Embed Size (px)
Citation preview

Obstetric Anaesthetists' Association
Three-day Course on ObstetricAnaesthesia and Analgesia
Organised by Dr Roshan Fernando, University College London Hospitalsand Dr Chris Elton, University Hospitals of Leicester
Formed 1969. Registered Charity 1111382
Promoting the highest standards of anaesthetic practice in the care of mother and baby
9 – 11 November 2009Church House Conference Centre, Westminster, SW1P 3NZ
LONDON
LECTURE ABSTRACTS
OAA Secretariat, PO Box 3219 Barnes, London SW13 9XR UKTel: +44 (0)20 8741 1311 • Fax: +44 (0)20 8741 0611 • For email contact and all details: www.oaa-anaes.ac.uk
ObstetricAnaesthetists’Association
Obstetric Anaesthetists’ AssociationPromoting the highest standards of anaesthetic practice in the care of mother and baby
20 - 21 May 2010 (evening reception 19 May) The Sage, NewcastleGateshead
Obstetric Anaesthesia 2010
Enquiries: OAA Secretariat T: +44 (0) 20 8741 1311 F: +44 (0) 20 8741 0611 www.oaameeetings.info
Registered Charity 1111382
FUTURE MEETINGS & COURSES
2010 3 March 2010 Cases and Controversies in Obstetric Anaesthesia, London
19 - 21 May 2010 Obstetric Anaesthesia 2010 (Reception 19 May, Annual Meeting 20 & 21 May), The Sage, NewcastleGateshead
13 October 2010 Refresher Day on Obstetric Anaesthesia and Analgesia, London
8 - 10 November 2010 Three-day Course on Obstetric Anaesthesia and Analgesia, London
10 December 2010 Joint meeting with Royal Society of Medicine (Section of Anaesthesia and Section of Obstetrics and Gynaecology), London
201125 - 27 May 2011 Obstetric Anaesthesia 2011 (Reception 25 May, Annual Meeting 26 & 27 May),
Edinburgh
201223 - 25 May 2012 Obstetric Anaesthesia 2012 (Reception 23 May, Annual Meeting 24 & 25 May),
Liverpool
201322 - 24 May 2013 Obstetric Anaesthesia 2013 (Reception 22 May, Annual Meeting 23 & 24 May),
Bournemouth
OAA Secretariat, PO Box 3219 Barnes, London SW13 9XR UKTel: +44 (0)20 8741 1311 • Fax: +44 (0)20 8741 0611 • For email contact and all details: www.oaa-anaes.ac.uk
Obstetric A
naesthetists’ Association ● Three-day C
ourse N
ovember 2009

Dr Maggie Blott Consultant Obstetrician University College London Hospitals Professor Rob Dyer Professor & Second Chair, Department of Anaesthesia Groote Schuur Hospital, University of Cape Town, South Africa Dr Chris Elton Consultant Anaesthetist University Hospitals of Leicester Dr Roshan Fernando Consultant Anaesthetist University College London Hospitals Dr Wiebke Gogarten Consultant Anaesthetist & Head Department of Anaesthesiology, Intensive Care and Pain Medicine, Harlaching Hospital, Municipal Hospitals of Munich, Germany Dr David Hill Consultant Anaesthetist Ulster Hospital, Belfast Dr Paul Howell Consultant Anaesthetist St Bartholomew's & Homerton Hospitals, London Professor Beverley Hunt Professor of Thrombosis & Haemostasis Guy's & St Thomas' Hospitals, London Dr Ian Laing Consultant Neonatologist Edinburgh Royal Infirmary Dr David Levy Consultant Anaesthetist Queen's Medical Centre, Nottingham Dr Gordon Lyons Consultant Anaesthetist St James' University Hospital, Leeds Dr Lucy Mackillop Locum Consultant Obstetric Physician, John Radcliffe Hospital, Oxford
Dr Geraldine O'Sullivan Consultant Anaesthetist Guy's & St Thomas' Hospitals, London Dr Peter Pan Professor & Director of Anesthesia Clinical Research Wake Forest University School of Medicine, Winston-Salem, USA Dr Anil Patel Consultant Anaesthetist Royal National Throat, Nose & Ear Hospital, London Dr Felicity Plaat Consultant Anaesthetist Queen Charlotte's & Hammersmith Hospitals, London Dr Mansukh Popat Consultant Anaesthetist John Radcliffe Hospital, Oxford Professor Felicity Reynolds Emeritus Professor of Obstetric Anaesthesia Consulting Editor, International Journal of Obstetric Anesthesia Professor Steve Robson Professor of Fetal Medicine Royal Victoria Infirmary, Newcastle-upon-Tyne Dr Ian Russell Consultant Anaesthetist Hull Royal Infirmary Dr Robin Russell Consultant Anaesthetist John Radcliffe Hospital, Oxford Dr Mark Scrutton Consultant Anaesthetist St Michael's Hospital, Bristol Professor Andrew Shennan Professor of Obstetrics Guy's & St Thomas' Hospitals, London Prof Dr Marc Van de Velde Professor of Anesthesiology University Hospitals Gasthuisberg, Leuven, Belgium Dr Cynthia Wong Associate Professor, Chief of Obstetrical Anesthesia Northwestern University Feinberg School of Medicine, USA

MONDAY 9 NOVEMBER
08.30 REGISTRATION, COFFEE & EXHIBITION 09.45 Opening remarks Dr Roshan Fernando Session 1: Topical Issues 1 · Chairman: Dr Roshan Fernando 09.50 New epidural drugs & adjuvants Dr Mark Scrutton 4 10.10 What's new in obstetric anaesthesia
- a snapshot of the literature Professor Cynthia Wong 11 10.50 Discussion 11.00 COFFEE & EXHIBITION Session 2: Topical Issues 2 · Chairman: Dr Gordon Lyons 11.25 Oxytocic drugs during caesarean delivery
- essential, but toxic Professor Rob Dyer 15 11.55 Neurological injury associated with childbirth
& regional anaesthesia Professor Cynthia Wong 19 12.20 Remifentanil for labour analgesia Dr David Hill 24 12.50 Discussion 13.00 LUNCH & EXHIBITION Session 3: Labour Analgesia · Chairman: Dr David Hill 14.00 CSE or epidural for labour analgesia? Professor Peter Pan 29 14.25 Maintaining labour epidurals - an update Professor Cynthia Wong 35 14.50 Optimizing your labour epidural
- from insertion to delivery / clinical pearls Professor Peter Pan 41 15.15 Discussion 15.30 TEA Session 4: New Developments · Chairman: Dr Roshan Fernando 16.00 Tracheal intubation - what's new? Dr Anil Patel 47 16.30 Acute to chronic pain after delivery: from predictors to spinal oxytocin Professor Peter Pan 48 17.00 Discussion 17.15 DRINKS (close 18.15)
TUESDAY 10 NOVEMBER
08.15 REGISTRATION, COFFEE & EXHIBITION Session 5: Blood Issues · Chairman: Dr David Levy 09.00 Obstetric Haemorrhage - rFVlla, interventional
radiology, cell salvage and beyond Dr Felicity Plaat 55 09.25 Thromboprophylaxis, heparins and regional techniques Dr Beverley Hunt 58 09.50 Use of the coagulation laboratory and point of patient
testing in thrombosis & bleeding Dr Wiebke Gogarten 59 10.15 Discussion 10.30 COFFEE & EXHIBITION Session 6: Caesarean Section · Chairman: Professor Marc Van de Velde 11.00 General anaesthesia for caesarean section
- what's new? Dr David Levy 63

11.25 Managing the difficult airway in obstetrics Dr Mansukh Popat 71 11.55 Cardiac output monitoring during caesarean section
- what have we learnt Professor Rob Dyer 82 12.20 Discussion 12.30 LUNCH & EXHIBITION Session 6 (cont): Caesarean Section · Chairman: Dr Felicity Plaat 13.30 Spinal anaesthesia for caesarean section
- dose, position & baricity Professor Marc Van de Velde 85 13.55 The obese parturient Dr Wiebke Gogarten 89 14.15 Managing pain & distress during caesarean section
under regional anaesthesia Dr Geraldine O'Sullivan 93 14.35 Discussion 14.45 TEA & EXHIBITION Session 7: The Baby 1 · Chairman: Dr Geraldine O'Sullivan 15.10 The decision to deliver - the obstetrician's viewpoint Professor Andrew Shennan 95 15.40 Emergency caesarean section following the decision
to deliver - the anaesthetist's viewpoint Dr Chris Elton 96 16.00 Intrapartum fetal assessment and resuscitation
- what the anaesthetist needs to know Professor Steve Robson 101 16.30 Discussion
WEDNESDAY 11 NOVEMBER
08.15 REGISTRATION, COFFEE & EXHIBITION Session 8: Challenges for the Obstetric Anaesthetist · Chairman: Dr Chris Elton 09.00 Major trauma in pregnancy Dr Paul Howell 106 09.20 Pulmonary oedema in the third trimester
- a perspective from South Africa Professor Rob Dyer 112 09.40 Prevention and treatment of postdural puncture headache Professor Cynthia Wong 115 10.00 Discussion 10.15 COFFEE & EXHIBITION Session 9: The Baby 2 · Chairman: Dr Robin Russell 10.45 Current issues in neonatal resuscitation Dr Ian Laing 125 11.10 Effect of analgesia and anaesthesia on the baby Professor Felicity Reynolds 126 11.40 Discussion 11.55 LUNCH & EXHIBITION Session 10: Pre-eclampsia Revisited · Chairman: Dr Roshan Fernando 12.45 Obstetric issues Mr Maggie Blott 133 13.10 Medical management of pre-eclampsia Dr Lucy Mackillop 138 13.35 Anaesthetic issues Dr Robin Russell 144 14.00 Discussion The OAA Gold Medal Lecture · Chairman: Dr Paul Howell 14.10 Lateral thinking Dr Ian Russell 14.35 Discussion & Closing remarks Dr Roshan Fernando 14.45 TEA 15.15 Close

Session 1: Topical issues 1 New epidural drugs and adjuvants Dr Mark Scrutton Consultant Anaesthetist, St Michael's Hospital, Bristol
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
4

New LAs: Key issues
1. Sensory/motor differential
2. Toxicity
Bupivacaine toxicity
‘Between the years 1973 and 1983, at least 24
maternal deaths were reported in the USA
following accidental intravascular
administration of bupivacaine….after intended
epidural injection of bupivacaine in parturients
scheduled for cesarean section’
Marx 1997
UK experience
• 8 deaths assoc 0.25% bup in IVRA
• 1 obstetric death – caudal epiduralTOXICITY
…the evidence
Ropivacaine toxicityanimal studies
Rats:↓ arrhythmias with ropivacaine
↓ Ericson 1996
Dogs:CNS toxicity ratio (R:B): 1:1Deaths @ 2x CNS toxic dose (R:B): 1:5Bupivacaine dogs hard to resuscitate
Feldman 1989,91
Pregnant sheep:
CNS toxic dose (R:B): 1.5:1CVS toxic dose (R:B): 1.5:1
Santos 1995
Ropivacaine toxicityhuman studies
Infusion 10mg/m up to total 150mg
Stopped when symptoms occurred
124mg ropivacaine v 99mg bupivacaine
Scott et al, A&A 1989
Infusion 10mg/m
Stopped when symptoms occurred
115mg ropivacaine v 103mg bupivacaine
Knudsen et al, BJA 1997
BUT:
What about relative potencies?
The MLAC studies……….
MLAC
Ropivacaine: 0.111% Polley, 1999
Bupivacaine: 0.067% Polley, 1999
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
5

Predicted therapeutic index
Columb & Polley, SOAP 1999
Therapeutic index (TI) = Toxic dose50/Effective dose50
Rop Bup Ratio
ED50 (mg) 22.2 13.4 0.6
TI(Scott)
(Toxic dose) 5.5
(124mg) 7.4
(99mg) 0.75
TI(Knudsen)
(Toxic dose) 5.2
(115mg) 7.7
(103mg) 0.67
Is MLAC relevant?
Only relates to FIRST dose for labour analgesia: 13-25mg
When does toxicity occur?
Big, intravenous doses
eg LSCS: 20ml 0.5% bupivacaine or
0.5% ropivacaine
ie: 100mg
Ropivacaine toxicity
Caesarean section:
0.5% Ropivacaine 20ml is as effective as
0.5% Bupivacaine 20mlDatta 1995
Griffin & Reynolds 1995
Alahuhta 1995
Crosby 1998
……but safer
LEVOBUPIVACAINE
Levobupivacaine toxicity
Isolated hearts: pig, rabbit, guinea pig
Intact animals: rat, sheep, human
…levobupivacaine safer than bupivacaine
Toxicity: human studies
Bardsley et al, A&A 1998:
Infusion 10mg/m up to total 150mg
Stopped when symptoms occurred
56.1mg levobupivacaine v 49.6mg bupivacaine
Ropivacaine toxicityhuman studies
Infusion 10mg/m up to total 150mg
Stopped when symptoms occurred
124mg ropivacaine v 99mg bupivacaine
Scott et al, A&A 1989
Infusion 10mg/m
Stopped when symptoms occurred
115mg ropivacaine v 103mg bupivacaine
Knudsen et al, BJA 1997
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
6

Toxicity: human studies
Bardsley et al, A&A 1998:
Infusion 10mg/m up to total 150mg
Stopped when symptoms occurred
56.1mg levobupivacaine v 49.6mg bupivacaine
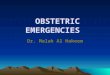
CVS changes occurred at lower plasma concentrations of bupivacaine
-25
-20
-15
-10
-5
0
stroke index accelerationindex
ejectionfraction
levobupivacainebupivacaineP
erce
nt r
educ
tion
Bardsley et al 1998
Cardiac effects of levobupivacaine and bupivacainein maximum tolerated doses in healthy volunteers
MLAC
Levobupivacaine: 0.083% Lyons et al
Bupivacaine: 0.081% Lyons et al
Are they worth it?
1. No: only one maternal death in many years of UK use…
Intravenous misplacement
Accidental intravenous misplacement of the epidural catheter can occur in up to 15% of pregnant patients
Negative aspiration tests may be unreliable
Test doses are inconclusive
Catheters may ‘migrate’ at any time
“Now don’t you fret Mrs. Firkin, my eyes are glued to your ECG”
1. No: only one maternal death in years of UK use
2. Yes: targetted use
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
7

Levobupivacaine (or Ropivacaine) are better options when………
large doses are needed, for example:
epidural top-up for emergency LSCS
when accidental i.v. injection is likely or may not be noticed
Lipid and LA toxicity
Pretreatment or resuscitation with a lipid
infusion shifts the dose-response to
bupivacaine-induced asystole in rats
Weinberg et al. Anesthesiology, 1998; 88(4): 1071-5
Lipid emulsion infusion rescues dogs from
bupivacaine-induced cardiac toxicity
Weinberg et al. Regional Anesthesia and Pain Medicine, 2003; 28(3): 198-202
Successful resuscitation of a patient with ropivacaine induced assystole after axillaryplexus block using lipid infusion
RJ Litz et al. Anaesthesia 2006;61:800-1
Successful use of a 20% lipid emulsion to resuscitate a patient after presumed bupivacaine related cardiac arrest
M Rosenblatt et al. Anesthesiology 2006;105:217-8
Lipid and LA toxicity
• 1ml/kg over 1 minute with chest compressions
• Repeat every 3-5 minutes up to 3ml/kg• Continuous infusion at 0.25ml/kg/min, until
haemodynamic recovery• Total dose above 8ml/kg is unlikely to be
required in responders and of no benefit in non-responders
Weinberg. Regional Anesthesia and Pain Medicine, 2004; 29(1): 74
Lipid regimen
500ml 20% Intralipid
£15
Shelf life of 2 years
Possibility of recycling it before it expires
Lipid: practicalities
Dose: LSCS: 20ml 3% solution
Pros: Fast onsetBjornestad, Acta Anaesthesiol Scand 2006;50:358-63
Gaiser, IJOA 1994;3:208-10
Cons: not available in UK?neurotoxicMunnur, Anesthesiol Clin North Am 2003;21:71-86
Taniguchi, Anesthesiology 2004;100:85-91
2-chloroprocaine
Topics
1. Local anaesthetics RopivacaineLevobupivacaine2-Chloroprocaine
2. Epidural adjuncts: OpioidsAdrenalineBicarbonateClonidineNeostigmine
Dose: Load 50mcg, Infuse 2mcg/ml
Pros: ↓ MLAC of local anaesthetics
↓ motor block
Cons: ↑ side-effects for neonate
↓ gastric emptying
↑ Itching, nausea,vomiting
Fentanyl: labour analgesia
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
8

Dose: 1:200,000-300,000
Pros: ↓ MLAC of local anaestheticsPolley, Anesthesiol 2002:1123-8
Shue, Anesthesiol 2006;104(Sup):A-46
? Value as test dose
Cons: ? Motor blockSoetens, Anesth Analg 2006;103:182-6
Adrenaline: labour analgesia
Dose: 50-75mcg (25-150mcg)
Pros: ↓ MLAC of local anaesthetics
↓ motor block
↓ shivering
Cons: sedation (>75mcg)
hypotension (>75mcg)
Clonidine: labour analgesia
Dose: 500mcg
Pros: ↑ quality of blockRoelants, Anesthesiol 2004;101:439-44
Cons: sedation
nausea and vomiting (spinal)
Neostigmine: labour analgesia
Dose: 50-100mcg
Pros: ↑ quality of the blockKing, Anaesthesia 1990;45:285-288
? speed of onsetGoring-Morris, IJOA 2006;15:109-14
Malhotra, IJOA 2006;15(Sup):S6
Cons: ↑ side-effects for neonate
↑ itching, nausea,vomiting
Fentanyl: Epid LSCS
Dose: 1:200,000 (100mcg)
Pros: ↑ quality of the blockLaishley, Anaesthesia 1988;43:100-3
? speed of onset
? value as a test dose
Cons: Hypertension
Adrenaline: Epid LSCS
Dose: 1ml 8.4%
Pros: ? speed of onset
Cons: Precipitation with bupivacaine
Bicarbonate: Epid LSCS
Lam, Anaesthesia 2001;56:790-4 Pro
Gaggero, Can J Anaesth 1995;42:1080-4 Con
Capogna, Can J Anaesth 1993;40:425-30 Pro
Fernando, Br J Anaesth 1991;67:699-703 Pro
Capogna, J Clin Anesth 1991;3:211-4 Pro
Liepert, Can J Anaesth 1990;37:333-6 Con
Benhamou, Reg Anesth 1989;14:240-3 Con
McMorland, Can J Anaesth 1988;35 457-61 Pro
Allam, Anaesthesia 2008;63:243-9 Pro
Bicarbonate: Speed of onset
Multiple drug combinations:
1. Take time
2. Introduce errorsLucas, Br J Anaesth 2000;84:494-6
Goring-Morris, IJOA 2006;15:109-14
⇒⇒⇒⇒ Keep it simple, be prepared
Category 1 LSCS
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
9

Extended release epidural morphine (EREM):
Single dose, prolonged effect (Depodur)
Extended release local anaesthetics:
Phase II clinical trials
Future developments
Epidural analgesia in labour:
Bupivacaine is cheap, safe and effective
Opioids, adrenaline, clonidine will ↓MLAC and therefore may reduce motor block if LA dose is appropriately reduced
Technique (infus/top-ups/PCEA) may be more important
Epidural anaesthesia for LSCS:
Levobupivacaine or lidocaine
Consider opioid, adrenaline and bicarbonate
Preparation & technique
Summary
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
10

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 1: Topical Issues 1 What's new in obstetric anaesthesia - a snapshot of the literature Professor Cynthia Wong Associate Professor, Chief of Obstetrical Anesthesia, Northwestern University Feinberg School of Medicine, USA
Antepartum
1. Lyell DJ, Pullen KM, Mannan J, et al. Maintenance nifedipine tocolysis compared with placebo: a randomized controlled trial. Obstet Gynecol 2008; 112: 1221-6 Double-blind, randomized controlled trial of maintenance therapy for preterm labor. Groups: Nifedipine vs. placebo (N = 71). Outcome: Attainment of 37 weeks’ gestation. Results: No difference between groups. Conclusions: no evidence that maintenance tocolysis with any agent prolongs pregnancy. 2. Rouse DJ, Hirtz DG, Thom E, et al. A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. N Engl J Med 2008; 359: 895-905 Multi-center, double-blind, randomized controlled trial of magnesium therapy for women in preterm labor. Groups: Magnesium vs. placebo (N = 2241) Outcome: Primary: Composite of stillbirth or infant death by 1 year; secondary: moderate or severe cerebral palsy at or beyond 2 years of age. Results: Primary outcome, no difference between groups. Secondary outcome, less moderate or severe CP in magnesium group (1.9% vs. 3.5%, RR 0.55; 95% CI 0.32 to 0.95). Conclusions: Fetal exposure to magnesium may reduce risk of cerebral palsy in survivors. Intrapartum Obstetric Complications
3. Mercer BM, Gilbert S, Landon MB, et al. Labor outcomes with increasing number of prior vaginal births after cesarean delivery. Obstet Gynecol 2008; 111: 285-91 Multi-center, 4-year observational study of vaginal birth after cesarean Groups: 0, 1, 2, 3, or ≥ 4 prior VBACs Outcomes: Successful VBACs, frequency of uterine rupture, neonatal morbidity Results: Increasing VBAC success in with increasing number of prior VBACs, rate of uterine rupture
decreased after first successful VBAC, no difference in neonatal morbidity or mortality. Comments: Women with prior successful VBACs at low risk for maternal or neonatal complications. 4. Knight M, Kurinczuk JJ, Spark P, Brocklehurst P. Cesarean delivery and peripartum hysterectomy. Obstet Gynecol 2008; 111: 97-105 Case-controlled, 1-year study using the United Kingdom Obstetric Surveillance System of peripartum hysterectomy Groups: women who has peripartum hysterectomy (N = 318) and matched controls (N = 614) Outcomes: incidence, mortality, risk factors of hysterectomy Results: Incidence 4.1/10,000 births; maternal mortality 0.6%. Risk factors: previous cesarean delivery, age > 35 years, parity ≥ 3, previous manual removal of placenta, previous myomectomy, twin pregnancy, cesarean delivery. Conclusions: Peripartum hysterectomy strongly associated with previous cesarean delivery, age > 35 y, and parity ≥ 3. Neuraxial Labor Analgesia
5. Friedman Z, Siddiqui N, Katznelson R, Devito I, Davies S. Experience is not enough: repeated breaches in epidural anesthesia aseptic technique by novice operators despite improved skill. Anesthesiology 2008; 108: 914-20 Prospective observational study of second year anesthesia residents (N = 35) videotaped initiating epidural anesthesia and evaluated by blinded investigators. Outcomes: Scores of manual skills checklists, global rating scale, and an aseptic technique checklist. Results: Strong positive correlation between clinical experience and better scores on the manual skills checklist and global rating score, but nonsignificant or weak correlation with experience and aseptic technique score. Conclusions: There may be major gaps in how we teach trainees about aseptic technique.
11

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 6. Arkoosh VA, Palmer CM, Yun EM, et al. A randomized, double-masked, multicenter comparison of the safety of continuous intrathecal labor analgesia using a 28-gauge catheter versus continuous epidural labor analgesia. Anesthesiology 2008; 108: 286-98 Multi-center randomized controlled trial of spinal analgesia (administered via spinal microcatheters vs. epidural labor analgesia. Groups: Intrathecal sufentanil analgesia (N = 329) with 28-g catheter vs. epidural bupivacaine analgesia (N = 100). Outcome: Primary: incidence of neurologic complications at 24-, 48-h, 7-10 and 30-days. Results: No patient had a permanent neurologic change. Intrathecal analgesia resulted in better early analgesia, more pruritus, less motor block and higher patient satisfaction, but more technical failures. There was no difference in the postdural puncture headache rate (9% vs. 4%). Conclusions: The study was underpowered for the PDPH outcome. 7. Abrao KC, Francisco RP, Miyadahira S, Cicarelli DD, Zugaib M. Elevation of uterine basal tone and fetal heart rate abnormalities after labor analgesia: a randomized controlled trial. Obstet Gynecol 2009; 113: 41-7 Randomized controlled trial (n=77) of laboring women who received neuraxial labor analgesia. Groups: Epidural vs. combined-spinal epidural analgesia. Primary outcome: uterine tone and FHR abnormalities within 15 min of initiation of analgesia. Results: Greater incidence of uterine hypertonus in CSE group (41% vs. 17%: P = 0.02) and FHR abnormalities (32% vs. 0.06%; P < 0.01). Comments: Only evaluated FHR tracing for 15 min, assessed blood pressure every 5 min after analgesia. 8. Wang F, Shen X, Guo X, Peng Y, Gu X. Epidural analgesia in the latent phase of labor and the risk of cesarean delivery: A rive-year randomized controlled trial. Anesthesiology 2009 Randomized controlled trial of 12,793 nulliparous Chinese women in spontaneous labor who requested labor analgesia greater than 1 cm and less than 4 cm cervical dilation. Groups: Early vs. late (≥ 4 cm cervical dilation) epidural analgesia Primary outcome: rate of cesarean delivery. Results: No difference in cesarean delivery rate between groups (Early 23.2%, Late 22.8%: P = 0.51).
9. Landau R, Kern C, Columb MO, Smiley RM, Blouin JL. Genetic variability of the mu-opioid receptor influences intrathecal fentanyl analgesia requirements in laboring women. Pain 2008; 139: 5-14 Prospective double-blind observational study of ED50 of intrathecal fentanyl for labor analgesia in women with single nucleotide polymorphism at position 304 for the mu-opioid receptor gene (OPRM1). Groups: Nulliparous women (N = 224), homozygous 304AA vs. heterozygous or homozygous for the mutant 304A/G or GG. Results: Using both a up-down sequential allocation method and random-dose allocation method, the ED50 was lower in women with the mutant a mutant allele. Conclusions: Polymorphism at the mu-opioid receptor may affect response to opioids administered during labor.
10. Sia AT, Lim Y, Lim EC, et al. A118G single nucleotide polymorphism of human mu-opioid receptor gene influences pain perception and patient-controlled intravenous morphine consumption after intrathecal morphine for postcesarean analgesia. Anesthesiology 2008; 109: 520-6 Prospective observational study of post-cesarean morphine consumption in women with single nucleotide polymorphism at position 304 for the mu-opioid receptor gene (OPRM) who received spinal anesthesia with intrathecal morphine. Groups: Nulliparous women (N = 588), OPRM1 homozygous 304AA vs. heterozygous 304A/G and homozygous 304GG. Outcome: Self-administered intravenous morphine for 24 h after cesarean delivery. Results: Morphine consumption and pain scores were lower in the AA (5.9 mg) compared to AG (8.0 mg) and GG 9.4 mg) groups (P = 0.001). Conclusions: The study results agree with other studies of postoperative pain: patients with OPRM1 304GG require more analgesia. The results are difficulty to reconcile with those of Landau, et al.
Drugs and Drug Toxicity
11. Mayr VD, Mitterschiffthaler L, Neurauter A, et al. A comparison of the combination of epinephrine and vasopressin with lipid emulsion in a porcine model of asphyxial cardiac arrest after intravenous injection of bupivacaine. Anesth Analg 2008; 106: 1566-71 Randomized controlled trial in a porcine model (N = 10) of vasopressin/epinephrine vs. lipid emulsion for
12

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 success of resuscitation after IV bupivacaine cardiac arrest. Groups: vasopressin/epinephrine vs. lipid emulsion Outcome: Rate of survival. Results: 5/5 vasopressin/epinephrine pigs survived and 0/0 lipid emulsion pigs survived. Conclusions: Vasopressin/epinephrine resulted in higher coronary perfusion pressures and survival rates during CPR initiation for bupivacaine cardiac arrest.
12. Svanstrom MC, Biber B, Hanes M, et al. Signs of myocardial ischaemia after injection of oxytocin: a randomized double-blind comparison of oxytocin and methylergometrine during Caesarean section. Br J Anaesth 2008; 100: 683-9
Randomized trial comparing oxytocin to methylergometrine during elective cesarean delivery for signs of myocardial ischemia. Groups: Term gestation: oxytocin (10 U IV bolus) vs. methylergometrine (0.2 mg) (N = 40) vs. non-pregnant control (oxytocin, N = 10). Outcome: EKG changes (ST segment depression). Results: Oxytocin produced greater ST depression and decreases in MAP than methylergometrine. Conclusions: Oxytocin results in significant decrease in MAP and signs and symptoms (chest pain) of myocardial ischemia). 13. Ngan Kee WD, Khaw KS, Tan PE, Ng FF, Karmakar MK. Placental transfer and fetal metabolic effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery. Anesthesiology 2009; 111: 506-12 Randomized double-blind trial comparing placental transfer of ephedrine and phenylephrine used for the treatment of spinal anesthesia-induced hypotension for cesarean delivery. Groups: Phenylephrine vs. ephedrine (N = 104) Outcome: Placental transfer of phenylephrine and ephedrine, markers of fetal metabolism Results: Placental transfer of ephedrine is greater than phenylephrine, as were umbilical artery concentrations of lactate, glucose, epinephrine, and norepinephrine. Conclusions: Results support hypothesis that lower umbilical artery pH associated with ephedrine due to direct fetal metabolic effect. General Anesthesia for Cesarean Delivery
14. Kodali BS, Chandrasekhar S, Bulich LN, Topulos GP, Datta S. Airway changes during labor and delivery. Anesthesiology 2008; 108: 357-62
Two observational studies (N = 61 and N = 21) assessing airway changes (modified Mallampati classification and acoustic reflectometry) in laboring women. Groups: Women in labor. Outcome: Modified Mallampati classification and upper airway volume Results: Airway classification increased by one grade in 33% and two grades in 5%. There was a decrease in oral volume and pharyngeal airway as labor progressed. Conclusions: Airway examinations worsen during labor, and presumably, airway management becomes more difficult. Airway examinations performed at the start of labor may not reflect actual airway conditions after hours of labor. 15. McDonnell NJ, Paech MJ, Clavisi OM, Scott KL. Difficult and failed intubation in obstetric anaesthesia: an observational study of airway management and complications associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008; 17: 292-7 Multi-center, 2-year prospective observational study in 13 Australian and New Zealand hospitals in women receiving general anesthesia for cesarean delivery. Groups: Data from 1095 women (classes 1 to 4). Outcome: Incidence of difficult and failed intubation, and aspiration. Results: 3.3% considered difficult intubation, 4 failed intubations (0.4%; 95% CI 0.01-0.9%), 8 cases of aspiration (0.7%), no cases of serious airway morbidity. Conclusions: Incidence of failed intubation consistent with other studies. 16. Paech MJ, Scott KL, Clavisi O, Chua S, McDonnell N. A prospective study of awareness and recall associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008; 17: 298-303 Multi-center, 2-year prospective observational study in 13 Australian and New Zealand hospitals in women receiving general anesthesia for cesarean delivery. Groups: Data from 1095 women (classes 1 to 4). Outcome: Incidence of intraoperative awareness. Results: 2 cases consistent with awareness (0.26%; 95% CI 0.03-0.9%); in 32% of cases a depth-of-anesthesia monitor was used. Conclusions: Awareness remains a significant complication of general anesthesia for cesarean delivery. 17. Yoo KY, Jeong CW, Kang MW, et al. Bispectral index values during sevoflurane-nitrous oxide general anesthesia in women undergoing cesarean delivery: a
13

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 comparison between women with and without prior labor. Anesth Analg 2008; 106: 1827-32 Observational study of BIS values in women (N = 40) undergoing cesarean delivery with sevoflurane/nitrous oxide anesthesia. Groups: Laboring patients who required cesarean delivery, and non-laboring scheduled cesarean delivery patients. Outcome: BIS values. Results: BIS values between induction and delivery were lower in the labor group than non-labor group even though end-tidal sevoflurane concentrations were comparable. Conclusions: Further study is required to elucidate the mechanism of higher BIS scores in non-laboring women. Does this mean they are at higher risk for awareness? 18. Laudenbach V, Mercier FJ, Rozé J-C, et al. Anaesthesia mode for caesarean section and mortaility in very preterm infants: An epidemiologic study in the EPIPAGE cohort. Int J Obstet Anesth 2009; 18: 142-9 Secondary analysis of prospective, population-based, cohort study in 9 regions of France in 1977 in infants born between 27 and 32 weeks’ gestation, influence of maternal cesarean anesthesia on neonatal mortality. Group: Etude éPIdémiologique sur les Petitis Ages Gestationnels cohort, general vs. epidural vs. spinal anesthesia. Outcome: Neonatal mortality. Results: Neonatal mortality was 10.1% for general anesthesia, 12.2% for spinal anesthesia, and 7.7% for epidural anesthesia. There was a higher risk of neonatal death with spinal than general anesthesia (adjusted odds ratio 1.7; 95% CI 1.1-2.6). Conclusions: Multivariate analysis does not prove causation, but it could exist. Further study is required.
Post-Cesarean Delivery Analgesia
19. McDonnell JG, Curley G, Carney J, Benton A, Costello J, Maharaj CH, Laffey JG. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg 2008; 106: 186-91 Randomized controlled trial of transversus abdominis plane (TAP) block with ropivacaine after cesarean delivery (N = 50). Groups: TAP block vs. saline. Outcome: 48 h morphine consumption
Results: Mean 48-h morphine requirements were lower in the TAP group (18 vs. ± 14 mg vs. 66 ± 26 mg; P < 0.001). Conclusions: The TAP block is an excellent component of multimodal postoperative analgesia that can be performed blindly or with ultrasound guidance.
14

Session 2: Topical Issues 2 The use of oxytocic drugs during caesarean section Professor Rob Dyer Professor & Second Chair, Department of Anaesthesia, University of Cape Town, South Africa
Uterotonic drugs are essential pharmacological interventions during caesarean section, in order to diminish the risk of postpartum haemorrhage. They therefore contribute significantly to maternal safety. At the same time, these agents have a narrow therapeutic range in terms of maternal morbidity. The exact dose, route and rate of administration are thus important, as well as a detailed knowledge of their pharmacology. Central to the mechanism of the contraction of uterine smooth muscle during labour, which is enhanced by the action of oxytocin, is the enzyme myosin light chain kinase (MLCK). Intracellular calcium, the levels of which are controlled by voltage and receptor operated channels and by release from the sarcoplasmic reticulum, is bound to calmodulin and stimulates conversion of MLCK-P to MLCK, which in turn phosphorylates myosin and initiates smooth muscle contraction.1 The nonapeptide oxytocin was discovered by Sir Henry Dale and was the first polypeptide hormone synthesised, by Du Vigneaud, in 1953. The peptide binds to a G-Protein on the surface of the uterine myocyte, resulting in the generation of diacylglycerol (DAG) and inositol tri-phosphate (IP3) via the action of phospholipase – C on phosphatidyl inositol bisphosphate. DAG stimulates prostaglandin synthesis, and IP3 stimulates the release of calcium from the sarcoplasmic reticulum. Oxytocin also activates COX-2 via a further G-Protein interaction, and in so doing stimulates prostaglandin synthesis.1 The concentration of myometrial receptors as well as myometrial gap junctions increase as gestation advances, thus increasing sensitivity to oxytocin. Oxytocin has numerous physiological effects. Most importantly, it causes contraction, followed by relaxation of the uterus, and, at pharmacological doses, can cause an increased frequency of contractions and incomplete relaxation of the uterine musculature. It also has a role in sexual and maternal behaviour, and in memory and the regulation of food and drink intake. This agent remains the first line uterotonic during caesarean section.
The cardiovascular effects are complex. Hypotension is predominantly caused by transient relaxation of vascular smooth muscle cells, probably via calcium dependent stimulation of the nitric oxide pathway. It also causes the release of atrial and brain natriuretic peptide, and oxytocin or its preservative chlorbutanol may have negative inotropic effects on atrial myocytes.2 Oxytocin causes selective vasoconstriction of coronary, renal, splanchnic and skeletal muscle arteries, as well as umbilical vessels. Some papers have suggested the possibility of positive inotropic effects. Due to structural similarities with vasopressin, overdose of oxytocin may cause water retention, hyponatraemia, seizures and coma.3 Several papers have described the haemodynamic effects in the non-pregnant population and in the pregnant population during caesarean section. Early studies used intermittent indicator dilution or thermodilution technology,4,5 and more recently, beat by beat pulse wave form monitors,6,7 as well as monitors of changes in transthoracic bioimpedance,7,8 have elucidated a clinical picture of peripheral vasodilatation, hypotension, and increased cardiac output mediated by an increase in heart rate and stroke volume. Pulmonary artery pressures are markedly increased after a bolus of 10 IU.5 One observational study has demonstrated similar effects in patients with severe preeclampsia.9 These effects would be poorly tolerated if ventricular function were abnormal, and in the presence of mitral or aortic stenosis, or hypovolaemia. One fatality was recorded in the Confidential Enquiry into Maternal Deaths of the United Kingdom in the triennium 2002-2004, when oxytocin was administered during the resuscitation of a hypovolaemic patient during spinal anaesthesia for caesarean section.10 Co-administration of phenylephrine with oxytocin has been shown to obtund the peripheral vascular effects.7 Also, administration of 5 IU of oxytocin by slow infusion has been shown to produce less cardiovascular instability than a bolus of 5 IU.11 The efficacy of such infusions in terms of uterine contraction is difficult to assess other than by subjective means, but these probably suffice in most cases. The use of oxytocin in incremental doses of 0.1 IU in parturients with cardiac disease has recently
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
15

been shown to be associated with haemodynamic stability.12 In view of the multiple side effects of oxytocin, including nausea, vomiting, flushing, pruritus, headache, and possible chest pain,13,14 it is desirable to administer the lowest possible effective dose in the most haemodynamically stable manner. The dose and rate of intravenous infusion of oxytocin after delivery during caesarean section remain controversial. There have been only two dose response studies, one in healthy uncomplicated pregnancies at low risk for uterine atony,15 and another in a case series of patients with labour arrest.16 Both studies employed the up-down sequential method of establishing the median effective dose. The ED90 for low risk patients was found to be 0.35IU, and in patients with labour arrest the value was 3.0IU. In keeping with the mechanism of action, involving G-Protein receptor interactions, the phenomenon of receptor desensitisation may influence the effectiveness of the dose given by the anaesthetist at delivery. A recent publication in which a second dose of oxytocin was administered in the same patient, suggested that the cardiovascular response to the second dose was diminished,17 although at least one previous investigator did not demonstrate this effect. A diminished cardiovascular response would be in keeping with down-regulation. More definitive laboratory work has shown that loss of oxytocin receptors does occur during oxytocin-induced and oxytocin-augmented labour.18 Prior exposure of rat myometrium to oxytocin suggests a concentration-, but not time-dependent, reduced efficacy of oxytocin.19 On balance, then, it appears that repeated doses of oxytocin may become progressively less effective, and that pharmacological alternatives are still required. The newly developed synthetic analogue of oxytocin, carbetocin, has a half-life 4-10 times the duration of oxytocin. A tetanic uterine contraction is produced 2 minutes after an IV or IM injection of 100ug; this persists for 60 and 120 minutes after IV and IM injection respectively. Randomised trials suggest a diminished subsequent requirement for uterotonics when compared with oxytocin administered at caesarean section, and a lower risk for >500mL bloodloss following caesarean section.20 The side effect profile is similar to that of oxytocin. Preeclampsia remains a contraindication to its use, for reasons which are unclear.21 The issue of receptor desensitisation is as yet unstudied.
Currently, the ergot alkaloid ergometrine is the second line agent if uterine atony persists after oxytocin administration during caesarean delivery. Ergot alkaloids are all derivatives of 6-methylergoline. Ergometrine is a naturally occurring alkaloid, first isolated in 1932 by Dudley and Moir. Ergometrine maleate or methylergometrine may be administered IV or IM after delivery. It causes a rapid and sustained contraction of the pregnant and non-pregnant uterus. Little is known about the mechanism of action, which may be via a calcium channel. Ergometrine is also a partial agonist at alpha-adrenergic, 5HT-1, and dopamine receptors22 There are no published dose response curves. The recommended IV dose is 0.1mg IV slowly, to be followed by a further 0.1mg if required. The half-life of ergometrine is 120 minutes. Although ergometrine and methylergometrine have the least vasoconstrictor effects of all the ergot alkaloids, there is a significant incidence of hypertension, and myocardial infarction has been reported.23,24 In addition, troublesome nausea and vomiting can make caesarean delivery under spinal anaesthesia unpleasant. The incidence of nausea has been reported as 29%, and vomiting 9% after a bolus of 5 IU of oxytocin,25 and 10% after 250µg 15-methyl prostaglandin F2α26 during elective caesarean delivery under spinal anaesthesia. A high incidence of 46% of nausea or vomiting has been reported after 0.5mg ergometrine IV.27 Prostaglandins also increase intramyometrial calcium concentrations and enhance uterine contraction. Side effects include fever, diarrhoea, nausea and vomiting. The use of intramyometrial prostaglandin F2α for atonic postpartum haemorrhage was first described by Takagi in 1976.28 Subsequently, 15-methyl prostaglandin F2α was shown to have an extended half-life, fewer gastrointestinal and vasopressor side-effects, and good uterotonic activity.29,30 Since 15-methyl prostaglandin F2α may be associated with bronchospasm,31 ventilation perfusion mismatch and hypoxaemia,32 this agent is best used as a last resort therapy and not as prophylaxis.33 There is very limited experience with intravenous administration.34 Infusion at 100µg/minute during early pregancy has been shown to cause systemic and pulmonary hypertension, in contrast with prostaglandin E2, which is associated with a marked decrease in systemic vascular resistance and hypotension.35
Prostaglandin E1 is a safe, cheap and widely available oxytocic which may be a useful adjunct administered rectally during caesarean section in a dose of 800-1000µg in cases of uterine atony.36
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
16

In summary, uterotonic drugs remain an important adjunct to the surgical management of haemorrhage during caesarean section. Current evidence is that oxytocin remains the uterotonic of first choice. There are few definitive studies upon which to base a protocol for recommendations for dosing of oxytocin or second-line uterotonics. A bolus dose of 2.5 IU IV in combination with phenylephrine,7 or a 3-5 minute infusion of 2.5-5 IU is a reasonable approach, followed by a continuous infusion at less than 20 milliunits per minute.37 Down-regulation of oxytocin receptors following prior exposure to oxytocin, requires further study. This phenomenon results in the requirement for uterotonics with a different mechanism of action, such as ergometrine and prostaglandin F2α. Currently, ergometrine 0.1mg IV slowly, followed by a repeat dose of 0.1mg, is a logical second line agent in the absence of contraindications such as preeclampsia. 15-methyl prostaglandin F2α, 250µg intramyometrially, repeated every 15 minutes to a maximum of 8 doses, is the last resort. Dose response curves for the latter two agents would provide useful guidelines for the use of drugs with a very narrow therapeutic index. References
1. Arias F. Pharmacology of oxytocin and prostaglandins. Clin Obstet Gynecol 2000; 43: 455-68.
2. Rosaeg OP, Cicutti NJ, Labow RS. The effect of oxytocin on the contractile force of human atrial trabeculae. Anesth Analg. 1998; 86: 40-4.
3. Bergum D, Lonnee H, Hakli TF. Oxytocin infusion: acute hyponatraemia, seizures and coma. Acta Anaesthesiol.Scand. 2009; 53: 826-7.
4. Weis FR, Jr., Markello R, Mo B, Bochiechio P. Cardiovascular effects of oxytocin. Obstet Gynecol. 1975; 46: 211-4.
5. Secher NJ, Arnsbo P, Wallin L. Haemodynamic effects of oxytocin (syntocinon) and methyl ergometrine (methergin) on the systemic and pulmonary circulations of pregnant anaesthetized women. Acta Obstet Gynecol Scand 1978; 57: 97-103.
6. Langesaeter E, Rosseland LA, Stubhaug A. Hemodynamic effects of oxytocin during cesarean delivery. Int J Gynaecol Obstet 2006; 95: 46-7.
7. Dyer RA, Reed AR, van Dyk D, Arcache MJ, Hodges O, Lombard CJ, Greenwood J, James MF. Hemodynamic effects of ephedrine, phenylephrine and the coadministration of phenylephrine and oxytocin during spinal anesthesia for elective cesarean section. Anesthesiology 2009; 111: 753-65.
8. Pinder AJ, Dresner M, Calow C, Shorten GD, O'Riordan J, Johnson R. Haemodynamic changes caused by oxytocin during caesarean section
under spinal anaesthesia. Int J Obstet Anesth 2002; 11: 156-9.
9. Dyer RA, Piercy JL, Reed AR, Lombard CJ, Schoeman LK, James MF. Hemodynamic changes associated with spinal anesthesia for cesarean delivery in severe preeclampsia. Anesthesiology 2008; 108: 802-11.
10. Cooper GM, McClure JH. Maternal deaths from anaesthesia. An extract from Why Mothers Die 2000-2002, the Confidential Enquiries into Maternal Deaths in the United Kingdom: Chapter 9: Anaesthesia. Br.J Anaesth. 2005; 94: 417-23.
11. Thomas JS, Koh SH, Cooper GM. Haemodynamic effects of oxytocin given as i.v. bolus or infusion on women undergoing Caesarean section. Br J Anaesth 2007; 98: 116-9.
12. Langesaeter E, Dragsund M, Rosseland LA. Regional anaesthesia for a Caesarean section in women with cardiac disease: a prospective study. Acta Anaesthesiol Scand, in press.
13. Dogan R, Birdane A, Bilir A, Ekemen S, Tanriverdi B. Frequency of electrocardiographic changes indicating myocardial ischemia during elective cesarean delivery with regional and general anesthesia: detection based on continuous Holter monitoring and serum markers of ischemia. J Clin Anesth 2008; 20: 347-51.
14. Svanstrom MC, Biber B, Hanes M, Johansson G, Naslund U, Balfors EM. Signs of myocardial ischaemia after injection of oxytocin: a randomized double-blind comparison of oxytocin and methylergometrine during Caesarean section. Br J Anaesth 2008; 100: 683-9.
15. Carvalho JC, Balki M, Kingdom J, Windrim R. Oxytocin requirements at elective cesarean delivery: a dose-finding study. Obstet Gynecol 2004; 104: 1005-10.
16. Balki M, Ronayne M, Davies S, Fallah S, Kingdom J, Windrim R, Carvalho JC. Minimum oxytocin dose requirement after cesarean delivery for labor arrest. Obstet Gynecol 2006; 107: 45-50.
17. Langesaeter E, Rosseland LA, Stubhaug A. Haemodynamic effects of repeated doses of oxytocin during Caesarean delivery in healthy parturients. Br J Anaesth 2009; 103: 260-2.
18. Phaneuf S, Rodriguez LB, TambyRaja RL, MacKenzie IZ, Lopez BA. Loss of myometrial oxytocin receptors during oxytocin-induced and oxytocin-augmented labour. J Reprod Fertil 2000; 120: 91-7.
19. Magalhaes JK, Carvalho JC, Parkes RK, Kingdom J, Li Y, Balki M. Oxytocin pretreatment decreases oxytocin-induced myometrial contractions in pregnant rats in a concentration-dependent but not time-dependent manner. Reprod Sci 2009; 16: 501-8.
20. Rath W. Prevention of postpartum haemorrhage with the oxytocin analogue carbetocin. Eur.J Obstet Gynecol Reprod Biol, in press.
21. Vercauteren M, Palit S, Soetens F, Jacquemyn Y, Alahuhta S. Anaesthesiological considerations on tocolytic and uterotonic therapy in obstetrics. Acta Anaesthesiol Scand 2009; 53: 701-9.
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
17

