Embed Size (px)
Citation preview

A Failure Analysis of Invasive Breast Cancer
Most Deaths From Disease Occur in Women Not Regularly Screened
Matthew L. Webb, AB1,2; Blake Cady, MD1,2,3,4; James S. Michaelson, PhD1,2,5; Devon M. Bush, JD1;
Katherina Zabicki Calvillo, MD4,6,7; Daniel B. Kopans, MD4,8; and Barbara L. Smith, MD, PhD1,2,4
BACKGROUND: Mortality reduction from mammographic screening is controversial. Individual randomized trials and meta-analyses
demonstrate statistically significant mortality reductions in all age groups invited to screening. In women actually screened, mortality
reductions are greater. Individual trials and meta-analyses show varying rates of mortality reduction, leading to questions about
screening’s value and whether treatment advances have diminished the importance of early detection. This study hypothesized that
breast cancer deaths predominantly occurred in unscreened women. METHODS: Invasive breast cancers diagnosed between 1990
and 1999 were followed through 2007. Data included demographics, mammography use, surgical and pathology reports, and recur-
rence and death dates. Mammograms were categorized as screening or diagnostic based on absence or presence of breast signs or
symptoms, and were substantiated by medical records. Breast cancer deaths were defined after documentation of prior distant me-
tastases. Absence of recurrent cancer and lethal other diseases defined death from other causes. RESULTS: Invasive breast cancer
failure analysis defined 7301 patients between 1990 and 1999, with 1705 documented deaths from breast cancer (n 5 609) or other
causes (n 5 905). Among 609 confirmed breast cancer deaths, 29% were among women who had been screened (19% screen-
detected and 10% interval cancers), whereas 71% were among unscreened women, including >2 years since last mammogram (6%),
or never screened (65%). Overall, 29% of cancer deaths were screened, whereas 71% were unscreened. Median age at diagnosis of
fatal cancers was 49 years; in deaths not from breast cancer, median age at diagnosis was 72 years. CONCLUSIONS: Most deaths
from breast cancer occur in unscreened women. To maximize mortality reduction and life-years gained, initiation of regular screening
before age 50 years should be encouraged. Cancer 2013;000:000-000. VC 2013 American Cancer Society.
KEYWORDS: breast cancer; mortality; mammography; screening; cancer.
INTRODUCTIONEvidence for the benefit of early detection of breast cancer by mammography screening has been substantial1-3 but contro-versial.4-7 Meta-analysis of 8 randomized trials (RCTs) of women offered mammography screening found significantreduction in breast cancer mortality of approximately 20%, but 2 of these 8 trials showed no benefit.1 Meta-analysis of tri-als underestimate true effectiveness of mammography due to compliance and contamination biases in experimental andcontrol groups, respectively.8 Population-based evaluations of women actually screened usually show reductions in mor-tality much greater than those found by RCTs.9-11
Systemic reviews of evidence, however, emphasize results of RCTs over population-based studies.8,12 Meta-analysesof RCTs, which underestimate effectiveness of screening mammography, result in recommendations for national screen-ing guidelines that may not reflect the greater mortality reductions found by long-term follow-up of women actuallyscreened,13 which indicate mortality reductions as good as or better than the highest reductions from RCTs.14,15
One previous retrospective failure analysis of invasive breast cancer revealed that 72% of deaths from diseaseoccurred in the 15% of women not regularly screened.16 To assess the validity of those findings, we conducted a similarfailure analysis of a greater number of cases with longer follow-up. We determined the cause of death and history of mam-mography of women who died following a diagnosis of breast cancer.
Corresponding author: Blake Cady, MD, 24 Walnut Place, Brookline, MA 02445; Fax: (617) 655-2070; [email protected]
1Department of Surgery, Massachusetts General Hospital, Boston, Massachusetts; 2Gillette Center for Breast Cancer, Massachusetts General Hospital, Boston, Mas-
sachusetts; 3Cambridge Breast Center, Cambridge Hospital, Cambridge, Massachusetts; 4Harvard Medical School, Boston, Massachusetts; 5Department of Pathol-
ogy, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts; 6Department of Surgery, Brigham & Women’s Hospital, Boston,
Massachusetts; 7Breast Care Center, Dana-Farber Cancer Institute, Boston, Massachusetts; 8Department of Radiology, Massachusetts General Hospital, Harvard
Medical School, Boston, Massachusetts
We thank Kimberly Sanzi for extensive administrative contribution.
