Embed Size (px)
Citation preview

HFMA Dixie
February 19th
3:30pm ET
A Crash Course in Cost Accounting and Cost Reduction
Dan Michelson Chief Executive Officer
Strata Decision Technology
Tushar PandeyDirector of Consulting Services, Decision Support
Strata Decision Technology

Today’s TopicsSix quick “lessons” in our crash course
1. Why do we need Cost Accounting?
2. How does Cost Accounting work?
3. What Cost Buckets should we use and how should we allocate overhead?
4. What Costing Methodologies should we use?
5. How is Advanced Cost Accounting different?
6. How can we leverage cost data to take action and drive out costs?
©2015 Strata Decision Technology

Historic Announcement…
NewsFOR IMMEDIATE RELEASEJanuary 26, 2015 Contact: HHS Press Office
Better, Smarter, Healthier: In historic announcement, HHS sets clear goals and timeline for shifting Medicare reimbursements from volume to value
In a meeting with nearly two dozen leaders representing consumers, insurers, providers, and business leaders, Health and Human Services Secretary Sylvia M. Burwell today announced measurable goals and a timeline to move the Medicare program, and the health care system at large, toward paying providers based on the quality, rather than the quantity of care they give patients.
HHS has set a goal of tying 30 percent of traditional, or fee-for-service, Medicare payments to quality or value through alternative payment models, such as Accountable Care Organizations (ACOs) or bundled payment arrangements by the end of 2016, and tying 50 percent of payments to these models by the end of 2018. HHS also set a goal of tying 85 percent of all traditional Medicare payments to quality or value by 2016 and 90 percent by 2018 through programs such as the Hospital Value Based Purchasing and the Hospital Readmissions Reduction Programs. This is the first time in the history of the Medicare program that HHS has set explicit goals for alternative payment models and value-based payments.
% of payments
Program 2016 2018
Medicare payments to quality or value through alternative payment models, such
as Accountable Care Organizations (ACOs) or bundled payment arrangements
30% 50%
Traditional Medicare payments to quality or value via programs like
Hospital Value Based Purchasing and the Hospital Readmissions Reduction Programs
85% 90%
©2015 Strata Decision Technology

A Major Shift…
RCMREVENUE CYCLE
MANAGEMENT
MOMMARGIN & OUTCOMES
MANAGEMENT
2014 2017
% OF INSURED
COVERED BY
PAYMENT
APPROACH
LOW
HIGH
2015 2016
©2015 Strata Decision Technology
2018

The Financial Challenge
1 Centers for Medicare & Medicaid Services, Office of the Actuary, 2012 data2 Annual Cost of Waste in the US Healthcare System according to a 2012 CBO report3 HIMSS Innovation Survey 2013
BY THE NUMBERS
2.2%
Hospitals are struggling
The average operating margin for hospitals is
~2.2% (1/3 have negative operating margins)1,2
$700B
There is significant waste…and opportunity
Over $700B spent on healthcare annually is considered waste (overuse, misuse, variation,
inefficiency, harm)2
#1
Cost reduction has taken center stage
Finding cost reduction solutions has emerged as
the #1 priority for healthcare providers3
©2015 Strata Decision Technology

As revenue shrinks
and margins tighten,
providers have identified
cost reduction as
their #1 priority
Facing reimbursement pressure, hospitals must dramatically lower their cost structure and reduce waste while delivering outstanding care in order to remain viable.
1 HIMSS Innovation Survey (2013)
26%
40%
46%
51%
52%
54%
64%
65%
New Patient Acquisition
Service Expansion toNew Markets / Populations
Hospital ReadmissionReduction
Better Manage Risk andValue-Based Payments
Medical Error Reduction
Improve KnowledgeSharing & Management
Improve PatientSatisfaction
Cost Reduction
Hospitals and Health Systems Must Cut Costs to Survive
HIGHEST PRIORITY FOR HEALTHCARE PROVIDERS1
©2015 Strata Decision Technology

$330M
$220M
$40M
$200M
$1B
$300M
$150M
$100M
©2015 Strata Decision Technology
Everyone has a target…

