Embed Size (px)
Citation preview

64 IRISH JOURNAL OF MEDICAL SCIENCE
A S T U D Y OF FOUR CASES OF A U R I C U L A R FLUTTER.*
By HENRY MOORE.
T H E clinical picture of auricular fibrillation is too well know~ to need description; on the other hand, auricular flutter, which is closely allied to fibrillation, is comparatively
rarely encountered.
The Nature of Aur icular F lu t t er and Aur icular Fibrillation.
The explanation of these conditions which is now most widely accepted is based on the circus movement theory, first proposed by Oarrey I and by Mines 2 and extensively studied and elaborated by the work of Lewis and his co-workers. 3 In the normal heart each beat originates in the sinu-auricular node and travel~ radially along all available paths in the auricular muscle until the whole auricular musculature is in contraction; when the contrac- tion reaches the limits of the auricular muscle it finds no fur ther available paths open to it in the auricles and it dies out therein. Lewis has demonstrated clearly that auricular flutter, on the contrary, is due to a " circus movement " in the auricle, namely, a continuous movement of the contraction wave in a ring of muscle such as that which surrounds the mouths of the superior and inferior venae cavae, or the mitral orifice. This revolving wave of contraction governs the movement of the auricle; it is inefficient as compared with the normal auricular systole; ther~ is no starting point, the wave moves continuously in a circular path and its crest follows its wake separated from the latter by a gap of responsive and temporarily uneontracted muscle. In different cases the wave may travel clockwise or anti-clockwise. From the outskirts of this central or mother wave, as Lewis calls it, centrifugal waves spread at each revolution into the more out- lying parts of the auricles and their appendages. I t is the central wave, however, which controls the movement. Auricular fibrilla- tion is also due to a circus movement, but the path of the wave is sinuous and varies in greater or lesser degree from cycle to cycle. The usual rate of the circus movement in flutter is abou~ 300 per minute, but in special circumstances it may fall as low as 150 or rise to 360 per minute. Flut ter may occur in paroxysms, appearing and disappearing abruptly, but, once established, it usually persists for months or years; the ventricle can rarely respond to every such circus movement in the auricle, and it generally responds to every alternate one---2 : 1 block ; the resulting ventricular tachycardia, however, is usually of a rate sufl~eiently high to cause circulatory embarrassment.
In experiment it can be shown that heart muscle is incapable of responding by contraction to the strongest stimulus during a
* From the Mater Misericordi~ Hospital, Dublin. Received for publi- cation Oct. 29th, 1927.

FOUR CASES OF AURICULAR FLUTTER 65
period beginning with its contraction and continuing until the contraction begins to subside--the absolute refractory period; during the succeeding phase of recovery the muscle will at first respond to strong stimuli (induction shocks) and later to weaker ones--the period of increasing excitability is known as the relative or partial refractory period. Neither the absolute nor partial refractory periods may be quite the same in 'adjacent muscle bundles; they may differ by very small fractions of a second.
In heart muscle responding to experiment to high rates of ~timulation, 300 to 480 per minute, the absolute refractory period becomes gradually increased, so that the muscle tends to respond only to every second stimulus. As Lewis described it, this half- rhythm is not assumed simultaneously by all fibres, and therefore islets of muscle may be irresponsive to a given stimulus; the excitation wave travelling through muscle in this state will be obstructed between given points (delayed conduction), and it may swerve from side to side in a more or less sinuous manner as it passes through the only channels which are open to it, viz., through the muscle bundles not in the refractory state. I t is necessary to understand these changes when considering auricular flutter and fibrillation, for here also we are dealing with muscle responding to high rates of stimulation. Vagus stimulation, on the other hand, shortens the refractory period in the auricle and for this reason quickens conduction therein.
In auricular flutter the central wave of contraction circulates in a practically constant path at a rate which is constant in a given ease, usually about 300 times per minute. In auricular fibrillation the rate is higher, about 450 per minute, and the circus movement is irregular, inasmuch as the same path is not followed from cycle to cycle; a single circus movement does exist but the path changes constantly in its details while following the same general direction. In flutter the gap of responsive muscle between the crest and wake of the circus movement is about one-fifth of the whole circle in which the wave moves; in auricular fibrillation the gap is shorter and the wave of contraction flows through muscle in which more numerous fibres are irrcsponsive. The close relation between flutter and fibrillation is shown by the fact that the former may pass into the latter under treatment.
Consider the circus movement in auricular flutter: the wave begins at one point, and moves continuously around a circular path; the crest of the wave of contraction is separated from its wake by a gap of muscle which is not yet contracting, but which, being in a state of only slight partial refractoriness, is ready to contract when the stimulus to do so (crest of circus movement) enters it.
I f the refractory period lengthens or the rate of propagation of the wave increases, the gap shortens; if the refractory period shortens or conduction decreases, the gap widens. I f the former changes are of sufficient magnitude that the gap disappears, the crest of the wave overtakes its wake and if then the muscle at the

66 I R I S H JOURNAL OF M E D I C A L S C I E N C E
wake of the wave remains a little longer in the re f rac tory state the circus movement comes to an end. When this happens in clinical aur icular f lut ter or fibrillation, the a r rhy thmia ceases and the dominant normal sinus rhy thm is restored.
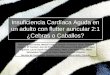
Fic. A. FIG. B. FIG. A.--Schematic representation of the central wave as it circulates in
auricular flutter. The blackened portion of the ring represents those portions which are refractory at a given instant. The crest of the wave travel~ through muscle in a slight state of jpartial refractoriness. The whole gap forms about one-sixth of the ring.
Fro. B.--A similar representation ~)f the wave in auricular fibrillation. The ring is smaller and the gap relatively shorter. The crest of the a~lvancing wave, and its wake, are deeply erenated. The wave is advancing through small and irregular channels of responsive tissue, as these open up deviously to receive it.
After Lewis: The Mechanis~ and Graphic Registration oJ the Heart Beat.
Act ion of Drugs on the Auricle. (1) Quinidine.4--This drug, by acting direct ly on the auricular
muscle, prolongs the effective re f rac tory per iod; it also slows con- duction and therefore the transmission intervals widen and the auricular rate slows. A priori, the lengthening of the effective re f rac tory period tends to close the gap of a circus movement and thus to br ing the circus movement to an end, whilst the slowing of conduction tends to have the opposite effect. I t is only when the action of quinidine in lengthening the effective re f rac tory period is greater than its action in slowing conduction that this drug is effective in abolishing clinical auricular fibrillation, and thus is explained the fact that quinidine is therapeutical ly efficient in only about 5 4 ~ of cases of aur icular fibrillation. In the instances in which it is not successful, its effect is probably more marked in slowing conduction (or the gap being shortened owing to increase in the effective re f rac tory period the circus movement is diverted into a longer path, where a sufficiently large gap for the main- tenance of the circus movement may persist).
Quinidine, also, par t ly (or completely in experiments) depresses vagus action (probably by acting on the nerve ganglia) and i t therefore acts indirect ly on the auricular muscle by increasing the effective re f rac tory period. These effects of quinidine are more in evidence in aur icular fibrillation than in flutter. There is also evidence that this drug may produce delay in in t ravent r icular conduction which is evidenced electroeardiographically by changes in the height, width, and form of the QRS complex (as illus- t ra ted in Case 2) and possibly by changes in the T Wave. 5.

