Embed Size (px)
Citation preview
Vol. 42 No. 4 October 2011 Journal of Pain and Symptom Management 535
Original Article
A Prospective Study of the Incidence of Fallsin Patients With Advanced CancerCarol Stone, MB ChB, MSc, Peter G. Lawlor, MB, MMedSc,Br�ıd Nolan, RN, RM, MSc, and Rose Anne Kenny, MB, BCH, MDOur Lady’s Hospice & Care Services (C.S., B.N.), Harold’s Cross, Dublin, Ireland; Division of
Palliative Care (P.G.L.), University of Ottawa, and Palliative Care Unit (P.G.L.), Bruy�ere
Continuing Care, Ottawa, Ontario, Canada; and Department of Medical Gerontology (R.A.K.),
Trinity College Dublin, and Centre of Excellence for Successful Ageing (R.A.K.), St. James’ Hospital,
Dublin, Ireland
Abstract
Context. The association between aging and falls risk, and the morbidity andmortality resulting from falls in older persons, is well documented. Results froma small number of studies of patients with cancer in inpatient settings suggest thatpatients with advanced cancer may be at high risk of falling. We presentpreliminary results pertaining to the incidence of falls in patients with advancedcancer from an ongoing study of risk factors for falls.
Objectives. To measure incidence of falls in patients with advanced cancerreceiving palliative care, and to test the hypothesis that patients aged $65 yearsare at greater risk of falling than those aged <65 years.
Methods. Ambulant patients with cancer admitted to palliative care serviceswere recruited. Demographic details were ascertained by patient interview androutine record review. Participants were followed-up by weekly telephone calls forup to six months.
Results. Follow-up has been completed for 119 patients; mean age was 66.91(�12.86) years and 53.8% were male. Sixty-two participants (52.1%) fell duringfollow-up. The median time to fall for participants aged <65 and $65 years was 85days (95% confidence interval [CI] 51.54e118.46) and 80 days (95% CI44.07e115.93), respectively (c2¼ 0.034, P¼ 0.85). The incidence density of fallswas 2770 per 1000 person-years.
Conclusion. One in two patients with advanced cancer fell during follow-up of upto sixmonths, regardless of age. There is a need to investigate the sequelae of falls inpatients with cancer, to ascertain the risk factors, and in particular, the modifiablerisk factors in this population. J Pain SymptomManage 2011;42:535e540.� 2011U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved.
Key Words
Accidental falls, cancer, palliative care, risk factors, epidemiologyAddress correspondence to: Carol Stone, MB ChB, MSc,Our Lady’s Hospice & Care Services, Harold’s Cross,Dublin, Ireland. E-mail: [email protected]
Accepted for publication: January 6, 2011.
� 2011 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
0885-3924/$ - see front matterdoi:10.1016/j.jpainsymman.2011.01.006

536 Vol. 42 No. 4 October 2011Stone et al.
Introduction retrospective case finding in cohorts of older
The association between aging and falls riskin older persons has long been recognized byspecialists and generalists alike. As a result ofresearch conducted over the past threedecades, it is recognized that approximately30% of community-dwelling older personsfall per annum because of a complex interac-tion of intrinsic and extrinsic risk factors. Ap-proximately 10% of falls result in fracture,head injury, or serious soft tissue injury.1,2
Even noninjurious falls have significant nega-tive consequences for the individual, with upto 40% of those who fall subsequently experi-encing a fear of falling. Fear of falling is associ-ated with self-imposed activity restriction,leading to decline in physical performance in-dependent of baseline function, and to devel-opment of gait and balance problems.3 Theevidence supports the theory of a functionaldownward spiral, whereby the negative se-quelae of falling predispose to further falls:a history of falling in the past year is associatedwith a relative risk of further falls of 3.7.4 Thefinancial cost of falling in older persons is notinsignificant. In Ireland, during 2004, directcosts of falls and fractures in persons aged 65years and older accounted for 1.6% of the totalpublic health expenditure.5,6
Prevention of falls in older persons is a princi-pal strategic objective for health and social pol-icy makers in developed countries. Initiativesinclude screening all older persons annuallyfor a history of falls, conducting a comprehen-sive fall evaluation in those presenting witha fall, and increasing awareness in the generalpopulation of interventions that may improvebalance and falls risk.7,8 Evidence of effective in-terventions for reducing falls risk, in selected orunselected populations of older persons, issteadily emerging. Multicomponent interven-tions that target multiple risk factors, targetedexercise interventions, home hazard modifica-tion, reducing psychotropic medication, andcorrection of vitamin D depletion have allbeen shown to be effective interventions forcommunity-dwelling older persons.9,10
