Embed Size (px)
Citation preview
J Cutan Pathol 2014doi: 10.1111/cup.12353John Wiley & Sons. Printed in Singapore
© 2014 John Wiley & Sons A/S.Published by John Wiley & Sons Ltd
Journal ofCutaneous Pathology
Review
A review of the solitary cutaneousT-cell lymphomas
Cutaneous T-cell lymphomas (CTCL) account for almost 65-92%of all cutaneous lymphomas, many of which usually present withmultiple lesions. However, a number of well-recognized and raretypes of CTCL, including mycosis fungoides, can present inisolated fashion. These solitary lesions often run a relativelyindolent clinical course but often pose diagnostic difficulties. Wereview histopathologically challenging solitary cutaneous T-celllymphomas, including criteria for diagnosis, clinical course andprognosis, particularly for primary cutaneous CD4+small/medium pleomorphic lymphoma and indolent CD8+lymphoid proliferation of acral sites. In addition, we suggest analgorithm and nomenclature to aid in the diagnosis of suchproblematic lesions.
Keywords: solitary mycosis fungoides, pagetoid reticulosis, indolentCD8+ lymphoid proliferation of acral sites, primary cutaneousCD4+ small/medium pleomorphic lymphoma
Ally MS, Robson A. A review of the solitary cutaneous T-celllymphomas.J Cutan Pathol 2014. © 2014 John Wiley & Sons A/S. Published byJohn Wiley & Sons Ltd
Mina S. Ally1 and AlistairRobson2
1Department of Dermatology, StanfordUniversity School of Medicine, Redwood City,CA, USA, and2St. John’s Institute of Dermatology,St. Thomas’ Hospital, London, UK
Alistair Robson, FRCPath Dip RCPath,St. John’s Institute of Dermatology, St. Thomas’Hospital, Westminster Bridge Road, London SE17EH, UKTel: 0207 1887188Fax: +44 207 1886382e-mail: [email protected]
Accepted for publication December 16, 2013
Primary cutaneous T-cell lymphomas presentin the skin with no evidence of extra-cutaneousinvolvement.1 Cutaneous T-cell lymphomas(CTCL) account for almost 65–92% of all cuta-neous lymphomas,2 of which, mycosis fungoides(MF) is the most common and characteristicallypresents with multiple lesions. However, solitaryMF, including and distinct from pagetoid retic-ulosis (Woringer-Kolopp), is well documented;3similarly, other well-characterized forms oflymphoma can present as an isolated lesion.Finally, a number of increasingly recognizedrarer CTCL commonly present with an isolatedlesion, including CD4+ small/medium pleomor-phic T-cell lymphoma (SMPTCL) and indolentCD8+ lymphoid proliferation of acral sites.4Although it seems that these isolated lesions
run a relatively indolent clinical course, theycontinue to pose diagnostic difficulty.
In this review, we present an overview of thesolitary cutaneous T-cell lymphomas that, inour opinion, present the greatest challenge indiagnosis and that have been emerging over thelast 5 years. We have excluded some of the moreclinically aggressive tumors that may present assolitary lesions as they tend to be well recognizedand histopathologically and immunopheno-typically distinct. We discuss the criteria fordiagnosis, particularly for primary cutaneousCD4+ small/medium pleomorphic lymphomaand indolent CD8+ lymphoid proliferationof acral sites. Finally, we suggest an algorithmto aid in the diagnosis of such problematiclesions.
1

Review
Cutaneous lymphoma classification and reviewThe recent détente and concord betweenthe World Health Organization (WHO) andEuropean Organization for the Research andTreatment of Cancer (EORTC) classificationsacknowledges the unique features of primarycutaneous lymphomas, which differ greatly fromthe nodal and other extranodal lymphomas.1,5
An accurate diagnosis of primary cutaneouslymphoma requires the correlation of the clini-cal findings with the microscopic, immunophe-notypic and genetic features. Given that themajority of lymphomas usually present with mul-tiple lesions it is difficult to make a diagnosisof a specific cutaneous lymphoma when facedwith the clinical presentation of a solitary lesion.Moreover, in the absence of multiple lesions thesurgical pathologist is frequently in difficulty indetermining whether an infiltrate is neoplasticor reactive.
To date, of the solitary cutaneous T-celllymphomas reported in the literature, approxi-mately 166 cases represent MF,3 231 representSMPTCL, 22 represent indolent CD8+ lym-phoid proliferation and 62 represent pagetoidreticulosis (Table 1).
Solitary MFMF accounts for almost 50% of all primary cuta-neous lymphomas and is characterized by mul-tiple patches and plaques.1 Indeed, given thatthe finding of multiple patches and plaquesis a defining feature it is somewhat contradic-tory to consider a solitary variant. Nevertheless,since 1981, 166 solitary cases of MF have beendescribed that are distinct from pagetoid retic-ulosis, including 10 of the folliculotropic variant(follicular MF)2,3,6–8 and 9 cases of syringotropicMF.9–12
Clinical featuresSolitary MF, clinically and histopathologicallyresembles classic MF. Clinically, it presents as a
single erythematous scaly patch or plaque, innon-sun-exposed areas.1 Solitary MF has beenreported to have an excellent prognosis,3,13,14
although recurrence of treated lesions has beenreported2,13,15–18 six of which occurred distantfrom the site of the original lesion (Table 1). Twoof these distant recurrences presented as multi-ple lesions, but in both cases, there was completeresolution with further treatment and no furtherdisease at follow-up.2 The other four cases pre-sented as a unilesional recurrence.11,17 In addi-tion, four cases of solitary MF have progressedto further cutaneous involvement, three of whichhad large cell transformation.2,8,16,19
Solitary lesions of follicular and syringotropicMF are also clinically and pathologically indis-tinguishable from lesions seen in classical dis-ease. Solitary folliculotropic MF presents as aninfiltrated patch, plaque or an isolated area offollicular papules without prominent scaling,usually in the head and neck area.2,6,8 Solitarysyringotropic MF usually presents with a singleerythematous, indurated plaque, often studdedwith small pinhead-sized papules, in the trunk,hip and thigh area,11,20 although cases havebeen reported in the head and neck area.11,12
Alopecia is a prominent feature in both cases.11
There is still uncertainty about the relation-ship between these two MF subtypes, but theyoften co-exist.6,11,20 When compared with clas-sic MF, folliculotropic MF is typically associatedwith a poorer prognosis.21 This is sometimes,8but not always the case for solitary lesions.2,6Syringotropic MF, however, has a prognosis sim-ilar to that of classic MF.22 Out of the nine soli-tary cases of syringotropic MF reported, one hasshown recurrence of the lesion distant from theoriginal site.11
Finally, the report of an EORTC workshop con-cerning granulomatous MF and granulomatousslack skin (GSS) detailed one solitary exampleof GSS.23 Recently, at the senior author’s insti-tution, a case of GSS presented with a singlependulous axillary skin fold, which was followed
Table 1. Number of reports of each solitary cutaneous T-cell lymphoma and reported instances of recurrence or disease progression
Cutaneouslymphoma type Total cases
Cases with cutaneous/systemic progression
Cases with lesion recurrencepost-treatment*
Solitary MF 166 4 (Cutaneous spread, 3 × large cell transformation) 15 (six distant from original site)Pagetoid reticulosis (Woringer-Kolopp) 62 1 (Cutaneous spread) 8 (1 distant from original site)SMPTCL 231 5 (Extracutaneous spread, one died of lymphoma) 12Indolent CD8+ lymphoid proliferation of
acral sites22 0 4 (one distant from original site)
*Recurrence occurred at the same site of the original lesions unless stated otherwise.
2
Review
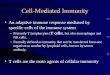
Fig. 1. A solitary plaque of granulomatous slack skin, affectingthe groin.
several years later with involvement of the groin(Fig. 1).24 A recent report by Ally et al.3 of 15cases suggested that the observation of solitaryMF might be expected, albeit exceptional, inwhich the disease is simply found at an uncom-monly early stage. The unsurprising excellentprognosis of such cases indicates that therapyshould aim to be curative.