22. de Groot AN, van Dongen PW, Vree TB, Hekster YA, van Roosmalen J. Ergot alkaloids. Current status and review of clinical pharmacology and therapeutic use compared with other oxytocics in obstetrics and gynaecology. Drugs 1998; 56: 523-35.
23. Hayashi Y, Ibe T, Kawato H, Futamura N, Koyabu S, Ikeda U, Shimada K. Postpartum acute myocardial infarction induced by ergonovine administration. Intern Med 2003; 42: 983-6.
24. Lin YH, Seow KM, Hwang JL, Chen HH. Myocardial infarction and mortality caused by methylergonovine. Acta Obstet Gynecol Scand 2005; 84: 1022.
25. Dansereau J, Joshi AK, Helewa ME, Doran TA, Lange IR, Luther ER, Farine D, Schulz ML, Horbay GL, Griffin P, Wassenaar W. Double-blind comparison of carbetocin versus oxytocin in prevention of uterine atony after cesarean section. Am J Obstet Gynecol 1999; 180: 670-6.
26. Balki M, Carvalho JC. Intraoperative nausea and vomiting during cesarean section under regional anesthesia. Int J Obstet Anesth 2005; 14: 230-41.
27. Moodie JE, Moir DD. Ergometrine, oxytocin and extradural analgesia. Br J Anaesth 1976; 48: 571-4.
28. Takagi S, Yoshida T, Togo Y, Tochigi H, Abe M, Sakata H, Fujii TK, Takahashi H, Tochigi B. The effects of intramyometrial injection of prostaglandin F2alpha on severe post-partum hemorrhage. Prostaglandins 1976; 12: 565-79.
29. Corson SL, Bolognese RJ. Postpartum uterine atony treated with prostaglandins. Am J Obstet Gynecol 1977; 129: 918-9.
30. Hayashi RH, Castillo MS, Noah ML. Management of severe postpartum hemorrhage due to uterine atony using an analogue of prostaglandin F2 alpha. Obstet Gynecol 1981; 58: 426-9.
31. Harber CR, Levy DM, Chidambaram S, Macpherson MB. Life-threatening bronchospasm after intramuscular carboprost for postpartum haemorrhage. BJOG 2007; 114: 366-8.
32. Andersen LH, Secher NJ. Pattern of total and regional lung function in subjects with bronchoconstriction induced by 15-me PGF2 alpha. Thorax 1976; 31: 685-92.
33. Chou MM, MacKenzie IZ. A prospective, double-blind, randomized comparison of prophylactic intramyometrial 15-methyl prostaglandin F2 alpha, 125 micrograms, and intravenous oxytocin, 20 units, for the control of blood loss at elective cesarean section. Am J Obstet Gynecol 1994; 171: 1356-60.
34. Granstrom L, Ekman G, Ulmsten U. Intravenous infusion of 15 methyl-prostaglandin F2 alpha (Prostinfenem) in women with heavy post-partum hemorrhage. Acta Obstet Gynecol Scand 1989; 68: 365-7.
35.Secher NJ, Thayssen P, Arnsbo P, Olsen J. Effect of prostaglandin E2 and F2alpha on the systemic and pulmonary circulation in pregnant anaesthetised
women. Acta Obstet Gynecol Scand 1982; 61: 213-18.
36. O'Brien P, El Refaey H, Gordon A, Geary M, Rodeck CH. Rectally administered misoprostol for the treatment of postpartum hemorrhage unresponsive to oxytocin and ergometrine: a descriptive study. Obstet Gynecol 1998; 92: 212-4.
37. Basson E, Odendaal HJ, Grove D. Oxytocin use in South Africa--a review. S Afr Med J 2004; 94: 839-45.
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
18

Session 2: Topical Issues 2 Neurological injury associated with childbirth & regional anaesthesia Professor Cynthia Wong Associate Professor, Chief of Obstetrical Anesthesia, Northwestern University Feinberg School of Medicine, USA
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
19

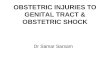
Position of Conus Medullaris
01020304050607080
Num
ber
(%)
T12-L1 L1 body L1-2 L2 body L2-3 <L3body
N = 100
Broadbent CR. Anaesthesia 2000
Damage to the Conus MedullarisT12
Syrinx
Reynolds F. Anaesthesia 2001
Preventing Direct Damage to the Spinal Cord/Nerve Roots
• Lumbar puncture < L3 vertebral body
• Halting needle advancement if patient reports pain
• Inject only if pain completely resolves
Direct Complications of Neuraxial Anesthesia
• Direct trauma
• Injection into unintended places
• Injection of unintended substances
• Transient neurologic syndrome
• Spinal epidural hematoma
• Spinal infection
• Vascular catastrophes
ASA Closed Claims Database
Lee LA. Anesthesiology 2004;101:143
Estimated incidence: 1:302,757 Reynolds F 2008
Sources of Infection
• Abscess: skin flora– Staph aureus
• Meningitis: Streptococcus viridans species
Skin Preparation:PI vs. Chlorhexidine
P < 0.02
Kinirons B. Anesthesiology 2001
N = 96
Skin Preparation: PI vs. Duraprep
Positive cultures DuraPrep
N (%)
PI
N (%)
Skin
Before disinfection 27 (90) 27 (90)
After disinfection 1 (3) 9 (30)*
Catheter removal 15 (50) 29 (97)*
Catheter tip 2 (7) 6 (20)*
*P < 0.01Birnbach DJ. Anesthesiology 2003
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
20

Sources of Infection
• Abscess: skin flora
• Meningitis: Streptococcus viridans
Meningitis Reports
Clinical Scenario Number
Spinal analgesia in labor 9
Spinal anesthesia for CS 11
Spinal anesthesia for retained placenta 1
CSE in labor 7
Epidural dural puncture in labor 3
“Uncomplicated” epidural in labor 6
TOTAL 38
Reynolds F. Anesthesiol Clin 2008;26:23
Viridans streptococci: vagina and oral cavity
Meningitis Case Clusters
• 4 cases of viridans streptococci meningitis after spinal anesthesia in 15 months
• One anesthesiologist– Recurrent pharyngitis– No handwashing– Did not remove jewelry– Did not wear a face mask– Wore sterile gloves
Schneeberger PM. Infection 1996;24:29
ASRA Consensus Conference 2004
Hebl JR. Reg Anesth Pain Med 2006;31:311-23
AAGBI
Anaesthesia 2008;63:1027
Direct Complications of Neuraxial Anesthesia: Lessons Learned
• Aim low (< L3)
• Spinal lidocaine: OK in OB
• Skin prep with EtOH w/ PI or chlorhexidine
• Wear a mask and don’t be too chatty
• Direct complications of neuraxial anesthesia
• Intrinsic obstetric palsies
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
21

Beatty 1838
Ann Kierman, aged 21 delivered of her first child, November 26th, 1836, after a labour of 7 hours; infant alive. Nothing remarkable occurred during labour, or afterwards, until she complained on the second day, that she could not move her right leg, and that it felt benumbed and dead….
…She continued to improve until the month of February, at which time she was walking about nearly well, and preparing to leave the hospital, when puerperal fever made its appearance in our wards.
She died of pericarditis 1 week later.
Intrinsic Obstetric Palsies
• Incidence
6157 Live births
9 Not interviewed6148 Interviewed
5594 Labored⇒⇒⇒⇒80 Nerve injuries⇒⇒⇒⇒72 examined by physiatrist
454 CS w/o labor ⇒⇒⇒⇒ 1 Nerve injury (0.22%)
9 Pre-existing injuries 55 new injuriesverified by physiatrist
(0.92%)Wong CA. Obstet Gynecol 2003
Postpartum Nerve Injury
Study/year N Incidence/10,000 (%)
Early 1900’s 400 (4)
Dar, 2002 2,615 58 (0.58)
Wong, 2003 6,157 92 (0.92)
23LAT FEM CUT
2 bilateral 19
FEM14 mixed5 sensory
5
33
2 LATERAL FEMORALCUTANEOUSFEMORAL
RADICULOPATHY
PERONEAL
LUMBOSACRALPLEXUSOTHER
Postpartum nerve injuries (patients with labor)
Multivariate analysis
Variable RR 95% CI P
Nulliparity 2.55 1.32 – 4.94 0.005
Prolonged 2nd stage
2.32 1.11 – 4.84 0.025
Neuraxial analgesia
2.00 0.98 – 4.08 0.057
Wong CA. Obstet Gynecol 2003
Intrinsic Obstetric Palsies and Neuraxial Analgesia
• Possible indirect relationship:
– Neuroblockade
• Prevents recognition of impending nerve injury
• Prolongs 2nd stage of labor
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
22

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Bibliography
1. Holdcroft A, Gibberd FB, Hargrove RL, Hawkins DF, Dellaportas CI. Neurological complications associated with pregnancy. Br J Anaesth 1995; 75: 522-6 2. Paech MJ, Godkin R, Webster GS. Complications of obstetric epidural analgesia and anaesthesia: a prospective analysis of 10,995 cases. Int J Obstet Anesth 1998; 7: 5-11 3. Dar AQ, Robinson APC, Lyons G. Postpartum neurologic symptoms following regional blockade: a prospective study with case controls. Int J Obstet Anesth 2002; 11: 85-90 4. Auroy Y, Benhamou D, Bargues L, Ecoffey C, Falissard B, Mercier FJ, Bouaziz H, Samii K. Major complications of regional anesthesia in France: The SOS Regional Anesthesia Hotline Service. Anesthesiology 2002; 97: 1274-80
5. Wong CA, Scavone BM, Dugan S, Smith JC, Prather H, Ganchiff JN, McCarthy RJ. Incidence of postpartum lumbosacral spine and lower extremity nerve injuries. Obstet Gynecol 2003; 101: 279-88 6. Broadbent CR, Maxwell WB, Ferrie R, Wilson DJ, Gawne-Cain M, Russell R. Ability of anaesthetists to identify a marked lumbar interspace. Anaesthesia 2000; 55: 1122-6 7. Reynolds F. Damage to the conus medullaris following spinal anaesthesia. Anaesthesia 2001; 56: 238-47 8. Lee LA, Posner KL, Domino KB, Caplan RA, Cheney FW. Injuries associated with regional anesthesia in the 1980s and 1990s: a closed claims analysis. Anesthesiology 2004; 101: 143-52 9. Kinirons B, Mimoz O, Lafendi L, Naas T, Meunier J, Nordmann P. Chlorhexidine versus povidone iodine in preventing colonization of continuous epidural catheters in children: a randomized, controlled trial. Anesthesiology 2001; 94: 239-44 10. Birnbach DJ, Meadows W, Stein DJ, Murray O, Thys DM, Sordillo EM. Comparison of povidone iodine and DuraPrep, an iodophor-in-isopropyl alcohol solution, for skin disinfection prior to epidural catheter insertion in parturients. Anesthesiology 2003; 98: 164-9 11. Reynolds F. Neurological infections after neuraxial anesthesia. Anesthesiol Clin 2008; 26: 23-52, v 12. Schneeberger PM, Janssen M, Voss A. Alpha-hemolytic streptococci: a major pathogen of iatrogenic meningitis following lumbar puncture. Case reports and a review of the literature. Infection 1996; 24: 29-33 13. Hebl JR. The importance and implications of aseptic techniques during regional anesthesia. Reg Anesth Pain Med 2006; 31: 311-23 14. Infection control in anaesthesia. Anaesthesia 2008; 63: 1027-36
23

Session 2: Topical Issues 2 Remifentanil for labour analgesia Dr David Hill Consultant Anaesthetist, Ulster Hospital, Belfast
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
24

Remifentanil pharmacokinetics in neonates
• Infants under 2 months
• Pharmacokinetics similar– to older children
– to adults
Davis, Ross Henson et al, Remifentanil pharmacokinetics in neonates.
Anesthesiology 1997; 87: A 1054
Pharmacokinetics
• Faster clearance in pregnancy
• Plasma levels 50% lower in pregnancy
• Effect site peak 1.3-1.6 min
• analgesia peak 30 sec - 2.5 min
• Typical contraction 70 sec
can a single bolus = a single contraction?
Kan et al 1998, Glass et al,1993, Babenco et al 2000, Caldeyro-Barcia et al 1960
Published data on efficacy
Bolus Dose
mcg/kg
Lockout time
(min)
Median or reduction in
pain scores (mm)
Conversion rate
to regional analgesia
Blair 2001 0.25-0.5 2 50 median 9.5%
Thurlow 2002 0.20 2 48 median 38%
Volmanen 2005 0.4 1 15 reduction Not reported
Blair 2005 40mcg 2 64 median 10%
Volmanen 2002 0.2-0.8 1 42 reduction Not reported
Evron 2005 0.27-0.93 3 35 median 10.8%
Volikas 2005 0.5 2 46 median 10%
Balki 2007 0.25 + infusion 2 not reported 5%
Published data on efficacy:comparison with entonox
• Crossover study 15 women
• Entonox or 0.4mcg/kg bolus remifentanil
• Reduction in pain scores– 15mm remifentanil
– 5mm entonox
14/15 preferred remifentanil
Volmanen et al 2005
Published data on efficacy: comparison with pethidine
• PCA pethidine– Analgesia similar– CTG benefit– Neonatal benefit
• IM pethidine– Analgesia benefit– More desaturation
• IVI pethidine– Analgesia benefit– CTG benefit– Desaturation benefit
Blair et al 2005, Thurlow et al 2002, Evron et al 2005
Data on 603 labouring women using PCA remifentanil
• 85% satisfied or very satisfied
• 77% no pain or bearable pain
• 84% used Entonox
• 10% conversion to regional
Hodgkinson et al 2008
What do women want?Sytematic review of 137 reports of the views of 14,000 women in 9 countries
Satisfaction– Expectations
– Support
– Quality of relationship with midwife
– Involvement in decision making
Dissatisfaction
– Failure of timing & lack of availability of analgesia
Hodnett 2002, Saisto 2001, Ranta 2002, May 2000
Complete analgesia did not rate highly
Maternal adverse effects (603 labouring women with remifentanil)
Hodgkinson et al 2008
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
25

Maternal desaturation: (603 labouring women with remifentanil)
• SpO2 <90% in 12%
– Independent of sedation score – 0.66% (4 women) had PCA stopped
• Rx – Continuous portable pulse oximeter
– Nasal oxygen 2l/min– Midwife
Hodgkinson et al 2008
Reasons for discontinuing (603 labouring women with remifentanil)
Inadequate analgesia 3.98%
Sedation/pushing 2.65%
Equipment failure 0.83%
Desaturation 0.66%
Nausea 0.5%
Itch 0.17%
Hodgkinson et al 2008
Remifentanil PCA launched for routine use in August 2005
• Bolus 40 mcg
• Delivered over 10 sec
• Lockout 2 min
Remifentanil PCA: practical safeguards
• Prescribed by anaesthetist
• Drug made up by 2 midwives
• Dedicated pumps
• Pumps locked
• Dedicated labelled cannula
Remifentanil PCA: monitoring1 to 1 Midwifery care– Continuous Sp02
– Regular observations
– CTG monitoring as normal
Anaesthetist present
for 1st 4 doses
Remifentanil PCA: Midwife training
• iv cannulation course
• iv drug course
• Drug preparation “5-5-10”
• Analgesia management “5-5”
• Extended training folder
• 6 month mentoring
Remifentanil PCA: Governance
• Continuous audit – outcomes & user satisfaction
• Policies & guidelines review
• Risk assessment review
• Critical incident reporting
• Work force planning
• Staff feedback
Remifentanil PCA: change in practice
• 2nd stage– Pushing-sedation conflict
– Pudendal nerve block “remi-pendal”
• More spinals – For trials
– For caesarean
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
26

Impact of remifentanil PCA
Northern Ireland Maternity System (NIMATS)
• Data retrieved from 5400 women
• Analgesia uptake
• Need for neonatal resuscitation
• Obstetric outcome
Analgesia uptake in 2yr period
0
20
40
60
80
100
120
09/2
005
10/2
005
11/2
005
12/2
005
01/2
006
02/2
006
03/2
006
04/2
006
05/2
006
06/2
006
07/2
006
08/2
006
09/2
006
10/2
006
11/2
006
12/2
006
01/2
007
02/2
007
03/2
007
04/2
007
05/2
007
06/2
007
07/2
007
08/2
007
Up
take
An
alg
esia
Epidural
Remifentanil
Analgesia uptake in 2yr period
0
20
40
60
80
100
120
09/2
005
10/2
005
11/2
005
12/2
005
01/2
006
02/2
006
03/2
006
04/2
006
05/2
006
06/2
006
07/2
006
08/2
006
09/2
006
10/2
006
11/2
006
12/2
006
01/2
007
02/2
007
03/2
007
04/2
007
05/2
007
06/2
007
07/2
007
08/2
007
Num
ber
Ana
lges
ia G
iven
Opiates
Epidural
CSE
Remifentanil
Neonatal effects: APGAR scores from 5400 neonates
APGAR SCORE @ 5 MINS
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Apgar 0 Apgar 1 Apgar 2 Apgar 3 Apgar 4 Apgar 5 Apgar 6 Apgar 7 Apgar 8 Apgar 9 Apgar 10
% o
f n
eon
ates
Epidural
Remifentanil
IM Opiates
Neonatal resuscitation: data from 5400 births
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
11.0
12.0
13.0
Pethidine EPIDURAL REMIFENTANIL
% R
ES
US
ITA
TE
D
BAG AND MASK
INTUBATION
OXYGEN
SUCTION + O2 VIA MASK
SUCTION ONLY
Analgesia choice by parity in 5400 women
Analgesia by Parity
0
200
400
600
800
1000
1200
IM Opiates Remifentanil Epidural
Nu
mb
er o
f w
om
en
Para 0
Para 1
Para 2
Para 3
Para 4+
Mode of delivery by analgesia choice in 5400 women
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
Pethidine Remifentanil Epidural
Normal
vacuum
Forcep
Caesarean
Effect of analgesia or midwife influence?
NIMATS data on obstetric outcome:
• 2yr before remi (4942 women)
• 2 yr after remi (5874 women)
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
27

Obstetric outcomes 2 yr before (4942 deliveries) and 2 yr after (5874 deliveries)
Remifentanil PCA
• Epidural rate
• Overall Caesarean
• Elective caesarean
• Emergency caesarean
• Vacuum
• Forceps
33 vs 17%
23.8 vs 23.6%
9.4% vs 9.5%
14.4 vs 14.2%
9.8 vs 12.3%
6.2 vs 9.2%
Obstetric outcome within analgesia groups: Remi vs epidural
• Forceps
• Vacuum
• Emergency caesarean
4.6 vs 21.4%
12.4 vs 18.3%
2.4 vs 21.7%
Remifentanil PCA offers……
• Modest analgesia
• Few neonatal effects
But requires………
• 1-1 midwifery
• Training
• Appropriate monitoring
In our unit……..
The introduction of Remifentanil PCA has
- Reduced the epidural rate
- Reduced anaesthetic workload
- Changed working practices
- Empowered our midwives
“midwive managed” analgesia:
Parturients using Remifentanil PCA should on average expect:
– 71% chance of a normal delivery
– 9.6% chance of caesarean delivery
– 2.4% emergency caesarean
– 6% neonates will require bag & mask
“midwive managed” analgesia
Parturients using Epidural analgesia should on average expect:
– 42% chance of a normal delivery
– 23% chance of caesarean delivery
– 21.1% emergency caesarean
– 11% neonates will require bag & mask
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
28

Session 3: Labour Analgesia CSE or epidural for labour analgesia? Professor Peter Pan Professor & Director of Anesthesia Clinical Research, Wake Forest University School of Medicine, Winston-Salem, USA
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
29

Traditional Epid vs CSE – Need for Rescue
� Only 3/26 outcomes showed differences**:
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
�** Urinary Retention (0.87) [0.80, 0.95]
Traditional Epid vs CSE
� Only 3/26 outcomes showed differences**:
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
Traditional Epid vs CSE - Pruritus
� Only 3/26 outcomes showed differences**:
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
�** Urinary Retention (0.87) [0.80, 0.95]
Traditional Epid vs CSE
� Only 3/26 outcomes showed differences**:
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
�** Urinary Retention (0.87) [0.80, 0.95]
Traditional Epid vs CSE – Urinary Retention
� Only 3/26 outcomes showed differences**:
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
�** Urinary Retention (0.87) [0.80, 0.95]
Traditional Epid vs CSE
� Only 3/26 outcomes showed differences**:
� Time to Effective Analgesia (-4.00min) [-8.08,0.08]
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
�** Urinary Retention (0.87) [0.80, 0.95]
� Instrument Delivery (0.82) [0.67, 1.00]
Traditional Epid vs CSE – Onset Time
� Only 3/26 outcomes showed differences**:
� Time to Effective Analgesia (-4.00min) [-8.08,0.08]
�** Need for Rescue Analgesia (0.31) [0.14, 0.70]
�** Pruritus (1.74) [1.40, 2.15]
�** Urinary Retention (0.87) [0.80, 0.95]
� Instrument Delivery (0.82) [0.67, 1.00]
Low Dose Epid vs CSE
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
� Need for Rescue Analgesia (0.96) [0.77, 1.20]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (-0.02) [-0.02, -0.02]
� Instrument Delivery (1.07) [0.88, 1.30]
� Cesarean Delivery (0.99) [0.82, 1.20]
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
30

Low Dose Epid vs CSE – Onset Time
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
� Need for Rescue Analgesia (0.96) [0.77, 1.20]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (-0.02) [-0.02, -0.02]
� Instrument Delivery (1.07) [0.88, 1.30]
� Cesarean Delivery (0.99) [0.82, 1.20]
Low Dose Epid vs CSE
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
Low Dose Epid vs CSE – Effective @ 10min
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
� Need for Rescue Analgesia (0.96) [0.77, 1.20]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (-0.02) [-0.02, -0.02]
� Instrument Delivery (1.07) [0.88, 1.30]
� Cesarean Delivery (0.99) [0.82, 1.20]
Low Dose Epid vs CSE
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
�** Pruritus (1.62) [1.34, 1.97]
Low Dose Epid vs CSE - Pruritus
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
� Need for Rescue Analgesia (0.96) [0.77, 1.20]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (-0.02) [-0.02, -0.02]
� Instrument Delivery (1.07) [0.88, 1.30]
� Cesarean Delivery (0.99) [0.82, 1.20]
Low Dose Epid vs CSE
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (** Umbilical Artery pH (** Umbilical Artery pH (** Umbilical Artery pH (----0.02) [0.02) [0.02) [0.02) [----0.02, 0.02, 0.02, 0.02, ----0.02]0.02]0.02]0.02]
Low Dose Epid vs CSE – Umbilical A pH
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
� Need for Rescue Analgesia (0.96) [0.77, 1.20]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (-0.02) [-0.02, -0.02]
� Instrument Delivery (1.07) [0.88, 1.30]
� Cesarean Delivery (0.99) [0.82, 1.20]
Low Dose Epid vs CSE
� Only 4/26 outcomes showed differences**:
�** Time to Effective Analgesia (-5.59 min) [-6.59, -4.58]
� **Analgesia Effective @10min (1.96) [1.50, 2.57]
� Need for Rescue Analgesia (0.96) [0.77, 1.20]
�** Pruritus (1.62) [1.34, 1.97]
�** Umbilical Artery pH (-0.02) [-0.02, -0.02]
� Instrument Delivery (1.07) [0.88, 1.30]
� Cesarean Delivery (0.99) [0.82, 1.20]
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
31

Labor Progress and Process
� Effects on C/S Rate
� Effects on Progress of Labor
Meta-analysis of EA on OB outcomes
1. Halpern (JAMA 1998)
• 10 Randomized Clinical Trials, N=2369
• Epid gp N=1183, IV/IM gp N=1186,
• C/S Rate: No Difference between gps
– 8.2% C/S (Epid gp)
– 5.5% C/S (IV/IM gp);
• 1st Stage Labor: Longer in Epidural gp
• 2nd Stage Labor : Longer in Epidural gp
• Instrument Delivery: Higher in Epidural gp
• (Especially vs. high LA Conc Epid)
Meta-analysis of EA on OB outcomes
2. Leighton (AJOBG 2002)
• 14 Randomized Clinical Trials Updated
• Almost 4300 pts, Epid vs IV/IM
• Similar Conclusions as Halpern
3. Zhang (AJOBG 1991)
• 4 RCTs, 4 observational studies.
All 3 series of meta-analysis concluded:
EA NOT affecting C/S rate.
Effects of CSE on Labor Progress
� Cervical DilationCervical DilationCervical DilationCervical Dilation
� ((((TsenTsenTsenTsen. Anesthesiology 1999;91:920. Anesthesiology 1999;91:920. Anesthesiology 1999;91:920. Anesthesiology 1999;91:920----5.)5.)5.)5.)
� CSE sufentanil 10 CSE sufentanil 10 CSE sufentanil 10 CSE sufentanil 10 ugugugug + + + + bupbupbupbup 2.5mg (n=50)2.5mg (n=50)2.5mg (n=50)2.5mg (n=50)
� EpidEpidEpidEpid 12ml 0.25% bupivacaine (n=50)12ml 0.25% bupivacaine (n=50)12ml 0.25% bupivacaine (n=50)12ml 0.25% bupivacaine (n=50)
� NulliparousNulliparousNulliparousNulliparous SpontaneoulsySpontaneoulsySpontaneoulsySpontaneoulsy laboring laboring laboring laboring parturientsparturientsparturientsparturients
� Faster dilationFaster dilationFaster dilationFaster dilation(p<.01)(p<.01)(p<.01)(p<.01)---->>>>2.3cm/hr CSE 2.3cm/hr CSE 2.3cm/hr CSE 2.3cm/hr CSE vsvsvsvs 1.3cm/hr EA1.3cm/hr EA1.3cm/hr EA1.3cm/hr EA....
� Pan et al. (SOAP 96,97) reported a Pan et al. (SOAP 96,97) reported a Pan et al. (SOAP 96,97) reported a Pan et al. (SOAP 96,97) reported a shorter duration of 1st shorter duration of 1st shorter duration of 1st shorter duration of 1st
stage labor, and less instrumentstage labor, and less instrumentstage labor, and less instrumentstage labor, and less instrument delivery with CSE delivery with CSE delivery with CSE delivery with CSE fentanylfentanylfentanylfentanyl
versus EA.versus EA.versus EA.versus EA.
Effects of CSE on Labor Progress and C/S Rate
Wong. NEJM 2005; 352:655Wong. NEJM 2005; 352:655Wong. NEJM 2005; 352:655Wong. NEJM 2005; 352:655----65.65.65.65.
� 750 750 750 750 nulliparousnulliparousnulliparousnulliparous sponsponsponspon labor or ROM, <4cm dilatelabor or ROM, <4cm dilatelabor or ROM, <4cm dilatelabor or ROM, <4cm dilate
� 1111stststst
analganalganalganalg request: IT fentanyl or IV request: IT fentanyl or IV request: IT fentanyl or IV request: IT fentanyl or IV HydromorphoneHydromorphoneHydromorphoneHydromorphone
� 2222ndndndnd
analganalganalganalg request: EA initiated in both groupsrequest: EA initiated in both groupsrequest: EA initiated in both groupsrequest: EA initiated in both groups
� AnalgAnalgAnalgAnalg to CCto CCto CCto CC ---->>>>295min CSE 295min CSE 295min CSE 295min CSE vsvsvsvs 385min IV/EA385min IV/EA385min IV/EA385min IV/EA (P<.001)(P<.001)(P<.001)(P<.001)
� AnalgAnalgAnalgAnalg to VDto VDto VDto VD ----> > > > 398 min CSE 398 min CSE 398 min CSE 398 min CSE vsvsvsvs 479min IV/EA479min IV/EA479min IV/EA479min IV/EA (P<.001)(P<.001)(P<.001)(P<.001)
� No difference in No difference in No difference in No difference in C/S rateC/S rateC/S rateC/S rate between CSE between CSE between CSE between CSE vsvsvsvs IV/EA group IV/EA group IV/EA group IV/EA group
(17.8% (17.8% (17.8% (17.8% vsvsvsvs 20.7%)20.7%)20.7%)20.7%)
Fetal Brady – CSE vs EA
�Cohen. Anesth Analg 1993;77:1155-1160.
�15% FHR changes with IT suf 10ug
�Clark. Anesthesiology 1994;81:1083.
�IT fentanyl: 9 fetal brady, 5/9 with uterine
tetany
CSECSECSECSE
A cause of fetal A cause of fetal A cause of fetal A cause of fetal bradycardiabradycardiabradycardiabradycardia????
• PROPOSED MECHANISMPROPOSED MECHANISMPROPOSED MECHANISMPROPOSED MECHANISM::::
• Labor Labor Labor Labor →→→→ pain pain pain pain →→→→ ↑↑↑↑ epinephrine epinephrine epinephrine epinephrine
• CSE CSE CSE CSE →→→→ ↓↓↓↓ pain pain pain pain →→→→ ↓↓↓↓ epinephrine more than NE epinephrine more than NE epinephrine more than NE epinephrine more than NE →→→→↓↓↓↓ ββββ agonist (relaxant) effects on uterus agonist (relaxant) effects on uterus agonist (relaxant) effects on uterus agonist (relaxant) effects on uterus →→→→↑↑↑↑ uterine toneuterine toneuterine toneuterine tone
Fetal Brady – CSE vs EA� Lack of Agreement in Literature – Norris. IJOA 2000;9:264-9
� Van de Van de Van de Van de VeldeVeldeVeldeVelde. . . . Anesth Anesth Anesth Anesth AnalgAnalgAnalgAnalg 2004;98:11532004;98:11532004;98:11532004;98:1153----9999. (100/gp X3). (100/gp X3). (100/gp X3). (100/gp X3)
� 24%24%24%24% (IT 7.5 7.5 7.5 7.5 ugugugug sufsufsufsuf) ) ) ) ---- Fetal Brady/Fetal Brady/Fetal Brady/Fetal Brady/AbnAbnAbnAbn DecelDecelDecelDecel
� 11% (EA) 11% (EA) 11% (EA) 11% (EA) & & & & 12% (IT 1.5ug12% (IT 1.5ug12% (IT 1.5ug12% (IT 1.5ug suf+bup+epi)
� NielsenNielsenNielsenNielsen.... Anesth Anesth Anesth Anesth AnalgAnalgAnalgAnalg 1996;83:7421996;83:7421996;83:7421996;83:742----6666....
� 65 IT opioid vs 69EA sequentially
� NO DiffNO DiffNO DiffNO Diff in abn FHR changes (17%)
� MardirosoffMardirosoffMardirosoffMardirosoff.... Br J Obstet Br J Obstet Br J Obstet Br J Obstet GynaecolGynaecolGynaecolGynaecol 2002;109:2742002;109:2742002;109:2742002;109:274----81818181....
� Review 24 studies
� 2020 IT opioid, 1493 control
� 1.8 X1.8 X1.8 X1.8 X (95% CI 1.04-3.1) for IT opioid incr fetal brady
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
32

Fetal Brady – CSE vs Epid� Abrao KC et al. (Obsetrics and Gynecology 2009; 113:41-7)
�RCT, mixed parity, < 7 cm, Intrauterine pressure
�CSE (2.5mg bup+ 2.5ug suf) (n=41)
�EPID (10mL .125% bup + 10ug suf) (n=36)
� Primary Outcome measure: (monitor 15m post analg)
�Prolong decel = baseline HR - 15 for >2-10min
�Bradycardia = baseline <100 bpm
�Incr Uterine tone = >10mmHg incr from basal
Abrao KC et al. (Obsetrics and Gynecology 2009; 113:41-7)
.49.49.49.490 (0%)0 (0%)0 (0%)0 (0%)2 (5%)2 (5%)2 (5%)2 (5%)
FHR Abnormal with FHR Abnormal with FHR Abnormal with FHR Abnormal with
HypotensionHypotensionHypotensionHypotension
<.01<.01<.01<.011 (3%)1 (3%)1 (3%)1 (3%)11 (27%)11 (27%)11 (27%)11 (27%)
FHR Abnormal with FHR Abnormal with FHR Abnormal with FHR Abnormal with
HypertonusHypertonusHypertonusHypertonus
<.01<.01<.01<.012 (6%)2 (6%)2 (6%)2 (6%)13 (32%)13 (32%)13 (32%)13 (32%)Fetal HR AbnormalFetal HR AbnormalFetal HR AbnormalFetal HR Abnormal
.018.018.018.0186 (17%)6 (17%)6 (17%)6 (17%)17 (42%)17 (42%)17 (42%)17 (42%)Uterine Tone ElevatedUterine Tone ElevatedUterine Tone ElevatedUterine Tone Elevated
PEPID (n=36)CSE (n=41)Outcomes
Abrao KC et al. (Obsetrics and Gynecology 2009; 113:41-7)
0.0490.0490.0490.0490.590.590.590.59----0.990.990.990.990.7720.7720.7720.772
FHR Abnormal + FHR Abnormal + FHR Abnormal + FHR Abnormal + IncrIncrIncrIncr Uterine ToneUterine ToneUterine ToneUterine Tone
DecrDecrDecrDecr pain scores 5 m after pain scores 5 m after pain scores 5 m after pain scores 5 m after AnalgAnalgAnalgAnalg
<0.001<0.001<0.001<0.001
0.5410.5410.5410.541
4.464.464.464.46----77.7277.7277.7277.72
0.090.090.090.09---- 3.573.573.573.57
18.6218.6218.6218.62
0.560.560.560.56
FHR AbnormalitiesFHR AbnormalitiesFHR AbnormalitiesFHR Abnormalities
IncrIncrIncrIncr Uterine Tone After Uterine Tone After Uterine Tone After Uterine Tone After AnalgAnalgAnalgAnalg
PostblockPostblockPostblockPostblock Hypotension Hypotension Hypotension Hypotension
0.0220.0220.0220.022
0.7190.7190.7190.719
1.211.211.211.21----10.3610.3610.3610.36
0.880.880.880.88---- 1.091.091.091.09
3.5263.5263.5263.526
0.9810.9810.9810.981
IncrIncrIncrIncr Uterine Tone After Uterine Tone After Uterine Tone After Uterine Tone After AnalgAnalgAnalgAnalg
CSE CSE CSE CSE vsvsvsvs EpiduralEpiduralEpiduralEpidural
Oxytocin dose @ Oxytocin dose @ Oxytocin dose @ Oxytocin dose @ AnalgAnalgAnalgAnalg InitiationInitiationInitiationInitiation
P95% CIO.R.Outcome Variables Impact of Bradycardia on OB Outcomes
• Gambling (98) showed no diff in spon del or C/Sbetween CSE and IV meperidine.
• Albright et al series showed no difference in emergent C/S in CSE vs Epid.(1997)
• Abrao et al. No cases need tocolysis or C/S for suspected fetal distress. No neonatal outcome differences.
Some Classic Comments about CSE
• “A labor epidural catheter is being dosed for C/S and is not “A labor epidural catheter is being dosed for C/S and is not “A labor epidural catheter is being dosed for C/S and is not “A labor epidural catheter is being dosed for C/S and is not
quite working.”quite working.”quite working.”quite working.”
• Typical Comment:Typical Comment:Typical Comment:Typical Comment: “Was it a CSE catheter?”“Was it a CSE catheter?”“Was it a CSE catheter?”“Was it a CSE catheter?”
• Question:Question:Question:Question:
• Does CSE Does CSE Does CSE Does CSE cathcathcathcath has has has has more chance to failmore chance to failmore chance to failmore chance to fail when used for when used for when used for when used for
C/S than Traditional C/S than Traditional C/S than Traditional C/S than Traditional EpidEpidEpidEpid cathcathcathcath ((((bbbbeeeeccccaaaauuuusssseeee iiiitttt iiiissss uuuunnnntttteeeesssstttteeeedddd oooorrrr
not fully testednot fully testednot fully testednot fully tested) ?) ?) ?) ?
•
Attempts to answer the controversial question
� 3 yrs (2000-2)
� Retrospective Analysis
� 19 259 deliveries,
� 7849 (47%) EA
� 4741 (28%) CSE for Labor Analg
� Limitation Limitation Limitation Limitation –––– Retrospective, not controlled Retrospective, not controlled Retrospective, not controlled Retrospective, not controlled
Complications – FMC Experiences
<.0000011.5%.65%1.9%Multiple Replaced
<.0021.2%(30%).8%(28%)1.4%(31%)Wet Tap/EBP needed
<.0000015.6%3.2%7.1%Epid Cath Replaced
<.0000016.8%4.2%8.4%Inadeq Epid Analg
NS.25.25%.24%Subseq Migrated IV
<.0003
<.000001
P-value
6%5%7%Initial IV Cath
12%10%14%Overall Failure
Total
(n=12590)
CSE
(n=4741)
Epidural
(n=7849)Labor Analgesia
How about Labor Epid Cath-in-situ needed for C/S?
4%6%Norris
10.5%Garry
18%
7.1%
Labor Epid-in-
situ for C/S
Eappen
Pan
Labor CSE-in-
situ for C/S
Labor Epid Cath
Fail @ C/S
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
33

Labor Epidural vs CSE for C/S (2007-8)
�2 year prospective data collection ongoing study
�All pts with Labor Epid/CSE presenting for C/S
�Incidence of Failed labor epidural catheters
when needed for C/S
�Identify when catheters Failed or Replaced and
for what reasons
�Normalize between groups for:
� BMI
� Provider experience
� Labor duration.
Labor Epidural vs CSE for C/S (2007-8)
8.0%8.0%8.0%8.0%6.8%6.8%6.8%6.8%D. Catheters Failed and/or replaced just for D. Catheters Failed and/or replaced just for D. Catheters Failed and/or replaced just for D. Catheters Failed and/or replaced just for
C/S C/S C/S C/S ---- (%) (sum of B and C)(%) (sum of B and C)(%) (sum of B and C)(%) (sum of B and C)
1.2%0.5%F. Unknown cath function @ C/S (not dosed or
inadequate time) – (%)
17.4%12.6%E. All Failed + Replaced @ labor or C/S – (%)
5.4%4.5%C. Known Non-functioning cath + Failed cath
for C/S despite adequate dosing – (%) (not B)
2.6%2.3%B. Catheters Replaced just for C/S
9.4%5.8%A. Catheters Replaced during Labor – (%)
Epid
(n=700)
CSE
(n= 310)Outcomes - (%) (Prelim Results)
Is CSE catheter more likely to fail for C/S ?
�Evidences do support higher CSE catheter failure.
�How often do you replace a catheter immediately
after initial dosing (i.e. excluding spinal, iv and
obvious misplaced indications)?
�Indications – IV/spinal cath, poor LOR, difficult
catheter insertion, or (in CSE – no spinal CSF)
�Answer also depends on experience and
aggressiveness of testing the catheter.
Who would I personally use or not
use CSE labor analgesia
� Consider USE CSEConsider USE CSEConsider USE CSEConsider USE CSE
� Early labor Early labor Early labor Early labor
� Late LaborLate LaborLate LaborLate Labor
� Severe Labor PainSevere Labor PainSevere Labor PainSevere Labor Pain
� ?back surgery pt?back surgery pt?back surgery pt?back surgery pt
�Consider NOT USE CSEConsider NOT USE CSEConsider NOT USE CSEConsider NOT USE CSE
�Pending C/S Pending C/S Pending C/S Pending C/S (<1(<1(<1(<1----2h or so2h or so2h or so2h or so))))
�Underlying fetal heart rate Underlying fetal heart rate Underlying fetal heart rate Underlying fetal heart rate
abnormalities/concernsabnormalities/concernsabnormalities/concernsabnormalities/concerns
�Underlying fetal Underlying fetal Underlying fetal Underlying fetal
stress/distress concernsstress/distress concernsstress/distress concernsstress/distress concerns
Conclusion� CSE faster onset labor analgesia, but more CSE faster onset labor analgesia, but more CSE faster onset labor analgesia, but more CSE faster onset labor analgesia, but more prurituspruritusprurituspruritus
� Motor block depends upon dose of LA used in EA or CSE.Motor block depends upon dose of LA used in EA or CSE.Motor block depends upon dose of LA used in EA or CSE.Motor block depends upon dose of LA used in EA or CSE.
� No significant diff in C/S rate No significant diff in C/S rate No significant diff in C/S rate No significant diff in C/S rate
� Similar instrument delivery if low Similar instrument delivery if low Similar instrument delivery if low Similar instrument delivery if low concconcconcconc LA with opioid is used in EA. LA with opioid is used in EA. LA with opioid is used in EA. LA with opioid is used in EA.
� CSE “may” offer faster cervical dilation.CSE “may” offer faster cervical dilation.CSE “may” offer faster cervical dilation.CSE “may” offer faster cervical dilation.
� EpidEpidEpidEpid cathcathcathcath failure seems same or less with CSE with similar failure seems same or less with CSE with similar failure seems same or less with CSE with similar failure seems same or less with CSE with similar
complications rate. complications rate. complications rate. complications rate. RCTsRCTsRCTsRCTs to confirm or refute this finding.to confirm or refute this finding.to confirm or refute this finding.to confirm or refute this finding.
� DP itself in CSE does not alter the DP itself in CSE does not alter the DP itself in CSE does not alter the DP itself in CSE does not alter the epidepidepidepid cathcathcathcath success/failure, but may success/failure, but may success/failure, but may success/failure, but may
offer additional information on success/failure of epidural offer additional information on success/failure of epidural offer additional information on success/failure of epidural offer additional information on success/failure of epidural cathcathcathcath....
Old and New Thoughts on Combined
Spinal Epidural (CSE): Can CSE be used
for all Laboring Patients?
Peter H. Pan, MSEE, MD
Department of Anesthesiology
Wake Forest University School of Medicine
Winston-Salem, North Carolina
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
34

Session 3: Labour Analgesia Maintaining labour epidurals - an update Professor Cynthia Wong Associate Professor, Chief of Obstetrical Anesthesia, Northwestern University Feinberg School of Medicine, USA
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
35

CSE vs. Epidural
Nageotte MP. N Eng J Med 1997
Conclusions:
• Dense second stage analgesia may increase the rate of instrumental vaginal delivery
Methods of Maintaining Epidural Analgesia
• Manual bolus
• Continuous infusion
• PCEA with and without background infusion
• Programmed intermittent bolus
Epidural Maintenance
• Continuous infusion vs. bolus– Fewer manual boluses
– Greater patient satisfaction
– Greater anesthesiologist satisfaction
– Greater bupivacaine consumption
Intermittent Epidural Boluses vs. Continuous Infusion
StudyBupivacaine Dose (mg)
Motor BlockBolus Infusion
Bogod 1987
130 ± 70 178 ± 83† 44% vs. 64%†
Smedstad 1988
87 ± 54 161 ± 71†Forceps
24% vs. 54%†
Boutros 1999
10.6 ± 2.4 (/h)
14.6 ± 3.8†(/h)
4% vs. 22%†
†P < 0.05
Epidural Maintenance
• Continuous infusion vs. bolus– Fewer manual boluses
– Greater patient satisfaction
– Greater anesthesiologist satisfaction
– Greater bupivacaine consumption
– Greater motor block
– Increased incidence of instrumental vaginal delivery
Conclusions
• Dense second stage analgesia may increase the rate of instrumental vaginal delivery
• Continuous infusions result in more dense neuroblockade than bolus injections– Use dilute (< bupivacaine 0.125%) infusion
solutions
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
36

Methods of Maintaining Epidural Analgesia
• Manual bolus
• Continuous infusion
• PCEA with and without background infusion
• Programmed intermittent bolus
van der Vyver M. Br J Anaesth 2002:89:459
The number of patients who required no unscheduled interventionsby the clinician
PCEA (no BI) vs. CEIPCEA CEI
RD/WMD (95% CI)n or n/N
No interventions 187/272 100/243 27% (18 to 36%) *
LA consumption (mg/h)
257 221 -3.9 (-5.4 to -2.4) *
No motor block 131/167 103/129 18% (6 to 31%) #
Satisfied w/ analgesia
65/75 73/84 0% (-11 to 10%)
*P < 0.001, #P < 0.003
van der Vyver M. Br J Anaesth 2002:89:459
Epidural Maintenance
• Bolus vs. continuous infusion
• Continuous infusion vs. PCEA
• PCEA with and without background infusion
• Programmed intermittent bolus
• Maintenance solutions/protocols
PCEA: w/ and w/o Background Infusion
N BI (mL/h) Bolus (mL)
Outcome
Ferrante 1994 600, 3, 6, 12
(CEI)3
Inc suppl at 0, 3
Inc dose at 12
Paech 1992 52 4 4 No differences
Petry 2000 80 3 3 No differences
Bupivacaine 0.125% / fentanyl or sufentanil
PCEA: w/ and w/o Background Infusion
Ropivacaine 0.1% / sufentanil 0.5 µg/mL
Boselli E. Anesthesiology 2004;100:968
8894
8791
N=133
PCEA: w/ and w/o Background Infusion
Boselli E. Anesthesiology 2004;100:968
PCEA: w/ and w/o Background Infusion
0 mL/h
N = 34
3 mL/h
N = 34
6 mL/h
N = 32
9 mL/h
N = 33
Supplemental bolus (1-2) (%)
15 19 16 16
NSVD (%) 79 64 84 82
Satisfaction (0-10)
9 9 9 9
Boselli E. Anesthesiology 2004;100:968
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
37