In comparison, very little is known of the ep-idemiology of falls in people with cancer. Theliterature published to date is limited to a smallnumber of studies of incidence of and riskfactors for falls in inpatient settings and
persons with cancer attending outpatientservices.11e18 Based on the analysis of incidentforms in inpatient palliative care units, where97.5%e100% admissions had malignant dis-ease, researchers in the United Kingdom,Canada, and Switzerland reported fall ratesof 15.6, 16.9, and 6.9 falls per 1000 patientbed days, respectively; in comparison, the aver-age rate of falling in acute hospitals in theUnited Kingdom in 2005e2006 was 4.8 fallsper 1000 bed days, suggesting that a diagnosisof advanced cancer confers a greater risk offalling than other illnesses.11,13,14,19
The existing research on falls in community-dwelling patients with cancer seems to refutethis: The proportion of patients aged $70years with cancer at any stage, reporting atleast one fall in the preceding 12 months inthe studies conducted by Overcash et al.,were 22.4% (37/165) and 27% (81/297).Bylow et al. reported that only 22% (11/50)of men aged $70 years with prostate cancer,with either biochemical recurrence or asymp-tomatic metastatic disease, reported at leastone fall in the preceding three months. How-ever, all of the studies used convenience sam-pling of patients and used retrospectivereporting of falls. The latter is particularly sus-ceptible to recall bias, as elucidated by Over-cash and Rivera in a later study of 20 cancerpatients aged $70 years, in which 13 patientsreported having fallen in the past year but 15reported having fallen in the past threemonths.15e18
In this article, we present preliminary find-ings pertaining to the incidence of falls, anddetails of falls, in consecutive recruits to an on-going prospective study designed to evaluatethe risk factors for falls in patients with ad-vanced cancer. We hypothesized that patientswith advanced cancer have a high incidenceof falls and that patients with advanced canceraged $65 years have a greater risk of fallingthan those aged <65 years.
MethodsSetting and ParticipantsConsecutive admissions to the palliative care
services provided by Our Lady’s Hospice andCare Services (November 24, 2008 until June

Vol. 42 No. 4 October 2011 537Incidence of Falls in Advanced Cancer
15, 2010) were invited to participate. The pal-liative care services consist of inpatient careprovided in a 36-bed inpatient unit (IPU),a Day Hospice service, and a Home Care Ser-vice. The IPU offers admission to patients forsymptom control, terminal care, rehabilita-tion, and respite; in 2009, there were a totalof 427 admission episodes and 250 deaths.The activity of Day Hospice follows the modelof therapeutic rehabilitation whereby patientsattend a six-week individualized program de-signed to assist return to their prior level offunctioning.
Patients aged 18 years or older with a diagno-sis of metastatic or loco-regionally advancedcancer were eligible for inclusion. Exclusioncriteria were as follows: being unable to standand mobilize unassisted, actively dying orconsidered too unwell by the admitting and re-search teams, registered as blind, using contin-uous oxygen, and being aphasic or unable toconverse in English.
Eligible patients received written informa-tion on the study at the time of admission toservices. Enrollment of patients with impairedcognition (Short Orientation-Memory testgreater than 11) required the assent of the pa-tient in addition to consent from their proxy.20
All other participants provided informed con-sent. The study was approved by St. Vincent’sUniversity Health Group Ethics Committee.
Data Collection and Patient Follow-UpDemographic data were collected by tran-
scription of data routinely recorded on the ad-mission proforma and verified by patientinterview at the time of risk factor assessment.Performance status was measured using thePalliative Performance Scale.21 Patients werecontacted weekly from the date of baseline as-sessment, by telephone or in person, to deter-mine if they had fallen during the precedingseven days and to record details of the fall ifthis had occurred. A fall was defined as anevent whereby an individual inadvertentlycomes to rest on the ground or lower level,with or without loss of consciousness.22
Follow-up continued until six months fromthe time of baseline assessment, or until theoccurrence of a fall or death if these occurredbefore six months. Information regarding sur-vival of patients who completed the study wasobtained from an electronic palliative care
patient administration database system, usedby Our Lady’s Hospice & Care Services andthe hospitals within its catchment area.
