-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
1/12
Review
A systematic review and meta-analysis of lower limb
neuromuscularalterations associated with knee osteoarthritis during
level walking
Kathryn Mills a, Michael A. Hunt b, Ryan Leigh a, Reed Ferber
a,a Faculty of Kinesiology, University of Calgary, Calgary,
Alberta, Canadab Department of Physical Therapy, University of
British Columbia, Vancouver, British Columbia, Canada
a b s t r a c ta r t i c l e i n f o
Article history:
Received 21 February 2013Accepted 16 July 2013
Keywords:
Knee osteoarthritis
Neuromuscular alterations
Level walking
Systematic review
Background: Neuromuscular alterations are increasingly reported
in individuals with knee osteoarthritis (KOA)
during level walking. We aimed to determine which neuromuscular
alterations are consistent in KOA individualsand how these may be
inuenced by osteoarthritis severity, varus alignment and/or joint
laxity.
Methods:Electronic databases were searched up to July 2012.
Cross-sectional observational studies comparing
lower-limb neuromuscular activity in individuals with KOA,
healthy controls or with different KOA cohorts
wereincluded. Two reviewers assessed methodological quality.
Effect sizes were used to quantify the magnitude
of observed differences. Where studies were homogenous, effect
sizes were pooled using a xed-effects model.
Findings: Fourteen studies examining neuromuscular alterations
in indices of co-contraction, muscle amplitude
and muscle activity duration were included. Data pooling
revealed that moderate KOA individuals exhibit in-
creased co-contraction of lateral knee muscles (ES 0.64 [0.3 to
0.97]) and moderately increased rectus femoris
(ES 0.73 [0.23 to 1.22]), vastus lateralis (ES 0.77 [0.27 to
1.27]) and biceps femoris (ES 1.18 [0.67 to 1.7]) mean
amplitude. Non-pooled dataindicated prolonged activity of these
muscles.Increased medial kneeneuromuscular
activity was prevalent for those exhibiting varus alignment and
medial knee joint laxity.
Interpretation: Individuals with KOA exhibited increased
co-contraction, amplitude and duration of lateral knee
muscles regardless of disease severity, limb alignment or medial
joint laxity. Individuals with severe disease,
varus alignment andmedial joint laxitydemonstrate
up-regulationof medialknee muscles. Future research inves-
tigating the ef
cacy of neuromuscular rehabilitation programs should consider
the effect of simultaneous up-regulation of medial and lateral knee
muscles on disease progression.
2013 Elsevier Ltd. All rights reserved.
1. Introduction
Knee osteoarthritis (KOA) is a progressive disease resulting in
the
breakdown of joint cartilage and bone that is characterized by
joint
pain, stiffness and swelling (Bombardier et al., 2011).
Recently, several
studies have examined neuromuscular control of the lower limb in
indi-
viduals with KOA during walking. The results of these studies
provide
compelling evidence that neuromotor control of the lower limb is
al-
tered in this population. Altered neuromuscular control in
individuals
with KOA is concerning due to the deleterious effects on joint
loading
and stability.
Co-ordinated agonistic and antagonistic muscle activities play
major
roles in distributing load between the medial and lateral
tibiofemoral
joints during walking. Altered muscle activity, either an
increase in me-
dial activity or decrease in lateral activity, at the knee may
increase the
demand on lateral soft tissue to resist the external knee
adduction mo-
ment (the biomechanical proxy for medial knee joint load)
(Schipplein
and Andriacchi, 1991). A high external knee adduction moment in
an
individual with varus alignment and/or lateral joint laxity
could lead
to a condition where the entire external knee adduction moment,
and
potentially the dynamic load, occurs through the medial
compartment
of the tibiofemoral joint (Schipplein and Andriacchi, 1991).
This is be-
lieved to substantially increase in compressive forces and
accelerate de-
generation of the medial compartment.
As the medial compartment degenerates, the distance between
the
medialligamentinsertions is reduced andthe medialsoft
tissuecontrib-
uting to joint stability can become lax (Lewek et al., 2004;
Sharma et al.,
1999). Impairment in this passive stabilization system increases
the de-
mand for coordinated neuromuscular activity to compensate. An
inabil-
ity to adequately perform this task has been theorized to lead
to
recurrent episodes of instability and further degenerative
changes
(Lewek et al., 2004; Sharma et al., 1999). Thus, knee joint
stability and
load distribution is achieved through an interaction between
active
and passive strategies. As such, it is not surprising that
increased neuro-
muscular activity of the medialknee muscles hasrecentlybeen
correlat-
ed with rate of knee cartilage volume loss in individuals with
medial
Clinical Biomechanics 28 (2013) 713724
Corresponding author at: Faculties of Kinesiology and Nursing,
University of Calgary,
2500 University Drive NW, Calgary, Alberta, T2N 1N4 Canada.
E-mail address:[email protected](R. Ferber).
0268-0033/$ see front matter 2013 Elsevier Ltd. All rights
reserved.
http://dx.doi.org/10.1016/j.clinbiomech.2013.07.008
Contents lists available atScienceDirect
Clinical Biomechanics
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m
/ l o c a t e / c l i n b i o m e c h
http://dx.doi.org/10.1016/j.clinbiomech.2013.07.008http://dx.doi.org/10.1016/j.clinbiomech.2013.07.008http://dx.doi.org/10.1016/j.clinbiomech.2013.07.008mailto:[email protected]://dx.doi.org/10.1016/j.clinbiomech.2013.07.008http://www.sciencedirect.com/science/journal/02680033http://crossmark.crossref.org/dialog/?doi=10.1016/j.clinbiomech.2013.07.008&domain=pdfhttp://www.sciencedirect.com/science/journal/02680033http://dx.doi.org/10.1016/j.clinbiomech.2013.07.008mailto:[email protected]://dx.doi.org/10.1016/j.clinbiomech.2013.07.008
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
2/12
compartment KOA and varus lower limb alignment (Hodges et
al.,
2012).
A growing number of studies are reporting neuromuscular out-
comes during walking in individuals with KOA. As such, a review
of
how neuromuscular control of the lower limb is altered, with
respect
to amplitude, duration and antagonistic activity, in individuals
with
KOA is timely. To accomplish this task we conducted a systematic
re-
view of cross-sectional observational studies comparing
neuromuscular
activity in individuals with KOA with either similar healthy
controls oracross KOAsubgroups. Our aim was to
determinewhichneuromuscular
alterations are consistently observed in individuals with KOA
and how
these alterations may be different in the presence of knee varus
align-
ment and/or knee joint laxity. As there is evidence to suggest
that the
nature and magnitude of neuromuscular alterations may be
inuenced
by the severity of KOA (Astephen et al., 2008), we also examined
the
effect of disease severity on neuromuscular alterations during
level
walking. Our ndings will assist clinicians in designing
conservative
rehabilitation programs that incorporate neuromuscular
retraining as
well as highlight areas for future research.
2. Methods
2.1. Search strategy
We devised a search strategy for the following electronic
databases:
MEDLINE, EMBASE, CINAHL, SportDiscus, PubMed and Web of
Science
and included all references listed until the 30th July 2012. The
search
terms and strategy were identical forall databases: (1) Knee
osteoarthr*
OR gonarth*, (2) Walking OR gait, (3) Combined 1 AND 2, (4)
Neuromotor OR neuromuscular OR electromyography OR EMG OR
mus-
cle activity and (5) Combined 3 AND 4. No restrictions were
placed on
the year, status or language of publication. All titles returned
by the
search strategy were reviewed by a single reviewer (KM), with
abstracts
of those papers potentially meeting the selection criteria
retrieved for
further consideration. Full text versions of studies meeting the
selection
criteria, as determined by two reviewers(KM, RL), were obtained
for in-
clusion in the review. Reference lists of included papers and
published
knee osteoarthritis reviews were hand-searched (KM) to ensure
alleligible data were included.
2.2. Selection criteria
Publications were required to be human-based, cross-sectional
ob-
servational studies examining neuromuscular activity in a KOA
cohort
and a comparator group during level walking. Diagnosis of KOA
was re-
quired to be made using radiographic or clinical criteria. No
restriction
was placed on disease severity, involved compartment or lower
limb
alignment. Papers were excluded if they contained: (a)
participants
with radiographically conrmed OA in other weight-bearing
joints,
(b) participants who had undergone a total joint arthroplasty or
joint
preservation surgery in the study limb or (c) participants who
required
the assistance of walking aids. These exclusion criteria were
imposeddue to potential confounding of results (Ouellet and Moffet,
2002;
Rudolph et al., 2007; Simic et al., 2011).