FOUR CASES OF AURICULAR FLUTTER 67
(2) Digitalis.6--This drug, in full therapeutic doses, by increas- ing vagal tone, reduces the length of the refractory period and tends to increase the rate of conduction; therefore it usually increases the rate of the circus movement in auricular fibrillation. On the other hand, digitalis, by acting directly on the heart muscle, increases the length of the refractory period, and, when the heart muscle is responding rapidly, retards conduction and therefore tends to decrease the rate of the auricular oscillations. The predominant action of the drug seems to be through the ~'agus, because in practice the rate of the auricular oscillations in fibrillation is somewhat increased, as a rule. But, from the point of view of closure of the gap, these two actions are opposed to each other, and therefore the circus movement is rarely abQlished by digitalis action. Lewis showed that by the action of digitalis auricular flutter may be frequently converted into auricular fibrillation and that, if then the drug be discontinued, normal sinus rhythm will frequently, but not always, appear. I t m not fully understood how flutter may be converted into fibrilla- tion by the use of digitalis; the fundamental differences between flutter and fibrillation seem to be that in fibrillation the refractory period is less, the path of the circus movement shorter, the rate of the circus movement greater, and the gap smaller, than in flutter; if, now, the vagus action of digitalis is predominant in flutter, the refractory period is shortened, the conduction rate is increased, and the rate of the circus movement is increased; the gap may therefore become shorter; in other words, there is a shifting of all these properties in a direction which could, one would suppose, favour the conversion of flutter to fibrillation. ~
The treatment of auricular fibrillation with quinidine or digitalis is fairly well understood and comparatively sucessfully employed, but, since flutter is relatively rare, reports of the treat- ment of the latter condition are not numerous. There seems to be a fairly common belief that quinidine administration should not follow the exhibition of digitalis without allowing an interval to elapse, but it is not easy to discern any reason why one should wait until the digitalis effect has worn off---indeed the argument seems to be the other way. Viko, Marvin and White, 7 in 1923, concluded from a study of seventy-one cases of chronic auricula~ fibrillation and four cases of chronic auricular flutter that all such cases showing objective cardiac failure should probably b(: digitalised before beginning quinidine treatment. Gordon s records two cases of auricular flutter in which quinidine followed digitalis treatment with good results. Wedd 9 reports that normal rhythm was restored by quinidine in three of six cases of auricular flutter, and Gallavardin 10 restored normal rhythm by quinidine in two cases in which digitalis was unsuccessful. Wedd n states that in three of four cases of auricular flutter fibrillation produced by digitalis persisted, and in one of these quinidine failed to produce normal rhythm; he suggests digitalis followed by quini- dine in the treatment of flutter. Detailed study of the treatmen~

68 I R I S H J O U R N A L O F M E D I C A L S C I E N C E
of f l u t t e r w i t h d i g i t a l i s f o l l o w e d b y q u i n i d i n e does n o t s e e m to be r e c o r d e d i n t h e l i t e r a t u r e .
I n th i s p a p e r a r e r e c o r d e d f o u r cases o f a u r i c u l a r f l u t t e r w h i c h m a y be of i n t e r e s t i n c o n n e c t i o n w i t h t h e f o r e g o i n g c o n s i d e r a t i o n s .
CAs~ 1 . - - I t was not possible to study this case in detail. Clergyman, age 69 years. Seen J u l y 9, 1923. He igh t 6 feet 2 inches. Family history and previous history not relevant .
Complaint.--Palpitation and rapid pulse ra te for 2 years previously, some breathlessness on modera te exer t ion ; feet and ankles became swollen towards evening; the pat ient , however, s tated tha t he was not great ly restr ic ted in his activities and could a t tend to his duties fairly efficiently.
Physical E~camination: Radia l and brachial ar tery walls s l ightly th ickened; re t inal ar ter ies ~ppeared normal ; hear t slightly enlarged to the left by palpitat ion and percussion. Pulse ra te varied from 108 to 120; the pauses between the beats were often somewhat unequal, but the beats were of equal s t rength. Blood pressure 180/80. The ur ine contained a t race of albumen, occasional g ranu la r casts, calcium oxala te crystals and �9 z few white and red blood cells. The pros t ra te was somewhat enlarged. There were no o ther abnormali t ies on clinical examinat ion . An electro- cardiogram * showed aur icular f lut ter with 2 : 1 to 3 : 1 block (Fie . 1). Pressure over the vagi did not slow the pulse.
Treatment.--The pa t i en t received 1 g ram of d ig ipura tum and 13�89 grains of powdered digital is leaves over 4 days; on the th i rd day the pulse ra te began to dr(~p, and on the fourth was about 70 per minute. An electro- cardiogram then showed tha t auricular f lut ter still persisted, but tha t the degree of block had increased to 4 : 1, g iv ing a pulse ra te of about 70; the blood pressure was 186/100. Tinct. Digitalis , (m. xxx. per day), by mouth, sufficed to keep the ven t r icu la r ra te the rea f te r about 70 per minute . The pa t i en t was advised to take the 30 minim doses of Tinct. Digi ta l is per day and given suitable instructions in relation to work, diet , and exercise; he was discharged on the unders tanding tha t he was to r~port from t ime to time. He was not again .seen for a year, unti l Ju ly 24th, 1924, when I was called to Vhe country to ex~amine h im; he was found to be suffering f rom mental confusion with some cerebral exc i tement ; the axillary tempera ture was 100 o F. , but otherwise physical examinat ion was in general nega t ive ; he was stil l taking the digitalis as prescribed, and his pulse was regular (76 per minute) . The blood pressure w.as 200/110. I t was not possible to ge~ a polygraph t rac ing. He was pu t on a salt-poor diet . and he made a complete recovery in a few weeks. He paid a flying visi t in May, 1925, and ajppeared t o ' b e in good health, with pulse ra te 76 anal regular, blood pressure 176/100, and hear t onIy slightly enlarged to the left. He was stil l t ak ing digitalis . He was advised to come for e lectrocardiographic examination, but did not do so unti l ,~eptember 5th, 1925 ; a t tha t t ime the pulse ra te was regular a t 74 per minute, blood pressure 172/102, Vhe hear t sl ightly enlarged to ~he lef t ; he looked and fel t well and was able to oarry on his work a t a s l ightly reduced level in comfort. The electrocardiogram showed sinus rhy thm (the flutter having disappeared) with spl inter ing of QRS in Lead I I I . (plate accidentally destroyed), l i e was advised to disc, ontinud the digitalis, which he was still taking, l i e reported himself on Jan . 10th, 1926, and was found to be in goott heal th and fairly active ; the pulse ra te was 74 an.d regular, l i e refused electrocardiegraphie examination.
l i e re turned again on May 30, 1927; he stated tha t he was comparat ively well and was able to walk, a t a moderate rate, from 4 to 6 miles per day, and to carry out his duties fair ly efficiently. For the last three weeks he noticed tha t his pulse was sl ightly i r r egu la r ; this, however, did not cause him any inconvenience. His blood pressure was 170/110 and pulse ra te 102. The impulse bea t was 12.5 cms. from the middle l ine in the fifth space. Tl~e radial ar tery ~ alls were normal or very slightly thickened. The pulse , /as stigh~ly i r regular in ra te and perhaps in force. Electrocardiographic examinat ion showed auricular flutter with 4:1 block, otherwise the electro- cardiogram was normal. He had not used salt for almost three years. In view of the fact tha t ~he circulation seemed to be fairly efficient, t h a t there was a 4:1 block, and also because of his age and of the possibility of
�9 Time marker shows fifths and twenty-fifths of a second ; one excursion of s t r ing is equal to one millivolt. The tracings are reduced for publication.


