Embed Size (px)
Citation preview
t h e s u r g e o n 8 ( 2 0 1 0 ) 1 1 9 – 1 2 1
avai lable at www.sciencedirect .com
The Surgeon, Journal of the Royal Collegesof Surgeons of Edinburgh and Ireland
www.thesurgeon.net
Correspondence: Surgical Technique
A simple intraoperative technique to avoid limb lengthdiscrepancy in total hip arthroplasty
Keywords
Limb length discrepancy
Total hip arthroplasty
Sir,
Introduction
Limb length discrepancy (LLD) following total hip arthroplasty
(THA) is a well-known and documented complication. LLD can
pose a substantial problem for both the patient and the
surgeon. Patient dissatisfaction with LLD after THA is the
most common reason for litigation against orthopaedic
surgeons.1,2 Failure to restore limb length may lead to an
unstable hip, whereas over-lengthening may cause low back
pain, sciatic nerve palsy and early mechanical loosening.3
Several intraoperative techniques both invasive and non-
invasive have been reported in the literature to overcome LLD
during THA.2,4–10 The accuracy of all the methods that measure
from pinsanchored intopelvis to point onthe greater trochanter
may be affected by the inherent variability of the leg position
when measurements are made. Bending or dislodging the pins
and using of calliper devices can be cumbersome during the
THA surgery and can compromise the measurements.
Hence we describe a simple, safe and reliable intra-
operative technique, which can be easily used in THA surgery
done by posterior approach without any additional equip-
ment, incision and radiographs.
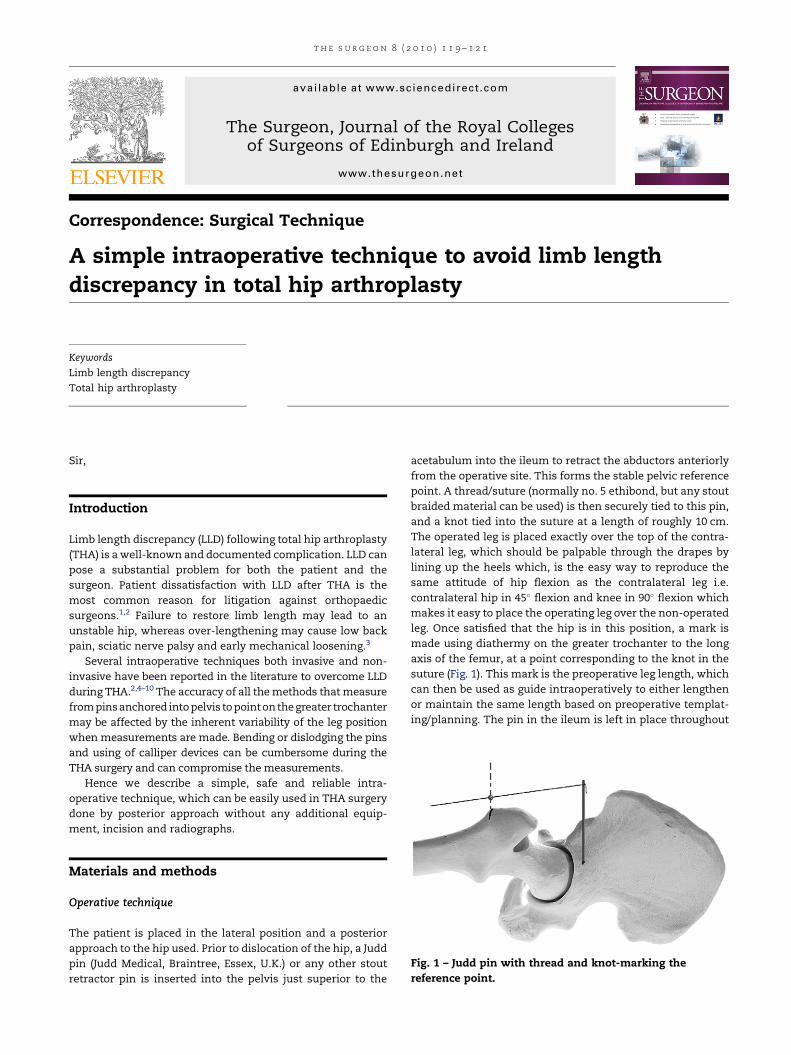
Fig. 1 – Judd pin with thread and knot-marking the
reference point.
