Embed Size (px)
Citation preview

Abdominal Pain and Bowel Obstruction
Mike GoodwinMike Goodwin
CRASH CourseCRASH Course
October, 2010October, 2010

Abdominal Pain - Approach
HistoryHistory PhysicalPhysical LabsLabs ImagingImaging Provisional DxProvisional Dx

History
PQRST AAA etxPQRST AAA etx But don’t forgetBut don’t forget
PSxPSx Bowel/Gyne/Urol ROSBowel/Gyne/Urol ROS




Physical Exam
CompleteComplete General appearance/vitals/H+N/ChestGeneral appearance/vitals/H+N/Chest Abdo:Abdo:
RigidityRigidity ReboundRebound GuardingGuarding IPPAIPPA DRE / Pelvic / Groin / Flank-CVADRE / Pelvic / Groin / Flank-CVA

Labs
Everyone:Everyone: CBC, lytes BUN CrCBC, lytes BUN Cr LFT, Bili, Amylase/Lipase, lactateLFT, Bili, Amylase/Lipase, lactate UrinalysisUrinalysis Urine PregUrine Preg

Imaging
AXRAXR 3-views3-views Free airFree air Distended bowel/air-fluidDistended bowel/air-fluid Calcifications (panc or kidney/ureter)Calcifications (panc or kidney/ureter)
USUS If GS disease suspectedIf GS disease suspected Lower abdo pain in femaleLower abdo pain in female

Imaging
CT AbdoCT Abdo Test of choice for most patientsTest of choice for most patients Protocols to minimize contrast Protocols to minimize contrast
nephropathynephropathy
Bowel Obstruction: Overview
HistoryHistory EtiologyEtiology PathophysiologyPathophysiology Clinical presentationClinical presentation ImagingImaging ManagementManagement Special considerationsSpecial considerations

Causes of Small Bowel Obstruction in Adults
Lesions Extrinsic to the Intestinal Lesions Extrinsic to the Intestinal WallWall
Lesions Intrinsic to the Intestinal Lesions Intrinsic to the Intestinal WallWall
Intraluminal/Obturator ObstructionIntraluminal/Obturator Obstruction

Lesions Extrinsic to the Intestinal Wall
Adhesions (usually postoperative) Adhesions (usually postoperative) Neoplastic Neoplastic
Carcinomatosis Carcinomatosis Extraintestinal neoplasms Extraintestinal neoplasms
Hernia Hernia External (e.g., inguinal, femoral, umbilical, or ventral External (e.g., inguinal, femoral, umbilical, or ventral
hernias) hernias) Internal (e.g., congenital defects such as paraduodenal, Internal (e.g., congenital defects such as paraduodenal,
foramen of Winslow, and diaphragmatic hernias or foramen of Winslow, and diaphragmatic hernias or postoperative secondary to mesenteric defectspostoperative secondary to mesenteric defects
Intra-abdominal abscessIntra-abdominal abscess

Lesions Intrinsic to the Intestinal Wall
Congenital Congenital Malrotation Malrotation Duplications/cysts Duplications/cysts
Inflammatory Inflammatory Crohn’s disease Crohn’s disease Infections Infections
Tuberculosis Tuberculosis Actinomycosis Actinomycosis DiverticulitisDiverticulitis
Neoplastic Neoplastic Primary neoplasms Primary neoplasms Metastatic neoplasmsMetastatic neoplasms
Traumatic Traumatic Hematoma Hematoma Ischemic strictureIschemic stricture
Miscellaneous Miscellaneous Intussusception Intussusception Endometriosis Endometriosis Radiation Radiation
enteropathy/strictureenteropathy/stricture

Intraluminal/Obturator Obstruction
GallstoneGallstone
EnterolithEnterolith
BezoarBezoar

Common causes of small bowel
obstruction in industrialized countries.