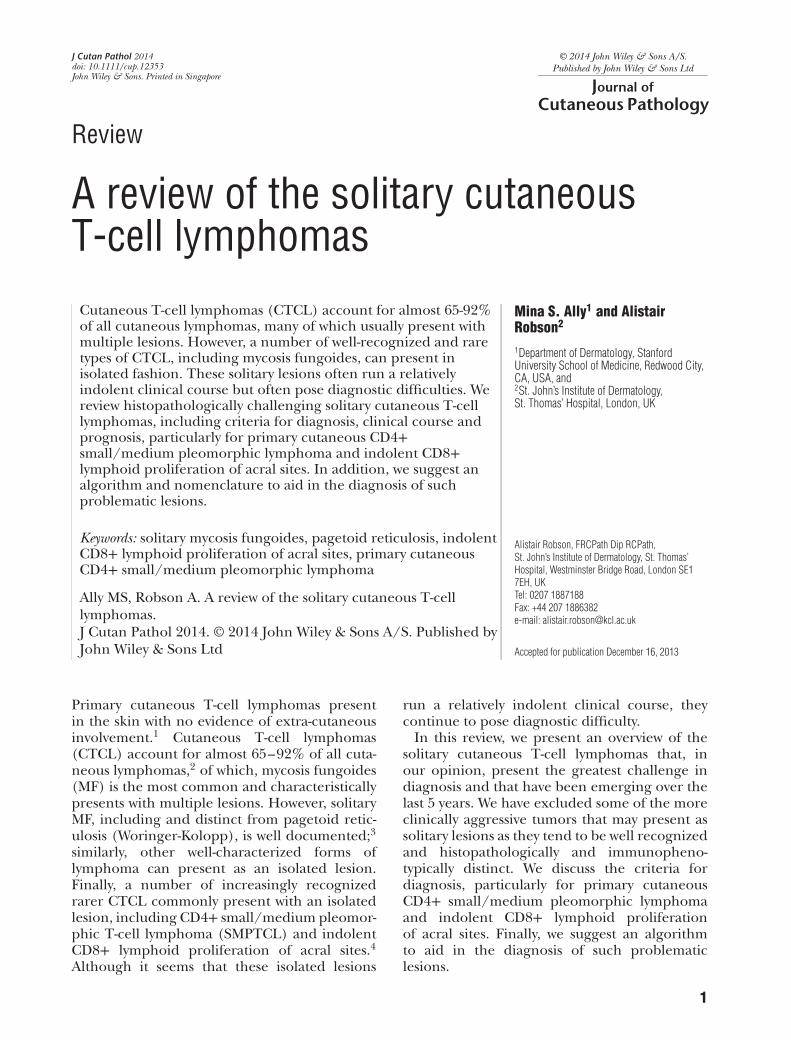
Histopathologic featuresIn solitary MF, microscopic sections show a super-ficial lymphoid infiltrate of epidermotropic andatypical lymphocytes.20,25 Atypia is usually morepronounced in the epidermotropic lymphocytesthan those in the dermis.26,27 Other histopatho-logic features include lining up of atypicallymphocytes at the dermoepidermal junction,Pautrier microabscesses and fibrotic changes inthe papillary dermis, none of which is specificfor the diagnosis of MF11 (Fig. 2). Indeed, Cer-roni et al.’s13 series of 20 cases lacked many ofthese features. Folliculotropic and syringotropicMF are characterized by infiltration of atypicallymphocytes within and around the hair follicleand/or eccrine epithelium6,8 sometimes withfollicular mucinosis.20 However, atypia can beminimal and distinction from idiopathic priorto follicular mucinosis is problematic; follow-upwith repeated biopsies may be required. Thus,in short, the histopathologic features of solitarylesions of MF mimic the features of the classicdisease.
In the context of a solitary lesion, perhaps theburden of proof for the diagnosis should beparticularly stringent; in Ally et al.’s3 series of 15patients there were at least two of the following;morphological and cytological features of MF,
Fig. 2. ’Lining up’ of atypical lymphocytes at the dermoepider-mal junction and fibrotic changes in the papillary dermis arenoted in a solitary patch of mycosis fungoides involving thethigh of a 75-year male (hematoxylin/eosin, ×100).
loss of T-cell associated antigens, T-cell clonalityand appropriate clinical appearance.
ImmunocytochemistryImmunophenotypically, solitary MF, like classicMF, is usually a neoplasm of CD4+ T-helpercells, although CD8+ and double negativeCD4−/CD8− variants have been described.28 Inaddition, there may be variable antigen loss ofCD2, CD5 and CD7.3 These immunophenotypesdo not seem to affect prognosis.28,29
T-cell receptor gene analysisT-cell receptor (TCR) gene rearrangements aredetected in approximately 57–71% of cases ofearly MF,29 so solitary lesions might be expectedto have a similar or perhaps lower clonal preva-lence. Out of the 166 cases of solitary MFpublished, approximately 76 were tested forTCR clonality, of which 45 cases had a clonalTCR rearrangement.3,13,16,20,28,30–32 The detec-tion of monoclonal TCR rearrangements doesnot appear to be of prognostic impact.13,16,29
Pagetoid reticulosis (Woringer-Kolopp)In 1939, Woringer and Kolopp reported a soli-tary plaque on the forearm of a 13-year-oldboy, which resembled MF. Since then, theterm pagetoid reticulosis was introduced, torecognize the similarity between the atypicalepidermotropic cells in this disease and theintraepidermal adenocarcinomatous cells ofPaget’s disease of the nipple.33 In the 2005,WHO/EORTC classification of cutaneous lym-phomas, pagetoid reticulosis is classified as a
3

Review
Fig. 3. A well-circumscribed, hyperkeratotic plaque of pagetoidreticulosis.
