Embed Size (px)
Citation preview

ARTICLE
A randomized, double-blind, placebo-controlled trial of the effect ofdried purple carrot on body mass, lipids, blood pressure, bodycomposition, and inflammatory markers in overweight and obeseadults: The QUENCH Trial1
Olivia R.L. Wright, Gabriele A. Netzel, and Amy R. Sakzewski
Abstract: Obesity is a significant health issue worldwide and is associated with chronic, low-grade inflammation predisposingthe individual to cardiovascular disease and impaired blood glucose homeostasis. Anthocyanins and phenolic acids from purplecarrots are effective at reversing inflammation and metabolic alterations in animal models, potentially through inhibition ofinflammatory pathways. The effects of dried purple carrot on bodymass, body composition, blood pressure, lipids, inflammatorymarkers, liver function tests, and appetite were investigated in 16 males (aged 53.1 ± 7.6 years and with a mean BMI of 32.8 ±4.6 kg/m2) with normal lipid and inflammatorymarkers. There was no evidence that 118.5 mg/day of anthocyanins and 259.2 mg/dayof phenolic acids for 4 weeks resulted in statistically significant changes in body mass, body composition, appetite, dietaryintake, low density lipoprotein, total cholesterol, blood pressure, or C-reactive protein in these obese participants at the dose andlength of intervention used in this trial. High density lipoprotein cholesterol was lower in the intervention group (p < 0.05).Aspartate amino transferase and alanine amino transferase did not change, indicating that the intervention was safe. Morestudies are required to establish the bioavailability and pharmacokinetic effects of purple carrot anthocyanins and phenolicacids prior to further trials of efficacy with respect to treating inflammation and metabolic alterations.
Key words: purple carrot, anthyocyanin, obesity, lipids, blood pressure.
Résumé : L'obésité constitue une importante préoccupation pour la santé a travers le monde et elle est associée a une inflam-mation chronique de faible niveau qui prédispose a la maladie cardiovasculaire et a une détérioration de l'homéostasie duglucose sanguin. Les anthocyanines et les acides phénoliques des carottes violettes sont efficaces pour renverser l'inflammationet les modifications métaboliques dans des modèles animaux, vraisemblablement a cause de l'inhibition de sentiers inflamma-toires. Les effets de carottes violettes séchées sur le poids corporel, la composition corporelle, la pression sanguine, les lipides,les marqueurs inflammatoires, la fonction hépatique et l'appétit ont été examinés chez 16 hommes âgés de 53,1 ± 7,6 ans ; IMC32,8 ± 4,6 kg/m2 dont les lipides et les marqueurs inflammatoires sont normaux. Il n'y avait pas d'évidence que 118,5 mg/jourd'anthocyanines et 259,2 mg/jour d'acides phénoliques pendant 4 semaines produisaient des changements statistiquementsignificatifs de poids corporel, de composition corporelle, d'appétit, d'apport alimentaire, de cholestérol associé aux lipoproté-ines de faible densité ou de cholestérol total, de pression sanguine et de protéine C-réactive chez ces patients obèses, auxconcentrations et a la durée d'intervention utilisées dans cette étude. Le cholestérol associé aux lipoprotéines de haute densitéétait plus faible dans le groupe avec intervention (p < 0,05). L'aspartate aminotransférase et l'alanine aminotransférase nechangeaient pas, indiquant que l'intervention était sécuritaire. D'autres études sont requises afin d'établir la biodisponibilité etles effets pharmacocinétiques des anthocyanines et des acides phénoliques des carottes violettes avant de poursuivre les testsd'efficacité. carottes violettes, anthocyanines, obésité, lipides, pression sanguine. [Traduit par la Rédaction]
Mots-clés : carottes violettes, anthocyanines, obésité, lipides, pression sanguine.
IntroductionOverweight and obesity is reaching epidemic proportions
worldwide. Clinical features of obesity lead to an increased risk ofdeveloping cardiovascular disease (CVD), insulin resistance, and(or) type 2 diabetes mellitus. The premise that metabolic altera-tions lead to a perpetuation of overweight and obesity is central towidely stated hypotheses that overweight and obesity are due to astate of chronic, low-grade inflammation. In an overweight orobese state, adipose tissue secretes tumor necrosis factor-alpha(TNF-�), which stimulates the recruitment of macrophages via
secretion of monochemotactic protein-1 (MCP-1) from preadi-pocytes (Zivkovic et al. 2007). These immune cells infiltrate adi-pose tissue and release more inflammatory cytokines, includinginterleukin-6 (IL-6) and interleukin-1� (IL-1�), which leads to acti-vation of the transcription factor and intracellular messenger nu-clear factor �B (NF-�B) (Zivkovic et al. 2007; Wallace 2011). Thisincreases lipolysis and the release of free fatty acids from adi-pocytes, resulting in insulin resistance (Laurencikiene et al. 2007).Activation of NF-�B increases activity of Jun N-terminal kinase(JNK) in adipocytes, worsening insulin resistance by (i) disturbing
Received 28 September 2012. Accepted 30 November 2012.
O.R.L. Wright. Centre for Dietetics Research (C-DIET-R), School of Human Movement Studies, and the Queensland Alliance for Agriculture and Food Innovation, The University ofQueensland, Brisbane, Queensland, Australia; Mater Medical Research Institute, Brisbane, Queensland, Australia; Translational Research Institute, Brisbane, Queensland, Australia.G.A. Netzel. Centre for Nutrition and Food Sciences, Queensland Alliance for Agriculture and Food Innovation, The University of Queensland, Brisbane, Queensland, Australia.A.R. Sakzewski. Centre for Dietetics Research (C-DIET-R), School of Human Movement Studies, The University of Queensland, Brisbane, Queensland, Australia.
Corresponding author: Olivia R.L. Wright (e-mail: [email protected]).1This article is one of a number of papers published in the Special Issue on Food as Medicine.
480
Can. J. Physiol. Pharmacol. 91: 480–488 (2013) dx.doi.org/10.1139/cjpp-2012-0349 Published at www.nrcresearchpress.com/cjpp on 2 January 2013.
