Embed Size (px)
Citation preview

205Visual field test in children
Correspondence and reprintrequests to:Drs. G.PorroDepartment of OphthalmologyUtrecht University HospitalHeidelberglaan 1003584 CX UtrechtThe NetherlandsTel: ++31-30-2507880Fax: ++31-30-2541855
Acknowledgements: The presentresearch was financially supported bythe Fischerstichting. The authors aregrateful to Prof. Dr. J. Van Hof-VanDuin for her important suggestionsduring the early phase of this study,and to Mrs. J. Rimmelzwaan for therevision of the English text.
Presented in part at the 22nd Meetingof the European PaediatricOphthalmology Group, Valencia,Spain, 20-22 September 1996.
Letters
Neuro-ophthalmology 0165-8107/98/US$ 12.00
Neuro-ophthalmology – 1998, Vol. 19,No. 4, pp. 205-214© Æolus PressBuren (The Netherlands) 1998
Accepted 22 December 1997
A new behavioral visual field test forclinical use in pediatric
neuro-ophthalmology
Giorgio Porro1
Julia Hofmann1
Dienke Wittebol-Post1
Onno van Nieuwenhuizen2
Yvonne T. van der Schouw3
Matthijs B.H. Schilder4
Marjoleine E.M. Dekker4
Willem F. Treffers1
1F.C. Donders Institute of Ophthalmology, 2Department of ChildNeurology, 3Julius Center for Patient Oriented Research,
4Department of Ethology & Socio-ecology, Utrecht University,Utrecht, The Netherlands
Abstract Background: In order to obtain a method to assess theperipheral visual field of neurologically impaired children in a clinicalsetting, the arc perimeter was modified into a simple behavioral visualfield test. This new test is based on a graded semicircular black metalarc with a white ball at the end. The arc is rotated by an examineraround the head of the subject in such a way that the white ball movesfrom the periphery towards the center of the visual field. Objective:Here we describe the device, the procedure, and its validation by testinghealthy subjects. Methods: Sixty subjects (infants, children, and adults)were tested. Results: The success rate of the test ranged from 63% ininfants to 100% in younger children. Normative and reference valuesfor clinical application were derived from the data obtained. Theextension of the monocular peripheral visual field increased progres-sively along each meridian with increasing age (p values for trend0.0062, 0.0069, 0.0077 and 0.0058, respectively). Conclusion: This newtest measures in a simple way behavioral reactions to a peripheral stim-ulus. Therefore, it may be useful for peripheral visual field assessmentof neurologically impaired children who cannot be tested by standardor simplified perimetry techniques.
Key words Infants; children; visual field; behavioral test
Introduction Conventional perimetry techniques (manual or auto-mated kinetic and static perimetry) are well established for use in adults.
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

G. Porro et al.206
However, most techniques are not appropriate for infants and youngchildren, due to the complex nature of the response required.1 Usingkinetic double-arc or simplified sphere perimeters, a clear insight hasbeen given into development and extent of the visual field in normalinfants and young children.2-8 Since for these techniques fixed positionand straight head posture are required, they are sometimes difficult toapply, especially in those neurologically impaired children who areforced to a wheelchair because of their poor motor skills (i.e. poorseating positions, hypotony, or postural anomalies). These are the verychildren to be expected to have visual field defects. Therefore, wemodified the arc perimeter into a simple behavioral kinetic perimetrydevice and technique (BEFIE test: BEhavioral visual FIEld screeningtest) for the assessement of the peripheral visual field of neurologicallyimpaired children in a clinical setting.
In this paper, we first provide a description of the device and the testprocedure. Then, we report the results obtained assessing the peripheralvisual field of 60 healthy subjects with the BEFIE test.
The BEFIE test
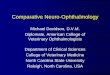
description of the device The device (Fig. 1) consists of:1. A graded semicircular black metal arc with a white ball at one end(A) and a foam rubber handle at the other end (B). The arc has a radiusof 35 cm, a length of 80 cm, and a diameter of 4 mm. During monoculartesting, the subject’s eye is located at its radius. The white ball, madeof polystyrene, has a diameter of 4 cm, equivalent to 6 degrees, and actsas peripheral stimulus. The marks are indicated along the arc’s backside every 5 degrees from the white ball (= 90 degrees) to the handle(= 0 degrees).2. A straight black metal stick 35 cm in length with a level fastenedonto it at an angle of 45 degrees (C).