variant of MF, despite having distinct clinicaland histopathologic features.14,34–36
Clinical featuresThe typical lesion of pagetoid reticulosis is asolitary, slow growing, well circumscribed, psori-asiform or hyperkeratotic plaque1,20,37 (Fig. 3).In some cases, patients present with multiplelesions.38 Pagetoid reticulosis typically affectsthe distal extremities,33 although, lesions onthe trunk39 and even the tongue38 have beendescribed. Pagetoid reticulosis can affect any agegroup including young children40 and usuallyhas an indolent clinical course, although thereis potential for dissemination and malignantbehavior.20,41 Some cases have been associatedwith the development of MF several years afterthe development of pagetoid reticulosis,38,42
highlighting the need for long-term follow-up.In contrast to solitary MF, extracutaneous dis-semination or disease-related death has neverbeen reported.1
Histopathologic featuresPagetoid reticulosis is characterized by epider-mal hyperplasia with parakeratosis, prominentacanthosis and florid epidermotropism of atyp-ical lymphocytes typically scattered throughoutthe epidermis1,20 (Fig. 4A). It is this patternof epidermotropism that is characteristic, anddespite the high number of intraepidermallymphocytes, Pautrier microabscesses are absentor rare in the authors’ experience. The dermalinfiltrate in pagetoid reticulosis consists of reac-tive lymphocytes and histiocytes. In contrast, MFis characterized by atypical lymphocytes aboveand below the dermal-epidermal junction.38
In observing a pagetoid reticulosis pattern,attention to clinical features is required to
distinguish these cases from lymphomatoidpapulosis (LyP) type D (Fig. 4B) or the morerecently described variant of LyP associatedwith 6p25.3 rearrangements, rare cases of MFwith this pattern and aggressive epidermotropicCD8+ T-cell lymphoma.43 In addition, micro-scopic distinction of pagetoid reticulosis fromsome cases of CD8+ pityriasis lichenoides etvarioliformis acuta cases may be challenging,especially when only sparse clinical data areprovided.44
ImmunocytochemistryIn a recent review by Mourtzinos et al.45 theneoplastic T-cells in pagetoid reticulosis wereCD8+/CD4− in 53% (Fig. 4C), CD4+/CD8−in 36% and CD4−/CD8− in 11% of cases.Furthermore, approximately 47% of pagetoidreticulosis cases showed strong and extensiveCD30 expression; in such cases the distinctionfrom lymphomatoid papulosis is particularlygermane. High CD30 expression is uncommonin patch stage MF, and is largely found in laterstages and/or large cell transformation.46 Toour knowledge, it has never been reported incases of solitary MF. The immunophenotype inpagetoid reticulosis appears to be prognosticallyirrelevant.45
T-cell receptor gene analysisPrevious studies have stated that the majorityof cases of pagetoid reticulosis reveal clonalrearrangements on analysis of TCR genes.20,38,41
However, approximately 13 cases in which page-toid reticulosis presented with a solitary lesionwere tested for clonality, and of those only 6 wereidentified as clonal.31,38,47–49
Primary cutaneous CD4+ small/mediumpleomorphic T-cell lymphoma (SMPTCL)SMPTCL has been credited to account forapproximately 3% of all primary cutaneouslymphomas and is listed as a provisional entityin the WHO-EORTC classification of cutaneouslymphomas.1 With recent increased recogni-tion, however, in the authors’ experience it isprobably the most common CTCL. To date,many series of cases have been reported50–55
the largest of which included 133 patients withsolitary lesions.51 The relatively recently recog-nized entity of CD8+ lymphoid proliferation ofacral sites56 has been speculated to be a pheno-typic variant of SMPTCL.57,58 It is a particularly
4
Review
A B
C
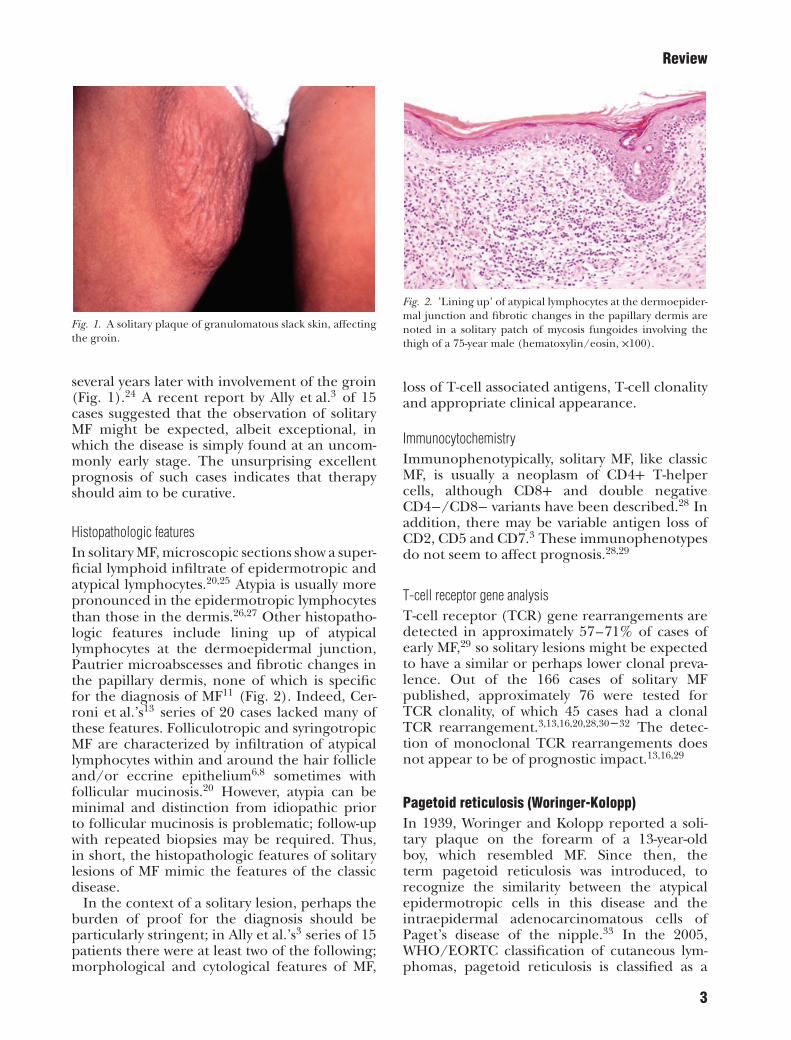
Fig. 4. Pagetoid reticulosis is characterized by epidermal hyperplasia with parakeratosis, prominent acanthosis and floridepidermotropism of atypical lymphocytes typically scattered throughout the epidermis (A, hematoxylin/eosin, ×100), similar tothat seen in lymphomatoid papulosis type D (B, hematoxylin/eosin, ×100). The neoplastic T-cells in pagetoid reticulosis are oftenCD8+/CD4(−) (C, CD8 immunostain, ×100).
contentious neoplasm, both nosologically anddiagnostically.
Clinical featuresSMPTCL usually presents with a solitary plaqueor tumor, on the face, neck or upper trunk1,51
(Fig. 5). In total, 231 solitary lesions of SMPTCLhave been described. Less commonly, it maypresent with multiple lesions.50,52,53 SMPTCLusually occurs in patients aged between 50 and60 years old, although paediatric cases havealso been described.50,51,53 Cases presenting assolitary skin lesions typically have an excellentprognosis,50,51,53 although some cases have expe-rienced recurrence of treated lesions50,51,53–55
or even extracutaneous spread and death52
(Table 1). The latter study describes five casesin which there followed an aggressive clinicalcourse, all of whom had nodules >5 cm in size.One of these cases co-expressed CD20, therewere technical problems with CD4 in anotherand at least focal loss of CD4 was observed inthree, one of which transformed to large celllymphoma. However, no immunophenotyp-ing for follicular helper T-cell expression wasperformed and perhaps the diagnosis in these
Fig. 5. The typical clinical presentation of SMPTCL, consistingof a solitary nodule on the left nose.
cases may be questioned. The WHO-EORTCclassification cites a 5-year survival of only70% although subsequent reports – and mostauthorities – now accept the prognosis is muchbetter.1 Baum et al.50 described waxing andwaning of lesions. The pathologic criteria fordiagnosis have evolved erratically rather thanbeen systematically defined, and framed within
5
Review
A B
C D
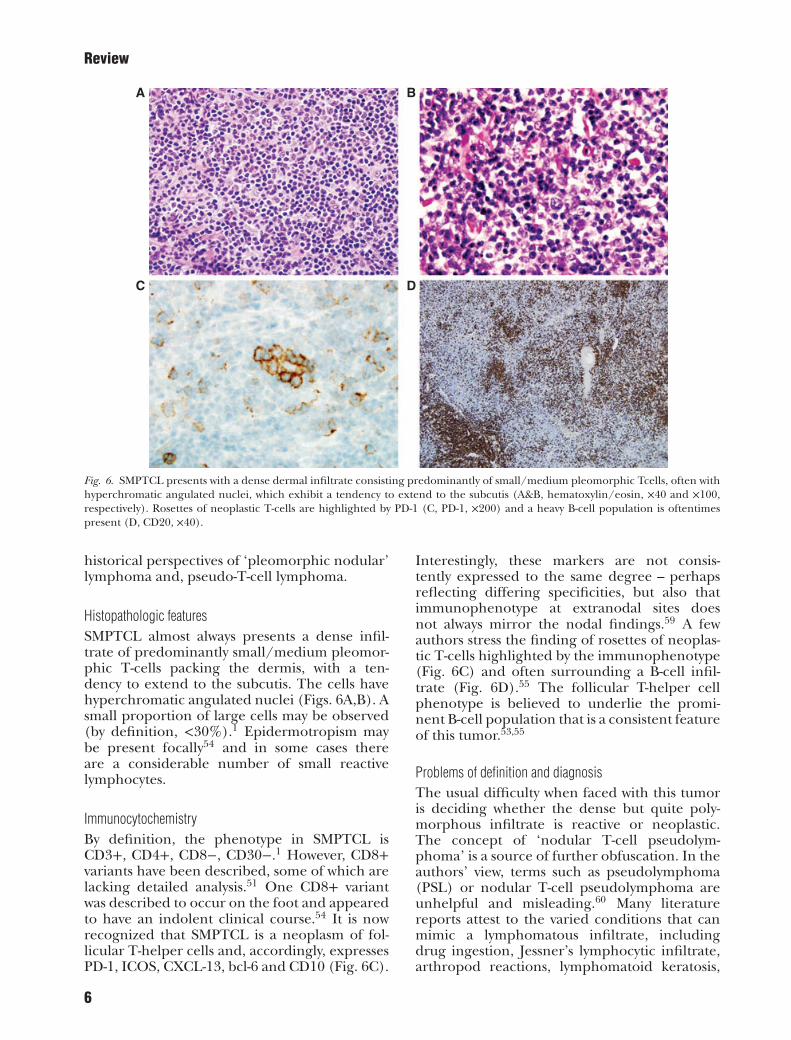
Fig. 6. SMPTCL presents with a dense dermal infiltrate consisting predominantly of small/medium pleomorphic Tcells, often withhyperchromatic angulated nuclei, which exhibit a tendency to extend to the subcutis (A&B, hematoxylin/eosin, ×40 and ×100,respectively). Rosettes of neoplastic T-cells are highlighted by PD-1 (C, PD-1, ×200) and a heavy B-cell population is oftentimespresent (D, CD20, ×40).