Included publications were juxtaposed for author names,
afliation
and participant characteristics to reduce the risk of bias
introduced
through duplicate data. Where multiple studies, authored by
identical
authors, presented outcome variables from the same participant
num-
bers, age, weight and sex ratio, only results of the publication
with
higher methodological quality were included.
2.3. Methodological quality
Methodological quality of included papers was assessed using
a
modied version (Munn et al., 2010) of a validated quality index
for
non-randomized trials (Downs and Black, 1998). This version
included
16 items assessing reporting quality, external validity, and
internal
validity (bias and confounding). It does not include items
relating to
an intervention but still includes items relating to the
blinding of
observers. Two independent reviewers (KM, MAH) assessed all
papers, with the second reviewer blinded to author names,
title,
afliation and journal name. Disagreements in initial ratings
were
discussed at a consensus meeting. Publications scoring less than
50%
on the quality index were excluded from further review
(Coombes
et al., 2010).
2.4. Data synthesis
Inter-rater reliability of the modied quality index was
evaluated
with the kappa () statistic. The magnitude of agreement was
quanti-ed usingHopkins (2000)system of very small (0 to 0.1), small
(0.1
to 0.3), moderate (0.3 to 0.5), high (0.5 to 0.7), very high
(0.7 to 0.9),
and almost perfect to perfect (0.9 to 1.0).
Two independent reviewers (KM, RL) extracted publication
details
(authors, year, publication source and type), sample
characteristics
(sample size, sampling technique, source of participants and
selection
criteria), participants' characteristics (age, gender, severity
of KOA,
limb alignment, knee joint laxity and method of diagnosis),
neuromotor
characteristics (electrode type, size, shapeand
placement,sampling fre-
quency and amplitude normalization) and point estimates of
effect di-
rectly from included papers. Differences were settled by
consensus.
Authors were contacted to provide any missing data and, if these
were
not provided, they were qualitatively extracted from graph or
result
sections. Point estimates of effect were used to calculate mean
differ-
ences and 95% condence intervals (CI) between groups. An effect
size
(ES = mean difference/pooled standard deviation) was used to
quanti-
fy the magnitude of the differences and permit a common metric
be-
tween studies. The magnitude of ES was interpreted using
Hopkins
et al. (2009)criteria: trivial (0.0 to 0.2), small (0.21 to
0.6), moderate
(0.61 to 1.2) and large (N1.2). Qualitative descriptionsof
differences be-
tween groups were also extracted from principle component
analysis of
electromyography (EMG) waveforms.
Meta-analysis was performed using the ES in a xed-effects
model
within Cochrane Review Manager (V5.1), using theI2 index to
measureinconsistency (the percentage of total variation due to
heterogeneity)
across included papers and referenced to thresholds of low
(N25%),
moderate (50%) and high (75%) evidence of heterogeneity
(Higgins
et al., 2003). The criteria for pooling were: (a) participants
exhibiting
the same KOA severity, (b) neuromuscular activity being
examined
over thesame time periods of thegaitcycle, (c) thesame
normalization
methods and (d) co-contraction indices formulated using
identical
methods. As this review did not include randomized control
trials, a
combination of ES and heterogeneity index was used to quantify
levels
of evidence based on those proposed byvan Tulder et al. (2003).
Evi-
dence of neuromotor alterations associated with KOA was
interpreted
as strong (large ES with low evidence of heterogeneity),
moderate
(moderate ES and low evidence of heterogeneity), limited (small
ES
with low heterogeneity or moderate/large ES with moderate
evidenceof heterogeneity), conicting (high evidence of
heterogeneity) and no
evidence (95% CI of ES crossed zero).
3. Results
3.1. Search strategy and study characteristics
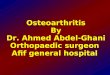
The search strategy retrieved 489 papers. Fifteen papers met the
se-
lection criteria and underwent quality assessment. No studies
met the
criteria for duplicate data, although several studies were
published
from thesame laboratory. Onepaper wasexcluded based on poor
meth-
odological quality, thus 14 papers were included in the review
(Fig. 1).
For 11 papers, inclusion in the KOA group was based on
radiographic
and clinical criteria while the remaining three papers used
only
714 K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
3/12
radiographiccriteria. KOAseverity was reported by the authors of
seven
papers and interpreted from the radiographic and clinical
ndings
(e.g., joint space narrowing, osteophyte formation, or scheduled
for
high tibial osteotomy) from a further two. From these studies,
there
were nine cohorts of individuals with moderate KOA and four
cohorts
with severe disease. Four studies included individuals with a
range ofseverities within a single KOA group and were subsequently
classied
as KOA.Schmitt and Rudolph (2007)also included individuals with
a
range of KOA severities, however as over 60% of their cohort
exhibited
mild radiographic changes and symptoms we considered them to be
a
predominantly mild KOA cohort. Five studies examined
individuals
with varus mechanical alignment. Individuals from three of these
stud-
ies also exhibited increased medial knee joint laxity, quantied
by stress
radiographs, compared with controls (Table 1).
Samplesizes ranged from 8 to 60 individuals in KOA groupsand 12
to
63 individuals in healthycontrol groups. Neuromuscular variables
exam-
inedwere: (a) indicesof muscle co-contraction, (b) magnitude of
muscle
activation and (c) muscle activity duration. The muscles
examined were
vastus medialis (VM), vastus lateralis (VL), rectus femoris
(RF),
biceps femoris (BF), semimembranosis (SM), tibialis anterior
(TA),
soleus (Sol), medial gastrocnemius (MG) and lateral
gastrocnemius
(LG). Electromyography data were primarily obtained using
surface
bipolar, circular Ag/AgCl electrodes. The inter-electrode
distances
ranged from 18 to 30 mm, which coincides with the distance
between
peaks of the propagating action potential (Kamen and Caldwell,
1996).
All studies positioned electrodes over the muscle belly parallel
withmuscle bers. Sampling rates ranged from 1000 to 2000 Hz and
data
were normalized to maximum voluntary isometric contraction
(MVIC)
in 12 papers and to maximum amplitude during walking (% Max)
in
the remaining two (Liikavainio et al., 2010; Schmitt and
Rudolph, 2007).
3.2. Methodological quality
The quality indices of included papers ranged from nine to 13
(of a
possible 17) and were interpreted as being, on average, moderate
quality
(Table 2). Initial inter-rater reliability between the two
reviewers was
very high (= 0.877) with items 18 (= 0.435) and 25 (= 0.562)
differing most. For the remaining items, there was almost
perfect
agreement (Hopkins et al., 2009)(Table 2). Consensus was
reached
on all differing items during the rst discussion. Overall,
papers did
Literature search: knee osteoarthr*, gonarth*, walking,
gait,
neuromotor, neuromuscular, electromyography, EMG, muscle
activity
Databases:
MEDLINE: 39
EMBASE: 94
CINAHL: 31
Sportdiscus: 63
PubMed: 89
Web of Science: 153
Hand search: 20Search results combined: 489
Excluded n = 450
Non-human
Not knee OA
Duplicates
Post surgical
Experimental design
Review paper
Abstracts screened on the basis of title
n = 39
Full text paper retrieved on basis of
abstract n = 19
Excluded n = 20
No neuromotor variables
Modeling study
Not level walking
Papers considered for inclusion
n = 15
Excluded n = 4
Within group design (no
comparison group)
Papers included in review
n = 14
Excluded n = 1
Quality index score
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
4/12
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
5/12
Lewek et al.
(2006)
OA n = 15 (6/9) Age: 47.7 (7.4), height 1.75 m (0.09),
mass 91.9 kg (17.4)
Moderate Radiographic Medial compartment and PFJ OA excluded
Clinical Scheduled for high tibial osteotomy
Control n = 15 (6/9) Age: 48.4 (6.3), height 1.71 m (0.09),
mass 83.8 kg (17.3)
Radiographic medial joint space
width = 1.6 (1.1) mm
Medial joint laxity = 4.9 mm (1.8)
Lateral joint laxity = 3.5 mm (1.5)
Weight bearing line = 28.9% (12.7)
Liikavainio et al.
(2010)
OA n = 54 (men only) Age: 59 (5.3), BMI 29.7 kg/m2 (4.7) General
OA Radiographic Most symptomatic limb used in analysis
Control n = 53 (men only) KL grade 1 to 4
Varus ranged from 3.2 (2.5) for
KL = 1 to 9.5 (2.5) for KL = 4
Rudolph et al.
(2007)
OA n = 15 (8/7) 0.1 (1.58)
varus
Age: 49.2 (4.5), BMI 30.7 kg/m2 (4.8) Moderate Radiographic
Scheduled for high tibial osteotomy
Control n = 15 (8/7) Age: 49.2 (4.25), BMI 28.7 kg/m2 (5.5)
Clinical 6.33 (2.39) varus
Rutherford et al.
