Embed Size (px)
Citation preview
CASE REPORT
A rare case of subcutaneous Sweet’s syndrome in a patientwith chronic myelogenous leukemia: a case reportand review of the literature
Congli Wang & Mary Ellen Martin & Roberta E. Smith &
Deline DaCosta & Raghava Levaka Veera & Irma E. Palazzo
Received: 18 February 2014 /Accepted: 23 May 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Subcutaneous Sweet’s syndrome (SS) is a rare var-iant of classic SS characterized by a neutrophilic infiltrateexclusively or predominantly in the subcutaneous tissue, withminimal or absent dermal involvement.We report the case of apatient with a history of chronic myelogenous leukemia whodeveloped subcutaneous SS. Although it has been describedin patients with myelodysplastic syndromes and acute mye-loid leukemia, this is the first report, to our knowledge, of thisrare entity occurring in the setting of a myeloproliferativedisorder.
Keywords Subcutaneous Sweet’s syndrome . Chronicmyelogenous leukemia . Neutrophilic infiltrates . Myeloiddisorders
Introduction
Sweet’s syndrome (SS), also known as acute febrile neutro-philic dermatosis, is characterized by the sudden onset offever, multiple tender erythematous papules and plaques,and the presence of intense neutrophilic infiltrates on skinbiopsy that are typically located in the upper dermis. SS isoften associated with hematologic disease, and to a lesserextent with solid tumors [1–5].
Subcutaneous SS is a rare variant in which the neutrophilicinfiltrate is exclusively or predominantly located in the sub-cutaneous tissue, with minimal or no dermal involvement [6,7]. Subcutaneous SS is almost exclusively associated withmyeloid disorders. To the best of our knowledge, only 16cases have been reported in such a setting in the English-language literature to date [8–19], including ten cases withmyelodysplastic syndromes (MDS) and six cases with acutemyeloid leukemia (AML). We describe the case of a patientwith chronic myelogenous leukemia (CML) who developedsubcutaneous SS, an association which has not been previ-ously reported.
Case report
