Embed Size (px)
Citation preview

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
A Longitudinal Cephalometric Study FromAge 5 to 18 Years on Individuals With Complete
Bilateral Cleft Lip and Palate
Wanda Maria Gnoinski, DMD and Gordian Rutz, DMD
Abstract: Development of the facial profile between the age of5 years and the end of pubertal growth in patients with completebilateral cleft lip and palate was studied by means of cephalometricradiographs obtained at the age of 5, 10, and 15 years as well as atthe end of the growth period. All 29 patients had been treatedaccording to the same plan and operated on by the same surgeon.
Values for the ANB angle are typically very high in 5-year-oldchildren and then decrease to values corresponding to those of thegeneral population by the end of the pubertal growth period. Verticaldevelopment maintains the initial pattern; no compensatory verticalexcess was observed. Owing to the wide range in all measurements,age-related mean values in a patient sample are of little consequencefor individuals but can point out tendencies.
The multidisciplinary concept of maintaining the initiallyprotrusive position of the premaxilla by means of a passive plate atthe newborn and infant stage, as well as using surgical procedureswith limited retrusive effect, proved to be correct in the long run: Atthe young adult stage, the ANB angle remained positive for almostall patients except for those with multiple-tooth agenesis in the upperarch. A potential benefit of 2-stage palate repair is seen in the neutralvertical development of the patients examined. This hypothesis issupported by comparing with other studies from the literature.
Key Words: Bilateral cleft lip and palate, maintenance ofpremaxillary protrusion, long-term development, cephalometricevaluation
(J Craniofac Surg 2009;20: 1672Y1682)
Complete bilateral cleft lip and palate (BCLP) is a major clinicalchallenge that is met by a multitude of treatment concepts1
differing greatly in the management of the initially protrusive positionof the premaxilla. Of course, the overall goal is to restore oral functionsin infancy and to obtain good aesthetic and functional results at theadult stage. However, there are only few longitudinal studies onpatients with BCLP, and owing to the relatively low incidence of thistype of cleft, samples are usually small. Thus, it is difficult to comparethe effects of various primary treatment concepts. In many publica-tions, postsurgical observation time is too short to allow conclusionsas to the long-term effect on growth and development. Furthermore,the superimposition of steps in secondary treatment as well as of in-dividual basic pattern and habits make it extremely difficult to drawgenerally applicable conclusions. In the literature, on the one hand,growth changes in BCLP samples were compared with those innoncleft controls2Y5; on the other hand, changes in specific areas suchas the cranial base were compared with those in a noncleft populationor to patients with unilateral cleft lip and palate.6 One important study7
deals with facial growth in 2 patient samples treated by differentsurgical concepts at the Universities of Nijmegen and Oslo. Otherslook at single surgical steps or short treatment sequences only.8,9
Obviously, the multitude of the necessary therapeutic steps and thelong time it takes to observe the full manifestation of primary in-terventions during the entire growth period make objective evalua-tion and respective conclusions for treatment planning very difficult.
There is great controversy on whether presurgical orthopedicsshould be applied or not and on the question of primary or secondarysurgical stabilization or even repositioning of the premaxilla.10Y12
Primary surgical repositioning of the premaxilla has largely beendiscarded because of severe disturbance of subsequent maxillarydevelopment13; few data on secondary repositioning of the premaxillaare available.12 One crucial question is whether an effort should bemade at all to bring the premaxilla back between the lateral maxillarysegments before lip repair. Here, the Zurich concept with orthopedicstabilization of the premaxilla and a delay of lip repair up to 6 monthsof age14 stands in contrast to others which advocate presurgicalrepositioning with extraoral or intraoral15 appliances, or whichrenounce infant orthopedics altogether.4 Still, other studies16Y18
recommend presurgical approximation of the maxillary segments toallow for gingivoperiosteoplasty as a simultaneous procedure with liprepair, but there is warning from long-term studies.8,19
Lip repair is a crucial step in which the future development ofthe face has to be considered. The retrusion of the premaxillarysegment resulting from the union of the orbicularis oris muscle iswelcome to a certain extent, but the repaired lip should not undulyrestrain further maxillary development.20 Simultaneous bilateral liprepair is rarely advocated.21 Most authors prefer a 2-stage approach,but timing and techniques do vary. In many instances, 1 side isclosed first, soon followed by repair of the other side; lip adhesionfollowed by proper muscle repair is another option. The Zurichapproach is a 2-stage procedure, which, in the first step, uses muscleunion through the prolabium in the cranial portion of the lip forgradual approximation of the maxillary segments.14,22
ORIGINAL ARTICLE
1672 The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
From the Department of Orthodontics and Pedodontics, Center for Dentaland Oral Medicine, University of Zurich, Switzerland.Received January 24, 2009.Accepted for publication February 18, 2009.Address correspondence and reprint requests to Wanda Maria Gnoinski,
DMD, Department of Orthodontics and Pedodontics, Center for Dentaland Oral Medicine, University of Zurich, Plattenstrasse 11,CH-8032 Zurich, Switzerland; E-mail: [email protected];[email protected]
This article did not require any sources of funding.The authors declare that they had no financial interests or commercial
associations during the course of this study.This article is presented in memory of Professor Milivoj Perko and his
dedicated work of 25 years for patients with BCLP in particular.Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181b2d8dd

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Palate repair cannot be ignored in discussing facial develop-ment. Apart from its influence on the transverse development of themaxillary complex, it also has its implications on verticaldevelopment.23 Treatment concepts vary greatly with regard to thesequence and timing of procedures.
Repair of the alveolar gap can be of great consequence forsubsequent growth if performed in infancy. For the patientsexamined in this study, bone grafting was performed as a secondaryprocedure at relatively late stages; thus, no relevant influence onfacial growth was to be expected.
MATERIALS AND METHODS
SampleThe sample comprised all 42 patients born 1970 to 1986 with
complete BCLP (no Simonart bands) and treated at the University ofZurich hospitals according to a set treatment plan, excluding thosewho, for severe medical reasons, could not be treated according tothe standard treatment plan.
Exclusion criteria:& Syndromes (except van der Woude)& Midline deficiency (3 patients)& Incomplete or irregular cephalometric documentation (9 patients,
5 of whom lived abroad)& Surgical reposition of the premaxilla in childhood (1 patient)
Thus, evaluation covered 29 patients (23 males, 6 females), ofwhom 2 females and 1 male had van der Woude syndrome and3 males had multiple-tooth agenesis outside the cleft area.
