muscles and to move.
We can take a few cases and go through thisprocess thoroughly … to understand how thepatient’s brain changes, how their behaviorchanges, how the patient changes, and howthe family changes.
£
£
£
£
Research in Progress


University Photography

circuit that, lacking motor fixed-action patterns, produced words almost like areflex. We saw how the first level up fromthe vegetative state with no evidence ofcortical activity might look.
On the TrailAs we studied other patients, we found moreexamples like the word reflex case, butnothing as dramatic. A concordance amongthe measurements we made with PET scan-ners, magnetoencephalography, and structuralimaging gave us a systematic way to studyit. Brains can be wiped out or almost wipedout. We began to see that there might befragments of behavior attached to them,which led to another question: what aboutthe many people who were not in the vege-tative state, but their level of functionranged from barely doing anything to beingconversant? And this led me to the brainstimulation work.
If we were to target patients for brain stim-ulation, these were the kinds of patients wemight be able to stabilize in their best levelof function. If we knew a patient was ableto talk every now and then, perhaps wecould get the patient into that state andhold the brain in that state. But could weget the brain to function in that state?
Play It Forward, Play It Backward The first study I conducted after the vegeta-tive work was to look at two patients withminimal levels of behavior. These patientswere not in the vegetative state, but theycould do no more than follow a command
inconsistently; we could not communicatewith them. We took them through the protocol of our previous study, but addeda study of functional magnetic resonanceimaging in collaboration with Joy Hirsch(then at Memorial Sloan Kettering, now at Columbia University), using a paradigmthe Hirsch lab had developed for anesthetizedbabies. We played spoken language—narrativesread by relatives the patients knew well. Thenwe turned around the narratives, recordedin digital audio, backwards in time so thatthey could not be understood.
Data showed that normal subjects activatednot only the same areas of the brain toboth stimuli (forward and backward) whenthey listened to each version, but they acti-vated these areas more strongly when theywere presented with the stimulus they couldnot understand—as if they were listeningmore carefully in order to understand. Thepatients activated the same auditory andlanguage areas. In one case we saw almostthe entire language system; it looked verynormal. But when we turned the narrativearound in time, activity shut down dramati-cally compared to the normal subjects. Itwas as if the patients alerted to the familiarvoice and engaged with it. We could notjudge that from the scan, but they certainlyactivated this network in both halves of thebrain and in all the relevant areas of the brain.
One of these patients became the first brainstimulation subject four years later. Westudied this patient because the patient fitthe profile—injuries to the central structures
43
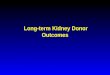
We interpreted our results as evidence thatstructural reconnection of existing cells overtime in a severely injured brain is possible.
Longitudinal measurements of regional fractional anisotropy over an 18-month interval following late recovery from MCS
Illustration: Schiff, Ribary, Plum, and Llinas, “Words without Mind” Journal of Cognitive Neuroscience 1999, 11:6; 650-656
Research in Progress

44
of the brain and inconsistent responses. Weobtained data that showed a robust languagesystem in this brain, even though it did notseem to be working properly. Wow! Whathad been occurring in the brain with thesemeasurements was not transparent, and thefindings raised more questions than theyanswered.
A Miracle Man and Cutting-Edge Research at CornellAs the work with that patient continued toevolve, we had an opportunity to study acase that came to public attention in 2003.A man in Arkansas, Terry Wallis, began tospeak fluently on his own for the first timein 19 years. One day his mother walkedinto the nursing home, and the nurse saidas she did every day, “Who’s that?” And hesaid, “Mom.” Everyone was stunned—he hadbeen silent for 19 years.
About eight months after his spontaneousrecovery, which was widely reported in theworld press, we got a chance to study him.We did the whole series of imaging studies—PET studies, EEG (electroencephalography),and we added a new study.
At the time, Henning Voss, a MR physicistat Cornell, had been working on diffusiontensor imaging, a modality of MRI. Diffusiontensor imaging enables a measurement ofhow water molecules move in the appliedmagnetic field. Instead of pursuing theinterpretive aspect of this technique thatinvolves using algorithms to create picturesof the fiber connections in the brain, wefocused on the actual MRI signal, whichcomes in a three-dimensional volume. Wequantitatively assessed the measured watermovement in three principal directions foreach volume. This allowed us a way ofdoing very precise quantitative structuralbrain assessments. We were able to assessthe extent of the injury in the man whorecovered after 19 years.
