Embed Size (px)
Citation preview
ACADEMIC EMERGENCY MEDICINE • August 1999, Volume 6, Number 8 823
A Health Promotion Intervention for Families in aMedicaid Managed Care Plan
VIDYA T. CHANDE, MD, DEANA KIMES, BA
Abstract. Objective: To determine whether imple-mentation of an intervention based on a model ofhealth promotion will encourage patients to seek carefrom their primary care provider (PCP) and reducevisits to the pediatric ED (PED) for minor illness.Methods: Prospective, randomized, controlled studyin the PED of an urban children’s hospital (CH). Chil-dren <13 months old, enrolled in a Medicaid managedcare plan, who identified the CH as their site for pri-mary care and presented to the PED for evaluationof minor illness were enrolled after being seen by thetriage nurse, before being seen by a physician. Sub-jects were randomly assigned to the intervention (I)group or control (C) group. Parents of all enrolleescompleted a survey about health care utilization hab-its. Each family in the I group received health pro-motion teaching from a single investigator. The in-tervention consisted of a review of the child’s medicalrecord with the parents, an explanation of what toexpect at future well-child visits, and a discussion ofthe role of the PCP. A follow-up appointment was alsoprovided prior to discharge from the PED. The Cgroup received usual care. Use of health care by allsubjects was tracked for one year by medical recordreview and phone interviews at six and 12 months.Results: 102 subjects in the I group and 93 in the C
group (mean 6 SD ages 6.4 months 6 3.8 and 7.2months 6 3.9, respectively, p = 0.15) were enrolledfrom March 1996 to November 1996. The two groupswere similar with respect to demographics and over-all health status at enrollment. At study entry: 94 of102 (92%) subjects in I and 87 of 93 (94%) in C hadmade at least one visit to the PED in the previous 12months (p = 0.11); 95 of 102 (93%) in I and 75 of 93(81%) in C had seen their PCP at least once for well-child care (p = 0.24). Twelve-month follow-up by med-ical record review was completed for all subjects;phone interviews were completed in 90 of 102 (88%)in I and 80 of 93 (86%) in C. At 12-month follow-up:84 of 102 (82%) in I and 73 of 93 (78%) in C had madeat least one visit to the PED (p = 0.59); 81 of 102(79%) in I and 77 of 93 (83%) in C had made at leastone visit to their CH PCP (p = 0.54). Conclusions:
There was no difference in health care utilization be-tween the intervention and control groups at 12-month follow-up. The health promotion interventiondid not alter utilization habits. Key words: emer-gency department utilization; managed care; healthpromotion; Medicaid; managed care; pediatrics; uti-lization. ACADEMIC EMERGENCY MEDICINE1999; 6:823–827
OVER THE past several years there has beenincreasing pressure from health insurance
agencies to keep patients with minor illness out ofEDs and to promote use of the primary care pro-vider (PCP). Several investigators have attemptedto reduce use of the ED by providing families withadditional education and support.1–4 These studieshave had mixed results, but in general, have notaltered long-term health care utilization habits.Additionally, a study by Gadomski et al. found thatturning away Medicaid patients who came to the
From the Department of Pediatrics, University of Pittsburgh(VTC) and Children’s Hospital of Pittsburgh (VTC, DK), Pitts-burgh, PA. Current affiliation: Children’s Memorial Hospital,Northwestern University Medical School (VTC), Chicago, IL.Received January 27, 1999; revision received March 8, 1999;accepted March 31, 1999. Presented at the American Academyof Pediatrics Section on Emergency Medicine meeting, SanFrancisco, CA, October 1998.Address for correspondence and reprints: V. T. Chande, MD,Children’s Memorial Hospital, 2300 Children’s Plaza, Box 62,Chicago, IL 60614. Fax: 773-880-8267; e-mail: [email protected]
ED for minor illness did not alter their ED utili-zation patterns5; patients continued to use the EDfor future illnesses.
