Embed Size (px)
Citation preview
Abnormal Uterine Bleeding
Benjie B. Mills, MD
Division Director, Pediatric & Adolescent Gynecology Medical Director of Gynecology, GHS OB/GYN Center
Associate Professor of Clinical Obstetrics & Gynecology
University of South Carolina School of Medicine Greenville

Disclosures
• I have nothing to disclose • This presentation will discuss off-label use of
medications

Objectives
• Describe etiologies, work up, and clinical course of abnormal uterine bleeding
• Formulate a patient-centered and evidence-based treatment plan
• Focus on issues of particular importance to the PCP such as prevention, therapeutic lifestyle changes, health maintenance, and when to refer to a specialist

Etiologies
Abnormal Uterine Bleeding Heavy Menstrual Bleeding (AUB-HMB)
Intermenstrual Menstrual Bleeding (AUB-IMB)
PALM: Structural Polyp (AUB-P)
Adenomyosis (AUB-A) Leiomyoma (AUB-L)
Malignancy & Hyperplasia (AUB-M)
COEIN: Non-Structural Coagulopathy (AUB-C)
Ovulatory Dysfunction (AUB-O) Endometrial (AUB-E)
Iatrogenic (AUB-I) Not Yet Classified (AUB-N)

Structural
• Polyps

Structural
• Adenomyosis

Structural
• Leiomyomata

Structural
• Malignancy and Hyperplasia

Coagulopathy
• Inherited and acquired • Occurs in up to 20% of patients with HMB • Indications for evaluation
– Heavy menstrual bleeding since menarche, or – Postpartum hemorrhage, excessive surgical bleeding
or bleeding with dental work, or – Any two of the following
• Bruising 1-2 times per month • Epistaxis 1-2 times per month • Frequent gum bleeding • Family history of bleeding symptoms

Ovulatory Dysfunction
• Encompasses amenorrhea to frequent irregular menses and in between – Hypothalamic hypogonadotropic hypogonadism – Thyroid dysfunction – Hyperprolactinemia – Hyperandrogenemia/PCOS – Premature ovarian insufficiency – Idiopathic anovulation – Chronic illness
Endometrial Abnormalities
• Abnormal endometrial angiogenesis • Prostaglandin production • Vasoconstriction • Increased fibrinolysis

Iatrogenic
• Contraceptives – OCPs, contraceptive patch or ring – DepoProvera (DMPA) – Contraceptive implant (Nexplanon) – Intrauterine device
• Hormonal (levonorgestrel IUD, Mirena, Skyla) • Non-hormonal (Paragard, copper T)
• Other medications – Antipsychotics – Anticoagulants – Other

Evaluation

Evaluation: History
• Age of menarche • Menstrual bleeding pattern • Severity of bleeding (clots or flooding) • Pain • Medical history • Surgical history • Family history of bleeding disorders, PCOS,
diabetes …

Medications
• Anticoagulants • Hormonal medications • NSAIDs • Antipsychotics • Ginkgo • Ginseng • Motherwort

Physical Exam
• Abnormalities of weight • Skin
– Acanthosis nigricans – Hirsutism – Pallor – Petechiae or ecchymoses
• Thyroid • Abdomen • Pelvic
Laboratory Testing
• Pregnancy test • STD testing if indicated • CBC with diff • TSH

Laboratory Testing
• Bleeding disorder – PT/PTT/INR – Platelet function screen – Fibrinogen
• Hyperandrogenism/PCOS – Testosterone, free and total – DHEAS – 17 hydroxyprogesterone – HgbA1C, lipids, CMP

Laboratory Testing
• Amenorrhea/Oligomenorrhea – Prolactin – FSH/LH – Estradiol

• Ultrasound – Transvaginal – Transabdominal
• MRI – Müllerian
anomalies – Fibroid mapping – Adenomyosis
• Saline infusion sonogram – Cavity assessment – Endometrial biopsy
• Hysteroscopy • Endometrial biopsy
Imaging and Tissue Sampling

Differential Diagnosis by Age Category
Ages 13-18 Years
• Pregnancy – UCG – TV Ultrasound for positive UCG and bleeding
and/or pain • Pelvic infection
– GC and chlamydia NAATs – Trichomonas or cervicitis – PID
Ages 13-18 Years
• Anovulation – immaturity or dysregulation of the hypothalamic-pituitary-ovarian axis – Irregular cycle length – Within 3 years of menarche (80% in a regular pattern) – Plan:
• R/O pregnancy • Cyclic medroxyprogesterone acetate 10 mg x 10 days per
month or OCPs if desires treatment • TSH in patients with other symptoms of thyroid dysfunction • Coagulopathy workup if heavy since menarche • Assess for anemia if heavy or prolonged bleeding
Ages 13-18 Years
• Coagulopathies – Prolonged, heavy menses – May be irregular due to immature HPO axis – Plan:
• TSH • Bleeding disorder labs • Treat underlying condition • Treatment choices
– OCPs (increases factor secretion) – Anti-fibrinolytics – Menstrual suppression

Ages 13-18 Years
• Hormonal contraceptive use – OCPs
Cycle 1 Cycle 4
Extended Cycle OCP
> 7 days 65% 42% > 20 days 35% 15%
Cycles 1-4 Cycles 10-13
28d Cyclic OCP
> 7 days 38% 39% > 20 days 6% 4%