Pathophysiology Early: Increased motility & contractilityEarly: Increased motility & contractility
• Bowel dilation, fluid/lytes accumulate in lumen and bowel wall
• Third spacing, intravascular volume depletion

Bowel obstruction
Increased intraluminal pressure
Decreased mucosal blood flow
Progressive Ischemia
Perforation & Peritonitis
Clinical Diagnosis
HistoryHistory Colicky abdominal painColicky abdominal pain Nausea / vomitingNausea / vomiting Abdominal distensionAbdominal distension Failure to pass flatus / fecesFailure to pass flatus / feces

Physical Examination Vitals: Tachycardia, hypotensionVitals: Tachycardia, hypotension Abdomen:Abdomen:
DistensionDistension Surgical scarsSurgical scars Bowel sounds, increased or decreasedBowel sounds, increased or decreased Localized tenderness / rebound / guarding Localized tenderness / rebound / guarding
suggests strangulationsuggests strangulation Hernia exam (ventral, groin, etc)Hernia exam (ventral, groin, etc)
Rectal exam:Rectal exam: Rectal massesRectal masses Blood – suggesting ischemia, malignancyBlood – suggesting ischemia, malignancy

Radiology
Plain Abdo X-RaysPlain Abdo X-Rays Confirm DiagnosisConfirm Diagnosis Localize obstruction to small bowel or Localize obstruction to small bowel or
coloncolon Evidence of complete or incompleteEvidence of complete or incomplete


Plain X-ray Features
Dilated Small Bowel (>3 cm)Dilated Small Bowel (>3 cm) Multiple air-fluid levelsMultiple air-fluid levels Colonic gas patternColonic gas pattern
Normal / Dilated (Ileus or partial Normal / Dilated (Ileus or partial obstruction)obstruction)
Absence of gas c/w complete obstructionAbsence of gas c/w complete obstruction *Thickened bowel wall*Thickened bowel wall *Pneumatosis intestinalis*Pneumatosis intestinalis
**Suggests ischemia/strangulationSuggests ischemia/strangulation

Plain X-rays Lappas Lappas et al 2001 et al 2001 RRevieweview of of 12 12 AXR AXR findings with SBOfindings with SBO Findings:Findings: CCombination of ombination of
AAir-fluid levels of different heights in the ir-fluid levels of different heights in the samesame bowel loop bowel loop
MMean air-fluid level diameter of 2.5 cm or ean air-fluid level diameter of 2.5 cm or greater greater
MMost predictive of a high-grade partial or ost predictive of a high-grade partial or complete SBOcomplete SBO

AXR Disadvantages
20-30% false negative rate20-30% false negative rate Does not localize site of obstructionDoes not localize site of obstruction Does not establish etiology of Does not establish etiology of
obstructionobstruction

CT Scan 95% sensitive95% sensitive 96% specific96% specific 95% accurate in determining the 95% accurate in determining the
presence of complete or high-grade presence of complete or high-grade SBOSBO
ShowsShows site and cause of obstruction in site and cause of obstruction in 95% of instances95% of instances
Less accurate for partial SBO (50% Less accurate for partial SBO (50% some studies)some studies)

CT for SBO
CT performed with CT performed with IV and PO IV and PO contrastcontrast HHigh-grade SBOigh-grade SBO seen even with no seen even with no
contrastcontrast Lesser Lesser grades of obstruction grades of obstruction seen seen with with
PO PO contrast contrast IV IV contrast contrast for for assessment of bowel assessment of bowel
wall for signs of edema or ischemia. wall for signs of edema or ischemia.