Physicians are Ready to Engage in Driving Down Costs
Physicians play a key role in reducing healthcare costs. However, they don’t have access to cost data. Closing this gap represents one of the most significant opportunities to drive value in healthcare.
~20% Only 1 in 5 MDs could correctly estimate the cost for common
orthopedic devices
>80% Over 8 of 10 MDs would consider
cost as a key criteria in the selection of a medical device
PHYSICIANS AT SIX MAJOR HEALTHCARE SYSTEMS WERE ASKED TO ESTIMATE THE COST OF 13 COMMONLY USED ORTHOPEDIC DEVICES
(ESTIMATES WITHIN 20% OF ACTUAL COSTS WERE CONSIDERED CORRECT)1
Physicians don’t know… …but do care about cost
n =503 MDs at orthopedic departments at Duke, Harvard, University of Maryland, Mayo, University of Pennsylvania, Stanford, and Washington University
1Survey Finds Few Orthopedic Surgeons Know the Costs of the Devices They Implant, Health Affairs, January 2014.
©2015 Strata Decision Technology

Linking Clinical and Financial Outcomes Will be Critical
©2015 Strata Decision Technology

Source: Harvard Business Review, The Strategy That Will Fix Healthcare (October 2013)
The Absence of Accurate Cost Information…“Astounding”
“The absence of accurate cost information in health care is nothing short of astounding”
“The existing systems are wholly inadequate”
“Healthcare organizations are flying blind in deciding how to improve processes and redesign care”
“Understanding true costs will finally allow clinicians to work with administrators to improve the value of care”
Michael PorterProfessorHarvard Business School
SIGNIFICANT MARKET OPPORTUNITY FOR COST
ANALYTICS SOLUTIONS
While hospitals and health systems understand the need to dramatically cut their cost structure, they cannot make informed decisions due to a lack of information.
Less than 10% of health systems have an advanced cost accounting solution
10%
51%9%
30%
Advanced Decision Support Legacy Decision Support
Self-Developed No System
Decision Support Market Penetration
Source: HIMSS Analytics, Company Analysis
©2015 Strata Decision Technology

Today…in Michigan
©2015 Strata Decision Technology

How do you price…when you don’t know your cost?
©2015 Strata Decision Technology

“10 Reasons Hospitals are Shifting to Advanced Cost Accounting”
©2015 Strata Decision Technology
The Top10
Reasons
Hospitals are
Shifting
to Advanced
Cost
Accounting

10. To Understand True Margins
9. To Identify Opportunities to Reduce Cost
8. To Understand Total Cost of Care from
Both Inpatient and Outpatient Costs
7. To Bring Together Financial + Clinical
Data
6. To Integrate with Organization’s EHR,
ERP and EDW
“10 Reasons Hospitals are Shifting to Advanced Cost Accounting”
Source: Becker’s Hospital Review, 4-1-2014
5. To Integrate Cost Accounting with
Overall Financial Management
4. To Understand How to Price Right
3. To Run Costing Quickly/Frequently
2. To Improve Accuracy of Costing Data
1. To Make Cost Data More Actionable
via Dashboards
©2015 Strata Decision Technology

Six quick “lessons” in our crash course today
1. Why do we need Cost Accounting?
2. How does Cost Accounting work?
3. What Cost Buckets should we use and how should we allocate overhead?
4. What Costing Methodologies should we use?
5. How is Advanced Cost Accounting different?
6. How can we leverage our cost data to take action and drive out costs?
©2015 Strata Decision Technology

Payor/Financial Class
Patient Type
Service Line
Understanding Profitability
©2015 Strata Decision Technology

Making The Vision Reality…Enterprise Profitability
©2015 Strata Decision Technology

The Costing Process
Decision Support
EHR
ERP
EDW
Clean-up Data
Allocate overhead expenses
Allocate total expenses to activities
Attribute supply-chain costs
Allocate costs to patient encounters
Report
Clinical & Financial
©2015 Strata Decision Technology

1. Department Level Costing (Align GL to Revenue Data)
– Reclassification – moving/aligning direct dollar
– Overhead Allocation – allocating indirect dollars
2. Charge Level Costing (Assigning department expenses to charge codes/activities)
– Charge Allocation (RCC, RVU, CCR, % Markup, etc)
The Costing Process Cont.
©2015 Strata Decision Technology