historical perspectives of ‘pleomorphic nodular’lymphoma and, pseudo-T-cell lymphoma.
Histopathologic featuresSMPTCL almost always presents a dense infil-trate of predominantly small/medium pleomor-phic T-cells packing the dermis, with a ten-dency to extend to the subcutis. The cells havehyperchromatic angulated nuclei (Figs. 6A,B). Asmall proportion of large cells may be observed(by definition, <30%).1 Epidermotropism maybe present focally54 and in some cases thereare a considerable number of small reactivelymphocytes.
ImmunocytochemistryBy definition, the phenotype in SMPTCL isCD3+, CD4+, CD8−, CD30−.1 However, CD8+variants have been described, some of which arelacking detailed analysis.51 One CD8+ variantwas described to occur on the foot and appearedto have an indolent clinical course.54 It is nowrecognized that SMPTCL is a neoplasm of fol-licular T-helper cells and, accordingly, expressesPD-1, ICOS, CXCL-13, bcl-6 and CD10 (Fig. 6C).
Interestingly, these markers are not consis-tently expressed to the same degree – perhapsreflecting differing specificities, but also thatimmunophenotype at extranodal sites doesnot always mirror the nodal findings.59 A fewauthors stress the finding of rosettes of neoplas-tic T-cells highlighted by the immunophenotype(Fig. 6C) and often surrounding a B-cell infil-trate (Fig. 6D).55 The follicular T-helper cellphenotype is believed to underlie the promi-nent B-cell population that is a consistent featureof this tumor.53,55
Problems of definition and diagnosisThe usual difficulty when faced with this tumoris deciding whether the dense but quite poly-morphous infiltrate is reactive or neoplastic.The concept of ‘nodular T-cell pseudolym-phoma’ is a source of further obfuscation. In theauthors’ view, terms such as pseudolymphoma(PSL) or nodular T-cell pseudolymphoma areunhelpful and misleading.60 Many literaturereports attest to the varied conditions that canmimic a lymphomatous infiltrate, includingdrug ingestion, Jessner’s lymphocytic infiltrate,arthropod reactions, lymphomatoid keratosis,
6
Review
A B
C
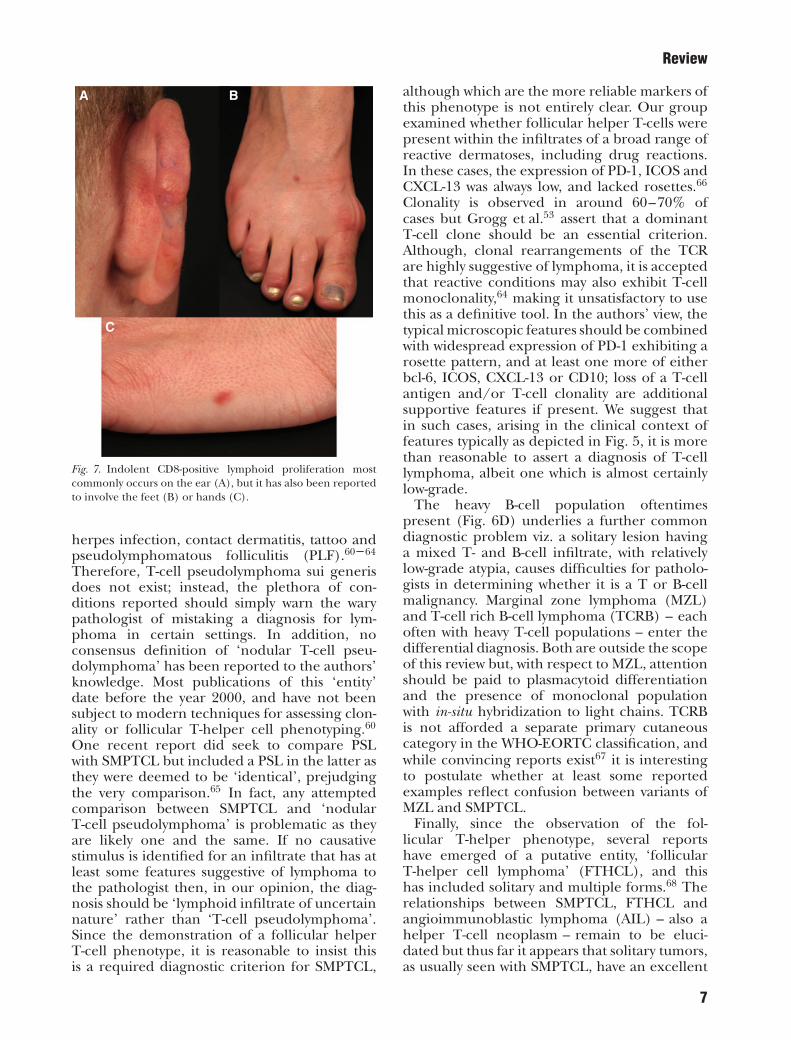
Fig. 7. Indolent CD8-positive lymphoid proliferation mostcommonly occurs on the ear (A), but it has also been reportedto involve the feet (B) or hands (C).
herpes infection, contact dermatitis, tattoo andpseudolymphomatous folliculitis (PLF).60–64
Therefore, T-cell pseudolymphoma sui generisdoes not exist; instead, the plethora of con-ditions reported should simply warn the warypathologist of mistaking a diagnosis for lym-phoma in certain settings. In addition, noconsensus definition of ‘nodular T-cell pseu-dolymphoma’ has been reported to the authors’knowledge. Most publications of this ‘entity’date before the year 2000, and have not beensubject to modern techniques for assessing clon-ality or follicular T-helper cell phenotyping.60
One recent report did seek to compare PSLwith SMPTCL but included a PSL in the latter asthey were deemed to be ‘identical’, prejudgingthe very comparison.65 In fact, any attemptedcomparison between SMPTCL and ‘nodularT-cell pseudolymphoma’ is problematic as theyare likely one and the same. If no causativestimulus is identified for an infiltrate that has atleast some features suggestive of lymphoma tothe pathologist then, in our opinion, the diag-nosis should be ‘lymphoid infiltrate of uncertainnature’ rather than ‘T-cell pseudolymphoma’.Since the demonstration of a follicular helperT-cell phenotype, it is reasonable to insist thisis a required diagnostic criterion for SMPTCL,
although which are the more reliable markers ofthis phenotype is not entirely clear. Our groupexamined whether follicular helper T-cells werepresent within the infiltrates of a broad range ofreactive dermatoses, including drug reactions.In these cases, the expression of PD-1, ICOS andCXCL-13 was always low, and lacked rosettes.66
Clonality is observed in around 60–70% ofcases but Grogg et al.53 assert that a dominantT-cell clone should be an essential criterion.Although, clonal rearrangements of the TCRare highly suggestive of lymphoma, it is acceptedthat reactive conditions may also exhibit T-cellmonoclonality,64 making it unsatisfactory to usethis as a definitive tool. In the authors’ view, thetypical microscopic features should be combinedwith widespread expression of PD-1 exhibiting arosette pattern, and at least one more of eitherbcl-6, ICOS, CXCL-13 or CD10; loss of a T-cellantigen and/or T-cell clonality are additionalsupportive features if present. We suggest thatin such cases, arising in the clinical context offeatures typically as depicted in Fig. 5, it is morethan reasonable to assert a diagnosis of T-celllymphoma, albeit one which is almost certainlylow-grade.
