Embed Size (px)
Citation preview

ABSTRACTS
Abstracts of the Winter Anaesthetic Research SocietyMeeting (ARS)The Royal College of Anaesthetists, London, UK, October 1–2, 2013
(The name of the person presenting the paper is shown in bold type. All authors have certified that, where appropriate, studies havebeen conducted with the approval of the relevant Human Ethics Committee or Animal Experimental Review Committee.)
Communication within operating theatres:a multicentre service evaluationK. Bauchmuller, M. Faulds, J. Rosser, D. Miller,G. H. Mills and I. WrenchSheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK
The drive forenhanced patient safety has led to thewidespreadimplementation of surgical safety checklists.1 We examinedaspects of theatre communication surrounding surgicalsafety checklists throughout our region, using a newly estab-lished trainee-led audit and research collaboration (SHARC),which is partly inspired by a model from the Southwest Penin-sula (SWARM).
We conducted a service evaluation across seven hospitalsover a 6 week period. Electronic data capture and paperforms were used to prospectively collect data from a largevariety of theatres, spanning all major surgical specialities.The project was approved by all trusts’ Clinical Governanceand Information Governance departments.
Datawere collected from 392 theatre listscovering 19 differ-ent surgical specialities. Formal team briefs were held in 85% oftheatre lists. Only 58% of these had all medical members of theteam present, with surgical consultants and surgical traineesmissing in 11% and 30% of cases, respectively, comparedwith a 5% non-attendance rate for each of their anaestheticcounterparts. Ninety-two percent of the time, however, the an-aesthetist felt the team brief had been adequate. Holding ateam brief was not associated with a delay (.10 min) in thestart of a theatre list (32% with team brief vs 37% without,P ¼ 0.47, x2 test). A surgical safety checklist was completedin 96% of theatre lists and the anaesthetist thought it hadbeen done properly in 90% of cases. Introduction by nameand role occurred in 58%. Subsequently, consultant anaesthe-tists and consultant surgeons knew each other’s names in 93%of theatre lists, whereas only 30% of trainee anaesthetists andtrainee surgeons could name each other. The majority ofanaesthetists (85%) found routine introductions useful and74% would find it helpful to have a whiteboard with namesand roles in theatre.
Completion of both ateam brief and surgical safety checklistare widely established across our region. However, there is stilla mismatch between our perception and the actual quality ofthese routine safety procedures, shown by inconsistent attend-ance at team briefs and poor rate of introductions, which forman essential part of the ‘time out’ step in the checklists. Further-more, trainees’ knowledge of their counterpart trainee collea-gues appears to be poor. The aviation industry places strongemphasis on their ‘first names only’ rule, reducing potentialbarriers to effective communication.2 In the theatre environ-ment, it is highly desirable to ensure knowledge of each col-league’s name and role, particularly across the large andoften complex teams. We therefore advocate the consistentuse of whiteboards with all names and roles for all theatrecases.
References1 Haynes AB, Weiser TG, Berry WR, et al. N Engl J Med 2009; 360: 491–9
2 Lewis GH,Vaithianathan R, Hockey PM, et al. Milbank Q 2011; 89: 4–38
Evaluation of the influence of ASAclassification on duration of anaestheticpre-assessment consultation timeR. Hawes1, J. Andrzejowski2, I. Goodhart2,G. Mills2 and M. Berthoud2
1The University of Sheffield School of Medicine and 2SheffieldTeaching Hospitals NHS Foundation Trust, Sheffield, UK
At Sheffield Teaching Hospitals, all patients undergoing an-aesthetic preoperative assessment are allocated the sameduration of time with a nurse practitioner, leading to poten-tial inefficiencies in patient flow through clinic. We have vali-dated a patient (self-completed) preoperative assessmentquestionnaire (ePAQ-PO)1 that estimates ASA status. Toevaluate the impact of introducing our online tool, werequired information on current duration of preoperative as-sessment.
British Journal of Anaesthesia 112 (1): 181–99P (2014)doi:10.1093/bja/aet373
& The Author [2014]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

After registering the project with the trust service evaluationdepartment, data were collected at the Sheffield TeachingHospital preoperative assessment units, between May 2012and January 2013. Twenty nurse practitioners recorded thefollowing information on all patients they assessed: age,speciality, estimated ASA grade, and duration of consultation.Data were analysed using SPSS 21 and subjected to ANCOVA,the Pearson product-moment correlation, and regressionanalysis.
A total of 8519 patients were fully assessed. Two hundredand twenty-one were excluded from analysis due to incom-plete time data. The mean (SD) age was 52 (18.1) yr; 55.8%were female, 20.9% were ASA I, 55.5% ASA II, 22.5% ASA III,and 1.1% ASA IV. The mean (SD) assessment duration for allpatients was 47 (16) min and for each ASA group, the meanduration was: ASA I 36 (12), ASA II 46 (14), ASA III 58 (17),and ASA IV 63 (19).
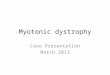
Univariate analysis found that the assessment time was sig-nificantly influenced by age, ASA grade, surgical speciality, andnurse practitioner. Gender had no effect. Figure 1 illustratesthat the duration of a preoperative assessment with a nursepractitioner increases with increasing ASA status (P,0.001).Regression analysis revealed an 11 min increase in assessmenttime for each progressive ASA grade.
Information about a patient’s ASA status as estimated byePAQ-PO would help with the efficient planning of clinics, po-tentially streamlining the preoperative assessment processand minimizing delays.
Reference1 Goodhart I, Andrzejowski J, Berthoud M, et al. Br J Anaesth 2012; 109:
655–68
Oxygen uptake efficiency slope and peakoxygen pulse predict outcome in abdominalaortic aneurysm repairB. Goodman1, E. Kothmann1, A. Batterham2,L. Cawthorn1, D. Yates3, H. Melsom4, K. Kerr5
and G. Danjoux1
1Department of Academic Anaesthesia, James Cook UniversityHospital, Middlesbrough, 2Health and Social Care Institute, TeessideUniversity, Middlesbrough, 3Department of Anaesthesia, YorkHospital, York, 4Department of Anaesthesia, University Hospital ofNorth Durham, Durham and 5Department of Anaesthesia, NorthernGeneral Hospital, Sheffield, UK
Oxygen uptake efficiency slope (OUES) and oxygen pulse havenot been extensively evaluated in the perioperative setting.Our aim was to determine the ability of OUES and oxygenpulse to predict length of stay and postoperative morbidity inabdominal aortic aneurysm (AAA) repair.
Consecutive patients undergoing cardiopulmonary exercisetesting (CPET) before elective open or endovascular infrarenalAAA repair were recruited to a prospective multi-centre obser-vational study. CPET was performed in the preoperative periodand measurements were determined byclinicians experiencedin CPET interpretation. Morbidity was measured using the post-operative morbiditysurvey (POMS). The length of stay (LOS) waslogarithmically transformed before linear regression. Onepatient who died was removed from LOS analysis.
Forty-nine patients (46 male) were recruited. Twenty-sevenunderwent open AAA repair. The mean age was 72 yr. Themedian LOS was 6 days (EVAR ¼ 4, open ¼ 8). The medianPOMS count on the third postoperative day was 2 (EVAR ¼ 0,open ¼ 3). The mean (standard deviation) of each CPET vari-able was: AT 11.3 (2.1) ml kg21 min21; peak VO2 16.2 (3.6) mlkg21 min21; VE/VCO2 34.5 (5.3); peak O2 pulse 11.6 (2.8) mlbeat21; change in O2 pulse from start of exercise to peak 6.9(2.5) ml beat21; OUES 1708 (459). The predictive ability ofeach variable is shown in Table 1.
100
80
60
40
Ass
essm
ent t
ime
(min
)
20
0
1 2
ASA grade
3 4
Fig 1 Time of consultation with nurse practitioner stratified by ASAgrade. Box shows the median and IQR. Whiskers show themaximum and minimum values excluding outliers.
Table 1 Ability of CPET variables to predict outcome. Each variablewas entered into a linear regression model with type of repair as acovariate. *P,0.05; **P,0.01
Variable Change in outcome for a1 SD increase in predictor
Mean LOS(%)
POMS counton day 3
AT (ml kg21 min21) 211 20.42
Peak VO2 (ml kg21 min21) 223* 20.33
VE/VCO2 17 0.12
OUES 230** 20.49*
Peak O2 pulse (ml beat21) 228** 20.36
Change in O2 pulse (ml beat21) 222* 20.33
BJA Abstracts of the Anaesthetic Research Society Meeting
182P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

In our study population, both OUES and peak O2 pulse weresuperior at predicting postoperative length of stay—and OUESearly postoperative morbidity—compared with conventionalCPET variables. An increase in OUES of 1 standard deviationreduced the mean length of stay by 30% [95% confidence inter-val (CI), 11–53%] and the number of POMS domains with mor-bidity by 0.49 (95% CI, 0.04–0.93). A 1 SD increase in peakoxygen pulse reduced the length of stay by 28% (95% CI, 10–48%). Ourdatasupport the use of OUES and oxygenpulse along-side conventional CPETvariables. These findings need to be con-firmed in larger samples and in other surgical populations.
Modelling neuronal synapses has thepotential to guide theories on anaestheticdrug mechanismsG. Hadjipavlou1 and J. Sleigh2
1Nuffield Department of Anaesthetics, John Radcliffe Hospital,Oxford, UK and 2Waikato Clinical School, University of Auckland,Auckland, New Zealand
A unifying theoryof anaesthetic drug mechanism eludes us. Cur-rently used experimental methods allow great spatial or tem-poral resolution but not simultaneously. We have built a modelof a synapse based on standard synaptic transmission theory in-cluding glial glutamate/gaba glutamine metabolic recycling.1
Themodelledsynapse has an excitatorycentre inhibitorysur-round receptive field made from eight inhibitory and a single ex-citatory ‘presynaptic terminal’. The receptive field is presentedwith randomly generated input to induce quantal synapticvesicle release into a theoretical synaptic cleft. The effect ofreleased excitatory and inhibitory transmitters in the synapticcleft on the post-synaptic membrane receptors is modelledusing a simple mathematical function and includes temporalsummative membrane voltage changes upon which actionpotentials are generated. The transmitter in the synaptic cleftis takenupbyatheoreticalglialcellandstoredinanunprocessedintracellular pool. This unprocessed pool is converted by a mod-elled ‘enzyme’ function into substrate which is released into thesynaptic cleft tobe takenupby the presynaptic terminalstogen-erate new transmitter vesicles. The ‘enzyme’ function does thisat a rate determined by the ratios of the unprocessed:substratepools; mimicking neuro-metabolic coupling.