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

the action of adiponectin, an anti-inflammatory and antiathero-genic adipokine significantly involved in fatty acid oxidation andinsulin sensitivity, and (ii) disrupting insulin receptor function(Hirosumi et al. 2002;Whitehead et al. 2006). The resulting inflam-mation causes fat cells to enlarge, perpetuating the inflammatorycycle observed during obesity. As this process continues, it in-duces adaptations in cardiovascular structure and function, alter-ations in glucose metabolism, blood pressure, lipid metabolism,coagulation, and inflammation, leading to endothelial dysfunc-tion and atherosclerosis (Van Gaal et al. 2006). It also increasessecretion of C-reactive protein (CRP) from hepatocytes and initi-ates liver fibrosis and liver function decline (Zivkovic et al. 2007).
Functional nutrition therapy involving the use of nutrients tosupport and enhance metabolic pathways and reduce inflamma-tion is an emerging field of interest. It may provide significantadjunctive methods for weight management, particularly sinceclinical studies of diet and (or) lifestyle interventions show thatthe majority of patients regain the weight lost within12 months, owing to reduced motivation because of the lack ofprofessional support (Ash et al. 2006), or from physiologicalmechanisms associated with the neuroendocrine regulation offood intake (Sumithran et al. 2011).
The work presented here focuses on the use of flavonoids as afunctional nutritional therapy for weight management. Fla-vonoids are polyphenolic compounds present in fruits and vege-tables, as well as some nuts and seeds. The most abundantflavonoids are anthocyanins (Kolodziejczyk et al. 2011). The mech-anism of action of anthocyanins is related to their inhibitory ef-fects on NF-�B (Wallace 2011). Strategies to downregulate theactivation of NF-�B using phytochemicals presents a promisingstrategy for reducing the chronic inflammation associated withobesity. Interest has recently burgeoned in the functional benefitsof flavonoid pigments in carrots, particularly the original purplevariety, first documented in the 10th century in Iran andNorthernArabia (Arscott et al. 2010). Anthocyanin is the phytochemicalcontributing to the purple pigment of these carrots and has beenassociated with inhibiting cytokines, the COX-2 inflammatorypathway in a mouse model of asthma (Park et al. 2007), and themetabolic syndrome in an obese rat model (Poudyal et al. 2010).In-vitro studies of mouse macrophages (RAW 264.7) and porcineaortic endothelial cells demonstrate that purple carrots reducethe expression of iNOS, IL-6, IL-1�, and TNF-� (Metzger et al. 2008).Approximately 76% of the total anthocyanins in the purple carrotare acylated and less bioavailable than the nonacylated form,withhuman plasma concentrations present in quantities 4 timeshigher for the nonacylated form (Charron et al. 2009). Thus, mea-surement of acylation of anthocyanins is important in clinicaltrials as an indicator of the bioavailability of this nutrient.
Although examined in an animal model of obesity (Poudyalet al. 2010), no studies of the effect of purple carrot on body mass,body composition, or metabolic markers in humans could be lo-cated. It is unclear whether increased consumption of purplecarrot would lead to the metabolic changes noted in animal orin-vitro studies. The primary objective of this study was to mea-sure the effect of a diet, supplemented daily with dried purplecarrot, on body mass, body composition, blood pressure, lipidprofile, and selected inflammatory markers. The secondary objec-tive was to examine the effect on safety biomarkers, includingliver function tests.
Materials and methods
ParticipantsHealthy male volunteers aged 18–65 years with a body mass
index ≥ 25 kg/m2 and ≤ 35 kg/m2 were recruited from Brisbane,Australia, in 2010, for this pilot study. Other inclusion criteriawere as follows: (i) stable blood pressure in the normal (≥110/70mm Hg), high-normal (120–139/80–90mm Hg), ormildly hyper-
tensive (140–159/90–99 mm Hg) ranges (1 mm Hg = 133.322 Pa);(ii) being stable on medication if blood pressure was 140/90–159/99 mm Hg; (iii) being otherwise healthy (i.e., no chronic diseasesor medical conditions); and (iv) having the capability to give in-formed consent. Potential participants were excluded if they werealready consuming purple carrots or purple carrot products.
The study was restricted tomales tominimize confounding dueto gender. Males and females are known to differ systematicallyfor 2 of the key outcomemeasures of the trial: inflammatory stateand body composition. Females experience regular fluctuations inhormones that influence inflammatory state, and generally have ahigher proportion of body fat than males. If both genders hadbeen included in the pilot trial, these effects may have con-founded the conclusions.
Men who responded to email advertisements posted by theWesley Research Institute (WRI), Brisbane, Queensland, the Uni-versity of Queensland, and through a commercial television pro-gram were screened via telephone. Eligible participants wererecruited through the WRI after further explanation about thestudy and written informed consent. Medical history, exercisehistory, and demographic details were collected on commence-ment. The study had approval from the University of Queen-sland's Medical Research Ethics Committee (2010000102) and theUniting Care Human Research Ethics Committee (0955). The trialis registered with the Australia and New Zealand Clinical TrialsRegistry (ACTRN: 12610000209099).
Intervention and controlAll participants and study investigators were blinded to
whether participants were consuming the intervention or pla-cebo throughout the trial. The intervention was presented asRefractanceWindow-dried (RW-dried) purple carrot in sachets forinstant rehydration, weighing 8.3 g per sachet. The 8.3 g driedpurple carrot is equivalent to approximately 100 g fresh carrotaccording to the RWconversion provided by NutraDry (Brisbane,Australia), which is approximately 1.3 servings of carrot (a typicalvegetable serving mass is 75 g).
Anthocyanin and total phenolic content was analyzed by HPLC–PDA following themethod previously described (Padayachee et al.2012). Acylated and nonacylated anthoycanins were separated ona Synergi Hydro-RP column (150 mm × 3 mm inner diameter,4 �m) (Phenomenex, Lane Cove, New South Wales, Australia) us-ing a binary gradient system. Individual anthocyanins were calcu-lated using an external cyanidin 3-glucoside calibration includinga molecular correction factor (Padayachee et al. 2012). The totalphenolic content was determined using the Folin–Ciocalteu assay(Netzel et al. 2012). The dissolved purple carrot powder was fur-ther diluted and assayed at 750 nm in a VICTOR 2030 microplatereader (PerkinElmer, Waltham, Massachusetts, USA). Gallic acidwas used as the standard, and values are expressed as milligramsof gallic acid equivalents (GAE) per 100 mL. The total anthocyanincontent of the intervention was 39.5 ± 1.3 mg/sachet after dissolu-tion in 100 mL water, while the phenolic acid content was 86.4 ±4.8 mg (Table 1).