DOI: 10.1002/cncr.28199, Received: January 1, 2013; Revised: March 29, 2013; Accepted: April 22, 2013, Published online Month 00, 2013 in Wiley Online
Library (wileyonlinelibrary.com)
Cancer Month 00, 2013 1
Original Article

MATERIALS AND METHODSTwo hospitals in Boston, Massachusetts General Hospital(MGH) and the Brigham and Women’s Hospital, form alarge part of the Partners HealthCare (PHC) system. Thisstudy was approved by the PHC and MGH institutionalreview boards and adhered to all privacy requirements.Personal data was de-identified; 2 authors (M.L.W.,B.C.) reviewed individual records. Differences in frequen-cies were tested using a 2-sided chi-square test. Differencesin mean or median values were assessed by t test or Wil-coxon rank sum-test where appropriate. Statistical signifi-cance was established at P< .05.
Information collected from medical recordsincluded date of initial histologic diagnosis, demographics(date of birth, age, race, and socioeconomic data), date ofdeath, and pathology data of the primary cancer (maxi-mum diameter, grade, and lymph node status). Proof ofdistant metastatic disease by biopsy, other operation,characteristic radiological pattern, or laboratory or clinicalreports was required for patients to be considered to havelater died of breast cancer. Clinical notes, progress notes,death certificates, hospital discharge summaries, andautopsies consistent with death caused by metastatic dis-ease characterized breast cancer death. Deaths not frombreast cancer were documented if the patient had neverhad recurrence or metastasis by clinical notes, dischargesummaries, death certificate, or autopsy, and the alternatedeath cause was confirmed by chart review. Most cases(88.8%) met these strict criteria for accuracy of cause ofdeath.
Patients determined to be highly likely, but notactually proven, to have died of breast cancer (4.2%) wereso categorized by palpable disease, poor prognostic fea-tures, presence of nodal, local, or systemic recurrence, andfew or no other competing mortality risks. Patients con-sidered to be highly unlikely to have died of breast cancer(7.0%) had early disease with good prognostic features,no evidence of recurrence, and had other diseases withhigh mortality risks, although a precise cause of death wasnot completely documented.
Biennial screening was defined as mammographyperformed at intervals of 2 years or less in the absence ofany breast signs or symptoms. Signs and symptomsincluded any abnormal breast or axillary lymph node find-ings or complaints. Assessment of mammography historyincluded dates and results of each study and was correlatedwith clinical notes, operative reports, and pathologicreports, to classify the presenting breast cancer as non-palpable and asymptomatic (screening mammography) oras palpable and/or symptomatic (diagnostic mammog-
raphy). Interval cancers were defined as symptomatic orpalpable cancers presenting less than 2 years after the pre-vious screening mammogram regardless of age. Twelvepercent of women under 40 had screening mammograms,presumably because of high risk defined by family history,high-risk benign pathology on previous biopsy, BRCAgene abnormalities, or such risk factors. A screening rateof 12% in women younger than 40 years with these riskfactors does not seem unusual in this population, espe-cially considering that these academic referral hospitalshave a larger proportion of high-risk patients.
Mammography screening use in Massachusettswomen was estimated by the Behavioral Risk Factor Sur-veillance System (BRFSS), a biennial random-digit tele-phone survey that includes queries regarding recenthistory of mammography,17 and data local to MGH.18
The PHC cancer registry and breast cancer databasedefined 7301 women diagnosed with potentially curableAmerican Joint Committee on Cancer (AJCC) stage I, II,or III invasive breast cancer from January 1990 throughDecember 1999, and followed through 2007. Duringthat time, 2141 deaths (29.3%) in these women wererecorded in either clinical or hospital records and definedin the Massachusetts Death Registry or the NationalDeath Registry (Table 1).