(2010)
OA n = 17 (10/7) Age: 56 (8.8), BMI 29.8 kg/m2 (6.5) Moderate
Radiographic Unil ateral knee OA
Control n = 20 (7/13) Age: 46.5 (7), BMI 25.9 kg/m2 (4.8)
Clinical Able to walk a city block, reciprocally
negotiate
10 stairs and jog 5 m
Rutherford et al.
(2011)
Moderate n = 16 (8/8) Age: 61 (6), BMI 31.3 kg/m2 (3.6) Moderate
Radiographic Predominantly medial compartment
Severe n = 15 (10/5) Age: 61 (9), BMI 30.7 kg/m2 (5.4) Severe
Clinical Severe group scheduled for TKA
Control n = 16 (8/8) Age: 56 (96), BMI 24.6 kg/m2 (3.9) All OA
groups able to walk N1.0 m/s
Schmitt and
Rudolph
(2007)
OA n = 28 (14/14) Age: 60.4 (9.75), Height 1.7 m (0.11),
mass 92.91 kg (16.16)
Median =
mild
Radiographic Unilateral and bilateral knee OA
(most symptomatic knee analyzed)
Control n = 26 (13/13) Age: 58.5 (9.5), height 1.68 m
(0.07),
mass 83.93 kg (1.85)
Medial compartment
(KL grade N2 in lateral and PFJ excluded)
KL grades 2 to 4 (61% exhibited KL grade =
2)
5.15 (3.43) varus Medial joint laxity = 4.23 mm (1.8)
Lateral joint laxity = 2.77 mm (1.35)
Zeni et al. (2010) Moderate n = 16 (6/10) Age: 62.8 (10)
Moderate Radiographic KL grades 2 to 3 for moderate and 4 for
severe.
Severe n = 8 (3/5) Age: 62.2 (8) Severe Medial compartment
Control n = 18 (8/10) Age 61 (11)
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
6/12
not adequately report the sampling method used to recruit
participants
(item 11) or provide the proportion of participants who were
asked to
participate compared with those who agreed to participate (item
12).
No study reported if they blinded assessors to group allocation
(KOAor control) duringanalysis of primary outcomemeasures, and few
stud-
ies provided adequate information regarding the source of
participants
included in the study or the time period for recruitment. These
issues
are possible sources of confounding and bias.
3.3. Muscle co-contraction
Ten studies examined the magnitude of co-contraction
associated
with KOA. Co-contraction indices were grouped into those
specically
comparing medial thigh and shank muscles (VM:SM, VM:MG),
those
comparing lateral thigh and shank co-activity (VL:BF, VL:LG,
TA:LG)
and those comparing medial muscles with lateral muscle (VM:BF
and
VL:SM). In order to examine the inuence of disease severity,
compari-
sons were partitioned into those examining general, mild,
moderatedand severe KOA cohorts when compared with healthy controls
and
when compared with other KOA severities.
3.3.1. KOA cohorts versus controls
Two studies, examining individuals with moderate KOA, met
the
criteria for pooling (Hubley-Kozey et al., 2009; Lewek et al.,
2004).
Data pooling revealed the only co-contraction index that was
systemat-
ically increased was VL:BF, where there was moderate evidence of
a
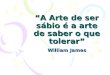
greater co-contraction (ES 0.64 [0.3 to 0.97] I2 = 0%) in
individuals
with moderate KOA, compared with healthy controls (Fig. 2A).
Non-pooled data of lateral muscle co-contraction also indicate
indi-
viduals with KOA walk with increased lateral muscle
co-contraction re-
gardless of disease severity, varus alignment and knee laxity
(Childs
et al., 2004; Hortobgyi et al., 2005; Lewek et al., 2006;
Schmitt and
Rudolph, 2007)(Table 3). Further,Heiden et al. (2009)reported
that
lateral muscles provided the greatest contribution to an
increased co-
contraction between knee extensors and knee exors. However,
lateral
thigh muscle co-contraction was only signicantly increased
duringmidstance (Lewek et al., 2006; Schmitt and Rudolph, 2007).
This sug-
gests that while lateral shank muscle co-contraction is
increased in
KOA during all phases of the stance phase, increased thigh
muscle co-
contraction only occurs when the osteoarthritic limb is fully
loaded.
Non-pooled data of medial co-contraction indices suggests that
me-
dial knee joint laxity may inuence the magnitude of medial
co-
contraction in KOA. Studies examining KOA participants with
medial
knee joint laxity report signicantly increased medial shank and
thigh
muscle co-contraction regardless of disease severity (Lewek et
al.,
2004, 2006; Schmitt and Rudolph, 2007) (Table 3). In studies
by
Lewek et al. (2006, 2004) moderate increases (ES 0.84 and 0.83)
in
VM:MG were observed during preparation and weight
acceptance.
Thus, the presence of greater medial muscle co-contraction may
reect
an attempt to increase medial stability by increasing
compressive forcesacross the knee.
Non-pooled data of medial and lateral thigh muscle
co-contraction
suggested disease severity might inuence the magnitude of
co-
contraction (Table 3).Zeni et al. (2010) reported VL:SM
co-contraction
was only consistently increased across a range of walking speed
in
those with moderate KOA. In contrast, co-contraction indices
were not
increased, compared with healthycontrols, in general and severe
KOAco-
hortswhentheywalked at a self selected,or fast speeds
(Liikavainio et al.,
2010; Zeni et al., 2010).
3.3.2. Between KOA cohorts
Two studies compared co-contraction between individuals with
moderate and severe KOA (Hubley-Kozey et al., 2009; Zeni et
al.,
2010). No data pooling was possible. Over similar phases of the
gait
Table 2
Modied quality index.
Reporting External validity Internal validity - bias Internal
validity - confounding
Publication
1.Hypothesis
clearlydescribed?
2.Mainoutco
mesclearly
described?
3.C
haracteristicsofthepatients
includedclearlydescribed?
5.D
istributionofprinciple
confoundero
feachgroupclearly
described?a
6.Mainfindingsclearly
described?
7.Estimateso
frandom
variabilityprovidedforthemain
outcomes?
10.Actualprobabilityvalues
reportedformainoutcomes?
11.Werethe
subjectsaskedto
participatere
presentativeofthe
entirepopula
tion?
12.Werethe
subjectswhowere
preparedtop
articipate
representativ
eoftheentire
15.Wasthereanattempttoblind
thosemeasur
ingthemain
outcomes?
16.Wasitcle
ariftheresults
werebasedondatadredging
18.Werethe
statisticaltests
appropriate?
20.Werethe
mainoutcome
measuresvalidandreliable?
21.Wereallp
atientsandcontrols
recruitedfrom
thesame
population?
22.Wereallp
atientsand
controlsrecruitedoverthesame
timeperiod?
25.Wastheir
adequate
adjustmentforconfounding?
b
Total(17)
Astephen et al. (2008) 1 1 0 2 0 1 1 0 0 0 1 1 1 0 0 0 9
Childs et al. (2004) 1 1 1 2 1 1 1 0 0 0 1 1 0 0 0 0 10
Heiden et al. (2009) 1 1 1 1 1 1 1 0 0 0 1 1 1 0 0 1 11
Hortobgyi et al. (2005) 1 1 1 1 1 1 0 0 0 0 1 1 1 0 0 0 9
Hubley-Kozey et al. (2006) 1 1 1 2 1 1 1 0 0 0 1 1 1 1 0 0
12
Hubley-Kozey et al. (2009) 1 1 1 2 1 0 0 0 0 0 1 1 1 0 1 0
10
Lewek et al. (2004) 1 1 1 2 1 1 1 0 0 0 1 1 1 0 0 1 12
Lewek et al. (2006) 1 1 1 2 1 1 1 0 0 0 1 0 1 0 0 1 11
Liikavanio et al. (2010) 1 1 1 2 1 1 0 0 0 0 1 1 0 1 0 1 11
Rudolph et al. (2007) 1 1 1 2 1 1 1 0 0 0 1 1 1 0 0 1 11
Rutherford et al. (2010) 1 1 1 1 1 1 1 0 0 0 1 1 1 0 0 0 10
Rutherford et al. (2011) 1 1 1 2 1 1 1 0 0 0 1 1 1 0 1 1 13
Schmitt and Rudolph (2007) 1 1 1 2 1 1 1 0 0 0 1 1 1 1 0 0
12
Zeni et al. (2010) 1 1 0 1 1 1 1 0 0 0 1 1 1 0 0 1 10
Kappa levels of agreement 0.98 1.0 0.63 1.0 0.98 1.0 1.0 0.98
0.97 0.97 1.0 0.44 1.0 1.0 1.0 0.56 0.877
Allitems,except item5, were scored1 forfullling thecriterionor 0
ifthe criterion were notlled. Publications that didnot
providesufcient detailsto fulll thecriterionwere alsogivena
0 for unable to be determined as perinstructions of theoriginal
index. Kappa scores indicate level of initialagreementbetween
reviewers prior to theconsensus meeting. Thetotal kappa
score indicates overall level of agreement.a Thiscategorywas
interpretedas theKOA diagnosis being clearlydescribedwithrespect to
radiographic severity, clinicalseverityand mechanicalalignment.If
allthreeof thecriteria were
described, 2 points were awarded for yes. If two of the criteria
were described, 1 point was awarded forpartially.b A full mark was
awarded in this category if authors demonstrated no statistically
signicant difference in walking speed or pain between KOA group(s)
and control or if analyses of
covariance were conducted. Publications that did not investigate
differences in walking speed or pain or did not adjust for these
potential confounders were awarded unable to be
determined.