PCEA: w/ and w/o Background Infusion
Ropivacaine 0.16% / sufentanil 0.5 µg/mL / BI: 4 mL/h
Bremerich DH. Int J Obstet Anesth 2005;14:114
8894
8791
8% 23% P < 0.001
N=66
(4 mL/h)(4 mL)
• PCEA with and without background infusion– Low volume background infusions make little
difference
– Higher volume (> 5 mL/h) helpful with longer labors, patients wanting to sleep
• ? Dependent of LA concentration
• ? Increase in LA consumption
• Little clinical significance with low concentration infusions
• 30-50% total volume via infusion
Halpern SH. Anesth Analg 2009;108:921
Methods of Maintaining Epidural Analgesia
• Manual bolus
• Continuous infusion
• PCEA with and without background infusion
• Programmed intermittent bolus
• Bolus injection through an epidural catheter may result in better drug distribution than continuous infusion
Kaynar AM. Anesth Analg 1999
0.4 mL 4 mL 10 mL
Hogan Q. Anesthesiology 1999:90:4
Tip epidural catheter
Anesth Analg 2006;102:904
Bupivacaine 0.0625% / fentanyl 2 ug/mL
RCT, N = 126
12 mL/h vs. 6 mL q30 min
P = 0.006
Wong CA. Anesth Analg 2006:102:904
Labor Analgesia
PIEB (n=63) CEI (n=63) P
Baseline VAS (mm) 59 ± 18 57 ± 16 0.59
Labor paina 6.7 (0, 42.3) 10.3 (0, 57.6) 0.25
Epidural dose (mg�h-1) 6.7 (5.1, 7.7) 7.4 (5.7, 7.4) 0.001
PCEA requests (n�h-1) 1.1 (0, 5.4) 1.3 (0, 6.7) 0.60
PCEA dose (mg�h-1) 2.5 (0, 6.7) 2.6 (0, 8.4) 0.87
Manual dose (n) 20 34 0.01
Manual dose (mg�h-1) 0 (0, 10.6) 1.6 (0, 17.4) 0.02
a = (Area under the VAS * time curve)/duration of neuraxial analgesia.
Wong CA. Anesth Analg 2006:102:904
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
38

Wong CA. Anesth Analg 2006:102:904 Chua SMH. Can J Anaesth 2004
PIEB vs. Continuous Infusion
Ropivaine 0.1% / F 2 µg/ml: 5 mL/h vs. 5 mL q60 min
N = 42
PIEB vs. Continuous Infusion
PIEB (n=30) CEI (n=30) P
Breakthrough pain n(%)
3 (10) 11 (37) 0.04
Satisfaction score (0 – 100 mm) 97 ± 8 89 ± 7 0.003
Lim Y. Int J Obstet Anesth 2005;14:305
L-bupivacaine 0.1% / fentanyl 2 µg/mL
5 mL q30 min vs. 10 mL/h
• Programmed intermittent bolus– Less drug
– Less breakthrough pain
– Improved satisfaction
– Current pump technology needs to catch up
Conclusions
• Dense second stage analgesia may increase the rate of instrumental vaginal delivery
• Continuous infusions result in more dense neuroblockade than bolus injections– Use dilute (< bupivacaine 0.125%) infusion
solutions
• PCEA and programmed intermittent bolus techniques are methods of continuous analgesia that rely on bolus dosing
Chicago 2008
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
39

References 1. Leighton BL, Halpern SH. Epidural dural analgesia
and the progress of labor, Evidence-Based Obstetric Anesthesia. Edited by Halpern SH, Douglas MJ. Oxford, Blackwel, 2005, pp 10-22
2. Comparative Obstetric Mobile Epidural Trial Study Group UK. Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomised controlled trial. Lancet 2001; 358: 19-23
3. Nageotte MP, Larson D, Rumney PJ, Sidhu M, Hollenbach K. Epidural analgesia compared with combined spinal-epidural analgesia during labor in nulliparous women. N Eng J Med 1997; 337: 1715-9
4. Bogod DG, Rosen M, Rees GA. Extradural infusion of 0.125% bupivacaine at 10 mL/hr to women during labor. Br J Anaesth 1987; 59: 325-30
5. Smedstad KG, Morison DH. A comparative study of continuous and intermittent epidural analgesia for labour and delivery. Can J Anaesth 1988; 35: 234-41
6. Boutros A, Blary S, Bronchard R, Bonnet F. Comparison of intermittent epidural bolus, continuous epidural infusion and patient controlled-epidural analgesia during labor. Int J Obstet Anesth 1999; 8: 236-41
7. van der Vyver M, Halpern S, Joseph G. Patient-controlled epidural analgesia versus continuous infusion for labour analgesia: a meta-analysis. Br J Anaesth 2002; 89: 459-65
8. Ferrante FM, Rosinia FA, Gordon C, Datta S. The role of continuous background infusions in patient-controlled epidural analgesia for labor and delivery. Anesth Analg 1994; 79: 80-4
9. Paech MJ. Patient-controlled epidural analgesia in labour--is a continuous infusion of benefit? Anaesthesia & Intensive Care 1992; 20: 15-20
10. Petry J, Vercauteren M, Van Mol I, Van Houwe P, Adriaensen HA. Epidural PCA with bupivacaine 0.125%, sufentanil 0.75 microgram and epinephrine 1/800.000 for labor analgesia: is a background infusion beneficial? Acta Anaesthesiol Belg 2000; 51: 163-6
11. Boselli E, Debon R, Cimino Y, Rimmele T, Allaouchiche B, Chassard D. Background infusion is not beneficial during labor patient-controlled analgesia with 0.1% ropivacaine plus 0.5 microg/ml sufentanil. Anesthesiology 2004; 100: 968-72
12. Bremerich DH, Waibel HJ, Mierdl S, Meininger D, Byhahn C, Zwissler BC, Ackermann HH. Comparison of continuous background infusion plus demand dose and demand-only parturient-controlled epidural analgesia (PCEA) using ropivacaine combined with sufentanil for labor and delivery. Int J Obstet Anesth 2005; 14: 114-20
13. Halpern SH, Carvalho B. Patient-controlled epidural analgesia for labor. Anesth Analg 2009; 108: 921-8
14. Kaynar AM, Shankar KB. Epidural infusion: continuous or bolus? Anesth Analg 1999; 89: 534
15. Hogan Q. Epidural catheter tip position and distribution of injectate evaluated by computed tomography. Anesthesiology 1999; 90: 964-70
16. Wong CA, Ratliff JT, Sullivan JT, Scavone BM, Toledo P, McCarthy RJ. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth Analg 2006; 102: 904-9
17. Chua SM, Sia AT. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labour. Can J Anaesth 2004; 51: 581-5
18. Lim Y, Sia AT, Ocampo C. Automated regular boluses for epidural analgesia: a comparison with continuous infusion. Int J Obstet Anesth 2005; 14: 305-9
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
40

Session 3: Labour Analgesia Optimizing your labour epidural - from insertion to delivery / clinical pearls Professor Peter Pan Professor & Director of Anesthesia Clinical Research, Wake Forest University School of Medicine, Winston-Salem, USA
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
41

(Airway Examinations – Anesthesiology 2008; 108:357-62)
• Acoustic Reflectometry (n=21)
2.70
P<0.05
21.80
P<0.001
6.0644.40
P<0.05
Post Labor
3.1026.875.8449.10PreLabor
Pharyngeal
Area (cm2)
Pharyngeal
Volume
(mL)
Oral
Area
(cm2)
Oral
Volume
(mL)Pre vs Post Labor
(Airway Examinations – Anesthesiology 2008; 108:357-62)
Airway Lessons to Clinical Practice
• Airways can change significantly during L/D.
• Airway incr 1 or more grades in 38% of parturients during
labor
• Co-inside with sig. Oral/Pharyngeal volumes decreases.
• A careful re-evaluation of airway prior to administration
of analgesia & anesthesia during labor course is essential
rather than relying on preop/prelabor exam.
Preparation - Parturients with thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� ASRA concensus guidelines
� Heparin SQ
� Systemic therapeutic Heparin
� LMWH – QD, BID, high dose
� Antiplatelet agents:
� ASA, NSAID
� Thienopyridine derivatives (ticlopidine(Ticlid),
clopidogrel(Plavix))
� Platelet GP IIb/IIIa antagonists (abciximab, epitfibatide,
tirofiban)
Preparation - Parturients with SQ Heparin thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� Hep SQ small dose 5000U SQ
� Typically not prolong aPTT or monitored
� 15% subset with measurable aPTT changes
� 2-4% subset assoc decr PLT with > 5 days Hep
� Non-linear (disproportionately) Dose dependent increase in effect
� Wide spread use and paucity of complications suggest safety with low dose SQ and neuraxial anesthesia
� Clinical judgement or monitoring may be required in higher doses or unique clincial situations
Preparation - Parturients with systemic Heparin thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� Systemic Therapeutic Heparin (1.5-2X baseline aPTT)
� Vandermeulen et al series – ½ spinal ½ spinal ½ spinal ½ spinal hematomashematomashematomashematomas at time of indwelling at time of indwelling at time of indwelling at time of indwelling
cathcathcathcath removal in presence of systemic removal in presence of systemic removal in presence of systemic removal in presence of systemic heparinizationheparinizationheparinizationheparinization
� Risk factors: Traumatic, other anticoag, Hep <1 hr after needle puncture
� Recommendation:
� Stop Heparin 4hrs and check aPTT prior to needle placement
� Delay Hep admin for 1-2 hours after needle placement
� Wait 2-4hrs after last heparin dose before catheter removal� + Check aPTT
� Delay Hep restart for 1-2 hrs after catheter removal
� Monitor patients for signs/symptoms after procedure/removal of catheter.
Preparation - Parturients with LMWH thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� LMWH – QD, BID, (high dose)
� 40mg QD; 30 mg q12h; (enoxaparin 1mg/kg q12h, dalteparin 120U/kg q12h; tinzaparin 175U/kg daily)
� Recommendation:� Wait 12h12h12h12h after last QD dose prior to needle placement
� Wait 24h24h24h24h after BID/higher dose prior to needle placement
� QD dose initiation 6-8 hr postop after needle placement
� BID/high dose initiation delay 24hrs after needle placement
� BID/high dose NOT recommend with indwelling catheter
� Wait 12h(QDdose) or 24h(BID) after last dose prior to catheter removal
� First dose administer Wait 2+ hours after catheter removal and 6-8h postop(QDdose) and 24h postop (if BID or high dose)
Preparation - Parturients with antiplatelet thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� ASA affects platelet lifetime
� NSAID affects platelet 3-4 days� (Collaborative Low Dose Aspirin Study in pregnancy – Lancet 1994; 343:619-29 – 1422 high risk
OB 60mg ASA daily, 0 neuro complic)
� (Risk assessment of hermorrhagic complication associated with NSAID and epidural steriod
injection. Anesth Analg 2002;95:1691-7. )
� CLASP study & paucity of case reports
given prevalence of ASA and NSAID use
suggest safety of neuraxial analgesia in
presence of low dose ASA/NSAID.
Preparation - Parturients with antiplatelet thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� Thienopyridine derivatives: (plavix, Ticlid)
� RECOMMENDATION
� Discontinue Time from last dose prior to neuraxial block
� Clopidogrel(Plavix) – Discontinue 7 days prior
� Ticlopidine(Ticlid) - Discontinue 14 days prior
� (Based on labeling and surgical review, no series involve performance of neuraxial block in presence of thienopyridine
derivatives or plt GP IIb/IIa antagonists)
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
42

Preparation - Parturients with antiplatelet thromboprophylaxis
RAPM 2003; 28:172-97. Anesth Analg 2005; 100:1482-8.
� Platelet GP IIb/IIIa antagonists (abciximab,
epitfibatide, tirofiban)
� RECOMMENDATION
� Discontinue Time from last dose prior to neuraxial block
� abciximab Discontinue 24-48 hrs prior
� Epitifibatide, tirofiban Discontinue 8hrs prior
� (Based on labeling and surgical review, no series involve performance of neuraxial block in presence of
thienopyridine derivatives or plt GP IIb/IIa antagonists. Time to normal platelet aggregation is 24-48hrs after
abciximab and 4-8 hrs after epitifibatide or tirofiban. But GP IIb/IIIa antagonists are contraindicated within 4
weeks after surgery)
Preparation - Parturients with thrombocytopenia
Anesth Analg 1997; 85:385-8
� Preg assoc incr in many clotting factors
� Hypercoagulable state suggested
� Beilin retrospective review 15,919 parturients
� 30 pts reported PLT 69-98K at time of epid placement without sequelae.
� But should be interpreted cautiously as coag involves more than plt #.
� Etiology of low plt is multifactorial, the number, the function, baseline value, extent and rapidity of their fall, as well as other clinical indicators and evaluation are essential to be interpreted together.
� Use of low conc LA allowing frequent assess M/S ability and postopfollow up are important to minimize adverse outcome.
http://www.rit.edu/~andpph/photofile-c/sneeze-k-17.jpg
Preparation – Sterile Technique
• Broad practice patterns
• Patient safety
• Medico-legal implications
Droplet Theory!
Recommendation Grade and
(Level of Evidence)
Sterile Technique Practice for
Neuraxial Analg/Anesth
A (Ia or Ib )*Alcohol based Chlorhexidine*NOT FDA approved for lumbar puncture
A (Ia or Ib)Sterile Gloves
A (Ia or Ib)Hand Wash with antiseptic
RAPM 2006; 31:311-323
Recommendation Grade
and (Level of Evidence)
Sterile Technique Practice for
Neuraxial Analg/Anesth
B (IIa or IIb or III)Surgical Masks
A (Ia or Ib )*Alcohol based Chlorhexidine*NOT FDA approved for lumbar puncture
A (Ia or Ib)Sterile Gloves
B (IIa or IIb or III)Jewelry Removal
A (Ia or Ib)Hand Wash with antiseptic
RAPM 2006; 31:311-323
Inadequate DataSurgical Sterile Gown
UnknownDuration/Method Handwash
Recommendation Grade and
(Level of Evidence)
Sterile Technique Practice for
Neuraxial Analg/Anesth
B (IIa or IIb or III)Surgical Masks
A (Ia or Ib )*Alcohol based Chlorhexidine*NOT FDA approved for lumbar puncture
B (IIa or IIb or III)Bacterial Filter in short term epidural
- Not Necessary
A (Ia or Ib)Sterile Gloves
B (IIa or IIb or III)Jewelry Removal
A (Ia or Ib)Hand Wash with antiseptic
RAPM 2006; 31:311-323
Is your Epidural Optimized?(From Literature to Clinical Practice)
• Preparation
• Procedure
– Needle Bevel Orientation
– Positioning – sitting vs lateral
– Air vs Saline
– Amount of Saline
• Bevel cephalad vs lateral and caudal when cath inserted
• Single orifice catheter inserted 3 cm
• Dose with total 13 mL 0.25% bupivacaine over 10mins (test on left, turn right, then turn left)
26252*One sided block (%)
23272*Asymmetric >3 level (%)
111216*Total Segment blocked
(median)
Caudal
n=42
L/R lateral
n=75
Cephalad
n=43
Procedure – Needle Bevel OrientationFrom Literature to Clinical Practice – Anesth Analg 1998;87:326-30
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
43

Procedure – Lateral vs Sitting PositioningFrom Literature to Clinical Practice
• Patient Comfort/Preference
• Vagal or Orthostatic Response
• Aortocaval Compression / CO
• Epidural Venous Puncture
• Distance/Movement to Epidural Space
Procedure – Lateral vs Sitting PositioningFrom Literature to Clinical Practice
4.4+/-0.8*cm5.0+/-1.1* cmDistance to Epid Space (cm)(J Clin Anesth 1996;8:84-6) (1916 sitting, 207 lateral, non randomize)
0.67+/-.42(<25BMI);0.75+/-0.42 (25-30BMI)
. 1.04+/-0.68 (>30BMI) (Range -.11 to +4.28)
Cath move (cm) flex-sitting to lat (Anesthesiology 1997;86:778-84) ( 255pts, 46(BMI<25),116(25-30BMI),92(>30BMI)
10.7%*13.3%>1 attempt
6%(lat),2%*(lat Tburg)
7-8% > 1 attempt
Epidural Venous Puncture(Can J Anesth 2001;48:48-53) (900pts randomized - sit, lat, lat Tburg)
(Eur J Anaesth 2005;22:103-6) (209 pts – vein puncture 15.7% sit vs 3.7% lat)
Less (-10%)Greater (-30%)Aortocaval Compression – COTEB(Can J Anesth 1993; 40:320-4) (40pts randomized sitting vs lateral)
20%0%Vagal or orthostatic syncope (J Cardiothorac Vasc Anesth 2007) (40pts randomized sitting vs lateral)
BMI > 30BMI < 25 Patient Comfort (IJOA 1991;9-11) (300pts - 3 BMI gps)
SittingLateral
Procedure – Air vs Saline LORTFrom Literature to Clinical Practice
• Incomplete Analgesia
• PDPH
• Nerve Root Compression
• CSE – Air vs Saline LORT
Procedure – Air vs Saline LORT From Literature to Clinical Practice
NO differences (Spinal Analg, Epid Cath
replaced, Epid Drug Consumed
& Supplement Dose)
CSE spinal success & subsequent epid analg(Anesthesiology 2009; In press) (360pts RCT, 3mL Air/NS prior spinal needle, measure spinal/epid success)
Minimal More Nerve Root Compression Cases reported(usually assoc large air volumes) (RAPM 2003;28:48-53)
2.7% DP
10% HA
2.6% DP
67% HA
DP and PDPH (Anesthesiology 1998;88:76-81) 1812 RCT 4-5mL Air/NS; DP same; PDPH 2/3(air) vs 1/10(NS) of DP
(Anaesthesia 1990; 45:1077-9) retrospective 3400 epidural, DP 0.6% (NS) vs 1% (air) (P<.01)
19%36%Incomplete Analgesia (% request suppl analg)(RAPM 2000;25:596-9) (n=160, RCT, 2mL air/NS LOR,13mL bup, % suppl analg, added dose same success)
SalineAir
Procedure – Amount of SalineFrom Literature to Clinical Practice
2% (10mL) vs 20% (0mL) in IV cath0 vs 10mL NS(Can J Anesth 2003;50:382-5) (100pts,
RCT, 2gps,CSE, multiport cath 3-5cm)
15-19(10mL) vs 12-15(2mL) dermatomes block to pinprick
& cold; No diff (Pain relief, IV, paresthesia & DP)
2 vs 10mL NS(JCA 2006;18:575-9)
(105pts, RCT 2gps)
15 (10mL) vs 12 (1mL) spinal segments block to cold
in 1% mepiv gp. No diff in all others
1, 5 & 10mL NS(Can J Anaesth 1999;46:930-4)
(152pts, RCT, 2X3gps, 10mL of 1% or
1.5% mepiv; 1, 5, 10mL gps )
No diff in block to cold ; LESS pinprick block -16
dermatomes(10mL) vs 22(1 mL); suggest diluted LA
1, 5 & 10mL NS(Can J Anaesth 1998;45:1091-3) (70
pts, RCT, epid 3 gps, 12mL 1% mepiv )
No Diff in IV cath, paresthesia & DP; Air gp more
initial incomplete block, improve with suppl dose2mL air vs NS(RAPM 2000; 25:596-9)
Is your Epidural Optimized?
(From Literature to Clinical Practice)
• Procedure
– Needle Bevel Orientation
– Patient Positioning
– Air vs Saline
– Effect of Epidural Saline
• Optimize Analgesia
–Initial Dosing after placement
– Incomplete Analgesia Management
• Post Neuraxial Analgesia
Procedure – Optimize Initial DosingFrom Literature to Clinical Practice – RAPM 1998;23:134-41.
• 58 primiparae, active
labor, < 5cm dilated
• RCT, 3 groups
• After test dose 3mL
2% lido with 200ug
epi
• Randomize to receive
20mg epidural bupiv
using 1 of 3 solutions
20mL 0.1% 20mL 0.1% 20mL 0.1% 20mL 0.1% bupivbupivbupivbupivGpGpGpGp 0.1%0.1%0.1%0.1%
n = 20n = 20n = 20n = 20
10mL 0.2% 10mL 0.2% 10mL 0.2% 10mL 0.2% bupivbupivbupivbupivGpGpGpGp 0.2%0.2%0.2%0.2%
n = 19n = 19n = 19n = 19
4mL 0.5% 4mL 0.5% 4mL 0.5% 4mL 0.5% bupivbupivbupivbupivGpGpGpGp 0.5%0.5%0.5%0.5%
n = 19n = 19n = 19n = 19
Procedure – Optimize Initial DosingFrom Literature to Clinical Practice – RAPM 1998;23:134-41.
20 (100%)
18 (95%)
8 (42%)
50% Pain
Relief
15 (75%)
11 (58%)
1 ( 5%)
Complete
Pain Relief
0.1% - 20mL(n=20)
0.2% - 10mL(n=19)
0.5% - 4mL(n=19)
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
44

Procedure – Optimize Initial DosingFrom Literature to Clinical Practice – RAPM 1998;23:134-41.
18
17
9
Dermatome
Blocked
Analgesic
Duration (min)
120+/-210.1% - 20mL(n=20)
100+/-260.2% - 10mL(n=19)
43+/-210.5% - 4mL(n=19)
Procedure – Optimize Initial Dosing
AnalgesiaFrom Literature to Clinical Practice – RAPM 1998;23:134-41.
20 (100%)
18 (95%)
8 (42%)
50% Pain
Relief
15 (75%)
11 (58%)
1 ( 5%)
Complete
Pain Relief
18
17
9
Dermatome
Blocked
Analgesic
Duration (min)
120+/-210.1% - 20mL(n=20)
100+/-260.2% - 10mL(n=19)
43+/-210.5% - 4mL(n=19)
• Suggest # dermatomes blocked and analgesia is
associated with epidural volume first and then drug
conc second with same amount of drug(mg)
Is your Epidural Optimized?
(From Literature to Clinical Practice)
• Optimize Analgesia
– Dosing Initial Dosing
–Incomplete Analgesia Management
• Post Neuraxial Analgesia
Procedure – Optimize Incomplete AnalgesiaFrom Literature to Clinical Practice – Anesthesiology 1998; 88:1502-6
• About 15% still have pain (Some blocks but Incomplete
Analgesia) after initial epidural placement & LA administration
• Should we
– just top up with additional LA ?
– Or pull catheter back 1 cm, then dose with LA?
– Or Replace catheter ?
Procedure – Optimize Incomplete AnalgesiaFrom Literature to Clinical Practice – Anesthesiology 1998; 88:1502-6
• 696 epidurals, multiorifice cath
• 5 cm inside epid space
• Dosed with (3+5+5) = 13mL .25% Bupivacaine
• 78 (12.2%) Incomplete Analgesia after 13mL LA
• All dosed on lateral decubitus position with hurting side down
(dependent)
Procedure – Optimize Incomplete AnalgesiaFrom Literature to Clinical Practice – Anesthesiology 1998; 88:1502-6
• Incomplete Analgesia (78 pts) randomized to:
• 1st Intervention:
– (1) Additional .25% bupiv 5 mL
– (2) Pull catheter back 1 cm, then admin same LA
• If 1st intervention not successful, 2nd intervention is reversed
• All dosed on lateral decubitus position with hurting side down
(dependent)
Procedure – Optimize Incomplete AnalgesiaFrom Literature to Clinical Practice – Anesthesiology 1998; 88:1502-6
R side 30
L side 9
R side 33
L side 6
Incomplete Analgesia
after initial 13mL dose
Pull Cath + LA
n = 39
Local Anesth Only
n = 39
Procedure – Optimize Incomplete AnalgesiaFrom Literature to Clinical Practice – Anesthesiology 1998; 88:1502-6
R side 30
L side 9
R side 33
L side 6
Incomplete Analgesia
after initial dose
(77%)(74%)Success after 1st
intervention
Pull Cath + LA
n = 39
Local Anesth Only
n = 39
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
45

Procedure – Optimize Incomplete AnalgesiaFrom Literature to Clinical Practice – Anesthesiology 1998; 88:1502-6
R side 30
L side 9
R side 33
L side 6
Incomplete Analgesia
after initial dose
(100%)(100%)Success after 2nd
(reverse) intervention
(77%)(74%)Success after 1st
intervention
Pull Cath + LA
n = 39
Local Anesth Only
n = 39
Procedure – Optimize Post Analg/AnesthFrom Literature to Clinical Practice – Anesthesiology 2007;106:1096-104
A Series of Anesthesia-related Maternal Deaths in Michigan, 1985-2003
• Pregnancy Associated Deaths 1985Pregnancy Associated Deaths 1985Pregnancy Associated Deaths 1985Pregnancy Associated Deaths 1985----2003 in Michigan2003 in Michigan2003 in Michigan2003 in Michigan
• Using MMMS and matched MDCH data with electronic linked Using MMMS and matched MDCH data with electronic linked Using MMMS and matched MDCH data with electronic linked Using MMMS and matched MDCH data with electronic linked
matched death certificatesmatched death certificatesmatched death certificatesmatched death certificates
• Of 855 pregnancyOf 855 pregnancyOf 855 pregnancyOf 855 pregnancy----associated death, 25 cases associated associated death, 25 cases associated associated death, 25 cases associated associated death, 25 cases associated
with perioperative arrest/with perioperative arrest/with perioperative arrest/with perioperative arrest/anesthanesthanesthanesth complication reviewedcomplication reviewedcomplication reviewedcomplication reviewed
• 8 were anesthesia8 were anesthesia8 were anesthesia8 were anesthesia----related and 7 were anesthesiarelated and 7 were anesthesiarelated and 7 were anesthesiarelated and 7 were anesthesia----
contributing; Of the 8 anesthesiacontributing; Of the 8 anesthesiacontributing; Of the 8 anesthesiacontributing; Of the 8 anesthesia----related deaths, 4 had related deaths, 4 had related deaths, 4 had related deaths, 4 had
neuraxialneuraxialneuraxialneuraxial blockadeblockadeblockadeblockade
Procedure – Optimize Post Analg/AnesthFrom Literature to Clinical Practice – Anesthesiology 2007;106:1096-104
A Series of Anesthesia-related Maternal Deaths in Michigan, 1985-2003
Breech C/S->Spinal->Brady->CP Arrest 17min after Spinal-
>Resuscitated->GA ETT->Intubated to ICU-> unplanned ICU
extubation-> Anoxic encephalopathy
4.
RepeatC/S->Epidural->HighSpinal after test dose->CP Arrest ->
>Resuscitated-> GA->Extubate in OR ->Transfer to PACU->2nd
CPArrest ->Failed resuscitate
3.
Urgent C/S(BP/LFT)->spinal/postop PCA->AW Obstruct 9hr
postop in pt room->apneic/pusless->Failed resuscitation
2.
Elect Repeat C/S->Spinal->Hypovent/AW Obstruct->apneic,
brady on PACU arrival �CP arrest-> Failed resuscitation
1.
�4 anesth-related death had neuraxial block :
Procedure – Optimize Post Analg/AnesthFrom Literature to Clinical Practice – Anesthesiology 2007;106:1096-104
A Series of Anesthesia-related Maternal Deaths in Michigan, 1985-2003
• Three Key Lessons:
– All anesth-related deaths from airway obstruction/hypovent
during emergence or recovery period and NOT induction
– Lapses in postoperative monitoring and inadequate
supervision contributed to 5/8 of anesth-related death
– Obesity and African-American race are important risk
factors.
Preparation
Airway can change over labor course
Thromboprophylaxis & Thrombocytopenia
Procedure
Sterile Technique – update with ASRA guidelines
Cephalad Needle Bevel Orientation
Positioning – sitting vs lateral
Saline may be more preferred
Dosing
Volume over Concentration
Volume first, adjust cath next
Post analgesia
Airway Obstruction, vigilance, monitor, risk factors
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
46

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 4: New Developments Tracheal intubation – what’s new? Dr Anil Patel Consultant Anaesthetist, Royal National Throat, Nose & Ear Hospital, London
The standard Macintosh laryngoscope and direct laryngoscopy remains the main technique for visualisation of the laryngeal inlet and the passage of a tracheal tube for the majority of anaesthetists in the UK. When problems with direct laryngoscopy are anticipated or encountered different types of laryngoscope have been tried to improve the view of the laryngeal inlet. These have included laryngoscopes utilising a paraglossal straight laryngoscopy technique (Miller, Belscope, Choi, and Henderson). More recently devices which allow indirect visualisation of the laryngeal inlet on a screen or eyepiece have been introduced in an attempt to improve the rate and speed of tracheal intubation, whilst minimising trauma to laryngo-pharyngeal tissues. Most of these devices are designed for patients in which conventional standard Macintosh laryngoscopy has proven to be or is expected to be difficult. These new devices can be grouped into those that employ a rigid stylet onto which a tracheal tube is loaded. The tip of the stylet contains a camera or fibreoptic technology that allows visualisation of the tip through an eyepiece or screen. These devices include the Bonfils Intubation Fibrescope, Shikani Optical Stylet and Levitan Stylet. Some of these rigid ‘visualised stylets’ allow the tip to be bent to optimise laryngeal entry whilst others are fixed. The second group include the Glidescope and McGrath laryngoscopes. These allow visualisation of ‘anterior’ structures in which conventional laryngoscopy would reveal a view of the tip of the epiglottis at best. These devices convert a difficult direct view to a better indirect view on a screen. Tracheal intubation can now be seen although the increased angle that the tube has to pass often requires the presence of a stylet or bougie to angle the tube in the correct direction. The third group include the Airtrac and Pentax AWS airway scope. These devices have channels along their lateral border that allow a tube to pass along and guide the tube to the distal end of the device. This results in the tube emerging near the laryngeal inlet
without the need for stylets or bougies. Both of these devices look, handle and are inserted in the mouth in a different manner to a standard laryngoscope. The fourth group (Storz CMAC) handle and function in an identical manner to standard Macintosh laryngoscopes but have cameras incorporated into the laryngoscope blade. This allows visualisation of the laryngeal inlet and may aid or confirm tracheal intubation. These devices are also useful in teaching standard laryngoscopy.
47

Session 4: New Developments Acute to chronic pain after delivery: from predictors to spinal oxytocin Professor Peter Pan Professor & Director of Anesthesia Clinical Research, Wake Forest University School of Medicine, Winston-Salem, USA
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
48

• So it would be important to be able to So it would be important to be able to So it would be important to be able to So it would be important to be able to
predict and identify those at risks for predict and identify those at risks for predict and identify those at risks for predict and identify those at risks for
severe painsevere painsevere painsevere pain
• Thereby, we can allocate resources, tailor Thereby, we can allocate resources, tailor Thereby, we can allocate resources, tailor Thereby, we can allocate resources, tailor
analgesic treatment or trials, and hopefullyanalgesic treatment or trials, and hopefullyanalgesic treatment or trials, and hopefullyanalgesic treatment or trials, and hopefully
prevent development of chronic pain.
PostOperative Pain• Multiple FactorsMultiple FactorsMultiple FactorsMultiple Factors: Physiological, Psychological, : Physiological, Psychological, : Physiological, Psychological, : Physiological, Psychological,
Sensory, Affective, cognitive, socioSensory, Affective, cognitive, socioSensory, Affective, cognitive, socioSensory, Affective, cognitive, socio----cultural, cultural, cultural, cultural,
age and gender.age and gender.age and gender.age and gender.
• High High High High interpatientinterpatientinterpatientinterpatient variabilityvariabilityvariabilityvariability in in in in postoppostoppostoppostop pain and pain and pain and pain and
analgesic needanalgesic needanalgesic needanalgesic need
• High % hosp pts mod to severe High % hosp pts mod to severe High % hosp pts mod to severe High % hosp pts mod to severe postoppostoppostoppostop painpainpainpain
• JCAHO JCAHO JCAHO JCAHO ---->3/10 rest and/or activity pain>3/10 rest and/or activity pain>3/10 rest and/or activity pain>3/10 rest and/or activity pain
• Severe Severe Severe Severe postoppostoppostoppostop pain may lead to Chronic painpain may lead to Chronic painpain may lead to Chronic painpain may lead to Chronic pain
Previous Studies for Predictors
• Granot: preop thermal suprathreshold
pain scores (not threshold) on the arm
correlated with postop pain. (r= 0.4-0.5)
• Hsu: preop pressure pain tolerance on the
arm correlated with postop pain (r=-0.5) and
pressure pain tolerance after fentanyl
predict analg consumed (r=-0.4)
Multifactorial Predictors
• Previous studies focused on individual predictive factor
have resulted in weak but signif correlation to postop pain.
• None in a comprehensive way to explore a multi-factorial
model to predict postop pain and analgesic need.
• Goal: Assess thermal pain threshold and supra-
threshold ; audio sensitivity, as well as a series of
psychological tests for anxiety, expectation and pre-
existing pain.
Preop Assessment
• STAI – State Trait and Anxiety Inventory
• Questionnaire:
– Preexisting Pain and Unpleasantness
– Anxiety Level
– Expectation of Pain and Analgesia Required
• A series Thermal Sensitivity Tests
• A series of Audio Sensitivity Tests
Factor analyses –> 7 Independent Predictive Factor Groups(Final principal components solution of predictor variables (with varimax rotation),
with reliability estimates)
• Thermal Pain and Unpleasantness – arm & back
• Thermal Pain Threshold – arm and back
• Blood Pressure – Preop BP
• Preexisting Pain – Pregnancy Pain &
Unpleasantness
• Expectation – Postop Pain & analg expected
• Intraoperative Factor –Surg dur & sensory block
at incision
• STAI
Resting Pain Standardized Predicted Value
ModelPain Outcomes Predictor Group b b t p F p R2 Adj. R2
Resting Pain 5.1 .01* .26 .21Thermal Pain & Unpleasant .07 .32 1.95 .06
Expectation 1.5 .35 2.2 .04*
Evoked Pain Standardized Predicted Value
ModelPain Outcomes Predictor Group b b t p F p R2 Adj. R2
Evoked Pain 7.7 .009** .20 .18Thermal Threshold (Back) -5.4 .45 2.8 .009**
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
49

Results – Multifactorial Pain Predictors
• Resting Pain: (R2=.26, p<.01)
– Thermal Pain & Unpleasantness
– Expectation
• Evoked Pain: (R2=.20, p<.009)
– Back Thermal Pain Threshold
• Composite Pain Score: (R2=.28, p<.008)
– Thermal Pain & Unpleasantness
– PreOp BP
Simplified Pain Predictors Model
Simplified Pain Predictors Model
• Audio ToneAudio ToneAudio ToneAudio Tone
• AnxietyAnxietyAnxietyAnxiety
• Pain ExpectationPain ExpectationPain ExpectationPain Expectation
Simplified Pain Predictors Model
Informed Demographics
Consent Anticipated Pain
Anxiety
Audio Testing
Preoperative Anesthetic Consultation PACU 24 Hours Postop
PACU
Narcotic
Usage
24 Hour Assess:
Resting Pain
Evoked Pain
Satisfaction
Narcotic Usage
Elective
Cesarean
Section
Prelim Results – Simplified Pain Predictorsusing Anxiety, Anticipated Pain and Audio Sensitivity
• Resting Pain: (R=.33, p<.005)
• Evoked Pain: (R=.41, p<.001)
• PACU Narcotic: (R=.39, p<.001)
• 24hr PostOp Narcotic: (R=.41, p<.001)
Prelim Results – Pain Predictorsusing Anxiety, Anticipated Pain and Audio Sensitivity
• Simple, readily obtainable preoperative indices can predict narcotic usage and pain scores
• Cut-off scores can identify patients at risk for inadequate pain control.
• Patients may benefit from individually tailored, multimodal pain management strategies
• Future step:– Test model with cut-off scores;
– Evaluate intervention strategies based on cut-off scores;
– Application of models to other surgery
�Does acute pain has long term implications?
Trauma and pain
Level of pain
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
50

Amputation CABG Breast Hernia C/S0
10
20
30
40
% w
ith
Ch
ron
ic P
ain
Kehlet, Lancet, 2006
What is the incidence of chronic pain after delivery?
Pain After Delivery
�Goal: Goal: Goal: Goal: PrevalancePrevalancePrevalancePrevalance of acute & chronic PAD; of acute & chronic PAD; of acute & chronic PAD; of acute & chronic PAD; PredictivePredictivePredictivePredictive
factorsfactorsfactorsfactors; ; ; ; Long termLong termLong termLong term implications.implications.implications.implications.
�Prospective, descriptive cohort longitudinal multiProspective, descriptive cohort longitudinal multiProspective, descriptive cohort longitudinal multiProspective, descriptive cohort longitudinal multi----
center study (4 international centers, 2350 patients)center study (4 international centers, 2350 patients)center study (4 international centers, 2350 patients)center study (4 international centers, 2350 patients)
� InterviewInterviewInterviewInterviewed in ed in ed in ed in hospital, F/U 2, 6, 12 monthshospital, F/U 2, 6, 12 monthshospital, F/U 2, 6, 12 monthshospital, F/U 2, 6, 12 months
� In HospitalIn HospitalIn HospitalIn Hospital: maternal/neonatal demographics and : maternal/neonatal demographics and : maternal/neonatal demographics and : maternal/neonatal demographics and
medical medical medical medical hxhxhxhx, pre, pre, pre, pre----existing pain, existing pain, existing pain, existing pain, somatizationsomatizationsomatizationsomatization, pain level, pain level, pain level, pain level
� F/UF/UF/UF/U: postpartum pain (freq, loc, intensity, : postpartum pain (freq, loc, intensity, : postpartum pain (freq, loc, intensity, : postpartum pain (freq, loc, intensity, txtxtxtx, daily , daily , daily , daily
activity impact), depression (Edinburgh Postnatal activity impact), depression (Edinburgh Postnatal activity impact), depression (Edinburgh Postnatal activity impact), depression (Edinburgh Postnatal
Scale); health changes.Scale); health changes.Scale); health changes.Scale); health changes.
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept
0
200
400
600
800
1000
1200
1400
1600
1800
2000
2200
2400
2005
Cu
mula
tive e
nro
llment
2004
Vaginal
CS
Chronic Pain Prevalence
0.3%0.0%0.45%Percent of patients
with pain @ 12 month
1.9%1.9%1.8%Percent of patients
with pain @ 6 month
9.8%9.2%10.1%Percent of patients
with pain @ 8 week
Combined
VD + C/S
Cesarean
Delivery
Vaginal
Delivery
Does acute pain has long term implications?
CesareanDelivery
Acute Pain
Score
DepressionScore
Odds ofPersist Pain
32.5% (4.0)*
4.4% (7.5)
-26.2% (32.1)
8.3% (0.2)*
12.7% (5.0)*
7.0% (3.0)*29.1% (7.5)*
Severity of acute pain after childbirth, but not type of delivery
predicts persistent pain and postpartum depression
Does acute pain has long term implications?
CesareanDelivery
Acute Pain
Score
DepressionScore
Odds ofPersist Pain
32.5% (4.0)*
4.4% (7.5)
-26.2% (32.1)
8.3% (0.2)*
12.7% (5.0)*
7.0% (3.0)*29.1% (7.5)*
Severity of acute pain after childbirth, but not type of delivery
predicts persistent pain and postpartum depression
After controlling for propensity to deliver via C/S, every point increase
in acute pain after delivery was associated with 8.3% increase in 8-wk
Depression score and a 12.7% increase in odds of experiencing
persistent pain at 8 wk. However pain at 1 yr remained very low.
Persistent pain is amazingly rare
TAH C/S0
1
2
3
4
5
6
% W
ith P
ain
at
1 Y
ea
r
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
51

But isn’t this strange since the system is setup for more pain?
Term pregnant
• IL1β• TNFα• NO
• PGE2
Why ???
• Why delivery and/or immediate post
delivery seem to provide protection from
development of pain hypersensitivity?
Previous Laboratory Findings
0 7 14 21 28 35 42 490
2
4
6
8
10
12
14
16
With
dra
wa
l T
hre
sh
old
(g
)
Days
Delivery Weaning
Separation
Pup interact
with mom
SNL = spinal nerve ligation
From Delivery
Remove pup
Pup interact
with mom
Remove pup
0 7 14 21 28 35 42 490
2
4
6
8
10
12
14
16
With
dra
wa
l T
hre
sh
old
(g
)
Days
Delivery Weaning
Separation
This study shows the effect of
delivery on Pre-Existing injury
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
52

Protection from neuropathic pain
immediately after delivery is permanent!
Pup removal
Surrogate Mom
(No Preg/Delivery)
+ Pup/Mom interact
MCN
Magnocellular Neurons
Parvocellular Neurons(PVN)
Posterior Pituitary
Peripheral Oxytocin
Central/spinal Oxytocin
PVN
Magnocellular neurons project to post pituitary then
peripheral oxytocin. Parvocellular neurons of PVN
project to non-pituitary and central/spinal oxytocin.
0 7 14 21 28 35 42 490
2
4
6
8
10
12
14
16
With
dra
wal T
hre
shold
(g
)Days
0 1 2 3 4 50
2
4
6
8
10
12
14
16
Withd
raw
al T
hre
shold
(g)
Time (hr)
Atosiban
Oxytocin
antagonist
Placebo
Vehicle
Atosiban – oxytocin antagonist
result in decrease withdrawal
threshold ->loss of protection
of pain hypersensitivity.
0 7 14 21 28 35 42 490
2
4
6
8
10
12
14
16
With
dra
wa
l T
hre
sh
old
(g)
Days
Delivery Weaning
Separation
0 7 14 21 28 35 42 490
2
4
6
8
10
12
14
16
With
dra
wa
l T
hre
sh
old
(g)
Days
Delivery Weaning
Separation
And oxytocin is protective in males
Central oxytocin infusion
oxytocin
vehicle
Protective Effect from Pain
Hypersensitivity Development
• Seems to associate with an increase in CSF
oxytocin (synthesized in parovcellular
neurons) but not peripheral oxytocin (from
magnocellular neurons).
• Central protective effect was inhibited by
intrathecal oxytocin antagonist
PVN
Magnocellular neurons
SON
Parvocellular neurons
Posterior Pituitary
Peripheral Oxytocin
Central/spinal Oxytocin
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
53

Level of pain
Injury
Sprouting
Excitability
Inflammation
Post-partum protection
? Spinal oxytocin
Predictor to OxytocinPredictor to OxytocinPredictor to OxytocinPredictor to Oxytocin
Thank You !!Thank You !!Thank You !!Thank You !!
Peter H. Pan, MSEE, MD
Predictor to OxytocinPredictor to OxytocinPredictor to OxytocinPredictor to Oxytocin
Peter H. Pan, MSEE, MDPeter H. Pan, MSEE, MDPeter H. Pan, MSEE, MDPeter H. Pan, MSEE, MD
Section on OB/GYN AnesthesiologySection on OB/GYN AnesthesiologySection on OB/GYN AnesthesiologySection on OB/GYN Anesthesiology
Wake Forest University School of MedicineWake Forest University School of MedicineWake Forest University School of MedicineWake Forest University School of Medicine
WinstonWinstonWinstonWinston----Salem, North CarolinaSalem, North CarolinaSalem, North CarolinaSalem, North Carolina
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
54

Session 5: Blood Issues Obstetric Haemorrhage- rFV11a, interventional radiology, cell salvage and beyond Felicity Plaat Consultant Anaesthetist, Queen Charlotte's & Hammersmith Hospitals, London
The need for effective therapies is indisputable. The World Health Organization estimates that >130 000 maternal deaths occur globally each year due to obstetric haemorrhage. A 1% case fatality rate suggests a yearly incidence of > 13 million cases. Thus obstetric haemorrhage represents the most common cause of severe maternal morbidity and long term sequelae world-wide [1, 2]. In the UK, the mortality rate per 100 000 maternities due to haemorrhage has not changed significantly over the past 15 years. Furthermore in the most recently published report ~60% cases were associated with substandard care, [3]. A review of the risk factors for haemorrhage suggest that both in Developed and Developing countries, the incidence is set to rise, with obesity and rise in cases of multiple section being of particular concern, [4] This lecture will review those aspects of management most relevant to anaesthesia, where there have been recent changes and where there is controversy. Intravenous resuscitation, transfusion and medical management of coagulopathy The crystalloid – colloid debate in immediate resuscitation continues. Crystalloids have the advantage of being cheap, readily available and associated with a lower incidence of anaphylactoid reactions. In vitro and animal studies show that colloids impair coagulation by interfering with fibrin polymerisation [5] Newer colloids such as hydroxyethylstarch HES130/0.4, (Voluven®) may have less effect [6] However all clear fluids lead to dilutional coagulopathy and large volumes of 0.9% saline should be avoided as they cause hyperchloraemic acidosis. The use of balanced solutions is advocated, [7] Many management protocols suggest the administration of 1500 ml clear fluid prior to transfusion. Given the problem of impaired coagulation, unless the situation appears to be rapidly self limiting, blood should be administered as soon as it is available. In animal models of uncontrolled haemorrhage, and in non-pregnant trauma patients, aggressive fluid administration seems to be associated with decreased survival. [8] Because of the reliance of the placental circulation on maternal venous return however, hypotensive resuscitation may only be appropriate in
the management of post-partum haemorrhage when definitive management is delayed. Transfusion of red blood cells is required when 30% or more of the circulation blood volume is lost to maintain oxygen delivery to the tissues. Current guidelines state that transfusion is rarely necessary when the haemoglobin concentration is > 10g/dL but almost always required at concentration at or below 6g/dL. [9] Due to the torrential nature of obstetric blood loss and increased oxygen requirements during pregnancy and labour, it would seem prudent to aim towards the upper end of this spectrum. Traditionally the use of blood products was dependant on the result of laboratory tests and if these were unavailable, empiric regimes such FFP to be given after a fixed number packed red cells, were widely advocated. Such formula based approaches have not been shown to improve outcome. [9] Recently such management has been challenged and experience gleaned from the management of military casualties, suggest that red cells and clotting factors should be given in roughly similar proportions especially early in resuscitation [10] In practice this is next to impossible to achieve as FFP has to be stored at -30°C and thawed to 37°C – a process that takes at least 30 minutes. Nevertheless in the UK, many units are now recommending such policies, (Personal communication). A possible adverse consequence may be an increase in transfusion related complications, such transfusion related acute lung injury (TRALI), which is 5-6 times more common after blood products than red cell transfusion. The latest report on transfusion related complications in the UK, includes 1 probable and one possible case of TRALI in obstetric patients [11] FFP contains variable amounts of fibrinogen, and is too dilute to increase levels enough to be effective without risking fluid overload. Cryoprecipitate is more concentrated – containing 150-250 mg fibrinogen per 10 ml in addition to the other vitamin K dependant clotting factors. However cryoprecipitate is unavailable in the pathogen inactivated form. Recent studies suggest that fibrinogen concentrate and prothrombin complex concentrates may be used to reduce the need or as substitutes, [12. 13,]
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
55