The patient is a 43-year-old black female from Bermuda witha history of CML admitted for anemia, thrombocytopenia,fever, fatigue, splenomegaly and abdominal pain, and severeright leg pain. She was diagnosed with CML that was con-firmed by the expression of BCR-ABL by FISH, in January2009. She failed therapy with multiple tyrosine kinase inhib-itors including ponatinib. At the time of hospital admission,her hemoglobin was 4 g/dl, platelet count was 5,000/ul, andthe white blood cell count was 2,500/ul with 9 % circulatingblasts. She received two units of packed red blood cells andtwo units of platelets. Plain films and MRI of the right hip
C. WangDepartment of Pathology & Laboratory Medicine, TempleUniversity Hospital, Philadelphia, PA 19140, USA
M. E. MartinDepartment of Medical Oncology, Fox Chase Cancer Center,Philadelphia, PA 19111, USA
R. E. Smith :D. DaCosta : I. E. PalazzoDepartment of Pathology, Jeanes Hospital, Philadelphia, PA 19111,USA
R. Levaka VeeraDepartment of Hematology/Oncology, Temple University Hospital/Fox Chase Cancer Center, Philadelphia, PA 19111, USA
C. Wang (*)Department of Pathology and Laboratory Medicine, TempleUniversity School of Medicine, 3401 North Broad Street,Philadelphia, PA 19140, USAe-mail: [email protected]
J HematopatholDOI 10.1007/s12308-014-0206-3
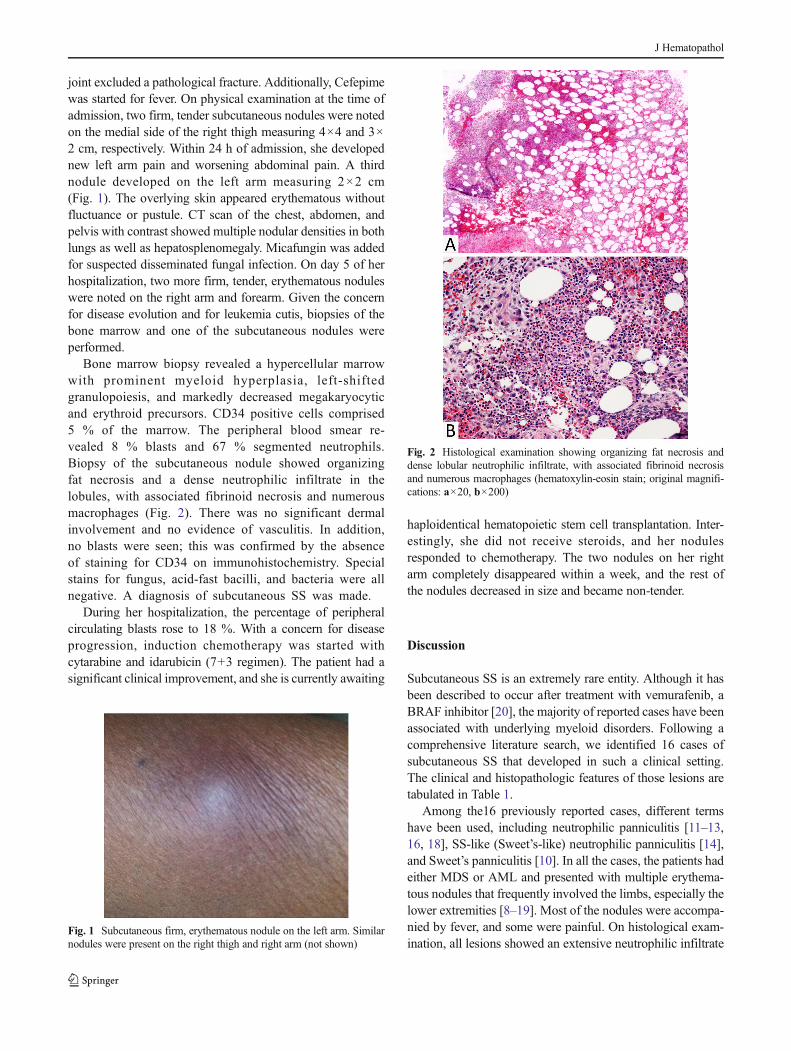
joint excluded a pathological fracture. Additionally, Cefepimewas started for fever. On physical examination at the time ofadmission, two firm, tender subcutaneous nodules were notedon the medial side of the right thigh measuring 4×4 and 3×2 cm, respectively. Within 24 h of admission, she developednew left arm pain and worsening abdominal pain. A thirdnodule developed on the left arm measuring 2×2 cm(Fig. 1). The overlying skin appeared erythematous withoutfluctuance or pustule. CT scan of the chest, abdomen, andpelvis with contrast showed multiple nodular densities in bothlungs as well as hepatosplenomegaly. Micafungin was addedfor suspected disseminated fungal infection. On day 5 of herhospitalization, two more firm, tender, erythematous noduleswere noted on the right arm and forearm. Given the concernfor disease evolution and for leukemia cutis, biopsies of thebone marrow and one of the subcutaneous nodules wereperformed.
