Embed Size (px)
Citation preview
A Review of the Literature: Managing Cervical Spine Injuries
MaryBeth Horodyski, EdD, LAT, ATC, FNATA Professor and Director of Research
Department of Orthopaedics and Rehabilitation

Funding Sources for Research
• Laerdal Foundation
• NOCSAE
• NCAA
• Southwestern Medical Foundation
• Stryker

Objectives
• Current Research and Best Practices
– Positioning on Spine Board
• Supine
• Prone
– Helmet & Equipment Removal
– Stabilization for Transport
• Cervical Collars
• Strapping Techniques
• Future Directions

What Happens After the Timeout?
• You are now Prepared to Act
– Appropriate equipment for spine boarding procedures has been assembled
• You met with Paramedics and all Medical Team personnel
• But are you using the best/safest practices? • Position on Spine board
• Equipment Removal
• Secure to Spine board

No one ever wants to be in this situation but….. will you know what is best to do when you are?

Why Immobilize?
• Case reports of exacerbation of injuries from standard actions or procedures
– Harrop et al. 2001
– Powell et al. 1995
• Amount of motion and forces required to create secondary neurologic injury unknown

Epidemiology
• Annual immobilization numbers in the US – Between 1 and 5 million patients
• (Stiell et al., 2001, Orledge and Pepe, 1998)
• Estimates for the US range from 10-12,000 new SCI annually (NSCISC, 2012)
– 7.6% caused by traumatic sports-related events • Majority due to diving and swimming (Ghiselli, et al., 2003)
• ~ 7% of patients have unstable spinal fractures but not complete SCI (Haut et al., 2010)

8
Research Team Goal: Investigate and develop techniques to
Prevent neurologic deterioration during initial stages of prehospital care, during transport, in the ED,
and in the OR when preparing for surgery.

Research Methods
• An electromagnetic tracking device (Liberty - Polhemus Inc., Colchester, VT) – To quantify the amount of
segmental motion generated
• Receivers of the tracking device were fastened onto the forehead and sternum

Methods: Variables Measured
• Dependent variables: • Angular motion (o)
– Flexion/extension
– Right and left lateral flexion
– Right and left rotation
• Linear displacement (mm) – Anteroposterior displacement
– Medial/lateral displacement
– Distraction/compression
• Independent variables: • Technique
• Injury condition

1
1
Traditional Hand Hold

1
2
Modified Hand Hold
Modified Hand Hold

1
3
Hand Placement
* #
Axial rotation and lateral bending: Significant differences between techniques (p<0.001) - both LR techniques had more motion
Supine Patient • Options
– Log roll (traditional)
– Lift-and-slide (straddle lift or 8 person lift)
– Mechanical device (Scoop stretcher, motorized spine board)
• Influencing factors – Patient size
– Personnel • Number
• Relative strength
• Preparedness (practice)

Supine Patient - Spine Board Transfer Techniques
• Log roll vs lift-and-slide (Del Rossi et al., JAT, 2003)
• Training study – 48 healthy subjects (8 teams)

Supine Patient - Spine Board Transfer Techniques
• Log roll vs lift-and-slide (Del Rossi et al., JAT, 2003)
Flexion- Extension
Axial rotation
Lateral flexion

Supine Patient - Spine Board Transfer Techniques
• Cadaveric study
• Log roll vs lift-and-slide vs 8 person lift (Del Rossi et al., JAT, 2008)

Supine Patient - Spine Board Transfer Techniques
• Log roll vs lift-and-slide vs 8 person lift • (Del Rossi et al., JAT, 2008)