Cut-down methods have been advocated for patients with difficult intravenous access, [14] Recently there has been a renewed interest in utilising the interosseous route and several new systems have been developed. The use of bedside investigations including thromboelastography will be discussed. Use of rFV11a in obstetrics Although rFV11a is still only licensed for use in haemophilia patients and for some platelet dysfunction disorders, its use in obstetrics is becoming widespread. Although often used as ‘last ditch’ therapy, there is growing evidence that used earlier, it may reduce the need for subsequent transfusion and or intervention, [15] There is currently a multicentre randomised controlled study underway to elucidate the role of rFV11a [16] The safety of rFV11a has not been established. In placebo controlled studies in non-pregnant patients, the risk of thrombosis is not increased, although thrombotic complications in an obstetric patient has recently been described [17] Hypothermia, acidosis and depletion of fibrinogen and platelets should be corrected to maximize the efficacy of rFV11a [18] Cell Salvage in obstetrics In the UK, the use of cell salvage in obstetrics was pioneered by Dr Catling in Swansea. To date there have been over 200 cases across Wales, in which cell salvage has been used. [S. Catling – Personal Communication] However blood was only re-transfused in less than ¼ of these cases, in contrast to the 80% re-transfusion rate for other specialties. The difficulty in predicting when haemorrhage will occur, lack of familiarity with equipment have been cited as impediments to its use, [19,20] A intensive period of training seems to overcome some of these problems, [21] Serious consequences of amniotic fluid contamination and rhesus immunisation have not been reported. The use of a leucocyte depletion filter has been shown reduce the presence of squame cells and AFP to close to zero, even when a separate suction system for amniotic fluid was not used, [22] In the current report on transfusion related injuries, there was one case of air embolism and 4 cases of hypotension associated with cell salvage [11]. Interventional radiology There have been several studies on the use of prophylactic interventional radiology for delivery when placenta accrete had been antenatally diagnosed. 3 studies showed a benefit but later ones showed little or no benefit. [23]
Although there is more evidence for the use of emergency procedures, practical considerations, including the need to transport haemodynamically compromised patients between maternity and radiology suites, restricts its use to a few patients in a few centres in the UK. References
1. Khan KS, Wojdyla D, Say L et al. WHO analysis of causes of maternal death; a systemic review. Lancet 2006; 367: 1066-74
2. AbouZahr C. Global burden of maternal death and disability. British Medical Bulletin 2003; 67: 1-11
3. Confidential Enquiry into Maternal & Child Health: Saving Mothers’ Lives 2003-2005. London 2007
4. Knight M, Kurinczuk JJ, Spark P, et al. Cesareandelivery and peripartum hysterectomy. O&G 2008; 111:97-105
5. Innerhofer P, Fries D, Margreiter J et al. The effects of per-operatively administered colloids and crystalloids on primary platelet-mediated hemostasis and clot formation. Anesth Analg 2002; 95: 858-65.
6. Langeron O, Doelberg M, Ang ET et al. Voluven® a lower substituted novel hydroxethyl starch (HES130/0.4), causes fewer effects on coagulation in major orthopaedic surgery than HES200/0.5. Anesth Analg 2001; 92: 855-62
7. Boldt J. The balanced concept of fluid resuscitation. Br J Anaesth 2007; 99: 312-15
8. Dutton RP, MacKenzie CF, Scalea TM. Hypotensive resuscitation during active haemorrhage: impact on in-hospital mortality. J Trauma 2002; 52: 1141-46
9. Stainsby D, Maclennan S, Thomas D et al. Guidelines in the management of major blood loss. British Committee for Standards in Haematology 2006
10. Holcombe JB, Jenkins D, Rhee P et al. Damage control resuscitation: Directly addressing the early Coagulopathy of trauma. The Journal of trauma, Injury, Infection and critical care 2007: 62:307-10
11. www.shot.org 12. Fries D, Haas T, Klingler A et al. Efficacy of
fibrinogen and prothrombin complex concentrate used to reverse dilutional coagulopathy – a porcine model. Br J Anaesth 2006; 97: 460-67
13. Fenger-Eriksen C, Lindberg-Larsen M, Christensen AQ, eta al. Fibrinogen concentrate substitution therapy in patients with massive haemorrhage and low plasma fibrinogen concentrations. Br J Anaesth 2008; 101: 769-73
14. Johanson R, Cox C, Grady K ey al. Managing obstetric emergencies and trauma: the MOET course manual. London RCOG Press 2003
15. Ahonen, Jokela R. Recombinant factor v11a for life-threatening post-partum haemorrhage. Br J Anaesth 2005; 94: 592-95
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
56

16. Recombinant human activated factor V11 as salvage therapy in women with severe post partum haemorrhage. www.clinicaltrial.gov
17. Van Veen EJW, Monteban-Kooistra WE, Meertens JHJM et al. Recombinant human activated factor V11 in postpartum haemorrhagic shock: the dark side. Intensive Care Med 2008; 34:211-12
18. McMorrow RCN, Ryan SM, Blunnie WP et al. Use of recombinant factor V11a in massive post-partum haemorrhage. Eur J Anesthesiol 2008; 25: 293-98
19. Harkness M, Clark V. The use of Cell salvage during obstetric procedures: an audit od Scotland’s maternity units. Scotish Med J 2008; 53: 24-27
20. Teig M, Harkness M, Catling S, Clark V. Survey of Cell salvage in obstetrics in the UK. Int J Obstet Anesth 2007; 16: S30
21. King M, Wrench I, Galimberti A, Spray R. Introduction of cell salvage to a large obstetric unit: the first 6 months. Int J Obstet Anesth 2009; 18: 111-17
22. Sullivan I, Faulds J, Ralph C. Contamination of salvaged maternal blood by amniotic fluid and fetal red cells during elective Caesarean section. Br J Anaesth 2008; 101:225-29
23. Levine AB, Kuhlman K, Bonn J. Placenta accrete: comparison of cases managed with and without pelvic artery balloon catheters. J Matern fetal Med 1999; 8: 173-76
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
57

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 5: Blood Issues Thromboprophylaxis, heparins and regional anaesthesia Professor Beverley J Hunt Professor of Thrombosis & Haemostasis, Guy's & St Thomas' Hospitals, London
Despite the increasing use of thromboprophylaxis, venous thromboembolism remains the number one medical cause of maternal death.
In response to this, the RCOG have revised their Green top guidelines again and the new version will increase the use of thromboprophylaxis further. One of the concerns is the increasing rate of obesity, which is epidemiologically a significant risk factor for VTE inside and outside pregnancy. In response the RCOG guidelines are advising routine thromboprophylaxis for women with a BMI >40 during antenatal admission and post delivery. Therefore there will be increasing numbers of patients on thromboprophylaxis prior to delivery: a challenge to the obstetric anaesthetists.
Despite a large number of new oral anticoagulants in clinical trial and some already licensed for use for thromboprophylaxis after hip and knee replacement, sadly these exciting new drugs will not impact on
pregnancy due to concerns about teratogenecity. Thus low molecular weight heparin (LMWH) will remain the main thromboprophylactic and treatment agent in pregnancy for the foreseeable future. Occasional use of fondaparinux and warfarin will continue in those with heparin allergy.
The insertion of epidural and spinal anaesthesia in mothers receiving LMWH is a subject that has not been formally studied. Observational studies suggest that having a thromboprophylactic dose LMWH 8-12 hours pre insertion, along with a normal coagulation screen and adequate platelets is acceptable practice. Treatment dose LMWH required 24 hours cessation before insertion.
Fondaparinux has a longer half- life than LMWH and the American College of Chest Physicians recommend it is not used with regional anaesthesia til more data is acquired.
58

Session 5: Blood Issues Use of the coagulation laboratory and point of patient testing in thrombosis & bleeding Dr Wiebke Gogarten Consultant Anaesthetist & Head, Department of Anaesthesiology, Intensive Care and Pain Medicine, Harlaching Hospital, Municipal Hospitals of Munich, Germany
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
59

Multiplate Electrode Aggregometry Multiplate to monitor platelet function and the risk of bleeding?
Rahe-Meyer et al., Anesth Analg 2008; 107: 1791-1797
Abnormal platelet aggregation required more platelet transfusions1.1 ± 1.2 U versus 0.3 ± 0.8 units*
Aspirin Resistance: Comparison of Different Methods
Lordkipanidze et al., Eur Heart J 2007; 28: 1702-1708
In patients who are receiving antiplatelet drugs, we suggest against the routine use of platelet function assays to monitor the antithrombotic effect of aspirin or clopidogrel.
Rationale: The clinical significance of the assay result is uncertain as they have not been shown to identify patients at increased risk for perioperative bleeding.
Thrombelastrography/Thrombelastometry Hemostatic Function in Healthy and Preeclamptic Parturients
Davies et al., Anesth Analg 2007; 104: 416-420
Fibrinogen, Platelet Numbers and Clot StrengthFibrinogen Levels and Clot Strength in Thrombocytopenia
Lang et al., Anesth Analg 2009; 108: 751-758
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
60

Fibrinogen Levels and Major Postpartum Hemorrhage
severe bleeding
mild bleeding
Charbit et al., J Thromb Haemost 2006; 5: 266-273
Fibrinogen Levels and Chest Tube Drainage After CABG
low drainage high drainage
Blome et al., Thromb Haemost 2005; 93: 1101-1107
Preoperative Fibrinogen Substitution and Hemoglobin Level
20 patients, 2 g fibrinogen, CABG, no antifibrinolytics
blood loss 565 ± 150 ml/12 h vs.830 ± 268 ml/12 h*
Karlsson et al., Thromb Haemost 2009; 102: 137-144 Rahe-Meyer et al., J Thorac Cardiovasc Surg 2009; 138: 694-702
Fibrinogen in Thoracic Aortic Aneurysm Repair
retrospective vs. prospective
fibrinogen 7.8 ± 2.7 g
Timing of blood loss assessment 5 minutes in group F, no definition in group A
TEG-Guided High Fibrinogen Levels and Bleeding after Aortic Surgery
Rahe-Meyer et al., Br J Anaesth 2009; 102: 785-792
5.7 g fibrinogen
Standard Laboratory or Point of Care?
CABG surgery
Avidan et al., British J Anaesth 2004; 92: 178-186
318 women with postpartum hysterectomy
PRCs 10 units (0-116 units)FFPs 4 units (0-24 units)Cryoprecipitate 0 units (0-40 units)Platelets 0 units (0- 21)Factor VIIa 9%
Fibrinogen?Antifibrinolytics?
Knight et al., BJOG 2007; 1380-1387
Survival of Trauma Patients and Ratio of Plasma to RBC
246 trauma patients with massive transfusion
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
61

„At the present time there is probably insufficient evidence to indicate that the technology (thrombelastography) should be routinely adopted for the prediction or management of bleeding...“
Semin Thromb Haemost 2009; 35: 9-22
Summary
� Standard laboratory testing
� Insensitive� Long turnaround time
� Point of care monitoring
� easy to use� Results rapidly available (20-30 minutes) (if not moved to a
central laboratory)
� Not recognized as valid and accurate by hematologists
� Standardization, maintenance?� No consistent correlation with clinically significant bleeding
� Advantage over conventional laboratory monitoring not proven
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
62

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 6: Caesarean Section General anaesthesia for Caesarean section: what’s new? Dr David Levy Consultant Anaesthetist, Queen's Medical Centre, Nottingham
A concise overview appeared in Anaesthesia and Intensive Care Medicine in 20071; an update on rapid sequence induction in obstetrics was published earlier this year in Current Opinion in Anesthesiology.2
General anaesthesia: incidence and mortality The Obstetric Anaesthetists’ Association’s National Obstetric Anaesthesia Database www.oaa-anaes.ac.uk revealed a rate of general anaesthesia (GA) for Caesarean section (CS) of 11% in 2005. There is an increasing likelihood that a trainee’s first experience of CS under GA will be an emergency case3 - a strong case for simulation-based team training.4 GA is indicated for a majority of Category 1 CS, and other cases in which a regional block is absolutely contra-indicated, or has failed. The decision-making process for GA versus regional block is complex, and depends not only on clinical urgency, but the experience, attitudes and skill levels of anaesthetist and obstetrician - the quality of communication and teamwork is pivotal.5
In the Report on Confidential Enquiries into Maternal Deaths (CEMD) in the United Kingdom for 1994-6, there were no deaths from GA: the solitary anaesthetic death followed combined spinal-epidural anaesthesia.6 However, a Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) highlighted four cases from 1994-5 in which GA was associated with life-threatening hazards (two cases of anaphylaxis, two airway crises).7 Two deaths in the 1997-9 triennium were attributable to complications of GA - one case of aspiration in a postpartum woman re-anaesthetised for removal of abdominal packs, and a case of airway obstruction during change of tracheostomy tube in a woman who had sustained major haemorrhage and multi-organ failure.8 The 2000-2 Report9 described 6 deaths, and featured the unwelcome reappearance of oesophageal intubation as a cause of mortality. Although the Report for 2003-5 cited 6 anaesthetic deaths, none was attributable to airway management at CS.10
1947: introduction of neuromuscular blocking agents The introduction of neuromuscular block to inhalational obstetric anaesthesia allowed a lighter plane of anaesthesia, with respiration assisted to avoid any ‘suboxygenation’. In 1947, Gray described
a technique of induction with kemithal (a thiobarbiturate), maintenance with cyclopropane, and the addition of d-tubocurarine 15 mg for neuromuscular block.11 The purported benefits were • Increased uterine contractility; • Less sleepy neonates; • Swifter maternal recovery. Only one patient in the series required tracheal intubation, when the 'ill-advised' insertion of a pharyngeal airway provoked vomiting. Occasional signs of slight residual curarisation at the end of an unusually quick operation were treated with neostigmine and atropine. 1959: succinylcholine 12 years later, Hamer Hodges and colleagues published the results of a comparison of a thiopental, succinylcholine, nitrous oxide/oxygen technique with three anaesthetic regimens in which mothers received trichloroethylene, cyclopropane or diethyl ether.12 Babies born to mothers who had minimal anaesthesia facilitated by neuromuscular block had shorter times to regular breathing and active crying. Succinylcholine was the ‘relaxant of choice’ on account of its freedom from adverse neonatal effects: there were concerns about the extent of placental transfer of the only two alternatives, d-tubocurarine and gallamine. Resumption of maternal spontaneous respiration reassured the investigators that the baby would not be affected. This landmark study led to the widespread replacement of mask and ether by intravenous induction, succinylcholine and tracheal intubation. The induction regimen has remained essentially unchanged for half a century, although certain aspects differed from contemporary practice: • Women received pre-operative atropine, but no
antacid; • Anaesthesia was induced with steep head-up tilt; • There was no attempt to relieve aortocaval
compression; • Pre-oxygenation was not undertaken; • The drug doses were smaller: thiopental 200-250
mg, succinylcholine 50 mg; • No application of cricoid pressure (it wasn’t
described until 1961); • The lungs were ventilated with oxygen by
mask/Magill breathing system before intubation;
63

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
• There was ‘absolutely no justification’ for the administration of any agent other than N2O between induction and delivery;
• 100% O2 was given just before delivery. Although babies born to mothers anaesthetised with ether by facemask were undoubtedly sleepier than those whose mothers who had light anaesthesia and neuromuscular block, they were not necessarily compromised. It is open to debate whether in the hands of non-specialist anaesthetists the new technique was any safer. In the CEMD for 1964-6 technical difficulties with tracheal intubation were first mentioned, and the number of maternal deaths from anaesthesia rose steeply.13 Scott wrote of the introduction of neuromuscular block to obstetric practice '…if we had been honest, the attraction of the new method was the speed and ease with which we could present the intubated paralysed mother to the obstetrician. We did not advertise the increased incidence of death due to Mendelson's syndrome and failed intubation resulting from suxamethonium and crash induction'.14 Cricoid pressure is used unquestioningly in the UK. The evidence base for the technique has been called into question by Priebe, who has argued that possibly more patients are endangered than protected, by interference with optimal airway management.15 In 1962, Crawford stipulated criteria to be satisfied in order that anaesthetic regimens for elective CS might be compared.16
• Women should be at or beyond the 36th week of pregnancy;
• Membranes must be intact; labour must not have been established;
• Neonatal weight must be greater than 2500 g. He proposed categorising elective cases according to whether or not placental function and fetal health were considered satisfactory. Crawford also used thiopental and succinylcholine, N2O and O2 and regarded uterine relaxation as the only indication for halothane.17 He accepted that 4.5% of women having elective CS were awake at some point, and since ‘lightness of anaesthesia was the aim’, did not consider it justifiable to alter the technique.
Some 25 years later, he wrote that uterine relaxation conferred by a volatile agent might actually improve fetal compromise to which uterine hyperstimulation had been contributory. It was by then recognized that a maternal stress response to excessively light GA is to the detriment of uteroplacental blood flow.18 1970: halothane Moir demonstrated improved Apgar scores with N2O/O2 50:50 + halothane 0.5% (inspired) compared to N2O/O2 70:30 without halothane.19 He surmised that it was the higher FIO2
permitted by the use of
halothane that was responsible for the better neonatal condition. Whereas two of 50 women who had unsupplemented N2O/O2 had clear recall, halothane ensured lack of awareness and did not cause increased blood loss. This paper led the move away from maintenance with only N2O/O2. Halothane 0.8% (inspired) was dismissed because systolic arterial pressure decreased to <90 mmHg in a quarter of patients, although blood loss was no greater. Moir’s paper was reproduced as a BJA 'citation classic' in 1998. In her commentary, Reynolds described GA as 'innocuous and reversible' for the baby.20
In the absence of asphyxia, the Apgar score at one minute does not have prognostic significance.21 Provided the following are ensured, GA per se is not harmful to the baby: • Maintenance of maternal oxygenation; • Maintenance of maternal normocapnia for
pregnancy; • Strict avoidance of aortocaval compression; • Uterine incision-delivery interval is minimised; • A paediatrician is present to support neonatal
ventilation. GA for incidental surgery in pregnancy for which local anaesthesia is not feasible (e.g. drainage of a breast abscess) should not be withheld for fear of adverse effects on the baby or uterus. Lack of fetal heart beat-to-beat variability with normal baseline rate should not be interpreted as evidence of fetal compromise.22
2000: opioids In an investigation of the stress response to tracheal intubation and surgery, the supplementation of thiopental 4 mg kg-1 at induction by alfentanil 10 µg kg-1 was compared with saline.23 Women in the alfentanil group had smaller increases in arterial pressure and heart rate. Mean plasma norepinephrine concentration was lower in the alfentanil group after tracheal intubation but at time of delivery was similar to that of the saline group. Apgar scores were lower at 1 minute in neonates whose mothers had received alfentanil, although not at 5 minutes, and neonatal adaptive capacity scores (NACS) were similar at 15 and 120 min. There was no difference in mean umbilical artery (UA) pH between groups. The slightly greater UA PO2 in the alfentanil group was attributed to decreased oxygen consumption. Mean cord UA norepinephrine concentration in the alfentanil group was approximately half that in the control group. It is not know whether attenuating the neonatal stress response is good or bad: high sympathoadrenal activity may promote neonatal adaptation to extra-uterine life.
64

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Remifentanil has been studied as an adjunct to GA regimens;24,25 numerous case reports attest to haemodynamic stability in women with cardiac disease.26,27
100% O2 Both isoflurane and enflurane in oxygen without N2O have been shown to provide satisfactory anaesthesia for CS.28 50% N2O/O2 + 0.6% isoflurane (inspired) has been compared with 100% O2 + 1.2% isoflurane for emergency CS. 100% O2 resulted in increased mean umbilical venous (UV) PO2, but no significant differences in UA pH.29 There was less need for neonatal oxygen and IPPV although a greater need for suction in the 100% O2 group. The authors’ widely quoted claim that this amounted to ‘less resuscitation’ is open to question. Any improvement in fetal oxygenation from 100% O2 might be limited by the prevailing pathophysiology (e.g. placental abruption). If N2O is omitted, it is important that overpressure is used to accelerate attainment of the desired end-tidal vapour tension. Administration of 100% O2 to the mother is associated with increased fetal oxygen saturation30 and UV oxygen content.31 However, maternal hyperoxia during regional anaesthesia causes increased free radical activity.32 Free radicals cause depletion of intrinsic antioxidant systems and are potentially detrimental to a neonate’s ability to withstand subsequent insults. The relationship between free radical formation and neonatal outcome is uncertain.33 The significance for neonatal well-being of minor differences in UA pH values between anaesthetic regimens is uncertain. Severe acidaemia (umbilical artery pH <7.0) with 1-minute Apgar ≤3 and 5-minute Apgar <7 is predictive of serious neonatal morbidity.34,35 It has been argued that UA standard base excess (SBE) is a better measure of fetal well-being than pH (which reflects both metabolic and respiratory acidosis).36 Respiratory acidosis can occur rapidly without hypoxic injury, whilst a large negative SBE might be indicative of prolonged oxygen debt and anaerobic metabolism. The validity of the Neonatal Neurologic and Adaptive Capacity Score (NACS) has been questioned.37
In short, there is insufficient evidence upon which to recommend an optimal FIO2
.
Which i.v. agent? There is little evidence that any agent is better than thiopental. According to the respective data sheets, the dose of thiopental should be limited to 250 mg: propofol is explicitly contra-indicated for use in obstetrics. It has been shown in sheep that peak brain concentrations are reached earlier with thiopental
compared to propofol.38 At CS in women, propofol 2 mg kg-1 attenuated maternal haemodynamic and catecholamine responses to intubation more effectively than thiopental 4 mg kg-1, although neonatal Apgar scores, NACS, cord blood gas tensions and catecholamine concentrations were similar.39 An OAA Controversies motion40 in 2003 was ‘Propofol should be the induction agent of choice for caesarean section under general anaesthesia’. There was overwhelming opposition to the motion amongst delegates before and after the debate. There were no instances of recall, unpleasant dreams, or dysphoria when ketamine induction was followed by N2O/O2.
41 It seems that emergence phenomena are avoided when awakening occurs some time after an induction dose of ketamine has been distributed. Investigations of midazolam were prompted by perceived potential benefits of its cardiovascular stability and amnesic effect.42 1 minute Apgar scores gave cause for concern in one study43 but not another (in which a larger dose was studied.44 Small doses of midazolam are certainly not contra-indicated for sedation during awake fibre-optic intubation.45, 46 Neonatal times to sustained respiration were shorter with etomidate 0.3 mg kg-1 compared to a rather small dose of thiopental (3.5 mg kg-1).47 Inhalation induction? Both sevoflurane48 and desflurane49 have been evaluated for maintenance of GA for CS, with no apparent adverse maternal or neonatal effects. These agents offer the advantage of more rapid approximation of alveolar to inspired tensions as the anaesthetic effect of the i.v. induction dose declines. Maternal recovery was not demonstrably faster with either of the newer agents (sevoflurane was compared with isoflurane, desflurane with enflurane). Crawford argued that using halothane for induction risked a dangerous tissue accumulation of the drug, and the threat of inadequate uterine contraction. He pointed out that the uterine response to discontinuing halothane was dependent upon the duration of its administration. Sevoflurane has a conspicuously low propensity for airway irritation and been use successfully for inhalational induction of anaesthesia for CS in the absence of vascular access50,51 and in status asthmaticus.52 The smooth, rapid onset and lack of coughing or vomiting suggest that the technique does not necessarily incur an increased risk of aspiration.53 The following approach is suggested: • 20 -30° head-up tilt; • breathing system primed with sevoflurane 8% in
N2O/O2 (2:1); • tidal respiration;
65

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
• i.v. canulation after loss of consciousness; • neuromuscular blockade, tracheal intubation. Non-depolarising neuromuscular block at induction Awake fibre-optic intubation should be considered if the history or evaluation of the airway suggest that tracheal intubation might be difficult. The principal reason for the continuing use of succinylcholine, the rapid recovery of maternal neuromuscular function in the event of an airway crisis, was never originally considered potentially advantageous. It has been estimated that a serious reaction to succinylcholine might be expected once in every 4000 inductions.54 Anaphylaxis to succinylcholine has been responsible for maternal deaths at CS, and many near misses.55 Rocuronium 0.6 mg kg-1 is licensed for CS, and has been shown to produce acceptable intubating conditions after thiopental 6 mg kg-1 within 90 s, without untoward neonatal effects.56 The onset of rocuronium 0.6 mg kg-1 is even faster with ketamine 1.5 mg kg-1.57 Doubling the intubating dose of rocuronium would, predictably, further shorten the onset time, but incur a duration of action excessive for CS. It might be expected that the mass of rocuronium transferred across the placenta would increase in proportion to the maternal dose, but it is uncertain whether the fraction of 1.2 mg kg-1 transferred in the event of protracted surgical delivery would be innocuous. In the event of failed tracheal intubation, it might be argued, controversially, that inserting a laryngeal mask airway (LMA) and ventilating the lungs with cricoid pressure applied is no less safe overall than using succinylcholine and attempting to proceed with inhalational anaesthesia by spontaneous respiration.58,59 Unlike the case with succinylcholine, optimal conditions will be sustained for airway management and maintenance of oxygenation, and vomiting cannot occur. Maintenance of a slight head-up tilt will allow gravity to reduce the risk of reflux of gastric contents. The evolving role of the LMA in obstetrics has been reviewed.60 The ProSeal LMA incorporates a second tube, which makes a sealed junction against the upper oesophageal sphincter, allowing continuity with the gastro-intestinal tract and isolation from the airway. Gastric insufflation during IPPV is minimised, and it is possible to pass a gastric tube.61 There are reports of use of the ProSeal LMA a rescue airway at CS.62,63 In the most unlikely event of airway obstruction at the glottis causing a ‘can’t intubate, can’t ventilate’ scenario, a better chance of successful cricothyrotomy will be afforded by profound neuromuscular block.
Sugammadex The rocuronium antagonist sugammadex was launched in Europe in late 2008. In a non-obstetric population, recovery evoked by sugammadex 16mg kg-1 (administered 3 min after rocuronium 1.2 mg kg-
1) was swifter than the same degree of spontaneous recovery from succinylcholine.64 Data on placental transfer of sugammadex are extremely sparse, and limited to animals: the manufacturer has indicated that <2-6% is transferred in rat and rabbit populations. There is no information about placental transfer of the sugammadex-rocuronium complex. However, adverse fetal effects of sugammadex-encapsulated rocuronium are unlikely. Awareness and uterine relaxation The tenet of Crawford's opposition to halothane was the feared effect on uterine tone. A dose-dependent reduction in uterine muscle contractility has been shown in vitro with sevoflurane and desflurane.65 This finding concords with earlier studies of the halothane, enflurane and isoflurane. However, myometrial responsiveness to Syntocinon at different end-tidal vapour tensions has never been studied in vivo. Experience with ex utero intrapartum treatment (EXIT) of babies with potential airway obstruction has provided evidence that the effect of deep inhalational anaesthesia with modern, insoluble agents is rapidly reversible. 2 MAC (end-tidal) vapour concentration (nevertheless requiring supplementation with glyceryl trinitrate) has been used to relax the uterus whilst allowing fetal oxygenation by continued uteroplacental perfusion.66
An OAA Controversies debate in 1996 explored whether awareness during GA for CS is negligent.67 If the uterus is failing to contract, haemorrhage is life-threatening and the volatile agent is discontinued, N2O should nevertheless be continued, and anaesthesia maintained by opioids or benzodiazepines. Ketamine is perhaps the ideal agent in this situation. I suggest that in 2009 with inhalational agent monitoring now universally available, the risk of awareness in obstetric anaesthesia should have been consigned to history. A prospective study from Australia and New Zealand found that the awareness remains a significant but avoidable complication of GA for CS.68 To maintain bispectral index (BIS) values <60 (for ‘adequate’ depth of anaesthesia) at CS, end-tidal vapour concentration >0.75 MAC (+ 50% N2O) has been recommended.69
Pre-eclampsia Uncorrected coagulopathy, or symptoms consistent with impending eclampsia (severe headache or visual disturbance) are potential maternal indications for GA. Potential benefit (smaller UA base deficit) has
66

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
been shown for compromised fetuses when mothers received GA as opposed to single-shot spinal anaesthesia.70 Prior communication with a paediatrician is essential in order that preparation can be made for antagonism of opioid or provision of ventilatory support for the neonate. Laryngeal oedema is a real risk – beware the patient with recent voice change. Any dubious notion of light GA for the baby’s benefit should be overridden by efforts to protect the mother’s cerebral circulation.71 Although the onset and duration of succinylcholine are unaffected by therapeutic serum magnesium concentrations, the durations of action of all non-depolarising drugs are potentiated. • Have a low threshold for direct arterial pressure
monitoring; • Attenuate the pressor response to intubation with
alfentanil 10 µg kg-1 or remifentanil 2 µg kg-1 before rapid sequence induction with a generous dose of thiopental;
• Peripheral nerve stimulator essential to ascertain the degree of neuromuscular block;
• Before extubation, consider additional antihypertensive therapy (e.g. labetalol in 10-20 mg increments) to avert a dangerous pressor response.
Any patient whose larynx was noted to be swollen at laryngoscopy, or in whom intubation was traumatic is at particular risk of laryngeal oedema. Postoperative care must be undertaken in an ICU or high-dependency area with an anaesthetist immediately available. Midwives should be alerted to the ominous significance of stridor. Placenta praevia & accreta UK72 and American73 retrospective studies and a small prospective randomised trial in Korea74 have compared regional and general anaesthesia for CS with placenta praevia. The commonly held obstetric view that placenta praevia necessarily dictates GA is not supported. Regional anaesthesia was associated with reduced estimated blood loss and transfusion requirements. However, risk factors for placenta accreta (anterior placenta praevia in women over 35 who have had previous CSs)75 flag up a particularly high risk of massive haemorrhage. GA with provision for postoperative ICU admission might be considered prudent.76 Conclusion Although the CS rate has increased, use of GA has declined and trainee hours of work have been decreased. Most anaesthesia trainees have minimal experience of GA in obstetrics, and should take every opportunity to practise the technique. Increased presence of consultant anaesthetists on obstetric units should help optimize training opportunities. Training
adjuncts, including medical simulation, may have a useful role. GA for operative obstetrics, especially elective cases, is not inherently unsafe. If trainees are instilled with excessive anxiety about the potential hazards of GA, complications (especially failed intubation) will remain prevalent.77
References 1. Banks A, Levy D. General anaesthesia for operative
obstetrics. Anaesthesia and Intensive Care Medicine 2007; 8: 317-9
2. Sharp LM, Levy DM. Rapid sequence induction in obstetrics revisited. Current Opinion in Anesthesiology 2009; 22: 357-61
3. Jenkins JG, Khan MM. Anaesthesia for Caesarean section: a survey in a UK region from 1992-2002. Anaesthesia 2003; 58: 1114-8
4. Lipman S, Carvalho B, Brock-Utne J. Editorial. The demise of general anesthesia in obstetrics revisited: prescription for a cure. International Journal of Obstetric Anesthesia 2005; 14: 2-4
5. Shroff R, Thompson ACD, McCrum A, Rees SGO. Prospective multidisciplinary audit of obstetric general anaesthesia in a District General Hospital. Journal of Obstetrics and Gynaecology 2004; 24: 641-6
6. Why mothers die 1994-1996. Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: HMSO, 1998 www.cmace.org.uk
7. Focus group. Obstetric anaesthesia delays and complications. In: Confidential enquiry into stillbirths and deaths in infancy. 7th annual report. London: Maternal and Child Health Research Consortium, 2000: 41-52 www.cmace.org.uk
8. Why mothers die 1997-1999. The confidential enquiries into maternal deaths in the United Kingdom. London: Royal College of Obstetricians and Gynaecologists, 2001 www.cmace.org.uk
9. Why mothers die 2000-2002. Report on confidential enquiries into maternal deaths in the United Kingdom. London: Royal College of Obstetricians and Gynaecologists, 2004 www.cmace.org.uk
10. Lewis, G (ed) 2007. The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer - 2003-2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH www.cmace.org.uk
11. Gray TC. d-Tubocurarine in Caesarean section. British Medical Journal 1947; 1: 444-5
12. Hamer Hodges RJ, Bennett JR, Tunstall ME, Knight RF. General anaesthesia for operative obstetrics. British Journal of Anaesthesia 1959; 31: 152-63
13. Morgan M. Anaesthetic contribution to maternal mortality. British Journal of Anaesthesia 1987; 59: 842-55
14. Scott DB. Awareness during Caesarean section. Anaesthesia 1991; 46: 693-94
67

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
15. Priebe H-J. Cricoid pressure: an alternative view. Seminars in Anesthesia, Perioperative Medicine and Pain 2005; 24: 120-6
16. Crawford JS. Anaesthesia for Caesarean section: a proposal for evaluation, with analysis of a method. British Journal of Anaesthesia 1962; 34: 179-94
17. Crawford JS. The place of halothane in obstetrics. British Journal of Anaesthesia 1962; 34: 386-90
18. Crawford JS. Editorial. Fetal well-being and maternal awareness. British Journal of Anaesthesia 1988; 61: 247-9
19. Moir DD. Anaesthesia for Caesarean section. An evaluation of a method using low concentrations of halothane and 50% of oxygen. British Journal of Anaesthesia 1970; 42: 136-42
20. Reynolds F. Commentary on reference 19. British Journal of Anaesthesia 1998; 80: 688-9
21. Akerman N, Lyons G. Problems with general anaesthesia for Caesarean section. Minerva Anestesiologica 2005; 71: 27-38 www.minervamedica.it/en/journals/minerva-anestesiologica/archive.php
22. Immer-Bansi A, Immer FF, Henle S, Spörri S, Petersen-Felix S. Unnecessary emergency Caesarean section due to silent CTG during anaesthesia? British Journal of Anaesthesia 2001; 87: 791-3
23. Gin T, Ngan-Kee WD, Siu YK, Stuart JC, Tan PE, Lam KK. Alfentanil given immediately before the induction of anesthesia for elective cesarean delivery. Anesthesia and Analgesia 2000; 90: 1167-72
24. Ngan Kee WD, Khaw KS, Ma KC, Wong ASY, Lee BB, Ng FF. Maternal and neonatal effects of remifentanil at induction of general anesthesia for caesarean delivery. Anesthesiology 2006; 104: 14-20
25. Draisci G, Valente A, Suppa E, Frassanito L, Pinto R, Meo F, De Sole P, Bossú E, Zafini BA. Remifentanil for cesarean section under general anesthesia: effects on maternal stress hormone secretion and neonatal well-being: a randomized trial. International Journal of Obstetric Anesthesia 2008; 17: 130-6.
26. Johnston AJ, Hall JM, Levy DM. Anaesthesia with remifentanil and rocuronium for caesarean section in a patient with long-QT syndrome and an automatic implantable cardioverter-defibrillator. International Journal of Obstetric Anesthesia 2000; 6: 133-6
27. McCarroll CP, Paxton LD, Elliott P, Wilson DB. Use of remifentanil in a patient with peripartum cardiomyopathy requiring Caesarean section. British Journal of Anaesthesia 2001; 86: 135-8
28. Tunstall ME, Sheikh A. Comparison of 1.5% enflurane with 1.25% isoflurane in oxygen for caesarean section: avoidance of awareness without nitrous oxide. British Journal of Anaesthesia 1989; 62: 138-43
29. Piggott SE, Bogod DG, Rosen M, Rees GAD, Harmer M. Isoflurane with either 100% oxygen or 50% nitrous oxide in oxygen for Caesarean section. British Journal of Anaesthesia 1990; 65: 325-9
30. Parpaglioni R, Capogna G, Celleno D, Fusco P. Intraoperative fetal oxygen saturation during Caesarean section: general anaesthesia using sevoflurane with either 100% oxygen or 50% nitrous
oxide in oxygen. European Journal of Anaesthesiology 2002; 19: 115-8
31. Ngan Kee WD, Khaw KS, Ma KC, Wong ASY, Lee BB. Randomised, double-blind comparison of different inspired oxygen fractions during general anaesthesia for Caesarean section. British Journal of Anaesthesia 2002; 89: 556-61
32. Khaw KS, Wang CC, Ngan Kee WD, Pang CP, Rogers MS. Effects of high inspired oxygen fraction during elective Caesarean section under spinal anaesthesia on maternal and fetal oxygenation and lipid peroxidation. British Journal of Anaesthesia 2002; 88: 18-23
33. Backe SK, Lyons G. Oxygen and elective Caesarean section. British Journal of Anaesthesia 2002; 88: 4-5
34. Van den Berg PP, Nelen WLDM, Jongsma HW, Nijland R, Kollée LAA, Nijhuis JG, Eskes TKAB. Neonatal complications in newborns with an umbilical artery pH<7.00. American Journal of Obstetrics and Gynecology 1996; 175: 1152-7
35. James DK. Caesarean section for fetal distress. British Medical Journal 2001; 332: 1316-7
36. McKinlay J, Lyons G. Obstetric neuraxial anaesthesia: which pressor agents should we be using? International Journal of Obstetric Anesthesia 2002; 11: 117-21
37. Camann W, Brazelton TB. Use and abuse of neonatal neurobehavioural testing. Anesthesiology 2000; 92: 3-5
38. Upton RN, Ludbrook GL. A model of the kinetics and dynamics of induction of anaesthesia in sheep: variable estimation for thiopental and comparison with propofol. British Journal of Anaesthesia 1999; 82: 890-9
39. Gin T, O'Meara ME, Kan AF, Leung RKW, Tan P, Yau G. Plasma catecholamines and neonatal condition after induction of anaesthesia with propofol or thiopentone at Caesarean section. British Journal of Anaesthesia 1993; 70: 311-6
40. Duggal K, Russell R. Propofol should be the induction agent of choice for caesarean section under general anaesthesia. International Journal of Obstetric Anesthesia 2003; 12: 275-9
41. Schhultetus RR, Paulus DA, Spohr GL. Haemodynamic effects of ketamine and thiopentone during anaesthetic induction for Caesarean section. Canadian Anaesthetists Society Journal 1985; 32: 592-6
42. Crawford ME, Carl P, Bach V, Ravlo O, Ohrt Mikkelsen B, Werner M. A randomized comparison between midazolam and thiopental for elective Cesarean section anesthesia: I. Mothers. Anesthesia and Analgesia 1989; 68: 229-33
43. Ravlo O, Carl P, Crawford ME, Bach V, Ohrt Mikkelsen B, Kirkegaard Nielsen H. A randomized comparison between midazolam and thiopental for elective Cesarean section anesthesia: II. Neonates. Anesthesia and Analgesia 1989; 68: 234-7
44. Bland BAR, Lawes EG, Duncan PW, Warnell I, Downing JW. Comparison of midazolam and thiopental for rapid sequence anesthetic induction for elective Cesarean section. Anesthesia and Analgesia 1987; 66: 1165-8
68

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
45. Glassenberg R. The church of the fiberoptic. An epistle to the faithful from an epigone. Today’s Anaesthetist 2000; 15: 80-6
46. Popat MT, Srivastava M, Russell R. Awake fibreoptic
intubation skills in obstetric patients: a survey of anaesthetists in the Oxford region. International Journal of Obstetric Anesthesia 2000; 9: 78-82
47. Downing JW, Buley RJR, Brock-Utne JG, Houlton PC. Etomidate for induction of anaesthesia at Caesarean section: comparison with thiopentone. British Journal of Anaesthesia 1979; 51: 135-9
48. Gambling DR, Sharma SK, White PF, Van Beveren TV, Bala AS, Gouldson R. Use of sevoflurane during elective Cesarean birth; a comparison with isoflurane and spinal anesthesia. Anesthesia and Analgesia 1995; 81: 90-5
49. Abboud TK, Zhu J, Richardson E, Da Silva EP, Donovan M. Desflurane: a new volatile anesthetic for cesarean section. Acta Anaesthesiologica Scandinavica 1995; 39: 723-6
50. Schaut DJ, Khona R, Gross JB. Sevoflurane inhalation induction for emergency cesarean section in a parturient with no intravenous access. Anesthesiology 1997; 86: 1392-4
51. Simon GR, Wilkins CJ, Smith I. Sevoflurane induction for emergency caesarean section: two case reports in women with needle phobia. International Journal of Obstetric Anesthesia 2002; 11: 296-300
52. Que JC, Lusaya VO. Sevoflurane induction for emergency Cesarean Section in a parturient in status asthmaticus. Anesthesiology 1999; 90: 1475-6
53. Levy DM. Inhalational induction of anaesthesia for caesarean section: not to be sniffed at? International Journal of Obstetric Anesthesia 2002; 11: 235-7
54. Watkins J. Anaesthetic reactions. In Watkins J, Levy CJ, eds. Guide to immediate anaesthetic reactions. London: Butterworths, 1988: p 27
55. Stannard L, Bellis A. Maternal anaphylactic reaction to a general anaesthetic at emergency caesarean section for fetal bradycardia. British Journal of Obstetrics and Gynaecology 2001; 108: 539-40
56. Abouleish E, Abboud T, Lechevalier T, Zhu J, Chalian A, Alford K. Rocuronium (Org 9426) for Caesarean section. British Journal of Anaesthesia 1994; 73: 336-41
57. Baraka AS, Sayyid SS, Assaf BA. Thiopental-rocuronium versus ketamine-rocuronium for rapid-sequence intubation in parturients undergoing Cesarean section. Anesthesia and Analgesia 1997; 84: 1104-7
58. Hewett E, Livingstone P. Management of failed tracheal intubation at Caesarean section. Anaesthesia and Intensive Care 18: 330-5
59. Levy DM. Controversies. Non-depolarising neuromuscular blockers can be used routinely instead of suxamethonium at induction of general anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 1999; 8: 266-70
60. Preston R. The evolving role of the laryngeal mask airway in obstetrics. Canadian Journal of Anaesthesia 2001; 48: 1061-5
61. Brain AIJ, Verghese C, Strube PJ. The LMA 'ProSeal' – a laryngeal mask with an oesophageal vent. British Journal of Anaesthesia 2000; 84: 650-4
62. Awan R, Nolan JP, Cook TM. Use of a ProSealTM laryngeal mask airway for airway maintenance during emergency Caesarean section after failed tracheal intubation. British Journal of Anaesthesia 2004 92: 144-6
63. Keller C, Brimacombe J, Lirk P, Pühringer F. Failed obstetric tracheal intubation and postoperative respiratory support with the ProSealTM laryngeal mask airway. Anesthesia and Analgesia 2004; 98: 1467-70
64. Lee C, Jahr JS, Candiotti KA, Warriner B, Zornow MH, Naguib M. Reversal of profound neuromuscular block by sugammadex administered three minutes after rocuronium: a comparison with spontaneous recovery from succinylcholine. Anesthesiology 2009; 110: 1020-5
65. Turner RJ, Lambros M, Kenway L, Gatt SP. The in-vitro effects of sevoflurane and desflurane on the contractility of pregnant human uterine muscle. International Journal of Obstetric Anesthesia 2002; 11: 246-51
66. Dahlgren G, Törnberg DC, Pregner K, Irestedt L. Four cases of the ex utero intrapartum treatment (EXIT) procedure: anesthetic implications. International Journal of Obstetric Anesthesia 2004; 13: 178-82
67. Hull CJ, Thorburn J. Awareness is due to negligence during general anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 1999; 6: 178-81
68. Paech MJ, Scott KL, Clavisi O, Chua S, Mcdonnell N. A prospective study of awareness and recall associated with general anaesthesia for caesarean section. International Journal of Obstetric Anesthesia 2008; 17: 298-303
69. Chin KJ, Yeo SW. A BIS-guided study of sevoflurane requirements for adequate depth of anaesthesia in Caesarean section. Anaesthesia 2004; 59: 1064-8
70. Dyer RA, Els I, Farbas J, Torr GJ, Schoeman LK, James MF. Prospective, randomized trial comparing general with spinal anaesthesia for Cesarean delivery in preeclamptic patients with a nonreassuring fetal heart trace. Anesthesiology 2003; 99: 561-9
71. Belfort MA, Varner MW, Dizon-Townson DS, Grunewald C, Nisell H. Cerebral perfusion pressure, and not cerebral blood flow, may be the critical determinant of intracranial injury in preeclampsia: A new hypothesis. American Journal of Obstetrics & Gynecology 2002; 187: 626-34
72. Parekh N, Husaini SWU, Russell IF. Caesarean section for placenta praevia: a retrospective study of anaesthetic management. British Journal of Anaesthesia 2000; 84: 731-4
73. Frederiksen M, Glassenberg R, Stika CS. Placenta previa: a 22-year analysis. American Journal of Obstetrics and Gynecology 1999; 180: 1432-7
74. Hong J-Y, Jee Y-S, Yoon H-J, Kim SM. Comparison of general and epidural anesthesia in elective cesarean section for placenta previa totalis: maternal haemodynamics, blood loss and neonatal outcome. International Journal of Obstetric Anesthesia 2003; 12: 12-16
69

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
75. Miller DA, Chollet JA, Murphy Goodwin TM. Clinical risk factors for placenta previa-placenta accreta. American Journal of Obstetrics and Gynecology 1997; 177: 210-4
76. Weiniger CF, Elram T, Ginosar Y, Mankuta D, Weissman C, Ezra Y. Anaesthetic management of placenta accreta: use of a pre-operative high and low suspicion classification. Anaesthesia 2005; 60: 1079-84
77. Russell R. Editorial. Failed intubation in obstetrics: a self-fulfilling prophecy? International Journal of Obstetric Anesthesia 2007; 16: 1-3
70

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 6: Caesarean Section Managing the difficult airway in obstetrics Dr Mansukh Popat Consultant Anaesthetist, John Radcliffe Hospital, Oxford
71

What are the consequences?
• Safe outcome if protocols followed
• Examples of protocol violationAirway not pre assessedRepeated muscle relaxantsRepeated intubation attemptsFailure to use appropriate equipmentPoor follow up
CEMD : 2000 – 2002 Anaesthesia Deaths
6 + (1) - All GA, all emergencies, all trainees
� Aspiration/Failed intubation; n = 1� Anaphylaxis; n = 1
� Oesophageal intubation n = 3SHO anaesthetists, equipment unavailable/not used, Auscultation OK
� Hypoventilation; n = 2Trainees, isolated sites, help late, ObesityCapnography not used in 1
Pre operative assessmentPlanning and Procedures for • Anticipated difficult airway• Unanticipated difficult airway
How to reduce the incidence of failed intubation and its consequences?
Individual Issues
Organisation issues
Pre operative Airway Assessment
How?
When and by whom?
• Duty Anaesthetist - ? Every woman/ anaesthetic intervention
• Midwives/obstetrician
• Antenatal referral (education)
How?
History
Notes
Bedside tests
• Eyeball test (obvious difficulty)
• Difficult laryngoscopy
• Difficult face mask
• Difficult LMA
airway oedema
BMI Recognition of difficult laryngoscopy
• Mouth opening Inadequate
• Mallampati class Post pharynx no seen
• Jaw protrusion- restricted
• Thyromental Inadequate
• BMI - at booking > 35
• Pathological airway - airway oedema due to PET
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
72