Fig. 1. Instruments necessary toperform the behavioral visual fieldscreening test (BEFIE test): a gradedsemicircular black metal arc with awhite ball at one end (A) and a foamrubber handle at the other end (B); astraight black metal stick with a levelattached to it used for the rightpositioning of both the semicirculararc and the fixation target (C); acardboard tube (D); a fixation target(E); and a scheme for the registrationof the measurements obtained in eachquadrant (F). Note also the modifieddevice with a black-and-white ballinserted at the end of a gradedsemicircular gray metal arc (G).
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

207Visual field test in children
3. A cardboard tube with a diameter of 4 cm and a length of 23 cm (D).4. A fixation target consisting of a white ball, similar to the former one,inserted at the top of a stick (E).
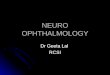
the test procedure The visual field by means of the BEFIE testis assessed by an examiner assisted by an unbiased observer (Fig. 2).The subject to be examined sits on a chair or on the parent’s lap. Auniform background is not necessary. The examiner stands behind thesubject with the straight metal stick in one hand and the gradedsemicircular arc in the other. If the subject is not able to maintain afixed head position, the parent is asked to support the chin so that thehead is facing straight at the fixation target, while allowing freemovement toward the peripheral stimulus. The observer sits in front ofthe subject. While holding the fixation target, which is positioned at 35cm opposite of the subject’s eye, the observer watches the subjectthrough the tube. This allows the observer to see the face, but not theperipheral stimulus. In order to control the distance of the fixationtarget, the straight metal stick with the level fastened onto it is positionedby the examiner perpendicular to the subject’s eye before each trial.Then, the same stick is rotated on the eye and it is placed parallel tothe subject’s forehead. Subsequently, it is inclined along one of thediagonal half meridia (45, 135, 225, and 315 degrees) by watching atthe level. This rotational movement of the stick defines the co-ordinatesof a virtual perimeter and positions the peripheral stimulus and thefixation target at an equivalent distance (35 cm) from the subject’s eye.For binocular examination, the center of the virtual perimeter is locatedat the visual egocenter, the midpoint between the eyes which correspondsto the midplane of the head.9,10 As soon as the examiner has defined theposition of both the fixation target and the peripheral stimulus, theobserver attracts the attention of the subject to the fixation target. Oncethe fixation is steadily captured, the observer signals the examiner topresent the peripheral stimulus. The examiners rotates the semicirculararc from the periphery towards the fixation target at a rate of 3-5 deg/sec
Fig. 2. Measurement of the rightsuperior quadrant of the binocularvisual field with the BEFIE test. Thechild, who was first gazing at thefixation target, suddenly looks at theperipheral stimulus moved by theexaminer. This reaction isimmediately reported by the observer.Consequently, the examiner stops themovement of the graded semicirculararc and places the straight metal stickparallel to the subject’s forehead. Thepoint indicated by the stick on thegraded semicircular arc (see arrow) isconsidered the measure in degrees ofthe peripheral visual field along theright superior quadrant.
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

G. Porro et al.208
along a virtual meridian. The observer, unaware of the quadrant fromwhich the stimulus is approaching, reports the subject’s reactions. Anyreactions, such as eye movements, eye and head movements, eye andhand movements, or any verbal answer related to the peripheral stimulus,are used as response measures. If the subject makes an appropriate eyemovement or any other stimulus-directed reaction towards the meridianinvestigated, the examiner immediately stops the peripheral stimulusand places the straight metal stick parallel to the subject’s forehead firstand then perpendicular to the graded semicircular arc. The point indicatedby the straight metal stick on the graded semicircular arc (see arrow onFig. 2) is considered the measure in degrees of the visual field extensionalong that quadrant.