Supine Patient - Spine Board Transfer Techniques
• Mechanical Transfer Devices • Log roll vs scoop stretcher (SS)
• (Krell et al., Prehosp Emerg Care, 2006)
• 31 healthy subjects
• Electromagnetic sensors • Forehead, C3 (surface), T12 (surface)
• Results • 6-8 degrees greater motion in all three planes during LR
compared to SS
LRLS
SCOOP
0
1
2
3
4
5
6
7
An
gu
lar
Mo
tio
n (
deg
rees)
Technique
Flexion - Extension
Axial Rotation
Lateral Flexion
LRLS
SCOOP
0
0.1
0.2
0.3
0.4
0.5
0.6
Lin
ear
Tra
nsla
tio
n (
cm
)
Technique
Medial - Lateral Translation
Distraction - Compression
Anterior - Posterior Displacement
*
*
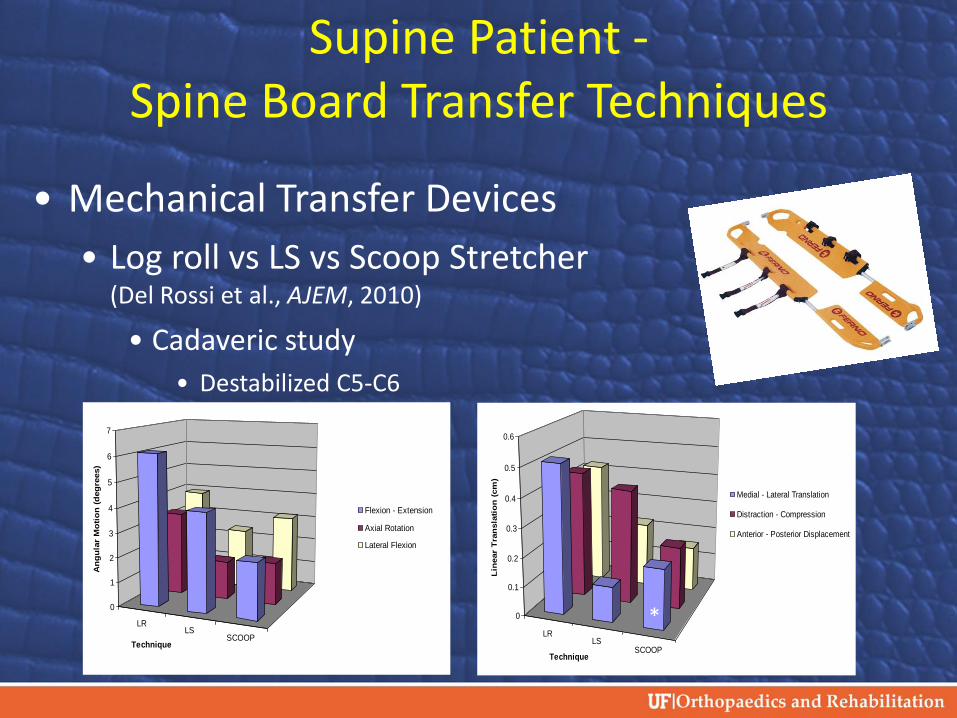
Supine Patient - Spine Board Transfer Techniques
• Mechanical Transfer Devices
• Log roll vs LS vs Scoop Stretcher (Del Rossi et al., AJEM, 2010)
• Cadaveric study
• Destabilized C5-C6
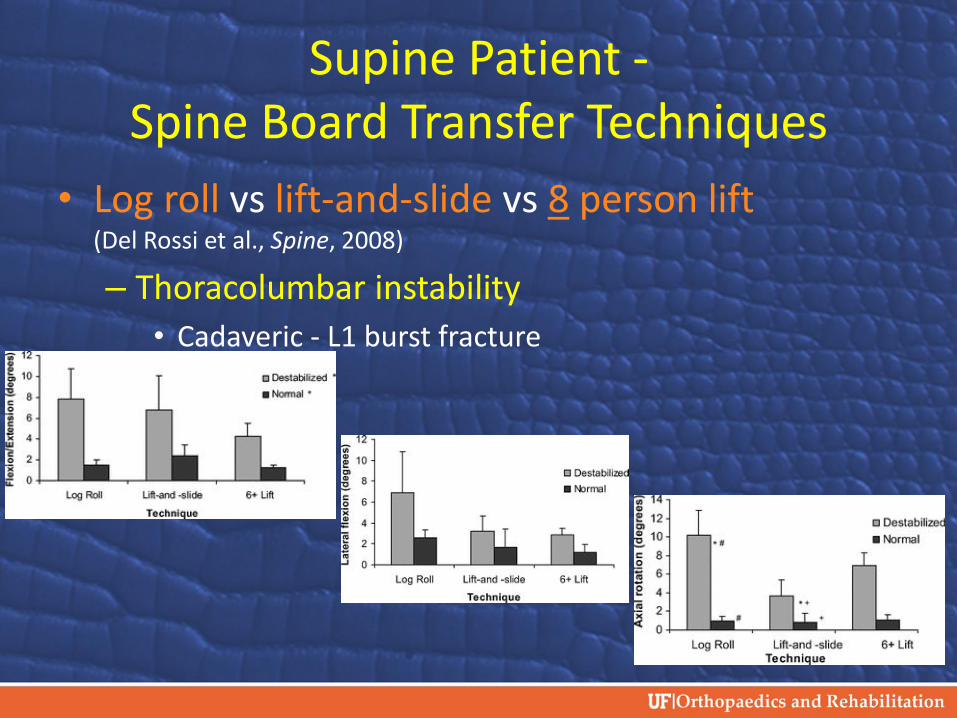
Supine Patient - Spine Board Transfer Techniques
• Log roll vs lift-and-slide vs 8 person lift (Del Rossi et al., Spine, 2008)
– Thoracolumbar instability
• Cadaveric - L1 burst fracture