Pre operative Airway Assessment
Which tests?
When and by whom?
• Duty Anaesthetist - ? Every woman/ anaesthetic intervention
• Midwives/obstetrician
• Antenatal referral (e.g. obese)
Pre operative assessmentPlanning and procedures for• anticipated difficult airway• unanticipated difficult airway
How to reduce the incidence of failed intubation and its consequences?
Anticipated difficult airway
• Antenatal team planning e.g. help from colleagueObstetric plan may need to be changed
• Regional anaesthesia is safe option
PLAN A - Regional Anaesthesia for C/S
Good reasons• Anaesthetic expertise
• Patient preference
• Sedation uncommon
• Airway accessible
Problems
• May be contraindicated
• Inadequate block
• High/total spinal
PLAN B must always be worked out in advance
Anticipated difficult airway
PLAN B Options� Awake intubation
� GA with supraglottic device +/- intubation
� Awake look and GA
� Local infiltration anaesthesia
Awake fibreoptic intubation skills in obstetric patients: a survey of anaesthetists in the Oxford region.
Popat M, Srivastava M, Russell R. IJOA 2000; 9: 78-82
Choice of anaesthetic technique if regional anesthesia fails in a patient with a known difficult airway
Awake intubation 75/83(88%)
GA with LMA 5/83
GA with mask and airway 1/83
LA infiltration 1/83
Plan A Combined spinal-epidural
Plan B Awake Fibreoptic Intubation (AFI)
Elective Caesarean sectionFAILED PLAN A
AFI following failed RA
for C- section in a parturient with Still’s disease
Popat M, Chippa J, Russell R
Eur J Anaesth 2000; 17: 211-14
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
73

Flexibility/continuous visualisation
Ability to apply local anaesthetic
Well tolerated by patients
High success rate
Flexible fibreoptic laryngoscope -advantages for awake intubation
AFI in Obstetrics: Practical issues
Patient related
� Regurgitation and aspiration
� Nasal bleeding
� Fetal/neonatal welfare
Environment related� Equipment, expertise
Awake fibreoptic intubation skills in obstetric patients: a survey of anaesthetists in the Oxford region
Popat M, Srivastava M, Russell R. IJOA 2000; 9: 78-82
Confidence in performing AFI in OB patients
All anaesthetists 30/68 (44%)
OB anaesthetists 12/31 (40%)
Practical Issues: Patient related
1. Patient preparation
2. Position of patient
3. Monitoring & oxygenation
4. Sedation
5. Intubation route
6. LA of upper airway
1. Patient Preparation
�Psychological
�Pharmacological
Aspiration prophylaxis
Antisialogogue e.g. glyco 0.2mg iv
2. Position of patient
Advantages of sitting position
� Reduced risk of aspiration
� Venacaval occlusion prevented
� Topical anaesthesia better tolerated
� Airway obstruction minimal
3. Monitoring and oxygenation
4. Sedation
Benefits
Patient comfort, amnesia and anxiolysis
Risks
� Effect on laryngeal competence
� Airway obstruction
� Effect on baby
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
74

Awake fibreoptic intubation following previous failed intubation.
Popat M, Russell R. IJOA 2001; 10: 332-333.
My recipe
• Midazolam 1-2mg
• Fentanyl 25-50mcg
• Propofol TCI
1mcg/ml and titrate
5. Oral Intubation route
Author Indication Route guideBroomhead 1995 Ankylosing spondylitits Bermen
D’Alessio 1995 Pre eclampsia / HELLP Williams
Mclure 1996 Noonan’s syndrome Ovassapian
Reid 1999 Thyroid goitre Rigid laryng
Popat 1999 Stills disease Ovassapian
Popat 2001 Previous failed intubation Safe Bite
A new device to facilitate oral fibreoptic intubation.
Otero J, Moaz K, Popat M. Anaesthesia 2001; 56: 272-73Safebite
Bermen6. Local anaesthesia of upper airway
� Nerve blocks
� Nebulised LA
� Topical anaesthesia
Awake fibreoptic intubation in the patient at high risk of aspiration.
Ovassapian A. et al Br J Anaesth 1989; 62: 13-16
123 patients/ 129 awake intubations
No LA Transtracheal SAYGO
n = 15 29 85
All except six were sedated (diazepam+/- fentanyl)
One patient vomited
No clinical/radiological evidence of regurgitation/aspiration
My recipe
• 2% lignocaine gargle
• Spray as you go -
4% via epidural catheter
Back up
Cricothyroid puncture
1. Should all Consultant Obstetric Anaesthetists’ be confident in performing an AFI?
2. Can an AFI be performed rapidly for category 1 C/S
Pre operative assessmentPlanning and procedures for • anticipated difficult airway• unanticipated difficult airway
How to reduce the incidence of failed intubation and its consequences?
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
75

• Delivering a ‘safe obstetric’ GA
• Following agreed ‘failed intubation drill’
Planning and procedures for Unanticipated difficult airway Delivering a ‘safe obstetric’ GA
• Preparation
• Positioning the mother
• Pre oxygenation : at least 3 min
• Perfect technique
Preparation
At the start of every shift• Airway equipment• Drugs• Help – Who? How?
Airway equipmentRoutine
• Laryngoscope - short handle & long blade
• ETT - 7.0 mm or smaller
• Gum elastic bougie
• Laryngeal mask airway
• Check cricothyroidotomy
equipment
Delivering a ‘safe obstetric’ GA
• Preparation
• Positioning the mother
• Pre oxygenation : at least 3 min
• Perfect technique
Positioning the mother
• Head & neck
• Breasts
• Hands
• Thoracic tilt
Ramping for obese patients
Table tilt
Wedge
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
76

Delivering a ‘safe obstetric’ GA
• Preparation
• Positioning the mother
• Pre oxygenation : tight mask
• Perfect technique
Perfect technique
1st attempt = best attempt
Cricoid pressure (correct technique)
Induction agent (Give enough)
Suxamethonium (Give enough and wait to act)
Good laryngoscopy technique
Confirmation of intubation (visual, CO2, Auscultate)
� Consensus
(discussion & feedback)
� Evidence
� Experience
Difficult Airway Society Guidelines
Henderson JJ, Popat MT, Latto IP, Pearce AC.
Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia 2004: 675-94.
Routine induction Rapid sequence induction
1st attempt
2nd attempt
3rd attemptFailed intubation drill
FAILED INTUBATION
• DECISION - tracheal tube cannot be passed and the lungs must be ventilated
Maintenance of Ventilation
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
77

Failed intubation Ventilation successful
Decision to continue anaesthesia or awaken
Indications for continuing
Definite Maternal (haemorrhage, cardiac arrest)
Definite RA contraindicated e.g. coagulopathy & expertise not available for awake intubation
May be Sudden severe fetal distress (cord prolapse, abruption)
In all other cases, Awaken & perform surgery under RA
� Should LMA be used for intubation?
Some thoughts
� ? LMA before bag and mask
� If LMA is positioned wellShould surgery always proceedIf so
Rapid sequence induction
Why not plan B?
• Cricoid pressure and LM devices
• Short apnoea time
Failed IntubationFailed Ventilation (face mask, LMA)
Increasing hypoxaemia
Maintenance of oxygenation
What needle do you use?
13G Ravussin
6.0F Cook
14G Venflon
What do you connect the needle to?
Manujet 3
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
78

Surgical cricothyrotomy
American College of Surgeons. ATLS course manual, 6th Ed 1997
Techniques for CICV
Intubation
AirtraqGlideScopePentax Airway scopeVideo laryngoscopes (McGrath, Storz)Optical stylets
Ventilation
Proseal
LMA supreme
I –gel
Ventilation & intubation
LMA C Trach®
New(er) Toys
Proseal LMA™
High seal pressure
Separates glottis & oesophagus
Prevent aspiration of regurgitated material
Oro-gastric tube
Better for IPPV
Learning curveAwan R, Nolan JP, Cook TM. Brit J Anaesth 2004; 92: 144
LMA Supreme
Single use
Shape = ILMA
Function = Proseal LMA
Intubating LMA
BJA 1997; 79:699 - 703, 704 -709, 710 -713
C Traq
Pre operative assessmentPlanning and procedures for • Anticipated difficult airway• Unanticipated difficult airway
How to reduce the incidence of failed intubation and its consequences?
Individual Issues
Organisation issues 0
200
400
600
800
1000
82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98
0
200
400
600
800
1000
82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98
GA for caesarean section
Total LSCSGA LSCS
Johnson et al. Anaesthesia 2000
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
79

0
5
10
15
20
25
30
35
82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98
0
5
10
15
20
25
30
35
82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98
GA for caesarean section
No of trainees
Mean no GA per trainee
Johnson et al. Anaesthesia 2000
GA for caesarean section
Caesarean Sections in OxfordYear Total CS Total GA Elective
LSCSElective
GAEmg LSCS
Emg GA Training
2003 1160 85 547 23 572 62 37
2002 1230 98 489 13 741 85 23
2001 1210 108 426 14 784 94 24
2000 1244 97 427 5 817 92 20
1999 1100 86 320 8 780 78 21
1998 1050 100 432 9 618 91 17
Lyons UK 1985 1 in 300
Hawthorne et al. UK 1996 1 in 250
Barnardo & Jenkins UK 2000 1 in 249
Samsoon & Young UK 1987 1 in 280
Rocke et al. S Africa 1992 1 in 750
Incidence of Failed Intubation
Competency Based Training
• knowledge
• skills
• attitude & behaviour
Technical skillsCan be taught on non obstetric patients
Non technical skills (attitudes/behaviour)Need to be taught on delivery suite
e.g. Communication, decision making, situation awareness
How?
Manikins/Simulators
Role play
Training for obstetric GA
02
46
810
1214
chec
k equ
ip
pre O2
drug
dose
time p
ost s
ux
head
pos
ition
get h
elp
bag+
mas
k
cricoi
d of
fLM
A
trache
02
46
810
1214
chec
k equ
ip
pre O2
drug
dose
time p
ost s
ux
head
pos
ition
get h
elp
bag+
mas
k
cricoi
d of
fLM
A
trache
Simulator training for failed intubation
GA for caesarean section
No
of fa
ilure
s
Goodwin & French IJOA 2001
1st simulation
2nd simulation
Role of Consultant Anaesthetists
Service
Antenatal planning
Back up for failed intubation
Skills – Awake intubation, Alternative techniques
Training
Good role models – safe GA/failed intubation drills
Educating others – obstetricians, midwives
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
80

We cannot eliminate general anaesthesia for obstetrics
We cannot eliminate failed intubation
Safe outcome is ensured by appropriate management of
Anticipated and unanticipated difficult airway
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
81

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 6: Caesarean Section Maternal haemodynamic monitoring in obstetric anaesthesia
Professor Rob Dyer Professor & Second Chair, Department of Anaesthesia, University of Cape Town
The physiological changes of pregnancy, including an initial gradual increase in cardiac output, followed by the development of increasing aortocaval compression in the third trimester, as well as co-morbidities such as preeclampsia, have generated considerable research into maternal haemodynamics. The use of the pulmonary artery catheter allowed a better understanding of the physiology of the healthy parturient1 and the haemodynamics of preeclampsia, including the effects of epidural analgesia in labour.2 Early use of dye dilution techniques gave clinicians insight into the haemodynamic changes during spinal anaesthesia for caesarean section.3 More recently, minimally invasive pulse wave form analysis has been used in the assessment of haemodynamic changes during this procedure.4,5 Heart rate and blood pressure are appropriately used as surrogate markers of maternal cardiac output in all routine obstetric anaesthesia deliveries, and in most of the clinically valuable obstetric anaesthesia research to date. Intra-arterial monitoring provides a useful indicator of beat by beat changes in the unstable patient. During regional anaesthesia for caesarean delivery, maintenance of baseline maternal blood pressure, using phenylephrine, has been shown to produce the closest to zero umbilical arterial base deficit, the currently accepted short-term marker of neonatal wellbeing.6 This is despite the fact that phenylephrine reduces maternal cardiac output. The effectiveness of phenylephrine may be related to the limited susceptibility of the uterine artery to the vasoconstrictive effects of alpha agonists in advanced pregnancy.6 However, the maximum change in cardiac output has been shown to correlate better with uteroplacental blood flow than upper arm blood pressure.7 The maintenance of blood pressure and maternal cardiac output are therefore both important for maternal safety and comfort, and fetal wellbeing. For clinical management and research purposes, there has been an increasing awareness of the potential complications of invasive monitoring. In addition the importance of the effects of fluid and vasopressor administration on flow rather than pressure, is now recognised in the non-obstetric population. In particular, central venous pressure and pulmonary
wedge pressure are unlikely to predict the response to fluid administration, and pulse pressure variation and stroke volume variation may be better indicators of fluid resuscitation.8 These factors have led to a resurgence of interest in minimally invasive techniques of cardiac output monitoring. Non-invasive methods of cardiac output measurement used in obstetric anaesthesia, have provided valuable information on maternal and fetal wellbeing and haemodynamics in the critical care setting and during regional anaesthesia for caesarean section. These techniques include transthoracic echocardiography,2 transoesophageal echocardiography, transoesophageal, suprasternal aortic7,9 and uterine artery Doppler ultrasound techniques, and transthoracic and whole body electrical bioimpedance.10 All these methods have disadvantages, including expense, the requirement for user education, movement artefact, and in the case of bioimpedance techniques, the potential for inaccuracy in terms of absolute cardiac output values in advanced pregnancy and in the presence of increased lung water. None provide beat by beat data. Arterial pulse wave form analysis methods are attractive to the obstetric anaesthetist, in that they provide beat by beat assessment of cardiac output, and could be used both in critical care monitoring (e.g. in complicated severe preeclampsia) and for research purposes (e.g. the effects of fluids, vasopressors and oxytocic drugs), in the labouring patient or during anaesthesia. Of crucial importance in the acceptance of these monitors are the precision and reliability of the employed algorithm in following changes in cardiac output (including in the setting of rapidly changing systemic vascular resistance), and the ability to predict ventricular preload response, through the derivation of fluid responsive parameters. When interpreting published data, usually involving Bland and Altman’s recommendation for the use of bias and precision statistics, the reader should bear in mind that in view of the +/- 10-20% accuracy of thermodilution, limits of agreement of up to +/- 30% between the new and the accepted technique are generally regarded as acceptable.11 Currently commercially available methods consist of calibrated devices (LiDCOplus [LiDCO, Cambridge, United Kingdom] and
82

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 PiCCOplus [Pulsion Medical Systems, Munich, Germany]), and the uncalibrated Vigileo monitor (Edwards Lifesciences, Irvine, California).12 The PulseCO algorithm employed in the LiDCOplus monitor requires only a peripheral arterial and venous line and calculates stroke volume by analysis of the arterial blood pressure trace using a pulse power algorithm. This a three step process, involving initial transformation (compliance correction) of the arterial pressure into a volume-time wave form, followed by derivation of a nominal stroke volume and beat duration, employing autocorrelation, and finally calibration/scaling of the stroke volume with a lithium indicator dilution curve measurement of cardiac output, which is comparable to intrapulmonary thermodilution.12 It is important to note that the PulseCO pulse wave form algorithm described in 2001 used the first harmonic of the blood pressure wave form and related this mathematically to the cardiac output; this bears no relation to the commercially employed algorithm.13 Despite concerns regarding the ability of this method to respond to acute changes in SVR, it is noteworthy that this original algorithm was employed successfully to examine the detailed time based effects of a 5ug IV dose of epinephrine.14 Several publications have shown the ability of the subsequently commercially employed pulse power algorithm to trend changes in stroke volume accurately, avoiding the requirement for frequent re-calibration.15,16 Three studies have demonstrated acceptable agreement11 between the LiDCOplus-derived cardiac output and Lithium dilution16,17, or thermodilution18 in the setting of systemic vascular resistance changes of up to 200%. Only one published investigation in obstetric anaesthesia has examined cardiac output trend changes during spinal anaesthesia for caesarean section in patients with severe preeclampsia, as well as acute responses to phenylephrine and oxytocin.19 This study elicited considerable debate20, but current knowledge suggests that this monitor is valuable in the setting of acute changes in systemic vascular resistance. Recently this technology has been used to investigate the optimal combination of spinal bupivacaine and sufentanil, and phenylephrine infusion, in order to preserve optimal maternal haemodynamics.4 A small dose of bupivacaine and opioid, in combination with a low dose phenylephrine infusion, gave the best haemodynamic stability in the 4 combinations studied, with minimal maternal symptoms. Induction of spinal anaesthesia was associated with a decrease in blood pressure and, interestingly, an increase in cardiac output. In a recent randomised trial, cardiac output changes were estimated by transthoracic
bioimpedance changes and the LiDCOplus monitor in the same patient, in order to corroborate the data.5 Once again, spinal anaesthesia for elective caesarean section was associated with a reduction in systemic vascular resistance, and a partial compensatory increase in cardiac output. A bolus of 80µg phenylephrine administered in response to a 20% decrease in mean arterial pressure, reduced maternal cardiac output (but not below baseline values), and decreased cardiac output when compared with 10mg ephedrine. Cardiac output changes correlated with heart rate changes following vasopressor administration, emphasizing the importance of heart rate as a surrogate indicator of cardiac output. Co-administered phenylephrine obtunded hemodynamic responses to oxytocin. Using suprasternal Doppler flow measurements, a dose dependent reduction in cardiac output has been demonstrated, in parturients receiving an infusion of phenylephrine at 100µg per minute during SA for CS.21 These studies suggest that doses of phenylephrine which induce increases in blood pressure to above baseline values, and sinus bradycardia, result in depression of maternal cardiac output, and should be avoided. The LiDCOplus monitor has recently been shown to predict fluid responsiveness in mechanically ventilated patients by providing reliable measurements of pulse pressure variation and stroke volume variation.8 This attribute could be useful in the management of patients with complicated severe preeclampsia, in whom pulmonary artery catheterisation has a significant complication rate.2 The recently developed PiCCO system employs an algorithm which analyses the systolic component of the arterial wave form. The calibration method, transpulmonary thermodilution, requires cannulation of a proximal artery and a central vein, which is problematic for obstetric anaesthesia research, but may be feasible for critical care management. An acute rise in systemic vascular resistance induced by phenylephrine, has resulted in increased bias when compared with thermodilution in cardiac surgical patients.22 The Vigileo monitor uses a specialised arterial transducer which is connected to a monitor that samples the pressure recording at a frequency of 100Hz, and analyses wave form characteristics by a multivariate polynomial equation. Patient demographic characteristics are used to estimate inter-patient variability and thereby reduce bias. It does not require calibration, and any artery can be used. There is currently little published comparative data. Moderate accuracy has been shown in comparisons with thermodilution. However, the administration of
83

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 phenylephrine has been shown to increase the cardiac output measurement using the Vigileo monitor when transpulmonary thermodilution showed a decrease in output, in cardiac surgical patients23. This would suggest that the monitor may not be suitable for the study of rapid haemodynamic changes associated with obstetric anaesthesia. Pulmonary artery catheterisation has only a limited application in the management of complex cardiac defects or multiple organ failure in the parturient. Less invasive cardiac output monitors will have an important role to play, both in the haemodynamic management of parturients with co-morbidities, and in research into the haemodynamics of healthy and critically ill mothers. The prediction of fluid responsiveness using clinical assessment and pulse wave form monitors, may prove to be of greater value than the measurement of filling pressures. Heart rate and noninvasive blood pressure measurement, as well as communication with the awake patient during regional anaesthesia, remain the most important monitors for the obstetric anaesthetist. It is however also important that the anaesthetist is constantly mindful of the effect of his/her interventions on both flow and pressure. In addition, research in the area of cardiac output contributes to a knowledge of the mechanism of spinal anaesthesia, and to the correct choice of vasopressors when the patient is haemodynamically unstable. References
1. Clark SL, Cotton DB, Lee W, Bishop C, Hill T, Southwick J, Pivarnik J, Spillman T, DeVore GR, Phelan J: Central haemodynamic assessment of normal term pregnancy. Am J Obstet Gynecol 1989; 161: 1439-42
2. Young P, Johanson R: Haemodynamic, invasive and echocardiographic monitoring in the hypertensive parturient. Best Pract Res Clin Obstet Gynaecol 2001; 15: 605-22
3. Ueland K, Gills RE, Hansen JM: Maternal cardiovascular dynamics. I. Cesarean section under subarachnoid block anaesthesia. Am J Obstet Gynecol 1968; 100: 42-54
4. Langesaeter E, Rosseland LA, Stubhaug, A: Continuous invasive blood pressure and cardiac output monitoring during cesarean delivery. A randomized double blind comparison of low dose versus high dose spinal anaesthesia with intravenous phenylephrine or placebo infusion. Anesthesiology 2008; 109: 856-863.
5. Dyer RA, Reed AR, van Dyk D, Arcache MJ, Hodges O, Lombard CJ, Greenwood J, James MF: Hemodynamic effects of ephedrine, phenylephrine and the co-administration of phenylephrine and oxytocin during spinal anesthesia for elective cesarean delivery. Anesthesiology 2009; 111: 753-765.
6. Macarthur A RE: Obstetric anaesthesia controversies: vasopressor choice for postspinal hypotension during cesarean delivery. International Anesthesiology Clinics 2007; 45: 115-32
7. Robson SC, Boys RJ, Rodeck C, Morgan B: Maternal and fetal haemodynamic effects of spinal and extradural
anaesthesia for elective caesarean section. Br J Anaesth 1992; 68: 54-9
8. Belloni L, Pisano A, Natale A, Piccirillo MR, Piazza L, Ismeno G, De Martino G: Assessment of fluid-responsiveness parameters for off-pump coronary artery bypass surgery: a comparison among LiDCO, transesophageal echochardiography, and pulmonary artery catheter. J Cardiothorac Vasc Anesth 2008; 22: 243-8
9. Bray JK, Fernando R, Patel NP, Columb MO: Suprasternal Doppler estimation of cardiac output: standard versus sequential combined spinal epidural anaesthesia for cesarean delivery. Anesth Analg 2006; 103: 959-64
10. Tihtonen K, Koobi T, Yli-Hankala A, Huhtala H, Uotila J: Maternal haemodynamics in pre-eclampsia compared with normal pregnancy during caesarean delivery. BJOG 2006; 113: 657-63
11. Critchley LA, Critchley JA: A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J Clin Monit Comput 1999; 15: 85-91
12. Morgan P, Al Subaie N, Rhodes A: Minimally invasive cardiac output monitoring. Curr Opin Crit Care 2008; 14: 322-6
13. Linton N: Pulse contour analysis to estimate cardiac output. Can J Anaesth 2006; 53: 850-1
14. Linton NW, Linton RA: Haemodynamic response to a small intravenous bolus injection of epinephrine in cardiac surgical patients. Eur J Anaesthesiol 2003; 20: 298-304
15. de Wilde RB, Schreuder JJ, van den Berg PC, Jansen JR: An evaluation of cardiac output by five arterial pulse contour techniques during cardiac surgery. Anaesthesia 2007; 62: 760-8
16. Pittman J, Bar-Yosef S, SumPing J, Sherwood M, Mark J: Continuous cardiac output monitoring with pulse contour analysis: a comparison with lithium indicator dilution cardiac output measurement. Crit Care Med 2005; 33: 2015-21
17. Hallowell GD, Corley KT: Use of lithium dilution and pulse contour analysis cardiac output determination in anaesthetized horses: a clinical evaluation. Vet Anaesth Analg 2005; 32: 201-11
18. Yamashita K, Nishiyama T, Yokoyama T, Abe H, Manabe M: Effects of vasodilation on cardiac output measured by PulseCO. J Clin Monit Comput 2007; 21: 335-9
19. Dyer RA Piercy JL, Reed AR, Lombard CJ, Schoeman LK, James MF: Haemodynamic changes associated with spinal anaesthesia for cesarean section in severe preeclampsia. Anesthesiology 2008; 108: 802-11
20. Pauca AL: Pressure wave analysis is useful to understand the pathophysiology of preeclampsia but perhaps not the rapid changes during cesarean delivery. Anesthesiology 2008; 108: 773-4
21. Stewart A, Fernando R, McDonald S, Hignett R, Jones T, Columb M, Abdul-Kadir R: Dose dependent effects of phenylephrine for elective caesarean section under spinal anaesthesia: implications for the compromised fetus? International Journal of Obstetric Anaesthesia 2008; 17: S1-9.
22. Rodig G, Prasser C, Keyl C, Liebold A, Hobbhahn J: Continuous cardiac output measurement: pulse contour analysis vs thermodilution technique in cardiac surgical patients. Br J Anaesth 1999; 82: 525-30
23. Lorsomradee S, Lorsomradee S, Cromheecke S, De Hert SG: Uncalibrated arterial pulse contour analysis versus continuous thermodilution technique: effects of alterations in arterial waveform. J Cardiothorac Vasc Anesth 2007; 21: 636-43
84

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 6: Caesarean Section Spinal anaesthesia for caesarean section – dose, position & baricity Marc Van de Velde, MD, PhD. Professor of Anesthesiology, University Hospitals Gasthuisberg, Leuven, Belgium
Introduction The spread of local anaesthetic solution within the spinal space can be modified by various factors or depends on various non-modifiable factors which need to be taken into consideration when designing an optimal neuraxial block strategy. The present manuscript reviews some of these factors in parturients undergoing a Caesarean delivery. When local anaesthetic solutions are injected into the subarachnoid space the uptake of the anaesthetic determines which neuronal functions are affected, while the duration of the effect is determined by the elimination process of the local anaesthetic solution. The distribution of the anaesthetics within the spinal space determines the extent of altered neuronal function. To evaluate the extent of distribution ideally we should measure cerebrospinal fluid concentration of local anaesthetic. This is however in humans impractical and unethical to do. Therefore the distribution is measured by determining the spinal segmental level of anaesthesia.
To establish the spinal segmental level of anaesthesia various methods can be used: cold, pinprick or touch, but also heat and transcutaneous electrical nerve stimulation (1,2). Block to cold sensation extends usually higher then pinprick which extends usually higher then block to touch. Although the mean difference between touch and cold is 3 segments, while the mean difference between touch and pinprick is 2 segments (1). However large patient variability exists and many authors conclude that pinprick and cold are incapable to reliably detect a sufficient anaesthetic block (1,2,3).
Many factors may influence the distribution of local anaesthetic in the intrathecal space (table 1) (4). In the present manuscript, we will review some of these factors in relationship to spinal anaesthesia for Caesarean section. Height and weight Greene noted that common sense and clinical experience tell us that patient height and weight influence the distribution of local anaesthetic (4). However, the data supporting this is limited. McCulloch et al. reported in non-obstetric patients that increased weight and obesity increased block
height (5). But in obstetric patients several investigations could not confirm these results.
Norris published two studies in which he administered 12 or 15 mg heavy bupivacaine intrathecally for Caesarean section and noted no relationship between block height and patient height, weight, vertebral column length and body mass index (BMI) (6,7). Ekelof more recently confirmed this using plain bupivacaine (8). However in an even more recent trial, Harten and co-workers compared a fixed dose of heavy bupivacaine with a weight and height adjusted dose (9). These authors however observed significant differences between the two groups, indicating that height and weight do play a role. With the adjusted dose onset time was longer, there was less hypotension and there were fewer patients having a segmental block higher than T1. In contrast to previous studies, they used considerably lower doses. Perhaps this can explain why eight/height adjusted doses performed better then a fixed dose. More studies are needed to determine the need to adjust the dose to weight or height when low bupivacaine doses are administered.
It is well known that due to pregnancy the lordotic curvature of the spinal column is accentuated (4). This results in a reduced cephalad spread of the local anaesthetic solution due to pooling of the solution in the deepest part of the S-shaped curve. The position in which the patient is during spinal puncture and the position during induction of the block also are factors that influence anaesthetic spread. Of course anaesthetic baricity influences the effect of positioning. Several studies have been performed in parturients scheduled for Caesarean section evaluating the effect of the sitting, lateral or Oxford positions. Other studies looked at the effect of left lateral versus right lateral positioning, while other studies evaluated whether a positional variation after the puncture but during establishment of the block played a role. It is difficult to draw firm conclusions since the literature is confusing and contradictory (10,11). However some suggestions can be made. Initiation of spinal anaesthesia in the left or right lateral position does not affect local anaesthetic spread (12,13). With hyperbaric solutions the sitting position has the following effects: the block extends less cephalad, produces less
85

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Table 1: factors influencing distribution of local anaesthetic solution in the cerebrospinal fluid (CSF).
Patient characteristics Age Height Weight Gender Intra-abdominal pressure Spinal column anatomy Position Technique of injection Site of injection Direction of needle Rate of injection Barbotage Diffusion characteristics of CSF Composition Circulation Volume Pressure Density Characteristics of anaesthetic solution Baricity Dose Concentration Volume injected Adjuvants Modulation of the epidural space Epidural volume extension (EVE) Combined spinal epidural (CSE)
Modified according to Greene. Anesth Analg 1985; 64, 715 – 730.
86

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 hypotension, better umbilical artery pH values, more epidural supplementation is required (when CSE with low spinal doses is performed), the block is technically easier to perform and onset time of anaesthesia is slightly prolonged (14,15). These effects are especially noted when lower spinal doses (< 9 mg) are used and become less clear or more variable when higher doses are used. Also experience of the anaesthetist with the position plays an important role in the eventual effects of the position.
Although Greene suggested that needle direction and spinal needle opening should influence the block height (4), no clinical studies in parturients could actually confirm these hypotheses. Massé et al. studied 40 parturients undergoing elective Caesarean section under spinal anaesthesia with a Whitacre spinal needle using hyperbaric bupivacaine (16). In 20 patients the orifice of the needle was directed cephalad, whilst in the other 20 patients the orifice pointed caudad. These investigators noted no difference between the groups.
Epidural volume extension (EVE) is the injection of an epidural solution (saline or local anaesthetic) into the epidural space with the intention to extend the block height of a spinally injected local anaesthetic solution (17). Most studies have demonstrated that, if EVE is performed within the first 5 – 10 minutes after the spinal injection, the upper dermatomal spread of the local anaesthetic can be increased by 1 to 5 dermatomes (17). The mechanisms involved to explain these effects remain theoretical and include a direct passage of epidural local anaesthetic through the dural hole, neurtralisation of the negative epidural pressure due to the Tuohy needle inertion and increased epidural pressure due to the injection of epidural solution resulting in a reduced CSF volume.
Local anaesthetic baricity is the ratio of local anaesthetic density and cerebrospinal fluid density. CSF density decreases in pregnancy (18). Most “plain” local anaesthetics are isobaric or even slightly hyperbaric at room temperature, but quickly become hypobaric following intrathecal injection due to a decreasing baricity with increasing temperature (19,20). If one discusses the effect of baricity one cannot see this free from posture while injecting. Many studies are flawed because they only used one position and compared local anaesthetics of different baricity. Hallworth et al. however performed an excellent study randomising 150 patients undergoing CSE anaesthesia for Caesarean section to 6 study groups (21). Half of the patients underwent CSE anaesthesia whilst seated, 75 patients received a CSE whilst in the right lateral position. They concluded that in the lateral position
baricity did not influence local anaesthetic spread, whilst in the sitting position the block spread higher with decreasing baricity. They and other authors also concluded that hypobaric solutions were much more unpredictable and resulted in more hypotension (21,22).
Dose is also an important determinant in the clinical effects of a spinal anaesthetic for C-section. Several authors have determined the full dose-response relationship of bupivacaine with opioids for spinal anaesthesia for Caesarean section. Significantly different results were obtained. Ginosar et al. and Carvalho et al. noted that the ED95 was > 11 mg, whilst Roofthooft et al. observed an ED95 of < 9 mg (23,24,25). These differences can be explained by differences in study population and study design, but emphasize that clinical practice and local experience is probably more important than an exact dose ! However, what is important to note is that with low dose spinal anaesthesia (< 9 mg or < 7.5 mg) bupivacaine, less hypotension occurs as was nicely summarized in a recent review (26). However, all authors agree that when low intrathecal doses are used, they should be administered as part of CSE technique. Conclusions Many factors influence the spread of the spinal block. Often the literature is confusing and contradictory. An important reason is that each and every factor is directly influenced by many of the other factors and by physician experience with a certain technique. Some conclusion can however be drawn: 1) Hyperbaric bupivacaine seems to give a more controllable and predictable block then is/hypobaric solutions; 2) The sitting position, especially with hyperbaric solutions, results in less hemodyamic perturbations; 3) Large variability exists in the literature concerning the ED95 dose of bupivacaine for C-section. Probably local practice and study design can account for these differences. However, low dose spinal anaesthesia has repeatedly been shown to provide effective anaesthesia conditions with limited duration. Therefore it is adviced that when a low dose technique is used, a back-up epidural catheter would be placed; 4) Low dose spinal anaesthesia results in less hemodynamic side-effects. References
1. Russell IF. A comparison of cold, pinprick and touch for assessing the level of spinal block at caesarean section. IJOA 2004; 13, 146 – 152.
2. Russell IF. At caesarean section under regional anaesthesia, it is essential to test
87

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
sensory block with light touch before allowing surgery to start. IJOA 2006; 15, 294 – 300.
3. Russell IF. Levels of anaesthesia and intraoperative pain at caesarean section under regional block. IJOA 1995; 4, 71 – 77.
4. Greene NM. Distribution of local anesthetic solutions within the subarachnoid space. Anesth Analg 1985; 64, 715 – 730.
5. McCulloch WTD, Littlewood DG. Influence of obesity on spinal analgesia with isobaric 0.5% bupivacaine. Brit J Anaesth 1986; 58, 612 – 614.
6. Norris MC. Height, weight, and the spread of subarachnoid hyperbaric bupivacaine in the term parturient. Anesth Analg 1988; 67, 555 – 558.
7. Norris MC. Patient variables and the subarachnoid spread of hyperbaric bupivacaine in the term parturient. Anesthesiology 1990; 72, 478 – 482.
8. Ekelof NP, Jensen E, Poulsen J, Reinstrup P. Weight gain during pregnancy does not influence the spread of spinal analgesia in the term parturient. Acta Anaesthesiol Scand 1997; 41, 884 – 887.
9. Harten JM, Boyne I, Hannah P, Varveris D, Brown A. Effects of a height and weight adhusted dose of local anaesthetic for spinal anaesthesia for elective Caesarean section. Anaesthesia 2005; 60, 348 - 353.
10. Rucklidge MWM, Paech MJ, Yentis SM. A comparison of the lateral, Oxford and sitting positions for performing combined spinal-epidural anaesthesia for elective Caesarean section. Anaesthesia 2005; 60, 535 – 540.
11. Proposer: Russell IA; Opposer: Dresner M. Routine use of the sitting position for spinal anaesthesia should be abandoned in obstetric practice. IJOA 2009; 17, 343 – 349.
12. Law ACS, Lam KK, Irwin MG. The effect of right versus left lateral decubitus positions on induction of spinal anesthesia for Cesarean delivery. Anesth Analg 2003; 97, 1795 – 1799.
13. Kapur D, Grimsehl K. A comparison of cerebrospinal fluid pressure and block height after spinal anaesthesia in the right and left lateral position in pregnant women undergoing Caesarean section. Eur J Anaesthesiol 2001; 18, 668 – 672.
14. Coppejans HC, Hendrickx E, Goossens J, Vercauteren MP. The sitting versus right lateral position during combined spinal epidural anesthesia for Cesarean delivery: Block characteristics and severity of hypotension. Anesth Analg 2006; 102, 243 – 247.
15. Inglis A, Daniel M, McGrady E. Maternal position during induction of spial anaesthesia for Caesarean section. Anaesthesia 1995; 50, 363 – 365.
16. Massé E, Drolet P, Girard M. Direction of injection does not affect the spread of spinal bupivacaine in parturients. Can J Anaesth 1997; 44, 816 – 819.
17. McNaught AF, Stocks GM. Epidural volume extension and low-dose sequential combined spinal-epidural blockade: two ways to reduce spinal dose requirement for caesarean section. IJOA 2007; 16, 346 – 353.
18. Richardson MG, Wissler RN. Density of lumbar cerebrospinal fluid in pregnant and non-pregnant humans. Anesthesiology 1996; 85, 326 – 330.
19. Heller AR, Zimmermann K, Rossel T, Koch T, Litz RJ. Modifying the baricity of local anesthetics for spinal anesthesia by temperature adjustment. Anesthesiology 2006; 105, 346 – 353.
20. Richardson MG, Wissler RN. Densities of dextrose-free intrathecal local anesthetics, opioids, and combinations measured at 37°C. Anesth Analg 1997; 84, 95 – 99.
21. Hallworth SP, Fernando R, Columb MO, Stocks GM. The effect of posture and baricity on the spread of intrathecal bupivacaine for elective Cesarean delivery. Anesth Analg 2005; 100, 1159 – 1165.
22. Vercauteren MP, Coppejans HC, Hoffmann VL, Saldien V, Adriaensen HA. Small-dsoe hyperbaric versus plain bupivacaine during spinal anesthesia for Cesarean section. Anesth Analg 1998; 86, 989 – 993.
23. Ginosar Y, Mirikatani E, Drover DR, Cohen SE, Riley ET. ED50 and ED95 of intrathecal hyperbaric bupivacaine coadministered with opioids for cesarean delivery. Anesthesiology 2004; 100, 676 – 682.
24. Carvalho B, Durbin M, Drover DR, Cohen SE, Ginosar Y, Riley ET. The ED50 and ED95 of intrathecal isobaric bupivacaine with opioids for cesarean delivery. Anesthesiology 2005; 103, 606 – 612.
25. Roofthooft E, Dreelinck R, Dubois J, Berends N, Van de Velde M. Determination of the dose response relationship of spinal bupivacaine, levobupivacaine and ropivacaine combined with sufentanil during anaesthesia for caesarean section. IJOA 2007; 16, S6.
26. Roofthooft E, Van de Velde M. Low dose spinal anaesthesia for Caesarean section to prevent spinal induced hypotension. Curr Opinion Anaesthesiol 2008; 21, 259 – 262.
88

Session 6: Caesarean Section The obese parturient Dr Wiebke Gogarten Consultant Anaesthetist & Head, Department of Anaesthesiology, Intensive Care and Pain Medicine, Harlaching Hospital, Municipal Hospitals of Munich, Germany
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
89

2003-2005 overweight or obese 52%
2000-2002 overweight or obese 30%
29.11.2009 7
Maternal Mortality During PregnancyDeaths per 100,000 Life Births: UK 2003-2005
www.cemach.org.uk/publications/wmd2003_2005
0 5 10 15 20 25 30 35 40 45
Cardiac causes
Thromboembolism
Preeclampsia
Sepsis
Psychiatric reasons
Postpartum hemorrhage
Early in pregnancy 14
14
18
18
18
41
48
Amniotic fluid embolism 17
Obesity in Pregnancy and Use of Health CareResources
Chu et al., N Engl J Med 2008; 358; 1444-1453
Obesity in Pregnancy
High risk pregnancy
Increased risks
• limited cardiac and pulmonary reserve
• sleep apnea
• increased gastroesophageal reflux
• preeclampsia
• recurrent miscarriage
• fetal macrosomia
• Caesarean delivery
• postpartum hemorrhage
• wound infections
• thromboembolism
• hypoxemia
•
Obesity: maternal and fetal outcome
Callaway et al., Med J Aust 2006; 184: 56-59
BMI > 30 kg/m2 BMI > 40 kg/m2
Gestational Weight Gain and Pregnancy Outcomes in Class III Obese Women
Kiel et al., Obstet Gynecol 2007; 110: 752-758
Weight Gain Suggestions in Obese Parturients
Class I obesity gain 10 - 25 lb (4.5 -11 kg)
Class II obesity gain 0 - 9 lb (0 - 4 kg)
Class III obesity loose 0-9 lb (0 - 4 kg)
Kiel et al., Obstet Gynecol 2007; 110: 752-758
Maternal Obesity and Congenital Cardiac Defects
� Increased rate of congenital heart defects (atrial and ventricular septal defects)
� All defects
� BMI > 29 kg/m2 OR 1.18 (1.09 - 1.27)
� BMI > 35 kg/m2 OR 1.41 (1.22 - 1.64)
Cedergren & Källen, Obes Res 2003; 11: 1065-1071
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
90

Severe Obesity and Neural Tube Defects
Rasmussen et al., Am J Obstet Gynecol 2008; 611-618 Schäfer-Graf et al., Diabetes Care 2005; 28: 1745-1750
Maternal Gestational Diabetes and Childhood Obesity
Maternal BMI > 30 kg/m2
obesity in 42% of children
*
*
Maternal Weight and Failure of Epidurals
Dresner et al., BJOG 2006; 113: 1178-1181
Retrospective analysis 1997-2005, 13299 epidurals
Subcutaneous Catheter Movement During Labor withTight Catheter Fixation
Carrie & Russel, Carrie & Russel, AnaesthesiaAnaesthesia 2000; 55: 12312000; 55: 1231--12331233
BMI and Depth of the Epidural Space
2009 parturients
1995 with normal Tuohyneedle
14 with longer Tuohy needle(13 cm)
ClinkscalesClinkscales et al., et al., IntInt J J ObstetObstet AnesthAnesth 2007; 16: 3232007; 16: 323--327327
BMI 26.3 kg/m2
block height T 10
BMI 39.5 kg/m2
block height T 8
BMI and Local Anaesthetic Requirements
Panni et al., Br J Anaesth 2006; 96: 106-110
Spinal Anaesthesia and Maternal Vital Capacity
Von Ungern-Sternberg et al., Anaesthesia 2004; 59: 743-749
8 anaesthesia-related deaths (2.3% of all maternal deaths)
6 parturients with severe obesity
2 anesthsia nurses (supervised by obstetrician)
6 anesthesia nurses (supervised by anesthesiologist, only in 2
cases present)
4 x cardiac arrest under spinal anesthesia
5 x hypoventilation, airway obstruction after anesthesia
2 x cardiomyopathy, myocardial infarction
lack of standard monitoring postoperatively (pulseoximetry)
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
91

Laryngoscopy and Morbid Obesity: Sniffingversus Ramped Position
Collins et al., Obes Surg 2004; 14: 1171-1175
Comparison of Different Videolaryngoscopes in Morbid Obesity (BMI 43 kg/m2)
Maassen et al., Anesth Analg 2009; 109: 1560-1565
Average intubation times
Glidescope 33 ± 18 sec
Storz 17 ± 9 sec
McGrath 41 ± 25 sec
Gastric Emptying in Obese Parturients
50 ml water300 ml water
Gastric emptying (T1/2)
23 ± 11 min (300 ml)32 ± 15 min (50)
Wong et al., Anesth Analg 2007; 105: 751-755
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
92

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 6: Caesarean Section Managing pain & distress during caesarean section under regional anaesthesia Dr Geraldine O’Sullivan Consultant Anaesthetist, Guy's & St Thomas' Hospitals, London
Pain. An unpleasant feeling caused by injury Distress. Acute physical or mental suffering Pain during caesarean section, which has not been appropriately managed, is one of the commonest reasons for complaints and litigation in obstetric anaesthesia. From a woman’s perspective a caesarean section is never ‘sensation free’; it should however never be painful. Therefore at the pre-operative visit (or in the operating theatre in the event of an emergency caesarean section) the anaesthetists must carefully explain to the woman that her caesarean section will be ‘pain free’ but not ‘sensation free’. If these facts are not carefully explained the more anxious and nervous woman may believe that her anaesthesia has failed. A complaint of pain (as opposed to discomfort) during caesarean section requires immediate action by the anaesthetist. If the pain is severe, this fact will probably be immediately apparent to all who are present in the operating theatre!! If the pain is less severe but is causing distress to the mother it can be helpful to ask her to rate her pain on a numerical scale, e.g. 0 - 10. In either event the anaesthetist must ask the surgeon to stop operating and offer the woman the option of continuing her surgery under general anaesthesia. If she accepts this option, general anaesthesia should be induced immediately using a rapid sequence induction. Surgery can re-commence once the airway has been secured with a cuffed endotracheal tube. If the pain is severe it is unlikely that the woman will refuse the offer of a general anaesthetic. However in some situations, the mother may initially refuse a general anaesthetic. In this instance the anaesthetist must carefully record that general anaesthesia was offered and refused. Every effort must then be directed at relieving the pain. It will often be appropriate to make further offers of general anaesthesia to the woman. The times of these offers and the woman’s response must be recorded. This documentation may help deal with complaints and even legal action over the forthcoming months.
Why does regional anaesthesia fail during caesarean section? 1. Failure (or apparent failure) to check the level of anaesthesia. If an anaesthetist has not recorded the level of anaesthesia on the anaesthetic chart, any subsequent complaints about inadequate anaesthesia will be indefensible
2. Inadequate block assessment The appropriate level of anaesthesia for a caesarean section and its method of assessment, has been one of the ongoing debates in obstetric anaesthesia. However, loss of cold sensation to T4 and touch to T5 usually implies an adequate level of anaesthesia. The lower level of anaesthesia should also be assessed, e.g. was the mother completely pain free when the urinary catheter was inserted? The level of motor block should also be assessed, if the women is fully mobile, the block is probably inadequate! Warm dry feet indicate that a sympathetic block has been achieved, and without which surgery should not be allowed to commence. Should surgery ever commence before an adequate level of anaesthesia has been achieved? Logic might suggest that the answer to this question would always be negative. However some bending of the rules can be permitted in the event of an emergency caesarean section in a woman who has had very effective epidural analgesia during labour. If such a woman requires an emergency section and the anaesthetist has satisfactorily demonstrated to the woman and him/herself that the level of anaesthesia is rising satisfactorily; then it might, in the event of severe fetal distress and after a thorough explanation to the woman, be permissible to make the skin incision before the block has reached T4 to cold. Failure of Anaesthesia during caesarean section
Spinal vs Epidural anaesthesia Local anaesthetic and opioid are required to produce adequate anaesthesia for both spinal and epidural anaestesia for caesarean section. In the UK 0.5% heavy bupivacaine is the local anaesthetic of choice for spinal anaesthesia whilst fentanyl or preferably diamorphine are the most appropriate opioids.
93