Treatment ProtocolThe treatment protocol had been agreed on between the
specialists involved right from the start of the series14 and wasclosely adhered to (Table 1). Newborns were fitted with a plate thatstabilized the premaxilla in its sagittal and vertical positions andallowed spontaneous narrowing of the palatal cleft by keeping the
tongue out of the cleft area. (In the early years, in cases with adiscrepancy between premaxillary width and intersegmental space,plates were fitted with fan screws, but this was later abandonedbecause of doubts as to its long-term effect.) Lip repair wasperformed according to the 2-stage )elexnik technique,22Y25 which,in its first step at around 6 months, provides soft tissue closure of themost anterior part of the nasal floor plus union of the cranial portionof musculus orbicularis oris through a tunnel in the prolabium. Thus,the maxillary segments are brought closer together by muscle forceacting at a level close to the nasal floor while no direct force isapplied at the incisal level of the premaxillaVpalatal tilting isminimized, and in asymmetric cases, symmetry is improved. Two tothree months later, the second step provides full muscle union, andgreat care is taken to create a deep labial sulcus and a mobile lip as aprerequisite for normal forward-downward development of themaxillary complex. A plate was worn postoperatively as well, up to amaximum age of 18 months (on average, 3 plates were usedaltogether). Around 18 months, soft palate repair was performedaccording to Perko’s technique,26,27 with special care being taken tofree the velar muscles from their insertion on the hard palate and toform a velar muscle sling in its correct position; no elevation ofpalatal mucoperiosteum at this stage. Hard palate repair28 wasdelayed up to approximately 5 years; individual timing depended onthe course of speech development. Orthodontic measures wereavoided in the deciduous dentition; 3 patients temporarily wore aplate to protrude upper incisors in the mixed dentition. Whereverpossible, appliances were started in the full permanent dentitiononly. Bone grafting was also postponed until the late mixed orpermanent dentition stage. This treatment regimen allows for thedocumentation of spontaneous development between primarysurgery and the age of approximately 10 years before further stepsin treatment are taken. In 16 males and 5 females of a total of 29,segmental osteotomy was performed after the end of pubertalgrowth, mostly for surgical space closure due to agenesis or in-sufficient size of upper lateral incisors. In 3 patients with multipleagenesis of maxillary teeth, osteotomy was performed for profilecorrection.
TABLE 1. Treatment Protocol for BCLP at the University of Zurich
Timing Orthopedics/Orthodontics Surgery
Birth First plateApproximately 5 mo Second plateApproximately 6 mo First step of )elexnik lip repair: union of cranial portion of orbicularis
muscle closure of anterior nasal floorApproximately 8 mo Second step of )elexnik lip repair: bilateral complete muscle repairApproximately 12 mo Third plate (up to max 18 mo)Approximately 18 mo Soft palate repair, Perko’s technique
Team checkup approximately once per year including speech assessment
4Y5 y No orthodontics in deciduousdentition
Hard palate repair, Perko’s technique
Team checkup approximately once per year including speech assessment (from age 8 to 9 y up to age 20 yevery 2 to 3 y), speech therapy where necessary
From average 15 y (timedindividually)
Orthodontic treatment (meanduration, 4.5 y)
Columella lengthening, alveolar bone grafting
18Y20 y Segmental osteotomy for space closure in case of missing laterals,aesthetic revisions (nose, lip)
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Longitudinal Cephalometric Study in BCLP
* 2009 Mutaz B. Habal, MD 1673

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Documentation/Cephalometric EvaluationDocumentation also followed a given plan. Cephalometric radio-
graphs were obtained at the ages of 5, 10, and 15 years and at the end ofpubertal growth or before corrective osteotomy at age 18 to 20 years(Table 2). The same x-ray unit and cephalostat with 200-cm focus filmdistance were used for the entire duration of this study. Enlargement forthemidsagittal plane is 7.5%.All cephalometric radiographswere tracedon acetate paper. Reference points were identified and then digitized
(Numonics Digitizer, Numonics Corporation, Montgomeryville, PA),all procedures were performed by the second author.
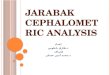
The primary parameters are illustrated in Figure 1.The secondary parameters (angles, distances, and propor-
tions) are listed according to their sequence in Tables 3 and 4:1. NSAr: Angle N-S-Ar2. NSBa: Angle N-S-Ba3. SNA: Angle S-N-A: sagittal position of maxillary alveolar
process relative to the anterior cranial base4. A¶-PNS: Length of maxilla: distance from PNS to A¶
(projection of point A on ANS-PNS)5. SNB: Angle S-N-B: sagittal position of mandibular alveolar
process relative to the anterior cranial base6. NAPg: The angle between points N-A-Pg (facial convexity)7. SNPg: The angle S-N-Pg8. ANB: Angle A-N-B: sagittal position of mandibular alveolar
process relative to the maxillary alveolar process and anteriorcranial base
9. Enlow ratio: The quotient of maxillary skeletal unit distance bymandibular skeletal unit distance (K + I):(N + J) according toEnlow29,30
TABLE 2. Age at Cephalometric Documentation
Age, y Mean SD Min Max
Cephalometric radiograph 1 5.04 0.21 4.7 5.7Cephalometric radiograph 2 10.11 0.32 9.4 11.4Cephalometric radiograph 3 15.11 0.39 13.8 16.1Cephalometric radiograph 4 19.26 0.92 17.8 21.2
All cephalometric radiographs were obtained with the same x-ray unitand cephalostat.