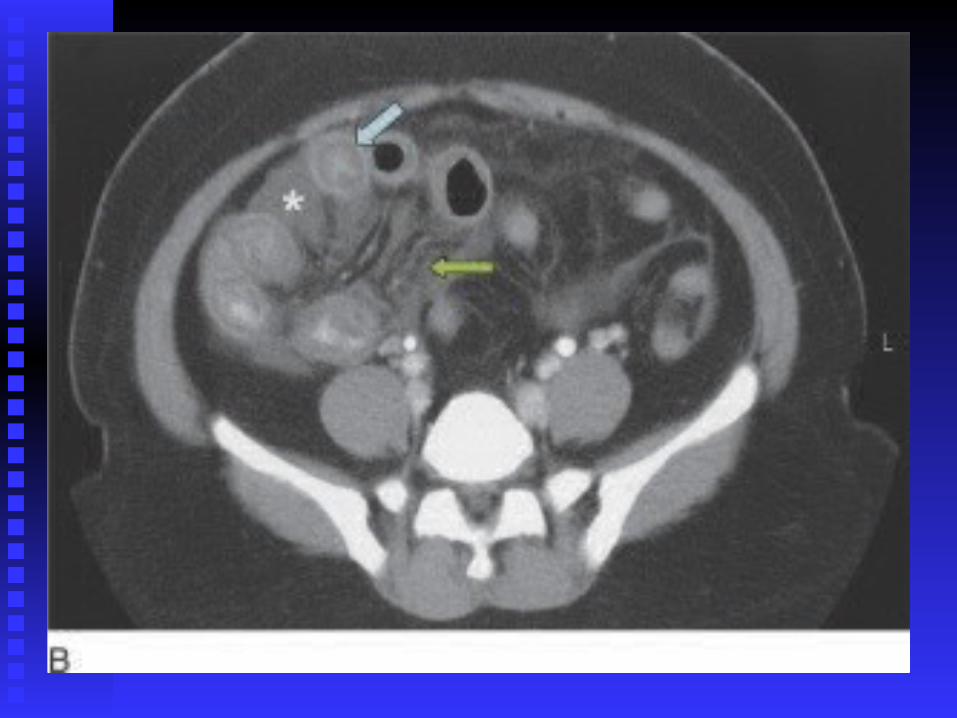
CT Findings in Patients with Small Intestinal Obstruction
Type of ObstructionType of Obstruction FindingsFindings
Simple obstruction, Simple obstruction, partial or completepartial or complete
Proximal bowel dilatationProximal bowel dilatationDDiscrete transition zone iscrete transition zone with collapsed distal small with collapsed distal small bowel bowel NNo passage of oral o passage of oral contrast beyond the contrast beyond the transition zonetransition zoneLittle gas or fluid in colonLittle gas or fluid in colon


CT Findings in Patients with Small Intestinal Obstruction
Type of ObstructionType of Obstruction FindingsFindings
Closed-loop obstructionClosed-loop obstructionBowel Wall ChangesBowel Wall Changes U-shaped, distended, U-shaped, distended,
fluid-filled bowel loopfluid-filled bowel loopWhirl signWhirl signBeak signBeak sign
Mesenteric ChangesMesenteric Changes RadialRadial distribution dilated distribution dilated bowel loops bowel loops TThickened mesenteric hickened mesenteric vessels converging toward vessels converging toward point of obstructionpoint of obstruction


CT Findings in Patients with SBOType of ObstructionType of Obstruction FindingsFindings
Strangulated ObstructionStrangulated ObstructionBowel Wall ChangesBowel Wall Changes Bowel wall thickeningBowel wall thickening
Target signTarget signPneumatosis intestinalisPneumatosis intestinalisDec. bowel Dec. bowel wall wall enhancementenhancement
Mesenteric ChangesMesenteric Changes BBlurring of mesenteric lurring of mesenteric vessels vessels OObliteration of mesentery bliteration of mesentery andand vessels vessels EEngorgement of ngorgement of mesenteric vasculaturemesenteric vasculature
OtherOther AscitesAscites
When to Order CT?
CClinical presentation or abdominal films linical presentation or abdominal films nondiagnosticnondiagnostic
Hx of Hx of abdominal malignancyabdominal malignancy Immediate pImmediate postsurgical patientsostsurgical patients PPatients who have no history of atients who have no history of
abdominal surgery abdominal surgery

Barium / Contrast Studies
HHistory of recurring obstruction istory of recurring obstruction LLow-grade mechanical obstruction ow-grade mechanical obstruction DDefineefiness the obstructed segment and the obstructed segment and
degree of obstructiondegree of obstruction

Gastrograffin Swallow in Adhesive SBO, Cochrane
Review, 2004 DiagnosticDiagnostic
Gastrofraffin seen Gastrofraffin seen in the cecum on in the cecum on AXR AXR within 24 hours predicts resolution within 24 hours predicts resolution
SSensitivity of 0.96, specificity of 0.96ensitivity of 0.96, specificity of 0.96 TherapeuticTherapeutic
Hospital length of stay 2-3 days shorter in Hospital length of stay 2-3 days shorter in non-operative patientsnon-operative patients
Studies prospective, non-blindedStudies prospective, non-blinded

Simple Versus Strangulating Obstruction
Classic signs:Classic signs: FeverFever WBC incWBC inc Constant Abdo painConstant Abdo pain
But no parameters reliably detect But no parameters reliably detect strang.strang.
CT findings detect CT findings detect latelate ischemic ischemic changeschanges