A total of 436 deaths (20.4%) were excluded fromour analyses (Table 1) because: 1) medical records wereincomplete or inadequate to determine the clinical course,cause of death, or mammography history (n 5 344); 2)another primary invasive breast cancer had been diag-nosed prior or subsequent to 1990 through 1999
TABLE 1. Inclusion Criteria and Characterization ofCauses of Death and Screening History
Characteristic No. (%)
Total no. of patients 7301 (100%)
Deaths 2141 (29.3%)
Patients deaths excluded 436 (20.4%)
Records incomplete or inadequate 344 (78.9%)
Patients with prior or subsequent breast cancer 52 (11.9%)
Patients refused treatment 20 (4.6%)
Patients with noninvasive cancer 11 (2.5%)
Patients with stage IV disease 9 (2.1%)
Confirmed deaths (all causes) 1705 (79.6%)
Deaths not from breast cancer 905 (53.1%)
Deaths unlikely from breast cancer 119 (7.0%)
Deaths confirmed from breast cancer 609 (35.7%)
Deaths likely from breast cancer 72 (4.2%)
Of 609 deaths confirmed from breast cancer:
Deaths from palpable/symptomatic cancer 491 (80.6%)
Deaths from asymptomatic/nonpalpable cancer 118 (19.4%)
Deaths from breast cancer in women not screened 431 (70.9%)
Deaths from breast cancer in women screened 178 (29.2%)
Original Article
2 Cancer Month 00, 2013

(n 5 52); 3) the original registry diagnosis of invasive can-cer, on review, was actually noninvasive ductal carcinomain situ (n 5 11); 4) disease was actually AJCC stage IV(curability rare and survival short) at diagnosis but errone-ously staged otherwise in the registry (n 5 9); or 5) thepatient had refused treatment of a proven breast cancer ora mass present for more than 2 years (n 5 20).
From 1705 cases remaining, our record analysisdefined 609 women who died of breast cancer while 905died of other diseases for a total of 1514 deaths (88.8%);72 (4.2%) deaths were highly likely from breast cancerbut not completely confirmed, and 119 (7.0%) weredeaths highly unlikely to have been from breast cancer butnot completely confirmed (Table 1).
Comparisons of age, pathologic features, and sur-vival found no differences between the 72 patients highlylikely to have died of breast cancer and the 609 confirmedto have died of breast cancer in age (P 5 .055) diameter(P 5 .161), grade (P 5 .912), rate of lymph node metasta-
sis (P 5 .452), or survival (P 5 .478). Similar comparisonof the 119 patients highly unlikely to have died of breastcancer also showed no differences in age (P 5 .298), di-ameter (P 5 .349), grade (P 5 .746), rate of lymph nodemetastasis (P 5 .081), or survival (P 5 .431) to the 905completely documented deaths not from breast cancer(Table 2). By virtue of statistical similarity, includingthese 191 (11.2%) cases in discussions of cause of death(breast cancer or not) did not introduce bias by compara-tive analyses. Thus, we may refer to 681 deaths as arisingfrom breast cancer (39.9%), and 1024 deaths as notrelated to breast cancer (60.1%). However, for detailedanalyses of mammography use, we analyzed only the 609deaths with complete documentation.
RESULTSAmong the 609 women who had completely documenteddeaths from breast cancer (Table 3), there were 118screen-detected cancers that were discovered either at an
TABLE 2. Compares Demographics and Pathological Data by Cause of Death.
All Patients
Patients Provento Have Died ofBreast Cancer
Patients Likelyto Have Died ofBreast Cancer
Patients ProvenNot to Have Diedof Breast Cancer
Patients Unlikelyto Have Died ofBreast Cancer
No. 7301 609 72 905 119
Median age (range), y 55 (20-98) 49 (24-91) 57 (28-89) 72 (26-98) 73 (35-91)
Median size (range), mm 15 (1-400) 25 (1-150) 30 (2-140) 15 (0.4-41) 12 (2-90)
% Grade 3 36.8% 60.5% 60% 22.5% 25.6%
% LN1 35.7% 70.8% 75.4% 36.5% 23.7%
% �4 LN1 13% 37.0% 57.4% 10.8% 4.3%
Median survival (range), y >12.5 (0.01-16.8) 4.6 (0.3-15.5) 4.4 (1.3-14) 8.2 (0.9-16.6) 7.3 (0.01-16.8)
Abbreviations: 1, positive; LN, lymph node.