Participants were requested to consume 3 sachets per day for 4weeks, providing a total daily anthocyanin intake of 118.5 mg(77.1 mg acylated anthocyanin and 41.4 mg nonacylated) and atotal daily phenolic acid intake of 259.2 mg. The control was driedorange carrot. It contained 0 mg/mL anthocyanins and 3.5 ±0.2 mg/100 mL phenolic acid. It was coloured purple using naturalpurple colouring. Participants were requested to maintain theirusual dietary and physical activity habits for the duration of thestudy. The recommended timing for consumption was at evenintervals throughout the day, for example, with the first meal,lunch, and dinner. All measures were completed at baseline andpost-intervention at 4 weeks.
Wright et al. 481
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

Measurement of body mass, body composition, and bloodpressure
Body mass was measured on standing scales attached to theBodPod prior to body compositionmeasurement. Standing heightwas measured, with shoes removed, using a dynamometer. Waistcircumference was measured using a steel measuring tape posi-tioned between the top of the hip bone and the bottom of the ribcage. The BodPod was used to measure fat mass and fat-free mass.It is a valid instrument for measuring changes in body composi-tion over time in obese adults, and utilizes air displacement plethys-mography, a more practical equivalent of underwater weighing(Minderico et al. 2006). Blood pressure was measured in duplicatewith a digital sphygmomanometer while participants were seated.Results were averaged.
Measurement of dietary intake, appetite, and physicalactivity
Participants completed the Wollongong Dietary Inventory tomeasure dietary intake at baseline and 4 weeks. This validatedinstrument collects detailed information about eachmeal, includ-ing the timing, foods consumed, and the amount and frequency ofconsumption. Information provided by participants was cross-checked by a dietitian and further detail was obtained, as re-quired, to assist quantification of intake. Appetite was measuredon a categorical scale from very good to poor. A visual analoguescale (VAS) was used to measure participants' perceptions of hun-ger, sense of fullness, desire to eat, and sense of thirst at baselineand follow-up. Results were reported in millimetre (mm) valuesalong a 100 mm VAS to detect changes (Flint et al. 2000). Partici-pants were asked for a brief description of the amount of timespent in intentional physical activity per week to qualitativelymonitor whether this changed during the trial.
Measurement of adherenceParticipants completed an intervention intake form for each
day of the trial. This was cross-checked against the empty sachetpackets returned at follow-up. Over 90% consumption of the pur-ple carrot sachets (76 out of a possible total 84 sachets for theentire trial period) was considered adherence to the intervention.
Biochemical studiesBlood was collected following an overnight fast at baseline and
post-intervention at 4 weeks. Standard laboratory techniqueswere used for the analysis of total cholesterol, high-density lipo-protein (HDL) and low-density lipoprotein (LDL) cholesterol, trig-lycerides (TG), liver function (aspartate amino transferase (AST)and alanine amino transferase (ALT)), blood glucose, and CRP at acommercial laboratory. Because of the overall low and sometimes
undetectable levels of CRP, results were grouped as ≤2 mmol/L or≥3 mmol/L for the presentation of results.
Statistical analysisStatistical analysiswas completedusing SPSS software version 16.0
(SPSS Inc. Chicago, Illinois, USA) and GraphPad Prism 5.03 (Graph-Pad Software, Inc.). Continuous data were summarized as themean and standard deviation. Categorical data were summarizedas counts and percentages. Normality was assessed using theShapiro–Wilk test. When normality assumptions were satisfied(age, mass, waist, percent body fat, percent fat-free mass, bloodpressure, LDL cholesterol, HDL cholesterol, CRP, and appetite),mean differences in outcome measures at baseline and 4 weekswere assessed using paired samples t tests. When normality as-sumptions were violated (TG and desire to eat), Mann–Whitneytests ofmedians were used to assess differences. Fisher's exact testor Pearson's �2 test was used to assess independence between2 categorical variables. Statistical significance was reported at the95% level (2-tailed). Controlling for age, physical activity habits,and bodymass stability were deemed unwarranted because of thegood randomisation and small sample sizes.
ResultsTable 2 summarises the characteristics of study participants at
baseline and week 4. Sixteenmenwere recruited into the study. Atotal of 15 men completed the study, with one not completing forunknown reasons. This participant was included in the final anal-ysis, in line with the intention-to-treat analysis. The control andintervention group were comparable for age, mass, BMI, waistcircumference, percent body fat, blood pressure, lipids, CRP, andappetite at baseline (Table 2). All participants were mass stable atbaseline. There was no significant association between any cate-gorical variables and treatment allocation (Table 2).
Themean age was 53.1 ± 7.6 years. Mean baseline BMI was 32.8 ±4.6 kg/m2, indicating obesity, while mean waist circumferenceand percent body fat was 115.5 ± 11.8 cm and 38.1% ± 7.0%, respec-tively, indicating central obesity. The sample was “over fat” basedon BMI and age-adjusted recommendations for a body fat percent-age of 29% for men (Gallagher et al. 2000). Despite their obesityand percent body fat, our sample demonstrated a relativelyhealthy metabolic phenotype. Lipids were within the upper nor-mal range at baseline. Most had mildly elevated blood pressure(i.e., <140–159/90–99 mm Hg); however, approximately a thirdhad blood pressure >140/90 <159/99 mm Hg, but were stable onmedication. Liver enzymes, AST and ALT, were in the normalrange at baseline (5–40 and <50 U/L, respectively).
Table 1. Anthocyanin and total phenolic content of intervention and control products.
Test Intervention Control
Anthocyanins (mg/100 mL)NonacylatedCya 3-xylglcgal 1.3±0.1 NondetectableCya 3-xylgal 12.5±0.5 Nondetectable
AcylatedSinapic acid derivative of cya 3-xylglcgal 1.1±0.1 NondetectableFerulic acid derivative of cya 3-xylglcgal 18.2±0.4 Nondetectablep-Coumaric acid derivative of cya 3-xylglcgal 6.4±0.2 Nondetectable
� Anthyocyanins 39.5±1.3 NondetectablePhenolic acids (mg/100 mL)Neochlorogenic acid 3.4±0.1 NondetectableChlorogenic acid 79.9±4.5 3.5±0.2Caffeic acid 2.4±0.1 NondetectableFerulic acid 0.8±0.1 Nondetectable� Phenolic acids 86.4±4.8 3.5±0.2Total phenolics (Folin–Ciocalteu) (mg GAE/100 mL) 131.3±7.2 3.5±0.2
Note: GAE, gallic acid equivalents.