. . . .
~ 3 , ' .
i ~ I Z ~ ~ .
�9 ~-~i ~. ~a,~.~1i~ ~ ~ ~

F O U R C A S E S O F A U R I C U L A R F L U T T E R 69
intra-auricular thrombi, it was decided not to attempt to abolish tile flutter. He was accordingly advised to take Tinct. Digitalis (m. xxii.) once a day.
This patient was again seen on Au~. 20, 1927, ~hen the blood pressure was 156/92, the impulse beat was 13.5 cms. from the middle line, and the pulse rate was 74 and regular; he had given up taking digitalis for two weeks previously. The electrocardiogram revealed auricular flutter with a 4:1 ventricular response (Fro. 2). He stated that he felt well, could attend to his work, and take a moderate amount of exercise without inconvenience.
He returned again on Oct. 4, 1927, complaining of slight breathlessness on exertion. Now, the electrocardiogram (FIG. 3) showed flutter with 2 : 1 to 3 : 1 block, and the pulse rate wasabout 108 and slightly irregular ; he had taken no digitalis for about eight weeks. The blood pressure (auscultatory method) was 170/90; it was noticed that only half the beats came through to the wrist, or were audible over the brachial artery, from 170 to 120 mm. (luring decompression of the armlet of the sphygTnomanometer, but all came through from 120 to 90 ram. Because these features seemed to indicate a doubtful prognosis and because of the aDparent escape of ~he auro-ventricular node from digitalis control with consequent increased ventricular rate, the patient was again put on Tinct. Digitalis, (m. xxvii. per day. When seen on Oct. 27, 1927, he was still taking digitalis as pre= scribed, the pulse rata was 86 per minute, and his only complaint was very slight ~areathlessness on moderate exertion and consciousness of his heart- beat when lying on his left side; he stated that he felt improved; the electrocardiogram (FI~. 4) showed flutter with 3:1 to 5:1 block (occasion- ally 2 : 1) ; the pulse rate was 90 and slightly irregular ; the blood pressure was 152/90, all beats coming through to the wrist at 152 mm. Hg.
Comment on Case 1 . - - I t is unprof i t ab le i n this case to speculate as to when or how, in the first ins tance, a m @ u l a r f lu t te r gave place to s inus r h y t h m as the obse rva t i ons were of necess i ty so i n f r e q u e n t a n d imperfec t . I t is i n t e re s t ing to no te the relapse to f lu t te r which a p p a r e n t l y occurred a f t e r an i n t e rva l of almost two years, as f a r as one can j u d g e f rom the his tory. F i n a l t r e a t me n t d i rec ted towards the abol i t ion of f lu t t e r a n d the res tora t ion of s inus r h y t h m (by d ig i ta l i s followed by q u i n i d i n e as described later) was considered unwise in this pa t ien t , owing to the possibi l i ty o~ the p re sence of i n t r a - a u r i c u l a r t h r o m b i which m i g h t become detached if s inus r h y t h m were induced , the age of the pa t i en t and the l ikelihood of progressive degenera t ive myoca rd ina l change; moreover, the efficiency of the c i rcu la t ion was qui te good when digi ta l is was g iven in such da i ly doses tha t 3 : 1 to 4 : 1 aur iculo- v e n t r i c u l a r block was m a i n t a i n e d even while a u r i c u l a r f lu t te r cont inued . I t is of in te res t to note the presence of f lu t te r at a c o m p a r a t i v e l y a d v a n c e d a g e - - ( f l u t t e r was las t observed w h e n the p a t i e n t was 73 yea r s o l d ) - - e s p e c i a l l y as the consequen t h e a r t f a i l u r e was eas i ly con t ro l l ed b y digi ta l i s .*
*This patient returned on Dec. 5, 1927; he was still taking digitalis (m. xxvii, per day); the blood pressure was 172/84, pulse rate 76 and regular, and impulse beat about 11 cms. from the middle line. The electro- cardiogram showed sinus rhythm (Fig. 4a). A few days after his previous examination (Oct. 27, 1927) he became aware that the slight breathlessness on exertion had disappeared, and that ~he was no longer aware of the beating of his heart when lying on his left side, as he had been for some months before. When flutter disappeared cannot be stated, but it was present on October 27, and it was no lon~er present on November 5,
T 1927. ~ h y flutter disappeared cannot be stated, but it is highly probable that its abolition was due to digitalis action. How flutter vanished and whether there was an intermediate stage of fibrillation it is impossible to say. Apparently our fear Vhat the inducing of sinus rhythm might cause detachment of auricular thrombi in this case was groundless.