TABLE 3. Comparison of Demographics and Pathological Data by Screening History
All Patients
Patients Proven toHave Died of
Breast Cancer
Patients Proven to Have Died of Breast Cancer (n 5 609)
Screened Unscreened
Screen-Detected True Interval Off-Program Unscreened
No. 7301 609 118 60 36 395
Percentage of deaths
Median age at diagnosis
(range), y
55 (20-98) 49 (24-91) 60 (32-88) 51.5 (30-81) 51 (35-80) 47 (24-91)
Median mammogram interval
(range), y
1.1 (0.1-2) 0.9 (0.02-2) 3.5 (>2-7.3) Unscreened
Median size (range), mm 15 (1-400) 25 (1-150) 14 (2-65) 25 (1-140) 21 (1-85) 27 (1-150)
Grade 3 36.8% 60.5% 38% 46.4% 65.5% 68.4%
LN1 �1 LN1 35.7% 70.8% 46.7% 72.4% 67.7% 77.7%
�4 LN1 13.0% 37.0% 24.8% 51.7% 25.8% 39.1%
Median survival (range), y >12.5 (0.3-15.5) 4.6 (0.3-15.5) 6.2 (0.7-15.5) 5.6 (1.4-13.8) 4.1 (0.7-12.6) 4.0 (0.3-14.9)
Abbreviations: 1, positive; LN, lymph node.
Most Breast Cancer Deaths Not Screened/Webb et al
Cancer Month 00, 2013 3

initial screening mammogram (n 5 7) or after 2 screeningmammograms separated by 2 years or less (n 5 111).Interval cancers (n 5 60) appeared in women who hadhad at least 1 screening mammogram but presented with apalpable or symptomatic cancer less than 2 years followingthat negative screening mammogram. “Off-program”women (n 5 36) had had at least 1 screening mammo-gram, but their most recent was more than 2 years prior todiagnosis (median 5 3.5 years; range 5 2-7.2 years). Themajority of women who died of breast cancer had neverhad a mammogram prior to diagnosis (n 5 395). For ana-lytical purposes, these 2 latter groups were characterized asunscreened, whereas the screen-detected and interval can-cers were characterized as screened.
Interval cancers made up 34% of all deaths inscreened women, but a strong inverse relationshipbetween age at diagnosis and deaths attributable to aninterval cancer was evident, ie, interval cancers accountedfor 60% of deaths in screened women who were first diag-
nosed before age 40 years, 47% of deaths for women aged40 to 49 years, 28% for women aged 50 to 59 years, 26%for women aged 60 to 69 years, and 24% of deaths inwomen aged 70 years and older.
Table 4 compares the proportion of all 7301 cases,the proportion of all breast cancer deaths, and the propor-tion of all deaths not from breast cancer by age decade atdiagnosis. In addition, the proportions that died of breastcancer or not are described for all women younger than 50years of age and for those in 2 age categories deemedappropriate for screening: 50 to 74 and 40 to 74 years ofage. Table 4 also compares the death rates for breast can-cer deaths and deaths not from breast cancer by age decadeat diagnosis. Death rates are the number of deaths ofwomen diagnosed in a particular age decade divided bythe total number of cases diagnosed at that age decade. Itis noteworthy that 50% of all breast cancer deathsoccurred in women younger than 50 years of age, 69% ofall breast cancer deaths occurred before 60 years of age,whereas 83% of all noncancer deaths occurred after 60.
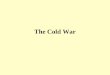
Figure 1 is a histogram demonstrating the numberof patients who died of breast cancer and the number ofpatients who died of other causes by year of age of diagno-sis. Women who died of breast cancer were diagnosed at amedian age of 49 years, whereas women who died of othercauses were diagnosed at median age of 72 years.
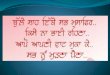
The pie charts of Figure 2 display the proportion ofbreast cancer deaths by age at diagnosis and show that atall age decades, the preponderance of women who diedfrom breast cancer were unscreened at the time ofdiagnosis.
DISCUSSIONPublished estimates of the proportional contribution ofscreening mammography to declining mortality vary
TABLE 4. Comparison of Age at Diagnosis by Cause of Death
Percentage of All BreastCancer Diagnoses by Age
Percentage of Deaths by Age Death Rate by Age
Breast Cancer Non-Breast Cancer Breast Cancer Non-Breast Cancer
All Patients Proven and Likely Proven and Unlikely Proven and Likely Proven and Unlikely
No. 7301 681 1024 681 1024
Age <40 y 10.6% 19.2% 1.1% 16.9% 1.6%
Age 40-49 y 25.2% 30.8% 5.5% 11.4% 3.1%
Age 50-59 y 23.9% 19.4% 10.8% 7.5% 6.5%
Age 60-69 y 20.7% 17.8% 24.6% 8.1% 17%
Age �70 y 19.5% 12.8% 58.0% 6.1% 41.9%
Age <50 y 35.8% 50.0% 6.6% 13.0% 2.6%
Age 40-74 y 78.1% 72.9% 58.8% 8.8% 10.6%
Age 50-74 y 52.9% 42.1% 53.3% 7.6% 14.1%
Figure 1. The ages at diagnosis are shown by cause of death.