1.00–40A B
C D
–50
–60
–70
–80
20 21 22 23 24 25Time (s)
Mili
volts
0.75
0.50
0.25
0.00
–0.25
50 80
70
60
50
40
30
20
10
0
40
30
20
10
0100 200 300 400 500
Time (s)
0:10 1:9 2:8 3:7 4:6 5:5 6:4Inhibiotry faciliation: metabolic suppression ratio
Cha
nge
in d
elta
ban
d po
wer
(dB
)
Freq
uenc
y (H
z)
50 80
70
60
50
40
30
20
10
0
40
30
20
10
0100 200 300 400 500 6000
Time (s)
Freq
uenc
y (H
z)
7:3 8:2 9:1 10:0
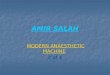
Fig 2 (A) Average pseudo-EEG output from four synapses (5 s sample). (B) Delta band absolute power change related to the ratio of inhibitoryfacilitation: metabolic suppression. (C) Spectogram of pseudo-EEG from four modelled synapses. (D) Spectogram of four modelled synapseswith abolished metabolism for 200 s.
Abstracts of the Anaesthetic Research Society Meeting BJA
183P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Drug action is simulated at: (i) the excitatoryand (ii) inhibitoryportionsof the post-synaptic membranefunction, (iii) the rateatwhich unprocessed transmitter is converted to substrate mim-icking drug–metabolic interaction, and (iv) the presynapticrelease of vesicles. These parts of the synaptic transmissioncycle were chosen to provide the unique opportunity to separatedifferent potential synapse drug interactions and estimatewhatproportions a real life anaesthetic might effect each synaptictransmission component by attempting to replicate real data.
Initial modelling based on four synapses produces a com-posite EEG output and spectrogram (Fig. 2A). To produceanaesthesia induced EEG delta band (1–3 Hz) changes,2 con-siderably more inhibitory ‘receptor’ facilitation is requiredthan metabolic suppression (Fig. 2B). Metabolic suppressionproduces wide spread reductions in all EEG bands (Fig. 2C).We hope that with further development of this model, itmight be used to guide future experiments and help revealmore about the mechanisms of anaesthetic drug action.
References1 Arhem P, Klement G, Nilsson J. Neuropsychopharmacol 2003; 28:
S40–7
2 Bak LK, Schousboe A, Waagepetersen HS. J Neurochem 2006; 98:641–53
Influence of patient posture on respiratorysignal size using RESpeckC. Whytock1, G. Drummond1, A. Bates2, J. Mann2
and D. Arvind2
1Department of Anaesthesia and Pain Medicine and 2Centre forSpeckled Computing, University of Edinburgh, Edinburgh, UK
We have developed a device (RESpeck) that provides a reliablemeasure of respiratory rate at frequent intervals in patients re-ceiving patient-controlled morphine analgesia after surgery.1
However, almost all the patients we studied were recumbentand inactive. The chest wall moves with a different patternwhen subjects are sitting because the abdominal musclesbecome tonically active.2 To assess the capacity to measurerespiration in patients who are not recumbent, we studiedwhether body orientation (e.g. sitting or recumbent) affectedthe size of the respiratory signal.
We approached 16 patients in a surgical ward to measuretheir movements. Eight had undergone surgery with generalanaesthesia and were receiving opioids for analgesia.A RESpeck device containing an encapsulated tri-axial acceler-ometer (MMA8451Q, Freescale, East Kilbride, UK) was fixedbelow the costal margin in the midclavicular line. The devicewas oriented with the Y measure directed craniocaudally, sothat the Y-axis reading would be zero if the patient anddevice were horizontal and 21 G if the patient were sitting ver-tically upright. Data were sampled at 12.5 Hz and transmittedusing Bluetooth LE to an iPod Touch (Model A1421, Apple Inc.,Cupertino, CA, USA) placed at the bedside. The axis data werecombined to generate respiratory signals analogous to flow
and volume, with a DC value of zero. The individual axissignals and combined breathing waveform were analysedusing proprietary software (Spike 2, version 5.19, CED, Cam-bridge, UK). Movement was measured as the root meansquare (RMS) of the signal amplitude.
Suitable data were obtained from 13 subjects aged 65 yr(range 48–82), mean weight 72 kg (SD¼ 20.2), mean height166 cm (SD¼ 9.5). We recorded 159 h of breathing (mean736 min per patient) and selected 100 time periods when thesubjectswere in astable bodyposition (12 h and47 minofdata).
One patient changed position very little (the 95% CI of theY-axis readings was 0.04 G). A further three patients had 95%CI values ,0.3 G. In the remainder, the Y-axis ranges (i.e. therange of posture) were 0.46 (0.34–0.54) G (median, quartiles)which we considered sufficient to influence the size of therespiratory signals. In each of these patients, we tested for acorrelation between Y-axis value and signal size. We foundno significant correlation between the mean Y-axis readingof each measurement and the RMS of the volume signal. Satis-factory signal amplitudes were present in all postures.
In this small sample of surgical patients, respiratory signalamplitude was not systematically affected by posture.
References1 Drummond G, Bates A, Mann J, Arvind D. Br J Anaesth 2011; 107:
462–9
2 Druz WS, Sharp JT. J Appl Physiol 1981; 51: 1552–6
Subclinical endotoxaemia enhances lungischaemia–reperfusion injuryH. Donaldson, K. Tatham, K. Odea, K. Wakabayashi,N. Marczin and M. TakataSection of Anaesthetics, Pain Medicine and Intensive Care, ImperialCollege London, Chelsea and Westminster Hospital, London, UK
Ischaemia and reperfusion (IR) of the pulmonary vasculature,associated with systemic inflammation due to infection or sur-gical stress, represent two principal mechanisms1 in acute lunginjury (ALI). In a mouse model of subclinical endotoxaemia,we have observed enhanced margination of inflammatoryleucocytes (Ly6Chigh monocytes and neutrophils) to thelungs, where they are primed towards secondary insults andcontribute to sepsis and high-stretch ventilation models ofALI.2,3 We hypothesized that increased lung margination andresponsiveness of inflammatory leucocytes during subclinicalsystemic inflammation would enhance the severity ofIR-induced ALI.
Subclinical endotoxaemia was induced in mice by i.v. in-jection of low-dose LPS (20 ng) in animals terminally anaes-thetized with ketamine/xylazine.2 IR injury was modelledusing an isolated perfused lung system. At 2 h after LPS injec-tion, the pulmonary vasculature was flushed with sterile per-fusate and no-flow ischaemia induced for 2 h at 378C. Thelungs were then perfused and ventilated for a further 2 h.Pulmonary oedema was assessed by lung wet–dry weightratios; lung-marginated cell number and activation by flow
BJA Abstracts of the Anaesthetic Research Society Meeting
184P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

cytometry and perfusate samples were analysed by ELISA forTNF.
Low-dose endotoxaemia was found to exacerbateIR-induced lung oedema compared with IR alone (P , 0.05).Despite flushing of the pulmonary vasculature, in thenon-LPS-treated IR group, leucocytes were largely retained inthe lungs until the end of the IR procedure [neutrophils: 2.3(0.8)×105, Ly-6Chigh monocytes: 3.1 (1.5)×105] comparedwith unflushed controls [neutrophils: 3.3 (1.8)×105, Ly-6Chigh
monocytes: 4.2 (1.4)×105]. The number of leucocytes after IRin the LPS pretreated group was significantly increased com-pared with IR controls: approximately nine-fold neutrophils(P , 0.0001), and approximately four-fold Ly6Chigh monocytes(P , 0.01). Leucocyte activation, evidenced by monocyteL-selectin shedding and increased neutrophil CD11b expres-sion, was increased in both the IR and LPS-IR groups, comparedwith untreated controls. However, perfusate TNF levels increasedonly in the LPS-IR group, whereas it was undetectable in the IRgroup.
These results suggest that latent pulmonary inflammationassociated with subclinical endotoxaemia could be an import-ant determinant of the subsequent IR-induced ALI throughthe enhanced margination of inflammatory leucocytes. Theobservation of TNF release in endotoxin-treated mouse lungsprovides evidence of priming towards IR, and is likely to repre-sent a monocyte-derived response based on patterns of TNFexpression in lung-marginated leucocytes.4
References1 de Perrot M, Liu M, Waddell TK, Keshavjee S. Am J Respir Crit Care Med
2003; 167: 490–511
2 O’Dea KP, Wilson MR, Dokpesi JO, et al. J Immunol 2009; 182:1155–66
3 Wilson MR, O’Dea KP, Zhang D, Shearman AD, van Rooijen N,Takata M. Am J Respir Crit Care Med 2009; 179: 914–22
4 O’Dea KP, Dokpesi JO, Tatham KC, Wilson MR, Takata M. Am J PhysiolLung Cell Mol Physiol 2011; 301: L812–21
Remote lung injury after renal graftischaemia–reperfusion injury in ratsH. Zhao, H. Huang and D. MaAnaesthetics, Pain Medicine and Intensive Care, Department ofSurgery and Cancer, Faculty of Medicine, Imperial College London,London, UK
Prolonged cold storage causes ischaemic injury of renal graftsand subsequent reperfusion injury after engraftment, whichhas been considered as one of the major deleterious factorsassociated with early dysfunction of transplanted grafts.12
In addition, such renal graft injury could result in remoteorgan injury, including lung. Indeed, remote lung injury is arecognized clinical complication in patients suffering fromacute renal injury and is associated with high morbidity.34
However, the acute lung injury and underlying molecularmechanisms after renal transplantation remain elusive. Theaim of this study was to investigate the acute lung injury at
histological and cellular levels in a rat syngeneic transplant-ation model.
The Lewis rat renal graft was extracted and stored in 48CSoltran preserving solution for 24 h and transplanted intothe Lewis rat recipient, the lungs were harvested 24 h aftergrafting for immunofluorescence staining and histologicalanalysis.
Cold ischaemia for 24 h in renal graft led to pulmonaryinjury 24 h after transplant surgery. The level of injury corre-lated strongly with the level of renal graft ischaemia–reper-fusion injury (IRI). Upon grafting, expression of toll likereceptor-4 (TLR-4) was significantly enhanced and nuclearfactor kappa B (NF-kB) expression and nuclear translocationwas significantly increased. The average injury score was sig-nificantly higher in the recipient receiving ischaemic renalgrafts.