The peripheral stimulus is presented at random in one of the fourquadrants (45, 135, 225, and 315 meridian), and each quadrant is testedthree times.6 For monocular testing, one eye is occluded with an orthopticeye patch. Testing of the visual field continues until all 12 trials arecompleted or until the subject is too tired to proceed or has becomeinattentive. After every four successful trials, all measurements obtainedare registered by the examiner. For each subject, the extent of the visualfield along each half-meridian is calculated as the mean of two or threemeasurements obtained along that meridian.3 If there is no eye movementaway from the fixation target, the trial is repeated immediately. If thesubject looks in the wrong direction, the eye movement in expectationof the peripheral stimulus is recorded as a spontaneous look, and thetrial is repeated as soon as the subject refixates on the fixation target.Whenever the total number of spontaneous looks is higher than half thetotal successful trials, the subject is excluded from the analysis or thetest is repeated. To reduce these errors and to become familiar with thetechnique, younger children are given two or three binocular practicetrials before performing the first test.11
Methods
subjects Sixty healthy infants and children one to five years of age(28 boys and 32 girls) were examined. Subjects were randomly selectedamong relatives of colleagues and patients of our department. Informedconsent was obtained from the parents before performing the investiga-tions. Twelve adults, students or researchers of the same department(mean age: 25 yr; range: 16-36 yr), were also tested. All the selectedsubjects underwent an additional ophthalmological investigation.
validation of the befie test: an ethological analysis Inthe BEFIE test, eye movements towards a peripheral stimulus are usedto establish whether a subject has noticed it. To validate the use of eyemovements as a functional behavior indicating the perception of anobject, eight subjects (6 children and 2 adults) were instructed to reactimmediately upon seeing the peripheral stimulus with a stimulus-directedbehavior (i.e., verbal answer, nodding, pointing at the stimulus, grabbingthe stimulus, or smiling). Thus, a reaction was obtained, independent ofthe eye movement, indicating that the subject had noticed the peripheralstimulus of the BEFIE test. By using two cameras and a professional
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

209Visual field test in children
video-mix equipment, video registrations were made in which a timecode was added. Each occurrence of behavior was recorded fromvideotape by “The Observer”, a computerized observation programme12
and analyzed at the Ethology Department of Utrecht University. Byusing the associated Video Tape Analysis System, the exact time eachbehavior occurred could be determined, as well as intervals betweenbehaviors or between stimulus and stimulus-directed behaviors. Regis-tered behavioral elements included the start of the presentation of theperipheral stimulus, the eye movements of the subject towards the peri-pheral stimulus at the correct meridian, spontaneous looks, as well asany stimulus-directed behavior. The start of the presentation of theperipheral stimulus was defined at the moment the examiner started tomove the stimulus along one of the virtual meridians towards the fixationtarget. None of the subjects had to be excluded as a result of too manyspontaneous looks. Only successful trials were used for this analysis. Inorder to establish the mean intra-rater reliability, five subjects werescored twice with an interval of one day. There was an 88.5% agreementwith a range of 84.3-91.5%.
Six children were tested using two types of BEFIE test, the above-described test with a white ball inserted at the end of a semicircularblack metal arc and a modified type with a black-and-white ball insertedat the end of a semicircular gray metal arc (see Fig. 1). The peripheralstimuli were of the same size and made of similar polystyrene material.The tests were all performed under similar conditions, differing only inthe used peripheral stimulus. The mean luminance of the balls used forthe BEFIE test was 80 cd/m2 as measured by a J-6523-2 1 Narrowangle luminance probe (Tektronics Instruments), with a room luminanceof 470 lux, as measured by a LX-101 LCD Lutron Digital lightmeter.
Subjects may be able to detect a stimulus of high contrast soonerthan a stimulus of lower contrast. Therefore, the latencies of detectingboth stimuli were measured based upon the time between the start ofthe stimulus and the moment the eye movement was made by the subjectin the correct direction of the stimulus.
Results
befie test: normal and reference values Subjects examinedwere divided into five age groups: group 1 (12-24 months; n=19);group 2 (25-36 months; n=17); group 3 (37-48 months; n=12); group4 (49-60 months; n=12); and group 5 (adults; n=12). Four children(6.6%) did not complete the test because of sleepiness, restlessness, ora high number of spontaneous looks: two belonged to group 1 and twoto group 2. Seven of the children tested (11.6%), five from group 1 andtwo from group 2, were excluded from our analysis because theyperformed the BEFIE test only binocularly. One child from group 3was excluded because of an interocular difference greater than 15degrees along two meridia and was referred for further neuro-opthalmological examinations. The success rate of the remaining 48children and 12 adults who performed the BEFIE test monocularly was63.1% in group 1, 76.4% in group 2, 91.6% in group 3, and 100% ingroups 4 and 5. In six younger subjects, only two measurements per
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

G. Porro et al.210
meridian were possible. The total duration of the test, including patching,was approximately 4-6 min for each eye. Mean results and standarddeviations of each diagonal meridian are shown in Table 1.