70 1 R I S H J O U R N A L O F M E D I C A L S C I E N C E
CAs~ 2 . - - A farmer , aged 39 years, consul ted me on Dee. 15th, 1925. H e was 6 feet 1�89 inches in h e i g h t and weighed 240 lbs. I-Ie complained of f lu t te r ing in hi.s chest and dyspncea on s l ight exer t ion .
P r e v i o u s H i s f o T y . - - M e a s l e s and m u m p s in chi ldhood; typhoid fever when 18 years o ld ; gonorrhoea 12 years ago. Bo th knees became swollen and pa in fu l 9 years ago, and t h e r e was also s l igh t swelling of t h e ankles ; he recovered a f t e r abou t 10 days in bed ; does no t know whe the r he had a r ise of t e m p e r a t u r e ; his tonsi ls were removed 10 m o n t h s l a t e r a l t hough he was never subjec t to sore t h r o a t .
P r e s e n t ] l l n e s s . - - O n December 1st, 1925, he not iced dyspn0ea, pa lp i ta - t ion a~d t achycard ia on s l ight exer t ion , bu t these syml)toms d isappeared on r e s t i n g ; since t h e n the same symptoms have recurred several t imes, somet imes while res t ing , bu t were especial ly p rone to a p p e a r a f t e r break- fast , or on exer t ion . I saw h im for t he first t ime in an a t t a c k which had a p p a r e n t l y pers i s ted for a t leas t 6 days.
P h y s i c a l E x a m i n a t i o n . - - F a c e slightl~y cyanoLic, s l ight oedema of legs, h e a r t seemed somewhat en la rged to the left, bu t was difficult to map ou t (full ches t ) . No cardiac m u r m u r s . Pu l se and hea r t - r a t e about 172 per m i n u t e and regular . L iver and spleen no t palpable. Lungs normal . Blood pressure 112/90. Blood W ~ s s e r m a n n react ion negat ive . The electrocar- d iogram showed a u r i c u l a r f lu t te r , w i th 2 : 1 block (Fig. 5). P re s su re over vagi or on eyeballs did no t slow t he pulse. U r i n e normal .
Cou~'se a n d Y r e a t m e n t . - - I t was decided to t ry the effect of quinidine sulphat~ by mou th a f t e r the admin i s t r a t i on of 0.4 g ram had shown t h a t t he p a t i e n t d id no t have an idiosyncracy for t he drug. F o u r t e e n and e i g h t - t e n t h g rams of qu in id ine su lpha te were g iven by m o u t h in doses of 0.4 g r am f rom Dec. 18th to 24th as f o l l o w s : - -
Doer. 18th . . . . . . . . . . . . I x 0.4 0.4 gram. ., 19th . . . . . . . . . . . . 4 x 0 . 4 1.6 ,, ,. 20th . . . . . . . . . . . . 5 x 0.4 2.0 ,, :, 21st . . . . . . . . . . . . 13• 0.4 5.2 ,, ,, 22nd . . . . . . . . . . . . 6 x 0.4 2.4 ,, ,. 23rd . . . . . . . . . . . . 5 x 0.4 2.0 ,, ,, 24th . . . . . . . . . . . . 3 x 0.4 1.2 ,,
Total 14.8 grams.
Af te r 9.2 g rams of t~he d r u g had been t aken (Dec. 21) the f lu t te r waves became increased in l eng th , a p p a r e n t l y due to slower au r i cu la r con- duct ion, and t h e i r r a t e was slower t h a n on admiss ion (Fig. 6). Af te r 11.6 granm of quinidine (Dec. 22) these changes in the f lu t te r waves were still marked , and t h e QRS complex in add i t i on to showing a va ry ing vol tage also man i fe s t ed abe r r a t i on in many beats ( in ter ference wi th the spread of t h e exc i ta t ion wave t h r o u g h t he ventr ic le) ; nmreover, t h e r e seemed to be a tendency on the p a r t of t im ventr ic le to respond mere f requen t ly to t h e indiv idual f lu t te r waves (Fig. 7). Ev iden t ly these electrocardiogral~hic changes were evidences of the toxic act ion of quinidine on the conduct ion- genet ic sys tem. The pa t i en t , whose clinical ,condition was qui te unchanged and who was fa i r ly comfor table while re~ting~ then decided aga ins t advice to go home for Chr i s tmas .
He was r e -admi t t ed on J a n u a r y 6th, 1926. His clinical condition was abou t the same as on the f i rs t admission, and t he e lect rocardiogram again showed aur icu la r f lu t ter , w i th 2:1 block. I t was now decided to t ry tbe effect of digi ta l is . The p repa ra t i on used was D ig ipu ra tum (Knoll) by m o u t h in t a b l e t form. Prev ious exiperienc~ has shown t h a t full clinical d ig i ta l i sa t ion in aur icu la r f ibri l lat ion is near ly always ob ta ined wi th digi- p u r a t u m by the adm i n i s t r a t i on by m o u t h of 1 g ram to a p a t i e n t of average weight. One and one - t en th g rams had been given by m o u t h in divided doses over t h r ee days when t he a r r h y t h m i a suddenly changed from aur i - cular f lu t te r to aur icu la r f ibri l lat ion, the pulse a n d hea r t r a t e dropping ~o abou t 82 pe r m i n u t e and be ing fai r ly regu la r (Fig. 8). The p a t i e n t now found t h a t he could u n d e r t a k e modera te exercise wi th comfort , t i e t hen ( J an . 10th) again ins is ted on leaving the hospi ta l to t r a n s a c t some u r g e n t business , no t t a k i n g digi ta l is .
l i e r e t u r n e d on J a n . 20th, 1926, in t he same condi t ion as on t he first occasion, and t h e e l ec t roca rd iogram showed au r i cu l a r f lu t te r , wi th 2 : 1 block. On J a n . 21st and 22nd he received 1 g r a m ( to ta l dosage) of d ig ipu- r a t u m in d iv ided doses, and shor t ly a f t e r t he las t dose au r i cu la r f ibr i l la t ion


~ ; {~7 ~ ; ~x ~;'~4~ ~ , ,~ ~ ~ 4
Z ~

F O U R C A S E S O F A U R I C U L A R F L U T T E R 71
appeared again. As he aga in wished to leave hospi ta l , we decided to endeavour to induce i~he r e t u r n of the normal r h y t h m wi th qu in id ine ; con- sequent ly, a f te r wai t ing in vain for 24 hours in t h e hope t h a t on the c~s- sat io~ of t he d i g i p u r a t u m t r e a t m e n t the normal r h y t h m would ~ppear, 2.4 g rams of q u i n i d i n e su lpha te were g iven in doses of 0.4 g r a m every second hour . An e lec t roca rd iogram t a k e n one hour a f t e r t h e las t dose showed a no rma l s inus r h y t h m (Fig. 9). The p a t i e n t now fe l t qu i te comfortable , even on considerable exer t ion , and lef t hospi ta l ( Jan . 26th) w i th a no rma l cardiac r h y t h m , pulse and h e a r t r a t e about 89 and blood pressure 124176. He r e t u r n e d on Feb. 13th and Apr i l 21st for e x a m i n a t i o n and electro- ca rd iogram, and was in every respect normal .
On Augus t 10th, 1926, the p a t i e n t was once more admi t t ed suffering f rom a n attacl~ of au r i cu la r f lu t te r which had commenced 10 days previously, wi th t he signs and symptoms prac t ica l ly t he same as on the first occasion. The e l ec t roca rd iogram (Fig. 10) showed aur icu la r f lut ter , t h e block vary- iag th i s t ime f rom 2 : 1 to 4 :1 .
D i g i p u r a t u m (0.8 :~n.) caused no change in the e lec t rocardiogram; a f t e r 24 hours ' i n t e rva l quinidine was s t a r t e d ; 4.8 g rams of the l a t t e r d rug were given over a period of two days, when the e lect rocardiogram again showed l eng then ing and d iminished vol tage of t he f lu t ter waves (2:1 block) wi th somet imes s l ight abe r r a t i on (Fig. 11). The quinidine was t hen stopped. I n 24 hours the f lu t te r waves were of the same type as on admission wi th 2:1 to 4:1 block ~Fig. 12). Af te r two days in te rva l (f lut ter still p r e sen t ) , i t was decided to push digi tal is in the hope of again inducing aur icular f ibri l lat ion, and 2.1 g rams of di~gipuratum w e ~ given over 4 days. One hou r a f t e r the las t dose of ~he 2.1 g rams of d ig ipu ra tum the pulse r a t e suddenly fell to abou t 70 per ln inu te and t he e lectrocardiogram sh~wed aur icu la r f ibri l lat ion (Fig. 13). No d rug w~s given now for 48 hours in t he hope t h a t on t he wi thdrawal of d igi ta l is aur icu lar fibril lation would give place to normal r h y t h m ; as ~his d id not occur, f ibri l lat ion pers i s t ing (Fig. 14), 2.4 g rams of quinidine su lpha te were given in divided doses of 0.4 gr~m every two h o u r s ; abou t one and a half hour a f te r the las t dose an e lec t rocard iogram showed normal s inus r h y t h m wi~h a pulse r a t e and h e a r t r a t e of 76 (Fig. 15). The p a t i e n t was d i scha rg~ l in a few days wi th a normal r h y t h m L f e e l i n g qui te well even a f t e r madera te exercise; he was advised to t ake Tinct . Dig i ta l i s (m. x i v . , t w i c e daily). As the h e a r t was normal 10 days la te r th is dose was changed to m. xvi. once daily. He was nex t seen th ree m o n t h s l a t e r ; as the h e a r t was still normal , and as no f u r t h e r a t t acks ~had t roubled him in the mean t ime , the dose was fu r the r reduced to an. xii. pe r day. The digi ta l is was completely stopped a mon th af te rwards . He repor ted for examina t ion on J a n . 28th, 1927, hav ing h a d no d ig i ta l i s for abou t a m o n t h previously ; t h e h e a r t was normal on physical examinat ion , apparen t ly no t enlarged, and ~he electrocardiogranl showed no rma l sinus r h y t h m ; blood pressure 124/80 and pulse r a t e 64; he had exper ienced no f u r t h e r a t t acks , and was l iv ing a no rma l life.
On May 26th, 1927, the p a t i e n t r e tu rned once more complaining Vhat his h e a r t t roub le h~d suddenly developed on May 25th a t about 9 p.m. Be- tween the onse t of t he a t t ack and his vLsit he had t a k e n one g ram of digi- p u r a t u m by mouth . The blood pressure wa~ 120/80, the cardiac dulness ex t ended abou t 11 cms. f rom t he middle l ine. He compla ined of some dyspn~ea on exe r t i on , and t h a t he was conscious of his h e a r t b e a t i n g rap id ly and abnormal ly even a t rest . The pulse r a t e wa~s 140 pe r m i n u t e and s l ight ly i r r egu la r . The e lec t rocard iogram showed aur i - cu lar f lu t te r wi th 2:1 to 3:1 h e a r t block. He received 3.6 gram~ of digi- p u r a t u m ( to ta l dosage) be tween t he onse t of th i s a t t ack of f lu t te r on May 26th and t h e appearance of aur icu la r f ibri l lat ion on May 30th. The elec- t roca rd iogram on May 30 a t 2 p .m. st i l l showed aur icular f lu t ter wi th 4:1 hea r t block p redomina t ing and pulse r a t e 76. The final dose of d i g i p u r a t u m (0.1 gin.) was given a t 2 p.m. May 30th, and a t 5 p.m. on t he same day he said t h a t he noticed some change in t he ~ea r t b e a t ; he was electrocar- d iog raphed a t 6.40 p.m., and th i s e l ec t roca rd iogram showed au r i cu la r fibril- l a t ion wi th a pulse r a t e of 68. I t is to be noted t h a t in t h i s a t t a c k a large dose of d ig i ta l i s was necessary to induce au r i cu la r f ibr i l la t ion. The fibril- l a t i on pers i s ted wi th a s l ight ly inc reas ing pulse r a t e up to 6.30 p.m. o a May 31st. On J u n e 1st ( f ibr i l la t ion sti l l p resen t ) he was g iven qu in id ine (0.4 gin.) a t 6 a .m. , a t 8 a.m. and a t 10 a.m. ( total 1.2 gm.) ; about U a.m. he noticed a s l ight pa lp i ta t ion , and t hen said Vhat he fe l t his pulse h a d become s teady and t h a t he was .~o longer conscious of abnormal beat-