Eliminating the Log Roll • When using log roll techniques for transfers
– Sum of the largest displacements during the total sequence • 2 times for flexion/extension • 2.6 times for axial rotation • 2.8 times for lateral bending
– Prasarn et al. 2012 Spine Journal
• No log roll • Sum of the greatest displacements for the complete
sequence was significantly decreased • Prasarn et al. 2012 Journal of Neurosurgery
• Overall cumulative motion to the unstable spine can be reduced by approximately 50% if the log roll is avoided and alternative measures are employed
• Conrad et al. 2012
Supine – Obese/Large Patient Spine Board Transfer Techniques
• Personnel or strength concerns
– 2001 NATA Consensus Statement suggested adding more personnel to 6+ person lift = 8+
– Log roll might be only other option
• Equipment concerns
– Scoop stretchers might be too narrow or too short to accommodate large patients.
Supine Patient – Equipment-laden Spine Board Transfer Techniques
• NATA Consensus Statement
– LS or 8 person lift with equipment on
– Rolling over equipment may induce motion (2001)
• Equipment fit
– Youth helmets may not fit securely as would be needed to be able to safely transfer patient
– May need to consider removing helmet before transferring patient

Supine Patient - Summary
• LS and 8 (6+) person lift generate less motion than LR
• Scoop stretcher • As safe as LS
• Consider LS, 8 person and scoop stretcher as alternative to LR (supine patient)
• 8 person and scoop stretcher are possible alternatives for equipment-laden athletes
• 8+ for large patients

Prone Patient
• Options – Log roll (pull) vs. log roll (push)
– Log roll (1x) vs. log roll (2x)
• Influencing factors – History (convention)
– Personnel • Availability of spine board
• Preparedness (practice)

Prone Patient – Spine Board Transfer Techniques
• Push vs Pull Cadaveric study • Thoracolumbar instability
– Conrad et al., J Spinal Cord Med, 2012

Prone Patient – Spine Board Transfer Techniques
• Significantly less motion with the Push technique • Flexion/Extension; Axial Translation; Ant/Post Translation

