Embed Size (px)
Citation preview
This article was downloaded by: [Tufts University]On: 05 October 2014, At: 08:51Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Health Marketing QuarterlyPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/whmq20
A Descriptive Narrative ofHealthy EatingMohar J. Dutta-Bergman PhD aa Purdue University, Department of Communication,Beering Hall of Liberal Arts and Education , Room2114, 100 North University Street, West Lafayette,IN, 47907-2067, USAPublished online: 04 Oct 2008.
To cite this article: Mohar J. Dutta-Bergman PhD (2004) A Descriptive Narrativeof Healthy Eating, Health Marketing Quarterly, 20:3, 81-101, DOI: 10.1300/J026v20n03_06
To link to this article: http://dx.doi.org/10.1300/J026v20n03_06
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness,or suitability for any purpose of the Content. Any opinions and viewsexpressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of theContent should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for anylosses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of theContent.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan,
sub-licensing, systematic supply, or distribution in any form to anyone isexpressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
A Descriptive Narrative of Healthy Eating:A Social Marketing Approach
Using Psychographicsin Conjunction with Interpersonal,
Community, Mass Mediaand New Media Activities
Mohar J. Dutta-Bergman, PhD
ABSTRACT. This paper explores the profile of healthy and unhealthyeating consumers in terms of demographic, psychographic and commu-nicative variables. Data from 3,388 respondents to the 1999 DDBNeedham Life Style Study were analyzed. The results show the healthyeaters to be environmentally conscious and health-oriented, suggestingan underlying theme of personal and social responsibility. The commu-nicative activities of healthy eaters demonstrate an information orienta-tion while unhealthy eaters are more entertainment oriented. Practicaland social implications are discussed for social marketers regarding tar-get segmentation and message design. [Article copies available for a feefrom The Haworth Document Delivery Service: 1-800-HAWORTH. E-mail ad-dress: <[email protected]> Website: <http://www.HaworthPress.com> © 2003 by The Haworth Press, Inc. All rights reserved.]
KEYWORDS. Psychographics, healthy eating, media, social marketing
Mohar J. Dutta-Bergman is affiliated with Purdue University, Department of Com-munication, Beering Hall of Liberal Arts and Education, Room 2114, 100 North Uni-versity Street, West Lafayette, IN 47907-2067.
Health Marketing Quarterly, Vol. 20(3) 2003http://www.haworthpress.com/web/HMQ
2003 by The Haworth Press, Inc. All rights reserved.Digital Object Identifier: 10.1300/J026v20n03_06 81
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
Diet-related health conditions cost approximately $250 billion inmedical costs and lost productivity in the United States (Frazao, 1995).Based on the finding that an improvement in dietary behavior wouldprevent 20% of deaths related to cardiovascular disease, cancer, and di-abetes (Frazao, 1995), a large number of prevention campaigns havebeen launched with the goal of changing consumer diet (Farquhar,Fortmann, Maccoby, Haskell, Williams, Flora, Taylor, Brown, Solo-mon & Hulley, 1985; Potter, Finnegan, Guinard, Huerta, Kelder,Kristal, Kumanyika, Lin, Motsinger, Prendergast, & Sorensen, 2000;Schooler, Chaffee, Flora, & Roser, 1998). With this increasing empha-sis of communication campaigns on improving what people eat, it iscrucial to develop a narrative of healthy eating that would guide thestrategic choices of dietary interventions. Coined the term “formativeresearch,” this process of profiling a specific behavior explores the pat-terns of needs, wants, desires, and tendencies among audience membersto formulate media planning, message strategy, source selection andother strategic decisions (Albrecht & Bryant, 1996; Dutta & Youn,1999; Fisher, 1988; Flora & Thorensen, 1988; Frankenberger &Sukhdial, 1994; Lefebvre & Flora, 1988).
Applying the fundamental principles of formative research, this pa-per informs the question: Who is the healthy eater? It explores the pre-dictive impact of health status, demographics, psychographics, andcommunicative factors on healthy eating. Indicative of the consumer’scurrent health, health status indicators are strong situational factors thatdetermine what the consumer eats. A review of the literature reveals ex-tensive research on demographic variables as antecedents of healthyeating (Kearney et al., 1998; Lahmann & Kumanyika, 1999; McIntoshet al., 1990; Goldberg et al., 1990; Medeiros et al., 1996; ADA Report,1997). Although these much-researched demographic factors explain aconsiderable level of variance in healthy eating, they are unable tothrow additional insight on the phenomenon of healthy eating. To com-plete the narrative, this paper introduces psychographic and communi-cative variables.
The success of psychographic variables in the realm of commercialmarketing has led to a growing interest in psychographic research inhealth communication (Dutta & Youn, 1999; Swenson & Wells, 1995).In addition to explaining additional variance in healthy eating beyonddemographic variables, they provide a descriptive picture of the con-struct (see, for instance, Dutta-Bergman, 2001; Dutta & Youn, 1999;Swenson & Wells, 1995). Psychographic variables often exist in clus-ters of cognitive categories that are associated with each other and are
82 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
tied together by an underlying theme. This theme is revealed throughthe associations among the variables. The psychographic variables ex-amined in this research are health orientation and environmental con-sciousness.
Finally, the paper proposes to look at the role played by the commu-nicative activities in the explanation of healthy eating. The communica-tion literature provides ample support for the speculation that the use ofinterpersonal channels, community activities, mass media channels,and new media outlets may be associated with different types of healthbehaviors (Zillman & Bryant, 1985). Based on extant literature(Zillman & Bryant, 1985), a theoretical framework is constructed forunderstanding how the choice of communicative activities affectshealthy eating.
FACTORS RELATED TO HEALTHY EATING
Current Health Status
In the context of health, a strong situation often becomes the determi-nant of health behaviors engaged in by individuals. Current health sta-tus predicts individual health activities by setting the constraints forconsumer lifestyle. For instance, consumers detected with high choles-terol or high blood pressure are probably more likely to eat healthy be-cause their life situation orients them toward such healthful activities. Inother words, an event in the individual’s life such as being detected withhigh blood cholesterol shifts his/her lifestyle toward more healthychoices. Therefore it is hypothesized:
Hypothesis One: Current health status (high blood pressure and/orhigh blood cholesterol) will be positively related to healthy eating.