Statistical AnalysisDescriptive analyses of number and details
of falls were conducted. Incidence density offalls was calculated as the total number of fallsper the sum of patient days of follow-up, ex-pressed as number of falls per 1000 patientyears. Time to first fall was examined using sur-vival analysis methods, including the log ranktest. A term for age <65 and $65 years was in-cluded and 95% confidence intervals (CIs)presented for median survival estimates. De-mographic characteristics of participants andthose who declined participation were com-pared using the Pearson Chi-squared test andthe two-sample t-test. Statistical analysis wasperformed using SPSS (Version 16) (SPSS,Inc., Chicago, IL) statistical software.
ResultsBetween November 11, 2008 and June 15,
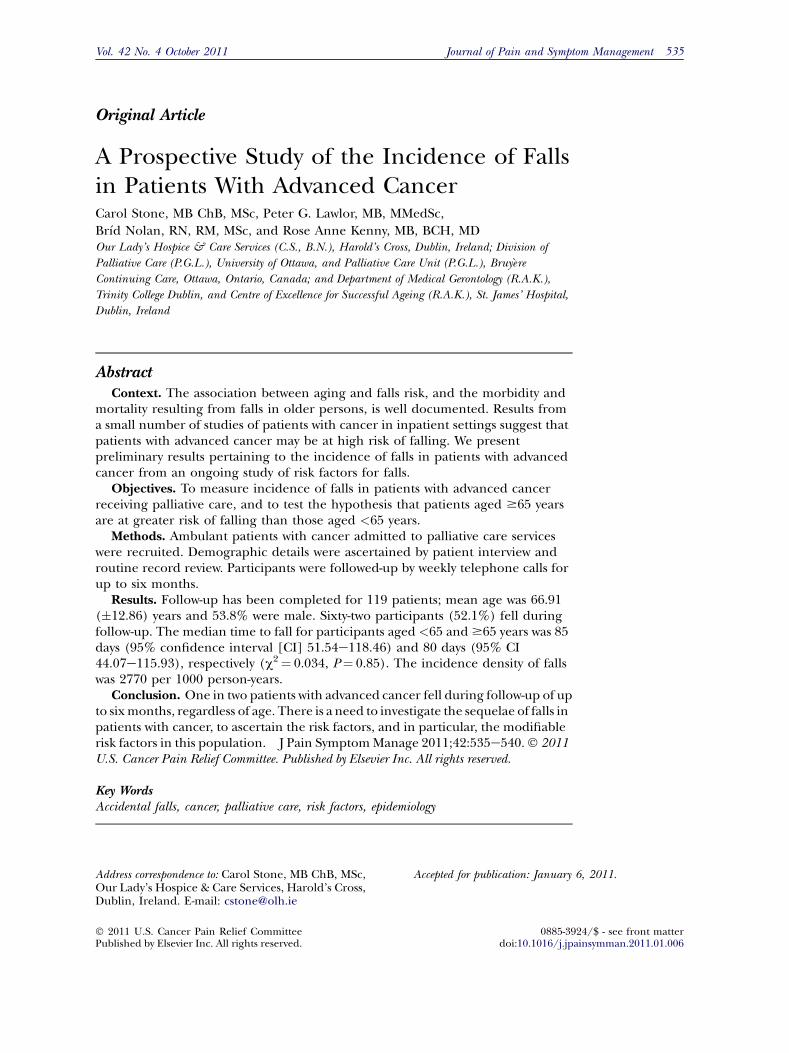
2010, there were 1076 admission episodes,for a total of 761 patients, to the servicesfrom which patients were being recruited;457 were ineligible and 169 declined. Onehundred thirty-five patients have been re-cruited, of whom 119 have completed follow-up and 16 remain under follow-up. Of theparticipants for whom follow-up is complete,55.5% were recruited from outpatient servicesand the remainder from the IPU; the meanage was 66.91 years (�12.86), and 53.8%were male. The most frequent cancer diagno-ses were bronchial, breast, and lower gastroin-testinal cancers. There were no significantdemographic differences between patientswho declined and those who participated(Table 1).