Prone Patient – Spine Board Transfer Techniques
• Prone to supine (Prasarn et al., in preparation)
– Options • LR to supine + LR onto spine board
• LR to supine + LS or 8 person or scoop stretcher
• LR directly to spine board
– Cadaveric study • C5-C6 instability
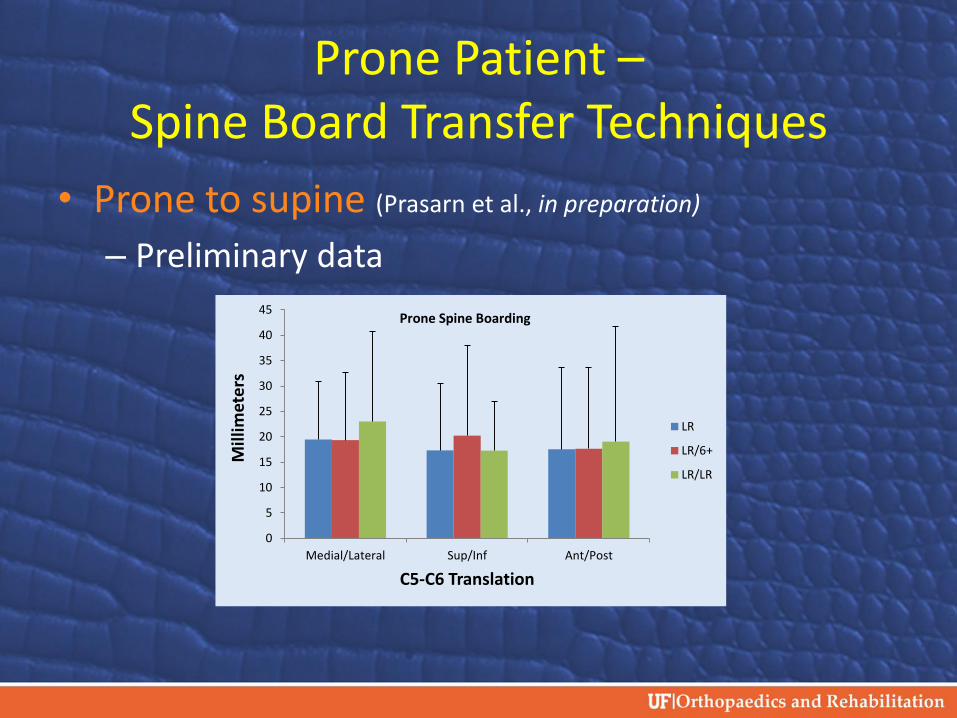
Prone Patient – Spine Board Transfer Techniques
• Prone to supine (Prasarn et al., in preparation)
– Preliminary data
0
5
10
15
20
25
30
35
40
45
Medial/Lateral Sup/Inf Ant/Post
Mill
imet
ers
C5-C6 Translation
LR
LR/6+
LR/LR
Prone Spine Boarding

Prone Patient – Equipment-laden
• Equipment fit – Hockey
• Mihalik et al. 2011
• Might this be a good time to initiate removal of equipment?
Prone Patient – Summary
• LR – only option; but how many times should you move the patient?
• Decide in advance how the situation should be handled based on circumstances.
• With every transfer there is the potential or opportunity for motion to occur.

•Spinal immobilization
• Spine board is current gold-standard for prehospital spinal immobilization
• Full body immobilization on a vacuum mattress also possible
• Pro and cons
Vacuum Mattress

Vacuum Mattresses • Spinal immobilization
• Vacuum mattress vs spine board • Johnson et al., AJEM, 1995
• 30 subjects
• Immobilization during lateral tilting (90o)

Equipment Issues in the Cervical Spine Injured Athlete
• Injured player’s helmet and shoulder pads pose challenges to the medical team’s ability to
– Properly assess the cervical spine region
– Immobilize the cervical spine
Facemask Removal
• Cordless screwdriver was the best way to remove a football helmet
• Pruners should be carried as a backup in case the cordless screwdriver fails
• Facemask removal practice and hardware inspection reduce chances of failure – Brandey et al. JAT, 2013