FIGURE 1. Reference points (primary parameters) for the deciduous and permanent dentition stages. 1. Or: Orbitale, the deepestpoint on the infraorbital margin; 2. S: Sella, center of sella turcica; 3. Po: Porion, top of external ear canal; 4. B: PointBVsupramentale: the deepest midline point on the mandible between infradentale and pogonion; 5. N: Nasion, most ventralpoint of sutura nasofrontalis; 6. A: Point AVsubspinale: the deepest midline point on the premaxilla between the anterior nasalspine and prosthion; 7. SE*: Sphenoethmoidale, intersection of the great wing of the sphenoid and the cranial floor; 8. PMF*:Pterygomaxillare, inferior and posteriormost point of fossa pterygomaxillaris; 9. C*: Condylion, the most posterior-superiorpoint on the mandibular condyle; 10. Ar: Articulare, the point of intersection of the dorsal contour of processus articularismandibulae and os temporale; 11. Ba: Basion, lowest point on clivus; 12. Go: Gonion, the most posterior inferior point of themandible. Found by bisecting the angle formed by the mandibular plane (tangent through menton) and a tangent to themandibular ramus through articulare; 13. Me: Menton, the most inferior point on the symphyseal outline; 14. Gn: Gnathion,point of the bony chin located on the midline perpendicular of the pogonion-menton line; 15. Pg: Pogonion, the most anteriorpoint on the contour of the bony chin; 16. AL: Apex of lower incisor; 17. ANS: Anterior nasal spine; 18. AU: Apex of upperincisor; 19. PNS: Posterior nasal spine; 20. FO1*: Anterior point on the functional occlusal plane: one-half overbite of canines orpoint of intersection of the diagonals between the 4 proximal contact points of the first deciduous molars 21. FO2*: Posteriorpoint on the functional occlusal plane: point of intersection of the diagonals between the 4 proximal contact points of the seconddeciduous molars or the first permanent molars if present; 22. RXA*: Point of intersection of the functional occlusal plane with theanterior contour of the ramus; 23. RXB*: Point of intersection of the functional occlusal plane with the posterior contour ofthe ramus; 24. TR*: Point of ramus contact for ramus tangent through articulare; 25. TC*: Point of corpus contact for corpustangent throughmenton; 26. IU: Incisal tip of themaxillary incisor; 27. IL: Incisal tip of themaxillary incisor. Points 7 to 9 and 20 to25 are used in the Enlow analysis.29,31 Points 16, 18, 26, and 27 for measurements on the dentition, and the soft tissue landmarks28 to 33 are not used in this presentation.
Gnoinski and Rutz The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1674 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
10. NSL-NL: The angle between the nasion-sella line (S-N) andnasal line (ANS-PNS)
11. RL-ML: The angle between the mandibular line and a tangentto the mandibular ramus through articulare
12. NSL-ML: The angle between the nasion-sella line (S-N) andmandibular line (tangent)
13. NSL-MeGo: The angle between the nasion-sella line (S-N) andMe-Go (total divergence)
14. NL-MeGo: The angle between nasal line (ANS-PNS) andMe-Go
15. NSGn: y axis (facial axis) in degrees (angle N-S-Gn)16. NL-ML: The angle between nasal line (ANS-PNS) and
mandibular line (tangent to corpus mandibulae throughmenton)
Evaluation was performed according to widely knownanalyses for the sake of comparison with published studies. Becausethese parameters tend to change already with normal growth, theEnlow analysis29 was applied additionally because of its aptness forrevealing changes in the facial pattern. The error of the method(Tables 2 and 3) was calculated by the equation, M = (3d2/2N)1/2,according to Dahlberg (1940)30 and includes all procedures (datacollection, identification of cephalometric landmarks, and digitiz-ing). For 20 patients, the first 2 tracings were measured twice;additionally, the first 2 cephalometric radiographs were tracedrepeatedly, landmarks were identified and digitized, and results werecompared. The error of the method for secondary parameters wassmaller than 2.4 mm for length measurements and below 3.2 degreesfor angles.
Statistical EvaluationThe mean (K), standard deviation (SD), maximum (Max),
minimum (Min), and median (Med) were calculated for allsecondary parameters. For statistical evaluation, SPSS 12.0 (SPSSInc., Chicago, IL) for Windows was applied. Because of the smallsample size and the partly nonparametric distribution of the groups,the Kruskal-Wallis test was applied to show a statistical differencebetween the 3 age groups at 5, 10, and 15 years. The Mann-WhitneyU test was applied to compare 2 age groups, respectively. Astatistically significant difference was attained with a P value of0.001. No sophisticated statistical analysis was performed on thecephalometric radiographs obtained at approximately 18 yearsbecause of the large age range; values calculated from thesecephalometric radiographs are regarded as indicative of the trend offurther development up to the end of growth.
Selected secondary parameters are graphically represented asfollows:- Box plots of the distribution of individual values at the various agelevels,
- Line graphs for individual development, and- Box plots of the individual longitudinal changes between ages 5to 10 years and 10 to 15 years, respectively.
The box is determined by the median value and quartiles1 and 3, whereas the whiskers correspond to a maximum of 1.5times the interquartile distance or to the maximum and min-imum, respectively. Outliers are represented by points beyond thewhiskers.
RESULTS
MaxillaAngle SNA
The premaxilla as the most ventral part of the maxillarycomplex was found to be in a prognathic position at the age of
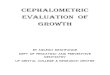
5 years, as expressed by a mean (SD) SNA angle of 84.4 (4.0)degrees. As will be seen for other parameters in this study as well,the range for SNA was extremely large (93.3Y77.1 degrees). In allbut 2 individuals, SNA decreased markedly between the age of 5 and10 years, by a mean (SD) ofj4 (3.0) degrees. Thus, the mean (SD)SNA was 80.5 (3.7) degrees by the age of 10 years and furtherdecreased to 78.1 (4.3) degrees by the age of 15 years. Thedifferences between the 3 age groups were statistically significant(P[5/10/15] = 0.000003), as was the difference between the ages of5 and 10 years (P[5j10] = 0.0005). In the overall developmentbetween the age of 5 years and the end of growth, all individualsshowed a marked decrease in the angle SNA (Fig. 2).
Maxillary Length in Terms of A¶-PNS (A¶ is theProjection of Point A on ANS-PNS)
From a mean (SD) of 50.7 (2.7) mm in the 5-year age group,there was only a small statistically not significant mean (SD)increase of 3.1 (3.1) mm up to the age of 15 years (mean [SD], 53.8[3.7] mm). Between the age of 15 years and the end of growth, themean maxillary length remained practically unchanged.
MandibleAngle SNB
The mean (SD) SNB of 71.4 (3.0) degrees for the age of5 years, with a range of 63.7 to 75.6 degrees, remained relativelyconstant throughout further development, and no statisticallysignificant differences were found between the 3 age groups of5, 10, and 15 years. By the end of growth, the mean (SD) SNBwas 73.4 (3.1) degrees. Individual longitudinal changes betweenthe ages of 5 and 15 years, however, lay within a range of j4.6 to
FIGURE 2. Angle SNA (degrees). A, Individual curves from age5 to 18 years. B, Box plot of the distribution of individual values(degrees) at age levels 5, 10, 15, and 18 years. C, Box plot ofthe distribution of individual change (degrees). $5/10: changebetween the ages of 5 and 10 years. $10/15: change betweenthe ages of 10 and 15 years.