Materials and methods
Operative technique
The patient is placed in the lateral position and a posterior
approach to the hip used. Prior to dislocation of the hip, a Judd
pin (Judd Medical, Braintree, Essex, U.K.) or any other stout
retractor pin is inserted into the pelvis just superior to the
acetabulum into the ileum to retract the abductors anteriorly
from the operative site. This forms the stable pelvic reference
point. A thread/suture (normally no. 5 ethibond, but any stout
braided material can be used) is then securely tied to this pin,
and a knot tied into the suture at a length of roughly 10 cm.
The operated leg is placed exactly over the top of the contra-
lateral leg, which should be palpable through the drapes by
lining up the heels which, is the easy way to reproduce the
same attitude of hip flexion as the contralateral leg i.e.
contralateral hip in 45� flexion and knee in 90� flexion which
makes it easy to place the operating leg over the non-operated
leg. Once satisfied that the hip is in this position, a mark is
made using diathermy on the greater trochanter to the long
axis of the femur, at a point corresponding to the knot in the
suture (Fig. 1). This mark is the preoperative leg length, which
can then be used as guide intraoperatively to either lengthen
or maintain the same length based on preoperative templat-
ing/planning. The pin in the ileum is left in place throughout
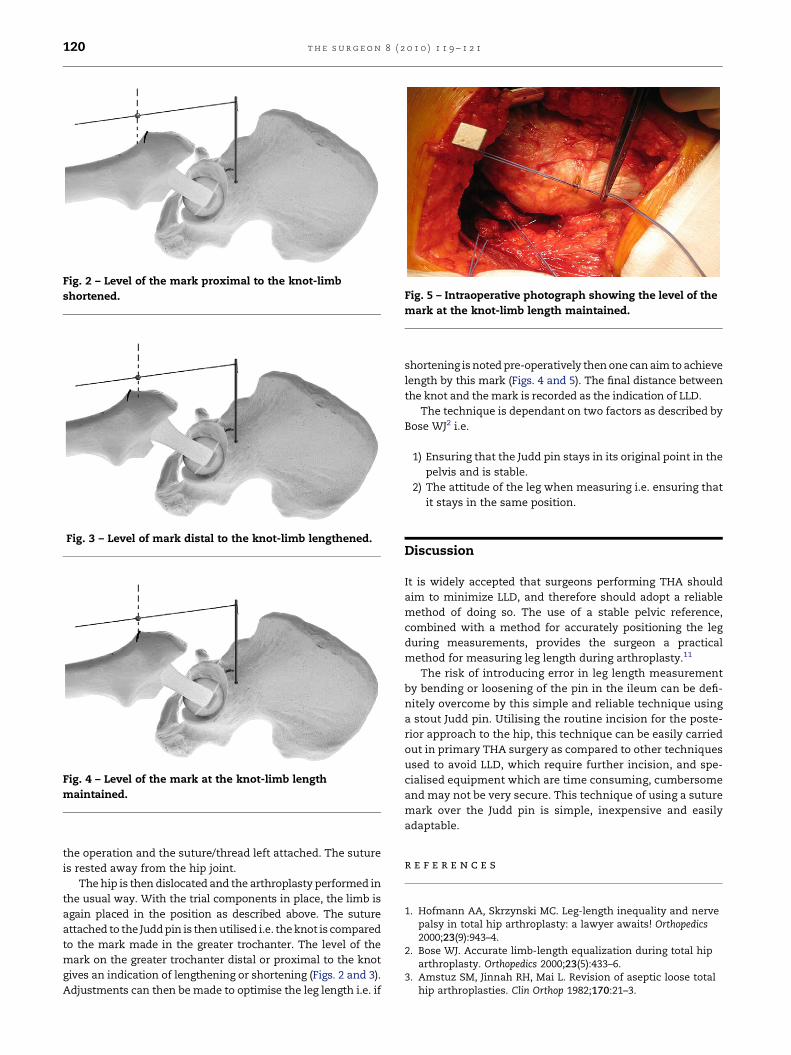
Fig. 2 – Level of the mark proximal to the knot-limb
shortened.
Fig. 3 – Level of mark distal to the knot-limb lengthened.
Fig. 4 – Level of the mark at the knot-limb length
maintained.