Facemask Removal
• Combined tool approach • CSD and cutting tool resulted in 100% success
• Average time: 37.84 ± 15.37sec
• Copeland et al. Clin J Sport Med, 2007
• On-field conditions throughout football season • 98.6% (75/76) of removal attempts were successful
with combined tool approach • Average removal time 40.1 ± 15.1 seconds
• Gale et al. JAT, 2008

Quick Release Facemask Removal
• Removal time of quick release face guard • Riddell Quick Release Helmet • After a season of football
– Removal of facemask • Satisfactory time and success rate • Gruppen et al. JAT, 2012; Scibek et al. JAT, 2012
• Quick release – More effective than other facemask removal
techniques • Better success rate • Swartz et al. JAT, 2010

Facemask: Other Options
• Feed mask through facemask – The PMI (Pocket Mask Insertion) technique significantly
faster • 19.86 ± 5.92 seconds
– QRM 50.37 ± 13.13 seconds
– CSD 68.98 ± 15.42 seconds • Toler et al. Clin J Sport Med, 2011
• PMI time – 14-19 seconds
• Ray et al. JAT, 2002

Time vs. Motion: Translational Movement for Airway Access

Time vs. Motion: Rotational Movement for Airway Access

Helmet Removal: Techniques • Helmet bladders should be left inflated when
the helmet is removed
• It takes longer to deflate a helmet and remove a helmet
• It is not always possible to access all the bladders in a supine athlete
• Beltz et al (http://www.nhmi.net/deflate.php)

Helmet Removal: Techniques
• After the helmet is removed, padding should be placed under the head to prevent hyperextension • Del Rossi G et al., 2014
• DeCoster LC et.al., Spine, 2012
• Waninger KM et.al., Current Sports Medicine Reports, 2011
• Shoulder pads can remain on if spinal alignment can be maintained

Helmet Removal Study
• A comparison between two removal techniques
– Facemask removal then helmet removal
– Direct helmet removal
• Helmet removal techniques were measured in cadaveric model with a suspected cervical spine injury

Helmet Removal Study
• Facemask removal then helmet removal (FMH)
– Facemask was removed first with an electric screwdriver
• Right ear side, left ear side, right frontal, and then left frontal was the screw removal order
– Helmet was then removed according to NATA position statement
Helmet Removal Study
• Direct helmet removal (Helmet) – The helmet was removed using the two rescuer-two
hands approach
• For both the FMH and Helmet removal techniques, cheek pads were removed. – Spinal alignment was maintained throughout the
helmet removal
• Head was placed on padding to maintain spinal
alignment
Helmet Removal Study
0
2
4
6
8
10
Flex/Ext Axial Rot Lat Bend
Deg
rees
(•)
Means of Angular Displacement at C5-C6
FMH
Helmet
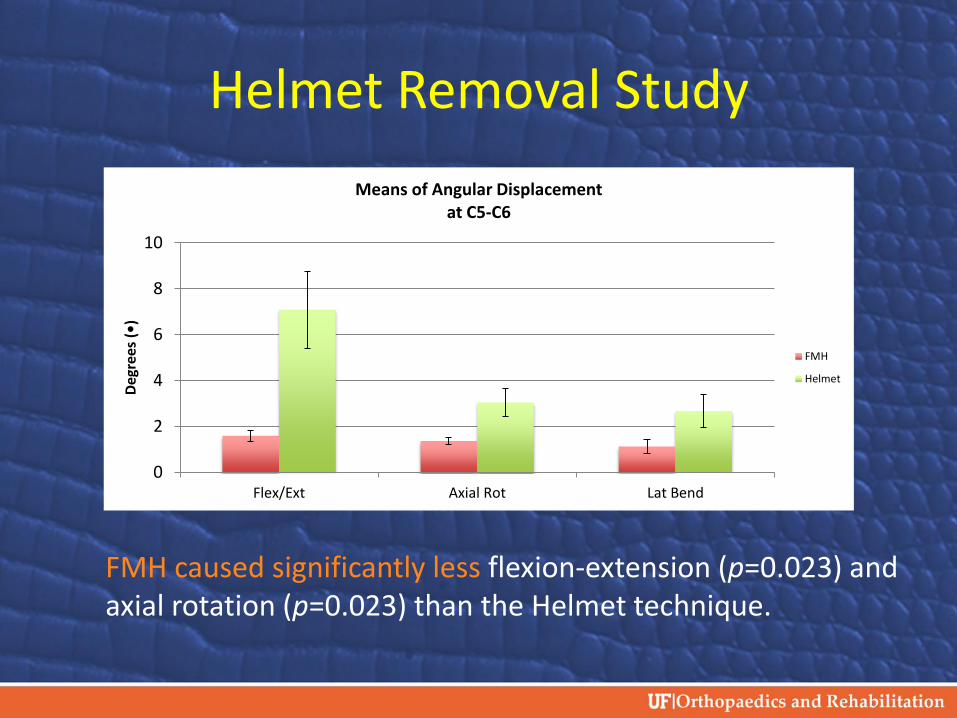
FMH caused significantly less flexion-extension (p=0.023) and axial rotation (p=0.023) than the Helmet technique.