Demographic Factors
Age, gender, income, and education have been extensively studied inthe context of their relationship with healthy eating (Kearney et al., 1998;Lahmann & Kumanyika, 1999; McIntosh et al., 1990; Goldberg et al.,1990; Medeiros et al., 1996; Neumark-Sztainer, Story, Resnick, & Blum,1998; Neumark-Sztainer, Story, Resnick, & Blum, 1996; Story, French,Resnick, & Blum, 1995). Interest in health and nutrition increases with age(Kearney et al., 1998; Lahmann & Kumanyika, 1999; McIntosh et al.,
Mohar J. Dutta-Bergman 83
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
1990; Goldberg et al., 1990; Medeiros et al., 1996; ADA Report, 1997).Older people are more likely to care about their health, engage in preven-tive health activities, and seek out additional health information than youn-ger people (Dutta & Youn, 1999). Hence it is hypothesized:
Hypothesis Two: Age will be positively related to healthy eating.
Furthermore, the importance on women’s physical appearance andbody shape added to the socially imposed responsibility of taking careof health are reflected in the key role played by gender in the determina-tion of health-related eating behavior (Andersen & DiDomenico, 1992;Hertzler & Grun, 1990; Mooney et al., 1994). Women are more likelythan men to eat healthy and engage in activities that focus on maintain-ing their health (Dutta & Youn, 1999). Women are also more likely thanmen to take supplements in their diets and engage in health-related in-formation gathering (Neumark-Sztainer, Story, Resnick, & Blum,1998). Hence it is hypothesized:
Hypothesis Three: Gender will be positively related to healthy eating.
The level of education affects a wide range of healthy behaviors in-cluding healthy eating (Neumark-Sztainer, Story, Resnick, & Blum,1998; Neumark-Sztainer, Story, Resnick, & Blum, 1996; Story, French,Resnick, & Blum, 1995). More educated consumers have greater accessto health-related information and may be expected to eat more healthythan less educated consumers. This leads to the following hypothesis:
Hypothesis Four: Education will be positively related to healthyeating.
A similar effect may be expected for income, with a higher level ofincome leading to a greater degree of healthy eating (Neumark-Sztainer, Story, Resnick, & Blum, 1998; Neumark-Sztainer, Story,Resnick, & Blum, 1996).
Hypothesis Five: Income will be positively related to healthy eating.
Psychographic Variables
Researchers in the domain of commercial marketing have long ar-gued that the activities, interests and opinions of consumers, the tripods
84 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

of consumer lifestyle, are more effective than demographics in guidingcommunication choices in commercial and social marketing strategies(Bellenger & Vallencia, 1982; Heath, 1996; Riche, 1989; Townsend,1997). The critical theoretical force driving psychographic research iscognitively oriented and is based on the premise that individuals maxi-mize the consistency among their attitudes directed at different objectsand issues (Dutta & Youn, 1999). According to the cognitive frame-work of lifestyle study suggested by Grunert, Bruns and Bisp (1997),cognitive structures are made of declarative and procedural knowledge,a system of cognitive categories, their associations, and scripts (Grunertet al., 1997). These cognitive categories and their associations resultfrom lifelong learning, and manifest themselves in enduring disposi-tions to behave (Grunert, Bruns, & Bisp, 1997). Therefore, the individ-ual becomes a repository of related activities, interests, and opinionsthat are enacted within a particular cognitive mind-frame.
This paper applies the theory of unified responsibility to integrate thepsychographic variables (Dutta-Bergman, in press). It argues that a keensense of responsible action drives healthy eating (Dutta & Youn, 1999).The psychographic variables examined in this study are linked by thissense of responsibility (Dutta-Bergman, in press). They reflect a commit-ment to engage in personally and socially responsible action and servethe foundation for the theory of unified responsibility. Borrowing fromTocqueville’s (1999) conceptualization of self-interest rightly under-stood, the theory of unified responsibility states that a sense of responsi-bility emanates across the personal and social domains of individuals(Dutta-Bergman, in press). Individuals that are more likely to be respon-sible actors in their personal lives are also likely to be actively engaged inresponsible actions in their social lives. A sense of responsibility servesas the fulcrum for the multitude of consumption practices enacted by theindividual, drawing them together by a strong centripetal force. Respon-sibility, it is argued here, becomes the transparent construct that mani-fests itself in the way of life of the healthy eater.
Health Orientation
With an internal locus of control, a high level of responsibility to-ward personal health, and a high level of self-efficacy, individuals whoare oriented toward maintaining a healthy body and mind are also morelikely to engage in healthy eating (Dutta & Youn, 1999; Rimal, Flora, &Schooler, 1999). The notion of performing healthy activities permeatesthroughout the different aspects of individual lifestyle, leading to a high
Mohar J. Dutta-Bergman 85
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

correlation among the different aspects of healthy activities (Maibach,Maxfield, Ladin, & Slater, 1996). Therefore, an overall health orienta-tion of the individual (Rimal, Flora, & Schooler, 1999) makes him/hermore likely to eat healthy. Eating healthy becomes a manifestation ofthis general health orientation. Exercising, nutrition label readership,health services usage and health information seeking reflect generalhealth orientation. Those consumers who exercise regularly, activelyseek out health information, use health services and read nutrition labelsalso eat healthy foods and participate actively in their food choices.Hence, it is hypothesized:
Hypothesis Six: Health orientation will be positively related tohealthy eating.
Environmental Consciousness
The theory of unified responsibility articulates that healthy eaters ex-perience a sense of responsibility toward the society they live in (Dutta &Youn, 1999; Swenson & Wells, 1995; Rosenbaum, 1980; Rosenbaum,1993). This sense of responsibility, it may be argued, is also felt in thehealthy eaters’ attitude toward their environment (Dutta & You, 1999;Swenson & Wells, 1995). Healthy eaters are more likely to have favor-able attitudes toward environmentally friendly products, harbor envi-ronmental concerns and demonstrate pro-environmental behaviors(Swenson & Wells, 1995). This leads to the following hypothesis:
Hypothesis Seven: Environmental consciousness will be posi-tively related to healthy eating.