Renal graft IRI triggered distant lung injury, which is likelythrough activation of TLR-4/NF-kB pathway. This study couldprovide the molecular basis for strategies to be developed toprevent or treat such complications after renal transplantation.
AcknowledgementThis work was supported by the Medical Research Council De-velopmental Pathway Funding Scheme (G802392).
References1 Perico N, Cattaneo D, Sayegh MH, Remuzzi G. Lancet 2004; 364:
1814–27
2 Grams ME, Rabb H. Kidney Int 2012; 81: 942–8
3 Canet E, Osman D, Lambert J, et al. Crit Care 2011; 15: R91
4 Deng J, Hu X, Yuen PS, Star RA. Am J Respir Crit Care Med 2004; 169:749–56
Microcirculatory and macrocirculatoryresponses in a porcine model of traumatichaemorrhagic shock and resuscitationS. Hutchings1, J. Wendon2, S. Watts3 and E. Kirkman3
1Royal Centre for Defence Medicine, Birmingham, 2Kings CollegeLondon, London and 3Defence Science and Technology Laboratory,London, UK
Haemorrhagic shock is the leading cause of preventable deathafter traumatic injury. However, our understanding of theeffects of tissue injury and haemorrhage on the microcircula-tion is incomplete. We aimed to examine the relationshipbetween the microcirculation and global systemic circulationin a porcine model of injury and haemorrhage and to assessthe impact of microcirculatory impairment on subsequentresuscitation.
Five terminally anaesthetized Large White pigs received astandardized limb injury followed by a controlled haemor-rhage (35% blood volume). After a 30 min shock, phase resus-citation was commenced with 0.9% saline to maintainhypotensive arterial pressure targets (80 mm Hg SAP) for
Abstracts of the Anaesthetic Research Society Meeting BJA
185P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

60 min. Thereafter, cross-matched porcine blood products(1:1 ratio PRBC/FFP) were administered to all animals to main-tain normotension. Sublingual SDF video microscopy was per-formed at the following time points: pre-injury baseline,shock, hypotensive resuscitation, normotensive resuscita-tion, and late normotensive resuscitation and analysed in ac-cordance with agreed consensus criteria for assessing themicrocirculation.1 Global cardiovascular parameters werealso recorded along with arterial and venous blood gas mea-surements.
Both macrocirculatory and microcirculatory parameterswere reduced during shock and hypotensive resuscitationand recovered during normotensive and late resuscitation,although not to baseline levels. Overall microcirculatory flowindex (MFI) showed a good correlation with both cardiacoutput (r ¼ 0.86; P , 0.01) and mean arterial pressure (r ¼0.78; P , 0.01). However, while the macrocirculation was uni-formly impaired, significant heterogeneity was observed inmicrocirculatory flow, particularly during the shock phase(P ¼ 0.03).
We have demonstrated that the microcirculation broadlyfollows the macrocirculation during injury, haemorrhagicshock, and subsequent resuscitation. However, the micro-circulation exhibits marked heterogeneity during low flowstates.
& Crown copyright. DSTL, 2013
Reference1 DeBacker D, Hollenberg S, Boerma C, et al. Crit Care 2007; 11:
R101
Observational study investigating bispectralindex trends in patients undergoing electivesurgical resection of non-small cell lungcancerM. Aslam1, J. Yeung1, F. Gao1, B. Naidu2, T. Melody1
and M. Wilson1
1Academic Department of Anaesthesia, Critical Care andResuscitation and 2Department of Thoracic Surgery, BirminghamHeartlands Hospital, UK
Bispectral index (BIS) monitoring is a non-invasive method ofquantifying depth of general anaesthesia (GA). Secondaryana-lysis of randomized studies has shown that prolonged deep GA,or cumulative deep hypnotic time, is associated with excessmortality.1 However, this relationship is less pronouncedwhen cancer patients are excluded,2 indicating that cancerpatients are more sensitive to deep anaesthesia or that cumu-lative low BIS (BIS , 45) is a surrogate for intrinsic vulnerabilityof this patient population. This study was performed to investi-gate depth of anaesthesia of patients undergoing thoracic
surgery for tumour resection, and if this varies with anaesthetictechnique and surgical procedure.
This prospective observational study was performedbetween Mayand July 2012. Forty patients undergoing electiveresection of non-small cell lung cancer (NSCLC) at BirminghamHeartlands Hospital (BHH), either by video-assisted thoraco-scopic surgery (VATS) or by open thoracotomy, were recruited.Before induction of anaesthesia, a BIS monitor was attachedto each patient and removed at the end of surgery. Intraopera-tive BIS data were collected blindly, and also total anaestheticand surgical times. A mean BISvalue of between 45 and 60 wasselected as the target for optimal depth of anaesthesia. Nor-mality of data was tested with the Shapiro–Wilk test, and rela-tive proportions of patients under, within, and over the targetrange were tested via x2 analysis (P , 0.05). Statistical differ-ences in means were tested via Fisher’s least significance dif-ference test (P , 0.05).
Out of the 40 patients, 15 (37.5%) had a VATS procedure,while 20 patients (50%) underwent true thoracotomies (exclud-ing VATS conversions). More patients undergoing open thora-cotomies (90%, n ¼ 18) had a mean BIS of ,45 (P , 0.05)than VATS procedures (60%, n ¼ 9). Cumulative deep hypnotictime was twice as great in patients having thoracotomy com-pared with VATS [126.6 (53.4) vs 63.6 (46.9) min, P , 0.05;mean (SD)]. In addition, the 10 patients (50% of total thoracoto-mies) who had open thoracotomy under GA and thoracic epi-dural had a mean BIS of 39.3 (SD 5.29), compared with 40.2 (SD
4.04) for the five patients (25% of total thoracotomies) whounderwent thoracotomy under GA and intrathecal morphine.
Our data show that BIS values were lower for longer inpatients undergoing surgical resection of NSCLC via openthoracotomy compared with those having VATS. Furthermore,this seems to be more pronounced in patients who have theirthoracotomy under GA and thoracic epidural. Therefore, thora-cotomy patients, anaesthetized under GA and thoracic epi-dural, may provide a suitable target population for futureinterventional studies investigating depth of anaesthesia andits effects on postoperative outcomes of surgical lung cancerpatients.
References1 Monk TG, Saini V, Weldon BC, Sigl JC. Anesth Analg 2005; 100: 4–10
2 Lindholm ML, Traff S, Granath F, et al. Anesth Analg 2009; 108:508–12
Noxious stimulation under sevofluranemonoanaesthesia in children results inan increase in d band activity in the EEGR. Poorun1, C. Hartley1, S. Goksan1, R. Rogers2,T. Ali2 and R. Slater2
1University of Oxford and 2Oxford University Hospitals NHS Trust,Oxford, UK
BJA Abstracts of the Anaesthetic Research Society Meeting
186P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

In the UK, more than 235 0001 children admitted to hospitaleach year receive an operation or investigation under generalanaesthesia. It is unknown whether noxious stimuli evoke achange in the brain activity of children receiving a general an-aesthetic. The insertion of an i.v. cannula provides an oppor-tunity to measure electrophysiological responses after aclinically noxious stimulus using EEG, EMG, and ECG. In thisstudy, we present a novel approach to investigating clinicallynoxious procedures, and demonstrate that noxious stimulievoke changes in the brain activity of the anaesthetized child.
Twenty children aged between 2 and 8 yr were studied undersevoflurane monoanaesthesia. Induction of anaesthesia wasperformed using volatile agents as per routineanaesthetic prac-tice. Once stable, patients were maintained under sevofluranemonoanaesthesia. Premedication or analgesia was not admi-nistered to any participants. Sevoflurane was kept constant atan end-tidal volume of 2.5%, relating to 1 MAC of sevofluraneacross this age range.2 Experimental noxious (pin-prick), non-noxious (tactile), and cannulation were performed on thedorsum of the hand while electrophysiological activity wasrecorded. In a subset of children, topical local anaestheticcream (Ametop) was applied to the stimulus site.
Changing patterns of neuronal activity evoked by noxiousand non-noxious stimuli were ‘time-locked’ to electrophysio-logical recordings by means of a high-speed camera and anevent-detection interface. Video recordings were captured at220 fps, a precision of 9 ms and accuracy of 4.5 ms, andtouch events marked with a precision and accuracy of 624and 256 ms, respectively.
Baseline EEG activity was dominated by d (,3Hz) and a
(8–12 Hz) band frequencies which is consistent with previouslyreported anaesthetic literature.3 The baseline remained stablethroughout the experimental protocol (P ¼ 0.23, three-wayANOVA). There was a significant increase in d band activity afterthe noxious stimuli, which was not observed after non-noxioustactile stimuli (P , 0.05, ANOVA). In the children receiving localanaesthetic, the response to noxious stimuli was diminished.No changes in EMG and ECG activity were observed after bothnoxious and non-noxious stimuli.
Studies describing the effect of noxious stimulation on theEEG during general anaesthesia describe two response patternsa ‘classical’ (shift towards high frequencies) and ‘paradoxical’(shift towards low frequencies) arousal. In animals, bothresponsescanbe elicitedbyelectricalstimulationofthereticularformation. In humans, the evoked activity is dependent onstimulus intensity, anaesthetic depth, and age. These studiesdemonstrate that noxious stimulation in anaesthetized childrenevokes a change in brain activity, even though no concomitantbehavioural or autonomic changes were observed.
References1 Cook T, Woodall N, Frerk C. Major Complications of Airway Manage-
ment in the United Kingdom, 2011. Fourth National Audit Project ofthe Royal College of Anaesthetists and the Difficult Airway Society
2 Lerman J, Sikich N, Kleinman S, Yentis S. Anesthesiology 1994; 80:814–24
3 Constant I, Sabourdin N. Paediatr Anaesth 2012; 22: 539–52
Comparison of measured vs predicted bloodpropofol concentration in childrenundergoing spinal surgery, preliminaryanalysisR. Day1, S. Panchatsharam2, M. Callaghan2
and M. Sury2
1Brighton and Sussex Medical School, Brighton and 2Great OrmondStreet Hospital for Children NHS Trust, London, UK
Target-controlled infusion (TCI) of propofol is used duringspinal surgery in children because spinal-evoked potentialsare suppressed by vapour anaesthetics. Because the dataused to develop TCI algorithms are limited, the relationshipbetween predicted and actual blood propofol concentrationsis uncertain in individual patients. Some children havingspinal surgery have had delayed return to consciousness, andcardiovascular depression has occurred, possibly caused byex-cessive blood levels. Also, during major blood loss, blood levelsmay be reduced. This pilot study aimed to identify the differ-ence between the predicted and measured blood propofol con-centration during spinal surgery.