The heavy B-cell population oftentimespresent (Fig. 6D) underlies a further commondiagnostic problem viz. a solitary lesion havinga mixed T- and B-cell infiltrate, with relativelylow-grade atypia, causes difficulties for patholo-gists in determining whether it is a T or B-cellmalignancy. Marginal zone lymphoma (MZL)and T-cell rich B-cell lymphoma (TCRB) – eachoften with heavy T-cell populations – enter thedifferential diagnosis. Both are outside the scopeof this review but, with respect to MZL, attentionshould be paid to plasmacytoid differentiationand the presence of monoclonal populationwith in-situ hybridization to light chains. TCRBis not afforded a separate primary cutaneouscategory in the WHO-EORTC classification, andwhile convincing reports exist67 it is interestingto postulate whether at least some reportedexamples reflect confusion between variants ofMZL and SMPTCL.
Finally, since the observation of the fol-licular T-helper phenotype, several reportshave emerged of a putative entity, ‘follicularT-helper cell lymphoma’ (FTHCL), and thishas included solitary and multiple forms.68 Therelationships between SMPTCL, FTHCL andangioimmunoblastic lymphoma (AIL) – also ahelper T-cell neoplasm – remain to be eluci-dated but thus far it appears that solitary tumors,as usually seen with SMPTCL, have an excellent
7
Review
A B
C D
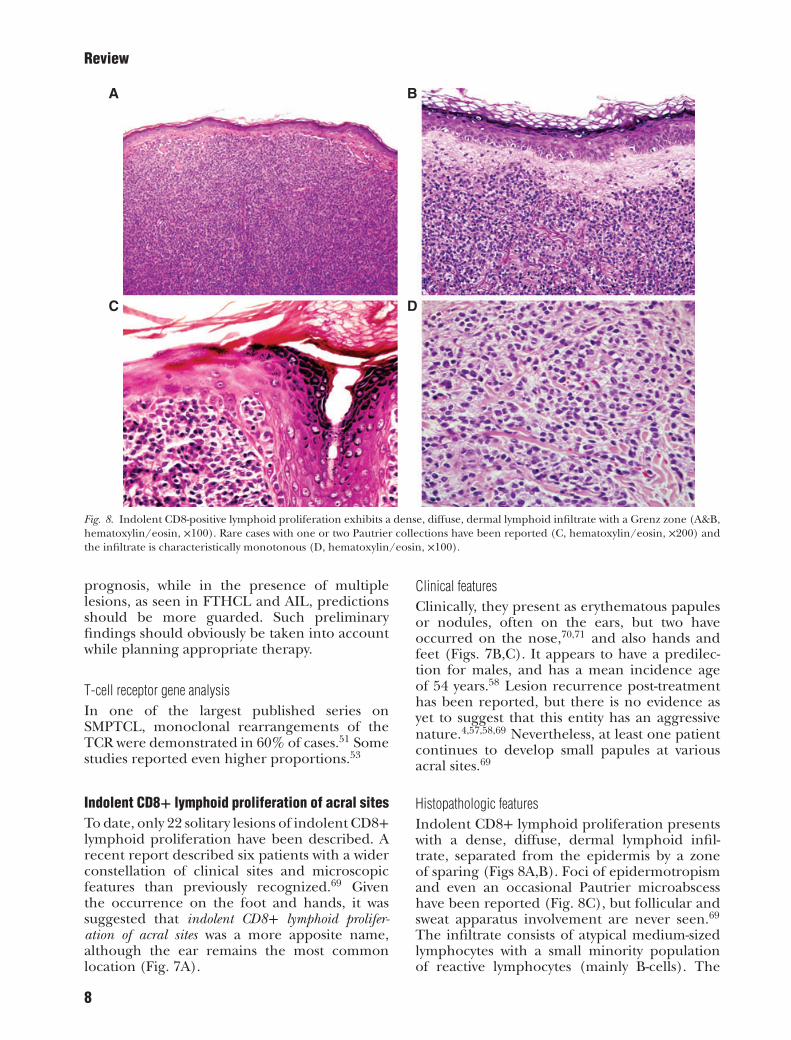
Fig. 8. Indolent CD8-positive lymphoid proliferation exhibits a dense, diffuse, dermal lymphoid infiltrate with a Grenz zone (A&B,hematoxylin/eosin, ×100). Rare cases with one or two Pautrier collections have been reported (C, hematoxylin/eosin, ×200) andthe infiltrate is characteristically monotonous (D, hematoxylin/eosin, ×100).
prognosis, while in the presence of multiplelesions, as seen in FTHCL and AIL, predictionsshould be more guarded. Such preliminaryfindings should obviously be taken into accountwhile planning appropriate therapy.
T-cell receptor gene analysisIn one of the largest published series onSMPTCL, monoclonal rearrangements of theTCR were demonstrated in 60% of cases.51 Somestudies reported even higher proportions.53
Indolent CD8+ lymphoid proliferation of acral sitesTo date, only 22 solitary lesions of indolent CD8+lymphoid proliferation have been described. Arecent report described six patients with a widerconstellation of clinical sites and microscopicfeatures than previously recognized.69 Giventhe occurrence on the foot and hands, it wassuggested that indolent CD8+ lymphoid prolifer-ation of acral sites was a more apposite name,although the ear remains the most commonlocation (Fig. 7A).
Clinical featuresClinically, they present as erythematous papulesor nodules, often on the ears, but two haveoccurred on the nose,70,71 and also hands andfeet (Figs. 7B,C). It appears to have a predilec-tion for males, and has a mean incidence ageof 54 years.58 Lesion recurrence post-treatmenthas been reported, but there is no evidence asyet to suggest that this entity has an aggressivenature.4,57,58,69 Nevertheless, at least one patientcontinues to develop small papules at variousacral sites.69
Histopathologic featuresIndolent CD8+ lymphoid proliferation presentswith a dense, diffuse, dermal lymphoid infil-trate, separated from the epidermis by a zoneof sparing (Figs 8A,B). Foci of epidermotropismand even an occasional Pautrier microabscesshave been reported (Fig. 8C), but follicular andsweat apparatus involvement are never seen.69
The infiltrate consists of atypical medium-sizedlymphocytes with a small minority populationof reactive lymphocytes (mainly B-cells). The
8
Review
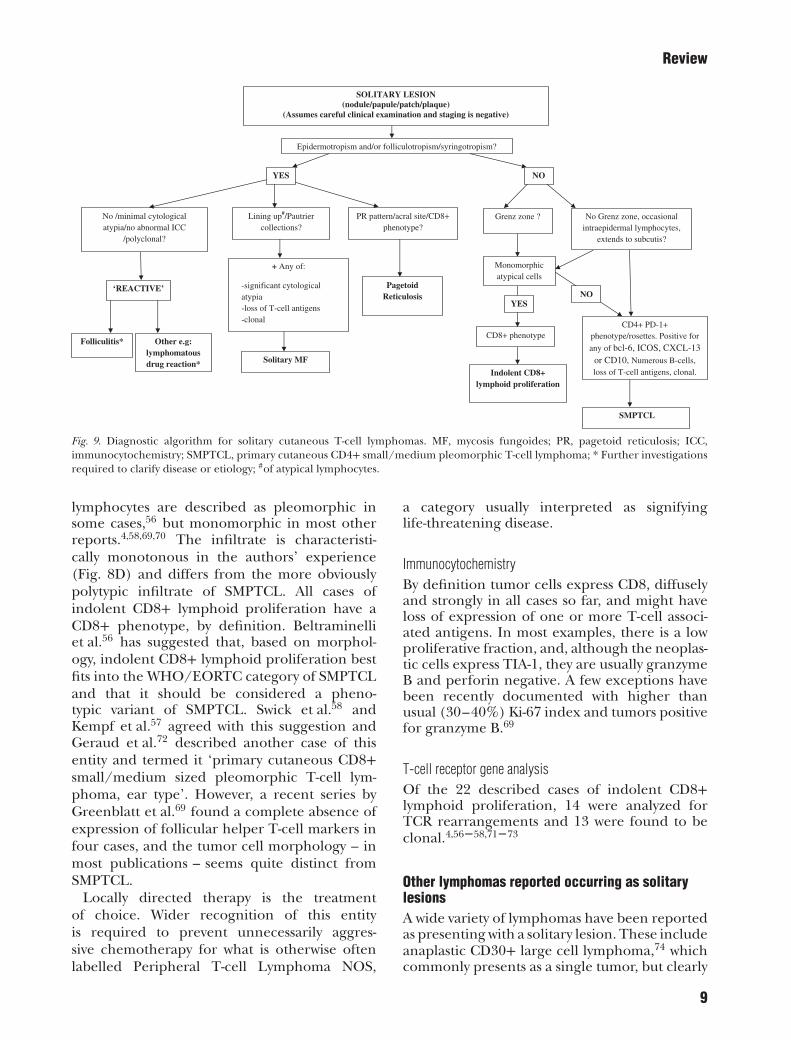
SOLITARY LESION(nodule/papule/patch/plaque)
(Assumes careful clinical examination and staging is negative)
Epidermotropism and/or folliculotropism/syringotropism?