Communicative Activities
Since the seminal work of William Stephenson (1967) on the dualnature of communicative activities, communication scholars have tradi-tionally categorized communicative activities into the domains of workand play. Classified as information versus entertainment orientations,these two distinct categories often emerge in uses and gratification stud-ies of different media. In harmony with the dichotomous nature of com-munication proposed by many scholars, this paper builds upon thetheory of unified responsibility to break down communicative activitiesinto two broad dimensions: communicative activities with a cognitiveorientation that involve responsible enactment and active consumption,
86 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

and those activities with a sensory orientation that involve passive con-sumption of communication for entertainment (Lichtenstein & Rosenfeld,1983; Rubin, 1977; Rubin & Rubin, 1982). For instance, while news-reading is categorized as a highly cognitive and responsible communi-cative act, watching sports on television is typically an affective com-munication act. In the following sections, systematic hypotheses aresuggested based on the cognitive and affective orientations of commu-nication acts.
Interpersonal Activities
Interpersonal relationships lie at the core of individual well-beingand health status. Epidemiologists have consistently presented supportfor the argument that social isolation determines health outcomes(Singer, 2000). The lack of social support and increased social isolationresults in an increased risk of various diseases as well as a reducedlength of life (Berkman & Breslow, 1983; House, Landis, & Umberson,1988; Seeman et al., 1993). Persons who engage in interpersonal activi-ties have been found to have a greater level of health (Berkman, 1995),demonstrating better health outcomes than those people who do not en-gage in interpersonal activities. Although the linkage between socialsupport and health has been clearly demonstrated, researchers suggestmultiple mechanisms for the linkage. One of the many mechanismsthrough which social support impacts health involves the role of inter-personal relationships in promoting healthy behaviors (Singer, 2000).Significant others and other meaningful relationships encourage posi-tive health practices (Berkman, 1995; Spiegel & Kimerling, 2000; Tay-lor et al., 1997). These relationships provide meaning to the life of anindividual, making him/her more likely to take care of himself/herself.Married status is often considered to be an indicator of meaningful in-terpersonal relationship. A greater degree of life-satisfaction and astronger sense of purposefulness are both associated with the participa-tion in such meaningful interpersonal bonds. The sense of purpose inlife makes an individual willing to invest greater time and energy inits maintenance, and subsequent monitoring of health to maintainlife. Based on the linkages between interpersonal activities and health-conscious activities, it may be hypothesized:
Hypothesis Eight: Interpersonal activities will be positively re-lated to healthy eating.
Mohar J. Dutta-Bergman 87
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

Community Activities
Denoting civic engagement as a form of social capital, researchershave argued that engagement in one’s community is an indicator of thewillingness and the ability to influence others in one’s social network. Aresponsible citizen that believes in his/her ability to catalyze socialchange and is motivated enough to participate in such activities may alsobe expected to demonstrate a personal level of responsibility towardhis/her health (Dutta & Youn, 1999). Health consciousness becomes in-tegrated with civic engagement under the broader umbrella of personaland social responsibility. This leads to the following hypothesis:
Hypothesis Nine: Civic engagement will be positively related tohealthy eating.
Mass Media Activities
In accordance with the dual model of communication, mass mediaare traditionally categorized into information-oriented and entertain-ment-oriented groups (Atkin, 1985; Wakshlag, 1985). Therefore, whiletelevision news content is information-oriented, television drama, com-edy, and sports are primarily entertainment oriented. Concurrent withthe information and entertainment orientations of media vehicles, me-dia researchers suggest a dichotomous scheme for categorizing the mo-tivations for the consumption of mass media content (Lichtenstein &Rosenfeld, 1983; Rubin, 1977; Rubin & Rubin, 1982).
The main argument put forth in this paper is that the cognitively-oriented consumption of informational content of mass media is a posi-tive predictor of health conscious behavior, including healthy eating(Korhonen, Uutela, Korhonen, & Puska, 1998). Three underlyingmechanisms with three different philosophical underpinnings may besuggested to explain this phenomenon. Given the primary presence ofusable health information in news and targeted health channels, selec-tive exposure theory suggests that health conscious consumers wouldselectively expose themselves to such media vehicles with health con-tent (Lichtenstein & Rosenfeld, 1983; Rubin, 1977; Rubin & Rubin,1982). Yet another explanation of the linkage between informationalmedia consumption and health consciousness ties in with the underly-ing notion of personal and social responsibility that unifies the differentactivities, interests, and opinions of healthy eaters. In other words, thoseconsumers who feel a sense of responsibility toward personal health
88 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
and engage in healthy eating are also probably more likely to engage inthe responsible consumption of mass media content, primarily consum-ing information-oriented media channels (Dutta & Youn, 1999). A thirdmedia-effect-based explanation would suggest that those consumerswho read news and consume information-oriented news media engagein healthy behaviors by virtue of their exposure to all the health infor-mation available on the information-based media vehicles. Exposure tohealth (information) media content, according to this view, makes aperson more health conscious. The three mechanisms may be unified bya model that argues that responsible consumers choose informa-tion-based health content which in turn leads to the further productionof health conscious behavior, thus leading to an increasing gap betweenthe health conscious (health rich) and not health conscious (health poor)consumers. Consumption of entertainment-oriented media, however,correlates with the lack of active responsibility in one’s media choices,and hence is a negative predictor of healthy eating. Hypotheses ten andeleven formally state the relationships between media consumption andhealthy eating.
Hypothesis Ten: Consumption of information-oriented and tar-geted media will be positively related to healthy eating.
Hypothesis Eleven: Consumption of entertainment-oriented me-dia will be negatively related to healthy eating.