We were able to show unambiguously that thepatient’s brain was overwhelmingly damagedwhen we qualitatively and quantitativelycompared his brain to normal subjects. Hehad the worst grade of diffuse axonal injury.When Voss and I sent the findings to bepublished, we received comments that said,“This is real interesting, but we want to see
another patient to determine whether or notthis might occur in other patients.” When wepublished the study, it made the front page ofthe New York Times (as did our fMRI study).
The Miracle Man Improves FurtherAround the time we brought in anotherpatient to study who also had very unusualchanges many years after severe braininjury, we were also able to study Wallis
again. He had improved. He was gainingmore control of his articulation and speech.His ability to form new memory, which hadbeen nearly absent, was beginning to showchanges. He was also starting to move hislower limbs, which we thought would bepermanently paralyzed. When we repeatedhis images, we saw that the areas in the brainthat had shown increased connection werestill changing while measurements in mostother areas in his brain were stable. We alsosaw new changes in another area related toa motor control system—a quantitative result.We interpreted our results as evidence thatstructural reconnection of existing cells overtime in a severely injured brain is possible.
At the same time of our finding, a prospec-tive study appeared in the journal Brain. Itincluded 30 patients with severe brain injurywho were studied over a one-year periodshowing very similar results to ours.Researchers discovered that in a cohort of these patients who were improving,brain areas showed recovery of the samediffusion tensor imaging measures, and somepatients, like Wallis, actually recovered tovalues above normal.
A Story of Parallel ProjectsI worked with ideas about how these structures in the center of the brain mightbe doing their jobs. History told us thatthese cells activate during wakefulness andhad something to do with consciousness inturning the brain on. But what were theseareas of the brain doing during the time
they were most active? They must be doingsomething. I searched the literature forcharacterizations of the cells in this part ofthe brain to give us insight into variationsin their activities during a wakeful state. Ifound two fascinating papers that had beendone in the early 1980s showing that thesecells in the part of the brain associated withactivation and arousal played a role in eyemovements.
Keith Purpura, a visual neurophysiologist at Cornell, had been working on how visualinformation was partitioned and the role ofthe eye movement as a signal to the visualcortex. Purpura and I began a discussionthat nearly immediately led to a publishedtheoretical paper, which became the kernelof my second NIH application—to developan animal model to test our theory.
At the same time, I worked with Plum todevelop a program where we could do brainstimulation in humans. I also worked withAli Rezai, who had returned to New Yorkafter a fellowship in brain stimulation andwas set to establish the brain stimulationprogram at the hospital for joint disease inthe Manhattan veterans administration. Oureffort to get a VA grant to do brain stimula-tion in 1998 began a seven-year process ofgrant rejections, with split reviews rangingfrom “the best proposal I have ever read” to“deep brain stimulation would never play arole in dramatic brain injury.” But the workof putting together ideas for grants led to amore precise formulation about how to setup a strategy for doing the brain stimulation.
Back in 1995 when we could not identifya source of funding to do the work, I hadthought about the companies that madethe brain stimulation units and contactedthe Medtronic Corporation. I was warned,however, to get a nondisclosure agreement.So, I worked with CRF (now the CornellCenter for Technology, Enterprise, andCommercialization, or CCTEC) for a year
We licensed this portfolio into a startupcompany, called intElect Medical Inc., whichis partly owned by Cornell and mostly ownedby the Cleveland Clinic.
Research in Progress

and a half and was asked by CRF to write adisclosure to protect the intellectual property(IP). Cornell applied in 1997 for a patentissued in 1999.
In 1997 I had begun a collaboration withJoseph Fins, Medicine/Public Health/Ethics,which was incredibly important as werecast our approach with a focus on whereit would be most ethical to apply brainstimulation. The team—Plum, Rezai, Victor,Purpura, Fins, and I—physically went tothe NIH to try to get funding for both thebasic and clinical work. After long meet-ings with the program officer and, later,rejected grant resubmissions, the programofficer finally said, “Well, you just can’tsubmit this grant until you do it.”