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Longitudinal Cephalometric Study in BCLP
* 2009 Mutaz B. Habal, MD 1675

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
TABLE 3. Secondary Parameters: Mean (K), SD, Max, Min, and Med for the 4 Age Groups
Variables
Age 5 Age 10
K SD Max Min Med K SD Max Min Med
NSAr 126.9 6.2 139.1 114.9 126.8 128.4 4.6 137.9 120.0 128.1NSBa 134.3 5.6 146.8 123.8 132.7 134.2 4.8 146.9 126.9 133.6SNA 84.4 4.0 93.3 77.1 84.8 80.5 3.7 85.7 71.8 81.1A¶-PNS 50.7 2.7 55.6 45.6 50.9 52.4 3.1 57.0 46.1 51.8SNB 71.4 3.0 75.6 63.7 72.2 72.3 3.1 77.7 63.2 72.7NAPg 155.3 5.7 169.4 146.6 155.2 165.9 6.9 182.3 156.2 164.7SNPg 71.4 3.1 76.4 63.6 71.7 73.4 3.0 79.3 65.5 74.1ANB 13.1 3.0 19.0 5.3 12.6 8.1 3.1 12.6 0.8 8.6Enlow ratio 1.12 0.04 1.20 1.04 1.12 1.06 0.04 1.14 0.96 1.07NSL-NL 10.2 3.5 17.0 2.8 10.5 10.7 3.4 19.0 3.8 10.8RL-ML 131.3 6.0 141.7 119.9 27.7 125.8 6.0 136.4 115.3 25.3NSL-ML 38.8 4.5 47.4 29.1 38.5 37.1 4.7 46.1 27.1 36.4NSL-MeGo 40.3 4.3 48.5 32.0 40.1 39.1 4.4 47.3 29.4 39.1NL-MeGo 30.1 5.2 40.7 22.8 28.8 28.4 5.4 38.7 20.4 27.0NSGn 71.1 3.3 77.3 65.8 70.9 71.4 3.6 77.0 63.4 70.7NL-ML 28.6 5.4 40.0 20.2 131.8 26.4 5.7 37.5 18.3 126.2
Except for A¶-PNS (maxillary length in mm) and for the Enlow ratio, the unit of measure is degrees.
TABLE 4. Changes in Secondary Parameters Between the Age of 5 Y and the End of Growth
Variables
$10 j 5 $15 j 10
K SD Max Min Med K SD Max Min Med
NSAr 1.5 3.6 7.0 j9.0 1.7 0.9 2.7 4.8 j4.9 1.2NSBa 0.0 4.2 12.1 j8.1 0.1 0.5 3.8 5.9 j11.4 1.6SNA j4.0 3.0 3.9 j10.0 j4.0 j2.3 2.5 1.2 j7.2 j1.7A¶-PNS 1.8 2.8 8.3 j4.0 1.6 1.4 2.5 7.4 j3.3 1.5SNB 0.8 2.2 6.9 j3.3 0.7 0.6 2.1 4.6 j3.5 1.00.3NAPg 10.2 5.1 24.7 j2.6 9.9 7.0 3.3 12.3 j0.8 7.45.1SNPg 1.8 2.1 7.6 j3.0 1.9 1.2 2.0 4.5 j2.5 1.4ANB j4.8 2.7 1.7 j12.0 j4.8 j2.9 1.6 0.5 j5.2 j2.8Enlow ratio j0.06 0.04 j0.01 j0.15 j0.06 j0.03 0.03 0.04 j0.07 j0.03NSL-NL 0.5 2.7 6.5 j7.2 0.7 0.6 3.0 6.2 j5.0 1.1RL-ML j5.4 3.8 2.1 j13.4 j4.8 j3.0 3.5 2.8 j12.6 j2.5NSL-ML j1.5 2.7 5.8 j6.9 j1.4 j0.8 2.9 4.6 j6.5 j1.0NSL-MeGo j1.0 2.5 5.0 j6.1 j0.9 j0.7 2.7 3.9 j6.1 j1.4NL-MeGo j1.5 3.0 6.4 j7.8 j1.4 j1.3 3.5 7.9 j7.6 j1.9NSGn 0.5 2.5 6.4 j4.0 0.1 0.7 2.1 4.5 j2.9 0.1NL-ML j2.0 3.2 7.2 j9.3 j1.9 j1.4 3.7 8.6 j8.2 j2.0
Mean (K), SD, Max, Min, and Med for change in 4 periods.Except for A¶-PNS (maxillary length in mm) and for the Enlow ratio, the unit of measure is degrees.$10 j 5: change between the ages of 5 and 10 y.$15 j 10: change between the ages of 10 and 15 y.$15 j 5: change between the ages of 5 and 15 y.$End of growth j15: between the age of 15 y and the end of growth.