Most states have at least some patients coveredby Medicaid managed care plans, and 17 stateshave statewide programs.6 Some of the Medicaidmanaged care plans that have been implementedacross the country have shown a decrease in EDutilization.7 However, plans in which a hospitaloutpatient clinic uses the ED for after-hours cov-erage have shown very small decreases in ED vis-its.8–11
Children’s Hospital of Pittsburgh expanded thehours of its Primary Care Center in response tothe pressure to increase availability of the PCP. Werecognized that simply expanding the hours thatthe PCP was available without providing any otherintervention was unlikely to alter use of the EDand designed this health promotion intervention tocoincide with the expansion of the primary careservices. By combining a health promotion inter-vention with increased availability of the PCP, we

824 HEALTH PROMOTION Chande, Kimes • HEALTH PROMOTION INTERVENTION
had the greatest opportunity to alter health careutilization patterns of families with young chil-dren.
In general, altering patients’ health behavior isa complex task. Green and Kreuter developed amodel, called the PRECEDE–PROCEED model,that addresses the factors involved in health be-havior.12 PRECEDE is an acronym for predispos-ing, reinforcing, and enabling causes in educa-tional diagnosis and evaluation, and PROCEEDstands for policy, regulatory, and organizationalconstructs in educational and environmental de-velopment. The model addresses the use of com-prehensive planning and encourages us to examinedesired outcomes closely and to understand whypatients behave the way they do, before imple-menting measures to alter their behavior. Themodel describes multiple factors that influencehealth behaviors, including predisposing factorssuch as knowledge, attitudes, and values, enablingfactors such as availability of resources, and rein-forcing factors such as the attitudes of health per-sonnel, peers, and parents. The model also recog-nizes the role of epidemiologic and social factors inhealth behaviors and has been applied to adult pa-tients.13–15 To date, the majority of interventionsdesigned to decrease ED utilization and encourageuse of the PCP have focused primarily on eitherpredisposing factors (educational interventions) orenabling factors (building new health centers).Green and Kreuter’s model suggests that an inter-vention that focuses on predisposing, reinforcing,and enabling factors simultaneously is most likelyto succeed at altering patients’ health behavior.
The goal of our study was to test the effective-ness of a health promotion intervention based onthe PRECEDE–PROCEED model at alteringhealth care utilization habits of young children en-rolled in a Medicaid managed care plan. The studytested the following hypotheses: the interventionwould reduce ED visits for minor illness and wouldincrease visits to the PCP for well-child care andminor illness.
METHODS
Study Design. This prospective, randomized,controlled study was conducted from March 1996through December 1997. The hospital’s institu-tional review board approved the protocol.
Study Setting and Population. Children lessthan 13 months old who identified Children’s Hos-pital of Pittsburgh as their site for primary carethrough one of the two existing Medicaid managedcare plans and presented to the ED for evaluationof minor illness were eligible for the study. Thestudy was limited to young children because they
need the highest number of visits per year for well-child care and immunizations. Patients with minorillnesses were defined as those children triaged bythe nurse as having ‘‘nonurgent illness,’’ based onestablished ED triage criteria.
Study Protocol. Patients were enrolled after be-ing seen by the triage nurse, while waiting in anexamination room to be seen by a physician. Con-sent to participate in the study was obtained fromthe parent/guardian. Parents were told that theywould need to complete a survey for the study andthat their child’s medical records would be re-viewed several times over the year to follow utili-zation of services at Children’s Hospital. Theywere not told that the objective of the study wasto alter health care utilization patterns. Subjectswere recruited Monday through Friday 8 AMthrough 5 PM because those are the hours that thePrimary Care Center was open before the ex-panded hours were implemented and the patientscould have been seen by their PCP. Patients com-ing to the ED during evening and night hours werenot included because their reasons for coming tothe ED might have been different from those ofpatients who come during the daytime, thus con-founding results. Patients presenting to the EDwith severe illness or injury were excluded fromthe study. Families without access to a phone werenot eligible for the study. Sample size calculationswere based on a previous study,11 which led us toexpect that 75% of patients in the control groupwould make two or more visits to the ED duringthe one-year follow-up period. We expected a 20%decrease in ED visits in the intervention group.3,11
Assuming alpha = 0.05 and beta = 0.2, we needed100 patients in each group.