Ages 13-18 Years
• Hormonal contraceptive use – Etonogestrel implant
Bleeding Patterns Definitions %*
Infrequent Less than three bleeding and/or spotting episodes in 90 days (excluding amenorrhea)
33.6
Amenorrhea No bleeding and/or spotting in 90 days 22.2
Prolonged Any bleeding and/or spotting episode lasting more than 14 days in 90 days
17.7
Frequent More than 5 bleeding and/or spotting episodes in 90 days 6.7

Ages 13-18 Years
• Hormonal contraceptive use – Depo Medroxyprogesterone Acetate (DMPA)
• 54% with AUB at 1 year • 46% with amenorrhea • 25% discontinue because of AUB

Ages 19-39 Years
• Pregnancy • Infection • Hormonal contraception • Structural abnormalities
– Fibroids – Polyps – Adenomyosis
Ages 19-39 Years
• Anovulation – Polycystic ovarian syndrome is the most common
cause – Chronic disease – Idiopathic – Premature ovarian insufficiency
• Endometrial hyperplasia and malignancy (rare) – Endometrial sampling in high risk patients
Ages 40 to Menopause
• Pregnancy • Anovulation
– Physiologic when approaching menopause – PCOS
• Structural abnormalities • Endometrial hyperplasia and malignancy
Imaging & Tissue Sampling

Who gets imaging?
• Abnormal pelvic examination • Unresponsive to initial treatment in a patient
with a normal pelvic exam • Suspicion for structural abnormality

Which imaging is best?
• Transvaginal ultrasound (2D and 3D) – Screening test – Intracavitary pathology
• Sensitivity 56% • Specificity 73%
– Endometrial thickness is not helpful • Saline infusion sonography
– Superior at determining intracavitary pathology – Global changes vs. specific lesions
• MRI is not recommended for evaluation of AUB
Who needs endometrial sampling? • Women > age 45 with AUB • Women < age 45 with AUB and chronic
anovulation (unopposed estrogen) – Obesity – PCOS – Endometrial cancers and hyperplasias can be
diagnosed in young patients at very high risk
Evidence-Based Evaluation and Treatment Plans
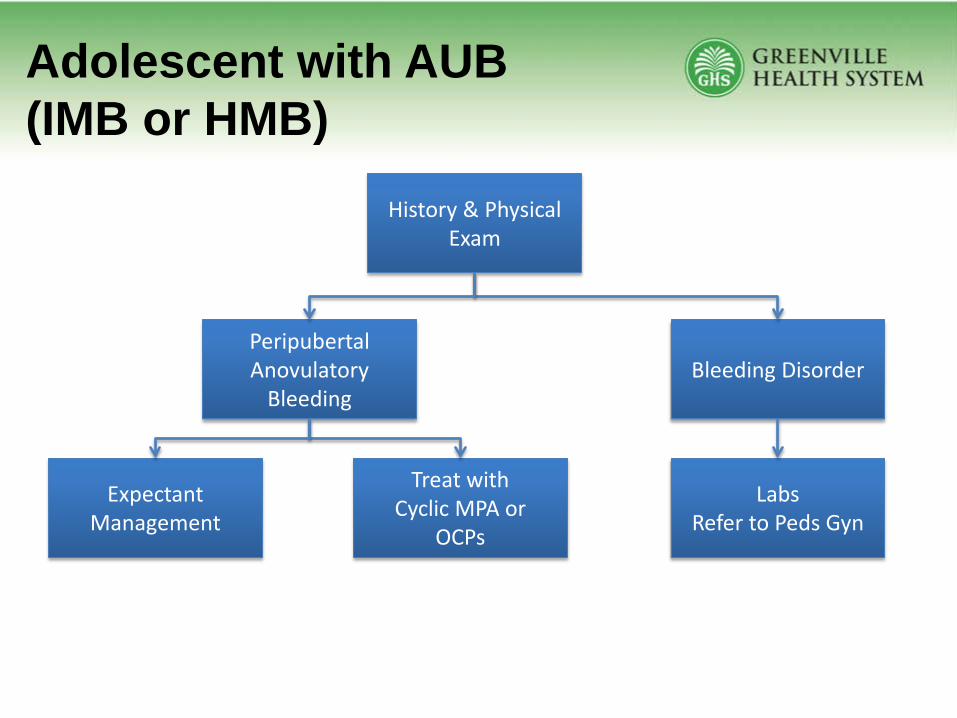
Adolescent with AUB (IMB or HMB)
History & Physical Exam
Peripubertal Anovulatory
Bleeding Bleeding Disorder
Labs Refer to Peds Gyn
Expectant Management
Treat with Cyclic MPA or
OCPs

Reproductive Age with HMB
History, Physical Exam & Labs
Abnormal Pelvic Exam Normal Pelvic Exam
Treat: OCPs
LngIUD DMPA
Tranexamic acid
Ultrasound Treat Abnormality
Treatment Success No further workup
Treatment Failure Ultrasound
Refer to OB/Gyn

Reproductive Age with IMB History, Physical Exam, Normal
Pelvic Exam & Labs
Long-standing IMB
Expectant Management or
Treat: OCPs
Cyclic MPA
Treatment Success No further workup
Treatment Failure Needs Cavity Eval Refer to OB/Gyn
Short-term IMB
EMB and Cavity Evaluation
Refer to OB/Gyn

Prevention

Prevention
• Maintain healthy weight • Evaluate for PCOS if patient is 3 years post-
menarche and having IMB – Prevent hirsutism – Prevent long-term morbidity of PCOS via education
and health maintenance – Prevent psychologic sequelae
• Avoid use of DMPA for AUB • Recognize patients at high-risk for hyperplasia or
malignancy