New Media Activities
In the uses and gratifications studies involving audience motives forthe consumption of new media, the different motives to use the new me-dia fall into two broad categories: motives with an information orienta-tion and motives with an entertainment orientation (Papacharissi &Rubin, 2000). The argument about the linkage between traditional me-dia consumption and health consciousness may also be extrapolated tothe domain of the new media, articulating the idea that consumption ofinformation-oriented new media is positively related with health con-sciousness while the entertainment-oriented consumption of new mediais negatively correlated with healthy eating.
Hypothesis Twelve: Consumption of functional new media will bepositively related to healthy eating.
Mohar J. Dutta-Bergman 89
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
Hypothesis Thirteen: Consumption of entertainment-oriented newmedia will be negatively related to healthy eating.
METHODOLOGY
Data
The 1999 DDB Needham Life Style Study, an annual standing-panelmail survey, was used for this study and was directly supplied to the re-searcher by DDB Needham. The sample was drawn to approximate “ac-tual distributions within the 9 census divisions of household income,population density, panel member’s age, and household size” (Groene-man, 1994, as quoted in Scheufele & Shah, 2000). The DDB NeedhamLife Style surveys have been used in multiple studies (see, for instance,Dutta & Youn, 1999; Dutta & Wells, in press; Putnam, 1995; Putnam &Yonish, 1999; Scheufele & Shah, 2000; Shah, McLeod, & Yoon, 2001)and have been validated against the General Social Survey and RoperPoll (Putnam & Yonish, 1999). Approximately 5,000 adult Americansare asked several hundred questions about their attitudes, interests,opinions, personality traits, activities, and product consumption. A totalof 3,388 subjects participated in the study. In 1999, 1,527 males and1,861 females provided usable data. The mean age of the respondentswas 48.25 years.
Dependent Variable
Healthy eating was measured by ten items. Each of these items wasmeasured on a 1 to 6 scale ranging from “definitely disagree” to “defi-nitely agree.” These ten items were “I try to avoid foods that are high infat,” “I try to avoid foods that are high in cholesterol,” “I try to avoidfoods with a high salt content,” “I am concerned about how much sugarI eat,” “I make a special effort to get enough fiber in my diet,” “I use alot of low calorie or calorie reduced products,” “I try to select foods thatare fortified with vitamins and minerals,” “I am careful about what I eatin order to keep my weight under control,” “I try to avoid foods thathave additives in them,” and “I am concerned about getting enough cal-cium in my diet.” These ten items were subjected to a principal compo-nent analysis with Varimax rotation. A single factor was produced thatexplained 47.8% of the variance. The aggregated scale had a high reli-ability (.89).
90 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
Independent Variables
Demographic Variables. Age was measured by a single item that sim-ply asked the respondent to report his/her exact age in number of years.Education was measured by a single item, “education level of respon-dent” on a 1 to 7 scale. Income was measured by a single item, “Intowhich one of the following categories does your annual household in-come fall?” Finally, respondents reported their gender on a single-itemdichotomous variable that asked them whether they were male or female.
Health Orientation. Exercising was measured by six items. These sixitems were “went to an exercise class,” “did exercise at home,” “went toa health club,” “jogged,” “walked more than one mile for exercise,” and“rode a bicycle.” Each of these items was measured on a 1 to 6 scaleranging from “definitely disagree” to “definitely agree.” When sub-jected to a principal component factor analysis with Varimax rotation, asingle factor with Eigenvalue greater than one was generated.Cronbach’s alpha of the scale was .63. Nutrition label readership wasmeasured by a single item “nutritional information on food labels deter-mines which products and brands I buy” on a 1 to 6 scale ranging from“definitely disagree” to “definitely agree.” Health information seekingwas tapped into by the item “I rely on a number of sources of health in-formation, besides my doctor.” “I have had a physical exam in the pastyear” measured health services usage.
Environmental Consciousness. Five items were put together to mea-sure environmental consciousness. These five items were “I worry a lotabout the effects of environmental pollution on my family’s health,” “Iwould be willing to accept a lower standard of living to conserve energy,”“I support pollution standards even if it means shutting down some facto-ries,” “I make a special effort to look for products that are energy effi-cient,” and “I make a strong effort to recycle everything I possibly can.”All five items yielded a single factor with factor loadings ranging from.56 to .63. Cronbach’s alpha of the aggregated scale was .61.
Communicative Variables. Interpersonal communication was mea-sured by five items: “gave or attended a dinner party,” “played cards,”“entertained people in my home,” “sent a greeting card,” and “I spend alot of time visiting friends.” The items were subjected to a PrincipalComponents factor analysis with Varimax rotation, producing a singlefactor with Eigenvalue greater than 1. Cronbach’s alpha for the aggre-gated scale was .60.
Community participation was measured by the items “sent a letter tothe editor,” “participated in a club meeting,” “attended a church,” “vol-
Mohar J. Dutta-Bergman 91
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

unteered in a community organization,” and “participated in a commu-nity project.” All items were measured on a six-point scale ranging from“definitely disagree” to “definitely agree.” On conducting a PrincipalComponent factor analysis with Varimax rotation a single factor wasgenerated. The Eigenvalue of the factor was 1.82. The aggregated scalehad a moderate reliability of .62.
Specific media vehicle choice was measured by dichotomous“Yes/No” responses to items representing individual newspapers, news-paper sections, magazines, and television programs. The following in-struction was provided: “Below is a list of media vehicles. Please ‘X’each vehicle that you read/watch/listen to most or all issues of.”