Patients were randomly assigned to the inter-vention or control group. Randomization was donewith a table of random numbers. All families wereasked to complete a survey about their health careutilization habits. Medical records of all the sub-jects were reviewed to document presence ofchronic illness and immunization status. Chronicillness was defined as a medical condition that re-quires continuous medical care, such as asthma orseizure disorder. Immunization status was deter-mined by using the American Academy of Pediat-rics standards in place at the time of the study,which included the administration of diphtheria–tetanus–pertussis vaccine (DTP) at ages 2, 4, 6,and 18 months, oral polio vaccine (OPV) at ages 2,4, and 18 months, measles–mumps–rubella vac-cine (MMR) by 15 months, Hemophilus influenzaeb vaccine at ages 2, 4, 6, and 15 months, and threehepatitis B vaccines by 18 months.16
Each family in the intervention group receivedthe health promotion intervention from a single in-
ACADEMIC EMERGENCY MEDICINE • August 1999, Volume 6, Number 8 825
TABLE 1. Patient Characteristics
InterventionGroup
(n = 102)
ControlGroup
(n = 93) p-value
Age—mean 6 SD 6.4 6 3.8months
7.2 6 3.9months
0.15
Gender—male 55 (54%) 56 (60%) 0.78
RaceWhite 18 (18%) 10 (11%)African American 73 (72%) 78 (84%) 0.15Other 10 (10%) 4 (4%)
Single-mother house-hold 87 (85%) 75 (81%) 0.45
Mother’s education11th grade 16 (16%) 16 (17%)High school graduate 29 (28%) 31 (33%) 0.58Attended/in college 40 (39%) 30 (33%)Unknown 17 (17%) 16 (17%)
Presence of chronic ill-ness 5 (5%) 7 (8%) 0.56
vestigator (DK). The investigator spent approxi-mately 20–30 minutes with each family in the in-tervention group. The intervention was designed toaffect the factors identified by Green and Kreuter’sPRECEDE–PROCEED model. The interventionconsisted of a detailed review of the child’s medicalrecord with the parents, an explanation of what toexpect at future well-child visits, and a discussionof the role of the PCP. Parents were reminded ofthe importance of continuous health care, includ-ing immunizations, preventive care, and sick vis-its, from their PCP and were reminded to call theirPCP when their child became ill, rather than goingdirectly to the ED. Families were informed thatthe Primary Care Center’s hours were being ex-panded so that children with minor illness couldbe seen during evening and weekend hours. Theywere also given a phone number they could call 24hours a day for advice from their PCP (or his orher on-call colleague). Parents were encouraged toask any questions they had about accessing theirPCP. The patients were given a follow-up appoint-ment with their PCP and the parents were advisedof the importance of keeping the appointment. Pa-tients in the control group did not receive thehealth promotion intervention and did not have afollow-up appointment scheduled.
Several systems changes were implemented inthe Primary Care Center during the study period.The hours of operation were expanded to 8 AM to8 PM on weekdays and 9 AM to 2 PM on Saturdays.Additional pediatric faculty and nurse practition-ers staffed the Primary Care Center so that walk-in patients could be seen more efficiently. A nurse-run, physician-directed (VTC) telephone triageprogram was implemented for evening, night, andweekend coverage of the Primary Care Center.Families who called the center after-hours weregiven advice by a trained nurse who could also givethem an appointment with their PCP for the nextday.
Measurements. Use of health care by all enrolledchildren was followed for one year by medical rec-ord review and phone follow-up. Visits to the Chil-dren’s Hospital of Pittsburgh PCP and ED weredocumented. For ED visits, severity of illness wasdetermined by using the visit codes marked by theED attending physician. The visits are routinelycategorized from 1 to 5, with 1 representing minorproblems such as diaper rash or head lice, 2 beinglow-severity problems such as otitis media or im-petigo, 3–4 representing moderate to severe illnesssuch as asthma or fever in a neonate, and 5 rep-resenting a life-threatening emergency such as de-hydration with shock. The ED faculty had been us-ing this method of coding for three years withreasonable consistency from person to person (in-
terrater reliability testing on a sample of tencharts showed kappa = 0.65).