The study had ethical committee approval and was regis-tered with MHRA. Children aged 5–18 yr undergoing spinalsurgery predicted to last over 3 h were studied. Children orparents gave written consent. Patients were excluded if theyhad major hepatic or renal disease.
During anaesthesia, propofol concentrations were mea-sured from arterial blood samples approximately every30 min: up to 10 samples per patient. Routine anaesthesiawas unaltered. The Paedfusor TCI model was used. The anaes-thetist was blinded from the propofol measurements. Propofolconcentrations were determined using a Pelorus 1500 analyser(analysis takes �3 min). Predicted propofol levels wereextracted from the TCI syringe driver and downloaded onto aPC for off-line analysis.
The performance error (PE) was calculated [PE ¼ (Cm-Cp/Cp)×100]. The main outcome of interest was the median per-formance error (MDPE) and the median absolute performanceerror (MDAPE ¼median |PE|) in each patient. MDAPE .30%was considered clinically significant. Wobble (PE–MDPE) anddivergence (regression coefficient of PE vs Time) were also cal-culated. The study aimed to recruit 20 patients. The followingdata are preliminary and are of the first 10 participants.
Participants had a median age of 13 (range 9–17) yr and amedian weight of 48 (range 24.5–95) kg. All 10 had posteriorspinal fusion surgery for scoliosis. A total of 85 samples weretaken, ranging from 6 to 10 per patient. Nine patients hadMDAPE .30%. The median MDAPE for all 10 patients was64.2% (range 216.3% to 103.3%), and the median wobblefor all patients was 13.2% (range 7.3–42.4%). Divergenceshowed a decrease in this difference over time, with themedian value recorded as ×0.3% h21 (range 21.2 to 0.1% h21).
There was a major difference between the predicted andmeasured propofol concentration: the Paedfusor model under-estimated propofol concentration. This difference was greatest
Abstracts of the Anaesthetic Research Society Meeting BJA
187P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

within the first hour of anaesthesia. Blood levels were not ex-cessively high towards the end of surgery and there was no evi-dence of propofol accumulation.
Systemic concentrations of levobupivacaineadministered by rectus sheath catheterS. Brown1, M. Daugherty3, L. Park3, J. Brittain3,M. Priston2, A. Rigby-Jones4, J. S. McGrath3
and J. R. Sneyd4
1Department of Anaesthesia and 2Department of Pharmacy,Derriford Hospital, Plymouth, 3Exeter Surgical Health ServicesResearch Unit, Royal Devon and Exeter Hospital, Exeter and4Plymouth University Peninsula Schools of Medicine and Dentistry,Plymouth, UK
Rectus sheath catheter (RSC) local anaesthetic infusions are apopular option for analgesia after midline laparotomy due tothe higher dependency and risks of perioperative epidurals.1
Concentrations of local anaesthetic during RSC infusion areunknown. Single-shot ropivacaine demonstrated a long ab-sorption profile with peak concentrations at 45 min and signifi-cant concentrations at 180 min.2 Bupivacaine concentrations.2.5 mg ml21 risk facial paraesthesia, slurred speech,3 hypo-tension,4 seizures, and cardiac arrest.
Patients undergoing cystectomy had RSCs placed underultrasound guidance after induction of anaesthesia. Twentymillilitres of 0.375% levobupivacaine were administered to
each side on the completion of surgery (dose did not exceed2 mg kg21). Top-up doses of 20 ml 0.25% levobupivacaine bi-laterally were administered every 4 h while the patient wason the intensive care unit (ICU) and every 6 h when on theward. Arterial blood samples were collected around the firstdose with pre- and post-dose samples for subsequent doseson ICU. Similarly, two venous samples were obtained on theward. Total bupivacaine concentration was measured by highperformance liquid chromatography and ultraviolet detection.
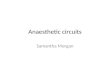
Bupivacaine concentration increased with each top-up,never reaching a plateau and passing the toxic level of2.5 mg ml21 (Fig. 3).
There is a need to review current dosing regimens and toperform appropriate dose finding studies supported by phar-macokinetic modelling.
AcknowledgementWith thanks for funding to the Royal Devon & Exeter smallgrants scheme.
References1 Cook TM, Counsell D, Wildsmith JA. Br J Anaesth 2009; 102: 179–90
2 Wada M, Kitayama M, Hashimoto H, et al. Anesth Analg 2012; 114:230–2
3 Griffiths JD, Le NV, Grant S, et al. Br J Anaesth 2013; 110: 996–1000
4 Bardsley H, Gristwood R, Baker H, et al. Br J Clin Pharm 1998; 46:245–9
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
0 200 400 600 800 1000 0 200 400
[Bup
ivac
aine
] (µg
ml–1
)
Time since first dose (min)
ICU arterial Ward venous
Ward sample time (min)
Fig 3 Plasma bupivacaine concentrations in six patients receiving levobupivacaine infusions.
BJA Abstracts of the Anaesthetic Research Society Meeting
188P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Pain during epidural catheter insertion:a prospective auditG. Churchhouse*, D. Coffey*, T. Jarbawi*,J. Williams* and Z. MilanAnaesthetic Department, St James’s University Hospital, Leeds, UK
*These authors contributed equally and their names are inalphabetical order.
Pain during epidural insertion despite local anaesthetic infiltra-tion of the skin and subcutaneous tissues is a complicationwhich is poorly understood and may be associated withadverse effects such as nausea, sweating, and the vasovagalreflex.12 Furthermore, the fear of pain during epidural insertionmay be associated with an increased risk of movement, thusincreasing the risk of injury to spinal nerves during epiduralplacement.3 This audit aimed to determine the incidence andseverity of procedural pain during epidural catheter insertionin non-anaesthetized patients.
Patients were identified using the epidural analgesia data-base (APIS) at St James’s University Hospital, Leeds, betweenSeptember 2012 and February 2013. Thirty-seven patientswere included in the audit. Patients were interviewed at thebedside using a structured questionnaire within a maximumof 48 h after operation. Pain scores were measured using avisual analogue score (VAS) 0–10. Retrospective analysis ofthe medical notes at the end of the data collection periodensured consistency of the data.
The incidence of procedural pain during epidural catheter in-sertion was 43.2% (n ¼ 16), with a mean pain score of 4.5 (2.22),range 1–10. The predominant pattern of pain was ‘brief’ (95%)and either dull (37.5%) or sharp (37.5%). Patients who werenervous before having an epidural in the sitting position hadstatistically significantly higher mean pain scores when com-pared with patients who were not nervous (P ¼ 0.02).
Mild-to-moderate pain during epidural catheter insertionwas common despite skin and subcutaneous tissue infiltra-tion with local anaesthetic before epidural catheter insertion.The impact of nervousness on procedural pain could be mini-mized by adopting measures to increase patient reassurance,
knowledge of the procedure, and familiarity with the teamand preoperative room surroundings (Fig. 4).
References1 Kinsella SM, Tuckey JP. Br J Anaesth 2001; 86: 859–68
2 Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B, Samii K. Anaesthesi-ology 1997; 87: 479–86
3 Yano T, Okubo S, Naruo H, Iwasaki T, Tsuneyoshi I. J Anesth 2010; 24:966–9
Laboratory evaluation of a novelanaesthesia delivery deviceA. Paul1, A. Wilkes2, I. Salama1, N. Goodwin2
and J. Hall21School of Chemistry and 2School of Medicine, Cardiff University,Cardiff, UK
Anaesthetic vaporizers generally consist of a means to separ-ate gas flows into two pathways: one going through the vapor-ization chamber and one as a bypass. This is required becausethe saturated vapour pressure of volatile anaesthetics is muchgreater than needed clinically. Vaporizers also tend to beheavy, bulky items of equipment to provide thermal stability.Incorrect placement on the backbar of the anaestheticmachine can lead to leaks and awareness in patients.1 Wehave developed a novel method of delivering volatile anaes-thetics where the liquid anaesthetic is formed into an emul-sion. The emulsion is contained in a compact, lightweightdevice through which all the gas flows. The extent of vaporiza-tion of the anaesthetic, and hence the vapour pressure, islimited because of the emulsion, providing controlled releaseof the anaesthetic. The concentration of delivered anaestheticis further precisely controlled bya magnetic stirrer placed in theemulsion.
Initial tests were carried out to measure the concentrationof anaesthetic delivered at temperatures ranging from 10 to308C at a flow of 1 litre min21 with the volatile anaestheticssevoflurane and isoflurane formulated separately into emul-sions. The sevoflurane formulation was prepared by mixing50 ml sevoflurane with 90 ml of aqueous Zonyl FSN-100 (acommercial non-ionic surfactant, ABCR, Karlsruhe, Germany)solution (20 w/w %). The isoflurane formulation is a mixtureof 30 ml isoflurane and 110 ml of aqueous Zonyl FSN-100 solu-tion (30 w/w %). Concentrations of anaesthetic were measuredusing a calibrated Capnomac Ultima monitor (Datex Instru-mentarium Inc., Heslinki, Finland).
The output of the device was repeatable and reproducibleand could be adjusted readily by altering the stirring rate, forexample, to maintain output at various temperatures (Fig. 5).The output could be maintained within 0.1% (v/v) of theintended setting and the device can deliver a controlled levelof anaesthetic for at least 70 min.
Forming liquid anaesthetics into an emulsion offers asimple, inexpensive method of delivering safe concentrationsof volatile agents. The water in the emulsion provides good
0
1
2
3
4
5
1 2 3 4 5 6 7 8 9 10
Num
ber
of p
atie
nts
Pain score (VAS)
Frequency of procedural pain scores
Fig 4 Frequency of procedural pain scores reported during epiduralcatheter insertion.
Abstracts of the Anaesthetic Research Society Meeting BJA
189P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

thermal stability, so that a heavy metallic container is notrequired.
Reference1 Cartwright DP, Freeman MF. Anaesthesia 1999; 54: 519–20
Effect of a perioperative haemodynamictherapy algorithm on outcomes after majorgastrointestinal surgery: a multi-centrerandomized controlled trialN. Macdonald and R. PearseRoyal London Hospital, London, UK
More than 230 million patients undergo surgery worldwide1
each year with reported hospital mortality between 1% and4%.2 Complications appear most frequent among high-riskpatients who are older patients or have co-morbid diseaseand undergo major gastrointestinal or vascular surgery.Patients who develop complications but survive to leave hos-pital often suffer reductions in functional independence andlong-term survival.3 Small trials suggest surgical outcomesmay be improved by cardiac output-guided haemodynamictherapy, but this remains uncertain.4 5 We evaluated thistreatment in specified high-risk surgical patient group.