No /minimal cytological atypia/no abnormal ICC
/polyclonal?
‘REACTIVE’
Folliculitis* Other e.g: lymphomatous drug reaction*
Lining up#/Pautrier collections?
+ Any of:
-significant cytological atypia-loss of T-cell antigens-clonal
Solitary MF
PR pattern/acral site/CD8+ phenotype?
Pagetoid Reticulosis
Grenz zone ? No Grenz zone, occasional intraepidermal lymphocytes,
extends to subcutis?
Monomorphic atypical cells
CD8+ phenotypeCD4+ PD-1+
phenotype/rosettes. Positive for
any of bcl-6, ICOS, CXCL-13 or CD10, Numerous B-cells, loss of T-cell antigens, clonal.
Num
Indolent CD8+ lymphoid proliferation
SMPTCL
YES NO
NOYES
Fig. 9. Diagnostic algorithm for solitary cutaneous T-cell lymphomas. MF, mycosis fungoides; PR, pagetoid reticulosis; ICC,immunocytochemistry; SMPTCL, primary cutaneous CD4+ small/medium pleomorphic T-cell lymphoma; * Further investigationsrequired to clarify disease or etiology; #of atypical lymphocytes.
lymphocytes are described as pleomorphic insome cases,56 but monomorphic in most otherreports.4,58,69,70 The infiltrate is characteristi-cally monotonous in the authors’ experience(Fig. 8D) and differs from the more obviouslypolytypic infiltrate of SMPTCL. All cases ofindolent CD8+ lymphoid proliferation have aCD8+ phenotype, by definition. Beltraminelliet al.56 has suggested that, based on morphol-ogy, indolent CD8+ lymphoid proliferation bestfits into the WHO/EORTC category of SMPTCLand that it should be considered a pheno-typic variant of SMPTCL. Swick et al.58 andKempf et al.57 agreed with this suggestion andGeraud et al.72 described another case of thisentity and termed it ‘primary cutaneous CD8+small/medium sized pleomorphic T-cell lym-phoma, ear type’. However, a recent series byGreenblatt et al.69 found a complete absence ofexpression of follicular helper T-cell markers infour cases, and the tumor cell morphology – inmost publications – seems quite distinct fromSMPTCL.
Locally directed therapy is the treatmentof choice. Wider recognition of this entityis required to prevent unnecessarily aggres-sive chemotherapy for what is otherwise oftenlabelled Peripheral T-cell Lymphoma NOS,
a category usually interpreted as signifyinglife-threatening disease.
ImmunocytochemistryBy definition tumor cells express CD8, diffuselyand strongly in all cases so far, and might haveloss of expression of one or more T-cell associ-ated antigens. In most examples, there is a lowproliferative fraction, and, although the neoplas-tic cells express TIA-1, they are usually granzymeB and perforin negative. A few exceptions havebeen recently documented with higher thanusual (30–40%) Ki-67 index and tumors positivefor granzyme B.69
T-cell receptor gene analysisOf the 22 described cases of indolent CD8+lymphoid proliferation, 14 were analyzed forTCR rearrangements and 13 were found to beclonal.4,56–58,71–73
Other lymphomas reported occurring as solitarylesionsA wide variety of lymphomas have been reportedas presenting with a solitary lesion. These includeanaplastic CD30+ large cell lymphoma,74 whichcommonly presents as a single tumor, but clearly
9

Review
spread from a systemic primary needs to beexcluded; lymphomatoid papulosis,75 althoughsuch cases reflect the initial presentation, asa single lesion is inevitably followed by cropsof papules; subcutaneous panniculitis-like T-celllymphoma,2 and CD20+ cutaneous T-cell lym-phoma NOS.76 A repeated observation in themajority of such cases is the excellent prognosis.
RecommendationsOn the basis of the literature review presentedherein, we have proposed a system for the diag-nosis of some of lymphomas that might presentas a solitary lesion, which involves clinical, micro-scopic, immunocytochemical and molecular
biologic features (Fig. 9). The proposed algo-rithm summarizes many of the points discussed.
ConclusionA variety of cutaneous T-cell lymphomas canpresent as a solitary lesion, and regardless oftype these almost always have a better clini-cal outcome than the more common multiplecounterpart; treatment can aim, therefore, to becurative. Nevertheless, follow-up is warranted.We propose a system to aid in the classificationof these lesions based on a combination of clin-ical, histopathologic, immunocytochemical andmolecular biologic features.
References1. Willemze R, Jaffe ES, Burg G, et al.
WHO-EORTC classification for cutaneouslymphomas. Blood 2005; 105: 3768.
2. Setyadi HG, Nash JW, Duvic M. The soli-tary lymphomatous papule, nodule, ortumor. J Am Acad Dermatol 2007; 57:1072.
3. Ally MS, Pawade J, Tanaka M, et al. Solitarymycosis fungoides: a distinct clinicopatho-logic entity with a good prognosis: a seriesof 15 cases and literature review. J Am AcadDermatol 2012; 67: 736.
4. Petrella T, Maubec E, Cornillet-LefebvreP, et al. Indolent CD8-positive lymphoidproliferation of the ear: a distinct primarycutaneous T-cell lymphoma? Am J SurgPathol 2007; 31: 1887.
5. Willemze R, Kerl H, Sterry W, et al.EORTC classification for primary cuta-neous lymphomas: a proposal from theCutaneous Lymphoma Study Group ofthe European Organization for Researchand Treatment of Cancer. Blood 1997; 90:354.
6. Hsiao PF, Hsiao CH, Tsai TF, Jee SH. Unile-sional folliculotropic/syringotropic cuta-neous T-cell lymphoma presenting as anindurated plaque on the nape. Int J Der-matol 2006; 45: 1268.
7. Marzano AV, Berti E, Lupica L, Alessi E.Unilesional follicular mycosis fungoides.Dermatology (Basel, Switzerland) 1999;199: 174.
8. Kempf W, Kazakov DV, Schermesser M,et al. Unilesional follicular mycosis fun-goides: report of two cases with progres-sion to tumor stage and review of the lit-erature. J Cutan Pathol 2012; 39: 853.