482 Can. J. Physiol. Pharmacol. Vol. 91, 2013
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

Indicators of bioavailability of the interventionThe anthocyanins in the intervention product were 65%
acylated. Nonacylation is associated with higher bioavailability(Charron et al. 2009).
Effects of purple carrot on body mass, body composition,blood pressure, lipids, and inflammatory markers
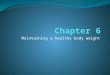
There were no significant differences for most variables be-tween baseline and week 4 for the control or intervention groups.Body mass showed an average decrease of 0.5 kg over 4 weeks inthe intervention group, but this was not statistically significant(p = 0.08). There were no significant alterations in body composi-tion. HDL cholesterol was significantly lower in the interventiongroup after 4 weeks (p < 0.05). Figure 1 presents graphs showing acomparison of body mass, percent body fat, HDL cholesterol,blood pressure, and CRP at baseline and week 4 for the controland intervention groups. Statistical parameters are presented oneach graph.
Biomarkers of safetyAST and ALT did not change significantly in the intervention or
control group over 4 weeks. Figure 2 shows comparisons of ASTand ALT at baseline and 4 weeks for the control and interventiongroups.
Effects of purple carrot on appetite, energy intake, andphysical activity
There were no changes in dietary intake or physical activityreported between baseline and week 4 for either the interventionor control group. The average dietary intake values at baselineand week 4 for both groups demonstrate under-reporting andsubstantial standard deviations (up to ±2000 kJ) and therefore
could not be used further. Average reported intakes representedapproximately 80%–90% of participants' resting metabolic rate, ascalculated by the BodPod.
Table 3 summarizes appetite ratings at baseline and week 4 forthe control and intervention groups. Data are presented as counts(percentages) and statistical data are provided. There were no sig-nificant differences in appetite changes between the interventionand control groups over the 4 weeks; however, at week 4, therewas a trend for lower overall appetite in the intervention group(p = 0.061). When the individual components of appetite wereexamined, there were no significant differences in reported hun-ger, sense of fullness, desire to eat, or sense of thirst betweenbaseline and 4 weeks for either the intervention or control group.
DiscussionThis is the first study to evaluate the effect of purple carrot
consumption on body mass, body composition, blood pressure,lipid profile, and selected inflammatorymarkers. Key strengths ofthe study include the randomised controlled trial design, the anal-ysis of both acylated and nonacylated anthocyanins in the inter-vention and control product, and the use of a robust measure ofbody composition, the BodPod, rather than relying solely on an-thropometric measurements. Our findings suggest that supple-menting the diet with purple carrot in the form of a powderedbeverage, equivalent to 118.5 mg anthocyanins and 259.2 mg phe-nolic acids per day for 4 weeks, is safe, but had no significanteffect on mass, body composition, blood pressure, waist circum-ference, appetite, or systemic inflammation. The levels of antho-cyanins and phenolic acids in the trial product were within theexpected range based on published analyses of a variety of breedsof purple carrots (1.5 ± 0.3 to 17.7 ± 1.9 mg anthocyanins/100 g and
Table 2. Characteristics at baseline and 4 weeks for participants (n = 16) in a randomized, double-blind, placebo-controlled trial of the effect ofdried purple carrot on body mass, lipids, blood pressure, body composition, and inflammatory markers.
Intervention (n = 8) Control (n =8) Intervention (n = 8) Control (n = 8)Variables Baseline Baseline p-value 4 weeks 4 weeks p-value
Age (years) 51.4±7.6 55.0±7.8 0.361 — — —Mass (kg) 102.9±14.1 100.9±17 0.802 102.4±14.4 101.1±16.3 0.867BMI (kg/m2) 32.4±5.0 34.0±4.4 0.517 31.9±5.1 33.7±4.3 0.457Waist circumference (cm) 115.2±11.8 115.5±12.3 0.917 115.3±11.8 115.5±12.3 0.914Average systolic BP (mm Hg) 135.4±15.5 141.2±15.2 0.574 135.4±15.5 141.2±15.2 0.359Average diastolic BP (mm Hg) 85.1±10.7 82.5±3.8 0.885 85.1±10.7 82.5±3.8 0.807Average RMR (kJ) 7500±740 7300±950 0.645 7400±740 7300±1000 0.783Daily reported total energy intake (kJ) 6100±1320 6500±2000 0.650 6100±1320 6500±2000 0.650Daily intake (kJ) as % of RMR (kJ) 82±20 90±30 0.540 83±20 90±30 0.604% Fat mass 37.9±6.6 38.4±7.9 0.887 37.3±6.9 38.8±7.5 0.678% Fat-free mass 62.1±6.6 61.6±7.9 0.887 62.7±6.9 61.2±7.5 0.678AST (U/L) 24.9±6.1 26.0±9.0 0.773 27.1±10.7 24.1±11.6 0.616ALT (U/L) 25.6±6.5 32.9±15.4 0.240 35.8±15.5 31.3±19.9 0.802HDL cholesterol (mmol/L) 1.2±0.2 1.2±0.3 0.760 1.1±0.2 1.1±0.2 1.000LDL cholesterol (mmol/L) 3.2±0.5 3.5±0.8 0.354 3.2±0.6 3.5±0.9 0.279Total cholesterol (mmol/L) 5.1±0.3 5.5±1.0 0.299 5.0±0.6 5.4±1.0 0.234Triglycerides (mmol/L) 1.3 (0.9–16) 1.6 (0.9–2.8) 0.382 1.2 (0.5–5.2) 1.9 (1.0–2.7) 0.083C-reactive protein≤2 mmol/L 3 (37.5) 4 (50.0) 0.614 4 (50.0) 6 (75.0) 0.614≥3 mmol/L 5 (62.5) 4 (50.0) 0.614 4 (40.0) 2 (25.0) 0.614AppetiteVery good 3 (37.5) 3 (37.5) 0.198 1 (12.5) 1 (12.5) 0.061Good 2 (25.0) 4 (50.0) 0.198 3 (37.5) 7 (87.5) 0.061Ok 3 (37.5) 0 (0.0) 0.198 4 (50.0) 0 (0.0) 0.061Poor 0 (0.0) 1 (12.5) 0.198 0 (0.0) 0 (0.0) 0.061Hunger (mm) 42.1±22.8 43.4±25.5 0.606 49.4±9.1 52.5±14.7 0.340Sense of fullness (mm) 53.4±24.8 40.5±21.8 0.950 48.6±25.3 52.3±16.6 0.867Desire to eat (mm) 46.5 (0–85) 62.5 (0–77) 0.645 52.5 (44–76) 62.5 (25–75) 0.721Sense of thirst (mm) 45.3±28.2 48.3±24.6 0.695 47.1±23.1 49.9±12.7 0.429
Note: Values represent the mean ± SD or median (range) except the variables for C-reactive protein and appetite, which represent the number of individuals withthe percent of individuals per group in parentheses. BMI, body mass index; BP, blood pressure; RMR, resting metabolic rate; AST, aspartate amino transferase; ALT,alanine amino transferase; HDL, high-density lipoprotein; and LDL, low-density lipoprotein; 1 mm Hg = 133.322 Pa.