This was a multi-centre, randomized, observer-blinded trialin 17 UK hospitals. The high-risk group was defined as patientsover 65 undergoing major gastrointestinal surgery or patientsover 50 with any of the following risk factors: diabetes mellitus,renal insufficiency, a predefined cardiorespiratory risk factor, oremergency surgery. Patients were randomized to a cardiacoutput-guided haemodynamic therapy algorithm for i.v. fluidand low-dose dopexamine during and 6 h after surgery orusual care. Randomization was performed through a secureInternet-based data entry system. Assuming a type I errorrate of 5%, 345 patients per group (690 total) were requiredto detect with 90% power a reduction in 30 day complicationsfrom 50% in the control group to 37.5% in the interventiongroup (absolute risk reduction 12.5%; relative risk reduction
25%). Allowing for a 3% one-way cross-over rate due to theuse of cardiac output monitoring in the usual care group, thiswas increased to 367 per group (734 total). An interim analysiswas performed after the recruitment of 376 patients. Prede-fined stopping guidelines permitted early termination of thetrial for harm but not effectiveness. The primary outcomewas moderate or major complications or death within 30days. Secondary outcomes included 30 and 180 day mortality.
We enrolled 734 patients between June 2010 and Novem-ber 2012; 368 patients were allocated to the haemodynamicintervention and 366 to usual care. Baseline characteristicswere similar between both groups. Patient care outside thetrial intervention was also similar, including admissions to crit-ical care. Protocol compliancewasgood with fewerthan 10% ofpatients in each group experiencing a deviation from the allo-cated intervention. This was achieved through the presence oftrained investigators where necessary, to observe, advise, ordeliver the intervention. Investigator self-assessment of blind-ing also suggested a high rate of compliance with trial proce-dures. We found that the intervention in this patient groupwas both feasible and was easily implementable.
References1 Weiser TG, Regenbogen SE, Thompson KD, et al. Lancet 2008; 372:
139–44
2 Pearse RM, Moreno RP, Bauer P, et al. Lancet 2012; 380: 1069–85
3 Khuri SF, Henderson WG, DePalma RG, Mosca C, Healey NA,Kumbhani DJ. Ann Surg 2005; 242: 326–41
4 Wilson J, Woods I, Fawcett J, et al. Br Med J 1999; 318: 1099–103
5 Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds RM, Bennett ED.Crit Care 2005; 9: R687–93
Blood transfusion and outcome after hipfracture: systematic review andmeta-analysisB. Doleman, L. Potter and I. MoppettUniversity of Nottingham, Nottingham, UK
Anaemia is common in patients with hip fracture.1 Our previousmeta-analysis showed a significant association between ad-mission haemoglobin and mortality in hip fracture patients.2
However, it is not clear if this increase in mortality is due toblood transfusion, as patients with anaemia are more likelyto be transfused than those without.3 We performed a system-atic review and meta-analysis on the association of bloodtransfusion and outcome in hip fracture.
A systematic search was conducted of MEDLINE, EMBASE,Cinahl, and AMED databases. Titles and abstracts were screenedto identify papers (n ¼ 17 747) containing data on anaemia inhip fracture patients and rejecting: duplicates; comparisons ofsurgical procedures; letters; review articles; and editorials. Full-text papers were assessed using The Newcastle–Ottawaquality assessment tool by two separate reviewers and agree-ment reached by consensus. Fourteen studies were included.Blood transfusion was associated with an increased odds ratio
3.530°C20°C10°C
3.0
2.5
Sev
oflu
rane
conc
entr
atio
n (%
)
2.0
1.5
1.00 10 20 30
Time (min)
40 50 60 70
Fig 5 Output of the device at three different temperatures. Notechange of stirring rate at about 40 min to control output.
BJA Abstracts of the Anaesthetic Research Society Meeting
190P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

of unadjusted mortality of 1.58 (1.39–1.79). When mortalitywas adjusted for confounding variables such as haemoglobinlevel, clinical status, age, sex, or mobility, the odds ratio for mor-tality was non-significant [0.99 (0.76–1.29)] as were adjustedhazard ratios [1.1 (0.98–1.23)].
Despite no difference in mortality, blood transfusion wasassociated with an increased odds ratio of infection of 2.36(1.60–3.48). This increasedrisk persisted evenwithadjusted out-comes. Although there was significant heterogeneity betweenstudies, all studies reported increased risk with transfusion.
Adjusted mortality figures show no evidence of increasedmortality in patients receiving blood transfusion in hip fracture.There is evidence that blood transfusion increases the risk ofpostoperative infection.
References1 Moppett IK, Parker M, Griffiths R, Bowers T, White SM, Moran CG. Br J
Anaesth 2012; 109: 546–50
2 Potter L, Moppett IK. Br J Anaesth 2013; 110: 869P
3 Carson JL, Duff A, Berlin JA, et al. J Am Med Assoc 1998; 279: 199–205
Evaluation of current practice with regard tothe maintenance of intraoperative arterialpressureT. Dessain and S. HowellUniversity of Leeds, Leeds, UK
Intraoperative hypotension (IOH) is common. There is evidencethatpatientswhoexperience areduction in intraoperativearter-ial pressure of ≥20% are at increased risk of complications.1 –3
The aim was to evaluate the incidence of IOH in patients under-going surgery for a fractured neck of femur.
Data were collected from 15 patients (12 males), with amedian age of 81.5 (59–95) yr. The mean arterial pressures(MAPs) were collected from the anaesthetic monitor at 5 minintervals. MAP 20% below preoperative pressure was definedas hypotension. MAP data are presented as the median(range). The burden of hypotension was calculated as thearea under the curve (AUC). Post hoc comparisons for thetype of anaesthesia and type of operation were made.
All 15 patients were .20% below their preoperative MAP formore than 5 min, and 93% (n ¼ 14) were below this thresholdfor .10 min (Fig. 6). The median duration of IOH was 65 (5–95)min. The median AUCwas 94 (3–2388) mm Hg min. Patients re-ceiving a general anaesthetic compared with neuraxial blocktended to have lower MAPs; the difference was not statisticallysignificant (P ¼ 0.13). Patients undergoing hemiarthroplastyhad lower MAPs compared with all other fracture neck offemur operations; the difference was not statistically signifi-cant in this small sample (P ¼ 0.16). The median AUC valuesfor general anaesthetic (1199 mm Hg min) were higher thanneuraxial block (466 mm Hg min). AUC values for hemiarthro-plasty were higher than those for all other fracture neck offemur operations (1492 and 635 mm Hg min, respectively).
IOH is common in patients undergoing fracture neck offemur surgery. Such hypotension may be associated with
80
60
40
20
0
–20
–40 –20 0 20 40 60 80 100 120
–40
–60
–80
–100Time from induction (min)
D B
P fr
om m
ean
preo
pera
tive
BP
(m
m h
g)
Is median operation start time
Is median operation end time
Fig 6 Median (range) perioperative MAP. Zero on the x-axis marks the point of induction and zero on the y-axis is the preoperative BP. The linemarks the IOH threshold.
Abstracts of the Anaesthetic Research Society Meeting BJA
191P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

adverse outcomes and an interventional study to intraopera-tive arterial pressure control may be justified.
References1 Monk TG, Saini V, Weldon BC, Sigl JC. Anesth Analg 2005; 100: 4–10
2 POISE Study Group, Devereaux PJ, Yang H, Yusuf S, et al. Lancet 2008;37: 1839–47
3 Bijker JB, van Klei WA, Vergouwe Y, et al. Anesthesiology 2009; 111:1217–26
Impact of sarcopenia on postoperativemorbidity in colorectal cancer patientsundergoing curative resectionK. Jones, B. Doleman, S. Shore, J. Clarke, J. Lundand J. WilliamsGraduate Medical School, University of Nottingham, Derby, UK
Preoperative identification of patients at risk of complicationsand increased length of stay after colorectal cancer resectionhas many potential benefits such as targeted post-surgicalcare, discharge planning, and risk stratification. It has beensuggested that sarcopenia (degenerative loss of musclemass) may impact on postoperative morbidity.
We identified 122 patients undergoing elective colorectalcancer resection; of which, 100 had preoperative computer-ized tomography (CT) staging scans. Lean muscle mass(LMM) was estimated using total psoas area (TPA) normalizedfor patient height. Psoas cross-sectional area was measuredat the L3 vertebral level by two independent assessors.Patient characteristic data, clinico-pathological details, andlength of stay were collected from patient notes. Com-plications were graded according to the Clavien Dindoclassification.1
Inter-rater correlation for TPA was high with an r2 ¼ 0.97.Similarly, observer assessed TPA correlated with image ana-lysis software analysis (r2 ¼ 0.94, P , 0.001). Sarcopenia wasdefined using sex-specific cut-off points of ,385 mm2 m22
for females and ,545 mm2 m22 for males2 with 15% ofpatients in our study identified as being sarcopenic. Sarcopeniawas associated with a significantly increased risk of developingmajor complications (grade ≥3, OR 5.41, P ¼ 0.01). Sarcopeniahad no effect on length of stay or time to mobilization.
Sarcopenia was associated with a significant increased riskfor major complication after colorectal cancer resection. Pre-operative CT and measurement of TPA may augment otherstrategies to identify patients at high risk of postoperativecomplications.
References1 Dindo D, Demartines N, Clavien PA. Ann Surg 2004; 240: 205–13
2 Fearon K, Strasser F, Anker SD, et al. Lancet Oncol 2011; 12: 489–95
Mechanistic profile of argonneuroprotection vs injury in vitroS. Mitchell, H. Zhao and D. MaImperial College London, London, UK
Argon has beenshown to be neuroprotective in in vivo and in vitromodels1–4 like other noble gases, namely xenon.5 However, it ischeaper and more readily available, but little is known about itsmechanism of action. Glycogen synthase kinase 3b (GSK3b) isinvolved in numerous signalling cascades, yet a link betweenthis kinase and argon has yet to be established. Perinatalhypoxic–ischaemic encephalopathy (HIE), one of the biggestcontributors to neonatal brain injury, has a high mortality rate.Twenty-five per cent of surviving individuals suffer from neuro-psychological impairment such as epilepsy.6 Current treatmentsforHIEare not fool proof with the need todiscovernew therapies.The objective of this study was to investigate the mechanismsthrough which argon is neuroprotective in vitro on cortical cul-tures looking at the cell apoptotic and cell signalling cascadesto see its potential application for HIE treatment.