Phone follow-up was conducted at three, six,nine, and 12 months. The three- and nine-monthcalls were very brief and were limited to verifyingthe subjects’ home phone numbers and trackingthe sample. At the six- and twelve-month calls, theinterviewer asked the parents about intercurrentillness and visits to any health care facility. Par-ents were asked about visits to other EDs duringthe follow-up period. Disenrollment/enrollmentfrom one insurance plan to the other was deter-mined, as was change in PCP.
Data Analysis. Data were analyzed using Epis-tat computer software (Epistat, Richardson, TX).Comparison of continuous variables between thecontrol and intervention groups was done withStudent’s t-test. Comparison of dichotomous vari-ables was done with chi-square analysis. Contin-uous data were analyzed by Mann-Whitney U test.A value of p < 0.05 was considered statistically sig-nificant.
RESULTS
Two hundred twenty-one patients were ap-proached for enrollment in the study from March1996 to November 1996; 195 of 221 gave consentto participate in the study. The most common rea-son for refusal was ‘‘not enough time.’’ All familiesapproached for the study reported access to aphone in their home. Of the 195 families who con-sented to participate in the study, 102 were ran-domly assigned to the intervention group and 93to the control group. Table 1 shows the character-
826 HEALTH PROMOTION Chande, Kimes • HEALTH PROMOTION INTERVENTION
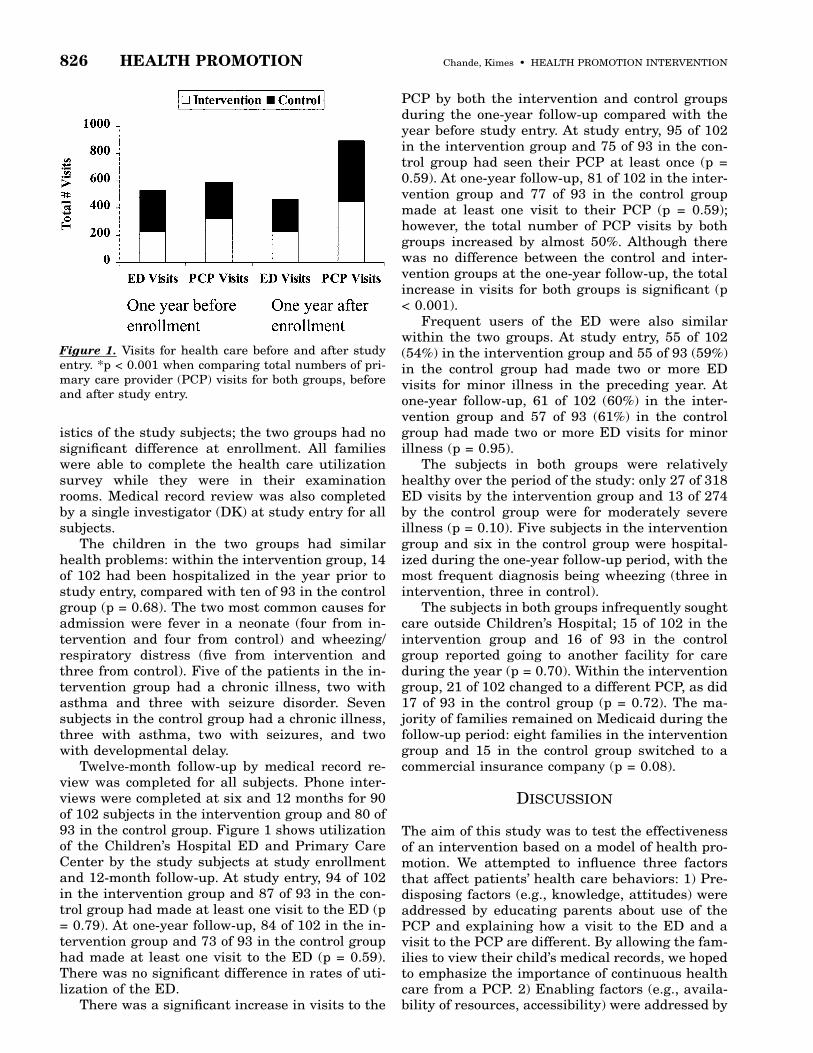
Figure 1. Visits for health care before and after studyentry. *p < 0.001 when comparing total numbers of pri-mary care provider (PCP) visits for both groups, beforeand after study entry.
istics of the study subjects; the two groups had nosignificant difference at enrollment. All familieswere able to complete the health care utilizationsurvey while they were in their examinationrooms. Medical record review was also completedby a single investigator (DK) at study entry for allsubjects.