RESULTS
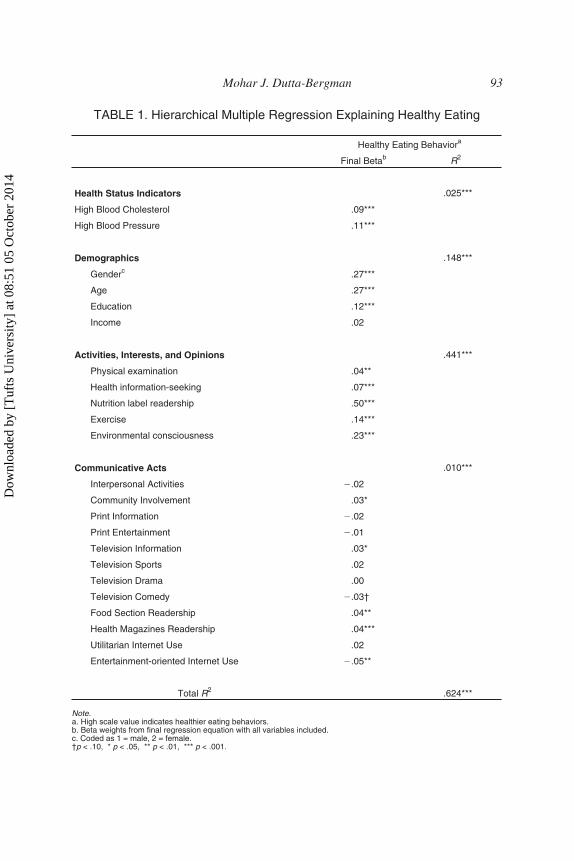
Overall, the variables included in the analysis accounted for 62.4%of the total variance in healthy eating. The results of this analysis indi-cate that in addition to the health status and the demographic variables,the psychographic and communicative variables together explained asignificant amount of additional variance (see Table 1).
Current health status accounted for 2.5% of the variance in healthyeating. Individuals detected with high blood pressure (b = .11, p < .001)or high blood cholesterol (b = .09, p < .001) levels were significantlymore likely to eat healthy than those individuals without these condi-tions. Demographic variables, as a block, accounted for 14.8% of thevariance. Gender (b = .27, p < .001) and age (b = .27, p < .001) were thestrongest demographic predictors of healthy eating, with women show-ing greater levels of healthy eating behavior than men. In support of thenomological network, older people demonstrated a greater willingnessto engage in healthy eating than younger people. Also, education (b =.12, p < .001) emerged as a significant predictor of healthy eating.
The psychographic constructs added another 44.1% to the explainedvariance, after controlling for the demographic variables. In support ofthe nomological network, an overall health orientation positively pre-dicted healthy eating. Nutrition label readership (b = .50, p < .001) wasthe strongest psychographic predictor of healthy eating. Additionally,other indicators of health orientation such as exercising (b = .14, p <.001), health information seeking (b = .07, p < .001) and getting a physi-cal exam (b = .04, p < .01) had significantly positive effects on healthyeating. Also, supporting hypothesis seven and in harmony with the the-
92 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
Mohar J. Dutta-Bergman 93
TABLE 1. Hierarchical Multiple Regression Explaining Healthy Eating
Healthy Eating Behaviora
Final Betab R2
Health Status Indicators .025***
High Blood Cholesterol .09***
High Blood Pressure .11***
Demographics .148***
Genderc .27***
Age .27***
Education .12***
Income .02
Activities, Interests, and Opinions .441***
Physical examination .04**
Health information-seeking .07***
Nutrition label readership .50***
Exercise .14***
Environmental consciousness .23***
Communicative Acts .010***
Interpersonal Activities �.02
Community Involvement .03*
Print Information �.02
Print Entertainment �.01
Television Information .03*
Television Sports .02
Television Drama .00
Television Comedy �.03†
Food Section Readership .04**
Health Magazines Readership .04***
Utilitarian Internet Use .02
Entertainment-oriented Internet Use �.05**
Total R2 .624***
Note.a. High scale value indicates healthier eating behaviors.b. Beta weights from final regression equation with all variables included.c. Coded as 1 = male, 2 = female.†p < .10, * p < .05, ** p < .01, *** p < .001.
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
ory of unified responsibility, environmental consciousness positivelypredicted healthy eating behavior (b = .23, p < .001).
Communicative activities accounted for an additional 1% of the vari-ance in healthy eating beyond the current health status indicators, de-mographic and psychographic variables. Hypothesis eight was notsupported. Interpersonal activities such as playing cards and attendingparties (b = �.02, n.s.) were not related to healthy eating. The resultsfound support for hypothesis nine, showing a significant effect of com-munity involvement on healthy eating (b = .03, p < .05).
In the context of the consumption of traditional media, while the ef-fect of print news on healthy eating was non significant (b = .02, n.s.),the consumption of television news positively impacted healthy eating(b = .03, p < .05). In addition, readership of health-oriented targeted me-dia such as food section of newspapers (b = .04, p < .01) and healthmagazines (b = .04, p < .001) had positive effect on healthy eating,showing support for hypothesis ten. While the consumption of print en-tertainment (b = �.03, p < .10), television sports and television dramahad no significant effect on healthy eating, the effect of comedy ap-proached significance (b = .03, p < .10). In the area of new media con-sumption, hypotheses twelve was not supported. The effect of theinformation uses of the Internet were non-significant. Finally, hypothe-sis thirteen was supported, with a significant negative effect of enter-tainment-based Internet usage on healthy eating, (b = �.05, p < .01).
DISCUSSION
The psychographic and communicative variables introduced into theframework of this paper support the notion of an interlinked web of cog-nitive categories. It is worth noting that the percent of variance inhealthy eating explained by the psychographic variables is considerablyhigher than the variance explained by demographic variables. Sup-porting the theory of unified responsibility, both health orientation andenvironmental consciousness emerged as predominant predictors ofhealthy eating.
The positive impact of health orientation on healthy eating supportsthe findings of earlier studies that demonstrate the co-occurrence of dif-ferent healthy behaviors in clusters. Highly motivated health consumerswho exercise, engage in health information gathering, read nutrition la-
94 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
bels and use health services are also more likely to eat healthy. Also,healthy eaters are concerned about various environmental issues andare willing to take responsibility for protecting the environment that en-compasses their lives.