Original Article
4 Cancer Month 00, 2013

from none,6 to 33% in a report from Norway,19 to a me-dian of 46% among 7 models published in 2005,20 to anestimated 75% to 80% in a study from the Netherlands.21
The relative contribution of screening mammography toreductions in breast cancer mortality was first reported in200122 and a recent report from Nijmegen, the Nether-lands, demonstrated a 65% mortality reduction inscreened women relative to unscreened women during 16years from 1992 to 2008.15 A report of Swedish servicescreening demonstrated a risk ratio of 0.56 among the85% of women attending service screening comparedwith unscreened women who, despite access to contempo-
rary systemic therapies, had a mortality rate not differentfrom women before the introduction of mammographyin 1978.23 These results support a central role ofmammographic screening and early detection in decliningmortality. Our results reflect effective service screening(screening rate of approximately 80%).24 It should also benoted that during the period of our study, all women(screened and unscreened) had access to contemporary ad-juvant systemic therapy, which was emphasized at our aca-demic centers.
In the presence of conflicting evidence, national rec-ommendations for screening mammography have become
Figure 2. Screening histories at age of diagnosis are shown for all women who died of breast cancer.
Most Breast Cancer Deaths Not Screened/Webb et al
Cancer Month 00, 2013 5

a point of contention.25 Surgical procedures, systemic ad-juvant therapies, and radiation treatments for breast can-cer have changed over recent decades, and as breast cancermortality continues to decline, it is important to deter-mine the proportional decrease in mortality, if any, that isdue to modern mammography.
Our method, a failure analysis, estimated the effectof screening mammography on mortality by review of thescreening histories of women who died from breast can-cer. A previous retrospective failure analysis examinedactual use of screening mammography prior to diagnosisin 207 women who died of breast cancer and found that72% of breast cancer deaths occurred in an estimated15% of unscreened women.16
Among the 609 confirmed deaths from breast cancerin our cohort, 80.6% of women presented with palpableor symptomatic breast cancers, and 19.4% were nonpalp-able or asymptomatic cancers discovered by screeningmammography (Table 3). In this population, in which anestimated 80% of women older than 40 were screened atleast biennially,17 we found that 70.8% of deaths frombreast cancer occurred among the estimated 20% ofwomen who were unscreened (Tables 1 and 3).
The median diameter, grade, and rate of lymph nodemetastasis of breast cancers in women who were unscreenedand died of disease were, as expected, prognostically muchworse than in women who were screened biennially (Table3). Interval cancers that presented symptomatically within2 years of a negative mammogram caused a significant pro-portion (34%) of deaths from breast cancer in screenedwomen: 47% in women aged 40 to 49 years comparedwith only 24% in women older than 69 years. This findingsupports a recommendation for an increased frequency ofscreening in younger women.
Although age-adjusted breast cancer mortality hasbeen declining, it is still the leading cause of prematuremortality among women.26 Among women younger than40 years with invasive breast cancer, the death rate was16.9%, but the death rate from other causes was very low(1.6%). The death rate from other causes rose to 17%between 60 and 69 years, and increased to 42% of womenolder than 69 years. In contrast, the death rate from breastcancer was high in younger women (16.9% and 11.4% inwomen under 40 and between 40 to 49 years, respec-tively) but decreased in older women to 8.1% and 6.1%in women 60 to 69 and� 70 years, respectively (Table 4).These trends are consistent with the decreasing breast can-cer lethality in older ages and competing comorbiditywith older age.27,28 Of all breast cancer deaths, only 13%occurred in women 70 years or older but 50% occurred in
women under age 50; 31% occurred in women initiallydiagnosed between ages 40 and 49 years (Table 4 andFig. 1), an age decade in which mammography screeningis vigorously debated. From their analysis of both mortal-ity and life years gained, the US Preventive Services TaskForce proposed to limit screening to women aged 50 to74 years13,25 biennially despite their own model’s findingof a 70% further improvement in both these outcomeswith annual screening. Our data would by inference sug-gest less or less frequent screening at ages older than 69years, but more or more frequent screening for womenyounger than 50 years. Such less frequent screening inolder women is supported in the literature.24
Such an emphasis is supported by evidence fromRCT trials,29 clinical reports,30 and mathematical model-ing,31,32 each of which show that the biological progres-sion of breast cancer is more rapid in younger patients andthat more deaths could be avoided by more frequentmammography screening in younger women. The cost-effectiveness of screening may also be improved if screen-ing were to begin at age 40 or 45 years rather than at 50years,24,33 in part because screening younger womenresults in greater salvage of disease-free life years.