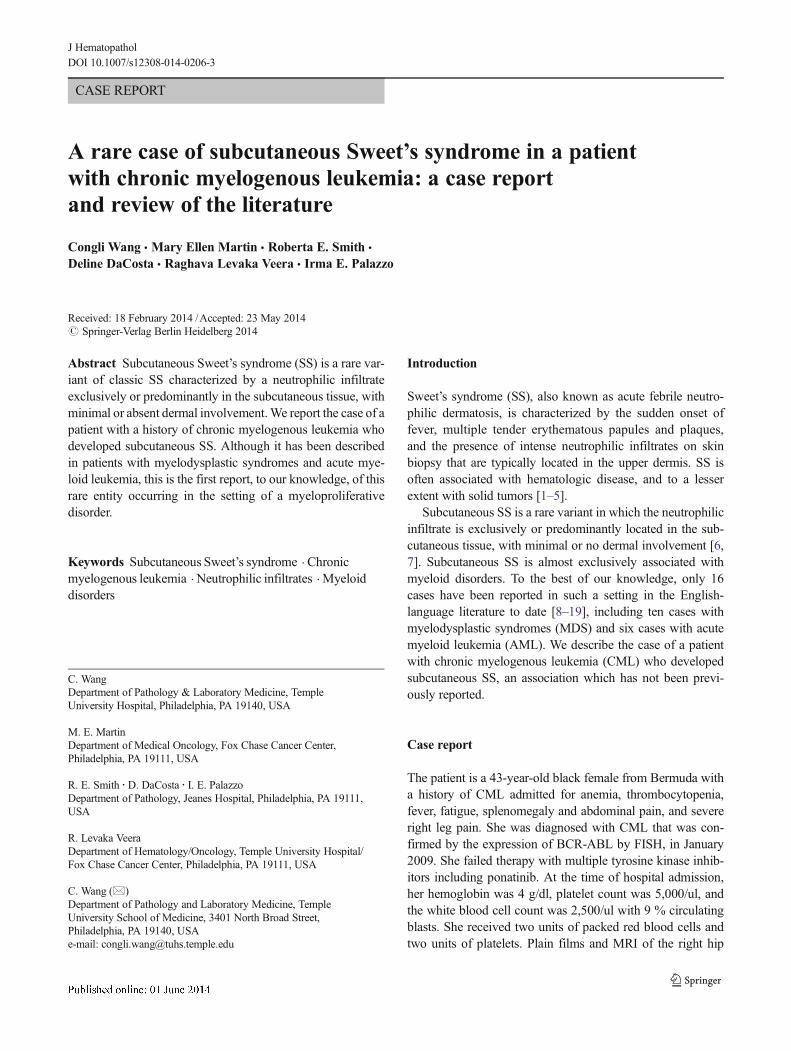
Bone marrow biopsy revealed a hypercellular marrowwith prominent myeloid hyperplasia, left-shiftedgranulopoiesis, and markedly decreased megakaryocyticand erythroid precursors. CD34 positive cells comprised5 % of the marrow. The peripheral blood smear re-vealed 8 % blasts and 67 % segmented neutrophils.Biopsy of the subcutaneous nodule showed organizingfat necrosis and a dense neutrophilic infiltrate in thelobules, with associated fibrinoid necrosis and numerousmacrophages (Fig. 2). There was no significant dermalinvolvement and no evidence of vasculitis. In addition,no blasts were seen; this was confirmed by the absenceof staining for CD34 on immunohistochemistry. Specialstains for fungus, acid-fast bacilli, and bacteria were allnegative. A diagnosis of subcutaneous SS was made.
During her hospitalization, the percentage of peripheralcirculating blasts rose to 18 %. With a concern for diseaseprogression, induction chemotherapy was started withcytarabine and idarubicin (7+3 regimen). The patient had asignificant clinical improvement, and she is currently awaiting
haploidentical hematopoietic stem cell transplantation. Inter-estingly, she did not receive steroids, and her nodulesresponded to chemotherapy. The two nodules on her rightarm completely disappeared within a week, and the rest ofthe nodules decreased in size and became non-tender.