72 I R I S H J O U R N A L OF M E D I C A L S C I E N C E
ing of the heart. He was electrocardiographed at 12 noon on the same day ; the tracing showed normal sinus rhythm with a pulse rate of 84. The blood pressure then was 122/74, and the cardiac dulness extended about 11 eros. from the middle line in the sixth space. He was discharged that after- noon, as he had urgent business, on small doses of Tinct. Digitalis (12 m. xii. once daily). During his last stay in hospital a careful search was made for s~ptic loci; the only positive finding was by rontgenographic examina- tion of the teeth carried out by Dr. J. A. Ger~ghty, which revealed an abcess around the posterior root of the first right upper molar tooth; the tooth was extracted. On Oct. 1, 1927, 3he reported that he was still well. He discontinued the digitalis in the first week of October, 1927.
He returned to hospital on Nov. 17th with a pulse rate of 140, blood pressure 104/82, dyspncea on slight exertion and auricular flutter (2:1 block) ; apparently from the history, flutter had re-appeared on Nov. 7th. On Nov. 18th at 2.30 p.m. he had received 1.2 gram of digipuratum and the electrocardiogram showed flutter with 3:1 to 8:1 block; at 3 ..p.m. he got 0.4 gram digipuratum (tetal 1.6 gram), and at 6.15 p.m. on Vhe same day there was auricuiar fibriliation present. Next day, at 7.30 a.m., auricular fibrillation was ~till shown in the electrocardiogram, and 1.2 gram. of quini- dine was subsequently given in divided doses; at 11.30 a.m. the patient noticed some vague changes in his heart beat; at 11.42 a.m. the electro- cardiogram showed sinus rhythm with pulse rate of 82 and blood pressure of 118-80; he was discharged feeling quite normal and directed to take Tinct. Digitalis (m. xxii. per day).*
Comment on Case 2.--This case apparent ly illustrates toxic effects of moderate doses of quinidine on the myocardium in auricular f lu t ter - -as evidenced by the electrocardiograms, viz., (a) delayed interauricular conduction and slowing of the rate of the auricular (flutter) circus movement; (b) ventrieular aber- ration. These changes were taken as showing that fu r the r quinindine dosage might not be safe, and the drug was discon- tinued. Quinidine alone proved ineffective in abolishing auricular flutter. Digitalis alone in adequate dosage caused flutter to be replaced by auricular fibrillation, but flutter reappeared later on cessation of digitalis treatment. When auricular fibrillation replaced flutter as a result of giving sufficient digitalis, a small amount of quinidine was sufficient to cause a re turn of normal sinus r h y t h m in a few hours wi thout any toxic signs appear- ing in the cardiogram. F lu t t e r reappeared after an interval of something over seven months, and normal rhythm was restored by digitalis followed by quinidine, as on the first occasion (quinidine alone, not preceded by digitalis, failing). Once again, af ter a fur ther interval of ahnost ten months, flutter again occurred, and on this occasion a large dose of digitalis was required to t ransform the ar rhythmia to fibrillation, but when this was accomplished a small dose of quinidine was sufficient to restore sinus rhythm. Finally, af ter something over seven months, he discontinued the digitalis, and after about five weeks flutter recurred; on this occasion digitalis caused flutter to be replaced by fibrillation in twenty-eight hours and subsequently small doses of quinidine succeeded in replacing the lat ter by normal sinus rhythm. Thus, four attacks of flutter occurred in two years, and each attack yielded to digitalis followed by quini- dine.
* This patient has remained well up to Jan. 8th, 1928, when the proofs of this paper were corrected.