Unfortunately, shared decision-making narrativestend to emphasize the harms of screening rather than thebenefits. Indeed, it may even be difficult to discuss the pri-mary advantage of screening, namely, early discovery ofcancer, as a benefit. Participating in mammography canbe likened to purchasing home insurance.34 The insuredpay a premium, despite the rarity that they ever file aclaim. In the event of disaster, however, the insured areprotected from financial ruin. Likewise, all suitably agedwomen should participate in mammography screeningeven though only a few will ever develop breast cancer. Inthe event of the diagnosis of breast cancer, however, thedisaster of death is largely avoided due to early detection.Our study found that most women who died of breastcancer had not been screened.
Several criticisms can be made of our study. In ourmedical record analysis, we did not examine cancer treat-ments or their bearing on mortality. It was assumed thatsurgery, systemic adjuvant therapy, and radiation treat-ments corresponded with standards for primary, recur-rent, and metastatic breast cancer treatment during thestudied decade in our academic hospitals and not on thebasis of whether a breast cancer was detected symptomati-cally or by screening. We acknowledge that systemic adju-vant therapy may prevent many deaths,19-21,23 and thatadvances in adjuvant therapy have contributed to declin-ing mortality from breast cancer, but in our data, the
Original Article
6 Cancer Month 00, 2013

proportional mortality decrease due to adjuvant therapycould not be estimated.
There have been investigations of differences inbreast cancer diagnosis,35 treatment,36 and survival37 cor-related with socioeconomic status. We did not find differ-ences in breast cancer mortality between women ofdiffering race, ethnicity, or socioeconomic status, but ourcohort was predominantly white (90%), of high socioeco-nomic status (median household income of $52,425),and received care at academic hospitals.
Our estimation of the prevalence of biennial screen-ing in Massachusetts between 1990 and 1999 was fromthe BRFSS, which may overestimate screening rates by asmuch as 20%.28,38 PHC patients are, however, generallyof high educational and socioeconomic status, both ofwhich are correlated with greater rates of screening,39,40
and mammography screening is strongly emphasized andhighly used in PHC facilities; a study at MGH estimatedthe rate of screening in women older than 40 years to be80%, consistent with the BRFSS survey (J. S. Michaelson,unpublished data).
Data derived from death registries are not free fromerrors.41 We therefore used multiple sources of confirma-tory information from the cancer registry, discharge sum-maries, office notes, hospital notes, and autopsies tominimize incorrect designation of cause of death. Despiteconfirmatory information, however, some errors are stillpossible.
Breast cancer mortality in 7301 women with inva-sive breast cancer diagnosed between 1990 and 1999 wasonly 9.3% at a median of 12.5 years, compared to the50% mortality before 1969. The American Cancer Soci-ety predicted that a 50% age-adjusted mortality reductioncould be achieved by 2015 compared with mortality ratefrom 1991 (from 32.7 to 16.4 per 100,000 per year) ifscreening and therapeutic guidelines were followed.42 Theaverage percentage change in age-adjusted mortality hasbeen declining by about 2% per year43 and may well meetthat goal; recent follow-up of the Two-County trial showsthat follow-up of 20 years or more may be necessary tomeasure the full impact of screening.3
Our study emphasizes that palpable breast cancersremain the major challenge to efforts to reduce breast can-cer mortality. Programs to achieve regular screening in allappropriately aged women should be encouraged.Although palpable breast cancers still occur as intervalcancers among women who have undergone screening,palpable or symptomatic cancers account for essentiallyall deaths in women who have not attended screening.With more prevalent regular screening, particularly in
younger women, breast cancer mortality may decrease tomuch less than 10% overall (age-adjusted rate of 6.5 per100,000 per year) in the coming decade, as seen in ourpatients, and perhaps as low as 5% overall by 2030.