Wright et al. 483
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

17.9 ± 1.4 to 97.9 ± 3.2mg GAE/100 g total phenolics) (Montilla et al.2011).
The purple carrot intervention was associated with a small reduc-tion in the HDL component of cholesterol (p < 0.05) rather than theLDL component; however, there were no significant differences intotal cholesterol. In contrast, a randomized placebo-controlled4-week crossover study of anthocyanin supplementation (640 mg/day) in prehypertensive men (n = 31) indicated positive effects oncardiovascular parameters, with significant elevations in HDLcholesterol (Hassellund et al. 2012). A 12-week study in dyslipide-mic patients (n = 120) established that a daily anthocyanin supple-ment (160 mg) achieved significant elevations in HDL cholesteroland reductions in LDL cholesterol, possibly due to suppression ofthe cholesterol ester transfer protein (CETP) pathway (Qin et al.2009). CETP transfers apolipoprotein A-I (apoA-I) to HDL (Davidson2011) and controls the transfer of TG between HDL and very-low-density lipoprotein, intermediate-density lipoprotein, and LDLcholesterol (Brewer 2011). Inhibiting the CETP pathway upregu-lates apoA-I synthesis through reducing its clearance rate(Badimón and Ibáñez 2010), thereby resulting in higher levels ofHDL cholesterol. It may also have the side effect of raising bloodglucose levels (Brewer 2011), as demonstrated by Hassellund et al.(2012). Our results suggest the dosage of anthocyanin used in ourtrial was not sufficient to suppress the CETP pathway to achievethese effects on lipid or glucose parameters. The participants inour study were also not dyslipidemic. This, combined with ourshorter trial length, may assist in explaining the discrepancy inresults.
Other studies of foods rich in anthocyanins have producedmixed findings across a range of biomarkers because of variationsin anthocyanin dose, food matrix and processing, participants'levels of baseline chronic disease biomarkers, ill-defined anthocy-anin bioavailability, study duration, and complex, not well under-stood dose–response relationships (Wallace 2011; Kay et al. 2012).Elderberry anthocyanins (500mg capsule/day for 12 weeks) had noeffect on plasma anthocyanin levels, CVD biomarkers, liver finc-tion, or kidney function in postmenopausal women with normallevels at baseline (Curtis et al. 2009). Conversely, consumption offreeze-dried blueberries (50 g for 8 weeks) in a sample of males(n = 4) and females (n = 44) with elevated blood pressure and lipidsat baseline resulted in a significant reduction in blood pressureand oxidized-LDL cholesterol (n = 48); however, the anthocyanincontent was not reported (Basu et al. 2010).
Another study using freeze-dried whole blueberry powder (45 gpowder per day; 668 mg anthocyanins; 1462 mg total phenolics;equivalent to 2 cups fresh blueberries per day for 6 weeks) dem-onstrated improvements in whole body insulin sensitivity asmea-sured by the hyperinsulinaemic–euglycaemic clamp (p < 0.05) inpatients who were insulin resistant; however, there were nochanges in adiposity, energy intake, or inflammatory biomarkers(Stull et al. 2010). Freeze-drying is well recognized as a superiorfood preservationmethod for nutrient retention (Orak et al. 2012).It is possible that several stages of processing of the purple carrotpowder used in our study resulted in nutrient losses, as the antho-cyanin and total phenolic content was within the lower-expectedrange for purple carrot.
In relation to the molecular mechanisms of the low-grade,chronic inflammation in obesity, Karlsen (2007) showed reduced
activation of NF-�B human monocytes in healthy adults (n = 140)after consumption of 600 mg bilberry anthocyanins daily for3 weeks, in addition to reductions in cytokines interleukin-4 (IL-4)and interleukin-13 (IL-13) (Karlsen et al. 2007). Lehtonen et al.(2010) examined the effects of 4 berry species on CVD risk factorsand liver function in overweight women with metabolic syn-drome (n = 61; 20 weeks). Reductions in ALT (23%) suggested thatliver function improved and adiponectin levels also increased. Nostudies have proposed hypotheses for the mechanisms of antho-cyanins improving adiponectin expression or secretion; however,it is known that vitamin C is an essential nutrient for the secretionof adiponectin, particularly the more metabolically active highmolecular weight form (Rose et al. 2010). The berries would havealso been rich in vitamin C. This highlights a significant challengewith clinical trials of phytochemicals, i.e., determining whichphytochemical, vitamin, ormineral is having themost significanteffect, or whether a range of compounds areworking additively orsynergistically. It also questions whether it is important to iden-tify a single phytochemical as a novel therapeutic or to recom-mend the consumption of the whole food. It is unclear whetheranthocyanins or their related compounds exhibit any effect inhumans in isolated form; however, this could be studied in moredepth if a consistent trend of results emerged showing these com-pounds had substantial and consistent effects on metabolic andinflammatory biomarkers in vivo. At present there is insufficientevidence to warrant such an investigation. It is also important tonote that the trial of 4 berries was significantly longer comparedwith other studies, which may account for the more positive re-sults obtained.
Lifestyle interventions with evidence-based kilojoule deficitsand exercise programs aim for a loss of approximately 0.5–1.0 kgper week, which in this case, would have equated to a loss of2–4 kg or 2%–4% bodymass over the course of the study. Althoughthere was a trend towards 0.5 kgmass loss over the 4 weeks in theintervention group, this is not considered clinically significantand was not statistically significant. The timeframe for this studywas stipulated by the Human Research Ethics Committee provid-ing approval, is half the length of previous animal trials (Poudyalet al. 2010), and approximately a third of the length of most ran-domized controlled trials in this field (Wallace 2011). It is not clearwhethermore significant changes would have occurred if the trialhad continued for a longer time period.