For this study, cortical neuronal cell cultures (n=10) derivedfrom rat fetuses were exposed to several gases (nitrogen andargon). The neuroprotective effects of argon were analysedwith immunofluorescence staining at 4 and 24 h after treat-ment with argon alone or superposed with culture mediumdeprived of oxygen and glucose.
Argon treatment of cortical cell cultures was shown to have asignificantly higher increase in extracellular receptor kinase 1/2(ERK) compared with nitrogen [1.8 (0.9) vs 1.2 (0.8), P , 0.01and1.3 (0.5)vs2.5(1.2),P , 0.01].Therewasan increase inphos-phatidylinositide 3-kinase (P13K) 4 h after exposure [1.1 (0.5) vs1.9 (1.1),P , 0.05].Protein levelsofcleavedcaspase3[1.0 (0.1)vs0.5 (0.1), P , 0.001 and 1.0 (0.1) vs 0.9 (0.2), P , 0.05], cyto-chrome c [1.2 (0.2) vs 0.9 (0.2), P , 0.01], and GSK3b, activatedtyrosine 216 isoform [1.0 (0.1) vs 0.9 (0.1), P , 0.05 and 0.9(0.1) vs 0.7 (0.1), P , 0.01] were significantly lower in the argon-treated group compared with the nitrogen-treated group afteroxygen glucose deprivation. Argon also increased expression ofBcl-2 compared with nitrogen [2.6 (0.8) vs 1.7 (0.6), P , 0.01].
In conclusion, argon was shown to have neuroprotectiveproperties via the inhibition of the intrinsic apoptoticpathway and the up-regulation of cellular survival pathways.These data may provide increasing evidence for its use as aneuroprotectant in HIE.
AcknowledgementThis project has been supported by SPARKS, London.
References1 Brucken A, Cizen A, Fera C, et al. Br J Anaesth 2013; 110: 106–12
2 Jawad N, Rizvi M, Gu J, et al. Neurosci Lett 2009; 460: 232–6
3 Ryang Y, Fahlenkamp AV, Rossaint R, et al. Crit Care Med 2011; 39:1448
4 Soldatov PE, Smirnov IA, Smolenskaia TS, et al. Aviakosm Ekolog Med2005; 42: 45–52
BJA Abstracts of the Anaesthetic Research Society Meeting
192P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

5 Dingley J, Tooley J, Porter H, Thoresen M. Stroke 2006; 37: 501–6
6 Vannucci RC. Am J Perinatol 2000; 17: 113–20
Neurotoxic potential of N2O in vitroI. Tse, S. Savage and D. MaImperial College London, London, UK
Nitrous oxide (N2O) is commonly used as labour pain relief,1 butits potential neurotoxicity to the neonatal brain2 has beenlargely ignored. N2O causes accumulation of homocysteineby irreversibly inactivating vitamin B12, an important co-factorin the remethylation pathway.3 4 Homocysteine has beenfound to be neurotoxic due to its injurious effect on mitochon-dria.5 6 Argon, a noble gas, is neuroprotective and has thepotential to be used during labour as protection againsthypoxia/ischaemia-induced brain injury.7 The aim of thisstudy was to determine the effects of these gases, in in vitroneuronal cultures.
Primary rat cortical neurones (n=10) from E18 rats were cul-tured. For ‘pretreated’ groups only, vitamin B12 (1025 M) wasadded to the medium on plating. Cultures were exposed toN2O or argon (each at 70%, 20% O2, and 5% CO2) for 2, 4, and6 h. Additionally, homocysteine (250 mM) was added for 4 has positive control. Cleaved caspase-3 (apoptotic marker),cytochrome c (mitochondria injurious marker), and Bcl-2 ex-pression (cell survival marker) were measured with in situ im-munofluorescence staining.
All markers produced their highest levels of expression after4 h gas exposure. N2O exposure for 4 h increased caspase-3(P , 0.001), cytochrome c (P , 0.001), and Bcl-2 expression(P , 0.001). Argon exposure for 4 h increased Bcl-2 expression(P , 0.001). Vitamin B12 pretreatment reduced expression ofcaspase-3 (P , 0.001), and cytochrome c (P , 0.001) whenexposed to N2O for 4 h.
N2O has neurotoxic effects via activation of the intrinsicapoptotic pathway, which can be abolished by vitamin B12 pre-treatment. Unlike N2O, argon has no such effect but promotesneuronal survival signal. The implications of our work couldbe that argon, when combined with N2O, may preventhypoxic–ischaemic brain injury in the newborn at deliveryand may also eliminate the side-effects of N2O.
AcknowledgementSupported by Action Medical Research, West Sussex, UK.
References1 Klomp T, van Poppel M, Jones L, Lazet J, Di Nisio M, Lagro-Janssen AL.
Cochrane Database Syst Rev 2012; 9: CD009351
2 Jevtovic-Todorovic V, Beals J, Benshoff N, Olney J. Neuroscience 2003;122: 609–16
3 Culley DJ, Raghavan SV, Waly M, et al. Anesth Analg 2007; 105: 83–8
4 Drummond JT, Matthews RG. Biochemistry 1994; 33: 3732–41
5 Ho PI, Ortiz D, Rogers E, Shea TB. J Neurosci Res 2002; 70: 694–702
6 Kruman II, Culmsee C, Chan SL, et al. J Neurosci 2000; 20: 6920–6
Non-invasive measurement ofcerebrovascular response to hypercapnia inthe brainstem using arterial spin labellingN. Jenkins1, E. Warnert3, K. Murphy3, J. Hall2
and R. Wise3
1Anaesthetic Department and 2Academic Department ofAnaesthesia, University Hospital of Wales, Cardiff and 3CardiffUniversity Brain Research Imaging Centre, Cardiff, UK
The cerebrovascular response (CVR) to hypercapnia is definedas the percentage change in cerebral blood flow (CBF) perunit change in carbon dioxide. It is a potentially clinicallyuseful tool but relies on being able to accurately measure re-gional CBF. Until recently, accurate measurement of brainstemCBF using fMRI has proven difficult due to breathing andcardiac-related noise, MRI signal loss, and a high arterialblood volume that confounds measurements. Recentadvances in arterial spin labelling (ASL) techniques have pro-vided us with accurate, non-invasive measurements of region-al CBF in areas of the brain other than the brainstem. A pilotstudy published by our group showed that ASL was a suitabletechnique for studying brainstem response to hypercapnicchallenges. Here we develop our previous work and present astudy of human brainstem CVR to hypercapnia using pulsed ar-terial spin labelling.
After approval from the local research ethics committee, 10participants were recruited (seven males, three females). Eachparticipant underwent a scan with periods of normocapnia andhypercapnia. Hypercapnia was defined as an increase in end-tidal carbon dioxide of 8 mm Hg above baseline and wasachieved by mixing of medical air and 5% carbon dioxideusing a semi-closed anaesthetic breathing circuit. Multi-inversion time-pulsed ASL was carried out during bothtasks. The resulting perfusion maps enabled calculation ofCBF and therefore CVR to hypercapnia in cortical grey matterand brainstem.
Results are summarized in Table 2.Multi-inversion time-pulsed ASL has resulted in values for
grey matter CVR to hypercapnia that are similar to thosequoted in perfusion literature. The values calculated for
Table 2 Mean values (standard deviation) for brainstem and greymatter CBF at normocapnia and hypercapnia and the CVR tohypercapnia
Region ofinterest
Normocapnia Hypercapnia CVR tohypercapnia (%increase mm Hgincrease CO221)
Brainstem(ml 100 g21
min21)
43.8 (11.5) 55.7 (15.9) 3.8 (5.7)
Grey matter(ml 100 g21
min21)
52.6 (10.4) 67.3 (12.8) 3.5 (1.9)
Abstracts of the Anaesthetic Research Society Meeting BJA
193P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

brainstem CVR to hypercapnia are comparable with thoseobtained by positron emission tomography. This is the firsttime brainstem CVR to hypercapnia has been measuredusing ASL. Quantification of a person’s CVR to hypercapniacould provide optimization of CBF on an individual basis,which has potential clinical uses in patients who have sufferedcerebrovascular accidents, acute brain injury, and the peri-operative management of neurosurgical tumours.
Correlation between end-tidal and arterialcarbon dioxide measurements inneurosurgical patientsM. Wiles, Z. Harclerode, A. Leeson andJ. AndrzejowskiSheffield Teaching Hospitals NHS Trust, Sheffield, UK
End-tidal PCO2 (PE′CO2) is commonly used as a surrogate for ar-
terial PCO2 (PaCO2 ). This clinical usefulness is dependent uponthe correlation between PaCO2 and PE′CO2
, which has beenshown to be poor in the pre-hospital setting1 and in criticallyill polytrauma patients.2 The correlation between PaCO2 andPE′CO2
in neurosurgical patients has not previously beenexamined.
Over a 6 month period (February to August 2013), a retro-spective analysis of two cohorts of neurosurgical patients[level 3 patients on intensive care unit (ICU) with traumaticbrain injury (TBI) and elective neurosurgical patients] was
undertaken. Contemporaneous PaCO2and PE′CO2
measure-ments were collected from electronic records (Metavision,iMDSoft, Needham, MA, USA) and anaesthetic records. Datawere analysed using regression coefficients and the Bland–Altman plots.
Twenty-two patients were identified; 10 had undergoneelective neurosurgery [40% male, mean age (SD) 52 (16) yr]and 12 had suffered TBI and had been ventilated on ICU[92% male, mean age (SD) 43 (16) yr]. In total, 600 pairedPaCO2 and PE′CO2
measurements were analysed (39 in the surgi-cal group and 561 in the ICU group).
The correlation between PaCO2and PE′CO2
for the whole studypopulation was highly variable (Fig. 7).
The mean (SD) PaCO2 − PE′CO2difference was 0.75 (0.41) kPa
[95% confidence interval (CI) 20.05 to 1.55] for the surgicalpatients and 0.65 (0.63) kPa (95% CI 20.59 to 1.89) for theICU patients. Correlation between PaCO2 and PE′CO2
was moder-ate for the surgical patients (R2 ¼ 0.50) and poor for the ICUpatients (R2 ¼ 0.27).