Sixty-two participants (52.1%) sustaineda fall during follow-up, including 24 of 46(52%) participants aged <65 years and 38 of73 (52.2%) aged $65 years. The median timeto fall for participants aged <65 and $65 yearswas 85 days (95% CI 51.54e118.46) and 80days (95% CI 44.07e115.93), respectively(c2¼ 0.034, df 1, P¼ 0.85). There was nodifference in gender composition, perfor-mance status, or median survival from time
Table 1Demographic Details of Participants Who Have Completed Follow-Up to Datea (n¼ 119) and Patients Who
Declined to Participate (n¼ 169)
Demographic Details Study Participants Patients Who Declined Results of Analysis of Differences
GenderMale, frequency (%) 64 (53.8) 83 (49.1) c2¼ 0.609; df 1; P¼ 0.44
Mean age (years) 66.9 (�12.9) 67.5 (�12.8) t¼ 0.372; P¼ 0.71
Cancer diagnosis, frequency (%)Bronchial 20 (16.8) 43 (25.4) c2¼ 11.75; df 9; P¼ 0.23Breast 18 (15.1) 21 (12.4)Lower gastrointestinal 14 (11.8) 23 (13.6)Upper gastrointestinal 15 (12.6) 19 (11.2)Prostate 11 (9.2) 11 (6.5)Gynecological 10 (8.4) 11 (6.5)Pancreatic and hepatobiliary 9 (7.6) 15 (8.9)Urological not prostate 5 (4.2) 10 (5.9)Brain 5 (4.2) 0Other 12 (10.2) 16 (9.5)
Palliative Performance Scale40 1 (1)50 12 (11)60 34 (29)70 42 (35)80 22 (18)90 6 (5)100 2 (2)
aJune 15, 2010.
538 Vol. 42 No. 4 October 2011Stone et al.
of recruitment between the two age groups.The incidence density of falls was 2770 per1000 person-years.
Of the 62 patients who fell, including 20who are alive at time of writing and hencehave a ‘‘censored’’ survival date, the mediansurvival post fall was 73 (95% CI 52.9e93)days. Fifty-five percent of falls occurred in thecommunity (38.7% at home, 11.3% outside,4.8% other indoors) and the remaining 45%in hospital or hospice inpatient settings. Ofthe 62 participants who fell, 28 sustained softtissue injuries, two sustained fractures, andone patient sustained a dislocation.
DiscussionOne in two adults with metastatic or loco-
regionally advanced cancer fell at least onceduring follow-up of up to six months, regard-less of age. Fifty-five percent of falls occurredoutside the hospital/hospice setting and halfresulted in physical injury. The estimated me-dian survival of patients at the time of fallwas 73 daysdan underestimation, as one-third of patients who fell were alive at thetime of analysis.
Our findings suggest that falls are morecommon in adults with advanced cancer thanin community-dwelling older persons: the inci-dence density of falls was 2770 per 1000person-years, more than double the rates re-ported for healthy older persons.23 These re-sults are unprecedented; prior studies ofpatients with cancer reported that 22.4%e27% patients experienced at least one fallper annum. Possible explanations for the dis-crepancy are that the previous studies mayhave included patients with earlier stage dis-ease, that case ascertainment was based on oc-currence of falls in an earlier time period orthat falls were under-reported because of recallbias.It is a limitation of our study that more than
50% of eligible patients declined participation.However, the demographic profiles of partici-pants and nonparticipants were similar and re-semble that of the total population of personsin Ireland living with advanced cancer. Al-though our results may be subject to selectionbias according to characteristics that make pa-tients more likely to be referred to palliativecare services, this may be offset to a certain ex-tent by the breadth of palliative care servicesprovided and our strategy of recruiting from

Vol. 42 No. 4 October 2011 539Incidence of Falls in Advanced Cancer
all facets of these services. Increasing age doesnot appear to be an independent risk factorfor falls in patients with advanced cancer, sug-gesting that the high prevalence of falls is re-lated to factors other than the demographicprofile of cancer.
We have identified that falls are an ex-tremely common experience in advanced can-cer, and yet have raised more questions thananswers: What psychological impact do fallshave in the context of cancer, and does this dif-fer between younger and older age groups? Dofalls cause a decline in physical performanceindependent of baseline functional ability, asin older persons? Are the risk factors, and inparticular the modifiable risk factors, for fallsin patients with cancer the same as in olderpersons? In the face of increasing numbersof people living with advanced cancer becauseof population aging and effectiveness of noveltreatment modalities, we contend that there isan urgent need to address these issues. Knowl-edge of the risk factors for falls in patients withcancer will facilitate identification of patientswho are most at risk and inform decision-making by clinicians and patients regardingbalancing the risk-benefit ratio of any treat-ments shown to increase falls risk. It also willprovide the foundation for falls prevention in-terventions tailored to the needs of patientswith advanced cancer.
Disclosures and AcknowledgmentsThis research was supported by the Health
Research Board and Irish Hospice Foundationthrough the Palliative Care Fellowship awardedto Dr. Stone (HSR/2008/17). Funding also wasreceived from The Atlantic Philanthropies anda gift from a donor. None of the authors havea relationship with any entities that have a finan-cial interest in this topic.