CONCLUSIONSThis analysis of deaths following diagnosis of invasivebreast cancer found that the majority of deaths frombreast cancer now occur in the minority of women notregularly screened. Even with effective adjuvant therapies,the best method for women to avoid death from breastcancer is to participate in regular mammography screen-ing. Regular screening increases the likelihood of detect-ing nonpalpable cancers, and annual screening furtherincreases that likelihood relative to biennial screening.Furthermore, detecting and treating breast cancer inyounger women to prevent death may further increase thedisease-free life years saved.24,30-33 Our findings suggestdecreasing the intensity of efforts to screen women olderthan 69 years while concomitantly emphasizing efforts toscreen younger women in particular.
FUNDING SOURCESNo specific funding was disclosed.
CONFLICT OF INTEREST DISCLOSUREThe authors made no disclosure.
REFERENCES1. Smith RA, Duffy SW, Gabe R, et al. The randomized trials of breast
cancer screening: what have we learned? Radiol Clin North Am.2004;42:793-806.
2. Tab�ar L, Duffy SW, Vitak B, et al. The natural history of breast car-cinoma: what have we learned from screening? Cancer. 1999;86:449-462.
3. Tab�ar L, Vitak B, Chen TH, et al. Swedish two-county trial: impactof mammographic screening on breast cancer mortality during 3decades. Radiology. 2011;260:658-663.
4. G�tzsche PC, Olsen O. Is screening for breast cancer with mam-mography justifiable? Lancet. 2000;355:129-134.
5. G�tzsche PC. Relation between breast cancer mortality and screen-ing effectiveness: systematic review of the mammography trials. DanMed Bull. 2011;58:A4246.
6. Autier P, Boniol M, Gavin A, et al. Breast cancer mortality in neigh-bouring European countries with different levels of screening butsimilar access to treatment: trend analysis of WHO mortality data-base. BMJ. 2011;343:d4411.
7. Welch HG. Screening mammography--a long run for a short slide?N Engl J Med. 2010;363:1276-1278.
8. Nelson HD, Fu R, Griffin JC, et al. Systematic review: comparativeeffectiveness of medications to reduce risk for primary breast cancer.Ann Intern Med. 2009;151:703-715, W-226-735.
9. Moss SM, Cuckle H, Evans A, et al. Effect of mammographicscreening from age 40 years on breast cancer mortality at 10 years’follow-up: a randomised controlled trial. Lancet. 2006;368:2053-2060.
10. Hellquist BN, Duffy SW, Abdsaleh S, et al. Effectiveness ofpopulation-based service screening with mammography for womenages 40 to 49 years: evaluation of the Swedish Mammography
Most Breast Cancer Deaths Not Screened/Webb et al
Cancer Month 00, 2013 7

Screening in Young Women (SCRY) cohort. Cancer. 2011;117:714-722.
11. Coldman A, Phillips N, Warren L, et al. Breast cancer mortality af-ter screening mammography in British Columbia women. Int J Can-cer. 2007;120:1076-1080.
12. Tonelli M, Gorber SC, Joffres M, et al. Recommendations onscreening for breast cancer in average-risk women aged 40-74 years.CMAJ. 2011;183:1991-2001.
13. USPSTF. Screening for breast cancer: U.S. Preventive Services TaskForce recommendation statement. Ann Intern Med. 2009;151:716-726, W-236.
14. Swedish Organized Service Screening Evaluation Group. Reductionin breast cancer mortality from organized service screening withmammography: 1. Further confirmation with extended data. CancerEpidemiol Biomarkers Prev. 2006;15:45-51.
15. van Schoor G, Moss SM, Otten JD, et al. Increasingly strong reduc-tion in breast cancer mortality due to screening. Br J Cancer. 2011;104:910-914.
16. Spencer DB, Potter JE, Chung MA, et al. Mammographic screeningand disease presentation of breast cancer patients who die of disease.Breast J. 2004;10:298-303.
17. Centers for Disease Control and Prevention. Self-reported use ofmammography among women aged > or 5 40 years -- UnitedStates, 1989 and 1995. MMWR Morb Mortal Wkly Rep. 1997;46:937-941.
18. Michaelson J, Satija S, Moore R, et al. The pattern of breast cancerscreening utilization and its consequences. Cancer. 2002;94:37-43.
19. Kalager M, Zelen M, Langmark F, et al. Effect of screening mam-mography on breast-cancer mortality in Norway. N Engl J Med.2010;363:1203-1210.
20. Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening andadjuvant therapy on mortality from breast cancer. N Engl J Med.2005;353:1784-1792.