718 K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
7/12
cycle,Hubley-Kozey et al. (2009) reported individuals with
severe KOA
exhibited moderately greater co-contraction indices in both
medial and
lateral muscle groups (VL:BF: ES 0.62, VL:LG: 0.68 and VM:MG:
0.61)
than those with moderate disease. In contrast, Zeni et al.
(2010)found
no difference in VL:SM co-contraction, regardless of whether
participants walked at 1.0 m/s, self-selected or fast walking
speeds
(Table 3). This difference in resultmay be dueto thestudies
using differ-
ent muscles in their calculations of co-contraction or due to
calculating
co-contraction using different equations.
3.4. Muscle amplitude
Ten studiesexamined alterations in amplitude of the
gastrocnemius,
soleus, quadriceps and hamstrings associated with KOA during
level
walking. Alterations in mean, peak and net (the sum of all
normalized
muscle activity (Heiden et al., 2009)) muscle amplitude were
investi-
gated. The potential inuence of disease severity was the focus
of sever-
al publications and walking data from those with general,
mild,
moderate and severe KOA were examined. ES, calculated from
differ-
ences in principal components between individuals with
moderate
KOA and healthy controls (Rutherford et al., 2010, 2011), was
pooled
for gastrocnemius, quadriceps and hamstring amplitudes.
3.4.1. Between KOA and controls
Pooled data revealed no evidence of gastrocnemius overall
ampli-
tude alteration associated with moderate KOA(Fig. 2B). While
this nd-
ings was supported by results of studies investigating
individuals with
severe KOA (Astephen et al., 2008; Rutherford et al., 2011),
data from
non-pooled studies investigating those with moderate KOA
suggest
that results may be inconclusive. Two studies, that were not
pooled,
supported the nding from pooled data (Astephen et al., 2008;
Rudolph et al., 2007). In contrast,Hubley-Kozey et al.
(2006)reported
a decrease in mean MG amplitude andHeiden et al. (2009)reported
a
net increase in muscle amplitude (Table 3). This suggests that
if individ-
uals with moderate KOA exhibit altered gastrocnemius amplitude,
there
is no consistency in the direction or magnitude of that
alteration.
Moderate increases in VL (ES 0.77 (0.27 to 1.27) I2 = 72%) and
RF
(ES 0.73 (0.23 to 1.22)I2 = 0%) amplitude were observed from
pooleddata of individuals with moderate KOA compared with healthy
controls
(Fig. 2B). Of the eight studies, that were not pooled, only one
(Rudolph
et al., 2007) did not report an increase in mean or peak
quadriceps am-
plitude in individuals with KOA regardless of disease severity
or joint
laxity. This suggests that increases in VL and RF amplitude are
consis-
tently associated with KOA regardless of disease severity or
joint laxity.
VM mean and net amplitude was only reported to be increased in
stud-
ies examining general and predominantly mild KOA cohorts
(Heiden
et al., 2009; Liikavainio et al., 2010; Schmitt and Rudolph,
2007).
There was no increasein VM mean amplitude in moderate or severe
co-
horts compared with controls (Hubley-Kozeyet al.,2006; Rudolphet
al.,
2007; Rutherford et al., 2011).
Pooled data reveal a systematic, moderate increase in amplitude
of
BF in those with moderate KOA compared with healthy controls
(ES1.18 (0.67 to 1.7) I2 = 0%)(Fig. 2B). This nding was supported
by a
Schmitt and Rudolph (2007),investigating differences in mean
ampli-
tude between a predominantly mild KOA cohort and controls. For
gen-
eral andsevere KOAcohorts, there were also trends(Zeni et al.,
2010) or
signicant increases (Astephen et al., 2008; Heiden et al.,
2009;
Liikavainio et al., 2010) in hamstring mean amplitude (Table 3).
While
SM mean and peak amplitude moderately increased compared
with
controls, at a range of walking speeds (Zeni et al., 2010), its
mean ampli-
tude was consistently lower than BF (Hubley-Kozey et al.,
2006;
Rutherford et al., 2010, 2011).
3.4.2. Between KOA cohorts
Three studies examined differences in muscle amplitude
between
individuals with moderate and severe KOA (Astephen et al.,
2008;
Rutherford et al., 2011; Zeni et al., 2010). As with KOA-control
compar-
isons, alterations in gastrocnemius mean amplitude were
inconsistent
in direction and magnitude between those with moderate and
severe
KOA(Astephen et al., 2008; Rutherford et al., 2011). There wasno
differ-
ence in quadriceps mean amplitude between moderate and severe
KOA
groups (Astephen et al., 2008; Rutherford et al., 2011; Zeni et
al., 2010),
except during fast walking where mean and peak VL activity was
mod-
erately increased in individuals with moderate KOA (ES 0.73 and
0.86)
(Zeni et al., 2010). There was a large reduction in BF mean
amplitude(ES 1.46) in those with moderate disease, but only during
midstance
(Rutherford et al., 2011) (Table 3).
3.5. Muscle activity duration
Five studies reported on differences in muscle activity duration
be-
tween individuals withKOA and controls. Comparisons of
gastrocnemi-
us, quadriceps and hamstrings muscles were made between
individuals
with moderate and severe KOA and controls (Table 3). No data
pooling
was performed.
3.5.1. Between KOA and controls
Data extracted from three studies, which analyzed gastrocnemius
du-
rations using principal component analysis, revealed the
duration of MG
activity did not differ in individuals with moderate KOA
compared with
healthy controls (Astephen et al., 2008; Hubley-Kozey et al.,
2006; Ruth-
erford et al., 2011). This nding was not supported by a study
examining
duration using discrete variables, which reported a moderate
increased in
MG duration (ES 0.97) (Childs et al., 2004). Two studies
compared gas-
trocnemius duration between individuals with severe KOA and
controls
reported those with severe KOA exhibited longer duration with MG
acti-
vating later than LG (Astephen et al., 2008; Rutherford et al.,
2011). This
was a different activation pattern than controls.
Waveform and discrete analysis indicate that the activity of the
VL
and RF was prolonged in both moderate and severe KOA,
compared
with controls (Childs et al., 2004; Hubley-Kozey et al., 2006;
Rutherford
et al., 2011). There was no change in VM temporal
characteristics for
those with moderate KOA (Hubley-Kozey et al., 2006).
With the exception of onestudy (Rutherford et al., 2011),
hamstringactivity was observed to be prolonged in individuals with
KOA. While
both BF and SM durations were increased in those with
moderate
KOA, compared with controls (Rutherford et al., 2010), BF
activity was
prolonged compared with SM in the KOA group. Analysis of
discrete
values suggests a large effect (SM: ES 1.38) (Zeni et al.,
2010)(Table 3).
3.5.2. Between KOA groups
Two studies examined differences in muscle activity and
duration
between individuals with moderate and severe KOA (Astephen et
al.,
2008; Rutherford et al., 2011). Compared with individuals with
moder-
ate KOA, those with severe disease exhibited delayed onset of
MG
(Rutherford et al., 2011) and longer duration (Astephen et al.,
2008).
RF activity was observed to be prolonged for both groups but
more so
in the severe group and there was no difference in hamstring
duration(Rutherford et al., 2011).
4. Discussion
The primary nding of this review is that many individuals with
KOA
exhibit altered neuromuscular activity across co-contraction,
amplitude
and temporal domains, when compared with healthy controls.