Helmet Removal Study
0
1
2
3
4
5
6
7
8
9
Med/Lat Axial Trans Ant/Post
Mili
met
ers
(mm
)
Means of Translation Displacement at C5-C6
FMH
Helmet
FMH caused significantly less anterior-posterior (p=0.035), medial-lateral (p=0.013), and axial (p=0.028) translations than the Helmet technique.
Shoulder Pad Removal

Traditional Pad Removal

Elevated Torso Removal
Shoulder Pad Removal
• Alterations to shoulder pads allow for quick removal if necessary – Riddell RipKord
• Shoulder pads are separated
into two halves and slid from under the athlete
• Allowed less motion than flat torso removal – Kordecki M et al., J of Sports
Phys Ther, 2011

Shoulder Pad Removal
• Methods of removal • Levitation
• Tilt
• Log roll
– Levitation caused more anterior displacement, shear and moment when compared to the other two methods
• Dahl et al. J Applied Biomechanics

Equipment Removal
• Football shoulder pads can be removed using the elevated torso method
• Horodyski et al 2009
• A new shoulder pad system
has been developed – RipKord
• Kordecki 2011
• Vest and racing collar assembled with front and back pieces – Removal by elevated torso
method
54

Cervical Collar
• NATA Position Statement
– Manual stabilization of the head should be converted to restriction using a combination of external devices • Cervical collars
• Various head stabilizing devices
Effectiveness of Cervical Collars
• Application of one and two piece collar on intact and unstable spine – Significantly more movement when applying the collar to an
unstable spine
• Two piece collar had significantly more movement than the one piece – Clinical relevance? - small difference
• Collars can be placed and removed with manual in-line stabilization and (potentially) minimal risk – Prasarn et al., Trauma Acute Care Surg, 2012
Effectiveness of Cervical Collars
• Application of a cervical collar caused increased separation at the injury site C1-C2 level
• Ben-Galim et al. J Trauma, 2010
• Biomechanics of cervical restriction with collars
– Rigid collars create pivot points that shift the center of rotation lateral to the spine and contribute to the intervertebral motion
• Lador et al. J Trauma, 2011

Effectiveness of Cervical Collars
– Often cannot correctly apply cervical collars when the athlete is wearing equipment
– Time of application and impact to beginning critical life saving procedures
– “Why do we put cervical collars on conscious trauma patients?” • Benger J and Blackham J, Scand J Trauma Resuscitation Emerg
Med, 2009

Effectiveness of Cervical Collars
• Cervical collars do not effectively reduce motion in an unstable cervical spine
– Horodyski et al. J Emerg Med, 2011
– Miller CP et al. Spine, 2010
– Bearden et al. J Neurosurgery, 2007
– Del Rossi et al. The Spine Journal, 2004