Discussion
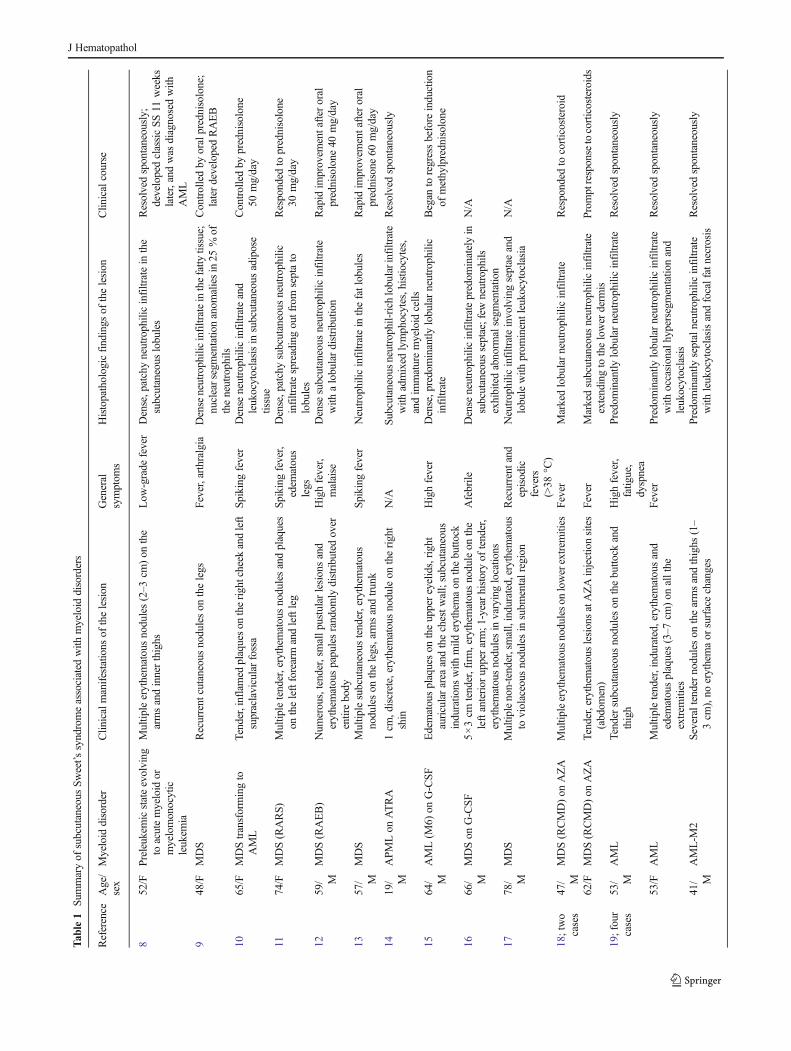
Subcutaneous SS is an extremely rare entity. Although it hasbeen described to occur after treatment with vemurafenib, aBRAF inhibitor [20], the majority of reported cases have beenassociated with underlying myeloid disorders. Following acomprehensive literature search, we identified 16 cases ofsubcutaneous SS that developed in such a clinical setting.The clinical and histopathologic features of those lesions aretabulated in Table 1.
Among the16 previously reported cases, different termshave been used, including neutrophilic panniculitis [11–13,16, 18], SS-like (Sweet’s-like) neutrophilic panniculitis [14],and Sweet’s panniculitis [10]. In all the cases, the patients hadeither MDS or AML and presented with multiple erythema-tous nodules that frequently involved the limbs, especially thelower extremities [8–19]. Most of the nodules were accompa-nied by fever, and some were painful. On histological exam-ination, all lesions showed an extensive neutrophilic infiltrate
Fig. 1 Subcutaneous firm, erythematous nodule on the left arm. Similarnodules were present on the right thigh and right arm (not shown)
Fig. 2 Histological examination showing organizing fat necrosis anddense lobular neutrophilic infiltrate, with associated fibrinoid necrosisand numerous macrophages (hematoxylin-eosin stain; original magnifi-cations: a×20, b×200)
J Hematopathol
Tab
le1
Summaryof
subcutaneous
Sweet’s
syndromeassociated
with
myeloid
disorders
Reference
Age/
sex
Myeloid
disorder
Clin
icalmanifestatio
nsof
thelesion
General
symptom
sHistopathologicfindings
ofthelesion
Clin
icalcourse
852/F
Preleukemicstateevolving
toacutemyeloid
ormyelomonocytic
leukem
ia
Multip
leerythematousnodules(2–3
cm)on
the
armsandinnerthighs
Low
-grade
fever
Dense,patchyneutrophilicinfiltratein
the
subcutaneous
lobules
Resolvedspontaneously;
developedclassicSS11
weeks
later,andwas
diagnosedwith
AML
948/F
MDS
Recurrent
cutaneousnoduleson
thelegs
Fever,arthralgia
Dense
neutrophilicinfiltrateinthefatty
tissue;
nuclearsegmentatio
nanom
aliesin25
%of
theneutrophils
Controlledby
oralprednisolone;
laterdevelopedRAEB
1065/F
MDStransformingto
AML
Tender,inflamed
plaqueson
therightcheek
andleft
supraclavicularfossa
Spikingfever
Dense
neutrophilicinfiltrateand
leukocytoclasisin
subcutaneous
adipose
tissue
Controlledby
prednisolone
50mg/day
1174/F
MDS(RARS)
Multip
letender,erythem
atousnodulesandplaques
ontheleftforearm
andleftleg
Spiking
fever,
edem
atous
legs
Dense,patchysubcutaneous
neutrophilic
infiltratespreadingoutfrom
septato
lobules
Responded
toprednisolone
30mg/day
1259/ M
MDS(RAEB)
Num
erous,tender,smallp
ustularlesionsand
erythematouspapulesrandom
lydistributedover
entirebody
Highfever,
malaise
Dense
subcutaneous
neutrophilicinfiltrate
with
alobulardistributio
nRapid
improvem
entafter