FOUR CASES OF AURICULAR FLUTTER 73
CAS~ No. 3 . - - t tousewi fe , age 50 years, seen on Decr. 13th, 1926, com- p l a in ing of p a l p i t a t i o n and breathlessness on exer t ion . Fami ly h i s to ry no t re levant .
Previo.vz history.--Measles and scar let fever in chi ldhood; " in f l amma- t ion of the t h r o a t " 20 years ago; since t h e n f r e q u e n t " sore t h r o a t s " ; ~er i - ton t i l l a r abscess opened 3 years ago ; f r equen t a t t a cks of acu te rh in i t i s and b ronch i t i s ; varicose veins in legs; all t e e t h extradited 4 years ago. Two chiMren born dead a t full t e r m ; no l iving children. Venerea l disease denied.
Comp~aint.--Dyspnoea and p a l p i t a t i o n on s l ight exer t ion . Present illness.--A year ago when r u n n i n g she got an a t t a c k of " pa lp i -
t a t i o n , " accompanied by dyspncea. Since then she go t several s imi lar a t t acks on exer t ion. I n October, 1926, she had acute bronchi t i s accom- panied by pa lp i t a t ion and dyspncea. She apparent ly recovered f rom t h e bronchi t is , bu t t he pa lp i t a t ion became progressively worse on exer t ion, and recent ly appeared on even s l ight physical effort.
Physical Examination.--Pulse 166, r esp i ra t ions 26, pe r minu te . Tempe ra tu r e (mouth) 98.8 ~ F. ]~he pulse w~s regular wi th occasional dropped beats , and all cardiac systoles gave rise to a pulse a t t he wrist . The face, hands and fee t were eyanosed, and the re was modera te dyspncea a t rest . The tonsi ls , submaxi l la ry lymph-glands and the superficial cer- vical g lands a long the r i g h t s t e rnomas to id were enlarged. S ib i lan t rhonchi were hea rd diffusely over the lungs and crep i ta t ions a t the bases ; t h e r e was impaired resonance and feeble b r e a t h sounds over bo th b~ses. The ~oa r t was en la rged to t he left , the impulse be ing in t he 5 th in tercos ta l space 11.5 cms. f rom t he middle l ine ; a mi t r a l systolic m u r m u r was heard over t he apex and t r a n s m i t t e d to the lef t axi l la ; t he re was s l ight accentua- t ion of the aor t ic second sound. There was s l ight r of t he shins and ankles . The abdomina l reflexes were absent . The blood pressure was 190/140. The r i g h t lobe of the thyro id g land was sl ightly and uniformly enlarged, firm, and could be pa lpa ted by L ahey ' s " dislocat ion " me,hod : t he re was a fine t r emor of the hands ( r a t e abou t 4 to 6 per second). The ur ine conta ined no a lbumen, sugar or cashs. The p a t i e n t was freely cough- ing up a modera te a m o u n t of mucoid sputum. There were no o ther abnor- mal i t ies on clinical examinat ion . Blood c h e m i s t r y : Urea n i t rogen 11.6 rag., non-pro te in n i t rogen 20 rag., uric-acid 3 rag., and c rea t in in 1.4 rag., pe r 100 c.c. of blood. Urea concen t ra t ion t e s t no rmal (2 .3%). F ixa t ion of specific g rav i ty a n d wa~er excre t ion testis ind ica ted some kidney de- ficiency. A provis ional d iagnosis was made of aur icu la r f lu t te r (or less l ikely paroxysmal t achyca rd ia ) , myocardia l fai lure, mi t r a l incompetence, chronic bronchi t i s and congest ion of the bases of the lungs. The Wasser- ~nann reac t ion was s t rongly posi t ive in t he blood b u t negat ive in t he eerebro-spinal fluid. An e lec t rocardiogram showed aur icu lar f lu t ter wi th 2 : 1 to 3 : 1 block (Fig 16). I t was discovered t h a t t he p a t i e n t had been h a v i n g Tinct . Dig i ta l i s (m. v. t h r i c e daily) for some weeks previously Af t e r t he t achycard ia thad been successfully t r ea t ed the basal metabolic r a t e was found ~o be + 3 2 % ; t h e r e were no hype r thy ro id eye s igns ; and i t was con- e luded t h a t the r i g h t thy ro id lobe probably c~nta ined a " toxic adenoma ." P re s su re over t he vagi or eyeballs d id no t slow the pulse.
Treatment.--Digipuratum was admin i s te red , by mouth , commencing on December 13th a t 10.12 a.m., s t a r t i n g wi th 0.4 g r am in one dose as a n in i t ia l dose, and cc~atinued a t in t e rva l s of f rom one to two hours wi th smal ler doses un t i l December 14th a t 1 a.m., when the las t dose was given ; t he p a t i e n t received in all 1.6 g r am of t he drug. T, he pulse r a t e r emained about 160 un t i l 1.30 a.m. on December 14th, when i t fell to about 68 and was s l ight ly i r regular . An e lec t rocard iogram t a k e n on December 14th a t 11.80 p.m. showed aur i cu la r f ibr i l la t ion (Fig. 17), t he pulse r a t e a t t h i s t ime being a round 90 per minu te . Several e lec t rocardiograms were ~here- a f t e r t a k e n on Deer. 15th and Decr. 16th which showed, general ly , an in- c reas ing ven t r i cu la r r a t e and aur icu la r f ibri l lat ion (Fig. 18, Dec. 15th) . I t was decided to endeavour to abolish the f ibri l lat ion and induce t he re- t u r n of ~inus r h y t h m by t he adm i n i s t r a t i on of quinidine. Accordingly, quinidine su lpha te (0.2 gin . ) was given orally a t 12.10 p.m. on Decr. 15 th ; as the re were ,no signs of idiosyncrasy, 0.4 g r a m was given a t 3 p.m., 0.4 g ram a t 4 p.m., and 0.4 g ram a t 5.30 p.m. on the same day. At 6.5 p.m. an electrocardiogran~ slmwed t h a t sinus r h y t h m had ajppeared wi th occa- sional ven t r i cu la r ext rasys to les (Fig. 19). Six hours la~er the ext rasys- toles became more f requent (about. 1 iu 5). F ig 20 shows an electrocardio-