The children in the two groups had similarhealth problems: within the intervention group, 14of 102 had been hospitalized in the year prior tostudy entry, compared with ten of 93 in the controlgroup (p = 0.68). The two most common causes foradmission were fever in a neonate (four from in-tervention and four from control) and wheezing/respiratory distress (five from intervention andthree from control). Five of the patients in the in-tervention group had a chronic illness, two withasthma and three with seizure disorder. Sevensubjects in the control group had a chronic illness,three with asthma, two with seizures, and twowith developmental delay.
Twelve-month follow-up by medical record re-view was completed for all subjects. Phone inter-views were completed at six and 12 months for 90of 102 subjects in the intervention group and 80 of93 in the control group. Figure 1 shows utilizationof the Children’s Hospital ED and Primary CareCenter by the study subjects at study enrollmentand 12-month follow-up. At study entry, 94 of 102in the intervention group and 87 of 93 in the con-trol group had made at least one visit to the ED (p= 0.79). At one-year follow-up, 84 of 102 in the in-tervention group and 73 of 93 in the control grouphad made at least one visit to the ED (p = 0.59).There was no significant difference in rates of uti-lization of the ED.
There was a significant increase in visits to the
PCP by both the intervention and control groupsduring the one-year follow-up compared with theyear before study entry. At study entry, 95 of 102in the intervention group and 75 of 93 in the con-trol group had seen their PCP at least once (p =0.59). At one-year follow-up, 81 of 102 in the inter-vention group and 77 of 93 in the control groupmade at least one visit to their PCP (p = 0.59);however, the total number of PCP visits by bothgroups increased by almost 50%. Although therewas no difference between the control and inter-vention groups at the one-year follow-up, the totalincrease in visits for both groups is significant (p< 0.001).
Frequent users of the ED were also similarwithin the two groups. At study entry, 55 of 102(54%) in the intervention group and 55 of 93 (59%)in the control group had made two or more EDvisits for minor illness in the preceding year. Atone-year follow-up, 61 of 102 (60%) in the inter-vention group and 57 of 93 (61%) in the controlgroup had made two or more ED visits for minorillness (p = 0.95).
The subjects in both groups were relativelyhealthy over the period of the study: only 27 of 318ED visits by the intervention group and 13 of 274by the control group were for moderately severeillness (p = 0.10). Five subjects in the interventiongroup and six in the control group were hospital-ized during the one-year follow-up period, with themost frequent diagnosis being wheezing (three inintervention, three in control).
The subjects in both groups infrequently soughtcare outside Children’s Hospital; 15 of 102 in theintervention group and 16 of 93 in the controlgroup reported going to another facility for careduring the year (p = 0.70). Within the interventiongroup, 21 of 102 changed to a different PCP, as did17 of 93 in the control group (p = 0.72). The ma-jority of families remained on Medicaid during thefollow-up period: eight families in the interventiongroup and 15 in the control group switched to acommercial insurance company (p = 0.08).
DISCUSSION
The aim of this study was to test the effectivenessof an intervention based on a model of health pro-motion. We attempted to influence three factorsthat affect patients’ health care behaviors: 1) Pre-disposing factors (e.g., knowledge, attitudes) wereaddressed by educating parents about use of thePCP and explaining how a visit to the ED and avisit to the PCP are different. By allowing the fam-ilies to view their child’s medical records, we hopedto emphasize the importance of continuous healthcare from a PCP. 2) Enabling factors (e.g., availa-bility of resources, accessibility) were addressed by

ACADEMIC EMERGENCY MEDICINE • August 1999, Volume 6, Number 8 827
providing families with a 24 hour-a-day phonenurse to provide advice and appointments at timesthat were convenient to them. 3) Reinforcing fac-tors (e.g., attitudes and behaviors of health person-nel and peers) were addressed by providing afriendly environment in which the families couldask questions about their child’s health and by in-creasing physician staff in the Primary Care Cen-ter. The hours that the PCP was available to seepatients was also extended to evenings and week-ends. By addressing these factors, we hoped tomaximize the impact of our intervention.