Gnoinski and Rutz The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1676 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Age 15 End of Growth
K SD Max Min Med K SD Max Min Med
129.3 5.3 137.3 115.8 129.5 129.2 6.5 137.4 116.8 130.2134.7 5.1 144.4 124.5 136.1 133.7 5.7 142.0 125.0 134.678.1 4.3 84.4 69.7 78.9 75.9 4.3 84.7 68.0 75.653.8 3.7 62.9 47.6 53.6 53.3 4.3 64.4 47.6 53.172.9 3.3 78.8 65.7 73.2 73.4 3.1 78.5 66.2 73.0172.9 7.6 191.3 161.3 171.1 178.7 7.0 192.6 166.1 178.274.6 3.2 81.8 69.2 74.7 75.3 2.9 79.4 69.5 75.25.2 3.3 9.9 j2.4 5.8 2.6 3.3 8.3 j4.7 3.01.04 0.05 1.12 0.93 1.04 1.01 0.05 1.10 0.91 1.0111.3 3.6 18.4 4.0 12.2 10.0 3.7 16.8 3.8 9.8122.8 6.2 135.2 111.7 25.1 121.5 7.1 135.2 109.2 120.336.3 5.1 45.8 26.5 35.2 34.7 5.7 45.5 23.8 35.438.4 4.9 47.2 27.8 38.0 37.1 5.2 46.4 25.6 37.627.1 5.5 38.8 17.6 27.9 27.1 5.2 39.1 18.5 27.272.1 3.8 81.1 64.5 72.0 71.9 3.5 77.0 64.1 72.824.9 5.8 37.8 15.8 122.3 24.7 5.7 38.2 15.7 24.1
$15 j 5 $End of Growth j 15
K SD Max Min Med K SD Max Min Med
2.5 3.9 7.5 j5.4 4.0 0.3 2.5 5.3 j4.3 0.60.4 4.3 9.9 j7.1 0.4 j0.9 3.6 4.9 j10.7 j0.4
j6.3 3.6 5.1 j13.2 j6.7 j2.5 2.3 0.7 j7.5 j2.13.1 3.1 8.2 j2.5 3.4 j1.3 3.1 4.7 j7.2 j1.51.3 2.8 8.4 j4.6 1.5 0.0 1.8 3.6 j3.8 0.3
17.1 5.7 36.3 8.4 15.7 5.5 4.3 17.8 0.0 5.12.9 2.8 9.9 j3.6 3.0 0.2 1.8 3.6 j3.8 0.4
j7.7 2.8 j3.0 j16.3 j7.3 j2.6 2.0 0.4 j8.0 j2.4j0.08 0.04 j0.02 j0.22 j 0.08 j0.03 0.03 0.01 j0.09 j0.031.1 3.9 8.9 j8.4 1.0 0.0 1.8 4.0 j3.0 0.2
j8.3 4.9 0.5 j17.6 j7.6 j1.5 2.3 3.4 j7.9 j1.8j2.2 4.4 7.7 j11.3 j2.2 j0.7 2.4 3.7 j4.7 j0.6j1.6 4.1 7.7 j10.6 j1.7 j0.4 2.0 3.7 j4.4 j0.3j2.7 4.6 7.5 j10.8 j3.0 j0.5 1.8 3.2 j3.3 j0.91.2 3.3 10.5 j5.6 0.9 0.5 1.7 3.4 j2.4 0.3
j3.3 4.9 7.4 j12.9 j3.5 j0.8 2.1 3.3 j4.0 j1.1
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Longitudinal Cephalometric Study in BCLP
* 2009 Mutaz B. Habal, MD 1677

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
+8.4 degrees, with a mean (SD) of +1.3 (2.8) degrees. Duringthese 10 years, 8 individuals showed a decrease (maximum,j4.6 degrees), whereas the rest showed an increase of 0.04 to8.4 degrees (Fig. 3).
Gonial Angle RL-MLThe tangent angle of ramus and corpus mandibulae decreased
slightly during the observation period. The difference was significantonly between the ages of 5 and 15 years, with a mean (SD) decreaseof j8.3 (4.9) degrees and a range from j17.6 to +0.5 degrees.
Sagittal Intermaxillary RelationshipAngle ANB
The significant decrease in this angle during the entire periodof observation was particularly evident up to the age of 10 years:From a very high mean (SD) value of 13.1 (3.0) degrees within arange of 19 to 5.3 degrees, there was a mean (SD) decrease of j4.8(2.7) degrees. Between the ages of 10 and 15 years, the mean (SD)decrease of j2.9 (1.6) degrees was much smaller but stillstatistically significant. At the age of 15 years, the mean (SD)ANB angle was 5.2 (3.3) degrees and further decreased at an aboutequal rate until the end of growth.
Again, individual longitudinal changes do differ a lot: of 3individuals who had negative ANB values at the age of 15 years(j0.9, j1.6, and j2.4 degrees), 2 had had values clearly less thanthe group average values (5.3 and 7.7 degrees) at the age of 5 yearsalready, whereas 1, starting from a value slightly greater than theaverage at the age of 5 years, showed a decrease of j12.1 degrees,which is more than double the average decrease for this period(Fig. 4).
Enlow’s Analysis of BEquivalent Balance[29Y31
The mean (SD) ratio between the sagittal length of themaxillary skeletal unit (K + I) and that of the mandibular skeletalunit (N + J) shifts from a maxilla-dominated ratio of 1.12 (0.04) atthe age of 5 years toward a balanced ratio of 1.04 (0.05) at the age of15 years and to 1.01 (0.05) by the end of growth. The change in thislength ratio is statistically significant between the ages of 5 and 10years but not any more for the later stages. In all patients, the sagittallength ratio decreased between the ages of 5 and 15 years, with amean (SD) of j0.08 (0.04). By the end of growth, 8 patients (3 ofthem with multiple-tooth agenesis outside the cleft area) had asagittal length ratio less than 1.0. Because not many colleagues willbe familiar with Enlow’s analysis, it may be added that a sagittallength ratio of approximately 0.96 corresponds to profiles that arevisually judged as borderline for corrective osteotomy at the Zurichclinic. Maximum decrease in this ratio (j0.22) was found in apatient with multiple-tooth agenesis where, from an average ratio atthe age of 5 years, the ratio fell to 0.93 (Fig. 5).
NAPg: Angle of ConvexityFrom a mean (SD) of 155.3 (5.7) degrees, there was a
significant increase over time. With a mean (SD) increase of 10.2(5.1) degrees between 5 and 10 years against 7 (3.3) degrees between10 and 15 years, change was more marked in the early period. Again,there is great variance in the individual changes: increases between8.4 and 36.3 degrees were measured.
Vertical DimensionsUpper Face Angulation NSL-NL
In relation to the anterior cranial base, the base of the maxillaappears posteriorly inclined at the age of 5 years with a mean (SD)
FIGURE 4. Angle ANB (degrees). A, Individual curves from age5 to 18 years. B, Box plot of the distribution of individual values(degrees) at age levels 5, 10, 15, and 18 years. C, Box plot ofthe distribution of individual change (degrees). $5/10: changebetween the ages of 5 and 10 years. $10/15: change betweenthe ages of 10 and 15 years.
FIGURE 3. Angle SNB (degrees). A, Individual curves from age5 to 18 years. B, Box plot of the distribution of individual values(degrees) at age levels 5, 10, 15, and 18 years. C, Box plot ofthe distribution of individual change (degrees). $5/10: changebetween the ages of 5 and 10 years. $10/15: change betweenthe ages of 10 and 15 years.