oral
prednisolone
40mg/day
1357/ M
MDS
Multip
lesubcutaneous
tender,erythem
atous
noduleson
thelegs,arm
sandtrunk
Spikingfever
Neutrophilic
infiltratein
thefatlobules
Rapid
improvem
entafter
oral
prednisone
60mg/day
1419/ M
APM
Lon
ATRA
1cm
,discrete,erythematousnoduleon
theright
shin
N/A
Subcutaneousneutrophil-rich
lobularinfiltrate
with
admixed
lymphocytes,histio
cytes,
andim
maturemyeloid
cells
Resolvedspontaneously
1564/ M
AML(M
6)on
G-CSF
Edematousplaqueson
theuppereyelids,right
auriculararea
andthechestw
all;subcutaneous
induratio
nswith
mild
erythemaon
thebutto
ck
Highfever
Dense,predominantly
lobularneutrophilic
infiltrate
Began
toregressbefore
induction
ofmethylprednisolone
1666/ M
MDSon
G-CSF
5×3cm
tender,firm,erythem
atousnoduleon
the
leftanterior
upperarm;1
-yearhistoryof
tender,
erythematousnodulesin
varyinglocatio
ns
Afebrile
Dense
neutrophilicinfiltratepredom
inatelyin
subcutaneous
septae;few
neutrophils
exhibitedabnorm
alsegm
entatio
n
N/A
1778/ M
MDS
Multip
lenon-tender,small,indurated,erythematous
toviolaceous
nodulesin
subm
entalregion
Recurrent
and
episodic
fevers
(>38
°C)
Neutrophilic
infiltrateinvolvingseptae
and
lobulewith
prom
inentleukocytoclasia
N/A
18;two
cases
47/ M
MDS(RCMD)on
AZA
Multip
leerythematousnoduleson
lowerextrem
ities
Fever
Markedlobularneutrophilicinfiltrate
Responded
tocorticosteroid
62/F
MDS(RCMD)on
AZA
Tender,erythem
atouslesionsatAZAinjectionsites
(abdom
en)
Fever
Markedsubcutaneous
neutrophilicinfiltrate
extendingto
thelower
derm
isProm
ptresponsetocorticosteroids
19;four
cases
53/ M
AML
Tender
subcutaneous
noduleson
thebutto
ckand
thigh
Highfever,
fatig
ue,
dyspnea
Predom
inantly
lobularneutrophilicinfiltrate
Resolvedspontaneously
53/F
AML
Multip
letender,indurated,erythem
atousand
edem
atousplaques(3–7
cm)on
allthe
extrem
ities
Fever
Predominantly
lobularneutrophilicinfiltrate
with
occasionalhypersegmentatio
nand
leukocytoclasis
Resolvedspontaneously
41/ M
AML-M
2Severaltendernoduleson
thearmsandthighs
(1–
3cm
),no
erythemaor
surfacechanges
Predom
inantly
septalneutrophilicinfiltrate
with
leukocytoclasisandfocalfatnecrosis
Resolvedspontaneously
J Hematopathol
that was exclusively or predominantly located in the subcuta-neous tissue. Although most of the cases described showed alobular distribution [8, 12–15, 18, 19], the infiltrate may alsodominate the septa [16, 19], or both [11, 17]. By definition, tobe called subcutaneous SS, there should be no associatedvasculitis or other cause of panniculitis. Clinically, the lesionmay resolve spontaneously or be successfully treated withcorticosteroids. It may also respond to chemotherapy, as inour patient. Since the cases shared similar clinical and patho-logical manifestations and all occurred in patients with mye-loid disorders, they should all be classified as subcutaneousSS [6, 19].
