Embed Size (px)
Citation preview

108 Journal of Tissue Viability 1992 Vol. 2 No 4
A NEW IN VITRO MODEL FOR STUDY OF WOUND HEALING
AVRIL BURTt, ANGUS McGROUTHER2
1Research Fellow, 2Professor of Plastic Reconstructive Surgery Dept. of Surgery, University College, London
SUMMARY This new in vitro wound model consists of layers of human keratinocytes grown on a very thin transparent silicone disc in which a central hole is cut before placing it on a layer of collagen gel containing human fibroblasts (simulating a dermis). The growth of epidermal keratinocytes across the 'wound' can easily be visualised and photographed by inverted light microscopy, at frequent intervals, to monitor the stimulating or adverse effect of many substances presently designed for wound treatment.
INTRODUCTION A number of full thickness skin models have been developed for grafting1 or pharmaceutical testing2
• We have developed this model to study the spread of keratinocyte cells from a 'wound' edge across a dermal bed of collagen fibre lattice. (This bed may also include other dermal elements such as vascular endothelia or macrophages). Theinteractionofthecellscan bestudiedcontinuously without resort to invasive biopsy methods which would be needed with animals or patients.
MATERIALS Silicone rubber discs 2.4mm diameter supplied by Bibby Sterilin, acid solution of rat tail (type 1) or other collagens obtained as Vitrogen from Imperial Labs, human keratinocyte and fibroblast cultures.
METHOD Primary humankeratinocytes (from mammary reduction, foreskin or biopsy) were cultured in medium as described by Green et al3 for 7-14 days to produce sub-confluent sheets. The cells were then trypsinised to produce a suspension containingaround4x10Scellspermlingrowth medium. The sterile silicone discs were placed firmly into petri dishes (35mm diameter) where they attached by natural adhesion and 0.5 m1 cell suspension carefully added to each disc so that the silicone was completely covered. This was incubated for 24-48 hours at 36.5oC to allow the keratinocytes to attach to the silicone before feeding with further growth medium. (Green's formula 3).
To produce the dermal layer of the wound model, rat-tail collagen in acid solution (or vitrogen) was mixed with 10-fold DMEM + 10% FCS i;n the ratio 8:1 at OOC. This was neutralised with IN sodiumhydroxidesolution(withcaretopreventover-alkalisation). 20ml of this collagen mixture was added to 4ml of fibroblast suspension, mixed and rapidly pipetted into 6 wells of a 6-well plate ( Sxl OS cells/well). This was allowed to gel at room temperature then placed in a humidified 5% CCY incubator at 36.50C to equilibrate for 2 hours.
The silicone discs with keratinocytes were drained of medium and a central hole was cut, using a sterile cork borer 1 em diameter and a sterile scalpel. The disc was lifted with forceps and t:he central piece usually remained attached to the culture plate. The culture disc was placed firmly on to the collagen/fibroblast layer and replaced in the incubator.
After 24 hours 1 ml ofkeratinocyte medium was carefully added to this wound model. (Where there was a tendency for the silicone disc to float a sterile stainless steel grid was placed over it to weigh it down).
Using this basic method it was possible to pre-treat the 'dermal' layer with growth factors and/or antiseptics which are available for burn wound care, before adding the keratinocyte layer. The cultures were examined daily by inverted microscope.
Human dermal fibroblasts were grown from split skin biopsies by explants in 25cm2 flasks and simple growth medium Dulbecco's MEM (DMEM) containing 10% foetal calf serum (FCS). Actively growing cultures were trypsinised and resuspended at 7.5 x lOS cells/ml in medium and cooled in an ice bath. Fig 1. Active keratinocytes on silicone disc (k) on collagen layer (c) containing no fibroblasts
( ~ indicates edge of disc).