The trend towards lower overall appetite levels reported by theintervention group in our study was interesting, but it is unclearwhat this was related to, as the individual components of appetitethat we measured remained unchanged. There were no reports ofappetite trends as a result of anthocyanin consumption in thepublished literature, but this may be worth investigating furtherin future work.
There was significant under-reporting of dietary intake in ourstudy. This is common in dietary research, particularly with par-ticipants who are overweight or obese (Karelis et al. 2009; Mendezet al. 2011). All participants would have been expected to loseweight based on their reported intakes, which were approxi-mately 80%–90% of their resting metabolic rate; however, this didnot occur. Additional strategies to improve accurate reporting ofintake, for example, the use ofmultiplemethods ofmeasurement
Fig. 1. Baseline and week 4 comparisons show that dried purple carrot supplementation (118.5 mg anthocyanins/day and 259.2 mg phenolicacids/day) for 4 weeks does not affect body mass, percent body fat, systolic blood pressure, or C-reactive protein in the control or interventiongroup. High-density lipoprotein cholesterol was significantly lower in the intervention group after 4 weeks (p < 0.05). (A and B) Mean bodymass (kg) at baseline and 4 weeks for the control and intervention groups respectively; (C and D) mean percentage body fat at baseline and4 weeks for the control and intervention groups respectively; (E and F) mean systolic blood pressure at baseline and 4 weeks for the controland intervention groups respectively; (G and H) mean high density lipoprotein cholesterol at baseline and 4 weeks for the control andintervention groups, respectively; (I and J) mean C reactive protein at baseline and week 4 for the control and intervention groupsrespectively; 1 mm Hg = 133.322 Pa.
484 Can. J. Physiol. Pharmacol. Vol. 91, 2013
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

Wright et al. 485
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

and standard portion size diagrams, might be of benefit in futurestudies.
There were no changes in body composition for either groupduring our trial, contrasting with results from an animal studywhere abdominal fat deposition was reduced after 8 weeks ofpurple carrot juice consumption (Poudyal et al. 2010). This raises asignificant challenge in translating the findings from animal tri-als of short-term diet-induced obesity into trials in humans whohavemaintained lifestyles leading to obesity for a number of years(i.e., long-term diet-induced obesity). The challenge for future re-search in this area is how best to use the results of animal trials todesign clinical trials of novel phytochemicals for the preventionand (or) treatment of chronic disease. It is important to questionwhether the potential role of these novel phytochemicals is as
adjunctive therapy to dietary and (or) lifestyle intervention or as asole therapeutic. Our trial indicates poor efficacy of purple carrotas a sole therapeutic; however, futurework examining its effect asan adjunctive therapy to an intensive diet and lifestyle interven-tion may provide further insight into its positive applications,which would be expected to add value to the consideration of arange of phytochemicals for this purpose.
Prior to commencing such adjunctive therapy studies, the bio-availability and pharmacokinetics of the range of compounds inpurple carrots requires further understanding. Anthocyanins gen-erally have poor bioavailability. It is thought that approximately76% of total anthocyanins in purple carrot juice are acylated andless bioavailable than the nonacylated form, with plasma concen-trations present in quantities 4 times higher for the nonacylatedform (Charron et al. 2009). In our study, 65% of the total anthocya-nins in the intervention product were acylated, which may havecontributed to the nonsignificant results. Absorption of anthocya-nins has been shown to decline as the dosage increases; however,an absorption saturation dose has not been identified (Charronet al. 2009). The measurement of AST and ALT was an importantcomponent for assessing safety of the trial intervention and isinfrequently completed in dietary studies. The results demon-strated no hepatotoxicity as a result of the intervention, confirm-ing future work utilising this intervention, at this dose, would notbe harmful. Future studies testing higher doses should continueto measure such indicators of safety.
LimitationsThis study was a pilot clinical trial. Because of the small sample
size, the study may lack statistical power, that is, the ability to
Fig. 2. Baseline and week 4 comparisons show that aspartate amino transferase and alanine amino transferase did not change significantly inthe intervention (fed dried purple carrot; 118.5 mg anthocyanins/day and 259.2 mg phenolic acids/day) or control (fed dried orange carrot)groups after 4 weeks. (A and B) Mean alanine amino transferase at baseline and week 4 for the control and intervention groups respectively;(C and D) mean aspartate amino transferase at baseline and week 4 for the control and intervention groups respectively.
Table 3. Change in appetite rating for interventionand control groups at 4 weeks for participants (n = 16)in a randomized, double-blind, placebo-controlledtrial of the effect of dried purple carrot on bodymass,lipids, blood pressure, body composition, and inflam-matory markers.
Appetiterating
Intervention(n = 8)
Control(n = 8)
Declined 3 (37.5) 2 (25.0)Improved 2 (25.0) 1 (12.5)No change 3 (37.5) 5 (62.5)
Note:Values represent the number of individuals with thepercent of individuals per group in parentheses.. The differ-ence between groups was not significant based on a Pear-son's �2 test (p = 0.485).
486 Can. J. Physiol. Pharmacol. Vol. 91, 2013
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

detect genuine differences between groups; however, the studyprovides important pilot data for the planning of future trials.Results for the outcomemeasure of weight change will be used todetermine sample size requirements for such work. Anthocyaninlevels in plasma were not measured but should be examined infuture studies as markers of bioavailability and adherence to theintervention.
ConclusionsThe results of this study do not support the use of dietary sup-
plementation with dried purple carrot (118.5 mg anthocyanins/day and 259.2 mg phenolic acids/day) to achieve weight loss,improvements in body composition, lipids, blood pressure, orinflammation in obese men with normal lipid levels and low lev-els of inflammatory biomarkers; however, results suggest that it issafe. Examining the effects of this intervention in men with dys-lipidemia and higher levels of inflammatory biomarkers would beworthwhile, as there appears to be minimal effects for those withnormal levels at baseline. Effects of interventions in groups withhealthy metabolic phenotypes may be subtle and not detected byroutine clinical measurements. A deeper investigation of molec-ular and gene-level effects may be required to better understandthe roles of functional nutrition therapy in these groups.
Broader investigation of other potentially significant phyto-chemicals in purple carrots, including polyacetylenes, is war-ranted given their reported anti-inflammatory effects (Metzgeret al. 2008). Future research should focus on understanding themolecularmechanisms and active ingredients of purple carrots asadjunctive therapies to intensive dietary and (or) lifestyle inter-vention, and their effects on other inflammatory and (or) cardio-vascular markers, for example, low and high molecular weight,and total adiponectin. Clinical trials of longer duration withlarger sample sizes are required to establish the bioavailabilityand pharmacokinetic effects of anthocyanins and other poten-tially therapeutic phytochemicals in purple carrot prior to addi-tional studies of efficacy.