6
0
Strapping Techniques
• Minimize excess movement
• Secure enough to roll spine board if athlete vomits
• Hands secured on top of the chest – Journal of Athletic
Training 2009;44(3):306–331
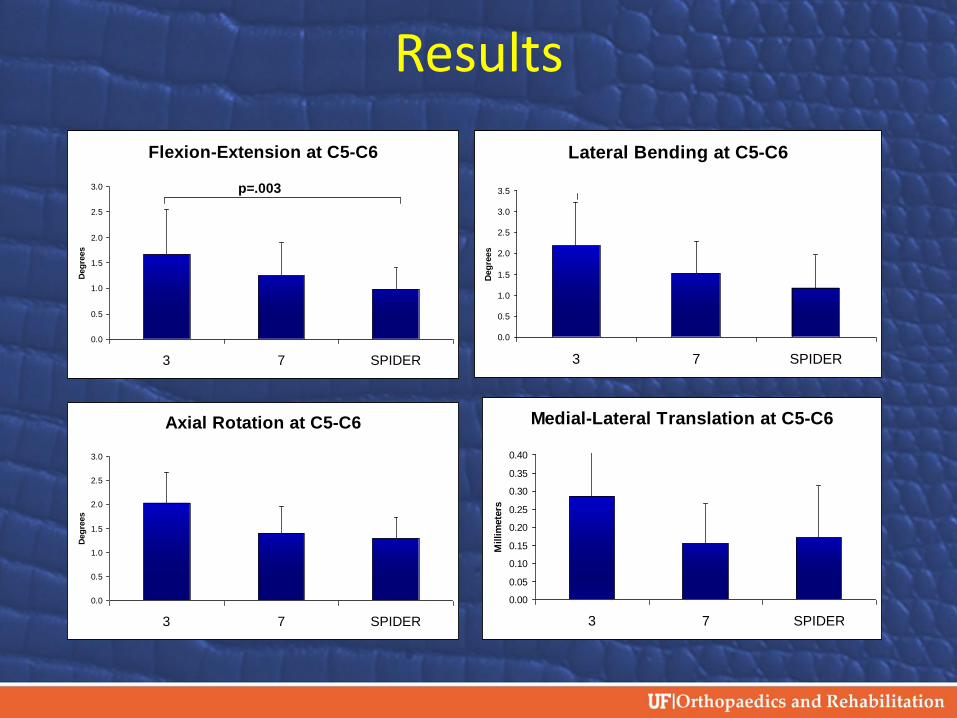
Results
Axial Rotation at C5-C6
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3 7 SPIDER
Deg
rees
Lateral Bending at C5-C6
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
3 7 SPIDER
Deg
rees
Flexion-Extension at C5-C6
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3 7 SPIDER
Deg
rees
p=.003
Medial-Lateral Translation at C5-C6
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
3 7 SPIDER
Millim
ete
rs