Specical-
ly, pooled resultsdemonstrated that individuals withmoderate KOA
con-
sistently exhibited moderately increased lateral thigh
co-contraction
compared with healthy controls over the period of 100 ms prior
to heel
contact until the peak external knee adduction moment
(approximately
25% of stance). Pooled data also revealed those with moderate
KOA
walk with consistent moderate increases in RF and BF amplitude
and a
moderate, although heterogeneous, increase in VL amplitude.
While
719K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
8/12
non-pooled data cannot provide the precision of meta-analysis,
the num-
ber of studies reporting elevated lateral muscle co-contraction
and
prolonged VL,RF and hamstring duration suggests thatthese
arealso con-
sistently associated with KOA regardless of disease severity,
knee joint
laxity or varus alignment. Medial knee joint laxity may have an
important
inuence on medial knee muscleco-contractionas it
wasonlyconsistent-
ly observed in individuals with laxity, regardless of disease
severity. Dis-
ease severity does appear to inuence the presence of increased
medial:
lateral muscleco-contraction, as it was only signi
cantlyincreased, acrossa range of walking speeds,in those with
moderate KOA (Zeni et al., 2010).
Concurrent increases in medial and lateral muscle amplitudes, as
ob-
served inthe general KOA group(Liikavainio et al.,2010), could
potential-
ly explain the lack of increase in the co-contraction index.
However, for
the severe KOA group, who only exhibited an increased
co-contraction
when there wasa concurrent increase in
medialandlateralmuscleampli-
tudes (Zeni et al., 2010), it could be due to the observed
slower walking
speeds or reect an arthrogenic muscle inhibition component in
the
disease process (Hurely, 1999).
Several authors have hypothesized that the primary reason
why
individuals with KOA adopt neuromuscular alterations is to
unload
the medial knee joint (Heiden et al., 2009; Hortobgyi et al.,
2005;
Hubley-Kozey et al., 2009). Further, they suggest that lateral
muscle
activity has a protective effect on the knee and preserves knee
function.
Findings from this review demonstrate that increased lateral
muscle
activity is a prevalent adaptation, particularly when the knee
is
fully loaded. Recently, a delay in lateral knee muscle
co-contraction
was correlated with increased lateral cartilage loss in KOA
patients
with varus malalignment over a 12-month period ( Hodges et
al.,
2012). However, further research is needed to determine
whether
increased lateral muscle activity is a neuromuscular adaptation
that
should be encouraged as a protective mechanism in
individuals
with KOA.
A second, frequently postulated reason for increased
neuromuscular
activity is the need for increased knee joint stability (Heiden
et al., 2009;
Hortobgyi et al.,2005; Hubley-Kozey et al., 2009). Specically,
increased
coordinated muscle activity is required when the passive
stabilization
provided by soft tissue is compromised (Schipplein and
Andriacchi,
1991). The ndings of this review support this statement. Medial
co-
contraction indices were signicantly greater than controls for
individ-
uals with medial knee joint laxity (Hubley-Kozey et al., 2009;
Lewek
et al., 2004, 2006; Schmitt and Rudolph, 2007). This suggests
that onlythose individuals who have a lack of medial passive knee
support, poten-
tially through an approximation of medial ligament insertions
resulting
from the loss of cartilage and bone height (Lewek et al., 2004;
Sharma
et al., 1999), exhibit increased medial muscle activation.
Even though individuals without knee joint laxity exhibited
similar
medial knee muscle neuromuscular activity as healthy control,
they
exhibited elevated and prolonged activity of RF regardless of
disease se-
verity. This could also be an attempt to protect and stabilize
the knee.
However, current evidence questions the efcacy of increased
neuro-
muscular activity of the RF and medial knee muscles in
accomplishing
this task (Hodges et al., 2012; Schipplein and Andriacchi,
1991;
Schmitt and Rudolph, 2008). Increased neuromuscular activation
of
muscles that cross the knee increases compressive forces. While
this
would increase stability, it would also increase load on the
joint and
could accelerate degeneration of the medial compartment
(Schipplein
and Andriacchi, 1991). Further, increased duration medial knee
muscle
co-contraction hasrecently been correlated with increasedloss of
medi-
al knee cartilage volume (Hodges et al., 2012). Interestingly,
it is possi-
ble for increased neuromuscular activity of medial and lateral
knee
muscles as well as RF to co-exist as demonstrated in a severeKOA
cohort
(Hubley-Kozey et al., 2009) and in a predominantly mild KOA
cohort
with varus alignment and medial knee joint laxity (Schmitt
and
Rudolph, 2007). However, due to the cross-sectional nature of
studies
Fig. 2. Forest plot of data pooling. Filled diamonds indicate
pooled data ES and 95% condence intervals. Condence intervals that
do not cross zero indicate a systematiceffect. The con-
sistencyof neuromuscularalterations wasdeterminedbasedon
thepresence of a systematiceffectanda low I2 index. (A)PooledES
forco-contraction indices.(B) PooledES foramplitude.
Amplitude ES was calculated from mean (SD) factor scores of
principal components so mean differences were not calculated.
720 K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
9/12
Table 3
Results of included papers.
Authors Variable Knee OA Comparator Result/mean difference (95%
CI) and effect size (ES)
Co-contraction index
Childs et al. (2004) VL:BF (% MVIC) General OA Control 13.0
(2.37 to 23.63) ES 0.68
TA:MG (% MVIC) 9.0 (4.17 to 13.83) ES1.04
Heiden et al. (2009) Muscles: lateral muscles
(SM, VM, MG:BF, VL, LG % MVIC)
General OA Control OA group exhibited signicantly greater
co-contraction during loading and early
stance and signicantly less during midstance. Lateral muscle
activation was the
greatest contributor to the co-contraction index
SM:BF (% MVIC) OA group exhibited greater co-contraction during
loading, early and midstance.BF activation was the major
contributor to the co-contraction index.
Knee exors: knee extensors
(SM, BF, MG, LG:VL, VM, RF %
MVIC)
OA group exhibited greater co-contraction during midstance.
There was no
difference between groups during loading and early stance.
Hortobgyi et al. (2005) 200 ms prior to IC to toe-off General OA
Control
BF:VL (% MVIC) 41.0 (23.85 to 58.15) ES 1.26
LG:TA (% MVIC) 40 (15.95 to 64.05) ES 0.9
Hubley-Kozey et al.
(2009)
100 ms prior to IC to peak KAM
VL:BF (% MVIC) Moderate Control 10.17 (4.39 to 15.94) ES
0.66
Sever e Control 23 .49 (17 .07 to 2 9.9) ES 1.52
Moderate Severe 13.32 (21.52 to 5.12) ES 0.62
VL:LG (% MVIC) Moderate Control 2.16 (0.69 to 5.02) ES 0.28
Severe Con trol 9. 57 (5.72 to 13.42) ES 1.01
Moderate Severe 7.41 (11.68 to 3.14) ES 0.68
VM:SM (% MVIC) Moderate Control 4.46 (0.73 to 9.65) ES 0.32
Severe Con trol 7. 6 (3.26 to 11.94) ES 0.32
Moderate Severe
3.14 (
9.05 to 2.77) ES
0.2VM:MG (% MVIC) Moderate Control 1.22 (1.27 to 3.71) ES
0.18
Severe Control 6.88 (10.21 to 3.64) ES 0.85
Moderate Severe 5.66 (9.26 to 2.06) ES 0.61
Lewek et al. (2004) 100 ms prior to IC to peak KAM
VL:BF (% MVIC) Moderate
(varus and lax)
Con tro l 5.7 (2.55 to 13.95) ES0.53
VL:LG (% MVIC) 2.8 (3.21 to 8.81) ES 0.36
VM:SM (% MVIC) 0.4 (7.13 to 6.33) ES 0.05
VM:MG (% MVIC) 6.3 (0.5 to 12.1) ES 0.84
Lewek et al. (2006) Preparation Moderate
(varus and lax)
Control
VL:BF (% MVIC) 4.6 (2.63 to 11.83) ES 0.44
VL:LG (% MVIC) 2.9 (2.9 to 8.7) ES 0.35
VM:SM (% MVIC) 0.7 (6.24 to 4.84) ES 0.09
VM:MG (% MVIC) 6.2 (1.01 to 11.39) ES 0.83
Liikavainio et al. (2010) VM: BF (% Max) G eneralOA (var us) C
ontrol No d ifferenc e between groups
Rudolph et al. (2007) 100 ms prior to IC to peak KAM Moderate
(varus) Control No difference between groups
VL:BF (% MVIC)VL:LG (% MVIC)
VM:SM (% MVIC)
VM:MG (% MVIC)
Schmitt and Rudolph
(2007)
Preparation and weight
acceptance
Mild
(varus and lax)
Control
VL:BF (% Max) No difference between groups
VL:LG (% Max) OA group exhibited a trend towards greater
co-contraction during preparation
and signicantly higher co-contraction during weight
acceptance.