In addition to the traditional psychographic variables, the communi-cative activities in this study were significant predictors of healthy eatingand in general, supported the theory of unified responsibility. Participa-tion in community activities had a significant effect on healthy eating,suggesting that a sense of responsibility percolates into the differentdomains of consumer lifestyle. Also supporting the theory of unified re-sponsibility, the study demonstrated that the consumption of health-oriented media (targeted media) was a positive predictor of healthy eat-ing. Readers of “Health” and “Prevention” magazines were more likelyto eat healthy than the non-readers. Also, entertainment-orientedInternet consumption was a negative predictor of healthy eating.
Limitations
This study suffers from some important limitations. Self-reportedmeasures of the psychographic and communicative variables poseproblems to the validity of the measures. The mailback panel used in thestudy suffers from problems of attrition and panel bias. Finally, the useof an American sample that is predominantly White limits thegeneralizability of the study results. Future research needs to extrapo-late the research findings to other cultural domains.
Implications
The study results provide a descriptive profile of the healthy eaterthat may be used to segment consumers and to develop appropriatemessages for healthy eating campaigns. First, healthy eating occursamidst a cluster of responsible activities. In other words, the healthyeater is more likely to be responsibility-oriented compared to the un-healthy eater. Campaigns promoting the theme of individual responsi-bility in the context of healthy eating are unlikely to appeal to theunhealthy eater (Guttman, 2000). For the unhealthy eater, life choicesare not governed by a commitment to responsibility. Therefore, insteadof focusing on rational choices and decision making (inherent in tradi-tionally used models such as the health belief model and the theory ofreasoned action), healthy eating campaigns should perhaps focus on ap-pealing to the sensory and affective needs of the target audience.
Mohar J. Dutta-Bergman 95
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

The unhealthy eater is less likely to seek out health information.Therefore, information-based campaigns in traditional health outletsare unlikely to reach the group. Rather, message content of campaignstargeting unhealthy behaviors would have a greater likelihood of suc-cess in using entertainment-oriented strategies. Also, campaign mes-sages would perhaps be more effective when placed in entertainmentcontexts. The unhealthy eater is also less likely to visit the doctor for aphysical examination. As a consequence, campaigns targeting un-healthy eaters are unlikely to reach the group through medical practition-ers. In addition, the co-occurrence of healthy eating, exercising andhealth services usage suggests a critical need to effectively reach the un-healthy segment that suffers a significantly greater risk of cardiovascu-lar disease, cancer, diabetes, and other life-threatening diseases.
The exploration of communicative choices of unhealthy eatersdemonstrates a lesser likelihood of attending community organiza-tions. This finding questions the validity of using community organi-zations for reaching unhealthy eaters. Those consumers who suffer thegreatest lifestyle-related risks need to be reached through innovativecommunicative channels beyond churches and volunteer organiza-tions. Community organizations can, however, serve as effectivechannels for reinforcing positive health behavior. The readership oftargeted media such as food sections of newspapers and health-ori-ented magazines positively predicted healthy eating. These health-based outlets can be effectively used to reach the healthy eater. Cam-paigns seeking to inform healthy eaters of a new research finding or anew diet would reach the desired target audience through such tar-geted vehicles. However, these communicative vehicles are unable toreach the unhealthy eater.
Using television for informative purposes positively predictedhealthy eating. Therefore, while television news might serve as an ef-fective channel for reinforcing healthy behavior or informing thehealthy segment about a new product innovation, news content wouldbe ineffective in reaching the unhealthy eater. Video news releases, cir-culated to television news stations, are not likely to succeed in commu-nicating the message to the unhealthy eater. Other forms of news-basedcontent are also likely to be ineffective in reaching the group.
However, the unhealthy eater is likely to watch television comedy.Concepts related to healthy eating may be placed within comedy pro-gram content. In addition, healthy eating advertisements may be placedon television comedy programs. The unhealthy eater is also more likelyto seek out entertainment-based content on the Internet. Therefore, con-
96 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

cepts related to healthy eating may be placed within Internet games,hobby-related Websites, etc. Banner advertisements may also be placedin these domains.
Directions for Future Research
This study provided preliminary support for the theory of unified re-sponsibility. Healthy eating exists amidst a cluster of responsible activi-ties. Future research needs to further explore the mechanism underlyingthe relationship among the different constructs introduced in this paper.Also, although the critical role of responsibility emerged through the re-lationship among the variables studied here, this paper did not measureresponsibility. Future scholarship needs to measure responsibility andinterrogate its relationship with a wide range of lifestyle variables.Also, worth examining are the questions: What are the antecedents ofresponsibility? How does education impact the sense of responsibility?Additional research is needed in exploring the relationship of demo-graphic variables with responsibility.
The results also demonstrated that entertainment-based media activi-ties are positively related with unhealthy practices. Particularly salientwas the finding that the unhealthy eater is more likely to use the Internetfor entertainment purposes. Given the limited use of the Internet as asite for public health intervention and research (Chamberlain, 1996),the results of this study provide fodder for future scholarship. Future re-search needs to look at the impact of information-oriented and enter-tainment-oriented usage of the Internet on audience response toInternet-based health campaigns.
REFERENCES
Abusabha, R., & Achterberg, C. (1997). Review of self-efficacy and locus of controlfor nutrition and health-related behavior. Journal of the American Dietetic Associa-tion, 97(10), 1122-1133.
Albrecht, T. L., & Bryant, C. (1996). Advances in segmentation modeling for healthcommunication and social marketing campaigns. Journal of Health Communica-tion, 1, 65-80.
Andersen, A. E., & DiDomenico, L. (1992). Diet vs. shape content of popular male andfemale magazines: A dose-response relationship to the incidence of eating disor-ders. International Journal of Eating Disorders, 11, 283-287.
Mohar J. Dutta-Bergman 97
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

Andreasen, A. (1997). Challenges for the science and practice for social marketing. InM. E. Goldberg, M. Fishbein, & S. E. Middlestadt (Ed.), Social Marketing: Theo-retical and Practical Perspectives (pp. 3-19). Mahwah, New Jersey: LawrenceErlbaum Associates, Publishers.
Atkin, C. K. (1985). Informational Utility and Selective Exposure to EntertainmentMedia. In D. Zillman, & J. Bryant (Eds.), Selective Exposure to Communication,63-87.