Fig. 5 – Intraoperative photograph showing the level of the
mark at the knot-limb length maintained.
t h e s u r g e o n 8 ( 2 0 1 0 ) 1 1 9 – 1 2 1120
the operation and the suture/thread left attached. The suture
is rested away from the hip joint.
The hip is then dislocated and the arthroplasty performed in
the usual way. With the trial components in place, the limb is
again placed in the position as described above. The suture
attached to the Judd pin is then utilised i.e. the knot is compared
to the mark made in the greater trochanter. The level of the
mark on the greater trochanter distal or proximal to the knot
gives an indication of lengthening or shortening (Figs. 2 and 3).
Adjustments can then be made to optimise the leg length i.e. if
shortening is noted pre-operatively then one can aim to achieve
length by this mark (Figs. 4 and 5). The final distance between
the knot and the mark is recorded as the indication of LLD.
The technique is dependant on two factors as described by
Bose WJ2 i.e.
1) Ensuring that the Judd pin stays in its original point in the
pelvis and is stable.
2) The attitude of the leg when measuring i.e. ensuring that
it stays in the same position.
Discussion
It is widely accepted that surgeons performing THA should
aim to minimize LLD, and therefore should adopt a reliable
method of doing so. The use of a stable pelvic reference,
combined with a method for accurately positioning the leg
during measurements, provides the surgeon a practical
method for measuring leg length during arthroplasty.11
The risk of introducing error in leg length measurement
by bending or loosening of the pin in the ileum can be defi-
nitely overcome by this simple and reliable technique using
a stout Judd pin. Utilising the routine incision for the poste-
rior approach to the hip, this technique can be easily carried
out in primary THA surgery as compared to other techniques
used to avoid LLD, which require further incision, and spe-
cialised equipment which are time consuming, cumbersome
and may not be very secure. This technique of using a suture
mark over the Judd pin is simple, inexpensive and easily
adaptable.
r e f e r e n c e s
1. Hofmann AA, Skrzynski MC. Leg-length inequality and nervepalsy in total hip arthroplasty: a lawyer awaits! Orthopedics2000;23(9):943–4.
2. Bose WJ. Accurate limb-length equalization during total hiparthroplasty. Orthopedics 2000;23(5):433–6.
3. Amstuz SM, Jinnah RH, Mai L. Revision of aseptic loose totalhip arthroplasties. Clin Orthop 1982;170:21–3.

t h e s u r g e o n 8 ( 2 0 1 0 ) 1 1 9 – 1 2 1 121
4. Charnley J. Low friction arthroplasty of the hip. Berlin, Germany:Springer-Verlag; 1979.
5. Mihalko WM, Phillips MJ, Krackow KA. Acute sciatic andfemoral neuritis following total hip arthroplasty: a case report.J Bone Joint Surg Am 2001;83:589–92.
6. Mcgee HMJ, Scott JHS. A simple method of obtaining equal leglength in total hip arthroplasty. Clin Orthop 1985;194:269–70.
7. Bal BS. A technique for comparison of leg lengths during totalhip replacement. Am J Orthop 1996;25:61–2.
8. Huddleston HD. An accurate method for measuring leg lengthand hip offset in hip arthroplasty. Orthopedics 1997;20:331–2.
9. Naito M, Ogata K, Asayama I. Intraoperative limb lengthmeasurement in total hip arthroplasty. Int Orthop 1999;23:31–3.
10. Takigami I, Itokazu M, Itoh Y, Matsumoto K, Yamamoto T,Shimizu K. Limb-length measurement in total hiparthroplasty using a calipers dual pin retractor. Bull NYU HospJt Dis 2008;66(2):107–10.
11. Clark CR, Huddleston HD, Schoch EP, Thomas BJ. Leg-lengthdiscrepancy after total hip arthroplasty. J Am Acad Orthop Surg2006;14:38–45.
Aravind Desai*, Bilal Barkatali, Asterios Dramis,
Timothy N. Board
Centre for Hip Surgery, Wrightington Hospital, Wigan, UK
*Correspondence to: Aravind Desai, 297 Lovely Lane,
Warrington WA5 0AF, UK. Tel.: þ44 07885994545;
fax: þ44 01257253853.
E-mail address: [email protected] (A. Desai)
Available online xxx
1479-666X/$ – see front matterª 2009 Royal College of Surgeons of Edinburgh (Scottish charity
number SC005317) and Royal College of Surgeons in Ireland.Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.surge.2009.10.023