74 I R I S H J O U R N A L O F M E D I C A L S C I E N C E
g r a m t a k e n th ree days la te r (Dec. 18th) ; i t shows s inus r h y t h m wi th one ven t r i cu la r ex t rasys to le giving a r e t rog rade inver ted P wave ind ica t ing r e t r o g r a d e conduc t ion f rom ven t r i c le to auricle. The pulse r a t e abou t th i s t ime var ied from 86 to 106 per minu te . A few hours a f te r the appear- ance of aur icu la r f ibri l lat ion and slowing of the ven t r i cu la r ra te , t he cyanosis and dyspncea disappeared, a l i t t le l a te r t he (edema van ished and the congest ion of the pu lmonary base,s showed signs of c lear ing u p ; two days l a t e r the latter" had completely disappeared, and on D e ~ m b e r 19th the pa t i en t was able to walk about the ward wi thou t discomfort . (The p a t i e n t was k~pt in bed d u r i n g the ac t ive t r e a t m e n t . )
Up to J u n e 1st, 1927, the re was no r e t u r n of f lut ter , bu t ex t rasys te les were present , ra l lying f rom 1 in 3 to 1 in 10 (Fig. 21) ; t he p a t i e n t fe l t well and was able to take modera te exercise w i thou t diseonlfort . Ant i - ~yphilitic, and indeed any form of t r e a t m e n t , was refused.
On J u n e 17th, 1927, the p a t i e n t r e tu rned again complaining of dyspn0ea and p a l p i t a t i o n ; t h e r e w,~s cyanosis, s l igh t cedema of the feet and copious muco-pm'ulent s p u t u m ; sonorous and s ib i lant rhonchi were heard over the lower lobes of bo th lungs, the resonance of which was d iminished on por- cus~sion ; tem,perature 97 ~ F. (axil la) , respi ra t ion 26 and pulse r a t e 150 aald r e g u l a r ; a m i t r a l systolic h igh-p i tched blowing m u r m u r was heard , t r a n s - mi t t ed to the axil la ; V'he cardiac impulse was located in t he 5 th in te rcos ta l space 13 cms. f rom the middle line. The p a t i e n t was not iceably drowsy and apa the t ic . The blood pressure was 102/78. The e lec t rocard iogram showed aur icu la r f lu t te r wi th 2:1 block (Fig. 22). F r o m 9.20 p.m. on J u n e ][7th to 12.30 p.m. on J u n e 19th the pa t i en t received 2.1 g r am digi- pure ' turn by mou th in divided doses, b u t owing to oocasional vomit ing, which began 20 m i n u t e s a f te r t he f irst dose and cont inued i r regular ly t h r o u g h o u t the adm i n i s t r a t i on of the d ig ipu ra tnm, i t is impossible to know how much of the d rug was absorbed. Dur ing th i s period the pulse r a t e g radua l ly slowed down ; a t 12.30 tp.m. on J u n e 19th i t was fair ly s teady a t 70 per m i n u t e and t he e l ec t roca rd iogram showed f lu t t e r w i th 3 : 1 to 4 : 1 block (Fig. 23: Lead I l l m i g h t be i n t e r p r e t e d as i m p u r e f lu t te r , the middle por t ion of t im curve app r oach ing coarse f ibr i l la t ion) . In t i l ls t r a c i n g i t will be seen t h a t t he au r i cu l a r waves are in- creased in l eng th (slowed aur i cu la r conduct ion) and of lower vol tage t h a n in Fig . 20. On J u n e 20th, a f t e r t he p a t i e n t h a d received the re la t ively large dose of 2.9 g r a m d ig ipu ra tum, aur icu la r fib- r i l ]a t ion appeared. An in t e re s t ing addi t ional a r r h y t h m i a now, however, appea red for t he f irst t i m e ; in add i t i on to f ibr i l la t ion, t he p a t i e n t exh ib i t ed a t t acks of t a c h y c a r d i a of 15 to 45 seconds du ra t i on , t he pulse r a t e suddenly c h a n g i n g f rom abou t 86 to 150 pe r minu te . I t was difficult to get good t r a c i n g s of t h e t a c h y c a r d i a owing to t h e rest lessness of t he pa t i en t , bu t Figs. 24 to 27 i l lu s t r a t e t he findings. Ev iden t ly th i s new a r r h y t h m i a was an example of t he compara t ive ly r a re condit ion known as ven t r i cu l a r tachycard ia . I t is i n t e r p r e t ed as such because (a) t)he auricles were f ibri l la t ing and the re fore i t could no t have an aur icu la r o r ig in ; (b) because the ven t r i cu la r complexes were d is t inc t ly abnormal in fomn and (c) because of t he presence of s imilar ec4opic bea t s before (Fig. 21) and a f t e r (Fig. 28) t he pa roxysms (12). I t is p robable t h a t t he a t t acks of tachyca~xtia, which appa ren t ly arose f rom a focus in t he left ventr ic le , were due to digi4alis in toxicat ion, because they became shor te r and mor~ in f requen t f rom t h e cessat ion of digitali~ the rapy on J u n e 20 th and they were no longer p re sen t on J u n e 24th, when only occasional ex t rasys te les of s imilar form were seen; f ibri l lat ion, however, pe1*sisted. I t was now judged safe to give q u i n i d i n e su lpha te by mouth , and on J u n e 24th 1.6 g r a m was g iven in d iv ided doses. Fig. 28 is a t r a c i n g t a k e n on J u n e 24th two and t h r ee -qua r t e r hours afe0er the las t dose of quinidine ; i t shews sinus r h y t h m wi th lef t ven t r i cu l a r extrasysColes. An e lec t rocard iogram t a k e n a t noon nex t day showed sinus r h y t h m with one ectopic aur icu la r contrac- t ion, no ven t r i cu la r ex t rasys to les and a spli t I ~ wave in Leaxl I and occa- sionally in Lead ] I . (Fig. 29). The pulse r a t e was now abou t 80 and regu la r , t he impulse 12 cms. f rom the middle l ine (5th space), t he m i t r a l systolic m u r m u r was still hea rd and in addi t ion a f a in t m i t r a l m u r m u r was hea rd in la te diastole. The drowsiness, cyanosis and dyspn~ea had. com- pletely passed off a n d the patien.t was qui te comfortable. She was dis- charged a few days a f t e rwards on an t i - syphi l i t i c t r e a t m e n t and t a k i n g Tinct . Dig i ta l i s (m. xxii . p e r day). On Sept . 14th, 1927, s inus r h y t h m was sti l l p r e sen t wi th occasional ext rasys to les a r i s ing somet imes in t he lef t and


'~. ~ ,'7
.~-----~=~=~G-_ ~- i ~ ~ ~ ~ :~=--i!:~i~i~i~.=.-i}i~-
I i ~_ _ . _ _ - J ~ .... J__ --~-- . .... ~ - F - - ~ -~-~- .
| - - ' " II I H I I ~ lift I ~ . . . . . . . .

F O U R C A S E S O F A U R I C U L A R F L U T T E R 75
sometimes in the right ventricle (Fig. 30) ; the P wave w~s normal in type and the . . . . pulse rate wa~s 88 per minute, the basal metabolic rate was +28% ~, the dtastohe murmur ~ad dlsappeared,~ and the patmnt stated that she felt well. She was still taking digitalis as prescribed above on Nov. 6th, 1927, and flutter had not recurred.
Camment on Case 3 . - - A u r i c u l a r f lu t t e r gave place to a u r i c u l a r f ibr i l la t ion a f t e r d ig i ta l i sa t ion , and f ibri l lat ion, in i ts t u r n was abol ished by qu in id ine , s inus r h y t h m being res tored. The case r e l apsed to f lu t t e r a f t e r six months , and once aga in the same f o r m of t r e a t m e n t was success fu l ; on this occasion, however , pa roxysmal v e n t r i c u l a r t a c h y c a r d i a a p p e a r e d as a toxic digi ta l is effect a t a. t ime when a u r i c u l a r f ibr i l la t ion was p re sen t and qu in id ine t r ea t - ment , which was de layed f o u r days un t i l the v e n t r i c u l a r t a c h y c a r d i a d i sappeared , was aga in successful in res to r ing s inus r h y t h m . A t t he t i m e of w r i t i n g (Nov. 6th, 1927) the p a t i e n t has been on d ig i t a l i s and an t i - syph i l i t i c t r e a t m e n t f o r a lmos t f ive mon ths , a n d f l u t t e r has so f a r no t r e c u r r e d . §
CAS~ No. 4.--Housewife, age 46. Admitted Jan. 19th, 1927, from County Home and in such a serious condition that no history was obtained. Heart rate 216 per minute and regular, no murmurs heard; pulse could not be felt at the wrist; respirations 34 and temperature 96.2 o F. (axilla). Cyanosis of hands, feet and face; orthopn0ea and dyspnoea. Blood pressure could not be read by auscultatery method, hnpulse beat in anterior axillary line; liver edge felt 3 cms. below costal margin; loud rhonchi heard over thorax and crepitations heard at puhnonary bases. No ~dema of legs. Electrocardiogram (Fig. 31) showed auricular flutter with 1:1 response--the ventricle responding to each circus movement in the auricle. Pressure over vagi or on eyeballs did not show the pulse. Strophanthin (gr. 1/100) was given intravenously, after which the pulse temporarily returned to the wrist, but death occurred in two hours.
The heart alone wa.~ examined post-mortem, permission for a complete autopsy being refused. The following is the report of Dr. A. R. J . Dungan : - - - -
Macroscopic Examination.--The heart weighs 525 grammes. The pericardium is thin, smooth and shiny except for a small shaggy patch on the right margin near the apex, and another small slightly rough patch on the inferior aspect of the r ight ventricle. There is a moderate amount of epicardial fat. The myocard~um on section is normal in colour and consistency. The left auricle and ventricle are of normal size, and their walls are of normal thickness. The right ventricle is markedly dilated, and its myocardium is thinned out at the apex and along the anterior part of. the inferior wall; at the apex the wall is scarcely a milli- meter in thickness. The right auricle is a little dilated, and shows some hypertrophy The posterior cusp of the mitral valve is a little thickened and shortened ; the aortic cusp shows some thickening but no contraction, while along its line of closure is a thin ridge of minute organising vegetations. The aortic valve shows on the lower surfac~ of each cusp a few small organising vegetations; the leaflets appear otherwise practically normal. The tricuspid and pulmonary valves appear normal. The site �9 of the foramen ovale is large, and closed by a comparatively thin mem- brane. The root of the aorta shows small patches of commencing atheroma. The coronary arteries show a similar change, but i t is so slight as to produce no narrowing of the lumen.
Microscopical Examination.--Blocks for sectioning were taken as follows: Three blocks were cut at different levels from tlm right auricle, at r ight angles to the sulcus terminalis, and including the sulcus and the adjacent portion of the auricular wall. The uppermost of. these blocks was taken near the entrance to the superior vena cava, and the lowest about midway down the sulcus terminalis. Two further blocks were taken, one from each ventricle near the auriculo-ventricular ring.
�9 This patient was placed under restraint in Dec., 1927, suffering from melancholia.