Treatment – Nonoperative Fluid resuscitationFluid resuscitation
IV resuscitation with isotonic salineIV resuscitation with isotonic saline Electrolyte replacementElectrolyte replacement Monitor urine outputMonitor urine output
Tube decompressionTube decompression Empties stomachEmpties stomach Reduces aspiration riskReduces aspiration risk No benefit to long intestinal tubesNo benefit to long intestinal tubes
In partial obstruction: 60-85% success rateIn partial obstruction: 60-85% success rate


Treatment - Operative
Complete obstructionComplete obstructionGenerally mandates operationGenerally mandates operationSome have argued for Some have argued for
nonoperative approach in nonoperative approach in selected patientsselected patients
12-24hr delay of surgery is safe12-24hr delay of surgery is safe>24hr delay is unsafe >24hr delay is unsafe

Operative Technique Dependent on underlying problemDependent on underlying problem Adhesive band: Lysis of adhesionsAdhesive band: Lysis of adhesions Incarcerated hernia: manual reduction Incarcerated hernia: manual reduction
and closure of defectand closure of defect *Presence of hernia with SBO *Presence of hernia with SBO
mandates ORmandates OR Malignant tumors: Difficult challengeMalignant tumors: Difficult challenge
Diverting stomaDiverting stoma Resection / anastamosisResection / anastamosis EnteroenterostomyEnteroenterostomy

Intestinal Viability at Surgery Release obstructed segmentRelease obstructed segment Place in warm sponge x 15-20 minutesPlace in warm sponge x 15-20 minutes If normal colour and peristalsis: return to If normal colour and peristalsis: return to
abdabd Doppler probe adds little to clinical Doppler probe adds little to clinical
judgment (Bulkley, 1981)judgment (Bulkley, 1981) Fluorescein may be useful in difficult Fluorescein may be useful in difficult
casescases ““Second look” in 24 hrs if questionable Second look” in 24 hrs if questionable
viability or if clinically deteriorates post-opviability or if clinically deteriorates post-op
Laparoscopy in Acute SBO?
Criteria:Criteria:Mild distensionMild distensionProximal obstructionProximal obstructionPartial obstructionPartial obstructionAnticipated single-band obstructionAnticipated single-band obstructionNo matted adhesions / No matted adhesions /
carcinomatosiscarcinomatosis

Special Considerations: Recurrent Adhesions
Multiple agents have been tried, none Multiple agents have been tried, none successfulsuccessful
Hyaluronate-based membrane shown to Hyaluronate-based membrane shown to reduce severity of adhesion formation reduce severity of adhesion formation (Becker, 1996; Vrigland, 2002)(Becker, 1996; Vrigland, 2002)
No studies yet to show reduction in No studies yet to show reduction in obstructionobstruction

Special Considerations: Recurrent Adhesions So far, best evidence to prevent So far, best evidence to prevent
adhesions is good surgical technique:adhesions is good surgical technique: Gentle handling of bowelGentle handling of bowel Avoid unnecessary dissectionAvoid unnecessary dissection Exclusion of foreign material from Exclusion of foreign material from
peritoneumperitoneum Adequate irrigation / removal of debrisAdequate irrigation / removal of debris Place omentum around site of surgeryPlace omentum around site of surgery

Special Considerations: Acute Post-op Obstruction
OObstructive symptoms after an initial return of bstructive symptoms after an initial return of bowel function and resumption of oral intakebowel function and resumption of oral intake
Technical complication versus adhesionsTechnical complication versus adhesions CT scan useful to evaluate for complications:CT scan useful to evaluate for complications:
Anastamotic leakAnastamotic leak Narrow anastomosisNarrow anastomosis Internal herniaInternal hernia Obstruction at stomaObstruction at stoma
Early reoperation may be indicated Early reoperation may be indicated

Acute Adhesive Postoperative Obstruction
DDifficult to distinguish ifficult to distinguish from from ileusileus IIncidence 0.7%ncidence 0.7% HHighest incidence on small intestine ighest incidence on small intestine
(3(3% – 10%)% – 10%) Present as early as POD 4Present as early as POD 4 UUsually partial SBOsually partial SBO CT preferred modalityCT preferred modality

Acute Postoperative Obstruction (Adhesive) 80% spontaneous resolution of 80% spontaneous resolution of
symptoms symptoms 4% of patients required more than 2 4% of patients required more than 2
weeks of treatmentweeks of treatment SBO after laparoscopySBO after laparoscopy:: suspect herni suspect herniaa
at at trocar sitetrocar site