American Dietetic Association. (1997). Fewer American reading labels, more awareof the food guide pyramid. Chicago: American Dietetic Association.
Bellenger, D. N., & Valencia, H. (1982). Understanding the Hispanic market. BusinessHorizons, 47-50.
Chavez, E. L., & Michaels, A. C. (1980). Evaluation of the health locus of control forobesity treatment. Psychology Rep, 46, 620-628.
Chamberlain, M. A. (1996). Health Communication: Making the Most of New MediaTechnologies–An International Overview. Journal of Health Communication, 1(1),43-50.
Dawson, S. (1989). Health care consumption and consumer social class: A differentlook at the patient. Journal of Health Care Marketing, 9, 15-25.
DeWolfe, J. A., & Shannon, B. M. (1993). Factors affecting fat consumption of Uni-versity students: Testing a model to predict eating behavior change. Journal of theAmerican Dietetic Association, 54(3), 132-137.
Diener, E. (1984). Subjective Well-being. Psychological Bulletin, 95(3), 542-575.Dutta-Bergman, M. (in press). Demographic and Psychographic Antecedents of Commu-
nity Participation: Applying a Social Marketing Model. Social Marketing Quarterly.Dutta, M. J., & Youn, S. (1999). Profiling Healthy Eating Consumers: A
Psychographic Approach to Social Marketing. Social Marketing Quarterly, 5(4),5-21.
Edwards, N. J., & Klemmack, D. L. (1973). Correlates of life satisfaction: A re-exami-nation. Journal of Gerontology, 28, 497-502.
Ellen, P. S., Wiener, J. L., & Cobb-Walgren, C. (1991). The role of perceived con-sumer effectiveness in motivating environmentally conscious behaviors. Journal ofPublic Policy & Marketing, 10 (Fall), 102-117.
Endler, N. S., & Rosenstein, A. J. (1997). Evolution of the personality construct inmarketing and its applicability to contemporary personality research. Journal ofConsumer Psychology, 6(1), 55-66.
Farquhar, J. W., Fortmann, S. P., Flora, J. A., Taylor, B., Haskell, W. L., Williams,P. T., Maccoby, N., & Wood, P. D. (1990). Effects of community-wide educationon cardiovascular disease risk factors: The Stanford Five-City Project. Journal ofthe American Medical Association, 264, 359-365.
Farquhar, J. W., Fortmann, S. P., Maccoby, N., Haskell, W. L., Williams, P. T., Flora,J. A., Taylor, C. B., Brown, B. W., Solomon, D. S., & Hulley, S. B. (1985). TheStanford Five-City Project: Design and Methods. American Journal of Epidemiol-ogy, 122, 323-334.
Fisher, J. D. (1988). Possible effects of reference-group based social influence onAIDS-risk behavior and AIDS prevention. American Psychologist, 43(November),914-920.
98 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

Flora, J. A., & Thorensen, R. E. (1988). Reducing the risk of AIDS in adolescents.American Psychologist, 43(November), 914-920.
Frankenberger, K. D., & Sukhdial, A. S. (1994). Segmenting teens for AIDS preven-tive behaviors with implications for marketing communications. Journal of PublicPolicy and Marketing, 13, 133-150.
Goldberg, J. P., Gershoff, S. N., & McGandy, R. B. (1990). Appropriate topics for nu-trition education for the elderly. Journal of Nutrition Education, 22, 303-310.
Green, P. E., & Krieger, A. M. (1991). Segmenting markets with conjoint analysis.Journal of Marketing, 55, 20-31.
Heath, R. P. (1996). The frontiers of psychographics. American Demographics, 18(7),38-44.
Guttman, N. (2000). Public health communication interventions. New York, NY: SagePublications.
Hertzler, A. A., & Grun, I. (1990). Potential nutrition messages in magazines read bycollege students. Adolescence, 25, 717-724.
Kearney, M., Kelly, A., & Gibney, M. J. (1998). Attitudes toward and beliefs about nu-trition and health among a nationally representative sample of Irish adults: Applica-tion of Logistic Regression Modeling. Journal of Nutrition Education, 30, 139-148.
Korhonen, T., Uutela, A., Korhonen, H. K., & Puska, P. (1998). Impact of Mass Mediaand Interpersonal Health Communication on Smoking Cessation Attempts: A studyin North Keralia, 1989-1996. Journal of Health Communication, 3, 105-118.
Kotler, P. (1988). Marketing Management, 6th Ed. Englewood Cliffs, NJ: PrenticeHall.
Kotler, P., & Andreason, A. (1991). Strategic marketing for nonprofit organizations.Englewood Cliffs, New Jersey: Prentice Hall.
Kotler, P., & Roberto, E. (1989). Social marketing: strategies for changing public be-havior. New York: Free Press.
Lahmann, P. H., & Kumanyika, S. K. (1999). Attitudes about health and nutrition aremore indicative of dietary quality in 50- to 75-year-old women than weight and ap-pearance concerns. Journal of the American Dietetics Association, 99(4), 475-479.
Larson, R. (1978). Thirty years of research on the subjective well-being of elder Amer-icans. Journal of Gerontology, 33(1), 109-125.
Lefebvre, R. C., & Flora, R. A. (1988). Social marketing and public health interven-tion. Health Education Quarterly, 15, 299-315.
Lichtenstein, A., & Rosenfeld, L. (1983). Uses and Misuses of Gratifications Re-search: An Explication of Media Functions. Communication Research, 10, 97-109.
Maibach, E. W., Maxfield, A., Ladin, K., & Slater, M. (1996). Translating Health Psy-chology into Effective Health Communication: The American Healthstyles Audi-ence Segmentation Project. Journal of Health Psychology, 1(3), 261-277.
McIntosh, W. A., Kubena, K. S., Walker, J., Smith, D., & Landmann, W. A. (1990).The relationship between beliefs about nutrition and dietary practices of the elderly.Journal of the American Dietetic Association, 90, 671-676.