During the same time, the director of theNIH National Institute for Child Health andHuman Development, which has its ownsubcommittee on brain injury, contactedme and said, “We have a request for grantsgoing out, but it disallows surgical costs.However, you could write a planning grant.”We got an easily fundable score for theplanning grant, but the same grant with thesurgical budget submitted to the traditionalreview panel had received an insanely high(poor) score. The only way to do the surgicalwork, which brings us to 2002–3, was tofind a way to capitalize it ourselves.
Licensing the IPIn 2003 Cornell began negotiations withthe Cleveland Clinic, which was foundinga company around the technology they haddeveloped for brain stimulation tools, meth-ods, and systems. They were interested inour patent portfolio, which now included aseries of patents. We licensed this portfoliointo a startup company, called intElectMedical Inc., which is partly owned byCornell and mostly owned by the ClevelandClinic. The Cleveland Clinic used gap fundingto develop their own technology. Cornellagreed to license these patents and principlesto the Cleveland Clinic, and the ClevelandClinic put up the seed capital to do the firstsurgery. This is how we were able to start thetrial. Cornell and Cleveland then partneredwith the JFK Johnson Rehabilitation Centerand Joseph Giacino, a neuropsychologistand expert in quantitative behavioral
assessments of patients with limited rangesof behavior.
How the Brain Stimulation Trial WorkedFor the study, I wanted to get the patientwith inconsistent eye-movement commu-nication and language responsive networksin the brain we had studied in 2001 (pub-lished in the 2005 paper). The patient hadbeen in a nursing home several years priorto the approval of the study. When webrought the patient back to JFK JohnsonRehabilitation Center, which had become thesite for the trial, the patient was measuredto be in the same condition as four yearsearlier, and therefore fit the profile for thestudy. There was a four-month period ofreentry into rehabilitation, getting healthyand recovering from various problems, andthen off to surgery.
We had a two-month period when the brainstimulators were not on. We compared thebehavioral data of the on and off states.We had a five-month period of adjustmentof the deep brain stimulation, during whichmany things improved, and a six-monthperiod in a trial in which every 30 daysthe patient was on and off the stimulationand blinded evaluations were obtained.Over this period of 11 months when thepatient was exposed to brain stimulation,compared to the earlier six months ofmeasurements when the patient was notexposed to brain stimulation, we foundthat turning on the brain stimulator, atfirst gradually and then effectively, restoredspoken language, the ability to eat, andthe ability to control muscles and to move.
What Is a Brain Stimulator?A brain stimulator is like a cardiac pace-maker—an electrode that goes into the braintissue and delivers an electrical current. Itturns on and off, and we in this particulartrial turned it on and off at 100 cycles persecond (hertz). One of the reasons we didthis is because my collaborator, Dan Hererra,Psychiatry, developed a study in rodents onbrain stimulation looking at the effects ofgene expression and behavior. We found thatif we stimulated this part of the thalamusat 100 hertz, memory function in normalrats improved when we turned on thestimulator.
45
Years as Cornell faculty11
Came to Cornell fromStanford University
Favorite spot on campusA seven-block radius around WeillCornell Medical College in New York City
Cornell’s research distinctionCollaborative environment
Cornell’s trademarkA legacy of unique talent
I am alsoA hobbyist dropout
About Schiff
Back row: (l. to r.) Keith Purpura PhD, Neurology andNeuroscience; Daniel Herrera MD/PhD, Psychiatry;Renee Kahn RN, Nursing Staff Citigroup BiomedicalImaging Center; Jennifer Hersh MA, Public Health; Erik Kobylarz MD/ PhD, Neurology and Neuroscience
Front row: Stanley Goldsmith MD, Nuclear Medicine;Schiff; Joseph Fins MD, Medicine/Public Health/MedicalEthics; Shankar Vallabhajosula PhD, Nuclear Medicine


Now That We Know We Can Actually Do This …We have a lot of work to do. We and hundreds of other people could work onthis for at least the rest of my career or alifetime—figuring out the details will take a long time. How much of the how andthe why of brain stimulation do we know?We have increasingly better ideas about howit works. And the “whys” that we proposemake sense: the geometry of the cell con-nections to and from the area we stimulatemakes these cells vulnerable to any processthat causes a lot of neuronal death in thebrain. Their main anatomical specializationis that they are connected to very wide areasof the brain, and they have an importantfunctional capacity to maintain activitythat allows us to hold a behavioral set—tofocus attention, allocate attention over time,or keep things in our working memory.