9. Burg G, Schmockel C. Syringolymphoidhyperplasia with alopecia--a syringotropiccutaneous T-cell lymphoma? Dermatology(Basel, Switzerland) 1992; 184: 306.
10. Hobbs JL, Chaffins ML, Douglass MC.Syringolymphoid hyperplasia with alope-cia: two case reports and review of the liter-ature. J Am Acad Dermatol 2003; 49: 1177.
11. Pileri A, Facchetti F, Rutten A, et al.Syringotropic mycosis fungoides: a rarevariant of the disease with peculiar clini-copathologic features. Am J Surg Pathol2011; 35: 100.
12. Zelger B, Sepp N, Weyrer K, GrunewaldK, Zelger B. Syringotropic cutaneous T-celllymphoma: a variant of mycosis fungoides?Br J Dermatol 1994; 130: 765.
13. Cerroni L, Fink-Puches R, El-Shabrawi-Caelen L, Soyer HP, LeBoit PE, Kerl H.Solitary skin lesions with histopathologicfeatures of early mycosis fungoides. Am JDermatopathol 1999; 21: 518.
14. Oliver GF, Winkelmann RK. Unilesionalmycosis fungoides: a distinct entity. J AmAcad Dermatol 1989; 20: 63.
15. Heald PW, Glusac EJ. Unilesional cuta-neous T-cell lymphoma: clinical features,therapy, and follow-up of 10 patients witha treatment-responsive mycosis fungoidesvariant. J Am Acad Dermatol 2000; 42(2 Pt1): 283.
16. Hodak E, Phenig E, Amichai B, et al.Unilesional mycosis fungoides: a study ofseven cases. Dermatology (Basel, Switzer-land) 2000; 201: 300.
17. Micaily B, Miyamoto C, Kantor G, et al.Radiotherapy for unilesional mycosis fun-goides. Int J Radiat Oncol Biol Phys 1998;42: 361.
18. Wilson LD, Kacinski BM, Jones GW. Localsuperficial radiotherapy in the manage-ment of minimal stage IA cutaneous T-celllymphoma (Mycosis Fungoides). Int JRadiat Oncol Biol Phys 1998; 40: 109.
19. Subhawong AP, Subhawong TK, Ali SZ.Large cell transformation of mycosisfungoides on fine needle aspiration: anunusual case mimicking classical Hodgkinlymphoma. Acta Cytol 2012; 56: 321.
20. Cho-Vega JH, Tschen JA, Duvic M, VegaF. Early-stage mycosis fungoides variants:case-based review. Ann Diagn Pathol 2010;14: 369.
21. Agar NS, Wedgeworth E, Crichton S,et al. Survival outcomes and prognosticfactors in mycosis fungoides/Sezarysyndrome: validation of the revisedInternational Society for CutaneousLymphomas/European Organisation forResearch and Treatment of Cancer stagingproposal. J Clin Oncol 2010; 28: 4730.
22. van Doorn R, Scheffer E, Willemze R. Fol-licular mycosis fungoides, a distinct dis-ease entity with or without associated fol-licular mucinosis: a clinicopathologic andfollow-up study of 51 patients. Arch Der-matol 2002; 138: 191.
23. Kempf W, Ostheeren-Michaelis S, PaulliM, et al. Granulomatous mycosis fun-goides and granulomatous slack skin:a multicenter study of the CutaneousLymphoma Histopathology Task ForceGroup of the European OrganizationFor Research and Treatment of Cancer(EORTC). Arch Dermatol 2008; 144:1609.
24. Benton EC, Morris SL, Robson A, Whit-taker SJ. An unusual case of granuloma-tous slack skin disease with necrobiosis.Am J Dermatopathol 2008; 30: 462.
25. Pimpinelli N, Olsen EA, Santucci M, et al.Defining early mycosis fungoides. J AmAcad Dermatol 2005; 53: 1053.
26. Kinney MC, Jones D. Cutaneous T-cell andNK-cell lymphomas: the WHO-EORTCclassification and the increasing recogni-tion of specialized tumor types. Am J ClinPathol 2007; 127: 670.
27. Naraghi ZS, Seirafi H, Valikhani M, Far-naghi F, Kavusi S, Dowlati Y. Assessment ofhistologic criteria in the diagnosis of myco-sis fungoides. Int J Dermatol 2003; 42: 45.
28. Hodak E, David M, Maron L, AviramA, Kaganovsky E, Feinmesser M. CD4/CD8 double-negative epidermotropiccutaneous T-cell lymphoma: an immuno-histochemical variant of mycosisfungoides. J Am Acad Dermatol 2006; 55:276.
10
Review
29. Massone C, Crisman G, Kerl H, Cerroni L.The prognosis of early mycosis fungoidesis not influenced by phenotype and T-cellclonality. Br J Dermatol 2008; 159: 881.
30. Ardigo M, Cota C, Berardesca E. Unile-sional mycosis fungoides successfullytreated with imiquimod. Eur J Dermatol2006; 16: 446.
31. Burns MK, Chan LS, Cooper KD.Woringer-Kolopp disease (localized page-toid reticulosis) or unilesional mycosisfungoides? An analysis of eight cases withbenign disease. Arch Dermatol 1995; 131:325.
32. Chan DV, Aneja S, Honda K, et al.Radiation therapy in the managementof unilesional primary cutaneous T-celllymphomas. Br J Dermatol 2012; 166:1134.
33. Braun-Falco O, Marghescu S, Wolff HH.[Pagetoide reticulosis--Woringer-Kolopp’sdisease]. Der Hautarzt; Zeitschrift fur Der-matologie, Venerologie, und verwandteGebiete. 1973; 24: 11.
34. Jones RR, Chu A. Pagetoid reticulosis andsolitary mycosis fungoides. Distinct clinico-pathological entities. J Cutan Pathol 1981;8: 40.
35. Lee J, Viakhireva N, Cesca C, et al. Clini-copathologic features and treatment out-comes in Woringer-Kolopp disease. J AmAcad Dermatol 2008; 59: 706.
36. Steffen C. Ketron-Goodman disease,Woringer-Kolopp disease, and pagetoidreticulosis. Am J Dermatopathol 2005; 27:68.
37. Kempf W, Sander CA. Classificationof cutaneous lymphomas - an update.Histopathology 2010; 56: 57.
38. Haghighi B, Smoller BR, LeBoit PE,Warnke RA, Sander CA, Kohler S.Pagetoid reticulosis (Woringer-Koloppdisease): an immunophenotypic, molec-ular, and clinicopathologic study. ModPathol 2000; 13: 502.
39. Medenica M, Lorincz AL. Pagetoid retic-ulosis (Woringer-Kolopp disease). Histo-pathologic and ultrastructural obser-vations. Arch Dermatol 1978; 114:262.
40. Miedler JD, Kristjansson AK, Gould J, Tam-burro J, Gilliam AC. Pagetoid reticulosis ina 5-year-old boy. J Am Acad Dermatol 2008;58: 679.
41. Yagi H, Hagiwara T, Shirahama S, TokuraY, Takigawa M. Disseminated pagetoidreticulosis: need for long-term follow-up. JAm Acad Dermatol 1994; 30(2 Pt 2): 345.
42. Ioannides G, Engel MF, Rywlin AM.Woringer-Kolopp disease (pagetoid retic-ulosis). Am J Dermatopathol 1983; 5:153.
43. Karai LJ, Kadin ME, Hsi ED, et al. Chromo-somal rearrangements of 6p25.3 define anew subtype of Lymphomatoid Papulosis.Am J Surg Pathol 2013; 37: 1173.
44. Kempf W, Kazakov DV, Palmedo G,Fraitag S, Schaerer L, Kutzner H. Pityr-iasis lichenoides et varioliformis acutawith numerous CD30(+) cells: a variant
mimicking lymphomatoid papulosis andother cutaneous lymphomas. A clinico-pathologic, immunohistochemical, andmolecular biological study of 13 cases. AmJ Surg Pathol 2012; 36: 1021.