AcknowledgementsThe authors acknowledge the support of the University of
Queensland's Early Career Researcher Fund and Summer Scholar-ship Program, and industry funding from Dr. Red Nutraceuticals.The authors acknowledge preliminary statistical support fromDr.Mary Waterhouse and preliminary trial support from ProfessorSandra Capra, Associate Professor Judy Bauer, Professor LindsayBrown, Melanie Bannister, Christie Fay, Yun-Chi Hung, andNatalie Webster. The authors thank Professor Capra for com-ments on the manuscript draft.
ReferencesArscott, S.A., Simon, P.W., and Tanumihardjo, S.A. 2010. Anthocyanins in
purple-orange carrots (Daucus carota L.) do not influence the bioavailability of�-carotene in young women. J. Agr. Food Chem. 58(5): 2877–2881. doi:10.1021/jf9041326. PMID:20131807.
Ash, S., Reeves, M., Bauer, J., Dover, T., Vivanti, A., Leong, C., et al. 2006. Arandomised control trial comparing lifestyle groups, individual counsellingand written information in the management of weight and health outcomesover 12 months. Int. J. Obes. 30(10): 1557–1564. doi:10.1038/sj.ijo.0803263.PMID:16534529.
Badimón, J.J., and Ibáñez, B. 2010. Increasing high-density lipoprotein as a ther-apeutic target in atherothrombotic disease. Rev. Esp. Cardiol. 63(3): 323–333.doi:10.1016/s1885-5857(10)70065-7. PMID:20196993.
Basu, A., Du, M., Leyva, M.J., Sanchez, K., Betts, N.M., Wu, M., et al. 2010. Blue-berries decrease cardiovascular risk factors in obese men and women withmetabolic syndrome. J. Nutr. 140(9): 1582–1587. doi:10.3945/jn.110.124701.PMID:20660279.
Brewer, H.B., Jr. 2011. Clinical review: the evolving role of HDL in the treatmentof high-risk patients with cardiovascular disease. J. Clin. Endocr. Metab.96(5): 1246–1257. doi:10.1210/jc.2010-0163. PMID:21389140.
Charron, C.S., Kurilich, A.C., Clevidence, B.A., Simon, P.W., Harrison, D.J.,Britz, S.J., et al. 2009. Bioavailability of anthocyanins from purple carrotjuice: effects of acylation and plant matrix. J. Agr. Food Chem. 57(4): 1226–1230. doi:10.1021/jf802988s. PMID:19166298.
Curtis, P.J., Kroon, P.A., Hollands, W.J., Walls, R., Jenkins, G., Kay, C.D., et al.2009. Cardiovascular disease risk biomarkers and liver and kidney functionare not altered in postmenopausal women after ingesting an elderberry ex-tract rich in anthocyanins for 12 weeks. J. Nutr. doi:10.3945/jn.109.113126.PMID:19793846.
Davidson, M.H. 2011. Apolipoprotein A-I therapy: promise, challenges, and dis-appointment. J. Am. Coll. Cardiol. 57(9): 1120–1121. doi:10.1016/j.jacc.2010.11.025. PMID:21255956.
Flint, A., Raben, A., Blundell, J.E., and Astrup, A. 2000. Reproducibility, powerand validity of visual analogue scales in assessment of appetite sensations insingle test meal studies. Int. J. Obes. 24: 38–48. doi:10.1038/sj.ijo.0801083.PMID:10702749.
Gallagher, D., Heymsfield, S.B., Heo, M., Jebb, S.A., Murgatroyd, P.R., andSakamoto, Y. 2000. Healthy percentage body fat ranges: an approach fordeveloping guidelines based on body mass index. Am. J. Clin. Nutr. 72(3):694–701. PMID:10966886.
Hassellund, S.S., Flaa, A., Kjeldsen, S.E., Seljeflot, I., Karlsen, A., Erlund, I., et al.2012. Effects of anthocyanins on cardiovascular risk factors and inflamma-tion in pre-hypertensivemen: a double-blind randomized placebo-controlledcrossover study. J. Hum. Hypertens. doi:10.1038/jhh.2012.4. PMID:22336903.
Hirosumi, J., Tuncman, G., Chang, L., Gorgun, C.Z., Uysal, K.T., Maeda, K., et al.2002. A central role for JNK in obesity and insulin resistance. Nature,420(6913): 333–336. doi:10.1038/nature01137. PMID:12447443.
Karelis, A.D., Lavoie, M.E., Fontaine, J., Messier, V., Strychar, I., Rabasa-Lhoret, R.,et al. 2009. Anthropometric, metabolic, dietary and psychosocial profiles ofunderreporters of energy intake: a doubly labeled water study among over-weight/obese postmenopausal women. A Montreal Ottawa New EmergingTeam study. Eur. J. Clin. Nutr. 64(1): 68–74. doi:10.1038/ejcn.2009.119. PMID:19756035.
Karlsen, A., Retterstøl, L., Laake, P., Paur, I., Kjølsrud-Bøhn, S., Sandvik, L., et al.2007. Anthocyanins inhibit nuclear factor-�B activation in monocytes andreduce plasma concentrations of pro-inflammatory mediators in healthyadults. J. Nutr. 137(8): 1951–1954. PMID:17634269.
Kay, C.D., Hooper, L., Kroon, P.A., Rimm, E.B., and Cassidy, A. 2012. Relativeimpact of flavonoid composition, dose and structure on vascular function: Asystematic review of randomised controlled trials of flavonoid-rich foodproducts. Mol. Nutr. Food Res. 56(11): 1605–1616. doi:10.1002/mnfr.201200363.PMID:22996837.
Kolodziejczyk, J., Saluk-Juszczak, J., Posmyk, M., Janas, K., and Wachowicz, B.2011. Red cabbage anthocyanins may protect blood plasma proteins and lip-ids. Cent. Eur. J. Biol. 6(4): 565–574. doi:10.2478/s11535-011-0037-5.
Laurencikiene, J., vanHarmelen, V., ArvidssonNordström, E., Dicker, A.,Blomqvist, L., Näslund, E., et al. 2007. NF-�B is important for TNF-�-inducedlipolysis in human adipocytes. J. Lipid Res. 48(5): 1069–1077. doi:10.1194/jlr.M600471-JLR200. PMID:17272828.