Conclusions: Strapping Techniques
• 3-Strap technique was significantly inferior in four of the six outcome measures – Measured difference was small
• SPIDER technique resulted in less motion than the 7-Strap – Not significantly different
• Overall, our study demonstrated that the SPIDER technique resulted in less slipping motion in the event the immobilized patient must be rolled to clear the airway
Spine Board Centering Methods
• Examine which method causes the least amount of angular and translational movement
• Techniques tested
– Horizontal Slide
– Diagonal Adjustment
– V-Adjustment Technique
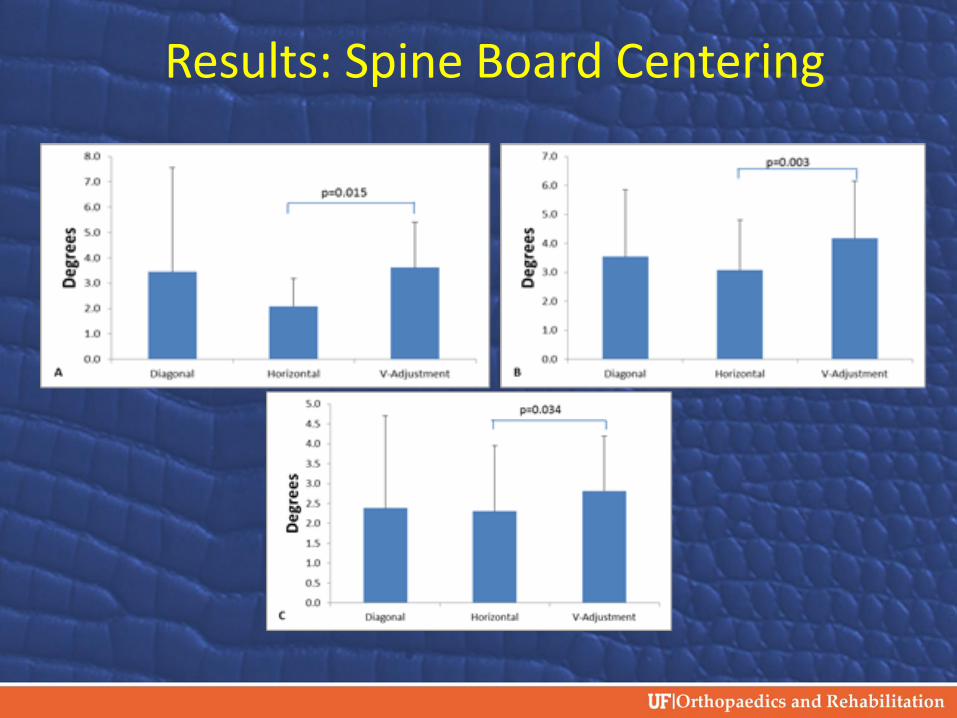
Results: Spine Board Centering

Results: Spine Board Centering
Conclusions: Spine Board Centering
• First responder should minimize movement
• Horizontal slide has less movement than diagonal and V-adjustment
• Horizontal slide easier to complete

NEW STUFF: Calculating SAC
• Our lab has developed a program that can calculate the space available for the cord during range of motion trials
– Tested cadaveric model using a intact and total instability in a cervical spine specimen
– Data was collected in mm2

Calculating SAC
Specimen and robot set-up for calculating SAC

Calculating SAC
Three dimensional representation of the cervical spine specimen.

Calculating SAC
• Spinal canal overlap of the C5-C6 vertebrae • The black and white image is the SAC in the C5-C6
segment
70

Calculating the SAC
• Levels of instability
– Intact cervical spine
– First – interspinous ligament
– Second – anterior longitudinal ligament
– Third – the entire facet joint
• Results
– No significant differences between the levels of instability
– As the level of instability increased, the SAC decreased
– Extension caused the greatest decrease in SAC
Future Research
• Further develop the software to account for changes in soft tissue inside the spinal canal – Intervertebral disc, posterior longitudinal
ligament, ligamentum flavum
• Use this program to calculate SAC during pre-hospital treatment techniques – Collar application, spine boarding, bed transfers
• Lesser chance of secondary injury
72 72

What is Next?
• Inter-association Spine Task Force
• Spinal Precautions versus Immobilization
• Spinal Motion Restriction versus Immobilization
– Restriction: cervical collar; caution patient
• Potential risks to patients on spine board

What is Next? • What MOIs require immobilization
– Blunt trauma and altered level of consciousness
– Spinal pain or tenderness
– Neurologic complaint
• Numbness or motor weakness
–Anatomic deformity of the spine
–High-energy mechanism of injury
–Any of the following • Drug or alcohol intoxication
• Inability to communicate
• Distracting injury





![Clearing the Pediatric Cervical Spine · family. Cervical spine injuries are often associated with a sig-nificant mortality (19–27 %) [6] and morbidity (e.g., up to 67 % of patients](https://img.pdfslide.net/doc/110x75/5ed3a1bf18dc2351871e448a/clearing-the-pediatric-cervical-spine-family-cervical-spine-injuries-are-often.jpg)
