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 Bupivacaine 0.5%, L-Bupivacaine 0.5% and Ropivacaine in combination with opioids are all effective agents for epidural analgesia. Subarachnoid anaesthesia produces a denser block than epidural anaesthesia and complaints of discomfort are therefore more commonly associated with epidural anaesthesia. Approximately 66% of caesarean sections in the UK are performed as emergency procedures during labour. Many of these women will already have an epidural catheter in-situ for analgesia in labour. If the analgesia during labour has not been 100% satisfactory the epidural must not be topped-up for surgery. Inadequate analgesia can rarely be converted to satisfactory anaesthesia. In this situation the catheter must be removed and the surgery should be performed under spinal anaesthesia. Treatment of pain/distress during caesarean section
1. Epidural top-up, if appropriate, e.g. 0.75% ropivacaine with either fentanyl 50-100.
2. IV fentanyl 50-100µg 3. 50:50 mixture oxygen and nitrous oxide 4. IV Ketamine 10-20mg 5. IV midazolam 1–1.5mg or Propofol 10-
20mg. These drugs will not relieve pain, but ally anxiety.
6. General anaesthesia will be necessary if pain persists or if the woman requests to be put to sleep
References Russell IF. Assessing the block for caesarean section. Int J Obstet Anesth 2001:10:83 Russell IF. Level of anaesthesia and intraoperative pain at caesarean section under regional block. Int J Obstet Anesth 1995;4:71 Orbach-Zinger S et al. Risk factors for failure to extend labor epidural analgesia to epidural anesthesia for Caesarean section. Acta Anaes Scand 2006;50:793 Lucas DN. Extending low0dose epidural analgesia for emergency caesarean section – a comparison of three solutions. Anaesthesia 199; 54:1173
94

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 7: The Baby 1 The decision to deliver - the obstetrician's viewpoint Professor Andrew Shennan Professor of Obstetrics, Guy's & St Thomas' Hospitals, London
When to delivery a baby is far from a precise science. Operative intervention rates, particularly Caesarean Section, have escalated in recent decades, with little evidence of improvements in perinatal outcomes. Caesarean Section rates have more then doubled since the 1980s. Even the recent trend to staff labour wards with senior obstetricians has little impact on intervention rates. Increasing trends in maternal choice for Caesarean Section cannot account for this increase. So why has the intervention rates increased? The expectation of a normal baby is high in modern society, yet absolute risks of serious morbidity in childbirth remains relatively high compared to risks generally accepted in society: a 1:1000 risk of dying in labour is not accepted in other aspects of life (This is equivalent to x2 plans crashing each week leaving Heathrow). This is confounded by an inability to
accurately judge fetal wellbeing. For all the apparent sophistication of fetal monitoring, the obstetrician is in fact waiting for gross and serious abnormality resulting in detectable biophysical changes (acidosis influences the autonomic system for example, causing abnormal fetal heart rate changes.) The decision to deliver from the obstetricians viewpoint is therefore fraught with anxiety and uncertainty. Poor monitoring techniques result in frequent false positive decisions. The consequences of “getting it wrong” are substantial. There is only a small window of opportunity from acidosis resulting in detectable biophysical changes and neurological damage. This talk will outline the factors that inform the decision to deliver, including the uncertainty of current fetal monitoring.
95

Session 7: The Baby 1 Emergency caesarean section following the decision to deliver - the anaesthetist's viewpoint Dr Chris Elton Consultant Anaesthetist, University Hospitals of Leicester
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
96

Don’t Believe Everything You’re told!
• Davies and Collis 2007
• 20 patients had GA section for Grade 1 CS
• Assessment by independent consultants
• 4/20 actually needed GA
• 10/20 could have had regional
• 6/20 did not need a caesarean section• Davies and Collis IJOA 2007 S23
Decision to Delivery Timing
• 30 min rule was/is “pragmatic” standard
• International standard BUT 20 mins in Germany
• More likely to be met if patient in theatre
within 10 minutes of decision
• Availability of 2nd theatre
• Shortening decision to delivery does not reduce
admission to NICU or neonatal acidaemia• Tuffnell et al BMJ 2001 1330
• MacKenzie et al BMJ 2001 1334
• Dunphy et al J Obstet Gynecol 1991 211
Decision to Delivery Timing
• Decision to Delivery Times less than 20 mins
associated with INCREASED fetal compromise • (Hillemans et al 2005 Arch Gynecol Obstet 161-5)
• Analysis of Sentinel Study patients showed NO
difference provided DDI was less than 75
minutes• (Thomas et al BMJ 2004 665)
“Special Cases”
• Placental Abruption with Fetal Bradycardia
• 20 mins vs 30 mins (OR 0.44 0.22-0.86)
• Kayani et al 2003 BJOG 679-83
• Bleeding vasa/placenta praevia
• (Cord Prolapse with absent pulsation)
CESDI
CESDI-7th Annual Report (2000)
• 873 Intrapartum deaths in 1994-5 report
• 54 cases commented on anaesthesia (6.2%)
• 25 anaesthetic “delay” identified (2.9%)
• 19 GA, 3 Spinal, 3 Epidural
CESDI (2000)
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
97

CESDI (2000)
• No evidence in recent
reports of “rushed”
anaesthesia causing
death• SHO’s
• Equipment problems
• Women opted for GA
(2000-2)
• Drug Problems
• Postop care (2003-5)
• Are we getting the
balance right?
Strategies for Improving Outcome
• 1) Proactive approach in labour
• 2)In utero resuscitation
• 3) Expedite arrival in theatre
• 4) Use appropriate anaesthetic technique
What has to be done between
decision to deliver and delivery!-Tuffnell BMJ 2001 1330
• Informed consent:
Consent form signed
Intravenous access
Blood samples to be taken
Blood forms to be filled in
Bloods to laboratory
Intravenous fluids running
Premedication to be got from drug cupboard
Premedication drawn up
Premedication injected
Anaesthetist informed
Operating department assistant informed
Consultant to be informed
Anaesthetist to arrive
Operating department assistant to arrive
• Theatre to be set:
Scrub nurse to scrubPacks to be opened
Sutures to be opened
Monitoring to be discontinued
Intravenous lines to be secured
Fetal scalp clip to be removed
• Woman to be moved to theatre:
Woman to be moved on to theatre table
Spinal pack to be opened
Anaesthetist to scrub
Spinal drugs to be drawn up
Monitoring to be attached
• Spinal anaesthesia
• Wait for block to work:
Paediatrician to be present
Resuscitaire to be checked
Catheter
Shave
Surgeons to scrub
Skin preparation
Skin incision
Sheath incision
Peritoneum opened
Bladder reflected
Uterine incision
• Deliver baby
Proactive Anaesthetic Management
• Attend Ward Rounds to Identify those at risk
of intervention
• “87% of 360 consecutive emergency CS can be
anticipated”
• (Morgan et al 1990 BJOG 420)
• Insert epidural- Regular follow up!
• Communicate (Distress, FBS, Progress)
• Coordinate
Proactive Anaesthetic Management-
CEMACH 2007
• Identify those at risk of anaesthetic complications
• Preconception
• During Pregnancy
• During labour (ward rounds)
• Particular Concerns
• Obesity
• Recent migrants
» Language, Social Issues, Undiagnosed/Untreated Illness
• Sepsis
• Preeclampsia
• Occult Haemorrhage
In Utero Fetal Resuscitation
• Syntocinon off
• Position full left lateral (allows rapid spinal)
• Oxygen
• I.v. infusion of 1 litre crystalloid
• Low blood pressure: i.v. vasopressor
• Tocolysis: terbutaline 250 μg (s.c), glyceryltrinitrate 400 μg (metered aerosol doses)
• Monitor Fetus-It may get better!• Thurlow JA, Kinsella M IJOA 2002 11 105-16
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
98

What Anaesthetic Technique?
• GA associated with significantly shorter DDI
• GA associated with 16.7X (now 1.7) greater
risk of maternal death• Hawkins et al 1997 Anesthesiology 273-6
• Overwhelming preference for RA for maternal
safety-CEMACH
• Risk for fetus?
General Anaesthesia vs Spinal with
Fetal Distress
Dyer et al Anesthesiology 2003 99 561-9
• Seventy patients randomised to GA or SAB
• “Non reassuring” fetal heart trace
• Neonatal indicators worse in SAB group
GA SAB
Neonatal
umbilical BE
4.68 +/-
3.3
7.13 +/-
4.0
Umbilical
pH
7.23 7.20
Topping up an epidural
• Is this epidural working?
• How Much?-20mls, Divided doses?
• What mixture?
• Laevobupivacaine (10 mins)
• Ropivacaine (10 mins)
• Lignocaine/Adrenaline/Bicarbonate (7 mins)
• Fentanyl/Sufentanil only if not used in labour• Malhotra, Yentis Anaesthesia 2007 667
• Tortosa et al BJA 2003 532
S. Ohmura, M. Kawada, T. Ohta, K. Yamamoto, and T. Kobayashi Systemic
Toxicity and Resuscitation in Bupivacaine-, Levobupivacaine-, or Ropivacaine-
Infused Rats Anesth. Analg., September 1, 2001; 93(3): 743 - 748
• Beware complacency with “less toxic agents”
• Aspirate
• Give intravascular test dose (1mg/kg
lignocaine)• Michels, Lyons, Hopkins. Lignocaine test dose to detect intravenous injection. Anaesthesia 1995, 50, 211-3
• Intralipid should be available• http://www.aagbi.org/publications/guidelines/docs/latoxicity07.pdf
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
99

“Single Shot Spinal”
• 15-20 mins to surgical anaesthesia
• May be shorter with “rapid sequence spinal”(Scrutton, Kinsella)
– Theatre in left lateral
– IVI (obstetrician)
– Pre O2
– Prep, “No touch”
– No diamorphine• Scrutton, Kinsella IJOA 2003, 12, 144
General Anaesthesia
• Trained Anaesthetist/Skilled Anaesthetic Assistant
• Fully Equipped Theatre (Advanced airway aids)
• Antacids
• Pre O2 (Sat Up?/30 degree head up)
• TILT
• RSI/Cricoid
• Thiopentone(sleep dose)/Suxemethonium/ETT
• MODIFY in Preeclampsia/Cardiac/Cerebrovascular Disease
– Pressor response to intubation AND extubation
• Give an anaesthetic (ie 1.3 MAC)!
• Intubating Aids/Failed Intubation Drill
Conclusion
• High risk patients should be seen antenatally and in
labour
• Emergency CS can often be anticipated
• Retrospective studies suggest that DDI in grade 1 CS
should be less than 75 minutes but NOT less than 20
minutes except in extreme circumstances
• Anaesthetists should not feel bullied to achieve
unsafe decision to delivery times
• Anaesthetists should work with not against
obstetricians
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
100

Session 7: The Baby 1 Intrapartum fetal assessment and resuscitation – what the anaesthetist needs to know Professor Steve Robson Professor of Fetal Medicine, Royal Victoria Infirmary, Newcastle-upon-Tyne
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
101

Intrapartum fetal distress
Decision-to-delivery interval
236 ‘crash’ CS [5.7% all Em CS] – 90% under GAMedian [IQR] intervals - BDI 16 [14-16] min, DDI 11 [10-13] min
All delivered within 19 min of decision
Irreversiblecause(n=40)
Potentiallyreversible cause
(n=22)
No identifiablecause (n=174)
Cord arterial pH
Cord pH < 7.0BDI (min)
DDI (min)
Spearman’s rho(cord pH & BDI)
7.09(6.99-7.21)11 (28%)
11.5 [9-15.8]
10[9-12] -0.372
(p=0.08)
7.16(7.06-7.25)1 (4.5%)
16.5[14-18.3]
11.5[10.8-13.3]
-0.204(p=0.36)
7.21(7.16-7.25)8 (4.6%)
16[14-19]
11[10-13]
0.04(p=0.57)
<0.001
<0.001<0.001
0.001
p
Rate of drop 0.013 / min
Leung et al. 2009
Nonreassuring FHR pattern
Intrauterine resuscitation
Maternal positioningTreatment epidural-related hypotension
Discontinue oxytocin infusionAdministration of oxygen
Intravenous fluidsAcute tocolysisAmnioinfusion
Maternal position
• Placing mother in left lateral or Sim’s position alleviates aortocaval compression
• Fetal oxygen saturation highest in left lateral position (Carbonne et al. 1996)
• Upright or lateral positions in II stage reduce rate of abnormal FHR patterns vs supine or lithotomy [1a] (1.2% vs 4.2% - RR 0.28 [0.08-0.98], NNT 33)
(CESU, RCOG 2001)
Mean BP
Mean fetal oxygenSaturation (%)
Left lateral Supine Right lateral
90.0 (9.1)
53.2 (12.2)
95.7 (12.1)
46.7 (9.0)*
95.4 (10.1)
50.5 (7.8)
Maternal oxygen therapy for nonreassuringFHR pattern
• Umbilical & placental vessels vasoconstrict with hyperoxia• Maternal hyperoxygenation immediately prior to CS does
not affect umbilical cord pH [Perrault et al. 1992, Crosby et al. 1992]
• Oxygen for ≤ 10 min may improve fetal pH and/or p02[Althabe et al. 1967, Mendez-Bauer et al. 1967, Gare et al. 1969]
• Oxygen for prolonged periods may adversely affect fetalacid-base status
Thorp et al. 1995 - ↓ cord arterial pH (RCT)
Saling et al. 1963 - ↓ scalp pHFawole & Hofmeyr (CDSR 2006)
• More acidaemia (cord arterial pH <7.2)
• Trend towards reduced cord arterial oxygen content &saturation (-0.8 [-2.2, 0.7]) mL/dL and -4.4 [-11.2, 2.4] %)
• No differences in Apgar scores
Oxygen during second stage of labour
Supplementary oxygen for Emergency CS under regional anaesthesia
Urgent & Emergent CS (DDI < 30 min)Oxygen via Venturi-type mask
N=125
21% oxygen 60% oxygen
UV P02 (kPa)Urgent
EmergentUV P02 content (mL/dL)
UrgentEmergent
3.2 (0.8)2.9 (0.7)
10.8 (3.9)8.7 (3.2)
3.8 (0.8)3.4 (0.8)
13.3 (2.8)11.5 (4.7)
No differences in markers of free radical activity (isoprostane, malondialdehyde)
in maternal & umbilical blood, acidosis (UA pH <7.2) or neonatal outcome
Khaw et al. 2004
p<0.002 p<0.04
p<0.002
p<0.04
Efficacy of IU resuscitation techniques in improving fetal SO2
RCT 3 techniques of IU resuscitation in healthy fetuses during labourFSpO2 measured using Oxifirst sensor (Nellcor)
• Rt & Lt lateral (48%) vs. supine (37%) position [p<0.05]
• IV fluid – 1000 mL RLS - 45% → 51% [p<0.05]
500 mL!000 mL
Simpson & JamesObstet Gynecol 2005(n=42)
• Oxygen10L/min43% → 52% [p<0.05]
Baseline FSpO2 <40%Baseline FSpO2 ≥40%
Effect of maternal oxygen on fetal pulse oximetry in fetuses with non-reassuring CTG
Haydon et al. 2006
20
25
30
35
40
45
50
55
30-40% 40-50% 50-60%
Room air 40% Fi02 100% Fi02
FpS
o2
**
***
*
* p<0.05, ** p<0.01, ***p<0.001
Non-reassuring CTG(n=24)
Oxygen4L/min (40% FiO2) for 30 min
Room air for 30 min10L/min (100% FiO2) for 30 min
Mean increase in FSpO2
4L10L
4.9% (p=0.001)6.5% (p=0.003)
Overstimulation with oxytocin
pH 7.22 7.21HCO3 28 27BE -1 -2
‘Aim for 3-4 contractions every 10 min’CESU, RCOG 2001
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
102

Tocolysis for nonreassuring FHR pattern
• Terbutaline - 250 µg i.v. or sc• Ritodrine – 1-2 mg i.v.• Hexoprenaline – 5-10 µg i.v. • Magnesium sulphate 4 g i.v. • Atosiban – 6.75 mg i.v.
Terbutaline associated with reduced uterine activity in greater proportion of women than Mg (RR 0.07 [0.0-1.1])
Magann et al. 1993
Tocolysis for fetal distress
• 250 µg in 5 ml saline i.v. over 5 min.
• Rapid (1-2 min) prolonged (15-20 min) tocolysis
• Few maternal side effects [HR ↑ 20 bpm, 10% palpitations]
• Propanolol 1-2 mg after delivery baby
• 1-2 mg nebulized no effect
Sp - Terbutaline (Sp)Aug - Terbutaline (+oxytocin stopped)Aug - oxytocin stopped
0
20
40
60
80
100
0 15 30 45 60 75 90Min
% r
educ
tion
uter
ine
activ
ity
Arulkumaran 1994
Terbutaline
Tocolysis for suspected intrapartum fetal distress
Terbutaline 250 mcg s/c
No improvement in FHR abnormalityApgar score <7 at 1 minApgar score <7 at 2 minUmbilical artery pH <7.20Perinatal mortality
.1 .2 1 5 10
ORRR 0.26
[0.13-0.53]
Kulier & Hofmeyer, CDSR 2009
Overview of 3 RCT’s
Tocolysis for fetal distress
Recurrent decelerations
• Recurrent late /severe variable decelerations
• Fetal scalp pH < 7.25• 0.25 mg terbutaline s/c
• Improvement in pH in 10/11 treated vs. 3/9 control
• 1 min Apgar <7 in 1/11 treated vs. 4/9 (p<0.025)
7.1
7.15
7.2
7.25
7.3
Fetal Capillary UA
Study (n=11) Control (n=9)
n=20
P<0.025
Patriarco et al. 1987
Tocolysis for fetal distress
Recurrent decelerations
1126 Pathological FHR tracesLate decelerations
Variable decelerationsSeverely reduced BLV
Bradycardia
553 ‘Acute fetal acidosis’IV Ritodrine
250-300 µg/min
Scalp pH <7.25
Repeat FBS after 15 min
pH increase > 0.05
Labour allowed to continue(unless other obstetric criteria present)
pH decreased or ‘unchanged’
Delivery expedited
Cabero et al. 1988
Tocolysis for fetal distress
Recurrent decelerations
0
10
20
30
40
50
60
70
80
7.20-7.24 7.15-7.19 7.10-7.14 7.05-7.09 <7.05
%
386 115N 36 12 4
Cabero et al. 1988
Inc > 0.04 Inc up to 0.04 Dec up to 0.04 Dec >0.04UA pH [SD] 7.20 [0.07] 7.20 [0.09] 7.16 [0.08] 7.14 [0.11]
Tocolysis for fetal distress
Recurrent decelerations
0
10
20
30
40
50
60
70
80
Uterine activity
Cord problems
Placentalinsufficiency
Other Unknown Total
Recovered Not recovered
N=553
Cabero et al. 1988
Nonreassuring FHR tracen=956
Prolonged deceleration (> 2 min)Severe variable decelerations
Late deceleration(s)Tachycardia with reduced BLV
110 Randomised
Pullen et al. 2007
Terbutaline 250 µg ivn=57
Nitorglycerin 400 µg ivn=53
Success¶
Em CS within 1 h for NRFHTUltimate CS for NRFHT
Contractions/10 min pre drug / TachysystoleContractions/10 min post drug
UA pH < 7.0∆ MAP (mm Hg) / HR (/min)
¶ Complete resolution NRFHT within 10 min, no recurrence of NRFHT or readministrationof tocolytic within 30 min and no operative delivery for NRFHT within 60 min
71.9%14.0%33.3%
5 (5-10) / 79%2.9 (1.7-3.3) / 2%
5.3%-1 / 19**
64.2%22.6%32.1%
5 (5-10) / 83%4 (2.5-5)* / 19%*
0- 5* / 9*
* p<0.01,** p<0.001
Tocolysis for fetal distress
Terbutaline vs nitroglycerin
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
103

Tocolysis for fetal distress
Prolonged bradycardia
FHR < 100 bpm for ≥ 3 min or < 80 bpm for ≥ 2 min
No change with oxygen, position change
33
FHR improved
FHR not improved (3)
FHR remained normal (22) FHR ominous later (6)
2 CS
CSCord prolapse
VD (2) CS (4)VD (21) CS (1)
30
Injection-recovery time2-3 min 234-6 min 47-9 min 1> 9 min 0 Ingemarsson et al. 1985
250µgterbutaline
Tocolysis for nonreassuring FHR pattern
Indications
• Recurrent decelerations (post FBS)- scalp pH ≥ 7.20 – review FHR after 15 min - scalp pH < 7.20 (prior to transfer to theatre – review FHR in theatre)
• Bradycardia- Prior to transfer to theatre – review FHR in theatre
Decision to continue with attempt at vaginal delivery influenced by:• cervical progress & dilatation
• contraction frequency pre / post tocolytic• base deficit
• associated complications e.g. clinical chorioamnionitis
Relationship between amniotic fluid volume and intrapartum ‘fetal distress’
0
10
20
30
40
50
60
AP AFI < 5 cm IP AFI < 5 cm Normal AFI
Abnormal FHR pattern Em CS 'fetal distrss'
%
Adapted from Irons & Robson 1999
Technique of amnioinfusion
• Initial bolus (250-600 mL) or 10-20 mL/min• Maintenance - 3 mL/min (Nageotte et al. 1985,Owen et al. 1990)
- 250 mL if AFI < 5 cm (Schrimmer et al. 1991)
Increase AFI by 4.3 cm (Strong et al. 1990)
• Outcomes not influenced by; - gravity or infusion pump (Glantz & Letteney 1996)
- warmed (37°C) or room temperature (Glantz & Letteney 1996)
Risks / complications• Maternal / neonatal infection – no evidence risk increased• AF embolism – 2 cases reported (Maher et al. 1994)• Uterine tone – Mean increase 4 mm [0-30 mm Hg]
Isolated cases of hyperactivity (Posner et al. 1990)
Intrapartum amnioinfusion
• Recurrent decelerations• AFI < 5 cm• Scalp pH > 7.20
• Warmed saline• Initial infusion until AFI
> 8 cm• Continuous infusion (100-200 ml/h to keep AFI > 8 cm
Amnioinfusion for potential or suspected umbilical cord compression in labour
Hofmeyr, CDSR 2009
Persistent variable decelerationsCS for suspected fetal distressForceps/VE for suspected fetal distressApgar score <7 at 1 minApgar score <7 at 5 minCord artery pH <7.2Admission to NICUNeonatal hospital stay for > 3 days
.1 .2 1 5 10
OR
RR 0.54 [0.43-0.68]
RR 0.51 [0.35-0.74]
RR 0.40 [0.26-0.62]
RR 0.35 [0.23-0.53]
Review 14 RCT’s transcervical amnioinfusion
Amnioinfusion for recurrent decelerations
Operative delivery for fetal distress
0
5
10
15
20
25
30
AVD CS
Infused Control
NS
P<0.0001N=305
Infusion associated with improvement in: UA ph (7.27 vs 7.23),Low (<7) 1 min Apgar scores: 8 vs 34%)Reduced IP stay (2.5 vs 3.0 dy)Schrimmer et al. 1991
Spinal anaesthesia for Caesarean Section
Potentially acidaemic fetus
SGA fetusGrowth restricted fetus- abnormal UA Doppler- Preeclampsia (± abnormal uterine artery Doppler)
Abnormal intrapartum CTG
Is spinal anaesthesia safe?
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
104

Caesarean section for fetal distressGeneral vs. regional anaesthesia
1 min Apgar scores ≤ 7 in 49% GA, 22% regional
7.1
7.15
7.2
7.25
7.3
Scalp UA
Regional
General
pH
Marx et al. 1984
Severe FHR abnormalitiesCapillary pH <7.20 or
↓steadily(n=168)
General(n=71)
Spinal(n=33)
EpiduralExtension
(n=22)
Maternal choice
Prospective RT comparing general with spinal anaesthesia for CS in PE with a nonreassuring FHR pattern
General Spinal
pHBE (mEq/L)
HCO3 (mEq/L)
All p<0.05
7.23 (7.05-7.4)
4.7 (3.3)
20.4 (3.0)
7.20 (6.93-7.34)
7.1 (4.0)
18.4 (3.3)
0
10
20
30
40
50
GA Spinal
p<0.05
<7.2 <7.1 5-7.9 >7.9
UA pH BD (mEq/L)
Dyer et al. 2003
Conclusions
• Appropriate interpretation of CTG ± FBS• Conservative measures (evidence limited)
- Lateral position, oxygen and fluid
• Identify candidates for resuscitation - Borderline or established acidaemia- Delay realistic chance of resulting in vaginal delivery or avoiding GA- Oligohydramnios & recurrent decelerations
• Resuscitation- Tocolytic (all cases acidaemia pre-CS)- Amnioinfusion (oligohydramnios with borderline acidaemia)
• Spinal anaesthesia reasonable - Phenylephrine to maintain BP ≥ 90% baseline- Timescale / experience key
RT of epidural vs spinal anaesthesia for non-immediate CS in women with potential fetal compromise
Spinal Group(n=27)
Epidural Group(n=30)
Umbilical artery pHBE (mmol/L)
Umbilical veinpHBE (mmol/L)
7.24 (0.11)-4.36 (4.38)
7.28 (0.10)-4.45 (4.01)
7.26 (0.07)-3.85 (2.93)
7.31 (0.05)-3.77 (2.60)
NSNS
NSNS
17.6 (5.7, 29.5)9.7 (1.3,18.1)
Mean difference(95% CI)
23.4 (27.9)14.4 (17.2)0.91 (1.18)
0.2 (0.4)
Max fall in SBP (mm Hg)Max fall in DBP (mm Hg)Max fall in CO (L/min)Max increase in UA PI
5.8 (15.5)4.7 (14.3)
0.98 (1.08)0.5 (1.0)
No statistically significant differences between PE & SGA groups
Spinal anaesthesia for Caesarean SectionPhenylephrine and rapid crystalloid cohydration
Kaplan-Meier plot showing proportion of patients remaining not hypotensive until uterine incision
PE +Cohydration
PE infusionalone
p<0.0002
Ngan Kee et al. 2005
Anaesthesia for CS in acute fetal compromise
• As fast as possible(< 15 minutes)
• Less than 30 minutes
Decision - delivery interval
RT of epidural vs spinal anaesthesia for non-immediate CS in women with potential fetal compromise
Phenylephrine for hypotensionMaternal and fetal haemodynamics (Doppler)
PowerTo detect difference in UA pH 0.05
or difference in BE 1.75 mmol/L need 25 in each group
(α = 0.05, β = 0.9)
Suitablen = 95
Stratified for UA Doppler
Entry criteriaMother with PE
No Yes
Mother No
With SGA Yes 25
14
18
60
Randomisedn = 60
Spinal12.5 mg hyperbaric bupivacaine 0.5%
+ 300 µg diamorphine
Epidural50 mg bupivacaine
+ 50 µg fentanyl
Comparison of phenylephrine infusion regimes for maintaining BP durting spinal anaesthesia for CS
PE - 100 µg/min for 2 min then 100 µg each min if SBP ≤ randomly assigned % of baseline (100, 90 or 80%)
7.30-2.379040
7.30-1.8107016
7.32-1.91520
4
UA pHUA BE (mmol/L)
Dose PE (µg)
N or V (%)
80(n=25)
90(n=25)
100(n=24)
*
****
*p<0.05, **p<0.001 Kee et al. 2004
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
105

Session 8: Challenges for the Obstetric Anaesthetist Major trauma in pregnancy Dr Paul Howell Consultant Anaesthetist, St Bartholomew's & Homerton Hospitals, London
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
106

Trauma in Pregnancy
Causes: Motor Vehicle Accidents
Morbidity & Mortality for Mother & Baby
when seat belts not used (properly)
Fetal death x 3 if no belt
NB: 1 in 3 Pregnant women in USA don’t use seat belt / properly
Airbags OK Hyde LK et al. Obstet Gynecol 2003; 102: 279-86
Saving Mothers’ Lives 2003-2005. CEMACH 2007
Trauma in Pregnancy
Causes: Domestic Violence
Previously poorly recognised / reported
= Major cause of maternal mortality
≤ 20% Pregnancies affected
Shadigan E. Obstet Gynecol Surv 2005; 60: 183-90Saving Mothers’ Lives 2003-2005. CEMACH 2007
Trauma in Pregnancy
Causes: Suicide
• Previously under-recognised / under-reported
• Major cause of maternal mortality
• Often atypical violent deaths
Why Mothers Die 1994-1996. CEMD 1998
Trauma in Pregnancy
Outcome: Maternal
• Most injuries are minor
• Mortality pregnant women > non-pregnant women
• Most deaths due to head injury + haemorrhage
• Obstetric Complications : Abruption (20-50%)
Preterm labour (25%)
Uterine rupture (0.6% but ..)
Amniotic fluid embolism ??
Feto-maternal haemorrhage
Patteson SK. Am Surg 2007; 73: 824-7
Rothenberger D. J Trauma 1978; 18: 173-9
Trauma in Pregnancy
Outcome: Maternal
• Most injuries are minor
• Mortality pregnant women > non-pregnant women
• Most deaths due to head injury + haemorrhage
• Obstetric Complications : Abruption (20-50%)
Preterm labour (25%)
Uterine rupture (0.6% but ..)
Uninjured MVA →→→→ ↑ 6 - 8 x Obstetric Complications
Schiff MA. Am J Epidemiol 2005; 161: 503-10
Trauma in Pregnancy
Outcome: Fetal / Neonatal
1st Trimester: Pelvis + thick uterus protect fetus
= miscarriage + isoimmunisation
2nd Trimester: Uterus emerges into abdomen
Protected by amniotic fluid
3rd Trimester: Uterus thin-walled
= risk of direct injury to fetus
Trauma in Pregnancy
Outcome: Fetal / Neonatal
> 80% Fetal deaths = motor vehicle accidents
= abruption / maternal death
Maternal injury αααα fetal morbidity + mortality
NB: Fetal death despite minor maternal injury
NB: Fetal death ++ penetrating abdo trauma
Trauma in Pregnancy
Resuscitation: New Concepts
• “Scoop & Run”
• Hypovolaemic resuscitation (fluid restriction)
• Permissive hypotension
• Relative anaemia (Hb 7-9 g.dL-1)
• Damage Control Surgery
• Conservative management of solid viscera injury
• Hypertonic saline
No data for pregnant patients
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
107

Multidisciplinary Care:
ObstetricianEmergency PhysicianAnaesthetistMidwife± General / Orthopaedic Surgeon± Internal Medicine± Intensivist± Social Worker± Psychiatrist
Trauma in Pregnancy
Resuscitation:Trauma in Pregnancy
Resuscitation: ATLS
Definitive Care
Data / Information /Response to Therapy
Secondary Survey
Resuscitation
Primary Survey(ABCDE's)
American College of Surgeons, 2004
Trauma in Pregnancy
Resuscitation: ABCDE
A irway: Clear obstruction / foreign body
NB: Pulmonary aspiration risk
Give oxygen
Protect airway if necessary (ETT)
Rapid sequence induction (usually)
Remember C-spine ……
Trauma in Pregnancy
Resuscitation: ABCDE
Breathing: Assess adequacy? Head injury / drugs / alcohol? C-spinal cord injury? Haemo/pneumo-thorax ? Open / flail chest
Intubation + IPPV if necessaryAvoid hyper / hypo-ventilationAim for PaCO2 ~ 25-30 mmHgUse minimum airway pressuresAvoid PEEP if possible± Chest drain (insert at higher level)
Spahn DR. Crit Care 2007; 11: R17
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Remember uterine tilt
Late decompensation in hypovolaemia
Poor FH may indicate hypovolaemiaMay lose 35% of circulating volume
before showing classic signs of hypovolaemia
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Remember uterine tilt
Late decompensation in hypovolaemia
Poor FH may indicate hypovolaemia
Stop compressible haemorrhage
≥ 2 x Large bore IV lines upper limbs
± CVP (beware in hypovolaemia)
± Arterial line
Beware pelvic fractures:
→→→→ XS Blood loss + XS Mortality
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Crystalloids vs. Colloids
SAFE Study
Saline versus Albumin Fluid Evaluation Study:
7000 Non-pregnant trauma patients in ICU
No difference in overall mortality
Mortality if brain injury + albumin
SAFE Study Investigators. N Engl J Med 2007; 357; 874-84
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Hypertonic Saline
→ Controversial
No evidence of improved survival
Studies ongoing……….
→→→→ No evidence for use in pregnancy
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
108

Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Blood Products
• NB: Physiological anaemia of pregnancy
• Access to Group O Rh-ve blood
• Aggressive Rx blood components in massive blood loss
→ ↓ Mortality (Military, non pregnant patients)
→ 1 unit FFP per unit blood
Borgman MA. J Trauma 2007; 63: 805-13
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Blood Products
• NB: Physiological anaemia of pregnancy
• Access to Group O Rh-ve blood
• Aggressive Rx blood components
• Recombinant Factor VIIa (rFVIIa)
• Tranexamic Acid ?
• Cell Salvage
Allam J. Int J Obstet Anesth 2008; 17: 37-45
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation:
• Hypothermia → XS Coagulopathy→ poor outcome
Warming is important!
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Cardiac Arrest
• Remember TILT!
- Sandbag under hip
- Cardiff Wedge
- Kneeling rescuer
- Manually pulling uterus across
Trauma in Pregnancy
Resuscitation: ABCDE
Circulation: Cardiac Arrest
• Remember TILT!
• Standard ACLS Management
• Empty uterus …… within 5 minutes
- Minimises aortocaval compression
- Reduces maternal oxygen consumption
- Makes ventilation easier
- Allows CPR in supine position
As part of maternal
resuscitation!
Katz VL. Obstet Gynecol 1986; 68: 571-6
Trauma in Pregnancy
Resuscitation: ABCDE
Disability: Traumatic Brain Injury
• Most common severe injury in motor vehicle accidents
• Leading cause of maternal death (with haemorrhage)
• ↓ Level of Consciousness = Intracranial pathology
Intoxication
Metabolic # (e.g. Diabetes)
Post-ictal state
Hypovolaemia
Low cardiac output
Regular assessment
is vital
Trauma in Pregnancy
Resuscitation: ABCDE
Disability: Traumatic Brain Injury
• CT Scanning
• Avoid IV colloids (SAFE study)
• Raised intracranial pressure → Raise head
Avoid hypoventilation
Avoid hyperventilation
Transient effect on ↓ ICP
↓ Utero-placental perfusion
Ventilate to normal (for pregnancy) PaCO2
Trauma in Pregnancy
Resuscitation: ABCDE
Disability: Traumatic Brain Injury
Aggressive Management of hypotension & hypoxia
is vital
• CT Scanning
• Avoid IV colloids (SAFE study)
• Raised intracranial pressure → Raise head
Avoid hypoventilation
Avoid hyperventilation
Mannitol / frusemide?
Hypertonic saline-dextrans
Corticosteroids?
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
109

Trauma in Pregnancy
Resuscitation: ABCDE
Exposure:
• Check for hidden injuries
• Convulsions or ↓ Level of Consciousness
Eclampsia
Epilepsy
Intracranial pathologyMetabolic (e.g. hypoglycaemia)Drugs (e.g. cocaine)
Trauma in Pregnancy
Resuscitation: ABCDEF
Fetus: Monitoring
Cardiotocography (CTG):Fetal Heart Rate + Variability
NB: Non-reassuring CTG may be 1st sign of hypovolaemia
NB: ↓↓↓↓ FHR Variability with opioid analgesia
Trauma in Pregnancy
Resuscitation: ABCDEF
Fetus: Monitoring
Cardiotocography (CTG):Fetal Heart Rate + Variability
Obstetrician looks for:Uterine activity
Ruptured membranes
Placental abruption
Fetal Heart ST Analysis (STAN)
Rosen K. Expert Rev Obstet Gynecol 2007; 2: 609-20
Trauma in Pregnancy
Fetus: Isoimmunisation
Rhesus +ve fetus Rhesus –ve mother
Feto-maternal Haemorrhage
Kleihauer-Betke Test
Give Rho(D) Immunoglobulin
to mother
+ve
Trauma in Pregnancy
Training:
Advanced Trauma Life Support (ATLS)American College of Surgeonswww.facs.org/trauma/atls/index.html
Managing Obstetric Emergencies and Trauma (MOET)Advanced Life Support Group (ALSG) / RCOGEndorsed by CEMACHwww.alsg.org
Primary Trauma Course (PTC)Developing world projectwww.primarytraumacare.org
European Trauma Course (ETC)European Resuscitation CouncilNew, simulator based course, in developmentwww.erc.edu
Trauma in Pregnancy
Radiographic Imaging:
• Do what needs to be done – Mother comes first!!
• Risks of teratogenesis / malignancy / gene mutation = SMALL
• Maximum risk of teratogenesis in 1st Trimester
• Protect fetus where possible (lead sheild over pelvis)
Multidetector CT Scan (MDCT) = Gold Standard
64 Slice MDCT → Whole body CT in ~ 30 secs
Sensitivity = 94%
Specificity = 100%
Accuracy = 97%
NB: Escort to CT ScanRemember uterine tilt!
Ahvenjarvi L. Acta Radiol 2005; 46: 177-83
Trauma in Pregnancy
Ultrasonography:
e.g. FAST Scan (Focused Assessment with Sonography for Trauma)
• Use for ? intrabdominal haemorrhage (has replaced DPL)
• Useful for pericardial fluid / haemopneumothorax
• Sensitivity similar in pregnant / non-pregnant
• May also be used to check fetal heart
Trauma in Pregnancy
Analgesia:
Opioids: OK = mainstay in trauma
NB: flat CTG / neonatal depression
NSAIDs: Generally discouraged
NB: Platelet / renal effects
?? Short term use OK
Paracetamol: Safe (IV Preparation available)
Tramadol: Embryotoxic in animal studies but ….?
Regional analgesia ± peripheral nerve blocks
± intercostal nerve blocks for rib fractures
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
110

Trauma in Pregnancy
Surgery: Do what is necessary!
• Remember tilt – to minimise aortocaval compression
• Antacid prophylaxis
• Rapid Sequence Induction
• IPPV to normal (for pregnancy) PaCO2
• CTG - before / after surgery (+ during…..?)
• Maintain BP / cardiac output (+ uteroplacental perfusion)
• Consider transoesophageal doppler (TEE)
• Consider cell salvage if available
• If caesarean section – beware IV bolus of syntocinon………..
• Post-operative HDU / ITU care
Three Lessons:
• Maternal resuscitation is the best form of fetalresuscitation – carry on as usual!
• Remember uterine tilt
• Consider early emptying of the uterus to facilitate
maternal / fetal resuscitation
Trauma in Pregnancy
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
111

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 8: Challenges for the Obstetric Anaesthetist Pulmonary oedema in the third trimester – a perspective from South Africa Professor Rob Dyer Professor & Second Chair, Department of Anaesthesia, University of Cape Town
Introduction In the developing world, the diagnosis and management of the causes of pulmonary oedema in the third trimester are made difficult due to the high prevalence of co-morbidities such as preeclampsia, valvular heart disease and HIV/AIDS. This presentation describes several case presentations which highlight key diagnostic and management points in this challenging area of obstetric anaesthesia.
A brief summary of anaesthesia considerations relating to peripartum cardiomyopathy (PPCM) is presented as an introduction. Clinical presentation and pathophysiology of PPCM The diagnosis of PPCM depends upon the following criteria:
(1) The development of cardiac failure in the last month of pregnancy or within 5 months postpartum,
(2) The absence of an identifiable cause of cardiac failure,
(3) The absence of heart disease before the last month of pregnancy, and
(4) Echocardiographic evidence of left ventricular systolic dysfunction, including left ventricular ejection fraction < 45%, and/or fractional shortening < 30%, and/or left ventricular end diastolic dimension >2.7cm/m2.1,2
PPCM remains a diagnosis of exclusion; there are no specific criteria distinguishing PPCM and other forms of dilated cardiomyopathy. The incidence is about one case per 1000 live births in South Africa, and one in 2289 to one in 4000 live births in the USA. 3-5 Although relatively rare, this condition is associated with mortality rates of 20-85%. The largest prospective case series reports have not confirmed previously suggested risk factors for PPCM, namely older age, multiparity, and long-term use of tocolytic agents.2 Preeclampsia has been thought to be a risk factor, although some authors state that the presence of hypertension or preeclampsia precludes the diagnosis of PPCM.
The pathogenesis remains poorly understood. Autoimmune and inflammatory mechanisms have been proposed and studied since the 1970’s. Myocarditis has been implicated, but no definite link established. Biopsies found an inflammatory component in only <10% of cases. A viral origin for the disease has also been postulated. Another theory is that male chromosomal DNA originating from fetal cells in the maternal circulation (microchimerism) may initiate an autoimmune myocarditis. Further evidence of immune activation is the finding of increased levels of tumour necrosis factor, C-reactive protein and a plasma marker of apoptosis, Fas/Apo-1. Prolactin cleavage is now thought to be implicated, influencing a pathway essential for the protection of the heart from postpartum stress.6,7 Yet another study has demonstrated that apoptosis of cardiomyocytes may be the crucial defect, in that inhibition of such apoptosis improves cardiac function in mice. The clinical presentation in South Africa3 consists of a displaced hypodynamic apex in 72% of cases, and a gallop rhythm in 92%. Mitral regurgitation was found in 43%. ECG changes included voltage criteria for LVH in 66% and ST-T wave abnormalities in 96% of cases. Q waves, non-specific ST segment changes, atrial or ventricular arrhythmias8, and left bundle branch block9 have all been reported. Other signs and symptoms are oedema, dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea, cough, abdominal discomfort, precordial pain and postural hypotension. As the heart dilates, thrombus formation, particularly in the right ventricle and left atrium, becomes an increasing risk. Peripheral embolisation can then involve lower extremities, the cerebral circulation, the splanchnic circulation, and the coronary or pulmonary arteries. The differential diagnosis includes myocardial infarction, sepsis, severe preeclampsia, amniotic fluid embolism and pulmonary embolism.10 Pharmacological management Treatment objectives are to reduce preload and afterload and increase contractility. Diuretics are safe and usually the first line therapy. Hydralazine is preferable to ACE inhibitors during pregnancy.11 Vasodilators in the form of nitrates and amlodipine may also have a place. The positive inotropic effects of dobutamine and even adrenaline may be necessary
112

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 in the management of acute deteriorations. Levosimendan is a newly developed agent which enhances contractility by improving the response of cardiac myofilaments to intracellular calcium, and reduces cardiac workload by opening adenosine dependent potassium channels, producing vasodilatation. This drug has been successfully used in one case of acute heart failure due to PPCM, in whom dobutamine did not improve haemodynamics.1 Digitalis is useful for contractility, rate control and atrial arrhythmias,12 but excessive concentrations may be hazardous in women. The phosphodiesterase inhibitor enoximone has also been successfully employed.13 The use of the ß-blocker carvedilol may improve survival in dilated cardiomyopathy, but there is no data on its use in PPCM. Amiodarone and ACE inhibitors are avoided in pregnancy because of fetal effects14, but ACE inhibitors are the mainstay of treatment after delivery. Heparinisation, particularly if EF is <35%, is often necessary, followed by warfarin in the postpartum period.5
Obstetric and anaesthesia management Although this condition is uncommon, the anaesthetist should have a high index of suspicion of PPCM in any parturient presenting with symptoms attributable to cardiac failure in the last month of pregnancy. There are two well documented cases of undiagnosed PPCM who received conventional doses of thiopentone for induction of anaesthesia for CS and collapsed, requiring extensive cardiopulmonary resuscitation.15,16 Delivery of the fetus should reduce haemodynamic stress. A multidisciplinary team, including obstetrician, cardiologist and anaesthetist, should decide on the safest mode and timing of delivery in severe cases. It is important that the mother’s condition should be stabilised as best possible before delivery is attempted. Vaginal delivery is usually associated with minimal blood loss and less chance of postoperative infection and pulmonary complications. Effective analgesia is essential to minimise haemodynamic stress. Also, carefully titrated epidural analgesia can be used to carefully reduce afterload and preload, and decrease the fluctuations of cardiac output in labour. Caesarean delivery is reserved for fetal distress, failure to progess, or severe heart failure unresponsive to maximal medical therapy. For caesarean section, first and foremost the coagulation status determines whether regional anaesthesia can be used. Assuming no contraindication in this regard, the next consideration is whether the degree of severity of cardiac failure will permit a sensory block to the level of T4 (which implies sympathectomy to at least T2), as is required for CS, in the presence of some degree of aortocaval compression. Epidural or
combined spinal-epidural are preferable to single shot spinal anaesthesia,17,18 allowing gradual titration of the block, while permitting judicious use of fluids and vasopressors. The authors of a series of 4 case reports gave cogent reasons for the use of carefully performed epidural anaesthesia for CS. However, recent case reports suggest that even very low doses of intrathecal local anaesthetic can cause major haemodynamic effects,1,19 and regional anaesthesia for CS in PPCM should probably be reserved for NYHA Class 1-2, and occasionally Class 3 patients in experienced hands. In patients with pulmonary oedema and hypoxaemia, or refractory heart failure, general anaesthesia is advisable,20 optimally with maintenance of low to normal heart rates and minimal fluctuation in blood pressure, and avoidance of negative inotropes. Remifentanil has been shown to be useful in this setting.21 Invasive monitoring (arterial and central venous lines), are advisable in NYHA Class 3 and 4 patients. In critically ill patients, pulmonary artery catheterisation may have benefits intraoperatively19 and in the postoperative management of pulmonary oedema and/or renal failure.10 In patients with very poor ventricular function, left ventricular assist devices have been used to aid recovery or as a bridge to cardiac transplantation.22, 23 The outcome of PPCM is better than that of other non-ischaemic cardiomyopathies. However, in one recent prospective South African study, 15/100 patients died, and only 23% had normal LV function after 6 months.24 Follow-up should consist of echocardiography, 6 monthly until either recovery or until function reaches a plateau. Medication, either ACE inhibitors or ß-blockers, should continue for at least 1 year. Immunosuppressive or immunomodulatory therapy remain controversial. Symptoms of heart failure have been shown to occur in 21% of patients who enter a subsequent pregnancy with normal LV function, and in 44% in whom LV function is abnormal at the start of the subsequent pregnancy. Summary • Although rare, anaesthetists should have a high
index of suspicion for PPCM in any patient presenting with symptoms compatible with heart failure in the last month of pregnancy.
• A combination of clinical judgement, exclusion of other causes, and investigations (ECG, chest radiograph and echocardiography where available), should point to the diagnosis.
• The cornerstones of stabilisation of the mother include diuretics, vasodilators (within the constraints of individual exclusions in pregnancy), positive inotropes and anticoagulants.
113