The etiology of subcutaneous SS is still unknown. It hasbeen postulated that uncontrolled release of pro-inflammatorymediators may contribute to the development of subcutaneousSS [11]. Indeed, increased level of granulocyte colony-stimulating factor (G-CSF) and all-trans retinoic acid(ATRA) chemotherapy have been linked to the disease[14–16]. G-CSF induces neutrophil mobilization by increas-ing the production of macrophage inflammatory protein 2(MIP-2) in the bone marrow [21]; and ATRA has been shownto induce gene expressions of a number of CXC and CCchemokines in acute promyelocytic leukemia cells [22].
Interestingly, subcutaneous SS may occur prior to the acutetransformation of the underlying myeloid disorders. Cooperet al. reported a patient with MDS and subcutaneous SS whodeveloped AML 11 weeks after the skin lesion appeared [8].Cullity et al. described a case of “Sweet’s panniculitis” occur-ring on a patient with MDS transforming to AML [10]. Thepresent case demonstrated a clear association between thecourse of the skin lesion and the underlying CML, in whichthe nodules occurred prior to the patient entering a presumedaccelerated phase and regressed after starting chemotherapy. Ithas been shown that high expression of CXC chemokineligand 4 (CXCR4) and activation of the CXCR4-CXCL12axis can promote leukemogenesis and the progression ofAML [23]. On the other hand, increased cytokines/chemokines will lead to the activation or recruitment ofmacrophages/neutrophils which may play a role in the patho-genesis of subcutaneous SS.
A diagnosis of subcutaneous SS should be made only afterruling out other possible conditions [24]. Leukemia cutis is animportant differential, as both entities may occur in a similarclinical setting. Microscopically, leukemia cutis typicallyshows a perivascular and/or periadnexal leukemic infiltrateor a dense interstitial/nodular infiltrate involving the dermisand subcutis. Immunohistochemistry, in most cases, is veryhelpful in confirming a diagnosis of leukemia cutis [25].Erythema nodosum (EN) may be indistinguishable from sub-cutaneous SS, both clinically and histologically. EN is themost common form of panniculitis. EN is a hypersensitivityreaction with a spectrum of histologic features that is related tothe morphologic chronology of the disease [26]. TheT
able1
(contin
ued)
Reference
Age/
sex
Myeloid
disorder
Clin
icalmanifestatio
nsof
thelesion
General
symptom
sHistopathologicfindings
ofthelesion
Clin
icalcourse
Fever,diffuse
swellin
gof
the
extrem
ities
62/F
MDS
Violaceousplaqueson
thelegs
N/A
Dense
neutrophilicinfiltratewith
inthe
superficialsubcutis,som
eneutrophils
appeared
hyposegm
ented
Resolvedafteroralprednisone
Present
case
43/F
CML
Five
subcutaneous
firm
,tender,erythematous
noduleson
medialright
thighandarms(upto
4cm
)
Fever,fatig
ue,
pain
inabdomen
and
extrem
ities
organizing
fatn
ecrosisanddenselobular
neutrophilicinfiltrateassociated
with
fibrinoidnecrosisandnumerous
macrophages
Responded
tochem
otherapy
with
idarubicin
andcytarabine
AMLacutemyeloid
leukem
ia,A
PMLacuteprom