This study found no difference in utilization ofhealth care services between the control and inter-vention groups. Both groups continued to use theED for minor illness. There was an increase inPCP visits by both groups, which is possibly re-lated to improved access to the Primary Care Cen-ter and may reflect families’ increased willingnessto see the PCP for minor illness if the hours ofoperation are convenient.
LIMITATIONS AND FUTURE QUESTIONS
The main limitation of this study was our inabilityto keep the intervention and control groups trulyseparate during the one-year follow-up period. Theeducational component of the intervention oc-curred in the ED while families were in the ex-amination room to ensure privacy. However, thisstudy group of mostly single, African Americanmothers on Medicaid may have had social contactand could have exchanged information. Similarly,although only the intervention group was informedin detail about the telephone triage system and theexpanded clinic hours, all the families probablycame to know about these changes over time.Therefore, we speculate that in effect we had onlyone group, with utilization measured before andafter the intervention.
CONCLUSIONS
Results of this study suggest that patients on Med-icaid are unlikely to change their health careutilization habits even when a health promotion
intervention is applied. These findings, in conjunc-tion with previous studies,1–4 support the impor-tance of structuring ED services in a manner thatallows patients with minor illness to be seen effi-ciently.
The authors gratefully acknowledge project support from theChildren’s Hospital of Pittsburgh.
References
1. Shields MC, Griffin KW, McNabb WL. The effect of a patienteducation program on emergency room use for inner-city chil-dren with asthma. Am J Public Health. 1990; 80:36–8.2. Lewis CE, Rachelefsky G, Lewis MA, dela Sota A, KaplanM. A randomized trial of A.C.T. (asthma care training) for kids.Pediatrics. 1984; 74:478–86.3. Chande VT, Exum V. Follow-up phone calls after an emer-gency department visit. Pediatrics. 1994; 93:513–4.4. Chande VT, Wyss N, Exum V. An educational interventionto alter emergency department utilization habits. Arch PediatrAdolesc Med. 1996; 150:525–8.5. Gadomski AM, Perkis V, Horton L, Cross S, Stanton B. Di-verting managed care medicaid patients from pediatric emer-gency department use. Pediatrics. 1995; 95:170–8.6. American Academy of Pediatrics, Committee on ChildHealth Financing. Emergency Medical Services for Childrenand Managed Care. Elk Grove Village, IL: American Academyof Pediatrics, 1997.7. Hurley RE, Freund DA, Paul JE. Managed Care in Medi-caid. Ann Arbor, MI: Health Administration Press, 1993.8. Butx AM, Funkhouser A, Caleb L. Infant health care utili-zation predicted by pattern of prenatal care. Pediatrics. 1993;92:50–4.9. Hurley RE, Freund DA, Taylor D. Emergency room use andprimary care case management: evidence from four Medicaiddemonstration programs. Am J Public Health. 1989; 79:843–6.10. Glotzer D, Sager A, Socolar D, Weitzman M. Prior approvalin the pediatric emergency room. Pediatrics. 1991; 88:674–80.11. Chande VT. Effects of a new fee-for-service Medicaid man-aged care plan on pediatric emergency department utilization.Ambulatory Child Health. 1997; 3:269–74.12. Green LW, Kreuter MW. Health Promotion Planning: AnEducational and Environmental Approach. Mountain View,CA: Mayfield Publishing Co., 1991.13. Taylor VM, Taplin SH, Urban N, Mahlach J, Majer KA.Medical Community Involvement in a Breast Cancer ScreeningPromotional Project. Public Health Rep. 1994; 109:491–9.14. Eriksen MP, Green LW, Fultz FG. Principles of changinghealth behavior. Cancer. 1988; 62(8 suppl):1768–75.15. Green LW, Wilson AL, Lovato CY. What changes canhealth promotion achieve and how long do these changes last?The trade-off between expediency and durability. Prev Med.1986; 15:508–21.16. Committee on Infectious Diseases American Academy ofPediatrics. 1994 Red Book Report of the Committee on Infec-tious Diseases, Twenty-third Edition. Elk Grove Village, IL:American Academy of Pediatrics, 1994.