These neurons are the most vulnerable tomultifocal injury. Part of what happens aftera severe injury is that, although these cellsmay continue to play a key role in main-taining these functions, they do it poorly.This is in part why people with severe braininjury are cognitively slow. They have prob-lems being attentive, remembering things,and acting in the world and rememberingwhat they are doing. At this stage of thetechnology, we put electrodes in the thala-mus, turn them on, and leave them on. Thebrain cannot learn anything intrinsicallyfrom the signal we give it. But it can over-ride the output of the cells so that they keeptarget areas in different parts of the brainactive enough to better maintain theremaining processes that allow memory,attention, and the ability to sustain a task.This is how we think it works.
It turns out that, if we keep the brain stim-ulator on for a while, even if we turn it off,the person does not go back to the previousstate. Changes are occurring in the brainthat are like learning and memory, like thenatural recovery process associated withthis. The process to figure out the biologyof this aspect of our findings will be long.When we think about how this will workout as a scientifically based method in thefuture, it will be not only about electricalstimulation, but also about the biology ofthe response.
Next DirectionsWhat’s next? We have two major directions:one is to understand more and in finer detailwhy the brain stimulation does what it does.We can work with the tools we have, butwe also need to develop new tools. Wewant to know better how to assay circuitresponses. Victor is returning to do a math-ematical analysis of the EEG, and we havegotten a grant together. Part of the grant
will develop a center—at Rockefeller andCornell—for the study of long-term recovery.Fins and I will codirect the center and looknot just at the scientific aspect of the recov-ery of consciousness, but also at needs of thefamilies and patients and potential goals.
We are setting up a project to study long-term recovery following severe injury inwhich we look at the scientific biomarkersaiming to understand the circuit mechanismsand how the brain evolves its recovery pat-tern. Very importantly, we try to understandcarefully what happens as patients recoverand the impact on their caregivers and families. These are very tough problems.Sometimes we will find patients who makeamazing recoveries, and everyone is grati-fied by it. Most of the time, we will findin-between cases. We need to understandthe goals of care. What is achievable? Whatis not achievable? How do we communicateinformation? How do we communicateuncertainty? How do we help guide people,and how do we learn from their experiences?
Fins and his research staff interview andcompile data on the families of our studysubjects. We hope to have a routine wherewe can take a few cases and go throughthis process thoroughly day by day, monthby month, over a year’s time to understandhow the patient’s brain changes, how theirbehavior changes, how the patient changes,and how the family changes. We will build
a comprehensive database for understandinghow to handle this difficult area of medicine.
Fallen HobbiesI have hobbies that I have not been able todo for a while, but right now, I am raisingmy two children. Running, karate, andreading outside my work are among myfallen hobbies. I have little time for anythingexcept work and family.
The Last Word
Only a Few Special PlacesTo develop insights into human problemspresented by disease, to understand theirmechanisms, or to develop new treatmentsare the top three goals one could have as abiomedical scientist. To do this kind of workrequires a very special environment. Theword translational is thrown around a lot,but it is not easy to achieve. Having a top-flight academic medical center in a citywith one of the largest populations in theworld and access to science and medicinewith ease is rare. And because we do sys-tems science, which combines biology withimaging research, theoretical research,mathematics, and physics, vast opportunitiesfor collaborative research with the IthacaCornell faculty are yet to be realized.
For more information:E-mail: [email protected]
47
To develop insights into human problems presented by disease, to understand theirmechanisms, or to develop new treatmentsare the top three goals one could have as a biomedical scientist.
Research in Progress