-
8/10/2019 Abnormal Placentation in Preeclampsia
1/6
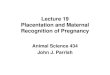
Abnormal placentation in preeclampsia. In normal placental
development, invasive
cytotrophoblasts of fetal origin invade the maternal spiral
arteries, transforming
them from small-caliber resistance vessels to high-caliber
capacitance vessels
capable of providing placental perfusion adequate to sustain the
growing fetus.
During the process of vascular invasion, the cytotrophoblasts
dierentiate from an
epithelial phenotype to an endothelial phenotype, a process
referred to aspseudovasculogenesis, or vascular mimicry (top. In
preeclampsia, cytotrophoblasts
fail to adopt an invasive endothelial phenotype. Instead,
invasion of the spiral
arteries is shallow, and they remain small-caliber resistance
vessels (bottom.
!igure reproduced with permission from "am et al.#$
-
8/10/2019 Abnormal Placentation in Preeclampsia
2/6
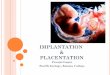
s!lt% and soluble endoglin (s&ng cause endothelial
dysfunction by antagoni'ing
vascular endothelial growth factor (&)! and transforming
growth factor-*% (+)!-
*% signaling. +here is mounting evidence that &)! and +)!-*%
are required to
maintain endothelial health in several tissues including the
idney and perhaps the
placenta. During normal pregnancy, vascular homeostasis is
maintained by
physiological levels of &)! and +)!-*% signaling in the
vasculature. Inpreeclampsia, ecess placental secretion of s!lt% and
s&ng ( endogenous
circulating antiangiogenic proteins inhibits &)! and +)!-*%
signaling,
respectively, in the vasculature. +his results in endothelial
cell dysfunction,
including decreased prostacyclin, nitric oide production, and
release of
procoagulant proteins. +*/II indicates transforming growth
factor-* type II receptor.
0ummary of the pathogenesis of preeclampsia. Angiotensin II +ype
I /eceptor
Activating Autoantibodies (A+%-AA, immunologic factors, oidative
stress, and otherfactors (such as decreased heme oygenase epression
may cause placental
dysfunction, which in turn leads to the release of
antiangiogenic factors (such as
s!lt% and soluble endoglin 1s&ng2 and other in3ammatory
mediators to induce
preeclampsia. 45 indicates natural iller6 7+4, hypertension.
-
8/10/2019 Abnormal Placentation in Preeclampsia
3/6
8reeclampsia is a ma9or contributor to the maternal and neonatal
mortality and
morbidity.%,It is the nd largest cause of maternal mortality
worldwide and aects
$: to ;: of pregnant women worldwide. wees of gestation in a
previously normotensive
woman,
-
8/10/2019 Abnormal Placentation in Preeclampsia
4/6
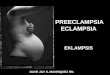
+he diagram represents the early development of the trophoblast
lineage. +he
decisive dierentiation steps are highlighted with gray boes. +he
dar gray boes
indicate the very early dierentiation steps. If there is a
failure during this time of
development the pregnancy may result in a combination of
preeclampsia (8& and
IE)/. If only the villous pathway is aected, it may result in a
preeclampsia (lower
left. And if only the etravillous pathway is aected it may
result in an IE)/ (lower
right.
-
8/10/2019 Abnormal Placentation in Preeclampsia
5/6
1. Normal PregnancyDuring normal pregnancy aged and late
apoptotic syncytiotrophoblast nuclei arepaced into apical
protrusions of the syncytiotrophoblast,
-
8/10/2019 Abnormal Placentation in Preeclampsia
6/6
occurs after midgestation. +his discrepancy can be eplained as
follows During the=rst trimester of pregnancy trophoblast turnover
is dierent to the turnover later ingestation. In the =rst trimester
most of the fusion events of cytotrophoblast cellswith the
syncytiotrophoblast are needed for growth of the
syncytiotrophoblastrather than for the maintenance of this
layer.