In neurosurgical patients, correlation between PaCO2 andPE′CO2
is generally poor and varies significantly. PE′CO2levels
should not be relied upon to maintain PaCO2 levels within anarrow therapeutic range, and regular checking of PaCO2
values is recommended for neurosurgical patients.
References1 Prause G, Hetz H, Lauda P, Pojer H, Smolle-Juettner F, Smolle J. Resus-
citation 1997; 35: 145–8
2 Leeson A, Wiles M. J Neurosurg Anesthesiol 2013; 25: 362–3
4
3
2
1
0
–1
–22 3 4 5
Mean CO2 value ([PaCO2 + PE¢CO2
]* 0.5)
Diff
eren
ce in
CO
2 va
lues
(P
a CO
2 + P
E¢ C
O2)
6 7
Fig 7 Bland-Altman plot showing end-tidal PCO2(PE’CO2
) and arterial PCO2(PaCO2
). Bias is represented by the solid lines and the limits of agreement bydashed lines.
BJA Abstracts of the Anaesthetic Research Society Meeting
194P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Variability of cerebral oximetry ‘baseline’in patients undergoing cardiac surgeryM. Bennett1, A. MacDonald2 and A. El-Kheir1
1South West Cardiothoracic Centre and 2Plymouth UniversityPeninsula Schools of Medicine and Dentistry, Plymouth, UK
Cerebral near-infrared spectroscopy (NIRS) is increasinglybeing used as a perioperative monitor to guide anaesthesiaand clinical perfusion and is most often based on NIRS thresh-olds that predict cerebral hypoxia. While some choose an abso-lute threshold of regional cerebral oxygen saturation (rScO2),more choose a threshold based on a percentage below whatis usually termed ‘baseline’. This term is subject to two mainsources of error: first, the timing of the ‘baseline’ varies. Itmay be the period before induction of anaesthesia or immedi-ately before the insult (carotid clamping, cardiopulmonarybypass). Secondly, ‘baseline’ readings may be affected byseveral interventions. The FIO2 (0.21–1.0) varies between pub-lications. This increases the rScO2 by up to 8%12 due to an in-crease in dissolved oxygen in the blood.3 rScO2 is alsoinfluenced by the cardiac variables left ventricular (LV) functionand dilatation. The purpose of this preliminary investigationwas to define the variability in rScO2 at different time pointsaround a standard anaesthetic induction in a group of patientswith different cardiac function.
Data from 29 patients [22 men, 70 (9.6) yr] were included.rScO2 was monitored in both frontal lobes using a NIRO200NX (Hamamatsu Photonics, UK). Readings were made at‘baseline’ on room air, during 3 min of pre-oxygenation (FIO2
0.8), for 6 min after induction of anaesthesia, and for 12 minof ‘steady state’ anaesthesia (FIO2
0.3–0.5 with 1% isoflurane).Sample rate was 1 Hz (average from left and right hemi-spheres) of tissue oxygenation index (TOI), and the tissuehaemoglobin index (THI), an indexed measure of cerebralblood volume. Preoperative LV function was classed as good(ejection fraction .50%) or moderate/poor (, 50%). Datawere downloaded into an excel spreadsheet and analysedusing independent samples t-test.
Seventeen patients with a good LV had baseline TOI 68.6%(5.4), 12 with a moderate/poor LV had baseline TOI 62.4 (6.5)(P , 0.01). These increased by similar amounts during preox-ygenation and induction and intubation. At steady state, TOIwas 1.0 and 4.4 (NS) higher than baseline. The increase in TOIwas most closely associated with a significant increase in THI(cerebral blood flow and dilatation) in the patients with mod-erate/poor LV compared with those with a good LV (P ,
0.001).These preliminary data reinforce the view that the concept
of ‘baseline’ rScO2 must be more clearly defined and that vari-ables such as LV function must form part of the analysis whendefining thresholds for intervention.
References1 Picton P, Chambers J, Shanks A, Dorje P. Anesth Analg 2010; 110:
581–7
2 Stoneham MD, Lodi O, de Beer TC, Sear JW. Anesth Analg 2008; 107:1670–5
3 Tisdall MM, Taylor C, Tachtsidis I, Leung TS, Elwell CE, Smith M. AnesthAnalg 2009; 109: 906–13
Cerebral near-infrared spectroscopy duringtrans-catheter aortic valve implantation: anobservational studyA. El-Kheir1, A. Bailey2, C. Brodie1, S. Asopa1,P. Robbins1 and M. Bennett1
1South West Cardiothoracic Centre, Plymouth Hospitals NHS Trust,UK and 2Plymouth University, Plymouth, UK
Near-infrared spectroscopy (NIRS) is a non-invasive tool forassessing cerebral oxygenation. Studies in cardiac surgerydemonstrate that intraoperative cerebral desaturation leadsto a greater incidence of early postoperative cognitivedecline and prolonged hospital stay.1 During trans-catheteraortic valve implantation (TAVI), the hypoperfusion duringrapid ventricular pacing (RVP) may contribute to postoperativeoutcomes. This observational studyexamines cerebral oxygen-ation during TAVI to assess changes in cerebral oxygenationassociated with RVP.
Thirty-six patients [80.4 (5.6) yr, 18 male] undergoing TAVIwith complete perioperative NIRS data were enrolled.Bi-frontal recordings of tissue oxygenation index (TOI) weremade using a NIRO 200NX (Hamamatsu Photonics, UK) witha sampling rate of 0.5–1 Hz until 20 min after aortic valve(AV) deployment. Results were analysed in Microsoft Exceland R. Baseline TOI was calculated as the median TOI for 3and 20 min of steady-state anaesthesia before RVP. Themedian TOI was calculated for each minute after commencingRVP. Significant deviations from baseline (10% decrease) werecalculated and reported as both seconds spent 10% belowbaseline and as the area under the curve (AUC) of thesaturation-time plot (% s). Comparisons between variableswere made using the Wilcoxon signed-rank test.
There was no statistical difference in baseline TOI averagedover 3 vs 20 min of steady-state anaesthesia (P ¼ 0.800). Themedian TOI for the left and right hemispheres were 65.4%(range 37.7–81.3%) and 61.7% (49.2–82.8%), respectively.The median TOI decreased by an absolute 0.86% for theminute after RVPcommenced in the left [95% confidence inter-val (CI) 0.35–1.40%, P ¼ 0.002] and 0.55% in the right hemi-sphere (CI 0.10–1.00%, P ¼ 0.035). At 2 min post-RVP, themedian TOI were not statistically different to baseline. AfterRVP, the average time per minute spent below 10% of baselineincreased by 7.4 s (CI ¼ 4.9–13.1 s, P , 0.001) in the left and9.3 s (CI ¼ 6.1–13.9 s, P , 0.001) in the right hemisphere.The AUC increased by 24.5% (CI ¼ 11.4–39.8%, P , 0.001)and 22.8% (CI ¼ 14.6–33.1%, P , 0.001), respectively. Themedian TOI showed an absolute increase from baseline of2.35% in the left hemisphere (CI ¼ 1.2–3.3%, P ¼ 0.001) and2.05% in the right (CI ¼ 1.0–3.2%, P ¼ 0.001) at 5 min postAV deployment.
Abstracts of the Anaesthetic Research Society Meeting BJA
195P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Three minutes of steady-state anaesthesia were adequateto determine baseline TOI. The small decrease in the averageTOI that occurs after RVP is of dubious clinical significance.However, shorter periods of marked desaturation may be im-portant. Periods spent below 10% of baseline saturationswere shown to increase in the period after RVP until AV deploy-ment. Larger studies are needed with patient follow-up todetermine whether these periods are of clinical significancein the TAVI cohort.
Reference1 Slater JP, Guarino T, Stack J, et al. Ann Thorac Surg 2009; 87:
36 –44. Available from http://www.ncbi.nlm.nih.gov/pubmed/19101265
In vitro hyporesponsiveness of CD4+ andCD8+ T cells in septic patients with faecalperitonitisD. Gore1, L. Preciado-Llanes2, G. H. Mills1,2, A. Heath2
and R. Read1,2
1Sheffield Teaching Hospitals NHS Foundation Trust and 2TheUniversity of Sheffield, Sheffield, UK
Sepsis is associated with immune hyporesponsiveness. Thisstudy quantified the population differences of peripheralblood mononuclear cells (PBMCs) between septic patientswith faecal peritonitis, age- and gender-matched surgicalpatients (without sepsis), and age- and gender-matchedhealthy participants. PBMCs were stimulated with anti-CD3and anti-CD3+anti-CD28, in an in vitro model. After 4 days
incubation, T and B lymphocyte proliferation was measuredby CFSE (Carboxy-Fluorescein Succinimidyl Ester) dilutionassay. Cell activation was determined by expression ofsurface markers CD25 and CD69 on T lymphocytes and CD86on B lymphocytes. Cell viability was determined using UVlive–dead staining and an apoptosis assay.
Initial analysis of PBMC populations, on the day of bloodsampling, showed reduced percentages of CD4+ T lympho-cytes (P ¼ 0.0061) and increased percentages of CD19+ B lym-phocytes (P ¼ 0.0063) in septic patients compared with bothsurgical patients and healthy participants. In vitro, after 4days incubation, with and without stimuli, the percentage ofCD19+ B cells was higher in septic patients compared withboth surgical and healthy controls. Reduced proliferation ofCD4+ and CD8+ T lymphocytes from septic patients wasobserved when incubated with anti-CD3+anti-CD28 (P ¼0.0314), but not with anti-CD3 alone (Fig. 8). Both CD4+ andCD8+ T lymphocytes from septic patients were less activatedwhen exposed to anti-CD3+anti-CD28 stimulation (P ¼0.0328). No difference was found in levels of CD69. No differ-ences in PBMC viability were found on the day of blood sam-pling. However, in our in vitro model, across all conditions,septic patients had lower proportions of live PBMCs comparedwith healthy participants at day 4.
In summary, we demonstrated a reduction in B and Tlymphocyte populations in blood from septic patients, butnot surgical patients. We also demonstrated an in vitrofunctional impairment in response to T lymphocyte stimulitogether with reduced cell viability. Surgical patients de-monstrated a trend towards reduced T and B lymphocytenumbers. To our knowledge, this is the first attempt toperform an immune functional assay across these threegroups simultaneously.