VM:SM (% Max) OA group exhibited a trend towards greater
co-contraction during preparation
and signicantly higher co-contraction during weight
acceptance.
VM:MG (% Max) No difference between groups
Midstance OA group exhibited higher co-contraction for all
muscles
Zeni et al. (2010) VL:SM (% MVIC) (1.0 m/s) Moderate Control
12.4 (5.81 to 18.99) ES 1.29
Severe Control 11.5 (2.21 to 20.79) E S 1.33
Moderate Severe 0.9 (9.91 to 11.71) ES 0.07
VL:SM (% MVIC) (PW) Moderate Control 11.7 (4.81 to 18.59) E S
1.16
Severe Control 6.8 (2.51 to 16.11) ES 0.75Moderate Severe 4.9
(5.85 to 15.65) ES 0.37
VL:SM (% MVIC) (FW) Moderate Control 14.4 (5. 27 to 23.53) ES
1.08
Severe Control 6.2 (2.24 to 14.64) ES0.72
Moderate Severe 8.2 (3.41 to 19.81) ES 0.5
Muscle amplitude
Astephen et al. (2008) Gastrocnemius (LG, MG % MVIC) Moderate
Control No difference between groups
Severe C ontrol No d if ferenc e between groups
Moderate Severe Severe OA group exhibited higher mean MG
amplitude in early stance and in
swing phase and lower mean amplitude in late stance.
Quadriceps (VL, VM, RF % MVIC) Moderate Control Mean RF
amplitude was higher in moderate OA group throughout the
majority
of stance and late swing.
Severe Control Mean RF amplitude was lower in severe OA group
during early stance and early
swing but higher mean amplitude in mid to late stance.
Moder ate Sever e No d if ferenc e between groups
(continued on next page)
721K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
10/12
Table 3(continued)
Authors Variable Knee OA Comparator Result/mean difference (95%
CI) and effect size (ES)
Hamstrings (BF, SM % MVIC) Moderate Control No difference
between groups
Severe Control Mean SM and BF amplitude was higher in severe OA
group during stance.
Moderate Severe No difference between groups
Heiden et al. (2009) Net muscle activity of
BF, SM, VL, RF, VL, MG, LG (%
MVIC)
General OA Control OA group exhibited signicantly greater net
muscle activation during weight
acceptance and early stance compared with controls
Hortobgyi et al.
(2005)
BF (% of MVIC) General OA Control 47 (28.18 to 65.82) ES
1.27
VL (% of MVIC) 47 (20.53 to 59.47) ES 1.09
Hubley-Kozey et al.
(2006)
Gastrocnemius (MG, LG % MVIC) Moderate Control Mean MG amplitude
was decreased in OA group and peak amplitude occurred
earlier in gait cycle. The control group recruited MG more than
LG, whereas OA
group recruited both muscles equally.
Quadriceps (RF, VL, VM % MVIC) Mean VL amplitude was higher in
OA group during initial stance and there was a
trend towards higher mean RF amplitude. Mean VM amplitude was
similar
between OA and controls.
Hamstrings (BF, SM % MVIC) Mean B F amplitude w as h igher a nd
p eak a mplitude o ccurred p rior t o heel s trike i n
OA group compared with controls. Mean BF amplitude was higher
than SM for
both groups.
Liikavainio et al.
(2010)
BF (% Max) General OA Control OA group exhibited signicantly
higher mean BF amplitude at IC, except when
walking fast.
VM (% Max) Mean VM amplitude in late stance and early swing were
signicantly greater in
the OA group for all gait speeds
Rudolph et al. (2007) VL, VM, BF, SM LG, MG (% MVIC)
Moderate
(varus)
Control Tendency towards greater mean MG activity in the OA
group. No other difference
between groups.
Rutherford et al.
(2010)
Gastrocnemius (MG, LG % MVIC) Moderate Control OA group
exhibited moderately less difference between early and late
stance
activity than controls for MG activity (ES 0.68) and a moderate
tendency ofsmaller difference in LG activity (ES 0.63)
Quadriceps (VL, VM, RF % MVIC) OA group exhibited large
reduction in difference between mid and late stance
amplitude for RF (ES 1.2) and small tendency towards smaller
difference
between mid and late stance amplitude for VL and VM (ES 0.59,
0.55). RF
differential was moderately less than VM in OA group (ES 0.64),
and large
reduction compared with VL (ES 1.8) and VM (ES 1.71) in control
group.
Ha mstrings ( BF, SM % MVI C) OA group exhib ited which w as m
od erately great er overall a mp litu de of B F than
SM (ES 1.09). OA group SM amplitude differential between early
stance and late
swing versus midstance was moderately greater than control group
(ES 0.86)
Rutherford et al.
(2011)
Gastrocnemius (MG, LG % MVIC) Moderate Control OA group
exhibited moderately smaller difference between early and late
stance
amplitude (ES 0.83)
Severe Control OA group exhibited large reductions in late
stanceearly stance amplitude
differential for MG (ES 1.26) and LG (ES 1.21)
Severe Moderate Moderate OA group exhibited moderately greater
mean MG amplitude (ES 0.74)
and moderately larger difference between early and latestance
amplitude (ES 0.91).
Quadriceps (RF, VM, VL % MVIC) Severe Control
DifferenceinRFamplitudebetweenearlyandmidlatestancewas
moderatelylower
in OA group (ES 0.89). Difference between mid
late stance and swing phaseamplitude was moderately higher in OA
group for VL (ES 0.82) and RF (ES 0.83).
Moderate Severe No difference in mean amplitude. Severe group
exhibited moderately greater
difference between midlate stance and swing phase VL amplitude
compared
with moderate group (ES 0.83)
Hamstrings (BF, SM % MVIC) Moderate Control OAgroup exhibited
moderate reduction inmean SMamplitude duringmidstance
and late swing burst (P= 0.05, ES 0.69).
Severe Control OAgroup exhibited large reductionsin mean
BFamplitude duringmidstance and
late swing burst (P= 0.00, ES 1.46).
Moderate Severe Moderate group exhibited moderately lower BF
mean amplitude during
midstance and late swing burst (P= 0.04, ES 0.73)
Schmitt and Rudolph
(2007)
VL (% Max) Mild (varus and
lax)
C ontrol Signicantly greater mean amplitude in OA group during
midstance
VM (% Max) Signicantly greater mean amplitude in OA group during
weight acceptance and
midstance
BF (% Max) Trend towards greater mean amplitude in OA group
during preparation,
signicantly greater mean amplitude during midstance
SM (% Max) Signicantly greater mean amplitude in OA group during
weight acceptance
LG (% Max) Trend towards greater mean amplitude in OA group
during preparation,
signicantly greater mean amplitude during weight acceptance
MG (% Max) No difference between groups
Sol (% Max) No difference between groups
Zeni et al. (2010) VL (mean % MVIC) (1.0 m/s) Moderate Control
16 (7.06 to 24.94) ES 1.24
Severe Control 10.3 (1.5 to 19.1) E S 1.29
Moderate Severe 5.7 (6.46 to 17.86) ES 0.34
V L (mean % MVI C) ( PW) Mod erate C ontrol 15 .5 ( 6.06 to 24.4
9) ES1 .14
Severe Control 8.9 (1.02 to 18.82) ES 1.02
Moderate Severe 6.6 (6.78 to 19.98) ES 0.37
V L (mean % MVI C) ( FW ) Mod erate C ontrol 18.4 ( 5.21 to 31
.5 9) ES 0 .9 7
Severe Control 1.7 (5.7 to 9.1) ES 0.27
Mod erate Severe 16.7 ( 2.28 to 31 .1 2) ES0 .73
VL (peak % MVIC) (1.0 m/s) Moderate Control 26.8 (10.99 to
42.61) ES 1.18
Severe Control 21.2 (6.29 to 36.11) ES 1.55
Moderate Severe 5.6 (15.45 to 26.65) ES 0.19
Muscle amplitude
Astephen et al. (2008)
722 K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
11/12
included in this review, no conclusions can be drawn regarding
the in-
teraction between the potentially negative effects of increased
medial
knee muscle and RF activity and the potential positive effects
of in-creased lateral activity. Future research is needed to
determine how
this interaction affects KOA progression.