Six quick “lessons” in our crash course today
1. Why do we need Cost Accounting?
2. How does Cost Accounting work?
3. What Cost Buckets should we use and how should we allocate overhead?
4. What costing methodologies should we use?
5. How is Advanced Cost Accounting different?
6. How can we leverage our cost data to take action and drive out costs?
©2015 Strata Decision Technology

Looking at Cost Types
Describes cost source and cost type
– Fixed: Not impacted by volumes (maintenance, utilities)
– Variable: Increases with Volume(supplies, salaries)
– Direct: Directly related to patient care (lab, ICU)
– Indirect: Indirectly related to patient care (IT, Finance)
©2015 Strata Decision Technology

Looking at Cost Components
©2015 Strata Decision Technology

Looking at Cost Components Cont.
• Categorization of expenses used in cost reporting and allocation– Recommendation: Align with income statement line items
– Recommendation: Typically between 10-20 cost components
• Cost components can contain indirect and direct dollars – Salaries and Wages (indirect and direct)
• Cost Component can also be specific to a cost type– Recommendation: Typically between 10-20 cost components
©2015 Strata Decision Technology

Sample Cost Buckets
Salaries• Physicians• Non Physician Medical
Practioners• RN - Patient Care• RN - Nonpatient Care• LPN• Allied Health Professional• Allied Health Technical• Management• Specialized Professionals• Clerical and Admin• Service and Support• Research
Other• Employee Benefits• Medical Supplies• Pharmaceutical Supplies• Other Supplies• Purchased Medical Services• Purchased Services - Other• Repairs and Maintenance• Utilities• Rent• Insurance• General• Depreciation and Amortization
©2015 Strata Decision Technology

Must-Have Statistics
• Can be used to allocate expenses rather than using manual percentages
– Helps to automate costing
– Can be updated monthly, quarterly, or yearly
- Recommendation: Find the right balance!
©2015 Strata Decision Technology

DIRECT METHOD SEQUENTIAL/STEP-DOWN METHOD SIMULTANEOUS/RECIPROCAL METHOD
Allocate Overhead Expenses
Increasing accuracy of costing results
Allocation of overhead expenses as indirect dollars to revenue department. Example: IS and Accounting
©2015 Strata Decision Technology

• Allocates overhead costs only to revenue generating cost centers
• No interaction between overhead cost centers prior to allocation
Advantages:• Simplistic costing model• Easy to use and maintain
Disadvantages:• Inaccurate costing results
DIRECT METHOD SEQUENTIAL/STEP-DOWN METHOD SIMULTANEOUS/RECIPROCAL METHOD
Overhead Methods - Compare and Contrast
• Allocates overhead costs one cost center at a time to remaining overhead and revenue generating cost centers in a cascading manner
• One-way interaction between overhead cost centers prior to allocation
Advantages:• Simplistic costing model• Easy to validate
Disadvantages:• Costing results not very precise
• Allocates overhead costs to revenue generating cost centers by fully recognizing the mutual services provided among all overhead cost centers
• Full two-way interaction between overhead cost centers prior to allocation
Advantages:• Precise costing results• Easy to maintain
Disadvantages:• More complex to understand and
validate
©2015 Strata Decision Technology
Increasing accuracy of costing results

©2015 Strata Decision Technology

Six quick “lessons” in our crash course today
1. Why do we need Cost Accounting?
2. How does Cost Accounting work?
3. What Cost Buckets should we use and how should we allocate overhead?
4. What Costing Methodologies should we use?
5. How is Advanced Cost Accounting different?
6. How can we leverage our cost data to take action and drive out costs?
©2015 Strata Decision Technology

What Costing Methodology Should You Use?
1. Standard Cost: ‘hard coded’ based on charge code
2. RCC: ratio of cost to charge
3. RVU: relative value unit
4. CCR: ratio of cost to charge at the test level (encounter level)
5. % Markup: reverse markup charge schedule (encounter level)
6. Supply Cost: acquisition cost (encounter level)
7. Activity Based Costing (ABC) – allocation to chargeable and non-chargeable activities
8. Time Driven Activity Based Costing (TDABC) – identify max capacity
©2015 Strata Decision Technology