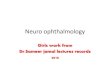
As a suggestion for reference values of a pathological visual field,four standard deviations (SD) for children and two SD for adults weresubstracted from the mean values obtained in each meridian for eachage group. Peripheral visual fields increase with increasing age; all testsfor trend were statistically significant (test for trend). The normaldevelopment of the peripheral visual field along each meridian is shownin Figure 3.
Five children from group 4 and three adults were retested forreproducibility on a different test day by the same examiner: the secondset of data was obtained without knowledge of the prior data. Averagedifferences greater than five degrees in children and three degrees inadults between two means along each meridian were not found. Thesubjects were retested the same day by a different examiner. An averageinterobserver variability of 12 degrees in children and five degrees inadults between two means along each meridian was found.
validation of the befie test Analysis of stimulus-directed be-haviors was conducted to determine validity of the child’s eye movementtowards the peripheral stimulus. A lag sequential analysis was used toestablish the frequencies and time relationships between the start of theperipheral stimulus, the eye movement, and the stimulus-directedbehavior (Table 2).
First, the sequential relationship between eye movements and the
Group Values Meridian Meridian Meridian Meridian45 135 225 315degrees degrees degrees degrees
1 Mean 67.71 47.73 48.03 76.5712-24 mo Standard deviation 6.8 5.1 6.7 8.8n=19 Reference value (Mean - 4 SD) 40 27 21 41
2 Mean 68.10 48.63 51.27 77.4725-36 mo Standard deviation 5.3 3.8 5.7 6.5n=17 Reference value (Mean - 4 SD) 47 33 28 51
3 Mean 71.06 49.73 52.65 79.0437-48 mo Standard deviation 7.3 4.1 4.0 7.6n=12 Reference value (Mean - 4 SD) 42 33 37 49
4 Mean 74.25 50.10 53.84 83.1249-60 mo Standard deviation 5.3 2.8 4.1 5.8n=12 Reference value (Mean - 4 SD) 53 39 37 60
5 Mean 74.79 52.43 54.81 87.47Adults Standard deviation 3.7 1.7 3.5 3.0n=12 Reference value (Mean - 2 SD) 67 49 48 81
p for trend 0.0062 0.0069 0.0077 0.0058
table 1. Normal and referencevalues per age group of the peripheralvisual field assessed with the BEFIEtest.
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

211Visual field test in children
Fig. 3. Means and standard deviationsof the monocular visual field alongfour meridians per age group. Notethat the extension of the peripheralvisual field increased progressivelyalong each meridian with increasingage.
Subject Start of the periperal Eye movements Eye movements Stimulus directed Total number ofstimulus followed followed by any not followed by behavior not successful trialsby eye movements stimulus directed any stimulus preceded by eye
behavior directed behavior movement
I-2 17 17 0 0 17I-3 28 28 1 1 29I-10 13 13 1 1 14II-1 8 8 2 2 10II-2 23 22 1 1 24II-3 21 17 4 4 25II-4 19 19 0 0 19II-5 20 19 2 2 23
Subject Mean SD Minimum Maximumduration duration duration
I-2 0.59 0.17 0.3 0.9I-3 0.85 0.24 0.4 1.4I-10 0.89 0.46 0.6 2.2II-1 0.54 0.12 0.4 0.8II-2 0.94 1.23 0 4.1II-3 0.91 1.08 0 4.1II-4 0.98 1.08 0.4 4II-5 1.02 1.07 0.1 4.2
table 3. The mean interval (inseconds) between eye movement andstimulus-directed behavior for eachsubject.
table 2. Frequencies and timerelationship between the behavioralelements for each subject.
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

G. Porro et al.212
start of the presentations of the peripheral stimulus was established.The results presented in Table 2 show that for most subjects thefrequency of eye movements following the start of the peripheralstimulus corresponded to the frequency of stimulus-directed behaviorfollowing the eye movements. The mean agreement between thesefrequencies is 96.5% with a range of 81-100%. Therefore, most trialsconfirmed that a directionally appropriate eye movement followed thestart of the presentation of the peripheral stimulus.