Along with the inability to draw conclusions regarding
inuenceson
the progression of KOA, there are several additional limitations
of this
review. The primary methodological concern of the studies
included
in this review was poor external validity specically a lack
of
reporting sampling methods and demonstrating that the people
who
participated in the study are representative of the population
they
were selected from. This makes generalizing results beyond
individuals
who meet specic inclusion criteria difcult. Another
methodological
issue was the variety of formulas used to calculate
co-contraction indi-
ces highlighting the numerous methods to achieve a single
number.
As such, interpretation of this index is difcult unless there is
also an in-
vestigation into how this number is reached. The relative
contributions
of muscles involved in any co-contraction formula are of
particular in-
terest to clinicians, particularly if the ratio contains both
medial and lat-
eral muscle contributions. Some studies explore this (Heiden et
al.,2009; Hubley-Kozey et al., 2009; Zeni et al., 2010) and future
studies
would benet from similar exploration.
An interesting issue in interpreting the validity of thendings
of this
review is that the majority of studies normalized their
neuromotor data
to MVIC. Normalizing EMGdata to MVIC provides information
regarding
the relative degree of muscle activation and facilitates
comparisons be-
tween groups. However, in injured and post-operativepatients,
the abil-
ity to perform an MVIC can be affected by pain (Arvidsson et
al., 1986;
Benoit et al., 2003). In KOA cohorts, higher pain levels and
lower physi-
cal function have been associated with increased neuromotor
activity
independent of radiographic disease severity (Heiden et al.,
2009;
Wilson et al., 2011). Thus, individuals with KOA may not be able
to pro-
duce an accurate MVIC and subsequent signicant differences in
neuro-
muscular activity may be erroneous. Conversely, reported
increases in
Table 3(continued)
Authors Variable Knee OA Comparator Result/mean difference (95%
CI) and effect size (ES)
VL ( peak % MVIC) (PW) Moder ate Control 23 .7 (7.31 to 40 .0 2)
ES 1 .0 1
Severe Control 16.1 (1.69 to 33.89) ES 1.0
Moderate Severe 7.6 (15.75 to 30.95) ES 0.24
VL ( peak % MVIC) (FW) Moder ate C ontrol 40 .20 (14 .31 to 6
6.09 ) ES 1.08
Severe Control 1.4 (11.54 to 14.34) ES 0.09
Moder ate Sever e 38 .8 (11.21 to 6 6.39) ES 0.86
SM (mean % MVIC) (1.0 m/s) Moderate Control 8.9 (1.64 to 16.16)
ES 0.84
Severe Control 10.9 (0.09 to 21.89) ES 1.1
Moderate Severe 2.0 (14.63 to 10.63) ES 0.13
SM (mean % MVI C) ( PW) Moder ate C ontrol 8.0 (2 .18 to 1 3.82
) ES 0 .92
Severe Control 10.0 (5.02 to 25.02)
Moderate Severe 2.0 (17.49 to 13.49) ES 0.13
SM (mean % MVI C) ( FW) Moder ate Control 8.6 (1.3 9 to 1 5.81 )
ES 0 .81
Severe Control 8.8 (1.96 to 19.56) ES 0.84
Moderate Severe 0.2 (12.19 to 11.79) ES 0.01
SM (peak % MVIC) (1.0 m/s) Moderate Control 16.5 (4.7 to 28.3)
ES 0.96
S ev ere Control 17.5 (2.78 to 32.22) ES 1.25
Moderate Severe 1.0 (18.84 to 16.84) ES 0.04
SM (peak % MVI C) ( PW) Mod er ate Control 14 .7 (2.53 to 26 .8
7) ES 0.8 1
Severe Control 18.8 (8.19 to 45.79) ES 0.76
Moderate Severe 4.1 (32.11 to 23.91) ES 0.15
SM (peak % MVIC) (FW) Moderate Control 12.7 (1.0 to 26.40) ES
0.62
Severe Control 13.3 (1.66 to 28.26) ES 0.75
Moderate Severe 0.6 (17.7 to 16.5) ES 0.03
Muscle activity duration
Astephen et al. (2008) Gastrocnemius (MG) Moderate Control MG
was active for the majority of the gait cycle in severe OA group
whereas
moderate
Sever e OA group and c ontr ols exhibited MG ac tivity during
late stance.
Childs et al. (2004) VL (ms) General OA Control 165 (82.98 to
247.02) ES 1.12
SM (ms) 167 (99.89 to 234.11) ES 1.38
TA (ms) 158 (108.92 to 207.08) ES 1.79
MG (ms) 140 (59.27 to 220.73) ES 0.97
Hubley-Kozey et al.
(2006)
Gastrocnemius (MG, LG) Moderate Control There was no difference
in temporal characteristics of LG or MG.
Quadriceps (RF, V L, VM) VL and RF a ctivities wer e prolonged
during mid- to lat e-sta nce. T here wa s no
change in temporal characteristics for VM.
Hamstrings (BF, S M) BF activity was highe r and prolon ged in
OA group compared with con trols. BF
activity was higher than SM for both groups.
Rutherford et al. (2010) Gastrocnemius (MG, LG) Moderate Control
No phase differences between groups for MG and LG
Quadriceps (VL, VM, RF) No phase shift between groups for VL, VM
and RF
Hamstrings (BF, SM) Duration o f BF and SM activities w as
moderately p rolonged in O A group compared
with controls (ES 1.16 and 0.91)
Rutherford et al. (2011) Gastrocnemius (MG, LG % MVIC) Moderate
Control MG onset was moderately earlier than LG onset for both
groups (OA:ES 1.18.
Control:ES 1.01).
Severe Control OA group exhibited moderately later MG onset
compared with controls (ES 1.1)
Moderate Severe Severe group exhibited largely later MG onset
than moderate group (ES1.2)
BF: biceps femoris, LG: lateral gastrocnemius, MG: medial
gastrocnemius, RF: rectus femoris, SM: semimembranosis, Sol:
soleus, TA: tibialis anterior, VL: vastus medialis, VM: vastus
medialis.
IC: initial contact, ms: milliseconds, MVIC: maximum isometric
voluntary contraction, m/s: meters per second, FW: fast walking,
PW: preferred walking speed, KAM: peak external knee
adduction moment.
Preparation: 100 ms prior to heel strike until initial
contact.
Weight acceptance: initial contact until single leg stance.
Muscle amplitude
Zeni et al. (2010)
723K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
-
8/10/2019 A Systematic Review and Meta-Analysis of Lower Limb
Neuromuscular Alteration Associates With Knee Osteoarthri
12/12
neuromotor activity may be due to those with more severe KOA
reporting higher pain levels than moderate or healthy
counterparts
rather than the radiographic severity of their diagnosis.
Further investi-
gation is needed into the association between pain, KOA severity
and
neuromuscular control during gait.
5. Conclusion
Pooled and non-pooled data from moderate quality
observationalstudies demonstrate individuals with KOA exhibit
altered lower limb
neuromuscular activity during gait compared with healthy
controls. In-
dividuals with KOA exhibited increased co-contraction, amplitude
and
duration of lateral knee muscles regardless of their disease
severity,
lower limb alignment or medial knee joint laxity. Neuromuscular
activ-
ity of RF was also increased and prolonged for many KOA cohorts
and
medial knee muscle activity was also increased. Based on current
evi-
dence, this suggests thatindividuals with KOAare adopting
neuromotor
patterns during gait that have the potential to protect the
medial knee
joint. However, those with severe disease or medial knee joint
laxity
and/or varus alignment are also exhibiting neuromuscular
patterns
that increase the risk of accelerated medial compartment
degeneration.
In some instances, both potentially protective and potentially
degener-
ative neuromuscular pattern occur simultaneously. Therefore,
while re-
sults of this review suggest neuromuscular rehabilitation
focusing on
increasing lateral muscle activity and down-regulating medial
muscle
and RF activity shows promise as way of potentially slowing this
pro-
gression, future research into the efcacy of such a program is
needed.
Such research needs to further investigate how simultaneous
up-
regulation in medial and lateral knee muscle activities inuences
dis-
ease progression and should also consider metrics of pain and
function
when comparing individuals with KOA.
Acknowledgments
Kathryn Mills is supported by Alberta Innovates Health
Solutions
Team in Osteoarthritis #200700596. Ryan Leigh is supported by
Alberta
Innovates Health Solutions Clinical Fellowship #201200131. The
au-
thors declare no conicts of interest.
References
Arvidsson, I., Eriksson, E., Knutsson, E., Arner, S., 1986.
Reduction of pain inhibition onvoluntary muscle activation by
epidural analgesia. Orthopedics 9, 14151419.
Astephen, J.L., Deluzio, K.J., Caldwell, G.E., Dunbar, M.J.,
Hubley-Kozey, C.L., 2008. Gait andneuromuscular pattern changes are
associated with differences in knee osteoarthritisseverity levels.