45. Mourtzinos N, Puri PK, Wang G, Liu ML.CD4/CD8 double negative pagetoid retic-ulosis: a case report and literature review.J Cutan Pathol 2010; 37: 491.
46. Wu H, Telang GH, Lessin SR, Von-derheid EC. Mycosis fungoides withCD30-positive cells in the epidermis. Am JDermatopathol 2000; 22: 212.
47. Mielke V, Wolff HH, Winzer M, SterryW. Localized and disseminated pagetoidreticulosis. Diagnostic immunophenotyp-ical findings. Arch Dermatol 1989; 125:402.
48. Palmer RA, Keefe M, Slater D, WhittakerSJ. Case 4: Pagetoid reticulosis (Woringer-Kolopp type) or unilesional mycosis fun-goides (MF). Clin Exp Dermatol 2002; 27:345.
49. Smoller BR, Stewart M, Warnke R. A caseof Woringer-Kolopp disease with Ki-1(CD30)+ cytotoxic/suppressor cells. ArchDermatol 1992; 128: 526.
50. Baum CL, Link BK, Neppalli VT, Swick BL,Liu V. Reappraisal of the provisional entityprimary cutaneous CD4+ small/mediumpleomorphic T-cell lymphoma: a series of10 adult and pediatric patients and reviewof the literature. J Am Acad Dermatol2011; 65: 739.
51. Beltraminelli H, Leinweber B, Kerl H,Cerroni L. Primary cutaneous CD4+small-/medium-sized pleomorphic T-celllymphoma: a cutaneous nodular prolif-eration of pleomorphic T lymphocytesof undetermined significance? A study of136 cases. Am J Dermatopathol 2009; 31:317.
52. Garcia-Herrera A, Colomo L, Camos M,et al. Primary cutaneous small/mediumCD4+ T-cell lymphomas: a heterogeneousgroup of tumors with different clinico-pathologic features and outcome. J ClinOncol 2008; 26: 3364.
53. Grogg KL, Jung S, Erickson LA,McClure RF, Dogan A. Primary cuta-neous CD4-positive small/medium-sizedpleomorphic T-cell lymphoma: a clonalT-cell lymphoproliferative disorder withindolent behavior. Mod Pathol 2008; 21:708.
54. Khamaysi Z, Ben-Arieh Y, Epelbaum R,Bergman R. Pleomorphic CD8+ small/medium size cutaneous T-cell lymphoma.Am J Dermatopathol 2006; 28: 434.
55. Rodriguez Pinilla SM, Roncador G,Rodriguez-Peralto JL, et al. Primarycutaneous CD4+ small/medium-sizedpleomorphic T-cell lymphoma expressesfollicular T-cell markers. Am J Surg Pathol2009; 33: 81.
56. Beltraminelli H, Mullegger R, Cerroni L.Indolent CD8+ lymphoid proliferationof the ear: a phenotypic variant of thesmall-medium pleomorphic cutaneousT-cell lymphoma? J Cutan Pathol 2010; 37:81.
57. Kempf W, Kazakov DV, Cozzio A, et al.Primary cutaneous CD8(+) small- tomedium-sized lymphoproliferative disor-der in extrafacial sites: clinicopathologicfeatures and concept on their classifi-cation. Am J Dermatopathol 2013; 35:159.
58. Swick BL, Baum CL, Venkat AP, Liu V.Indolent CD8+ lymphoid proliferation ofthe ear: report of two cases and review ofthe literature. J Cutan Pathol 2011; 38: 209.
59. Grogg KL, Attygalle AD, Macon WR,Remstein ED, Kurtin PJ, Dogan A. Expres-sion of CXCL13, a chemokine highlyupregulated in germinal center T-helpercells, distinguishes angioimmunoblasticT-cell lymphoma from peripheral T-celllymphoma, unspecified. Modern Pathol2006; 19: 1101.
60. Bergman R. Pseudolymphoma and cuta-neous lymphoma: facts and controversies.Clin Dermatol 2010; 28: 568.
61. Imafuku S, Ito K, Nakayama J. Cutaneouspseudolymphoma induced by adali-mumab and reproduced by infliximab ina patient with arthropathic psoriasis. Br JDermatol 2012; 166: 675.
62. Arai E, Okubo H, Tsuchida T, KitamuraK, Katayama I. Pseudolymphomatous folli-culitis: a clinicopathologic study of 15 casesof cutaneous pseudolymphoma with follic-ular invasion. Am J Surg Pathol 1999; 23:1313.
63. Cristaudo A, Forte G, Bocca B, et al. Per-manent tattoos: evidence of pseudolym-phoma in three patients and metal compo-sition of the dyes. Eur J Dermatol 2012; 22:776.
64. Arai E, Shimizu M, Tsuchida T, IzakiS, Ogawa F, Hirose T. Lymphomatoidkeratosis: an epidermotropic type ofcutaneous lymphoid hyperplasia: clinico-pathological, immunohistochemical, andmolecular biological study of 6 cases. ArchDermatol 2007; 143: 53.
65. Cetinozman F, Jansen PM, WillemzeR. Expression of programmed death-1in primary cutaneous CD4-positivesmall/medium-sized pleomorphic T-celllymphoma, cutaneous pseudo-T-celllymphoma, and other types of cutaneousT-cell lymphoma. Am J Surg Pathol 2012;36: 109.
66. Ally MS, Prasad Hunasehally RY,Rodriguez-Justo M, et al. Evaluationof follicular T-helper cells in primary cuta-neous CD4+ small/medium pleomorphicT-cell lymphoma and dermatitis. J CutanPathol 2013; 40: 1006.
67. Vezzoli P, Fiorani R, Girgenti V, et al.Cutaneous T-cell/histiocyte-rich B-celllymphoma: a case report and reviewof the literature. Dermatology (Basel,Switzerland) 2011; 222: 225.
68. Hu S, Young KH, Konoplev SN, MedeirosLJ. Follicular T-cell lymphoma: a mem-ber of an emerging family of follicularhelper T-cell derived T-cell lymphomas.Hum Pathol 2012; 43: 1789.
11

Review
69. Greenblatt D, Ally M, Child F, et al. Indo-lent CD8(+) lymphoid proliferation ofacral sites: a clinicopathologic study ofsix patients with some atypical features. JCutan Pathol 2013; 40: 248.
70. Ryan AJ, Robson A, Hayes BD, SheahanK, Collins P. Primary cutaneous periph-eral T-cell lymphoma, unspecified with anindolent clinical course: a distinct periph-eral T-cell lymphoma? Clin Exp Dermatol2010; 35: 892.
71. Suchak R, O’Connor S, McNamara C,Robson A. Indolent CD8-positive lym-phoid proliferation on the face: partof the spectrum of primary cutaneous
small-/medium-sized pleomorphic T-celllymphoma or a distinct entity? J CutanPathol 2010; 37: 977.
72. Geraud C, Goerdt S, Klemke CD. Primarycutaneous CD8+ small/medium-sizedpleomorphic T-cell lymphoma, ear-type: aunique cutaneous T-cell lymphoma with afavourable prognosis. Br J Dermatol 2011;164: 456.
73. Zeng W, Nava VE, Cohen P, OzdemirliM. Indolent CD8-positive T-cell lymphoidproliferation of the ear: a report of twocases. J Cutan Pathol 2012; 39: 696.
74. Booken N, Goerdt S, Klemke CD. Clin-ical spectrum of primary cutaneous
CD30-positive anaplastic large cell lym-phoma: an analysis of the MannheimCutaneous Lymphoma Registry. J GermanSoc Dermatol 2012; 10: 331.
75. de-Misa RF, Garcia M, Dorta S, et al. Soli-tary oral ulceration as the first appearanceof lymphomatoid papulosis: a diagnosticchallenge. Clin Exp Dermatol 2010; 35:165.
76. Oshima H, Matsuzaki Y, Takeuchi S,Nakano H, Sawamura D. CD20+ primarycutaneous T-cell lymphoma presenting asa solitary extensive plaque. Br J Dermatol2009; 160: 894.
12