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 • Timing and mode of delivery are a multi-
disciplinary decision. • Careful epidural anaesthesia for labour has major
benefits. • Anaesthesia for CS may be hazardous, and
regional anaesthesia (epidural or CSE) in patients with NYHA class greater than 2 should only be undertaken by experienced practitioners.
• In patients of NYHA Class 3 and 4 with PPCM, particularly if complicated by respiratory or renal failure or other co-morbidity, a balanced general anaesthesia technique which includes opioids such as remifentanil, with invasive monitoring and facilities for postoperative ventilation, has a significant role to play.
References
(1) Benlolo S, Lefoll C, Katchatouryan V, Payen D, Mebazaa A. Successful use of levosimendan in a patient with peripartum cardiomyopathy. Anesth Analg 2004; 98(3):822-4.
(2) Sliwa K, Fett J, Elkayam U. Peripartum cardiomyopathy. Lancet 2006; 368(9536):687-693.
(3) Desai D, Moodley J, Naidoo D. Peripartum cardiomyopathy: experiences at King Edward VIII Hospital, Durban, South Africa and a review of the literature. Trop Doct 1995; 25(3):118-123.
(4) Mielniczuk LM, Williams K, Davis DR, Tang AS, Lemery R, Green MS et al. Frequency of peripartum cardiomyopathy. Am J Cardiol 2006; 97(12):1765-1768.
(5) Pearson GD, Veille JC, Rahimtoola S, Hsia J, Oakley CM, Hosenpud JD et al. Peripartum cardiomyopathy: National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) workshop recommendations and review. JAMA 2000; 283(9):1183-1188.
(6) Hilfiker-Kleiner D, Kaminski K, Podewski E, Bonda T, Schaefer A, Sliwa K et al. A cathepsin D-cleaved 16kDa form of prolactin mediates postpartum cardiomyopathy. Cell 2007; 128(3): 589-600.
(7) Biteker M, Duran NE, Ozkan M. The role of bromocriptine in peripartum cardiomyopathy. Am J Obstet Gynecol 2009; 201(2): 13.
(8) Brown CS, Bertolet BD. Peripartum cardiomyopathy: a comprehensive review. Am J Obstet Gynecol 1998; 178(2):409-414.
(9) George LM, Gatt SP, Lowe S. Peripartum cardiomyopathy: four case histories and a commentary on anaesthetic management. Anaesth Intensive Care 1997; 25(3):292-296.
(10) Ray P, Murphy GJ, Shutt LE. Recognition and management of maternal cardiac disease in pregnancy. Br J Anaesth 2004; 93(3):428-439.
(11) Mastrobattista JM. Angiotensin converting enzyme inhibitors in pregnancy. Semin Perinatol 1997; 21(2):124-134.
(12) Rahimtoola SH, Tak T. The use of digitalis in heart failure. Curr Probl Cardiol 1996; 21(12):781-853.
(13) Robin NM, Wenstone R. The use of enoximone in peripartum cardiomyopathy. Intensive Care Med 1998; 24(9):988-989.
(14) Page RL. Treatment of arrhythmias during pregnancy. Am Heart J 1995; 130(4):871-876.
(15) Malinow AM, Butterworth JF, Johnson MD, Safon L, Rein M, Hartwell B et al. Peripartum cardiomyopathy presenting at cesarean delivery. Anesthesiology 1985; 63(5):545-547.
(16) McIndoe AK, Hammond EJ, Babington PC. Peripartum cardiomyopathy presenting as a cardiac arrest at induction of anaesthesia for emergency caesarean section. Br J Anaesth 1995; 75(1):97-101.
(17) Shnaider R, Ezri T, Szmuk P, Larson S, Warters RD, Katz J. Combined spinal-epidural anesthesia for Cesarean section in a patient with peripartum dilated cardiomyopathy. Can J Anaesth 2001; 48(7):681-683.
(18) Langesaeter E, Dragsund M, Rosseland LA. Regional anaesthesia for a Caesarean section in women with cardiac disease: a prospective study. Acta Anaesthesiol Scand, in press.
(19) Pirlet M, Baird M, Pryn S, Jones-Ritson M, Kinsella SM. Low dose combined spinal-epidural anaesthesia for caesarean section in a patient with peripartum cardiomyopathy. Int J Obstet Anesth 2000; 9(3):189-192.
(20) Kaufman I, Bondy R, Benjamin A. Peripartum cardiomyopathy and thromboembolism; anesthetic management and clinical course of an obese, diabetic patient. Can J Anaesth 2003; 50(2):161-165.
(21) McCarroll CP, Paxton LD, Elliott P, Wilson DB. Use of remifentanil in a patient with peripartum cardiomyopathy requiring Caesarean section. Br J Anaesth 2001; 86(1):135-138.
(22) Colombo J, Lawal AH, Bhandari A, Hawkins JL, Atlee JL. Case 1---2002---a patient with severe peripartum cardiomyopathy and persistent ventricular fibrillation supported by a biventricular assist device. J Cardiothorac Vasc Anesth 2002; 16(1):107-113.
(23) Lewis R, Mabie WC, Burlew B, Sibai BM. Biventricular assist device as a bridge to cardiac transplantation in the treatment of peripartum cardiomyopathy. South Med J 1997; 90(9):955-958.
(24) Sliwa K, Forster O, Libhaber E, Fett JD, Sundstrom JB, Hilfiker-Kleiner D et al. Peripartum cardiomyopathy: inflammatory markers as predictors of outcome in 100 prospectively studied patients. Eur Heart J 2006; 27(4):441-446.
114

Session 8: Challenges for the Obstetric Anaesthetist Prevention and treatment of postdural puncture headache Professor Cynthia Wong Associate Professor, Chief of Obstetrical Anesthesia, Northwestern University Feinberg School of Medicine, USA
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
115

Hustead
Special
Sprotte
Tuohy
Crawford
Angle PJ. Anesthesiology 2003; 99:1376
Incidence of PDPH
Needle type Fluid leak (mL/15 min)
17-g Hustead 516 ± 319
17-g Tuohy 405 ± 209
18-g Tuohy 420 ± 191
20-g Tuohy 100 ± 112*
18-g Special Sprotte 360 ± 208
18-g Crawford 356 ± 121
*P < 0.05 compared to all other needlesAngle PJ. Anesthesiology 2003; 99:1376
Incidence of PDPH: Needle Bevel Orientation
Lateral vs. Cephalad
Author N Lateral Cephalad
Norris, 1989 1558
(DP 41)
1.4%
(BP 0.05%*)
2.1%
(BP 1.2%)
Richardson, 1999
534
(DP 15)
0.4%
(BP 0%)
0.7%
(BP 0.7%)
*P < 0.05 compared to cephalad
Epidural Needle Bevel Orientation
Perpendicular(mL/15 min)
Parallel(mL/15 min)
P
367 ± 119 485 ± 216 0.12
18-g Tuohy needle: 10 cadavers
Angle PJ. Anesthesiology 2003; 99:1376-82
Incidence of PDPH after Unintentional Dural Puncture
• Risk factors
• Incidence:
– Needle type
– Bevel direction
– LOR to saline vs. air
Loss of Resistance with Air vs. Saline
0
0.5
1
1.5
2
Inci
denc
e of
PD
PH
(%
)
Saline Air
Aida. Anesthesiology 1998
*
*P < 0.05
• Postdural puncture headache (PDPH)– Incidence after unintentional dural
puncture
– Prevention
– Treatment
Prevention of PDPH
• Avoid dehydration
• ?Placement of an intrathecal catheter
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
116

Prevention of PDPH
0
20
40
60
80
100
% PDPH % EBP
Control IT catheter: short IT catheter long
% p
atie
nts
*
*
*
*
*P < 0.05Ayad S. Reg Anesth Pain Med 2003;28:512
Prevention of PDPH Incidence of PDPH (BP) with an Intrathecal Catheter
Author N Intrathecal Control
Paech, 2001 100 DP 87% (43%*) 86% (80%)
Norris, 1990 56 DP 55% (11%) 52% (19%)
Rutter, 2001 72 DP 71% (50%) 81% (73%)
Spiegel, 2001 153 DP 70% (53%) 81% (62%)
Ayad, 2003 115 DP 30%* (18%*) 91.9% (81.1%)
*P < 0.05 compared to control
Prevention of PDPH
• Avoid dehydration
• ?Placement of an epidural catheter
• ?Avoid 2nd stage pushing
Prevention of PDPH
Avoid 2nd stage pushing
Author N No Push Push
Stride, 1993 460 75% 86%
Angle, 1999 33 10%* (0%*) 74% (57%)
*P < 0.002
Prevention of PDPH
• Avoid dehydration
• ?Placement of an epidural catheter
• ?Avoid 2nd stage pushing
• Prophylactic saline injection– Subarachnoid
– Epidural
Prevention of PDPH
Subarachnoid Saline Injection (10 mL)N Saline Control
Charsley, 2001 54 25%*
(4%*)
62%*
(38%*)
*P < 0.05 compared to control
Prevention of PDPH
• Avoid dehydration
• ?Placement of an epidural catheter
• ?Avoid 2nd stage pushing
• ∅Prophylactic saline injection
• Prophylactic blood patch
Prophylactic Blood Patch Study:Methods
• Double-blinded (N = 64)
• Therapy recommendation by protocol
– VRSP 1 – 3: conservative
– VRSP 4-6, +ADL: conservative
– VRSP 4-6, -ADL: therapeutic EBP
– VRSP > 6: therapeutic EBP
• Followed for at least 5 days
Scavone BM. Anesthesiology 2004
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
117

Effect and Treatment of PDPH
Data presented as median (range) unless specified
SHAMN = 18
EBPN = 18
P
Onset of PDPH (d) 1.5 (1 – 6) 2.0 (1 – 4) 0.57
Maximum VRSP (0 – 10) 6 (2 – 10) 7 (1 – 9) 0.21
Inability to perform ADL (n) 13 10 0.69
Recommend therapeutic EBP (n) 15 11 0.14
Therapeutic EBP (n) 14 9 0.08
PDPH alleviated with therapeutic EBP (n)
9 3 0.15
2nd therapeutic EBP (n) 1 2 0.30
‡‡
Prevention of PDPH
• Avoid dehydration
• ?Placement of an epidural catheter
• ?Avoid 2nd stage pushing
• ∅Saline injection
• ∅Prophylactic blood patch
• Epidural/intrathecal morphine
Prevention of PDPH: Epidural Morphine
0%
4%
8%
12%
16%
20%
PDPH EBP
% p
atie
nts
Al-metwalli RR. Anaesthesia 2008
N = 50
*
*
*P < 0.05
Prevention of PDPH• Avoid dehydration
• ?Placement of an epidural catheter
• ?Avoid 2nd stage pushing
• Saline injection
• ∅Prophylactic blood patch
• Epidural/intrathecal morphine
• Prophylactic epidural Dextran 40 (Salvador, 1992)
• Prophylactic caffeine
Prevention of PDPH: Prophylactic Caffeine
0%
4%
8%
12%
16%
20%
Placebo Caffeine 75 mg q6h Caffeine 125 mg q6h
% p
atie
nts
w/
PD
PH
Esmaoglu A. J Clin Anesth 2005N = 210
• Postdural puncture headache (PDPH)– Incidence after inadvertent dural puncture
– Prevention
– Treatment
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
118

Differential Diagnosis of Postpartum Headache
• PDPH
• Migraine headache
• Tension headache
• Caffeine withdrawal
• Preeclampsia
• Pneumoencephalos
• Sinusitis
Differential Diagnosis of Postpartum Headache
• Meningitis
• Subarachnoid hemorrhage
• Intracranial hemorrhage
• Subdural hematoma
• Cortical vein thrombosis
• Posterior reversible encephalopathy syndrome (PRES)
Incidence of Postpartum Headache
Goldszmidt E. Can J Anaesth 2005 N = 985
Incidence of HA: 39%
Treatment of Postdural Puncture Headache
• Conservative
– Prevent dehydration
– Oral analgesics
– Abdominal binder
– Supine position
Treatment of Postdural Puncture Headache
• Conservative
• Caffeine: temporary
Treatment of Postdural Puncture Headache
• Conservative
• Caffeine
• Sumatriptan: ∅
Treatment of Postdural Puncture Headache
• Conservative
• Caffeine
• Sumatriptan
• ACTH
ACTH for treatment of PDPH
Author Mode N ACTHFoster, 1994 IV 20 70%
Kshatri, 1997 IV 2 2/2
Gupta, 1997 IM 48 83%
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
119

Treatment of Postdural Puncture Headache
• Conservative
• Caffeine
• Sumatriptan
• ACTH
• Epidural saline: ∅• Epidural Dextran
Dextran 40 for treatment of PDPH
Author N Success
Barrios-Alarcon, 1989
56 (28 CS) 100% (within 24 h)
Aldrete, 1993 13 100% (within 24 h)
?? Neurotoxicity of Dextran??
Treatment of Postdural Puncture Headache
• Conservative
• Caffeine
• Sumatriptan
• ACTH
• Epidural saline
• Epidural dextran
• Gelfoam/fibrin glue
Gelfoam and Fibrin Glue for Treatment of PDPH
Author Material N Success
Ambesh, 1991
Gelfoam 2
(18-g Tuohy)
100%
Gerritse, 1997
Fibrin glue 3
(catheter)
100%
Crul, 1999 Fibrin glue 1
(25-g PP)
100%
??Neurotoxicity of Gelfoam and fibrin glue??
Treatment of Postdural Puncture Headache
• Conservative• Caffeine• Sumatriptan• ACTH• Epidural saline• Epidural dextran • Gelfoam/fibrin glue• Epidural blood patch
Epidural Blood Patch
• Gold standard
• Only one randomized, double-blinded study
Epidural Blood Patch
Epidural blood patch for treatment of PDPH
Author N EBP Control
Seebacher, 1989 12 83%* 0%
*P < 0.05 compared to control
Possible Mechanisms of Action of EBP
• Plug dural hole/prevent leak
• Initiate inflammatory reaction in dura
• Acute increase in CSF pressure
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
120

Mechanism of Action of EBP
• Plug dural hole/prevent leak• Initiate inflammatory reaction in dura• Adenosine receptor inactivation (Raskin,
1990):Acute �CSF pressure �inactivation of adenosine receptors �
vasoconstriction ��headache(adenosine receptor activation � vasodilation)
EBP: Success Rate
Epidural blood patch success rate
Author N 1 st EBP 2nd EBP
Abouleish, 1975 118 105 (89%) 10 (98%)
EBP: Success Rate
Epidural blood patch success rate
Author N Complete Partial None
Stride, 1993
135 68% 16% 16%
Williams, 1999
41 34%
(55%)
54%
(36%)
7%
(9%)
Banks, 2001
58 50% 38% 12%
Factors Associated with Success of Epidural Blood Patch
• Dural puncture needle size
Factors Associated with Success of Epidural Blood Patch
Safa-Tisseront V. Anesthesiology 2001
N = 504
Factors Associated with Success of Epidural Blood Patch
• DP needle size
• Interval from dural puncture to epidural blood patch
Dural Puncture to EBP Interval
Success Rate of Therapeutic Blood Patch
N < 24 h > 24 h
Loeser, 1978 8 E, 16 L 29%* 96%
Success = partial or complete relief of PDPH
*P < 0.05
Factors Associated with Success of Epidural Blood Patch
Safa-Tisseront V. Anesthesiology 2001
N = 504
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
121

Factors Associated with Success of Epidural Blood Patch
• DP needle size
• ?Interval from DP to EBP
• ?Volume of blood injected
Volume of Epidural Blood Patch
Volume of Autologous BloodN Low
N = 166 – 15 mL
HighN = 10020 mL
Crawford, 1980 116 31% 98%*
Mixed DP with spinal and epidural needles
*P < 0.05
Observational study
Volume of Epidural Blood Patch
Volume of Autologous BloodN Low
(10 mL)High
(10-15 mL)
Taivainen, 1993 49 68% 66%
Randomized, unblinded
Volume of Epidural Blood Patch
Volume of Autologous Blood
N 10 mL 15 mL 20 mL
Wu, 1994 162 98% 98% 100%
Observational study
Volume of Epidural Blood Patch
N Success Failure
Safa-Tisseront, 2001
504 23 ± 5 mL 23 ± 5 mL
Volume of Autologous Blood
Prospective observational study
Factors Associated with Success of Epidural Blood Patch
Duration of lateral position after EBP
Success rate of EBP
30 min 60 min 120 min
Upon standing after EBP
3/10 6/10 7/10*
24 h later 6/10 8/10 10/10*
Martin R. Can J Anaesth 1994
P < 0.05 compared to 30 min
Factors Associated with Success of Epidural Blood Patch
• DP needle size
• Interval from DP to EBP
• ?Volume of blood injected
• ?Spinal level of EBP relative to DP
• ?Duration in lateral position after EPB
• ?Avoid Valsalva after EPB
Complications of EpiduralBlood Patch
• Back pain
• Nerve root or radicular pain
• Transient neck pain/meningeal symptoms
• Lumbovertebral syndrome
• ?Impairment of subsequent epidural analgesia/anesthesia
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
122

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Bibliography
1. Choi PT, Galinski SE, Takeuchi L, Lucas S, Tamayo C, Jadad AR. PDPH is a common complication of neuraxial blockade in parturients: a meta-analysis of obstetrical studies. Can J Anaesth 2003; 50: 460-9
2. Angle PJ, Kronberg JE, Thompson DE, Ackerley C, Szalai JP, Duffin J, Faure P. Dural tissue trauma and cerebrospinal fluid leak after epidural needle puncture. Anesthesiology 2003; 99: 1376-82
3. Norris MC, Leighton BL, DeSimone CA. Needle bevel direction and headache after inadvertent dural puncture. Anesthesiology 1989; 70: 729-31
4. Richardson MG, Wissler RN. The effects of needle bevel orientation during epidural catheter insertion in laboring parturients. Anesthesia & Analgesia 1999; 88: 352-6
5. Aida S, Taga K, Yamakura T, Endoh H, Shimoji K. Headache after attempted epidural block: the role of intrathecal air. Anesthesiology 1998; 88: 76-81
6. Ayad S, Demian Y, S.N. N, Tetzlaff JE. Subarachnoid catheter placement after wet tap for analgesia in labor: Influence on the risk of headache in obstetric patients. Reg Anesth Pain Med 2003; 28: 512-5
7. Paech M, Banks S, Gurrin L. An audit of accidental dural puncture during epidural insertion of a Tuohy needle in obstetric patients. Int J Obstet Anesth 2001: 162-7
8. Norris MC, Leighton BL. Continuous spinal anesthesia after unintentional dural puncture in parturients. Regional Anesthesia 1990; 15: 285-7
9. Rutter SV, Shields F, Broadbent CR, Popat M, Russell R. Management of accidental dural puncture in labour with intrathecal catheters: an analysis of 10 years' experience. Int J Obstet Anesth 2001; 10: 177-81
10. Spiegel JE, Tsen LC, Segal S. Requirement for and success of epidural blood patch after intrathecal catheter placement for unintentional dural puncture [abstract]. Anesthesiology 2001; April Suppl: A76
11. Stride PC, Cooper PC. Dural taps revisited. A 20-year survey from Birmingham Maternity Hospital. Anaesthesia 1993; 48: 247-55
12. Angle P, Thompson D, Halpern S, Wilson DB. Second stage pushing correlates with headache after unintentional dural puncture in parturients. Canadian Journal of Anaesthesia 1999; 46: 861-6
13. Charsley MM, Abram SE. The injection of intrathecal normal saline reduces the severity of postdural puncture headache. Regional Anesthesia & Pain Medicine 2001; 26: 301-5
14. Scavone BM, Wong CA, Sullivan JT, Yaghmour E, Sherwani SS, McCarthy RJ. Efficacy of a prophylactic epidural blood patch in preventing post dural puncture headache in parturients after inadvertent dural puncture. Anesthesiology 2004; 101: 1422-7
15. Al-metwalli RR. Epidural morphine injections for prevention of post dural puncture headache. Anaesthesia 2008; 63: 847-50
16. Esmaoglu A, Akpinar H, Ugur F. Oral multidose caffeine-paracetamol combination is not effective for the prophylaxis of postdural puncture headache. J Clin Anesth 2005; 17: 58-61
17. Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: a prospective cohort study. Can J Anaesth 2005; 52: 971-7
18. Foster P. ACTH treatment for post-lumbar puncture headache. Br J Anaesth 1994; 73: 429
19. Kshatri AM, Foster PA. Adrenocorticotropic hormone infusion as a novel treatment for postdural puncture headache. Reg Anesth 1997; 22: 432-4
20. Gupta S, Agrawal A. Postdural puncture headache and ACTH [letter]. J Clin Anesth 1997; 9: 258
21. Barrios-Alarcon J, Aldrete JA, Paragas-Tapia D. Relief of post-lumbar puncture headache with epidural dextran 40: a preliminary report. Regional Anesthesia 1989; 14: 78-80
22. Aldrete JA. Epidural dextran for PDPH. Regional Anesthesia 1993; 18: 325-6
123

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 23. Ambesh SP, Kumar A, Bajaj A. Epidural gelatin
(Gelfoam) patch treatment for post dural puncture headache. Anaesth Inten Care 1991; 19: 444-7
24. Gerritse BM, van Dongen RT, Crul BJ. Epidural fibrin glue injection stops persistent cerebrospinal fluid leak during long-term intrathecal catheterization. Anesth Analg 1997; 84: 1140-1
25. Crul BJ, Gerritse BM, van Dongen RT, Schoonderwaldt HC. Epidural fibrin glue injection stops persistent postdural puncture headache. Anesthesiology 1999; 91: 576-7
26. Seebacher J, Ribeiro V, LeGuillou JL, Lacomblez L, Henry M, Thorman F, Youl B, Bensimon G, Darbois Y, Bousser MG. Epidural blood patch in the treatment of post dural puncture headache: a double blind study. Headache 1989; 29: 630-2
27. Abouleish E, de la Vega S, Blendinger TO. Long term follow-up of epidural blood patch. Anesth Analg 1975; 54: 459-63
28. Williams EJ, Beaulieu P, Fawcett WJ, Jenkins JG. Efficacy of epidural blood patch in the obstetric population. Int J Obstet Anesth 1999; 8: 105-9
29. Banks S, Paech M, Gurrin L. An audit of epidural blood patch after accidental dural puncture with a Tuohy needle in obstetric patients. Int J Obstet Anesth 2001; 10: 172-6
30. Safa-Tisseront V, Thormann F, Malassine P, Henry M, Riou B, Coriat P, Seebacher J. Effectiveness of epidural blood patch in the management of post-dural puncture headache. Anesthesiology 2001; 95: 334-9
31. Loeser EA, Hill GE, Bennett GM, Sederberg JH. Time vs. success rate for epidural blood patch. Anesthesiology 1978; 49: 147-8
32. Crawford JS. Experiences with epidural blood patch. Anaesthesia 1980; 35: 513-5
33. Taivainen T, Pitkanen M, Tuominen M, Rosenberg PH. Efficacy of epidural blood patch for postdural puncture headache. Acta Anaesthesiol Scand 1993; 37: 702-5
34. Wu YW, Hui YL, Tan PP. Experience of epidural blood patch for post-dural puncture headache. Acta Anaesthesiol Sin 1994; 32: 137-40
35. Martin R, Jourdain S, Clairoux M, Tetrault JP. Duration of decubitus position after epidural blood patch. Canadian Journal of Anaesthesia 1994; 41: 23-5
36. Ong BY, Graham CR, Ringaert KR, Cohen MM, Palahniuk RJ. Impaired epidural analgesia after dural puncture with and without subsequent blood patch. Anesthesia & Analgesia 1990; 70: 76-9
37. Hebl JR, Horlocker TT, Chantigian RC, Schroeder DR. Epidural anesthesia and analgesia are not impaired after dural puncture with or without epidural blood patch. Anesthesia & Analgesia 1999; 89: 390-4
124

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 9: The Baby 2 Current issues in neonatal resuscitation Dr Ian Laing Consultant Neonatologist, Edinburgh Royal Infirmary
Resuscitation of the neonate has been bedevilled by well-intentioned practice with little evidence base. However, in the last 10 years there have been multicentre controlled trials which have begun to answer some of the urgent questions. In addition, The International Liaison Committee on Resuscitation (ILCOR) has published guidelines for Neonatal resuscitation (1, 2) and these are drawing on what little evidence is available to give advice to frontline clinicians. It is rare for newborn infants to suffer a primary cardiac arrest. Ventilation alone is usually effective in resuscitating the neonate at any gestation. Self-inflating bags, flow-inflating (anaesthesia) bags, and T-piece devices all may be used to provide effective ventilation after birth. Although non-invasive techniques, such as “bag and mask”, are widely taught, they are not always carried out effectively. Intubation (perhaps after preliminary stabilisation) has the merit of delivering intratracheal surfactant to the extreme preterm infant. Whichever method is used, ventilation is likely to be delivered more consistently if a pressure-monitoring device is incorporated. The best indication of successful ventilation is a prompt increase in heart rate. The role of positive end-expiratory pressure during resuscitation requires further research, particularly in preterm infants, in whom it may protect against lung injury. Atelectotrauma can be damaging to the extreme preterm’s alveolar epithelium. Should neonatal resuscitation be carried out with air or oxygen? There are very few studies in humans which attempt to answer this question. There is a case for initiating positive pressure ventilation using air, especially since primary apnoea is commoner than terminal apnoea. If the baby remains blue and bradycardic there is no evidence that increasing the inspired oxygen concentration is of benefit, but neither has it been shown to fail! It may be that cardiac compressions would be more effective at this stage. More studies are required to inform our decisions. The management of meconium associated deliveries has become clearer in the last decade. Suction of vigorous infants at birth does not prevent meconium aspiration syndrome (3). Furthermore suction of
meconium “on the perineum” does not improve outcome (4). It is still not known what role suctioning of thick meconium has in the resuscitation of the unresponsive or “depressed” infant, and perhaps we should continue to advocate this intervention. Cold injury to preterm infants is independently associated with neonatal death. The use of clean polythene bags can largely eliminate evaporative heat losses from the infant’s skin. Consequently every baby should now arrive at the Neonatal Unit with a temperature above 36.5 deg C. Drugs are rarely required in neonatal resuscitation. Adrenaline can be administered intravenously at a dose of 10 microgm/kg, increasing if necessary, but a dose of 30 microgm/kg should not be exceeded (5). Intratracheal adrenaline has not been shown to be effective but it is possible that this route might be beneficial if higher dosages are used (5). References: 1) Niermyer S, Kattwinkel J, Van Reempts P et al. International guidelines for neonatal resuscitation. Pediatrics 2000;106 2) International Liaison Committee on Resuscitation 2005. 3) Wiswell TE, Gannon CM, Jacob J et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter international collaborative trial. Pediatr 2000; 105:1-7 4) Vain NE, Szyld EG, Prudent LM et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicenter randomised controlled trial. Lancet 2004;364:597-602 5) Richmond S. ILCOR and neonatal resuscitation 2005. Arch Dis Child 2007;92:F163-165
125

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Session 9: The Baby 2 Effects of maternal analgesia and anaesthesia on the baby Professor Felicity Reynolds Emeritus Professor of Obstetric Anaesthesia, St Thomas’ Hospital, London
Drugs given to a mother during labour may affect the baby either after placental transfer (a direct effect) or via effects on maternal physiology and biochemistry (indirect effects). Clearly the former mechanism is potentially important for drugs that act systemically, while neuraxial analgesia does not depend for its effect on drug in maternal blood, so placental drug transfer is less important, while indirect effects may be more important.
It is widely assumed that any pharmacological analgesia must have adverse effects on the baby, and that unmodified labour is relatively harmless. In fact, it has long been known that painful labour produces adverse changes in maternal physiology and biochemistry (Fig 1) that are potentially harmful to the fetus, while effective analgesia may reverse these changes.1
Fig. 1. Effects of unmodified labour on maternal physiology and biochemistry.
Effects of systemic analgesia
Opioids given to provide systemic analgesia in labour produce dose-dependent direct fetal and neonatal effects. Pethidine has been extensively studied (table 1). All neonatal effects are maximum if pethidine is given 4-5 h before delivery, but negligible if given only within 1 h. In much of the research involving neonatal outcome, systemic opioids have been compared with neuraxial analgesia, but a recent randomised comparison of i.v. pethidine with placebo showed that umbilical artery respiratory and metabolic acidosis were more severe with pethidine.2 As systemic opioid analgesia is less complete than neuraxial analgesia, opioids are less able to mitigate the adverse effects of labour pain.
Evidence that diamorphine or remifentanil offer any neonatal advantage over pethidine is conflicting. Risk of neonatal respiratory depression and the need for monitoring remain.3,4
Table 1. Effects of pethidine on the baby Fetal effects Neonatal effects muscular activity ↓↓↓↓ aortic blood flow ↓↓↓↓ short-term variability ↓↓↓↓ oxygen saturation ↓↓↓↓ maternal saturation ↓↓↓↓
Apgar scores ↓↓↓↓ respiration ↓↓↓↓ neurobehavioural score↓↓↓↓ muscle tone ↓↓↓↓ suckling behaviour ↓↓↓↓
Maternal pain, work, stress
hyperventilation → respiratory alkalosis
Fetal metabolic acidosis
uterine vasoconstriction
left O2 shift metabolic acidosis
release of cortisol and catecholamines
lipolysis hyperglycaemia
placental flow ↓
Placental exchange ↓
O2 transfer ↓
free fatty acids ↑
fetal free fatty acids ↑
fetal hyperglycaemia
+ hypoxia
apnoeic episodes
s
Placental membrane
126

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
Direct effects of neuraxial analgesia
Adverse direct fetal drug effects are likely only if maternal systemic effects of the drugs given neuraxially reach a detectable threshold. Thus when lidocaine was used to provide continuous epidural analgesia, drowsiness was observed in both mother and baby. Longer-acting local anaesthetics (bupivacaine, ropivacaine, levobupivacaine), correctly sited, are more slowly absorbed, and systemic effects are usually observed only after accidental i.v. administration. Although opioids are well recognised to produce direct fetal and neonatal depression and to impair breast-feeding when used systemically, their potential to do so when used for neuraxial analgesia
is less,5 though still present with large doses (see below).
Indirect effects of neuraxial analgesia
Neuraxial analgesia may cause maternal changes that can affect the baby (Table 2). Focus on the potentially adverse effects may prompt the belief that neuraxial must be the worst type of analgesia for the baby, but this ignores its potentially favourable effects. Neonatal outcome depends on the balance between the two. No assumptions should be made as to overall neonatal effect without direct neonatal assessment.
Table 2. Maternal changes produced by neuraxial analgesia that may affect the baby
Potentially unfavourable effects Potentially favourable effects Maternal hypotension Reduced maternal stress and hyperventilation Maternal fever (reversal of all factors in fig 1) Increased need for oxytocin Uterine vasodilatation (sympathetic blockade) Prolonged second stage Fewer episodes of haemoglobin desaturation Increased need for instrumental delivery Placental drug transfer is unimportant
Assessment of the baby
Even fetal effects are poor predictors of neonatal outcome.
Fetal heart rate
Despite its shortcomings, cardiotocography is often considered mandatory for mothers receiving neuraxial analgesia.
In consequence loss of short-term variability, decelerations and major bradycardia may be noted, although meta-analysis of controlled trials shows that fetal heart rate abnormalities are not increased by epidural compared with systemic opioid analgesia,6 or by epidural fentanyl,7 though they are increased by intrathecal opioids.8 Fetal bradycardia may be associated with the rapid onset of analgesia, and various mechanisms have been considered to explain this. • Some bradycardias are associated with uterine
hypertonus, which may result from a decline in circulating epinephrine concentration, itself a myometrial inhibitor.
• In theory, a reduction in epinephrine would allow unopposed norepinephrine to cause uterine vasoconstriction.9
• Direct fetal effects from opioids (unlikely with small intrathecal doses).
• Maternal hypotension, reduced cardiac output, hypoventilation.
• Omission of local anaesthetic; sympathetic blockade causes uterine vasodilatation.
• Omission of fluid preload. An i.v. fluid load may inhibit uterine contractions and reduces the incidence of fetal heart decelerations.
• An external tocodynamometer belt is commonly removed before siting an epidural. Until the belt is replaced, once analgesia is achieved uterine contractions may be undetected.
• The obstetrician may be keen to continue the administration of oxytocin. This should be resisted during epidural insertion, to avoid undetected uterine hypertonus.
Provided the bradycardia is brief and does not reflect poor placental perfusion resulting from uterine hypertonus or vasoconstriction, maternal hypotension or aortocaval compression, its presence is claimed to be irrelevant to fetal outcome,8 though more attention has been paid to caesarean section rate than to actual neonatal welfare.
Fetal blood flow
Early Finish studies using radio-Xenon suggested that, provided maternal aortocaval compression and hypotension were avoided, maternal placental flow rose following epidural local anesthetic, particularly in the presence of preeclampsia.10 Since then, Doppler flow technology, a better predictor than cardiotocography of neonatal wellbeing,11 has spawned numerous studies, some again showing favourable changes with epidural analgesia in preeclampsia,12,13 but none demonstrating any
127

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
correlation with neonatal outcome. One study purports to demonstrate increased flow resistance with epidural analgesia,14 but, as there were no controls, the findings could simply reflect changes associated with labour.
Apgar score
Apgar score reflects the intrauterine environment but applies only to the first few minutes of life, a stimulating time for the newborn, so it may fail to detect delayed neonatal depression. Meta-analysis of controlled trials showed that there were significantly fewer low Apgar scores at one and five minutes with epidural than with systemic opioid analgesia.15
Neurobehavioural assessments
Over the years various neurobehavioural tests have therefore been developed to assess the newborn further into the post-natal period. The most used by anaesthetists, the neurological and adaptive capacity score (NACS), may not be very sensitive or reliable, although it tends to correlate with breast feeding (Table 3). Meta-analyses of randomised trials revealed no significant difference in NACS between epidural and systemic opioid analgesia,15 though higher doses of epidural fentanyl may be associated with lower scores.16
Acid-base balance
Umbilical artery acid-base balance is a valid index of the recent fetal environment. Fetal pH is increased by maternal hyperventilation, so base excess is a better marker of fetal metabolic status in painful labour. In 1974, three studies found that, whereas normal labour was associated with a progressive deterioration in base excess in mothers and babies, epidural analgesia appeared to mitigate this adverse effect,1,17 particularly in long labour. Meta-analysis of controlled trials conducted since then, comparing umbilical acid-base values after epidural and systemic analgesia,17 showed that both UA pH and base excess are better following epidural than systemic analgesia. The same neonatal benefit is seen when comparing epidural with no analgesia.18 This beneficial effect applies to both old-fashioned epidurals with local anaesthetic alone, and modern low-dose combinations.
Neuraxial analgesia comes in many guises, that have only minor neonatal impact. One randomised trial showed that umbilical artery pH was significantly lower following single-shot spinal analgesia using a low-dose bupivacaine-opioid combination, than with paracervical bupivacaine.19 Combinations including clonidine or epinephrine also have significant adverse neonatal effects.20,21
Breast feeding The numerous unrandomised trials that have been published demonstrate variable effects of neuraxial analgesia on breast feeding22-38 (Table 3), but only those purporting to show adverse effects receive much publicity. The many confounding variables (intention to breast-feed, parity, age, local tradition, social class, education, delivery type and the amount of help and support offered) make results of unrandomised trials unreliable. One observational study and one randomised trial, however, have suggested (perhaps unsurprisingly) an adverse effect on breast feeding of large epidural doses of fentanyl.34,35 More evidence is needed. Meanwhile, when prolonged epidural analgesia for labour using a local anaesthetic-opioid combination is extended for emergency caesarean section, it is unwise for the baby’s sake to give further opioid either epidurally or systemically.
Maternal anaesthesia While neuraxial analgesia in labour has a favourable neonatal effect (usually ignored), and spinal anaesthesia is preferred for the mother undergoing caesarean section for many reasons, it cannot be assumed to be better also for the baby. General anaesthesia sometimes depresses the Apgar score, but only at one minute.39 Traditional spinal anaesthesia, despite lack of maternal sedation, small dose requirement and careful attention to maternal haemodynamics, is associated with adverse fetal flow changes40 and more neonatal acidosis than either general or epidural anaesthesia,39 an effect only partly explained by the use of ephedrine with spinals. Using low-dose local anaesthetic-opioid combinations and phenylephrine as a vasopressor41 may improve neonatal outcome after spinal anaesthesia. There is no advantage to the baby in using a combination of ephedrine and phenylephrine, rather the reverse.42 The upshot is not that it is better to use general than spinal anaesthesia, but rather that if, for any reason, a mother is compelled to receive general anaesthesia, she should be reassured that it is not more damaging to the baby than neuraxial anaesthesia.
References 1. Thalme B, Belfrage P, Raabe N. Lumbar epidural
analgesia in labour: I. Acid-base balance and clinical condition of the mother, fetus and newborn child. Acta Obstet Gynecol Scand 1974; 53: 27-35.
2. Sosa CG, Buekens P, Hughes JM, et al. Effect of pethidine administered during the first stage of labor on the acid-base status at birth. Eur J Obstet Gynecol Reprod Biol 2006;129:135-9.
3. Rawal N, Tomlinson AJ, Gibson GJ, Sheehan TM. Umbilical cord plasma concentrations of free morphine following single-dose diamorphine analgesia and their
128

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
relationship to dose-delivery time interval, Apgar scores and neonatal respiration. Eur J Obstet Gynecol Reprod Biol 2007;133:30-3.
4. Hill D (proposer), Van de Velde M (opposer). Controversy: Remifentanil patient-controlled analgesia should be routinely available for use during labour. Int J Obstet Anesth 2008;17:336-41.
5. Porter JS, Bonello E, Reynolds F. The effect of epidural fentanyl on neonatal respiration. Anesthesiol 1998; 89: 79-85.
6. Leighton BL, Halpern SH. The effects of epidural analgesia on the progress of labor, maternal and neonatal outcomes: a systematic review. Am J Obstet Gynecol 2002; 186: S69-77.
7. Russell R, Reynolds F. Epidural infusions of low-dose bupivacaine and opioid in labour: does reducing motor block increase the spontaneous delivery rate? Anaesthesia 1996; 51:266-73.
8. Mardirosoff C, Dumont L, Boulvain M, Tramer MR. Fetal bradycardia due to intrathecal opioids for labour analgesia: a systematic review. BJOG 2002; 109: 274-81.
9. Segal S, Wang SY. The effect of maternal catecholamines on the caliber of gravid uterine microvessels. Anesth Analg 2008; 106: 888-92.
10. Jouppila P, Jouppila R, Hollmen A et al. Lumbar epidural analgesia to improve intervillous blood flow during labor in severe preeclampsia. Obstet Gynecol 1982; 59: 158-61.
11. Mires G, Williams F, Howie P. Randomised controlled trial of cardiotocography versus Doppler auscultation of fetal heart at admission in labour in low risk obstetric population. BMJ 2001; 322: 1457-60.
12. Mires GJ, Dempster J, Patel NB, Taylor DJ. Epidural analgesia and its effect on umbilical artery flow velocity waveform patterns in uncomplicated labour and labour complicated by pregnancy-induced hypertension. Eur J Obstet Gynecol Reprod Biol 1990; 36: 35-41.
13. Ramos-Santos E, Devoe LD, Wakefield ML, Sherline DM, Metheny WP. The effects of epidural anesthesia on the Doppler velocimetry of umbilical and uterine arteries in normal and hypertensive patients during active term labor. Obstet Gynecol 1991; 77: 20-6.
14. Chen LK, Lin CJ, Huang CH, et al. The effects of continuous epidural analgesia on Doppler velocimetry of uterine arteries during different periods of labour analgesia. Br J Anaesth 2006; 96: 226-30.
15. Halpern SH, Leighton BL, Ohlsson A, Barrett JFR, Rice A. Effect of epidural vs parenteral opioid analgesia on the progress of labor: a meta-analysis. JAMA 1998; 280: 2105-10.
16. Reynolds F, Russell R, Porter J, Smeeton N. Does the use of low dose bupivacaine infusion increase the normal delivery rate? Int J Obstet Anesth 2003;12:156-63.
17. Reynolds F, Sharma S, Seed PT. Analgesia in labour and funic acid-base balance: a meta-analysis comparing epidural with systemic opioid analgesia. Br J Obstet Gynaecol 2002; 109: 1344-53.
18. Schocket M, Garrison R, Wiley J, Sharma S. Epidural analgesia has a favorable effect on funic base excess compared to no analgesia during labor. Anesthesiology 2005; 102: SOAP abstract A-40.
19. Junttila EK, Karjalainen PK, Ohtonen PP, et al. A comparison of paracervical block with single-shot spinal for labour analgesia in multiparous women: a randomized controlled trial. Int J Obstet Anesth 2009;18:15-21.
20. Nakamura G, Ganem EM, Módolo NS, et al. Labor analgesia with ropivacaine added to clonidine: a randomized clinical trial. Sao Paulo Med J 2008;126:102-6.
21. Missant C, Teunkens A, Vandermeersch E, Van de Velde M. Intrathecal clonidine prolongs labour analgesia but worsens fetal outcome: a pilot study. Can J Anesth 2004;51:696-701.
22. Rajan L. The impact of obstetric procedures and analgesia/anaesthesia during labour and delivery on breast feeding. Midwifery 1994;10:87-103.
23. Halpern SH, Levine T, Wilson DB, MacDonell J, Katsiris SE, Leighton BL. Effect of labor analgesia on breastfeeding success. Birth 1999;26:83-8.
24. Jordan S, Emery S, Bradshaw C, Watkins A, Friswell W. The impact of intrapartum analgesia on infant feeding. BJOG 2005; 112: 927-34.
25. Albani A, Addamo P, Renghi A, Voltolin G, Peano L, Ivani G. The effect on breastfeeding rate of regional anesthesia technique for cesarean and vaginal childbirth. Minerva Anestesiol 1999;65:625-30.
26. Riordan J, Gross A, Angeron J, et al., The effect of labor pain relief medication on neonatal suckling and breastfeeding duration. J Hum Lact 2000;16:7-12.
27. Ransjö-Arvisdon AB, Matthlesen A-S, Lilja G, Nissen E, Widström A-M, Uvnäs-Moberg K. Maternal analgesia during labor disturbs newborn behavior: Effects on breastfeeding, temperature and crying. Birth 2001; 28: 5-12.
28. Radzyminski S The effect of ultra low dose epidural analgesia on newborn breastfeeding behaviors. JOGNN - Journal of Obstetric, Gynecologic, & Neonatal Nursing 2003;32:322-31.
29. Henderson JJ, Dickinson JE, Evans SF, McDonald SJ, Paech MJ: Impact of intrapartum epidural analgesia on breast-feeding duration. Aust N Z J Obstet Gynaecol 2003, 43:372-7.
30. Baumgarder DJ, Muehl P, Fischer M, Pribbenow B. Effect of labor epidural anesthesia on breast-feeding of healthy full-term newborns delivered vaginally. J Am Board Fam Pract 2003;16:7-13.
31. Volmanen P, Valanne J, Alahuhta S: Breast-feeding problems after epidural analgesia for labour: a retrospective cohort study of pain, obstetrical procedures and breast-feeding practices. Int J Obstet Anesth 2004;13:25-9.
32. Chang ZM, Heaman MI. Epidural analgesia during labor and delivery: Effects on the initiation and continuation of effective breastfeeding. J Hum Lact 2005;21:305-14.
33. Wang BP, Li QL, Hu YF. [Impact of epidural anesthesia during delivery on breast feeding.] Di Yi Jun Yi Da Xue Xue Bao 2005;25:114-5, 118.
129

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
34. Jordan S, Emery S, Bradshaw C, Watkins A, Friswell W. The impact of intrapartum analgesia on infant feeding. Br J Obstet Gynaecol 2005; 112: 927-34.
35. Beilin Y, Bodian CA, Weiser J, Hossain S, Arnold I, Feierman DE, Martin G, Holzman I. Effect of labor epidural analgesia with and without fentanyl on infant breast-feeding: a prospective, randomized, double-blind study. Anesthesiology 2005; 103: 1211-7.
36. Torvaldsen S, Roberts CL, Simpson JM, Thompson JF, Ellwoood DA. Intrapartum epidural analgesia and breastfeeding: a prospective cohort study. Int Breastfeed J 2006; 1:24. Accessed at www.internationalbreastfeedingjournal.com
37. Wiklund I, Norman M, Uvnäs-Moberg K, et al. Epidural analgesia: breast-feeding success and related factors. Midwifery 2009;25:e31-8.
38. Wilson MJA, MacArthur C, Shennan A. The effect of epidural analgesia on breast feeding: analysis of a randomized controlled trial. Int J Obstet Anesth 2009;18:S7.
39. Reynolds F, Seed PT. Anaesthesia for caesarean section and neonatal acid-base status: a meta-analysis. Anaesthesia 2005; 60: 636-53.
40. Valli J, Pirhonen J, Aantaa R, Erkkola R, Kanto J. The effects of regional anaesthesia for caesarean section on maternal and fetal blood velocities measured by Doppler ultrasound. Acta Anaesthesiol Scand 1994;38:165-9.
41. Lee A, Ngan Kee WD, Gin T. A quantitative systematic review of randomized controlled trials of ephedrine versus phenylephrine for management of hypotension during spinal anesthesia for cesarean delivery. Anesth Analg 2002; 94: 920-6.
42. Ngan Kee WD, Lee A, Khaw KS, Ng FF, Karmaker MK, Gin T. A randomized double-blinded comparison of phenylephrine and ephedrine infusion combinations to maintain blood pressure during spinal anesthesia for cesarean delivery: the effects on fetal acid-base status and hemodynamic control. Anesth Analg 2008;107:1295-302.
130