J. Biomech. 41, 868876.
Benoit, D.L., Lamontagne, M., Cerulli, G., Liti, A., 2003.The
clinical signicance of electro-myography normalisation techniques
in subjects with anterior cruciate ligamentinjury during treadmill
walking. Gait Posture 18, 5663.
Bombardier, C., Hawker,G., Mosher, D., 2011.The impactof
arthritis in Canada:today andover the next 30 years (no. fall).
Arthritis of Canada Alliance.
Childs, J.D., Sparto, P.J., Fitzgerald, G.K., Bizzini, M.,
Irrgang, J.J., 2004.Alterations in lowerextremity movement and
muscle activation patterns in individuals with knee
osteo-arthritis. Clin. Biomech. 19, 4449.
Coombes, B.K., Bisset,L., Vicenzino, B.,2010. Efcacy andsafetyof
corticosteroid injectionsand other injections for management of
tendinopathy: a systematic review ofrandomised controlled trials.
Lancet 376, 17511767.
Downs, S.H., Black, N., 1998. Thefeasibility of creatinga
checklist forthe assessmentof themethodological quality both of
randomised and non-randomised studies of healthcare interventions.
J. Epidemiol. Community Health 52, 377384.
Heiden, T.L., Lloyd, D.G., Ackland, T.R., 2009. Knee joint
kinematics, kinetics and muscleco-contraction in knee
osteoarthritis patient gait. Clin. Biomech. 24, 833841.
Higgins, J.P.T., Thompson, S.G., Deeks, J.J., Altman, D.G.,
2003. Measuring inconsistency inmeta-analyses. BMJ 327, 557560.
Hodges, P.W., vander Hoorn,W., Bennell, K.,Wrigley, T.V., 2012.
Rate of cartilage loss in me-dial knee osteoarthritis is faster in
patients with increased duration of cocontraction ofmedial knee
muscles. JOSPT A41.
Hopkins, W.G., 2000. A New View of Statistics [WWW Document].
wwwsportsciorg/
resource/stat(URL (accessed 10.6.12)).Hopkins, W.G., Marshall,
S.W., Batterham, A.M., Hanin, J., 2009.Progressive statistics
forstudies in sports medicine and exercise science. Med. Sci.
Sports Exerc. 41, 313.
Hortobgyi, T., Westerkamp, L., Beam, S., Moody, J., Garry, J.,
Holbert, D., Devita, P., 2005.Altered hamstring-quadriceps muscle
balance in patients with knee osteoarthritis.Clin. Biomech. 20,
97104.
Hubley-Kozey, C., Deluzio, K., Landry, S., McNutt, J., Stanish,
W., 2006. Neuromuscular alter-ations during walking in persons with
moderate knee osteoarthritis. J. Electromyogr.Kinesiol. 16,
365378.
Hubley-Kozey,C.L., Hill,N.A., Rutherford,D.J., Dunbar, M.J.,
Stanish, W.D., 2009. Co-activationdifferences in lower limb muscles
between asymptomatic controls and thosewith varying degrees of knee
osteoarthritis during walking. Clin. Biomech. 24,407414.
Hurely, M.V., 1999. The role of muscle weakness in the
pathogenesis of osteoarthritis.Rheum. Dis. Clin. N. Am. 25,
283298.
Kamen, G., Caldwell, G.E., 1996. Physiology and interpretation
of the electromyogram.J. Clin. Neurophysiol. 13, 366384.
Lewek, M.D., Rudolph, K.S., Snyder-Mackler, L., 2004.Control of
frontal plane knee laxityduring gait in patients with medial
compartment knee osteoarthritis. Osteoarthr.
Cartil. 12, 745751.Lewek, M.D., Scholz, J., Rudolph, K .S.,
Snyder-Mackler, L., 2006.Stride-to-stride variability
of knee motion in patients with knee osteoarthritis. Gait
Posture 23, 505511.Liikavainio, T., Bragge, T., Hakkarainen, M.,
Karjalainen, P.A., Arokoski, J.P., 2010.Gait and
muscle activation changes in men with knee osteoarthritis. Knee
17, 6976.Munn, J., Sullivan, S.J., Schneiders, A.G., 2010.Evidence
of sensorimotor decits in functional
ankle instability: a systematic review with meta-analysis. J.
Sci. Med. Sport. 13, 2 12.Ouellet, D., Moffet, H.L.N., 2002.
Locomotor decits before and two months after knee
arthroplasty. Arthritis Rheum. 47, 484493.Rudolph, K.S.,
Schmitt, L.C., Lewek, M.D., 2007.Age-related changes in strength,
joint lax-
ity, and walking patterns: are they related to knee
osteoarthritis? Phys. Ther. 87,14221432.
Rutherford, D.J., Hubley-Kozey, C.L., Stanish, W.D., 2010.The
neuromuscular demands ofaltering foot progression angle during gait
in asymptomatic individuals and thosewith knee osteoarthritis.
Osteoarthr. Cartil. 18, 654661.
Rutherford, D.J., Hubley-Kozey, C.L., Stanish, W.D., Dunbar,
M.J., 2011. Neuromuscular al-terations exist with knee
osteoarthritis presence and severity despite walking veloc-ity
similarities. Clin. Biomech. 26, 377383.
Schipplein, O.D., Andriacchi, T.P., 1991. Interaction between
active and passive kneestabi-lizers during level walking. J.
Orthop. Res. 9, 113119.
Schmitt, L.C., Rudolph, K.S., 2007. Inuences on kneemovement
strategies during walkingin persons with medial knee
osteoarthritis. Arthritis Rheum. 57, 10181026.
Schmitt, L.C., Rudolph, K.S., 2008. Muscle stabilization
strategies in people with medialknee osteoarthritis: the effect of
instability. J. Orthop. Res. 26, 11801185.
Sharma, L., Hayes, K.W., Felson, D.T., Buchanan, T.S.,
Kirwan-Mellis, G., Lou, C., Pai, Y.C.,Dunlop, D.D., 1999.Does
laxity alter the relationship between strength and physicalfunction
i n knee osteoarthritis? Arthritis Rheum. 42, 2532.
Simic, M., Hinman, R.S., Wrigley, T.V., Bennell, K.L., Hunt,
M.A., 2011. Gait modicationstrategies for altering medial knee
joint load: a systematic review. Arthritis CareRes. 63, 405426.
van Tulder, M., Furlan, A., Bombardier, C., Bouter, L.,
Editorial Board of the CochraneCollaboration Back Review Group,
2003.Updated method guidelines for systematicreviews in the
Cochrane Collaboration Back Review Group. Spine 28, 12901299.
Wilson, J.L.A., Deluzio, K.J., Dunbar, M.J., Caldwell, G.E.,
Hubley-Kozey, C.L., 2011.Theassociation between knee joint
biomechanics and neuromuscular control andmoderate knee
osteoarthritis radiographic and pain severity. Osteoarthr.
Cartil.19, 186193.
Zeni, J.A., Rudolph, K., Higginson, J.S., 2010.Alterations in
quadriceps and hamstrings co-ordination in persons with medial
compartment knee osteoarthritis. J. Electromyogr.Kinesiol. 20,
148154.
724 K. Mills et al. / Clinical Biomechanics 28 (2013) 713724
http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0160http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0160http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0160http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0160http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0165http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0165http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0035http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0035http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0035http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0035http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0040http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0040http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0040http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0040http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0170http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0170http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0170http://wwwsportsciorg/resource/stathttp://wwwsportsciorg/resource/stathttp://refhub.elsevier.com/S0268-0033(13)00164-2/rf0050http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0050http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0050http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0050http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0055http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0055http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0055http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0055http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0070http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0070http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0070http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0070http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0075http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0075http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0075http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0075http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0090http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0090http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0090http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0090http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0120http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0120http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0120http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0120http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0130http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0130http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0130http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0130http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0135http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0135http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0135http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0135http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0180http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0180http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0180http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0180http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0155http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0150http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0180http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0180http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0140http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0135http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0135http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0130http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0130http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0125http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0120http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0120http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0115http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0110http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0105http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0100http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0095http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0090http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0090http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0085http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0080http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0075http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0075http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0070http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0070http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0065http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0060http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0055http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0055http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0050http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0050http://wwwsportsciorg/resource/stathttp://wwwsportsciorg/resource/stathttp://refhub.elsevier.com/S0268-0033(13)00164-2/rf0170http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0170http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0170http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0040http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0040http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0035http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0035http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0030http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0025http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0020http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0165http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0165http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0015http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0010http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0160http://refhub.elsevier.com/S0268-0033(13)00164-2/rf0160