References1. Blake AJ, Morgan K, Bendall MJ, et al. Falls byelderly people at home: prevalence and associatedfactors. Age Ageing 1988;17:365e372.
2. Tinetti ME. Clinical practice. Preventing falls inelderly persons. N Engl J Med 2003;348:42e49.
3. Vellas BJ, Wayne SJ, Romero LJ, Baumgartner RN,Garry PJ. Fear of falling and restriction of mobility inelderly fallers. Age Ageing 1997;26:189e193.
4. Tinetti ME, Williams TF, Mayewski R. Fall riskindex for elderly patients based on number ofchronic disabilities. [see comment]. Am J Med1986;80:429e434.
5. Gannon B, O’Shea E, Hudson E. Economic con-sequences of falls and fractures among older peo-ple. Ir Med J 2008;101:170e173.
6. Department of Health and Children. Health inIreland: Key trends. Dublin, Ireland: Government ofIreland, 2007.
7. American Geriatrics Society, British GeriatricsSociety, and American Academy of Orthopedic Sur-geons Panel on Falls Prevention. Guideline for theprevention of falls in older persons. J Am GeriatrSoc 2001;49:664e672.
8. World Health Organization. WHO global reportof falls prevention in older age. Geneva,Switzerland: World Health Organization, 2007.
9. Gillespie L, Robertson M, Gillespie W, et al. In-terventions for preventing falls in older people liv-ing in the community. Cochrane Database Syst Rev2009; CD007146.
10. Bischoff-Ferrari HA, Dawson-Hughes B,Staehelin HB, et al. Fall prevention with supplemen-tal and active forms of vitamin D: a meta-analysis ofrandomised controlled trials. BMJ 2009;339:b3692.
11. Pearse H, Nicholson L, Bennett M. Falls in hos-pices: a cancer network observational study of fallrates and risk factors. Palliat Med 2004;18:478e481.
12. O’Connell B, Cockayne M, Wellman D, Baker L.Fall risk factors and the nature of falls in inpatientoncology and palliative care settings. ContempNurse 2005;18:247e257.
13. Goodridge D, Marr H. Factors associated withfalls in an inpatient palliative care unit: an explor-atory study. Int J Palliat Nurs 2002;8:548e556.
14. Pautex S, Herrmann F, Zulian G. Factors associ-ated with falls in patients with cancer hospitalisedfor palliative care. J Palliat Med 2008;11:878e884.
15. Overcash J. Prediction of falls in older adultswith cancer: a preliminary study. Oncol Nurs Forum2007;34:341e346.
16. Overcash J, Beckstead J. Predicting falls in olderpatients using components of a comprehensive geri-atric assessment. Clin J Oncol Nurs 2008;12:941e949.
17. Bylow K, Dale W, Mustian K, et al. Falls andphysical performance deficits in older patientswith prostate cancer undergoing androgen depriva-tion therapy. Urology 2008;72:422e427.
18. Overcash JA, Rivera HR Jr. Physical perfor-mance evaluation of older cancer patients: a prelim-inary study. Crit Rev Oncol Hematol 2008;68:233e241.
19. National Patient Safety Agency. Slips, trips andfalls in hospital. Third report from the Patient

540 Vol. 42 No. 4 October 2011Stone et al.
Safety Observatory. London, UK: National PatientSafety Agency, 2007.
20. Katzman R, Brown T, Fuld P, et al. Validation ofa short Orientation-Memory-Concentration Test ofcognitive impairment. Am J Psychiatry 1983;140:734e739.
21. Anderson F, Downing GM, Hill J, Casorso L,Lerch N. Palliative Performance Scale (PPS):a new tool. J Palliat Care 1996;12:5e11.
22. Davison J, Bond J, Dawson P, Steen N, Kenny R.Patients with recurrent falls attending Accident &Emergency benefit from multifactorial interven-tionda randomised controlled trial. Age Ageing2005;34:162e168.
23. Allan LM, Ballard CG, Rowan EN, Kenny RA.Incidence and prediction of falls in dementia: a pro-spective study in older people. PLoS One 2009;4:e5521.



















![Penicillin in Muco-Purulent Conjunctivitis fileFeb., 1951] MUCO-PURULENT CONJUNCTIVITIS: PUTTANNA 39 incidence falls considerably in adults over .16 years as seen in the age incidence](https://img.pdfslide.net/doc/110x75/5d17f25188c9938c2b8c15f0/penicillin-in-muco-purulent-conjunctivitis-1951-muco-purulent-conjunctivitis-puttanna.jpg)