Surgery for Malignant Bowel Obstruction in Advanced Gynaecological and Gastrointestinal Cancer
Cochrane ReviewCochrane Review::20042004 RRole of surgery controversialole of surgery controversial NNo firm conclusions from many retrospective o firm conclusions from many retrospective
case series case series Control of symptoms varies from 42% to over Control of symptoms varies from 42% to over
8080 RRates of re-obstruction, from 10-50%, though ates of re-obstruction, from 10-50%, though
time to re-obstruction was often not includedtime to re-obstruction was often not included Continues to be a challenging problemContinues to be a challenging problem

Steroids in Advanced Gyne/GI Cancer With SBO Cochrane Review of prospective data (89 Cochrane Review of prospective data (89
patients)patients) TTrend, not statistically significant, for rend, not statistically significant, for
resolution of bowel obstruction using resolution of bowel obstruction using corticosteroidscorticosteroids
NNo statistically significant difference in o statistically significant difference in mortalitymortality
NNNT 6 NT 6 MMorbidity associated with steroids orbidity associated with steroids appearsappears
lowlow

Summary
Guidelines for Operative and Guidelines for Operative and Nonoperative TherapyNonoperative Therapy

Emergent Operation
Incarcerated, strangulated herniaIncarcerated, strangulated hernia PeritonitisPeritonitis PneumatosisPneumatosis PneumoperitoneumPneumoperitoneum Suspected / proven strangulationSuspected / proven strangulation Closed-loop obstructionClosed-loop obstruction Complete bowel obstructionComplete bowel obstruction

Urgent Operation
Progressive bowel obstruction after Progressive bowel obstruction after conservative measures startedconservative measures started
Failure to improve with conservative Failure to improve with conservative therapy in 24-48 hourstherapy in 24-48 hours
Early post-op technical complications Early post-op technical complications (not adhesions)(not adhesions)

Operation Usually Delayed Safely Postoperative adhesionsPostoperative adhesions Immediate post-op obstruction Immediate post-op obstruction
(adhesive)(adhesive) Acute exacerbation of Crohn’s dx, Acute exacerbation of Crohn’s dx,
diverticulitis, radiation enteritisdiverticulitis, radiation enteritis Chronic, recurrent partial obstructionChronic, recurrent partial obstruction

Large Bowel Obstruction
CancerCancer CancerCancer Cancer (>90%)Cancer (>90%) Other thingsOther things
Sigmoid Volvulus (5%)Sigmoid Volvulus (5%) Diverticular Disease (3%)Diverticular Disease (3%)
Large Bowel Obstruction
ApproachApproach Contrast EnemaContrast Enema
CT AbdoCT Abdo Treat underlying causeTreat underlying cause

Acute Pseudo-Obstruction
Common ward consultCommon ward consult Predisposing Predisposing
Conditions:Conditions: Surgery Surgery Trauma Trauma Infection Infection Cardiac (CHF/MI)Cardiac (CHF/MI) Neurological (PD, SCI, Neurological (PD, SCI,
MS, ADMS, AD Metabolic (Metabolic (↓K/Na)↓K/Na)

Ogilvie’s Syndrome
Meds Assoc w/Ogilvie’sMeds Assoc w/Ogilvie’s NarcoticsNarcotics AnticholinergicAnticholinergic TCATCA ChlorpromazineChlorpromazine LevodopLevodop Ca++ blockersCa++ blockers ClonidineClonidine
Ogilvie’s Initial Tx:Ogilvie’s Initial Tx: Correct fluid and lyteCorrect fluid and lyte NPO/NGNPO/NG Rectal tube Rectal tube Limit offending Limit offending
medicationsmedications
>80% success>80% success

Ogilvie’s Treatment
NeostigmineNeostigmine 2 mg IV 2 mg IV Atropine at bedsideAtropine at bedside Monitored bedMonitored bed Patient supine, on Patient supine, on
bedpan bedpan 90% success rate90% success rate
ColonoscopyColonoscopy If neostigmine failsIf neostigmine fails DecompressionDecompression
SurgerySurgery Last resort; rarely Last resort; rarely
neededneeded If ischemia/perforationIf ischemia/perforation