Lehtonen, H.M., Suomela, J.P., Tahvonen, R., Vaarno, J., Venojarvi, M., Viikari, J.,et al. 2010. Berry meals and risk factors associated with metabolic syndrome.Eur. J. Clin. Nutr. 64(6): 614–621. doi:10.1038/ejcn.2010.27. PMID:20197789.
Mendez, M.A., Popkin, B.M., Buckland, G., Schroder, H., Amiano, P.,Barricarte, A., et al. 2011. Alternative methods of accounting for underreport-ing and overreporting when measuring dietary intake – obesity relations.Am. J. Epidemiol. 173(4): 448–458. doi:10.1093/aje/kwq380. PMID:21242302.
Metzger, B.T., Barnes, D.M., and Reed, J.D. 2008. Purple carrot (Daucus carota L.)polyacetylenes decrease lipopolysaccharide-induced expression of inflam-matory proteins in macrophage and endothelial cells. J. Agr. Food Chem.56(10): 3554–3560. doi:10.1021/jf073494t. PMID:18433135.
Minderico, C., Silva, A., Teixeira, P., Sardinha, L., Hull, H., and Fields, D. 2006.Validity of air-displacement plethysmography in the assessment of bodycomposition changes in a 16-month weight loss program. Nutr. Metab. 3(1): 32.doi:10.1186/1743-7075-3-32. PMID:16925811.
Montilla, E.C., Arzaba, M.R., Hillebrand, S., and Winterhalter, P. 2011. Anthocy-anin composition of black carrot (Daucus carota ssp. sativus var. atrorubensAlef.) cultivars Antonina, Beta Sweet, Deep Purple, and Purple Haze. J. Agr.Food Chem. 59(7): 3385–3390. doi:10.1021/jf104724k. PMID:21381748.
Netzel, M., Fanning, K., Netzel, G., Zabaras, D., Karagianis, G., Treloar, T., et al.2012. Urinary excretion of anthocyanins in healthy humans following QueenGarnet plum juice ingestion: a new plum variety rich in antioxidant com-pounds. J. Food Biochem. 36: 159–170. doi:10.1111/j.1745-4514.2010.00522.x.
Orak, H., Aktas, T., Yagar, H., Isbilir, S.S., Ekinci, N., and Sahin, F.H. 2012. Effectsof hot air and freeze drying methods on antioxidant activity, colour andsome nutritional characteristics of strawberry tree (Arbutus unedo L) fruit.Food Sci. Technol. Int. 18(4): 391–402. doi:10.1177/1082013211428213. PMID:22522307.
Padayachee, A., Netzel, G., Day, L., Zabaras, D., Mikkelsen, D., and Gidley, M.J.2012. Binding of polyphenols to plant cell wall analogues. Part 1: Anthocya-nins. Food Chem. 134: 155–161. doi:10.1016/j.foodchem.2012.02.082.
Park, S.-J., Shin, W.-H., Seo, J.-W., and Kim, E.-J. 2007. Anthocyanins inhibitairway inflammation and hyperresponsiveness in a murine asthma model.Food Chem. Toxicol. 45(8): 1459–1467. doi:10.1016/j.fct.2007.02.013. PMID:17512652.
Poudyal, H., Panchal, S., and Brown, L. 2010. Comparison of purple carrotjuice and �-carotene in a high-carbohydrate, high-fat diet-fed rat model
Wright et al. 487
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.

of the metabolic syndrome. Br. J. Nutr. 104(9): 1322–1311. doi:10.1017/S0007114510002308. PMID:20619064.
Qin, Y., Xia, M., Ma, J., Hao, Y., Liu, J., Mou, H., et al. 2009. Anthocyanin supple-mentation improves serum LDL- and HDL-cholesterol concentrations associ-ated with the inhibition of cholesteryl ester transfer protein in dyslipidemicsubjects. Am. J. Clin. Nutr. 90(3): 485–492. doi:10.3945/ajcn.2009.27814. PMID:19640950.
Rose, F.J., Webster, J., Barry, J.B., Phillips, L.K., Richards, A.A., andWhitehead, J.P. 2010.Synergistic effects of ascorbic acid and thiazolidinedione on secretion of highmolecular weight adiponectin from human adipocytes. Diabetes Obes. Metab.12(12): 1084–1089. doi:10.1111/j.1463-1326.2010.01297.x. PMID:20977580.
Stull, A.J., Cash, K.C., Johnson, W.D., Champagne, C.M., and Cefalu, W.T. 2010.Bioactives in blueberries improve insulin sensitivity in obese, insulin-resistant men and women. J. Nutr. 140(10): 1764–1768. doi:10.3945/jn.110.125336. PMID:20724487.
Sumithran, P., Prendergast, L.A., Delbridge, E., Purcell, K., Shulkes, A.,Kriketos, A., et al. 2011. Long-term persistence of hormonal adaptations toweight loss. New Engl. J. Med. 365(17): 1597–1604. doi:10.1056/NEJMoa1105816.PMID:22029981.
VanGaal, L.F., Mertens, I.L., and DeBlock, C.E. 2006. Mechanisms linking obe-sity with cardiovascular disease. Nature, 444(7121): 875–880. doi:10.1038/nature05487. PMID:17167476.
Wallace, T.C. 2011. Anthocyanins in cardiovascular disease. Adv. Nutr. 2(1): 1–7.doi:10.3945/an.110.000042. PMID:3042791.
Whitehead, J.P., Richards, A.A., Hickman, I.J., Macdonald, G.A., and Prins, J.B.2006. Adiponectin: a key adipokine in the metabolic syndrome. Diabetes Obes.Metab. 8(3): 264–280. doi:10.1111/j.1463-1326.2005.00510.x. PMID:16634986.
Zivkovic, A.M., Berman, J.B., and Sanyal, A.J. 2007. Comparative review of dietsfor themetabolic syndrome: implications for nonalcoholic fatty liver disease.Am. J. Clin. Nutr. 86: 285–300. PMID:17684197.
488 Can. J. Physiol. Pharmacol. Vol. 91, 2013
Published by NRC Research Press
Can
. J. P
hysi
ol. P
harm
acol
. Dow
nloa
ded
from
ww
w.n
rcre
sear
chpr
ess.
com
by
Dep
osito
ry S
ervi
ces
Prog
ram
on
11/0
7/14
For
pers
onal
use
onl
y.