76 i R I S H J O U R N A L OF M E D I C A L S C I E N C E
On examining sections from these blocks, nothing abnormal was noted~. in the myocardium of either ventricle. Sections from the uppermost block from tile right auricle showed only some fatty degeneration of the nmscle fibres; sections from the two lower auricular blocks showed, as well as the fatty degeneration, the presence in each of a patch of connec- tive tissue containing only scattered muscle-fibres. In the case of the middle auricular block this patch contained a comparatively largo arteriole in its centre, as well as some well-filled capillaries; in the lower auricular block it contained only small arterioles with a number of well- filled capillaries and showed a certain amount of. hmmorrhage. Witlr Mallory's stain no blood pi~inent could be found about this hsemorrhage. No nerve-cells were seen in this patch of connective tissue in sections. Item eigher block.
C o m m e n t o~ Case 4 . - - i n the vast ma jo r i ty of cases of aur icu lar f lut ter there is some degree of A - - V block, and only rarely, as in this case, do the ventricles respond to each aur icular circus move- ment. A perusal of the l i tera ture seems to show that only eigh- teen cases of f lut ter with 1:1 vent r icu lar response are recorded.
SUMMARY.
F o u r cases of aur icular f lut ter arc described. I n the first case sinus r h y t h m appeared a f t e r an unknowr~
interval following digitalis t rea tment , but relapse to f lut ter occurred la te r ; adequate digitalis administrat ion, however, causect the maintenance of 3 :1 to 4 :1 block between the f lu t ter ing auricles and the ventricles, with the result tha t the circulation was quite efficiently carr ied on for the pa t i en t ' s needs. In certain cases of fibrillation or f lut ter established for a considerable length of time, especially if associated with congestive hear t failure, the possibility of the presence of aur icu lar thrombi, and of the i r detachment a f t e r the appearance of sinus rhythm, should be considered; this consideration led us to believe tha t a combination of digitalis and quinidine t r ea tment in this case might be inad- visable, especially as digitalis alone produced a degree of block which permi t ted of a sufficiently slow vent r icu lar rate. Even tu- ally, however, without quinidine, while the pat ient was taking digitalis sinus rhy thm reappeared with no untoward results f rom detachment of thrombi.
I n the second and th i rd cases, on each occasion, digitalis in suit . able dosage caused f lut ter to be replaced by aur icu la r fibrillation, which, in its turn, gave place to sinus rhy thm as a result of t rea t - ment wi th quinidine; in the second case, a l though aur icular fibril- lation appeared a f t e r digitalis t reatment , relapse to f lu t ter occurred on discontinuance of the digitalis when quinidine was not used a f t e r fibrillation appeared, whilst quinidine alone in modera te ly large doses was unsuccessful in the t rea tment of flutter, bu t caused changes in the electrocardiogram which might be in te rpre ted as evidence of toxic actiou.
Each of the three relapses in the second case f rom sinus r h y t h m to flutter, as well as the first a t tack of flutter, was controlled by digitalis followed by quinidine: digitalis caused flutter Io b e

F OUR CASES OF AURICULAR F L U T T E R 77
replaced by fibrillation, and quinidine caused the lat ter to be replaced by sinus rhy thm; a large dose of digitalis, however, was required on the second occasion to convert f lut ter to fibrillation.
The two attacks of f lut ter in the third case were also success- ful ly t reated by digitalis followed by quinidine, but the large dose of digitalis given in the relapse caused t rans i tory paroxysmal vent r icular tachycardia to appear.
Cases 1, 2 and 3 il lustrate the tendency for auricular f lut ter to reappear a f te r successful treatment.
The four th case was an example of a comparatively rare con- di t ion: aur icular f lut ter with 1 :1 ventr icular response.
CONCLUSIONS.*
Digitalis alone, in a case of aur icular flutter, caused a degree ~f aurieulo-ventricular block sufficient to permit of the circulation being efficiently carried on; a f te r several months of digitalis t rea tment f lut ter was replaced by sinus rhy thm with no ill effects to, but ra ther improvement of, the pat ient ' s condition.
I t is suggested that, in certain cases of auricular f lut ter , this condit ion may be successfully t reated by full digitalisation with the object of inducing the appearance of auricular fibrilla- tion, and that the la t ter may in its t u rn be t reated by small doses
~ f quinidine, with resulting and rapid restoration of sinus rhythm. The above procedure was successful six times in two cases of au r i cu la r flutter, causing flutter to be replaced by auricular fibrillation and the latter, in its turn, to be replaced by sinus rhythm.
A case of auricular f lut ter with 1 :1 ventr icular response is described.
Re]erences.
1. Garrey: Amer. Jo. Physiol. 1914, XXXIII, 397. 2. Mines: 7tans. Roy. Sve. Canada, 1914, September. 3. Lewis: Heart, 1921, VIII, 193, 341, 361.
The Mechanism and Graphic Registration of the Hear~ Beat, London, 1925.
4. Lewis, Drury, Webb and Iliescu: Heart, 1922, IX, 207. Grant and Iliescu: Heart, 1922, IX, 289. Wedd: Heart, 1924, XI, 87. Lewis and Drury: Heart, 1926, XIII, 95.
5. Korns: Arch. Int. Med., 1923, 31, 15. 6. Lewis: Amer. Jo. Med. Sci.~ 1922, CLXIV, 157.
Lewis, Drury, Wedd and Ihescu; Heart, 1922, IX, 207. W e d d : Heart, 1924, XI, 87.
7. Viko, Marvin and White: Arch. Int. Med., 1923, XXXI, 345. 8. Gordon: Can. Med. Assn. Jo., 1924, XIV, 203. 9. Wedd: Annals oJ Clin, Med., 1924-5, III, 69.
10. Gallavardin and Gravier: Lyon M~d., March 10, 1923. 11. Wedd: Heart, 1924, XI, 87. 12. Robinson and l=Iermann: Heart, 1921, 8, 59.
* Since this paper was wri t ten , an extensive study of the course and t rea tment of auricular flutter by Parkinson and Bedford has appeared in the Quarte~'ly Journal of Medicine, Oct., 1927; in i t the treatment of flu~ter by digitalis and quinidlne are discussed; the article should be consulted by those interested.