Tab
le 3
. Bre
ast f
eedi
ng st
udie
s; e
pidu
ral v
s. ot
her
or n
o an
alge
sia
(Ref
eren
ces 2
2-38
)
Ty
pe o
f stu
dy
Epid
ural
type
(n)
C
ontro
ls (n
) O
utco
me
mea
sure
s Fi
ndin
gs
Raj
an 1
994
Subs
et o
f NB
T su
rvey
n=
1064
Var
ious
N
o ep
idur
al
Que
stio
nnai
re a
t 6 w
eeks
, bre
ast,
bottl
e or
a m
ixtu
re
Epid
ural
s and
Ent
onox
no
effe
ct o
n br
east
feed
ing.
Abn
orm
al
deliv
ery,
indu
ctio
n, sh
ort s
econ
d st
age,
gen
eral
ana
esth
esia
and
pe
thid
ine
redu
ced
it
Hal
pern
199
9 pr
ospe
ctiv
e m
ixed
par
ity
CSE
or e
pi
bup+
suf o
r fen
tany
l (1
13)
No
epid
ural
(74)
(som
e ha
d sy
stem
ic o
pioi
ds)
Tele
phon
e in
terv
iew
: bre
ast-
feed
ing
succ
ess a
t 6 w
eeks
72
% fu
lly b
reas
t-fee
ding
at 6
-8 w
eeks
. No
fact
ors r
elat
ing
to
labo
ur a
nalg
esia
had
any
sign
ifica
nt e
ffec
t on
feed
ing
whe
n le
avin
g ho
spita
l or 6
wee
ks la
ter
Alb
ani 1
999
Pros
pect
ive
obse
rvat
iona
l, m
ixed
par
ity
n=19
20 v
agin
al
deliv
erie
s
n/k
No
anal
gesi
a Fe
edin
g at
dis
char
ge
Vag
inal
: epi
dura
l 96.
5% v
. con
trols
97.
8% (N
S)
caes
area
n se
ctio
n: re
gion
al 9
5% v
. gen
eral
ana
esth
esia
85%
(P
=0.0
02)
Rio
rdan
200
0 Pr
ospe
ctiv
e pa
rity
n/k
Var
ious
dru
gs a
nd
dose
s, us
ually
bup
+fen
t (2
7)
No
med
iatio
n (3
7); i
.v.
(52)
; bot
h (1
3)
IBFA
T, L
ATC
H a
sses
smen
t not
pr
oper
ly b
linde
d.
Dur
atio
n of
bre
ast-f
eedi
ng a
t te
leph
one
at 6
wee
ks
LATC
H sc
ore
bette
r with
no
med
icat
ion.
IB
FAT
scor
e no
med
>i.v
.=ep
idur
al>b
oth.
Lo
w IB
FAT
= sh
orte
r fee
ding
but
unm
edic
ated
did
not
feed
long
er
than
the
rest
.
Ran
sjo-
Arv
idso
n 20
01
Pros
pect
ive
parit
y n/
k Ep
idur
al b
upiv
acai
ne o
r pe
thid
ine
(?sy
stem
ic)
or c
ombi
natio
n (1
2)
No
anal
gesi
a (1
0);
mep
ivac
aine
pud
enda
l bl
ock
(6);
Vid
eo o
f inf
ant b
ehav
iour
im
med
iate
ly a
fter d
eliv
ery,
as
sess
ed b
lindl
y.
Age
and
dur
atio
n of
firs
t suc
klin
g
Unm
edic
ated
infa
nts m
ore
activ
e
Rad
zym
insk
i 20
03
Obs
erva
tiona
l n=
56
tota
l U
ltra
low
dos
e bu
piva
cain
e +
fent
anyl
N
o an
alge
sia
Prem
atur
e in
fant
bre
astfe
edin
g be
havi
our s
cale
at b
irth
and
at 2
4 h
No
sign
ifica
nt d
iffer
ence
bet
wee
n gr
oups
in b
reas
t-fee
ding
be
havi
our
Hen
ders
on 2
003
obse
rvat
iona
l nu
llipa
ra
PCEA
bup
+fen
t 5
µg/m
l (69
0)
Supp
ort +
N2O
+ p
eth
(302
) Ti
min
g +
qual
ity o
f 1st fe
ed.
Dur
atio
n of
feed
ing
or st
ill fe
edin
g at
6/1
2
Still
feed
ing
at 6
/12:
epi
dura
l 38%
; con
trols
51%
. Fac
tors
fa
vour
ing
long
er b
reas
t fee
ding
: ter
tiary
edu
catio
n>ol
der
mot
hers
>non
-sm
oker
>no
epi
dura
l
Bau
mga
rder
200
3 se
quen
tial m
ixed
pa
rity
Not
stat
ed (1
15)
No
epid
ural
(116
) 2
succ
essf
ul fe
eds i
n 24
h L
ATC
H
scor
e
Succ
ess i
n 24
h: e
pidu
ral 6
9.6%
; con
trols
81%
; OR
0.5
3 (N
S).
Odd
s of s
ucce
ss in
crea
sed
with
dur
atio
n of
epi
dura
l, to
>1!
Vol
man
en 2
004
retro
spec
tive,
va
gina
l del
iver
y nu
llipa
ra
Bup
ivac
aine
(30)
+o
ccas
iona
l fen
tany
l (8
)
No
epid
ural
(34)
Po
stal
que
stio
nnai
re
Fully
bre
ast-f
eedi
ng in
1st 1
2 w
eeks
Fu
lly b
reas
t-fee
ding
: epi
dura
l 33%
; con
trols
71%
(usu
al re
ason
for
failu
re: n
ot e
noug
h m
ilk)
Fact
ors f
avou
ring
full
brea
st fe
edin
g: y
oung
er m
othe
rs, n
o ep
idur
al, N
OT
room
ing
in, e
arly
skin
con
tact
, edu
catio
n.
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
131

Cha
ng 2
005
pros
pect
ive
coho
rt; m
ixed
pa
rity
Not
stat
ed
(52)
N
o an
alge
sia
63
8-12
h in
itiat
ion
(LA
TCH
) 4/5
2 co
ntin
uatio
n +
NA
CS
8-12
h
Bre
ast-f
eedi
ng e
ffec
tiven
ess α
NA
CS,
no
diff
eren
ce b
etw
een
grou
ps
Still
feed
ing
4/52
: epi
dura
l 86%
, con
trols
81%
(NS)
Wan
g 20
05
obse
rvat
iona
l pa
rity
n/k
Not
stat
ed
(96)
N
o ep
idur
al
74
Ana
lges
ia; m
enta
l sta
te; t
ime
star
ting
lact
atio
n; m
ilk q
uant
ity;
prol
actin
Epid
ural
bet
ter a
nalg
esia
and
men
tal s
tate
; qui
cker
lact
atio
n; m
ore
milk
; hig
her p
rola
ctin
Jord
an 2
005
retro
spec
tive
coho
rt nu
llipa
ra
Neu
raxi
al (2
32)
[con
tain
ing
opio
id 1
58]
N2O
and
/or i
.m. p
ethi
dine
(5
70)
Feed
ing
on h
ospi
tal d
isch
arge
in
disc
harg
e su
mm
ary
(exc
lusi
ve o
r pa
rtial
bre
ast-f
eedi
ng c
f bot
tle-
feed
ing)
Bot
tle-f
eedi
ng o
n di
scha
rge:
N2O
onl
y: 3
2%; i
.m. p
ethi
dine
: 41%
; ne
urax
ial l
ocal
ana
esth
etic
alo
ne: 4
4%; n
eura
xial
with
opi
oid
53%
(N
S). F
inal
logi
stic
regr
essi
on m
odel
pre
dict
ors o
f bot
tle-f
eedi
ng:
mat
erna
l age
, fee
ding
inte
ntio
n, c
aesa
rean
sect
ion
and
fent
anyl
(d
ose-
depe
nden
t ↑bo
ttle
feed
ing)
Bei
lin 2
005
rand
omis
ed
doub
le-b
lind
mul
tipar
ae w
ho
had
prev
ious
ly
brea
st-f
ed
Infu
sion
of b
upiv
acai
ne
with
low
-dos
e fe
ntan
yl
(LF,
n=5
9) o
r hig
h-do
se
(HF,
n=5
7)
Epi
dura
l inf
usio
n:
bupi
vaca
ine
alon
e (0
F,
n=60
)
Day
1: m
ater
nal q
uest
ionn
aire
, la
ctat
ion
cons
ulta
nt a
sses
smen
t, N
AC
S.
Tele
phon
e en
quiry
6 w
eeks
Mat
erna
l ass
essm
ent a
t 24
h co
rrel
ated
with
NA
CS
and
subs
eque
nt
perf
orm
ance
, lac
tatio
n co
nsul
tant
’s d
id n
eith
er.
Not
bre
ast-f
eedi
ng a
t 6 w
eeks
: 0F
: 2%
; LF:
6%
; HF:
19%
(P=0
.002
)
Torv
alds
en 2
006
pros
pect
ive
coho
rt; si
ngle
ton
mix
ed p
arity
. No
sele
ctio
n of
thos
e in
tend
ing
to
brea
st-fe
ed
PCEA
bup
+ fe
nt 3
.3
µg/m
L
ALL
had
i.m
. pet
hidi
ne
(416
)
Non
-pha
rmac
olog
ic/
N2O
/pet
hidi
ne (7
62)
Que
stio
nnai
res o
n di
scha
rge
and
8,
16 a
nd 2
4 w
eeks
: ful
ly, p
artia
l or
not b
reas
t-fee
ding
. Haz
ard
ratio
of
stop
ping
feed
ing
in 2
4 w
eeks
Onl
y le
ss e
duca
ted
did
not b
reas
t-fee
d at
all.
Pre
dict
ors o
f par
tial
brea
st-f
eedi
ng 1
st w
eek:
you
ng m
othe
rs>l
ess e
duca
tion>
deliv
ery
type
& a
nalg
. GA
>epi
>N2O
>non
e>pe
thid
ine!
Afte
r adj
ustin
g fo
r de
liver
y ty
pe a
nd p
arity
, epi
dura
l eff
ect N
S. B
reas
t-fee
ding
at 2
4 w
eeks
: no
anal
g 72
%; n
o ep
idur
al 6
4%; e
pidu
ral:
52%
. Pre
dict
ors
of st
oppi
ng in
24
wee
ks: y
oung
>edu
catio
n>an
alg
Will
und
2009
re
trosp
ectiv
e al
l ep
idur
als;
co
ntro
ls m
atch
ed
for p
arity
, age
an
d ge
stat
ion
Usu
ally
bup
+suf
enta
nil
bolu
s or i
nfus
ion
± pa
race
rvic
al a
nd/o
r pu
dend
al b
lock
(3
51)
Not
hing
or p
arac
ervi
cal
and/
or p
uden
dal b
lock
N
o op
ioid
(3
51)
Bre
ast f
eedi
ng in
1st 4
h; a
rtific
ial
milk
giv
en; b
reas
t fee
ding
at
disc
harg
e
Bab
ies i
n th
e ep
idur
al g
roup
wer
e le
ss li
kely
to b
reas
t fee
d in
the
first
4 h
(OR
3.79
), m
ore
likel
y to
be
give
n ar
tific
ial s
uppl
emen
t (O
R 2
.19)
and
less
like
ly to
be
brea
st fe
edin
g at
dis
char
ge (O
R
1.79
)
Wils
on 2
009
CO
MET
plu
s no-
epid
ural
con
trols
m
atch
ed fo
r pa
rity,
del
type
an
d et
hnic
ity
CSE
+low
-dos
e bu
p+fe
nt b
olus
(351
) or
LDI:
low
-dos
e bu
p+fe
nt in
fusi
on (3
50)
or h
igh-
dose
bup
bol
us
(353
)
Peth
idin
e (1
51) o
r no
anal
gesi
a (2
00)
Inte
rvie
wed
24-
48 h
?in
itiat
ed
brea
st fe
edin
g. P
osta
l que
stio
nnai
re
12 m
onth
s: d
urat
ion
of b
reas
t fe
edin
g
Num
ber i
nitia
ting
brea
st fe
edin
g: a
ll ep
idur
al g
roup
s and
no-
peth
idin
e gr
oup
NS;
pet
hidi
ne g
roup
low
er in
itiat
ion
rate
s.
Dur
atio
n N
S
N
BT:
Nat
iona
l Birt
hday
Tru
st
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
132

Session 10: Pre-eclampsia Revisited Obstetric issues Dr Maggie Blott Consultant Obstetrician, University College London Hospitals
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
133

Trophoblast invasionTrophoblast invasion
•• CTBs invade and extend through CTBs invade and extend through out the decidua and inner third of out the decidua and inner third of myometriummyometrium
•• Remodeling of the spiral arteries Remodeling of the spiral arteries probably begins in the late first probably begins in the late first trimester and is completed by 18trimester and is completed by 18--20 weeks of gestation20 weeks of gestation
TwoTwo--stage evolution in prestage evolution in pre--eclampsiaeclampsia
plusplus
•• prepre --existing existing maternal conditionmaternal condition(obesity, BP(obesity, BP ↑↑↑↑↑↑↑↑))
•• genetic genetic predispositionpredisposition
•• pregnancy factorspregnancy factors(twins etc) (twins etc)
Soluble angiogenic factors Soluble angiogenic factors –– ‘‘sFltsFlt--11’’
‘‘Soluble FltSoluble Flt--11’’
•• Produced from placenta Produced from placenta –– a receptor that binds: a receptor that binds: -- PlGF PlGF (Placental Growth Factor) (Placental Growth Factor) --VEGF (Vascular Endothelial Growth Factor)VEGF (Vascular Endothelial Growth Factor)
•• sFltsFlt--1 1 ↑↑ in months 8in months 8--9 in normal pregnancy9 in normal pregnancy
•• Significant Significant ↑↑ ↑↑ in preeclampsiain preeclampsia
•• Changes are detectable 5 weeks before clinical diseaseChanges are detectable 5 weeks before clinical disease
Levine et al NEJM 2004Levine et al NEJM 2004
So what does sFltSo what does sFlt--1 do?1 do?
1.1. When present in circulation, sFltWhen present in circulation, sFlt--1 1 BINDSBINDS to VEGF and to VEGF and PlGFPlGF
2.2. Prevents them from binding to cell surface receptorsPrevents them from binding to cell surface receptors
3.3. Leads to a state of ENDOTHELIAL DYSFUNCTIONLeads to a state of ENDOTHELIAL DYSFUNCTION
PredictionPrediction
UADV as a Screening TestUADV as a Screening Test
Mires; PreMires; Pre--eclampsia, RCOG 2003eclampsia, RCOG 2003
•• Bilateral UA Bilateral UA ‘‘notchingnotching’’
•• Best PPV Best PPV –– 21% for proteinuric PIH21% for proteinuric PIH
•• RR 26 (11RR 26 (11--64) for 64) for ‘‘severe PE & delivery <34 wkssevere PE & delivery <34 wks’’
UTERINE ARTERY DOPPLER VELOCIMETRYUTERINE ARTERY DOPPLER VELOCIMETRY
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
134

‘‘sFltsFlt--11’’ –– A Predictive Role?A Predictive Role?
Stepan et al NEJM 18 Nov 2004Stepan et al NEJM 18 Nov 2004
PreventionPrevention
Prior studiesPrior studies
05
10152025
Number of women with
pre-eclampsia
Intention-to-treat
Completedstudy
Placebo
Vitamins C and E
Adjusted OR: 0.39 (0.17-0.90)p=0.02
0.24 (0.08-0.70)p=0.002
Vitamins In PreVitamins In Pre--eclampsia (VIP)eclampsia (VIP)
• Vitamin C & E
• No difference in rates of pre e clampsia
• Increase in low birth weight babies in Vitamin grou p
Aspirin in preAspirin in pre--eclampsiaeclampsia
Askie LM; Lancet 2007Askie LM; Lancet 2007
•• Meta analysisMeta analysis >32 000 women & babies>32 000 women & babies
Antenatal ManagementAntenatal Management
Antenatal Management
1. Screen for women at high risk
2. Interventions
3. Medical management
4. Timing of delivery
5. Mode of delivery
NICE Guidelines NICE Guidelines –– ‘‘Low riskLow risk’’ Antenatal CareAntenatal Care
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
135

Treatment for mildTreatment for mild--moderate hypertensionmoderate hypertension
in late pregnancy (15 trials)in late pregnancy (15 trials) Magee et al 1999Magee et al 1999Eclampsia in the UK Eclampsia in the UK -- 20052005
M Knight (UKOSS) 2007M Knight (UKOSS) 2007
When to deliver the baby?Hyaline membrane disease
NEC
When to deliver the mother?Renal failure
Placental abruption
Mode of Delivery
Caesarean section
Induction of labour
Conclusions IConclusions I
Beware of early onset preearly onset pre--eclampsiaeclampsia
Need to recognise and treat high SBP
Early involvement of Consultant Obstetrician
Watch for fluid overload
Substandard care in hospital & community
Institute PRECOG and NICE
Beware of lateBeware of late--onset eclampsia onset eclampsia Munjuluri BMJ 2005Munjuluri BMJ 2005
Conclusions IIConclusions II
Be aware of Be aware of atypicalatypical presentationspresentations
Prediction is possible in various risk groups Prediction is possible in various risk groups
The future The future -- consider the longconsider the long--term health implications term health implications of preof pre--eclampsiaeclampsia
The future The future -- prevention with aspirin, calcium (but not prevention with aspirin, calcium (but not antianti--oxidant vitamins)oxidant vitamins)
Perhaps the complex mechanisms underlying preeclampsia Perhaps the complex mechanisms underlying preeclampsia are becoming clearerare becoming clearer……....
Consequences for womenConsequences for women ’’s healths health
Age
Neonatal period Pregnancies Middle Age
Threshold for Threshold for vascular or vascular or metabolic diseasemetabolic disease
Complicated pregnancy e.g. pre-eclampsia, gestational diabetes
Healthy
Car
diov
ascu
lar
risk
Sattar & Greer BMJ 2002Sattar & Greer BMJ 2002
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
136

Maternal MortalityMaternal Mortality
0
20
40
60
80
100
120
52-5
4
55-5
7
58-6
0
61-6
3
64-6
6
67-6
9
70-7
2
73-7
5
76-7
8
79-8
1
82-8
4
85-8
7
88-9
0
91-9
3
94-9
6
97-9
9
00-0
2
03_0
5
Eclampsia Preeclampsia
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
137

Session 10: Pre-eclampsia Revisited Medical management of pre-eclampsia Dr Lucy Mackillop Locum Consultant Obstetric Physician, John Radcliffe Hospital, Oxford
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
138

Fulminating Pre-eclampsia
Pre-eclampsia protocol
Obstetric High Dependency UnitDeliver baby
Visual disturbancesHeadache
RUQ/epigastric pain
Pre-eclampsia ProtocolBlood PressureControl
Fluid Management
Seizure Prophylaxis
Hydralazineor
labetolol iv
Fluid restrict to 85ml/h
UO <80ml/4h
CVP
MgSO4loading &
maintenance
Complications in PET
StrokeEclampsia
Pulmonary OedemaRenal Failure
HELLP Syndrome
Yorkshire Critical Care Group• n = 210,631; 16 units; 1999 - 2003.• 1087 severe pre-eclampsia or eclampsia
(5.2/1000)• 151 serious complications
– 82 (39/10,000) having eclamptic seizures and – 49 (23/10,000) requiring ICU admission.
• 82 eclampsia– 45 occurred antenatally (55%)
• 18 before admission to the maternity unit
– 11 in labour (13%)– 26 following delivery (32%).
• 25 pulmonary oedema (2.3% of cases)• 6 renal dialysis (0.55% of cases).
BJOG. 2005; 112:875-80
Blood Pressure control to reduce the risk of stroke
Stroke in Pre-eclampsian = 18 deaths due to pre-eclampsia / eclampsia– 10/18 due to ICH, 2/10 due to cerebral infarction
CEMACH (2003-05)
Martin JN et al. Obstet Gynecol 2005; 105: 246. Mississippi
• n = 28 strokes (1980-2003)– 12 antenatal– 16 post partum– 93% haemorrhagic– 7% thrombotic arterial– 54% maternal mortality– 96% systolic BP > 160 mmHg– 12.5% diastolic BP > 110 mmHg– 25% MAP > 130 mmHg
Mean rise in BP baseline pre stroke
Systolic 64.4 mmHg
Diastolic 30.6 mmHg
Hypertension in Pre-eclampsia
• Pressor affects of intubation
• Active management of 3rd stage – avoid ergometrine
Seizure prophylaxis to reduce the risk of eclampsia
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
139

Eclampsia• Affects 1 in 2000 deliveries/1-2% of
women with pre-eclampsia• ~30% precedes hypertension/proteinuria• up to 50% postnatal
• 2.2% mortality
Duley MAGPIE. Lancet 2002; 359: 1877-1890
MAGPIEMgSO4 for prevention of eclampsia
• 175 centres, 33 countries, 10,141 women
MgSO4 placebo RREclampsia 0.8% 1.9% 0.42 (0.29-0.6)Death 0.2% 0.4% 0.55 (0.26-1.14)
Duley L et al. Lancet 2002; 359: 177-90
Halves rate of eclampsia
MAGPIENo difference in rate of: • baby death / SCBU
• CS (ie. not a tocolytic)• Severe morbidity
• Antihypertensive therapy24% of MgSO4 side effects eg. flushing / N+V
Need to treat 1000 women to prevent 11 cases
NNT = 70 for severe pre-eclampsia, 90-100 for less severe pre-eclampsia
Duley L et al. Lancet 2002; 359: 177-90
Strict Fluid Balance to reduce the risk of pulmonary oedema and
acute renal failure
Renal failure in pre-eclampsia
• 1.1% Duley MAGPIE. Lancet 2002; 359: 1877-1890
• Cohort study 1995-1998 Groote Schuur, Cape Town
28000 del/yr � 588 admitted to obstetric HDU
89 severe PET + ARF (obtained 72 case notes)
– Cr>100+ oliguria <100ml/4hrs)
– Median max creatinine = 341 µmol/l
Drakeley et al. AJOG 2002; 186: 253
Renal failure in PET
• Primips 43%• Mean gestation 32 w• CRD/hypertension 16%
Dialysis: 1:13500
Short term <2wk: 10% (3/4 HELLP)
Long term dialysis 0%Renal Transplant 0%
Predictor: creatinine doubles in 1st 1-2d post admission
• HELLP 50%
• Placental Abruption 32%
• Eclampsia 16%
• Perinatal Mortality 38%
• Maternal mortality 0%
Drakeley et al. AJOG 2002; 186: 253
ARF 1:1060 deliveries
Renal failure in pre-eclampsia
• Multi-factorial• Associated with HELLP/DIC/Abruption• Addition ATN/Cortical Necrosis
• Classical glomerular endotheliosis• Renal recovery is the rule in previously
healthy women (NB pre-existing renal disease/hypertension)
Pulmonary oedema in PET
• 9 yrs, n = 37
(78% black)
• Incidence: 2.9% (older, multips)
• Antenatal 30%
• Postnatal 70%
• Maternal Mortality 11%
• Fetal Mortality 53%
Sibai et al. AJOG 1987; 156: 1174-9
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
140

Haemolysis, Elevated Liver enzymes, Low Platelets Syndrome
• incidence 1 in 1000 pregnancies
• 4-20% of women with pre-eclampsia• 21% of early-onset <30 /40• 20% may not have preceding hypertension
or proteinuria • 30% Postpartum
Guntupalli SR & Steingrub J. Hepatic disease in pregnancy. Crit Care Med 2005. Vol 33 (10)
Murphy & Stirrat. Hypertension in pregnancy 2000; 19: 221-231
HELLP - Diagnosis
Low grade haemolysisRaised LDH >600 U/LRaised unconjugated bilirubin
Abnormal LFTsRaised transaminases AST ≥70 U/L
Low / falling platelets (< 100,000)DIC (20%)
Epigastric / RUQ pain (65%); N & V (35%)
RUQ tenderness (may precede abn LFTs)
Hypertension and proteinuria (mild)
Radiology
Hepatic infarcts
Subcapsularhaematoma
Liver Biopsy
necrosis
haemorrhage
Maternal morbidity in HELLP
n = 170
• ARF 13.5%• Abruption 6.6%• Pneumonia 3%• Liver haematoma 2.3%• Pulmonary oedema 2.3%• DIC 1.7%• Cerebral haemorrhage 1.2%
Morbidity increased with lower platelet counts
Romero Arauz et al. Ginecol Obstet Mex 2001; 69: 189
Corticosteroids in HELLP
• 5 studies (n=170) – 3 antepartum, 4 vs placebo• Dexamethasone (12 mg iv 12 h) superior to
betamethasone• No difference in maternal mortality/morbidity • (abruption, pulmonary oedema, liver
haematoma/rupture)• Reduced hospital stay (- 4.5 [-7.1,-1.9] day) • Longer interval to delivery (41 vs 15 h p=0.007)• ‘Tendency to greater platelet count increase over 48h’• (40.6 [-26.2, 107.3])
• No difference in perinatal mortality/morbidity• Greater mean birthweight (247 [65,428] g)
Cochrane Database of Systematic Reviews 2003
RCT Steroids for HELLP syndrome
• N = 132, dexamethasone 10 mg 12hrly + 3 doses postpartum
• Non significant shortening of hospitalization 6.5 vs 8.2 days
• No difference in– time to recovery of platelet counts– lactate dehydrogenase– aspartate aminotransferase– development of complications
• Results were found in both pregnant and puerperal women.
Fonseca JE et al. Am JOG 2005; 193: 1587
Effect of corticosteroids on regional anaesthesia rates
69 patients with HELLP
Steroid no steroidMean fall plts (ad to del) 4 x 109 15 x 109
No. with ↑ plts 15 1Mean plts at deliv 88 x 109 72 x 109
Regional anaesthesia 43% 35%
O’Brien JM et al. Am JOG 2002; 186:475-9
Effect of corticosteroids on regional anaesthesia rates
37/69 patients with HELLP and plts < 90 x 109
Steroid no steroidRegional anaesthesia 42% 0%GA for CS 46% 100%24 hr latency 54%RA if 24 hr latency 57% 0%GA if 24 hr latency 22% 100%
O’Brien JM et al. Am JOG 2002; 186:475-9
Management of Pre-eclampsia
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
141

Blood Pressure Control
Chronic• Methyl dopa• Nifedipine, hydrallazine• Labetalol, alpha blocker
Acute• IV labetalol• IV hydralazine• Oral nifedipine (not with MgSO4)
Drugs not used
• ACEI
• ARB• Diuretics
Keep BP < 160/100
Fluid Management• Post delivery oliguria is common
– ADH↑/Angiotensin II↑/ANP↑↓– Oxytocin– Vasodilators– Low albumin– ‘Third space’ losses– Non-steroidal anti inflammatory drugs
• Anuria is a blocked catheter or obstructed ureters until proved otherwise
• Measure Mg levels if on MgSO4
Fluid management• Assess patient first
– Clinical – Thirst, JVP, Hand veins, Lung bases– Non-invasive monitoring - Pulse oximeter, chest x-ray– Invasive monitoring - CVP (2-6)– Urine vol <0.5ml/kg/hr over 4 consecutive hours (80
mls/4hr)– Check biochemistry, exclude DIC, blood loss
• Reassess patient– Hartmann’s @ 1ml/kg/hr if not taking oral fluids– Do not use dextrose unless diabetic– No advantage of colloid, albumin and blood unless
abnormal loses
• Repeat assessment at least every 4 hours
Fluid management
• Avoid fluid overload
• Do not use >1 ‘fluid challenge’
• Avoid diuretics except in pulmonary oedema• No evidence that dopamine improves long term
outcome
• ATN does not kill but pulmonary oedema and ARDS does
Seizure Control & Prevention
Acute Management of seizure
• Lorazepam 2mg IV• MgSO4 infusion
Prevention
•MgSO4•IV 4g loading dose (over 5 minutes)•IV infusion 1g/hr•2-4g for recurrent seizures•Monitor level if:
OliguriaRenal impairmentSigns of toxicityLow BMI
HELLP - Management
• Control BP
• Fluid restrict
• Correct coagulopathy (FFPFFP ± Platelets)
• Deliver
• Steroids of no benefit
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
142

Additional management
• Thromboprophylaxis
• No NSAIDs
Postpartum Hypertension
• BP rises after normal delivery, reaching a peak at 3-4 days
• Methyldopa should be stopped / avoided
• Atenolol / Calcium antagonist / ACEI
SummarySummary
PrePre--eclampsiaeclampsia• is common and dangerous• always surprises
• Endothelial damage leads to a multi-system disorder of protean manifestations
• requires clear and agreed management plans
• should be managed on the labour ward
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
143

Session 10: Pre-Eclampsia Revisited Anaesthetic Issues Dr Robin Russell Consultant Anaesthetist, John Radcliffe Hospital, Oxford
Hypertensive disease in pregnancy remains one of the leading causes of maternal mortality in the UK. In the 2003-05 CEMACH report there were 18 deaths directly attributed to eclampsia or pre-eclampsia,1 a small increase from the previous report.2 Although the number of deaths has fallen in recent enquiries, nearly half of the reported cases showed features of substandard care. Antenatal Assessment The 2000-02 CEMACH report highlighted the need for early diagnosis and treatment of hypertension. There was a call for clear written protocols and input from senior obstetricians, anaesthetists and intensive care specialists. Poor communication and teamwork, and a lack of appreciation of the severity of illness, with failure to involve senior staff, have been recurring themes in both CEMACH and CEMD reports. For effective multi-disciplinary care, women with significant co-existing disease should be referred for anaesthetic assessment as early as possible during pregnancy. Those with hypertensive disease are more likely to require the services of an anaesthetist during labour and delivery and early consultation allows time to assess the severity of illness and current management following which options for analgesia and anaesthesia can be discussed. A recent claims that antepartum continuous infusion of epidural ropivacaine reduces uterine artery vascular resistance warrants further investigation.3
The 2003-05 report emphasised the need to control blood pressure adequately before inducing general anaesthesia for caesarean section (see below) especially when there was a desire to delivery the baby urgently. Labour Analgesia Regional analgesia is recommended for women with hypertensive disease. It provides superior pain relief when compared to systemic or inhalational analgesia,4 and prevents further surges in blood pressure associated with autonomic activity. Epidural analgesia promotes uteroplacental blood flow5 and results in improved umbilical blood gases.6 Furthermore, it can be readily extended to provide regional anaesthesia for instrumental delivery or caesarean section.
Regional blocks are contraindicated in the presence of abnormal coagulation as vascular trauma with
either needle or catheter has the potential to cause neurological damage, although in the obstetric population this is extremely rare. As thrombocytopenia is a recognized feature of hypertensive disease a recent platelet count should be performed to assess suitability of regional analgesia. Ideally this should be taken on admission to the labour ward and, for those with severe disease, repeated every six hours. Both the absolute number and rate of decline guide the anaesthetist to the risk of spinal haematoma. If the total platelet count is below 75 x 109/L or the number has dropped by more than 50 x 109/L in the previous 12 hours, many anaesthetists would avoid performing a regional block. Faced with such results the risks and benefits should be assessed on an individual basis by senior clinicians.7 Despite the publication of a number of case reports in which neuraxial blocks have been placed without complication in thrombocytopenic patients the risk of spinal haematoma must not be overlooked.8
Risk assessment should include history, examination, and evaluation of blood tests. Clotting studies are often performed when the platelet count falls below 100 x 109/L but are frequently normal. Bleeding times are not considered to be of benefit.9 Thromboelastography (TEG) measures whole blood coagulation although does not take into account the initial reaction between platelets and vessel wall. Changes in the maximum amplitude on the TEG are seen in pre-eclamptic women with platelet counts below 100 x 109/L.10 However, a normal TEG cannot predict the safety of regional anaesthesia in the presence of pre-eclampsia. Platelet function analyzers have so far failed to gain widespread popularity in clinical practice, although in severe pre-eclampsia they have been shown to detect impaired haemostatic function.11,12 Further assessment of coagulation is also necessary before removing an epidural catheter as there is again a risk of vascular damage and haematoma. Anaesthesia for Delivery Women with pre-eclampsia are more likely to require caesarean section. The decision whether to use regional or general anaesthesia is based both on the severity of pre-eclampsia and the urgency of delivery. Regional anaesthesia is usually preferred as it is associated with reduced maternal mortality and
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
144

morbidity. General anaesthesia is reserved for cases where regional block is contraindicated (see below), has failed or there is inadequate time to perform or extend a block. General Anaesthesia: In the presence of coagulopathy, pulmonary oedema or impaired consciousness, general anaesthesia is usually preferred. Pre-operative assessment should be as thorough as time permits. Difficult intubation should be anticipated. Upper airway narrowing is more common in pre-eclamptic women,13 and laryngeal oedema has been reported. At induction an exaggerated hypertensive response to laryngoscopy is to be expected;14 this increases the risk of precipitating pulmonary oedema or intracerebral bleeding.15 A number of drugs have been used to obtund this reflex, including lidocaine, short-acting opioids, magnesium and labetolol. Of these alfentanil is most widely used in the UK,16 possibly reflecting increased familiarity with this drug. A combination of alfentanil and magnesium has been shown to be more effective than either used alone.17 More recent interest has focused on remifenantil which blunts the hypertensive response to laryngoscopy in both non-hypertensive women18 and those with pre-eclampsia,19 although transient neonatal respiratory depression may result.18 The hypertensive response to extubation should not be overlooked. Potentiation of non-depolarising muscle relaxants by magnesium is not usually problematic,20 although monitoring neuromuscular function is necessary. Regional Anaesthesia: Despite concerns over hypotension, the effects of vasoconstrictors and excessive intravenous fluid administration, it is now widely accepted that, in the hands of an experienced anaesthetist, a regional technique is preferred for caesarean section in the pre-eclamptic patient.21,22 It was originally believed that because of reduced maternal plasma volume and the need to avoid large intravenous fluid boluses in pre-eclampsia, the rapid onset of autonomic block with spinal anaesthesia was best avoided. Fears that spinal, compared to epidural, anaesthesia might provoke excessive hypotension have been dispelled by a number of studies.21, 23-26 Furthermore it has been demonstrated that compared to healthy women, those with pre-eclampsia experience less hypotension and require smaller doses of vasoconstrictors with spinal anaesthesia.27-29 The effect of spinal anaesthesia on cardiac output has also been assessed. Using lithium dilution cardiac output (LiDCO) measurement in 15 women with severe pre-eclampsia, it has been shown that cardiac output remains stable during caesarean section under spinal anaesthesia, rising only after administration of an oxytocin bolus.30 However accompanying editorials
questioned whether cardiac output was the most appropriate cardiovascular parameter to study and if LiDCO was the best method of assessment.31,32 Two theories as to why hypotension should be seen less frequently in pre-eclampsia have been suggested. Firstly it may partly result from decreased aortocaval compression due to the relatively smaller weight of the baby, although this has been discredited.29 More likely is a humoral mechanism. Endothelial vasodilator systems are altered in pre-eclampsia decreasing the relaxation of small resistance vessels. Also increased local production of factors with a potent pressor effect and increased sensitivity to pressor agents produce widespread vasoconstriction which is not altered by the autonomic block associated with spinal anaesthesia. The preferred vasoconstrictor in pre-eclampsia has yet to be determined. In healthy pregnancy there is now good evidence that phenylephrine has advantages over ephedrine. However, given the increased sensitivity to alpha agonists in pre-eclampsia, caution is still required until more evidence to support their advantage is forthcoming. High Dependency Care Maternal plasma volume expansion seen in healthy pregnancy is usually much reduced in pre-eclampsia. Blood pressure and systemic vascular resistance are increased with low or normal central venous pressure. Correlation between right and left sided pressures are poor.33 Consequently, over reliance on CVP values can lead to over transfusion and it is recognised that inappropriate fluid management in the peripartum period can lead to adverse outcome, especially if pulmonary oedema is precipitated. Indeed many women with severe pre-eclampsia require high dependency or intensive care and early involvement of intensive care specialists has been recommended.2 Fluid management in pre-eclamptic patients requires a careful balance between restriction with possible exacerbation of end-organ hypoperfusion and renal dysfunction and volume overload with pulmonary oedema. The latter is more likely in pre-eclampsia because of increased vascular permeability from endothelial damage, decreased plasma oncotic pressure and in some women, left ventricular dysfunction. The situation is more hazardous when renal dysfunction is present. Oliguria is common after delivery, more so if oxytocic drugs have been used, and does not necessarily imply volume depletion. Acute renal failure is fortunately extremely uncommon. Although a number of protocols have been suggested, there is still no consensus on the optimal type or volume of fluid that should be given. Diuretics should be used with
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
145

extreme caution and only after discussion with senior staff.
Fluid preloading before regional analgesia in labour is usually unnecessary especially when low-dose local anaesthetic mixtures are used. Aggressive preloading before regional anaesthesia for caesarean section should be avoided as it is largely ineffective and increases the risk of pulmonary oedema. For particularly severe cases invasive monitoring may be useful. Opinions differ as to precise indications but it is useful when significant fluid resuscitation is required, in severe refractory hypertension, pulmonary oedema and oliguria unresponsive to fluid therapy.34 Central venous pressure monitoring may pick up hypovolaemia but used in isolation is an unreliable guide to fluid management. Pulmonary artery catheters allow monitoring of pulmonary artery wedge pressure and cardiac output and have been advocated in cases where assessment of left ventricular pre-load is important.35 However, recent evidence has questioned their effectiveness.36 Less invasive haemodynamic monitoring, such as whole body impedance cardiography, oesophageal Doppler and LiDCO are likely to become increasing popular.30,37
References
1. Lewis G (ed) 2007. The Confidential Enquiry into Maternal and Child Health. Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer 2003-05. The Seventh Report on Confidential Enquiry into Maternal Deaths in the United Kingdom. London: CEMACH.
2. Why Mothers Die 2000-2002. The Confidential Enquiry into Maternal Deaths in the United Kingdom. London: RCOG Press: 2004.
3. Ginosar Y, Madjari M, Hoffman A et al. Antepartum continuous epidural ropivacaine therapy reduces uterine artery vascular resistance in pre-eclampsia. Br J Anaesth 2009; 102: 369-78.
4. Halpern SH, Leighton BL, Ohlsson A, Barrett JFR, Rice A. Effect of epidural vs parenteral opioid analgesia on the progress of labor. JAMA 1998; 280: 2105-10.
5. Jouppila P, Jouppila R, Hollmen A, et al. Lumbar epidural analgesia to improve intervillous blood flow during labor in severe pre-eclampsia. Obstet Gynecol 1982; 59: 158-61.
6. Reynolds F, Sharma SK, Seed PT. Analgesia in labour and fetal acid-base balance: a meta-analysis comparing epidural with systemic opioid analgesia BJOG 2002; 109: 1344-53.
7. Douglas MJ. Platelets, the parturient and regional anesthesia. Int J Obstet Anesth 2001; 10: 113-20.
8. Gaiser R. Preeclampsia: What’s new? Advances in Anesthesia 2008; 26: 103-19.
9. Rodgers RPC, Levin J. A critical reappraisal of the bleeding time. Semin Thromb Hemost 1990; 16: 1-20.
10. Sharma SK, Philip J, Whitten CW, et al. Assessment of changes in coagulation in parturients with pre-eclampsia using thromboelastography. Anesthesiology 1999; 90: 385-90.
11. Beilin Y, Arnold I, Hossain S. Evaluation of the platelet function analyser vs. the thromboelastogram in the parturient. Int J Obstet Anesth 2005; 15: 7-12.
12. Davies J, Fernando R, Hallworth SP. Hemostatic function in healthy pregnant and preeclamptic women: an assessment using the platelet function analyzer and thromboelastograph. Anesth Analg 2007; 104: 416-20.
13. Izci B, Riha RL, Martin SE et al. The upper airway in pregnancy and pre-eclampsia. Am J Respir Crit Care Med 2003; 167: 137-40.
14. Hodgkinson R, Husain FJ, Hayashi RH. Systemic and pulmonary blood pressure during caesarean section in parturients with gestational hypertension. Can Anaesth Soc J 1980; 27: 389-94.
15. Ramanathan J, Angel JJ, Bush AJ, Lawson P, Sibai B. Changes in middle cerebral artery blood flow velocity associated with general anesthesia in severe preeclampsia. Anesth Analg 1999; 88: 357-61.
16. Wright WJ, Bythell V. Caesarean section for severe preeclampsia: a survey of UK consultant obstetric anaesthetic practice. Int J Obstet Anesth 2003; 12: S36.
17. Ashton WB, James MFM, Janicki P, Uys PC. Attenuation of the pressor response to tracheal intubation by magnesium sulphate with and without alfentanil in hypertensive proteinuric patients undergoing caesarean section. Br J Anaesth 1991; 67: 741-7.
18. Ngan Kee WD, Khaw KS, Ma KC et al. Maternal and neonatal effects of remifentanil at induction of general anesthesia for caesarean delivery. Anesthesiology 2006; 104: 14-20.
19. Yoo KY, Jeong CW, Park BY et al. Effects of remifentanil on cardiovascular and bispectral index responses to endotracheal intubation in severe pre-eclamptic patients undergoing caesarean delivery under general anaesthesia. Br J Anaesth 2009; 102: 812-9.
20. Dyer RA, Piercy JL, Reed AR. The role of the anaesthetist in the management of the pre-eclamptic patient. Curr Opin Anaesthesiol 2007; 20: 168-74.
21. Wallace DH, Leveno KJ, Cunningham FG et al. Randomized comparison of general and regional anesthesia for cesarean delivery in pregnancies complicated by severe preeclampsia. Obstet Gynecol 1995; 86: 193-9.
22. Dyer RA, Els I, Farbas J et al. Prospective randomized trial comparing general with spinal anaesthesia for caesarean delivery in preeclamptic patients with nonreassuring fetal heart trace. Anesthesiology 2003; 99: 561-9.
23. Hood DD, Curry R. Spinal versus epidural anesthesia for cesarean section in severely preeclamptic patients. Anesthesiology 1999; 90: 1276-82.
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
146

24. Sharwood-Smith G, Clark V, Watson E. Regional anaesthesia for caesarean section in severe preeclampsia: spinal anaesthesia is the preferred choice. Int J Obstet Anesth 1999; 8: 85-9.
25. Visalyaputra S, Rodanant O, Somboonviboon W et al. Spinal versus epidural anesthesia for cesarean delivery in severe preeclampsia. Anesth Analg 2005; 101: 862-8.
26. Chiu CL, Mansor M, Ng KP, Chan YK. Retrospective review of spinal versus epidural anaesthesia for caesarean section in preeclamptic patients. Int J Obstet Anesth 2002; 12: 23-7.
27. Aya AGM, Mangin R, Vialles N et al. Patients with severe preeclampsia experience less hypotension than healthy parturients. Anesth Analg 2003; 97: 867-72.
28. Clark VA, Sharwood-Smith GH, Stewart AVG. Ephedrine requirement are reduced during spinal anaesthesia for caesarean section in preeclampsia. Int J Obstet Anesth 2004; 14: 9-13.
29. Aya AGM, Vialles N, Tanoubi I et al. Spinal anesthesia-induced hypotension: a risk comparison between patients with severe preeclampsia and healthy women undergoing preterm cesarean delivery. Anesth Analg 2005; 101: 869-75.
30. Dyer RA, Piercy JL, Reed AR et al. Hemodynamic changes associated with spinal anesthesia for caesarean delivery in severe preeclampsia. Anesthesiology 2008; 108: 802-11.
31. Langesaeter E. Is it more informative to focus on cardiac output than blood pressure during spinal anesthesia for caesarean delivery in women with severe preeclampsia? Anesthesiology 2008; 108: 771-2.
32. Pauca AL. Pressure wave analysis is useful to understand the pathophysiology of preeclampsia but perhaps not the rapid changes during caesarean delivery. Anesthesiology 2008; 108: 773-4.
33. Young P, Johanson R. Haemodynamic, invasive and echocardiographic monitoring in the hypertensive parturient. Best Pract Clin Obstet Gyaecol 2001; 15: 605-22.
34. Englehart T MacLennan FM. Fluid management in pre-eclampsia. Int J Obstet Anesth 1999; 8: 253-9.
35. Martin SR, Foley MR. Intensive care in obstetrics. Am J Obstet Gyencol 2006; 195: 673-89.
36. Harvey S, Harrison DA, Singer M. Assessment of the clinical effectiveness of pulmonary artery catheters in the management of patients in intensive care (PAC-Man). Lancet 2005; 366: 472-7.
37. Tihtonen K, Koobi T, Yli-Hankala A, Huhtala H, Uotila J. Maternal haemodynamics in pre-eclampsia compared with normal pregnancy during caesarean delivery. BJOG 2006; 113: 657-63.
OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009
147

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 Notes
148

OAA: Three-day Course on Obstetric Anaesthesia and Analgesia, London, 9 – 11 November 2009 Notes
149

Obstetric Anaesthetists' Association
Three-day Course on ObstetricAnaesthesia and Analgesia
Organised by Dr Roshan Fernando, University College London Hospitalsand Dr Chris Elton, University Hospitals of Leicester
Formed 1969. Registered Charity 1111382
Promoting the highest standards of anaesthetic practice in the care of mother and baby
9 – 11 November 2009Church House Conference Centre, Westminster, SW1P 3NZ
LONDON
LECTURE ABSTRACTS
OAA Secretariat, PO Box 3219 Barnes, London SW13 9XR UKTel: +44 (0)20 8741 1311 • Fax: +44 (0)20 8741 0611 • For email contact and all details: www.oaa-anaes.ac.uk
ObstetricAnaesthetists’Association
Obstetric Anaesthetists’ AssociationPromoting the highest standards of anaesthetic practice in the care of mother and baby
20 - 21 May 2010 (evening reception 19 May) The Sage, NewcastleGateshead
Obstetric Anaesthesia 2010
Enquiries: OAA Secretariat T: +44 (0) 20 8741 1311 F: +44 (0) 20 8741 0611 www.oaameeetings.info
Registered Charity 1111382
FUTURE MEETINGS & COURSES
2010 3 March 2010 Cases and Controversies in Obstetric Anaesthesia, London
19 - 21 May 2010 Obstetric Anaesthesia 2010 (Reception 19 May, Annual Meeting 20 & 21 May), The Sage, NewcastleGateshead
13 October 2010 Refresher Day on Obstetric Anaesthesia and Analgesia, London
8 - 10 November 2010 Three-day Course on Obstetric Anaesthesia and Analgesia, London
10 December 2010 Joint meeting with Royal Society of Medicine (Section of Anaesthesia and Section of Obstetrics and Gynaecology), London
201125 - 27 May 2011 Obstetric Anaesthesia 2011 (Reception 25 May, Annual Meeting 26 & 27 May),
Edinburgh
201223 - 25 May 2012 Obstetric Anaesthesia 2012 (Reception 23 May, Annual Meeting 24 & 25 May),
Liverpool
201322 - 24 May 2013 Obstetric Anaesthesia 2013 (Reception 22 May, Annual Meeting 23 & 24 May),
Bournemouth
OAA Secretariat, PO Box 3219 Barnes, London SW13 9XR UKTel: +44 (0)20 8741 1311 • Fax: +44 (0)20 8741 0611 • For email contact and all details: www.oaa-anaes.ac.uk
Obstetric A
naesthetists’ Association ● Three-day C
ourse N
ovember 2009