Cost Accounting is Not One Thing (e.g. TD-ABC)
Private & Confidential ©2015 Strata Decision Technology
RELATIVE VALUE UNIT
(RVU)
ACCURATE
FLEXIBLE
COVERS MOST COST
TYPES
REQUIRES SOME
MAINTENANCE
SUPPLY/INVOICE
BASED
VERY ACCURATE
TRACKS PREFERENCES
TIMELY TRENDING OF
COSTS
REQUIRES ADDITIONAL
INTEGRATION
% MARKUPS
ALLOWS ACCURATE
COSTING OF BUNDLED
SUPPLIES
FOR SUPPLIES ONLY
DEPENDENT ON
ACCURACY OF CHARGES
AND MARKUP SCHEDULE
RCC
EASY TO UNDERSTAND
& MAINTAIN
ASSUMES COSTS ARE
PROPORTIONAL TO
CHARGES
OUTDATED
ABC
EASY TO UNDERSTAND
IN CLINICAL SETTINGS
COMPLEX TO
IMPLEMENT
TDABC
IDENTIFIES EFFICIENCY
BASED COST SAVINGS
VERY LABOR INTENSIVE
TO IMPLEMENT
APPLICABLE TO LABOR
ONLY

ChargeDirect Labor
Indirect Labor
PhysicianLabor
SuppliesAsset Cost
Contracted Services
Other
CHEST X-RAY
(2 VIEWS)
3 1 1 1 1 1
CHEST X-RAY
(4 OR MORE VIEWS)
4 1 1 1 1 1
HIP
(1 VIEW)
6 1 3 1 1 1
HIP
(2 VIEWS)
6 1 3 1 1 1
The RVU approach
• Determine RVU’s for each charge for each cost category
©2015 Strata Decision Technology

Every patient is different …so why is their cost the same?
PATIENT ACCOUNTING & MEDICAL RECORDS
DE
C
I
S
I
O
N
SU
P
P
O
R
T
PRACTICE MANAGEMENT
GENERAL LEDGER
& PAYROLL
Traditio
nal D
ata Eleme
nts
OR SUPPLIES/IMPLANT
COSTS FROM SURGICAL
SYSTEMS
©2015 Strata Decision Technology

Unit Charge Qty RVU AVERAGE COST RVU + AVERAGE COST
Hip Implant $8,500 1 200.0 $4,000 $4,200
OR Level 3 Per Minute $200 120 3.5 $12 $5,640
All Other Expenses $5,000
$14,840
The Impact of Advanced Methodologies
Variable LABOR
Expense
Variable SUPPLY
Expense
TOTAL Variable
Expense
Unit Charge Qty RCC RCC RCC
Hip Implant $8,500 1 $1,000 $3,000 $4,000
Hip Implant OR Time $9,600 1 $3,300 $1,500 $4,800
All Other Expenses $5,000
$13,800
Unit Charge Qty ABC ACQUISITION COST ABC + ACQSTN COST
Hip Implant - Uber Max $8,500 1 $400 $5,000 $5,400
OR Level 3 Per Minute $200 120 $50 $13 $7,560
All Other Expenses $5,000
$17,960Patient Level … More Accurate Cost of Care

Medicare Payment
Would You Grow This Service?
$13,800
$14,840
$15,200
-$2,760
$1,400
Variable Cost Per Case Margin
∆$1,040RCC Labor & Supplies
ABC + Supply Acquisition CostTRUE COST
$15,200$17,960
RVU + Average Supply Cost∆$3,120
$15,200 $360
©2015 Strata Decision Technology

Medicare Payment
Would You Take 110% of Medicare in Exchange for More Volume?
$13,800
$14,840
$16,720
-$1,240
$2,920
Variable Cost Per Case Margin
∆$1,040RCC
ABC + Acquisition CostTRUE COST
$16,720$17,960
RVU + Average Cost∆$3,120
$16,720 $1,880
©2015 Strata Decision Technology

Six quick “lessons” in our crash course today
1. Why do we need Cost Accounting?
2. How does Cost Accounting work?
3. What Cost Buckets should we use and how should we allocate overhead?
4. What Costing Methodologies should we use?
5. How is Advanced Cost Accounting different?
6. How can we leverage our cost data to take action and drive out costs?
©2015 Strata Decision Technology