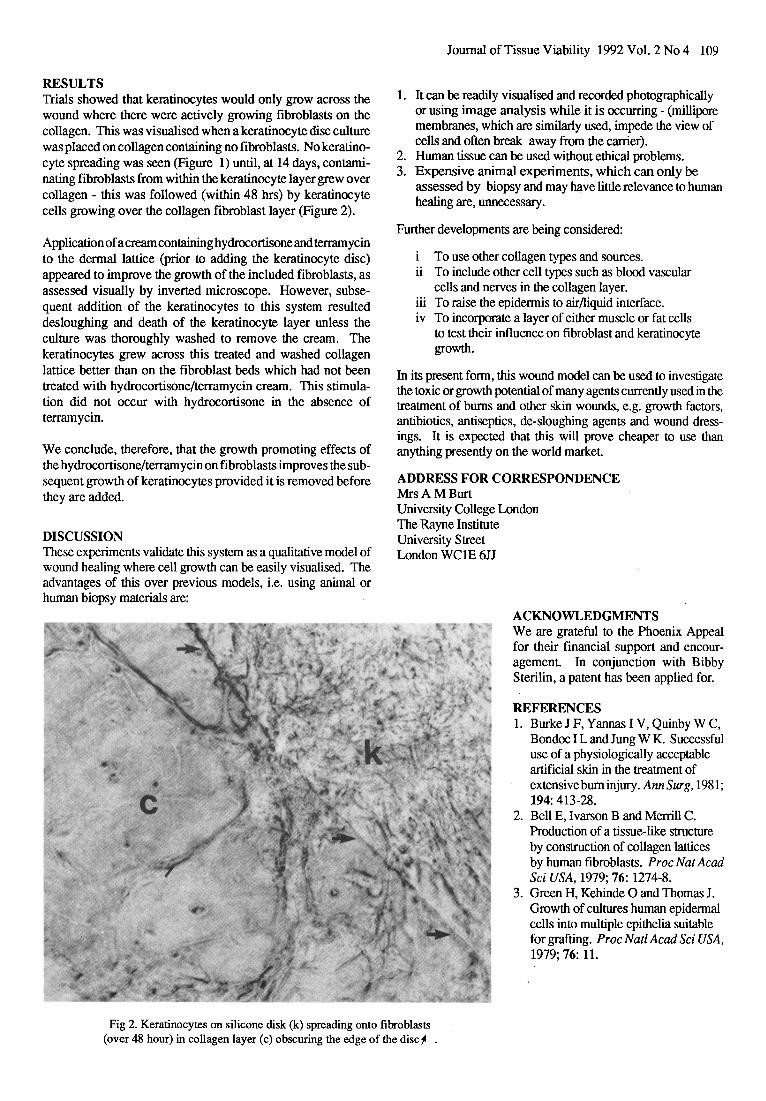
RESULTS Trials showed that keratinocytes would only grow across the wound where there were actively growing fibroblasts on the collagen. This was visualised when a keratinocyte disc culture was placed on collagen containing no fibroblasts. No keratinocyte spreading was seen (Figure 1) until, at 14 days, contaminating fibroblasts from within the keratinocyte layer grew over collagen- this was followed (within 48 hrs) by keratinocyte cells growing over the collagen fibroblast layer (Figure 2).
Application of a cream containing hydrocortisone and terramycin to the dermal lattice (prior to adding the keratinocyte disc) appeared to improve the growth of the included fibroblasts, as assessed visually by inverted microscope. However, subsequent addition of the keratinocytes to this system resulted desloughing and death of the keratinocyte layer unless the culture was thoroughly washed to remove the cream. The keratinocytes grew across this treated and washed collagen lattice better than on the fibroblast beds which had not been treated with hydrocortisone/terramycin cream. This stimulation did not occur with hydrocortisone in the absence of terramycin.
We conclude, therefore, that the growth promoting effects of the hydrocortisone/terramycin on fibroblasts improves the subsequent growth of keratinocytes provided it is removed before they are added.
DISCUSSION These experiments validate this system as a qualitative model of wound healing where cell growth can be easily visualised. The advantages of this over previous models, i.e. using animal or human biopsy materials are:
Journal of Tissue Viability 1992 Vol. 2 No4 109
1. It can be readily visualised and recorded photographically or using image analysis while it is occurring- (millipore membranes, which are similarly used, impede the view of cells and often break away from the carrier).
2. Human tissue can be used without ethical problems. 3. Expensive animal experiments, which can only be
assessed by biopsy and may have little relevance to human healing are, unnecessary.
Further developments are being considered:
To use other collagen types and sources. ii To include other cell types such as blood vascular
cells and nerves in the collagen layer. iii To raise the epidermis to air/liquid interface. iv To incorporate a layer of either muscle or fat cells
to test their influence on fibroblast and keratinocyte growth.
In its present form, this wound model can be used to investigate the toxic or growth potential of many agents currently used in the treatment of bums and other skin wounds, e.g. growth factors, antibiotics, antiseptics, de-sloughing agents and wound dressings. It is expected that this will prove cheaper to use than anything presently on the world market.
ADDRESS FOR CORRESPONDENCE MrsAMBurt University College London The Rayne Institute University Street London WC1E 6JJ
ACKNOWLEDGMENTS We are grateful to the Phoenix Appeal for their financial support and encouragement. In conjunction with Bibby Sterilin, a patent has been applied for.
REFERENCES 1. BurkeJF,YannasiV,QuinbyWC,
Bondoc I Land Jung WK. Successful use of a physiologically acceptable artificial skin in the treatment of extensive bum injury. AnnSurg,1981; 194: 413-28.
2. BellE, lvarson Band Merrill C. Production of a tissue-like structure by construction of collagen lattices by human fibroblasts. Proc Nat Acad Sci USA, 1979; 76: 1274-8.
3. Green H, Kehinde 0 and Thomas J. Growth of cultures human epidermal cells into multiple epithelia suitable for grafting. Proc Natl Acad Sci USA, 1979; 76: 11.
Fig 2. Keratinocytes on silicone disk (k) spreading onto fibroblasts (over 48 hour) in collagen layer (c) obscuring the edge of the discjl .