In order to establish the validity of the eye movements in relation tothe observed peripheral stimulus, the percentage of a directionallyappropriate eye movement followed by a stimulus-directed behaviorwas calculated. The mean percentage of directionally appropriate eyemovements followed by stimulus-directed behaviors was 92.1%, rangingfrom 80% to 100%. These results show that 92% of the directionallyappropriate eye movements were confirmed by accurate stimulus-directed behavior. Therefore, we may conclude that eye movement is auseful behavior to establish that the subject has noticed the stimulus.The mean interval between showing the stimulus-directed behavior andthe preceding eye movement for each subject, is presented in Table 3.The mean duration for all subjects is 0.84 seconds.
For six subjects, the latency time from the start of the stimuluspresentation to the eye movement was measured for both peripheralstimuli, the white ball, and the black-and-white ball. The mean latencytimes of each stimulus are given in Table 4. Two of the subjects (II-1and II-3) showed increased latency times when the black-and-white ballwas used in comparison to the white ball, giving the highest scores,rank 5 and 6. In general, the time between the start of the stimulus andthe eye movement of the subject does not seem to depend upon the typeof peripheral stimulus used. However, the number of children studiedis rather small to draw definitive conclusions.
Discussion The application of the BEFIE test on 60 healthy subjectsprovides data from which normative values for clinical applications arederived. We find that the extension of the monocular peripheral visualfield increases progressively along each meridian with increasing age (pvalues for trend <0.05). Moreover, we can establish reference values,which allow us to consider median results for each meridian belowthese values as pathological.
We compared our data with results obtained by Wilson et al.,1 whoperformed a study with a 110° double-arc perimeter in older children
Subject White ball Black-and- d Rank of dwhite ball
I-3 2.92 2.63 0.29 2II-1 1.58 4.48 3.1 6II-2 2.41 2.11 0.3 3II-3 2.86 3.48 0.62 5II-4 2.94 2.74 0.2 1II-5 2.54 2.2 0.34 4
table 4. Mean latency times inseconds for a white ball and for ablack-and-white ball used asperipheral stimuli in the BEFIE test.
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

213Visual field test in children
and adults. Results are presented in Table 5. Most of the results arecomparable. However, in 4- and 5-year-old children, we obtained sig-nificantly larger peripheral visual fields for meridian 45. On the contrary,in adults we found significantly smaller visual fields for meridian 135and 315. Probably, the absence of a uniform background and the factthat the semicircular arc of the BEFIE test is graded only up to 90degrees may explain these differences.
The BEFIE test shows several advantages. The device is simple,inexpensive, and can be easily used in a clinical setting. In addition,this rapid procedure requires only two examiners and it can be learnedafter a short period of training. The peripheral stimulus is presented atrandom in one of the four quadrants and each quadrant is tested threetimes: from a theoretical calculation based upon statistics in such afour-choice situation, the probability of spontaneous eye movement inthe direction of the peripheral object taking place thrice is less than1.6%.13 Moreover, the method seems suited to minimize the effects ofany physical handicap and it is very well accepted, since the directinteraction between the observer and the child is considered a game.Videotaping the session may allow both the observer and the examinerfurther comparisons over the results obtained.
The BEFIE test does, however, have some disvantages. In fact, thereare several inherent limitations, such as the variability in the speed andextent of movement of the hand-held peripheral stimulus. Moreover,both the positions of the peripheral stimulus and the measurementsalong the graded semicircular arc require accurate and repeated checks.The present research can be criticized because no uniform backgroundwas used, with subsequent high variability in contrast between theperipheral stimulus and the background. However, a uniform backgroundbars the interaction with the child and is rarely available in a clinicalsetting. This problem could be minimized by increasing the contrast of
Wilson Porro
Meridian Age Mean 95% CI Mean 95% CI
45 4 yr 59.2 55.1-63.3 71.6* 66.9-75.25 yr 63.4 58.7-68.1 74.25* 71.3-77.3Adults 72.6 67.3-77.9 74.79 72.7-76.9
135 4 yr 47.8 44.3-51.3 49.73 47.4-52.15 yr 51.7 48.6-54.8 50.10 48.5-51.7Adults 60.2 56.1-64.3 52.43* 51.5-53.4
225 4 yr 51.4 46.7-56.1 52.65 50.4-54.95 yr 52.4 47.3-57.5 53.84 51.5-56.2Adults 54.0 50.7-57.3 54.81 52.8-56.8
315 4 yr 84.7 81.6-87.8 79.04 74.7-83.35 yr 88.1 84.4-91.8 83.12 79.8-86.4Adults 94.9 92.1-97.6 87.47* 85.8-89.2
*p<0.05.
table 5. Comparison of results ofWilson and Porro.