yelocytic
leukem
ia,A
TRAall-trans-retin
oicacid,A
ZAazacitidine,C
MLchronicmyelogenous
leukem
ia,G
-CSF
granulocytecolony-stim
ulatingfactor,
MDSmyelodysplasticsyndrome,N/A
notavailable,RAEBrefractory
anem
iawith
excessblasts,R
ARSrefractory
anem
iawith
ringed
sideroblasts,R
CMDrefractory
cytopeniawith
multilineage
dysplasia,
SSSweet’s
syndrome
J Hematopathol

prototypical lesions present as a septal panniculitis with amixed cellular infiltrate comprising lymphocytes, neutrophils,histiocytes, giant cells, and variable eosinophils. Occasionally,EN may demonstrate a predominant neutrophilic component[27]. The presence of Miescher radial granulomas is thoughtto be relatively specific for EN [7, 19]. However, it has alsobeen reported in SS, Behcet’s disease, and necrobiosislipoidica [28]. Additionally, several other conditions that canlead to subcutaneous neutrophilic inflammation should beexcluded, including infection, pancreatic panniculitis, alpha-1 antitrypsin deficiency, rheumatoid arthritis, with inflamma-tory bowel disease, and local reaction secondary to injection[6, 19, 24].
In conclusion, we report the first case of subcutaneous SSoccurring in the setting of CML. Subcutaneous SS is a rareentity associated with MDS, AML, and CML. In our opinion,it is important to recognize and differentiate subcutaneous SSfrom other diseases and conditions, as subcutaneous SS maybe a warning sign of progression of the underlying myeloiddisorder.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Callen JP (2002) Neutrophilic dermatoses. Dermatol Clin 20:409–419
2. Clemmensen OJ, Menné T, Brandrup F, Thomsen K, LangeWantzinG (1989) Acute febrile neutrophilic dermatosis—a marker of malig-nancy. Acta Derm Venereol 69:52–58
3. Buck T, Gonzalez LM, Lambert WC, Schwartz RA (2008) Sweet’ssyndrome with hematologic disorders: a review and reappraisal. Int JDermatol 47:775–782
4. Cohen PR, Holder WR, Tucker SB, Kono S, Kurzrock R (1993)Sweet’s syndrome in patients with solid tumors. Cancer 72:2723–2731
5. von den Dreisch P (1994) Sweet’s syndrome (acute febrile neutro-philic dermatosis). J Am Acad Dermatol 31:535–556
6. Cohen PR (2005) Subcutaneous Sweet’s syndrome: a variant of acutefebrile neutrophilic dermatosis that is included in the histopathologicdifferential diagnosis of neutrophilic panniculitis. J Am AcadDermatol 52(5):927–928
7. Guhl G, García-Díez A (2008) Subcutaneous sweet syndrome.Dermatol Clin 26(4):541–551
8. Cooper PH, Frierson HF, Greer KE (1983) Subcutaneous neutrophil-ic infiltrates in acute febrile neutrophilic dermatosis. Arch Dermatol119:610–611
9. Morioka M, Otsuka F, Nogita T, Igisu K, Urabe A, Ishibashi Y(1990) Neutrophilic dermatosis with myelodysplastic syndrome:
nuclear segmentation anomalies of neutrophils in the skin lesionand in peripheral blood. J Am Acad Dermatol 23:247–249
10. Cullity J, Maguire B, Gebauer K (1991) Sweet’s panniculitis.Australas J Dermatol 32:61–64
11. Matsumura Y, Tanabe H, Wada Y, Ohta K, Okamoto H, Imamura S(1997) Neutrophilic panniculitis associated with myelodysplasticsyndromes. Br J Dermatol 136:142–144