Gnoinski and Rutz The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1678 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
angle of 10.2 (3.5) degrees. This remains rather constant during theentire observation period; no significant differences were foundbetween the 3 age levels. Individual values, however, varied betweena maximum of 19 degrees and a minimum of 2.8 degrees. Overall,an anterior rotation of the base of the maxilla was observed in 7patients (changes ranged from j0.1 to j8.4 degrees), whereas therest showed posterior rotation (ranged from 0.01 to 8.9 degrees).
Lower Face AngulationFor the sake of comparison to other studies, angulation was
measured twice; the baseline of the mandible being determined asMe-Go through points menton and gonion on the one hand and by atangent ML to the contour of corpus mandibulae through pointmenton on the other hand (NL-ML). The initial values are a mean(SD) of 30.1 (5.2) degrees and a range of 40.7 to 22.8 degrees forNL-MeGo, and a mean (SD) of 28.6 (5.4) degrees within a range of40.0 to 20.2 degrees for NL-ML. No statistically significant changewas found over time, although on an average, there was a slightdecrease (j2.7 or j3.3 degrees, respectively). Individual longitu-dinal changes varied greatly: from 7.5/7.4 degrees to j10.8/j12.9degrees, with 7 patients showing an increase in NL-MeGo and 6patients with an increase in NL-ML, respectively; although in mostcases, lower face angulation decreased over time (Fig. 6).
Total Face AngulationAgain, angulation was measured twice, as NSL-MeGo on the
one hand and NSL-ML on the other hand. With both ways ofmeasurement, on average, there was a slight but not statisticallysignificant decrease. But again, individuals did react in highlyvarious ways: An increase was found in 7 individuals for the angleNSL-MeGo (0.3Y77 degrees) and in 8 individuals for the angleNSL-ML (0.4Y7.7 degrees), respectively. For total face angulation as
well as for lower face angulation, a decrease over time was found formost patients (Fig. 7).
DISCUSSIONAlthough this is a retrospective study, the sample is clearly
defined. It comprises all patients with complete BCLP (without anySimonart bands) born 1970 to 1986 and treated at the ZurichUniversity Hospitals, except those who, for severe medical reasons,could not be treated according to the standard treatment plan.
Both the treatment protocol and the documentation followed agiven plan that had been agreed on between the specialists involvedright from the start of the series.14 All surgical interventions weredone by one man (M. Perko), and the orthopedic/orthodonticmeasures as well as the follow-up were surveyed by the first author(W.G.). The same x-ray unit was used for the entire duration of thisstudy. With the exception of infant plates, and of 3 patients whotemporarily wore a plate to protrude upper incisors in the mixeddentition, orthopedic/orthodontic treatment was avoided up to theage of 10 years at least to document for as long as possible only theeffects of primary interventions and spontaneous development.Patients excluded from this survey because of incomplete cepha-lometric records were followed up to adulthood and documented aswell at least at the final stage.
Development is determined to a great extent not only by themalformation, which, in itself, is not always the same althoughsummarized under a coined term, but also by the inherited basicindividual pattern. This accounts for an extreme heterogeneity andvariance in all secondary parameters examined. Under thesecircumstances, the small sample size is a massive handicap. Thereason for submitting this study all the same, although other studiesshowed similar results,4,5,7 lies in the fact that this treatment
FIGURE 6. Lower face angulation:maxillary base tomandibularbase (tangent). Angle NL-ML (degrees). A, Individual curvesfrom age 5 to 18 years. B, Box plot of the distribution ofindividual values (degrees) at age levels 5, 10, 15, and 18 years.C, Box plot of the distribution of individual change (degrees).$5/10: change between the ages of 5 and 10 years. $10/15:change between the ages of 10 and 15 years.
FIGURE 5. Enlow maxillary-mandibular length ratio: maxillaryskeletal unit distance (K + I) divided by mandibular skeletalunit distance (N + J).31 A, Individual curves from age 5 to18 years. B, Box plot of the distribution of individual values(maxillary-mandibular length ratio) at age levels 5, 10, 15, and18 years. C, Box plot of the distribution of individual change(ratio). $5/10: change between the ages of 5 and 10 years.$10/15: change between the ages of 10 and 15 years.
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Longitudinal Cephalometric Study in BCLP
* 2009 Mutaz B. Habal, MD 1679

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
approach probably goes to a maximum in maintaining the apparentlyprotruded initial position of the premaxilla. It shows, on the basis ofindividual longitudinal data, that at the end of growth, the sagittalposition of the premaxilla relative to the anterior cranial base is justabout correct. This means that, except for patients with multiple-tooth agenesis outside the cleft area, there is no need for surgicalcorrection of the skeletal facial profile. This is considered a greatadvantage because experience from former patients had shown that,however good the secondary surgery is, the soft tissue cover is thelimiting factor in profile correction. With the premaxilla as asupporting beam31,32 in its correct final position, good profile resultswill be more easily attainable.
In this study as in many others, the facial profile in the 5-yearage-group is dominated by a very prominent subnasal area.Accordingly, the mean SNA angle of 84.4 degrees clearly exceedsthe population average and extremes go up to 93 degrees. However,subsequent straightening of the profile is impressive, especially up tothe age of 10 years, with a mean decrease by 4 degrees in SNA. It isextremely rare for no change or even an increase in the angle SNA tooccur. The length of the maxillary complex has almost adultdimensions at the age of 5 years and does increase but little overtime. Similar observations were reported in the literature.4,32,33 Themandible that initially appears very retrusive does increaseconsiderably in length and catches up with the maxilla. Corre-spondingly, as an indicator of sagittal intermaxillary relationship, themean angle ANB in young children with BCLP was far greater thanthe population average (approximately 13 versus 5 degrees)but gradually normalized without any therapeutical interference.The fact that almost all patients starting from a marked or evenextreme class 2 sagittal relationship finally reached sagittal skele-tal balance would seem to confirm that appropriate support for
spontaneous development is provided by the treatment plandescribed. When compared with the Oslo BCLP sample,4 at theage of 5 years, ANB was clearly greater in our patient group. Thesubsequent relative decrease in ANB up to the end of growth wassimilar in both studies (mean approximate, j10 degrees). Conse-quently, individuals from our sample ended with an ANBapproximately 3 degrees greater than the Oslo values and thuscame closer to those found in 2 other studies.5,7 It might be surmisedthat delayed hard palate repair in one of these,7 same as in Zurich,could be a contributing factor.