FEATURES:
• NOT user-friendly
• Incredibly slow
• Data is not
integrated
• Data is not used
• System has low
utilization
Traditional Decision Support
©2015 Strata Decision Technology

Advanced Cost Accounting
USES A COMBINATION OF METHODOLOGIES TO PRODUCE THE
MOST ACCURATE COSTING
Creates the Foundation for Defensible Pricing and Effective Contracting
Analyze Cost Holistically andfor Specific Populations
ACCOMMODATES DIFFERENCES IN PRICING, ACUITY, & SALARY
PER PATIENT
INCLUDES SERVICES PROVIDED THROUGHOUT THE CONTINUUM
OF CARE
COSTS ARE UPDATED REGULARLY
FLEXIBLE w THOROUGH w ROBUST
ALGORITHMS TO DISCERN EXCESS CAPACITY AND EXPENSE
EXPENSES AND SERVICES ARE ALLOCATED TO SPECIFIC PATIENT
POPULATIONS
Know Your True Cost to Provide Care
Accepted by Clinicians and Leaders
Drives to Action
©2015 Strata Decision Technology

Six quick “lessons” in our crash course today
1. Why do we need Cost Accounting?
2. How does Cost Accounting work?
3. What Cost Buckets should we use and how should we allocate overhead?
4. What Costing Methodologies should we use?
5. How is Advanced Cost Accounting different?
6. How can we leverage our cost data to take action and drive out costs?
©2015 Strata Decision Technology

Your Call to Action:
Leverage Data to Drive Out Costs
©2015 Strata Decision Technology

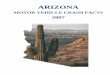
Cost Savings Initiatives are Falling Short
55%
44%
44%
27%
26%
Difficult to Quantify & Track Savings
Difficult to Keep Track of Projects
Lack of Accountability
Projects Don't Produce REAL savings
No Staff to Lead Projects
Source: Strata Decision Survey (n=100 providers)
88%of providers have cost savings initiatives underway
(Range: $50-$400M)
17%are hitting the target
WHY COST SAVINGS INITIATIVES UNDER DELIVER
©2015 Strata Decision Technology

MIND SET
SKILL SETTOOL SET
Requirements…
©2015 Strata Decision Technology

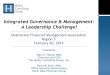
Cost Improvement in Action at CentraCare
• Cost of Variation of 65% of Inpatient Volume (17,500 Cases)• $11.3M in Savings • $4M in savings for top 10 DRGs alone
$0.0
$0.5
$1.0
$1.5
$2.0
$2.5
$3.0
$3.5
LOS Supplies DiagnosticTesting
Pharmacy Therapy Other
Mill
ion
s
Savings by Cost Driver OpportunitySize
# of Opps Total Savings
% of Savings
$500K+ 4 $2.7M 23%
$100-$400K 21 $4.7M 42%
<$100K 184 $3.9M 34%
Total 209 $11.3M

There is no silver bullet…everything has to be on
the table STREAMLINE Systems & Structures
• Benefits• PTO days• Capital
Budget/ Depreciation
• Insurance/ re-insurance
• Outsourced Services
• Consulting Services
• Duplicate IT systems
• Supply Chain
ELIMINATE VARIATION in
Care
• Implants • Physician
preference items
• High cost drugs
• Duplicate Imaging studies
• High cost labs as inpt
• End of life care
PURPOSE-BUILT
Org Structure
• Defining roles to fill distinct purpose
• Defining goals for roles
• Using data to drive accountability for results
LEVERAGE TECHNOLOGY for productivity
• Automate routine work
• Automate processes with rules based technology
• Identify and eliminate duplicative processes
LEAN OUT MGT
Structure
• Create ‘flow’ within a directors span of functions
• Bring functions together than work together often
STAFF to Demand
• Match staffing levels to volume levels
• Match skill level to skill needs
FLEX to Volume
• Adjust staffing levels to fluctuations in volume
©2015 Strata Decision Technology
Brainstorm, Validate, Then Operationalize Savings

Compare cost per case among physicians
Understand the labor cost and labor requirements to care for a population of patients
Negotiate favorable contracts
Identify opportunities to streamline administrative processes
Manage populations effectively across the continuum of care
Drive accountability for measurable results
With good cost data…
©2015 Strata Decision Technology