12. Chen HC, Kao WY, Chang DM, Gao HW, Lai WY, Lai JH (2004)Neutrophilic panniculitis with myelodysplastic syndromes presentingas pustulosis: case report and review of the literature. Am J Hematol76:61–65
13. Sutra-Loubet C, Carlotti A, Guillemette J, Wallach D (2004)Neutrophilic panniculitis. J Am Acad Dermatol 50:280–285
14. Jagdeo J, Campbell R, Long T, Muglia J, Telang G, Robinson-Bostom L (2007) Sweet’s syndrome-like neutrophilic lobularpanniculitis associated with all-trans-retinoic acid chemotherapy ina patient with acute promyelocytic leukemia. J Am Acad Dermatol56:690–693
15. Uhara H, Saida T, NakazawaH, Ito T (2008) Neutrophilic dermatoseswith acute myeloid leukemia associated with an increase of serumcolony-stimulating factor. J Am Acad Dermatol 59(Suppl):S10–S12
16. Becherer K, Golda N, Feldman M, Diaz-Arias A, Caldwell C (2009)Neutrophilic panniculitis associated with myelodysplastic syndromewith abnormal nuclear forms. J Cutan Pathol 36:1024–1026
17. HoodM, YuK,Magro C, ReisacherW (2010) Pathology quiz case 2:subcutaneous sweet syndrome of the neck. Arch Otolaryngol HeadNeck Surg 136(1038):1040–1041
18. Kim IH, Youn JH, Shin SH, Yahng SA, Lee SE, Kwon JC, Lee DG,Park KS, Choi MH, Jung SE, Kim YJ (2012) Neutrophilicpanniculitis following azacitidine treatment for myelodysplastic syn-dromes. Leuk Res 36:e146–e148
19. Chan MP, Duncan LM, Nazarian RM (2013) Subcutaneous sweetsyndrome in the setting of myeloid disorders: a case series and reviewof the literature. J Am Acad Dermatol 68(6):1006–1015
20. Kim GH, Levy A, Compoginis G (2013) Neutrophilic panniculitisdeveloping after treatment ofmetastatic melanomawith vemurafenib.J Cutan Pathol 40(7):667–669
21. Nguyen-Jackson HT, Li HS, Zhang H, Ohashi E, Watowich SS(2012) G-CSF-activated STAT3 enhances production of the chemo-kine MIP-2 in bone marrow neutrophils. J Leukoc Biol 92(6):1215–1225
22. Shibakura M, Niiya K, Niiya M, Asaumi N, Yoshida C, Nakata Y,Tanimoto M (2005) G-CSF-activated STAT3 enhances production ofthe chemokine MIP-2 in bone marrow neutrophils. Leuk Res 29(7):755–759
23. Ayala F, Dewar R, Kieran M, Kalluri R (2009) Contribution of bonemicroenvironment to leukemogenesis and leukemia progression.Leukemia 23:2233–2241
24. Gerami P, Guitart J (2007) Panniculitis with histiocytoid/immatureneutrophils is not limited to histiocytoid panniculitic Sweet syn-drome. Am J Clin Pathol 29(6):596
25. Cho-Vega JH, Medeiros LJ, Prieto VG, Vega F (2008) Leukemiacutis. Am J Clin Pathol 129(1):130–142
26. White WL, Hitchcock MG (1999) Diagnosis: erythema nodosum ornot? Semin Cutan Med Surg 18:47–55
27. Thurber S, Kohler S (2006) Histopathologic spectrum of erythemanodosum. J Cutan Pathol 33:18–26
28. WhiteWL,Wieselthier JS, HitchcockMG (1996) Panniculitis: recentdevelopments and observations. Semin Cutan Med Surg 15:278–299
J Hematopathol











![[Ghiduri][Cancer]Chronic Myelogenous Leukemia](https://img.pdfslide.net/doc/110x75/577cc6ea1a28aba7119f80de/ghiduricancerchronic-myelogenous-leukemia.jpg)

