With the substantial change in facial pattern in BCLP,traditional cephalometric parameters can change in highly unex-pected ways and are therefore not of great value for prognosis offuture development in individual cases. In the quest for a tool thatmight help to plan the most efficient course of treatment, forexample, by early identification of patients who will ultimately needcorrective osteotomy for profile reasons, Enlow’s analysis was foundto be of special interest. Under the key word Bequivalent balanceconcept,[29 it looks at the balance of functionally related counter-parts. Analysis of patient samples with cleft lip and palate accordingto this concept33,34 has revealed that it can give indications of thefuture development of facial balance at approximately the age of 10years already. In this sample, balance is initially slanting toward themaxillary side as expressed by sagittal length ratios up to 1.2, whichcorresponds to an extreme class 2 skeletal relationship. With time,the mandible catches up, and most individuals will end with aharmonious sagittal skeletal balance as expressed by length ratiosvery close to 1.00 (or 1:1). At the end of growth, only 6 patientsshowed ratios between 0.926 and 0.999. Our clinical experienceshows that a sagittal length ratio of approximately 0.96 correspondsto profiles that are visually judged as borderline for correctiveosteotomy at the Zurich clinic. As a matter of fact, 2 patients with
TABLE 5. Secondary Parameters: Comparison of Findings atthe 3 Age Levels
Variable P(5/10/15) P(5j10) P(10j15) P(5j15)
NSAr NS NS NS NSNSBa NS NS NS NSSNA *** *** * ***A¶-PNS * * NS **SNB NS NS NS NSNAPg *** *** ** ***SNPg ** * NS ***ANB *** *** *** ***Enlow ratio *** *** NS ***NSL-NL NS NS NS NSRL-ML *** ** NS ***NSL-ML NS NS NS NSNSL-MeGo NS NS NS NSNL-MeGo NS NS NS NSNSGn NS NS NS NSNL-ML NS NS NS *
Kruskal-Wallis test for calculation of statistically significant differencebetween 3 age levels (P[5/10/15]: ages 5, 10, and 15 y).
Mann-Whitney U test: for calculation of statistically significant dif-ference between 2 age levels (P[5/10]: ages 5 and 10 y; P[10/15]: ages 10 and15 y; P[5/15]: ages 5 and 15 y).
NS indicates P 9 0.05; *P G 0.05; **P G 0.005; ***P G 0.001.
FIGURE 7. Total face angulation: anterior cranial base tomandibular base (tangent). Angle NSL-ML (degrees).A, Individual curves from age 5 to 18 years. B, Box plot ofthe distribution of individual values (degrees) at agelevels 5, 10, 15, and 18 years. C, Box plot of the distribution ofindividual change (degrees). $5/10: change between theages of 5 and 10 years. $10/15: change between the ages of10 and 15 years.
Gnoinski and Rutz The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1680 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
multiple-tooth agenesis in the maxilla had the lowest ratios of0.926 and 0.955, respectively, and had to undergo surgical profilecorrection.
The vertical dimension and its changes over time are also afrequent topic in discussions on cleft lip and palate. Manystudies4,34Y36 report downward rotation of the maxillary base(nasal line = ANS-PNS) as a general tendency. In this survey, thisheld true for only 7 patients. It would seem that our treatmentconcept favors the regular vertical development of the maxilla(Table 5). Two points might be important in this: a 2-stage lip repairaccording to )elexnik is meant to avoid sudden heavy muscle forceon the premaxilla, which can lead to palatal tilting of the segment aswell as upward displacement of the repaired muscle relative to thepremaxilla. Great variance in the inclination of the maxilla reflectsnot only the effect of lip repair but also the consequences of palaterepair, which, depending on the technique applied, may leavescarring in the areas of the sutura palatina transversa, the maxillarytuberosities, or the fossa pterygopalatina. It is likely that such scarscould affect the forward and downward displacement of the entiremaxillary complex. Given the great variance of the maxillary base inour sample, it is amazing that the overall divergence of the facesremained very constant over time, without statistically significantchanges. Apparently, the vertical development of the upper andlower alveolar processes has a great compensatory effect. Finding atendency toward decrease rather than increase in facial divergence inour study stands in contrast to several reports4,5 but coincides withanother study23 where samples with 1-stage and 2-stage palate repairwere compared. Another factor that has to be considered whenlooking at developmental changes in facial profile in BCLP istongue position. It can be influenced by surgery in both the lip andpalate areas. Procedures that avoid early massive retrusion of thepremaxilla and preserve palatal vault space should result in lesscompensatory vertical development.
The great interindividual variance found for all parameters inthis study calls for great caution with regard to statements ondevelopmental tendencies derived from calculation with age-relatedmean values, for example, in mixed longitudinal studies. One fact,however, stands out despite all the heterogeneity in samples ofpatients with BCLP: the relatively protrusive position of thepremaxilla must be respected by all means. There is strong evidenceagainst all efforts toward achieving a normal skeletal profile inyoung children. Interventions toward this goal would end with aconcave facial profile at the young adult stage. This is supported bythe fact that the apparently excessive maxillary length at the 5-yearage level in this sample remained largely the same all through furtherdevelopment. Similar observations were repeatedly reported in theliterature,4,32,33 and it is hard to believe that, to this day, massiveretrusion of the premaxilla in infants is still advocated by someauthors. Those who do so must be ignorant of the literature as well asof their own patients’ long-term fate.