21. Vervoort MM, Draisma G, Fracheboud J, et al. Trends in the usageof adjuvant systemic therapy for breast cancer in the Netherlandsand its effect on mortality. Br J Cancer. 2004;91:242-247.
22. Tab�ar L, Vitak B, Chen HH, et al. Beyond randomized controlledtrials: organized mammographic screening substantially reducesbreast carcinoma mortality. Cancer. 2001;91:1724-1731.
23. Tabar L, Yen MF, Vitak B, et al. Mammography service screeningand mortality in breast cancer patients: 20-year follow-up before andafter introduction of screening. Lancet. 2003;361:1405-1410.
24. Michaelson JS, Kopans DB, Cady B. The breast carcinoma screeninginterval is important. Cancer. 2000;88:1282-1284.
25. Kopans DB. The 2009 U.S. Preventive Services Task Force guide-lines ignore important scientific evidence and should be revised orwithdrawn. Radiology. 2010;256:15-20.
26. Savidan A, Junker C, Cerny T, et al. Premature deaths in Switzer-land from 1995-2006: causes and trends. Swiss Med Wkly. 2010;140:w13077.
27. Bush D, Smith B, Younger J, et al. The non-breast-cancer death rateamong breast cancer patients. Breast Cancer Res Treat. 2011;127:243-249.
28. Mell LK, Jeong JH, Nichols MA, et al. Predictors of competingmortality in early breast cancer. Cancer. 2010;116:5365-5373.
29. Michaelson JS, Satija S, Kopans D, et al. Gauging the impact ofbreast carcinoma screening in terms of tumor size and death rate.Cancer. 2003;98:2114-2124.
30. Hunt KA, Rosen EL, Sickles EA. Outcome analysis for womenundergoing annual versus biennial screening mammography: a reviewof 24,211 examinations. AJR Am J Roentgenol. 1999;173:285-289.
31. Michaelson JS, Halpern E, Kopans DB. Breast cancer: computersimulation method for estimating optimal intervals for screening. Ra-diology. 1999;212:551-560.
32. Kopans DB, Rafferty E, Georgian-Smith D, et al. A simple model ofbreast carcinoma growth may provide explanations for observations ofapparently complex phenomena. Cancer. 2003;97:2951-2959.
33. Carles M, Vilaprinyo E, Cots F, et al. Cost-effectiveness of earlydetection of breast cancer in Catalonia (Spain). BMC Cancer. 2011;11:192.
34. Sasieni PD. Outcomes of screening to prevent cancer: think ofscreening as insurance. BMJ. 2003;327:50.
35. Lobb R, Ayanian JZ, Allen JD, et al. Stage of breast cancer at diag-nosis among low-income women with access to mammography.Cancer. 2010;116:5487-5496.
36. Coburn N, Fulton J, Pearlman DN, et al. Treatment variation by in-surance status for breast cancer patients. Breast J. 2008;14:128-134.
37. Sprague BL, Trentham-Dietz A, Gangnon RE, et al. Socioeconomicstatus and survival after an invasive breast cancer diagnosis. Cancer.2011;117:1542-1551.
38. Cronin KA, Miglioretti DL, Krapcho M, et al. Bias associated withself-report of prior screening mammography. Cancer Epidemiol Bio-markers Prev. 2009;18:1699-1705.
39. Breen N, Gentleman JF, Schiller JS. Update on mammographytrends: comparisons of rates in 2000, 2005, and 2008. Cancer.2011;117:2209-2218.
40. Gilliland FD, Joste N, Stauber PM, et al. Biologic characteristics ofinterval and screen-detected breast cancers. J Natl Cancer Inst. 2000;92:743-749.
41. McGarvey PB, Ladwa S, Oberti M, et al. Informatics and data qual-ity at collaborative multicenter Breast and Colon Cancer FamilyRegistries. J Am Med Inform Assoc. 2012;19:e125-e128
42. Byers T, Mouchawar J, Marks J, et al. The American Cancer Societychallenge goals. How far can cancer rates decline in the U.S. by theyear 2015? Cancer. 1999;86:715-727.
43. Siegel R, Ward E, Brawley O, et al. Cancer statistics, 2011: theimpact of eliminating socioeconomic and racial disparities on prema-ture cancer deaths. CA Cancer J Clin. 2011;61:212-236.
Original Article
8 Cancer Month 00, 2013