Neu
roop
htha
lmol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
11/
20/1
4Fo
r pe
rson
al u
se o
nly.

G. Porro et al.214
the peripheral stimulus and by decreasing the contrast of the semicirculararc, modifications which do not influence substantially the results. Infact, latency times between the start of the stimulus presentation andeye movements do not differ for the two types of balls used. The ratherpoor interobserver variability in children could certainly be reduced byintroducing a period of training for the right positioning of the graduatedsemicircular arc. Moreover, the high reference values established shouldminimize both the intra- and interobserver variations.
In conclusion, the present ophthalmological and ethological investi-gation on healthy subjects by means of a new behavioral visual fieldtest provided relevant data to establish normative and reference values.The fact that eye movements can be used by ophthalmologists as afunctional behavior indicating the perception of an object encouragesthe application of our test on those children who show good eye move-ments but may not be able to point at the peripheral stimulus. TheBEFIE test measures in a simple way behavioral reactions to a peripheralstimulus. Therefore, it may be useful for peripheral visual field assess-ment of neurologically impaired children who cannot be tested by stand-ard or simplified perimetry techniques.
References 1 Wilson M, Quinn G, Dobson W,
Breton M. Normative values for visualfields in 4- to 12-year old childrenusing kinetic perimetry. J PediatrOphthalmol Strabismus 1991;28:151-153.
2 Mohn G, Van Hof-Van Duin J. Thedevelopment of the binocular andmonocular visual field in fullterm andpreterm human infants. InvestOphthalmol Vis Sci 1985;26(Suppl):137.
3 Mohn G, Van Hof-Van Duin J.Development of the binocular andmonocular visual field of humaninfants during the first year of life.Clin Vision Sci 1986;1:51-64.
4 Van Hof-Van Duin J, Mohn G. Earlydetection of visual impairment. In:Galjaard H, Prechtl H, Velickovic M,editors. Cerebral Palsy, EarlyDetection and Management.Dordrecht: Martinus Nijhoff, 1987;79-100.
5 Van Hof-Van Duin J. Visual fieldmeasurements, optokinetic nystagmusand the visual threatening response:normal and abnormal development.Doc Ophthalmol Proc Ser1986;45:305-317.
6 Schwartz TL, Dobson V, SandstromDJ, Van Hof-Van Duin J. Kineticperimetry assessment of binocularvisual field shape and size in younginfants. Vision Res 1987;27:2163-2175.
7 Cummings M, Van Hof-Van Duin J,Fulton AB, Mayer L. Visual fieldassessment of young patients. InvestOpht Vis Sci 1987;28(Suppl):202.
8 Mayer DL, Fulton AB, Cummings M.Visual fields of infants assessed with anew perimetric tecnique. InvestOphthalmol Vis Sci 1988;29:452-459.
9 Moidell B, Steinbach MJ, Hiroshi O.Egocenter location in childrenenucleated at an early age. Invest
Ophthalmol Vis Sci 1988;29:1348-1351.
10 Bloch H, Carchon I. On the onsetof eye-hand coordination ininfants. Behav Brain Res 1992;49:85-90.
11 Quinn GE, Fea AM, Minguini N.Visual fields in 4- to 10-year oldchildren using Goldmann anddouble arc perimeters. J PediatrOphthalmol Strabismus 1991;28:314-319.
12 Noldus LPJJ. The Observer: asoftware system for collectionand analysis of observationaldata. Behav Res Methods InstrumComput 1991;23:415-429.
13 Groenendaal F. Perinatal hypoxiaand visual functions in infantsand children. Thesis.Alblasserdam: Kanters BV, 1987;72 p (in Dutch).N
euro
opht
halm
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Was
hing
ton
on 1
1/20
/14
For
pers
onal
use
onl
y.