REFERENCES1. Berkowitz S. A comparison of treatment results in complete bilateral
cleft lip and palate using a conservative approach versus Millard-LathamPSOT procedure. Semin Orthod 1996;2:169Y184
2. Friede H, Pruzansky S. Longitudinal study of growth in bilateral cleft lipand palate, from infancy to adolescence. Plast Reconstr Surg 1972;49:392Y403
3. Johnson GP. Craniofacial analysis of patients with complete clefts of thelip and palate. Cleft Palate J 1980;17:17Y23
4. Semb G. A study of facial growth in patients with bilateral cleft lip andpalate treated by the Oslo CLP Team. Cleft Palate Craniofac J 1991;28:22Y39
5. Trotman CA, Ross RB. Craniofacial growth in bilateral cleft lip andpalate: ages six years to adulthood. Cleft Palate Craniofac J 1993;30:261Y273
6. Horswell BB, Gallup BV. Cranial base morphology in cleft lip andpalate: a cephalometric study from 7 to 18 years of age. J OralMaxillofac Surg 1992;50:681Y685
7. Heidbuchel KL, Kuijpers-Jagtman AM, Freihofer HP. Facial growth inpatients with bilateral cleft lip and palate: a cephalometric study.Cleft Palate Craniofac J 1994;31:210Y216
8. Henkel KO, Gundlach KK. Analysis of primary gingivoperiosteoplastyin alveolar cleft repair: part I. Facial growth. J Craniomaxillofac Surg1997;25:266Y269
9. Hotz M, Perko M, Gnoinski W. Early orthopaedic stabilization of thepraemaxilla in complete bilateral cleft lip and palate in combination withthe Celesnik lip repair. Scand J Plast Reconstr Surg Hand Surg 1987;21:45Y51
10. Freihofer HP, van Damme PA, Kuijpers-Jagtman AM. Early secondaryosteotomyVstabilization of the premaxilla in bilateral clefts. JCraniomaxillofac Surg 1991;19:2Y6
11. Hayward JR. Management of the premaxilla in bilateral clefts. J OralMaxillofac Surg 1983;41:518Y524
12. Heidbuchel KL, Kuijpers-Jagtman AM, Freihofer HP. An orthodonticand cephalometric study on the results of the combinedsurgical-orthodontic approach of the protruded premaxilla in bilateralclefts. J Craniomaxillofac Surg 1993;21:60Y66
13. Friede H, Pruzansky S. Long-term effects of premaxillary setback onfacial skeletal profile in complete bilateral cleft lip and palate.Cleft Palate J 1985;22:97Y105
14. Hotz MM, Perko M. Early management of bilateral total cleft lip andpalate. Scand J Plast Reconstr Surg 1974;8:104Y108
15. Bitter K. Latham’s appliance for presurgical repositioning ofthe protruded premaxilla in bilateral cleft lip and palate.J Craniomaxillofac Surg 1992;20:110
16. Wood RJ, Grayson BH, Cutting CB. Gingivoperiosteoplasty andmidfacial growth. Cleft Palate Craniofac J 1997;34:17Y20
17. Santiago PE, Grayson BH, Cutting CB, Gianoutsos MP, Brecht LE,Kwon SM. Reduced need for alveolar bone grafting by presurgicalorthopedics and primary gingivoperiosteoplasty. Cleft PalateCraniofac J 1998;35:77Y80
18. Millard DR, Latham R, Huifen X, Spiro S, Morovic C. Cleft lip andpalate treated by presurgical orthopedics, gingivoperiosteoplasty, and lipadhesion (POPLA) compared with previous lip adhesion method: apreliminary study of serial dental casts. Plast Reconstr Surg1999;103:1630Y1644
19. Berkowitz S, Mejia M, Bystrik A. A comparison of the effects of theLatham-Millard procedure with those of a conservative treatmentapproach for dental occlusion and facial aesthetics in unilateral andbilateral complete cleft lip and palate: part I. Dental occlusion. PlastReconstr Surg 2004;113:1Y18
20. Da Silva Filho OG, Valladares Neto J, Capelloza Filho L. Influence oflip repair on craniofacial morphology of patients with completebilateral cleft lip and palate. Cleft Palate Craniofac J 2003;40:144Y153
21. Mulliken JB, Wu JK, Padwa BL. Repair of bilateral cleft lip: review,revisions, and reflections. J Craniofac Surg 2003;14:609Y620
22. Perko M. Vorteile und Ergebnisse der operation nach )elexnik bei derbilateral durchgehenden Spalte. Fortschr in der Kiefer Gesichts-Chir1973;(16/17):77Y79
23. Silvera QA, Ishii K, Arai T, Morita S. Long-term results of the two-stagepalatoplasty/Hotz’ plate approach for complete bilateral cleft lip,alveolus and palate patients. J Craniomaxillofac Surg 2003;31:215Y227
24. )elexnik F. Notre procede de traitement chirurgical du bec-de-lievrebilateral total. Revue de Stomatologie 1962;63:386Y388
25. Zajdela Z. )elexnik procedure in the surgical treatment of bilateralcomplete clefts. J Maxillofac Surg 1973;1:137Y142
26. Perko M, Hotz M. Primary treatment of cleft lip and cleft palate.Minerva Stomatol 1971;20:193Y201
27. Perko MA. Two-stage closure of cleft palate (progress report). JMaxillofac Surg 1979;7:46Y80
28. Perko M. Two-stage palatoplasty. In: Bardach J, Morriss HL, eds.Multidisciplinary Management of Cleft Lip and Palate. Philadelphia,PA: WB Saunders, 1990:311Y315
29. Enlow DH, Moyers RE, Stuart Hunter W, McNamara JA Jr. A procedure
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Longitudinal Cephalometric Study in BCLP
* 2009 Mutaz B. Habal, MD 1681

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
for the analysis of intrinsic facial form and growth. Anequivalent-balance concept. Am J Orthod 1969;56:6Y23
30. Riolo ML. and University of Michigan (Ann Arbor, MI) Center forHuman Growth and Development. An Atlas of CraniofacialGrowth: Cephalometric Standards From the University SchoolGrowth Study, the University of Michigan. Ann Arbor, MI:University of Michigan Center for Human Growth andDevelopment, 1974:356, 371
31. Dahlberg G. Statistical Methods for Medical and Biological Students.New York, NY: Interscience, 1940
32. Veau V. Bec-de-Lievre. Paris, France: Masson, 1938:246
33. Narula JK, Ross RB. Facial growth in children with complete bilateralcleft lip and palate. Cleft Palate J 1970;7:239Y248
34. Gnoinski W. Early identification of candidates for corrective maxillaryosteotomy in a cleft lip and palate group. Scand J Plast Reconstr SurgHand Surg 1987;21:39Y44
35. Hellquist R, Svardstrom K, Ponten B. A longitudinal study ofdelayed periosteoplasty to the cleft alveolus. Cleft Palate J 1983;20:77Y88
36. Lisson JA, Hanke I, Trankmann J. Changes of vertical skeletalmorphology in patients with complete unilateral and bilateral cleft lipand palate. Cleft Palate Craniofac J 2005;42:490Y494
Gnoinski and Rutz The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1682 * 2009 Mutaz B. Habal, MD