Medeiros, D. M., Auld, G. W., Bock, M. A., Bruhn, C. M., Gabel, K., Lauritzen, G.,Lee, Y. S., McNulty, J., Newman, R., Nitzke, S., Ortiz, M., Read, M., Schutz, H., &Sheehan, E. T. (1996). Diet fat and fiber knowledge, beliefs and practices are mini-mally influenced by health status. Nutrition Research, 16, 751-758.
Mohar J. Dutta-Bergman 99
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014

Mooney, K. M., & Lorenz, E. (1997). The effects of food and gender on interpersonalperceptions. Sex Roles: A Journal of Research, 36, 639-655.
Mooney, K. M., DeTore, J., & Malloy, K. A. (1994). Perceptions of women related tofood choice. Sex Roles, 31, 433-442.
Neumark-Sztainer, D., Story, M., Resnick, M. D., & Blum, R. W. (1998). Lessonslearned about adolescent nutrition from the Minnesota adolescent health survey.Journal of the American Dietetic Association, 98(December), 1449-57.
Neumark-Sztainer, D., Story, M., Dixon, L. B., Resnick, M. D., & Blum, R. W. (1997).Correlates of inadequate fruit and vegetable consumption among adolescents. Jour-nal of Nutrition Education, 29, 12-20.
Neumark-Sztainer, D., Story, M., Resnick, M. D., & Blum, R. W. (1996). Correlates ofinadequate fruit and vegetable consumption among adolescents. Preventive Medi-cine, 25, 497-505.
Neumark-Sztainer, D., Story, M., Toporoff, E., Himes, J., Resnick, M. D., & Blum,R. W. (1997). Covariations of eating behaviors with other health-related behaviorsamong adolescents. Journal of Adolescent Health, 20, 450-458.
Nir, Z., & Neumann, L. (1995). Relationship among self-esteem, internal-external lo-cus of control, and weight change after participation in a weight reduction program.Journal of Clinical Psychology, 52, 482-490.
Nunnally, J. C. (1978). Psychometric Theory. New York: McGraw-Hill Inc.Paine, E. L. (1980). Experienced control and participation in treatment of obesity. Psy-
chology Rep, 47, 709.Parcel, G. S., Edmundson, E., Perry, C. L., Feldman, H. A., O’Hara-Tompkins, N.,
Nader, P. R., Johnson, C. C., & Stone, E. J. Measurement of self-efficacy for diet-related behaviors among elementary school children. Journal of School Health,65(1), 23-27.
Park, C. W., Jaworski, B. J., & MacInnis, D. J. (1986). Strategic brand concept-imagemanagement. Journal of Marketing, 50 (October), 135-146.
Papacharissi, Z., & Rubin, A. (2000). Predictors of Internet Use. Journal of Broadcast-ing & Electronic Media, 44(2), 175-183.
Potter, J. D., Finnegan, J. R., Guinard, J-X et al. (2000). 5 A Day for Better Health Pro-gram Evaluation Report. Bethesda, MD: National Institutes of Health, NationalCancer Institute. November; NIH Publication Number 01-4904.
Riche, M. F. Psychographics for the 1990s. American Demographics, 11(7), 24-31.Rogers, E. M., & Shoemaker, F. F. (1971). Communication of Innovations. New York:
The Free Press.Rubin, A. (1983). Television Uses and Gratifications: The Interactions of Viewing Pat-
terns and Motivations. Journal of Broadcasting, 27, 37-51.Rubin, A., & Rubin, R. (1982). Contextual Age and Television Use. Human Communi-
cation Research, 8, 228-244.Saltzer, E. B. (1982). The weight locus of control (WLOC) Scale: A Specific Measure
for Obesity Research. Journal of Personality Assessment, 46, 620-628.Saturnino-Springer, N., Bogue, E. L., Arnold, M., Yankou, D., & Oakley, D. Nutrition
locus of control and dietary behaviors of pregnant women. Applied Nursing Re-search, 71, 28-31.
100 HEALTH MARKETING QUARTERLY
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014
Stephenson, W. (1967). The play theory of mass communication. Chicago, IL: Univer-sity of Chicago Press.
Story, M., French, S. A., Resnick, M. D., & Blum, R. W. (1997). Ethnic/racial and so-cioeconomic differences in dieting behaviors and body image perceptions in ado-lescents. International Journal of Eating Disorder, 18, 173-179.
Snyder, M. (1974). Self-monitoring of expressive behavior. Journal of Personality andSocial Psychology, 30, 526-537.
Snyder, M., & DeBono, K. G. (1985). Appeals to image and claims about quality: Un-derstanding the psychology of advertising. Journal of Personality and Social Psy-chology, 49, 586-597.
Swenson, M. R., & Wells, W. D. (1995). Target marketing for health communication.Social Marketing Quarterly, 2(1), 5-9.
Tocqueville, A. D. (1999). Democracy in America. New York, NY: Westvaco.Townsend, B. (1987). Market segmentation: Using demographics, psychographics,
and other segmentation techniques to uncover and exploit new markets. AmericanDemographics, 9(6), 10-11.
Urquhart, J. (1999). A Health Food Hits Big Time. The Wall Street Journal, August 3,p. B1.
VAN Beurden, E., James, R., Christian, J., & Church, D. (1991). Dietary self-efficacyin a community-based intervention: Implications for effective dietary counseling.Australian Journal of Nutrition and Diet, 48(2), 64-67.
Wakshlag, J. (1985). Selective Exposure to Educational Television. In D. Zillman, & J.Bryant (Eds.), Selective Exposure to Communication, 63-87.
Wells, W. D. (1989). Planning for R.O.I.: Effective advertising strategy. EnglewoodCliffs, NJ: Prentice-Hall.
Zillman, D., & Bryant, J. (1985). Selective Exposure to Communication. LawrenceErlbaum Associates: Hillsdale, NJ.
RECEIVED: 09/19/02REVISED: 02/02/03
ACCEPTED: 02/20/03
Mohar J. Dutta-Bergman 101
Dow
nloa
ded
by [
Tuf
ts U
nive
rsity
] at
08:
51 0
5 O
ctob
er 2
014