0.8A BSepticSurgical controlHealthy control0.6
0.4
ns ns nsns
ns nsns
ns
nsns
**
*
nsns
nsns
ns
ns
******
Div
isio
n in
dex
0.2
0.0
0.8
0.6
0.4
Div
isio
n in
dex
0.2
0.0
-VE A
B-V
E
aCD3
AB
aCD3
aCD28
aCD3
-VE A
B-V
E
aCD3
AB
aCD3
aCD28
aCD3
SepticSurgical controlHealthy control
Fig 8 Demonstrating reduced CD4+ (A) and CD8+ (B) T Q5 lymphocyte proliferation in response to the stimuli anti-CD3+- anti-CD28.
BJA Abstracts of the Anaesthetic Research Society Meeting
196P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Role of the PGC1a pathway in mitochondrialfunction under conditions of sepsisM. Scullion, D. Lowes and H. GalleyAcademic Unit of Anaesthesia and Intensive Care, University ofAberdeen, Aberdeen, UK
Mitochondria are the major physiological producer of reactiveoxygen species (ROS). During sepsis, mitochondrial ROS pro-duction exceeds antioxidant defences, leading to a state of oxi-dative stress which fuels inflammation and causes directmitochondrial damage. The resulting mitochondrial dysfunc-tion and subsequent bioenergetic failure is suggested toplay a central role in sepsis-induced organ dysfunction. Dam-pening of inflammatory responses, restoration of endogenousantioxidant levels, and maintaining or restoring mitochondrialenergetic function is likely to be beneficial in sepsis. The per-oxisome proliferator-activated receptor gamma (PPARg) co-activator 1-alpha (PGC1a) pathway is a potential target due toits effects on antioxidant expression, inflammation, and mito-chondrial biogenesis (generation of new mitochondria).
Human endothelial cells were treated with bis-(2-hydroxybenzylidene) acetone (2HBA), which activates downstr-eam transcription factor targets of PGC1a, or hexadecyl-azelaoylphosphatidylcholine (Azelaoyl PAF), a PPARgactivator, at severalconcentrations, with and without lipopolysaccharide (LPS) pluspeptidoglycan G (PepG) to mimic sepsis. Mitochondrial functionwas measured in intact cells as membrane potential, metabolicactivity and mitochondrial volume, and total glutathione as anindex of oxidative stress. Interleukin-6 (IL-6) was measured inculturemediumtodetermineeffectsoninflammation.Measuresof mitochondrial function were lower in cells treated with LPS/PepG than control cells, while IL-6 concentrations were higher(Fig. 9, P , 0.001). Under conditions of sepsis, 2HBA protected
against mitochondrial dysfunction, seen as maintenance ofmembrane potential and metabolic activity, lower IL-6 andincreased mitochondrial volume and glutathione levels (all P ,
0.05). Likewise, Azelaoyl PAF maintained membrane potential,maintained metabolic activity, and increased glutathionelevels (all P , 0.05).
These data show that promoting activation of the PGC1apathway protects against mitochondrial dysfunction and in-flammation in cells under conditions mimicking those seen insepsis and may be a novel future therapeutic target.
Mitochondrial sirtuin activation inendothelial cells under conditions of sepsisG. McCreath, D. Lowes and H. GalleyAcademic Unit of Anaesthesia and Intensive Care, University ofAberdeen, Aberdeen, UK
Sepsis remains a significant cause of mortality in the popula-tion due to lack of effective treatment options. Current evi-dence suggests that mitochondrial dysfunction is central tothe development of multiorgan dysfunction syndrome, theprimary cause of death in sepsis. The protein peroxisomeproliferator-activated receptor-g coactivator-1a (PGC-1a) reg-ulates mitochondrial biogenesis, metabolism, and antioxidantproduction, three key processes which become dysregulated insepsis. Regulation of PGC-1a is achieved through a number ofpost-translational modifications which include deacetylation.Deacetylation occurs through the action of the enzymesirtuin 1 (SIRT1) which increases the activity of PGC-1a. Chem-ical activators such as SIRT1 activator 3 can also activate SIRT1.This project aimed to investigate whether SIRT1 activation hada protective effect on mitochondria under conditions mimick-ing sepsis.
Human endothelial cells were cultured and treated with 0–8 mM SIRT1 activator 3 with and without 2 mg ml21 lipopolysac-charide (LPS) and 20 mg ml21 peptidoglycan (PepG) to mimicsepsis. Mitochondrial metabolic activity, membrane potential,volume, antioxidant expression, and interleukin-6 (IL-6) pro-duction was measured after 24 h or 7 days.
Metabolic activity after 7 days was significantly lower in cellstreated with LPS/PepG compared with untreated controls (P ¼0.004, Fig. 10A). Treatment of LPS/PepG-exposed cells withSIRT1 activator 3 protected against decreased metabolic activ-ity (Fig. 10A). IL-6 concentrations in culture medium were higherin cells treated with LPS/PepG for 24 h compared with untreatedcells (P ¼ 0.002) and SIRT1 activator 3 dampened this increase(Fig. 10B). SIRT1 activator 3 also protected against changes inmitochondrial membrane potential and volume, and totalglutathione in cells treated with LPS plus PepG.
These results suggest thatSIRT1 activation prevents againstmitochondrial dysfunction in cells under conditions of sepsis.Further research will fully elucidate the exact mechanismsinvolved and maysuggest novel therapeutic intervention strat-egies in the future.
P = 0.001*P = 0.0002
+
15
10
2HBA mM + LPS/PepG
IL-6
ng/
ml
5
0
Contro
l0+ 2+ 6+ 12
+
+
+
Fig 9 IL-6 concentrations in culture media from cells exposed to2 mg ml21 LPS and 20 mg ml21 PepG for 24 h and treated with2HBA. Data are shown as median, interquartile and full range(n=6). P value shown is Kruskal Wallis. + = significantly lowerthan cells without 2HBA (P,0.05, Mann–Whitney U-test).
Abstracts of the Anaesthetic Research Society Meeting BJA
197P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Investigation of indole-derivativemelatonin-like compounds as noveltreatments for sepsisE. Fisher, D. Lowes and H. GalleyAcademic Unit of Anaesthesia and Intensive Care, University ofAberdeen, Aberdeen, UK
Sepsis is a significant cause of morbidity and mortality world-wide. The multiple organ dysfunction syndrome (MODS) is acommon complication of sepsis. Mitochondrial dysfunctionassociated with oxidative stress has been implicated as thekey process in the pathogenesis of MODS. Melatonin is an en-dogenous indole hormone with major effects on sleeping pat-terns, but it is also a potent antioxidant and anti-inflammatoryagent and may be of benefit in the treatment of MODS. Indoleprecursors to melatonin may possess similar properties andmay have the added benefit of not affecting sleeping patterns.This project investigated the potential antioxidant effects ofthe indoles 5-hydroxytryptophan (5-HTP) and N-acetylserotonin(NAS) in endothelial cells under conditions mimicking sepsis.
Human umbilical vein endothelial cells were cultured andtreated with 0–100 mM 5-HTP or NAS in the presence andabsence of 2 mg ml21 lipopolysaccharide (LPS) plus 20 mg ml21
peptidoglycan (PepG) to mimic a mixed polymicrobial sepsis.Cell viability, mitochondrial volume, inner mitochondrial mem-brane potential and metabolic activity were measured after24 h and 7 d culture in six replicate independent experiments.
Neitherof the compounds studied had any detrimental effecton cell viability at the concentrations investigated. Treatment ofcells withLPS/PepGfor7dresulted in adecrease in mitochondrialinner membrane potential (P , 0.05) which was also decreasedin the presence of 5-HTP (P , 0.05), such that at 100 mM, 5-HTPmembrane potential was significantly lower than in cellstreated with LPS/PepG alone (P , 0.05). Mitochondrial volume
and metabolic activity also decreased in cells treated with LPS/PepG for 7 d (P , 0.05). Concurrent treatment of cells with5-HTP blunted the decrease in mitochondrial volume (P ¼0.036, Fig. 11) and at 100 mM, 5-HTP, mitochondrial volumewas higher than in cells exposed to LPS/PepG alone (P , 0.05,Fig. 11). Neither 5-HTP nor NAS had any effect on metabolic ac-tivity and NAS also did not alter mitochondrial volume or mem-brane potential in cells exposed to LPS/PepG.
This study showed that there were varying effects of NASand 5-HTP on measures of mitochondrial function, but not allthese effects were beneficial.
0.05A B
20
15
105
0
P = 0.025 P = 0.0008
* *
*
#
#
SIRT1 activator 3 (mM)
0.04M
etab
olic
act
ivity
uni
ts
Inte
rleuk
in-6
ng
ml–1
0.03
Untre
ated 0 1 4 8
SIRT1 activator 3 (mM)Untre
ated 0 1 4 8
Fig 10 (A) Mitochondrial metabolic activity after 7 days and (B) IL-6 levels after 24 h in culture medium in cells treated with LPS plus PepG with andwithout SIRT1-activator 3. Box and whisker plots show median, IQR, and full range (n=6). P-values are Kruskal–Wallis. *Significantly different fromuntreated cells (P,0.05). #Significantly different from cells treated with LPS/PepG without SIRT1-activator 3 (P,0.05). (Mann–Whitney U-test).
1.0
1.5
2.0
2.5
5-hydroxytryptophan, µM
Flu
ores
cenc
e un
its
0 1 10 100
Control2 µg ml–1 LPS plus 20 µg ml–1 PepG
*P < 0.05*
P = 0.036
Fig 11 Mitochondrial volume in endothelial cells after 7 days treat-ment with LPS and PepG plus with 5-hydroxytryptophan (5-HTP).Control is cells without LPS/PepG or 5-HTP. Box and whisker plotsshow median, interquartile and full range (n=6). P-value shown isKruskal–Wallis across LPS/PepG groups. *¼P,0.05 in comparisonto cells without 5-HTP.
BJA Abstracts of the Anaesthetic Research Society Meeting
198P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018

Towards an efficient biosensor for thedetection of lipopolysaccharide in sepsisusing molecularly imprinted polymersD. Huckle1, J. Hall1, J. Bowen2, C. Allender2,J. Cuenca3 and A. Porch3
1Cardiff Institute of Infection and Immunity, School of Medicine,2School of Pharmacy and Pharmaceutical Science and 3CardiffSchool of Engineering, Cardiff University, Cardiff, UK
Thetruepotentialofcirculatingbiomarkerdetectionandsurveil-lance in patients with sepsis is yet to be elucidated. The focus ofthis project is lipopolysaccharide (LPS), a major constituent ofgram-negative bacteria outer cell walls, and its use as a sepsismarker. The overarching hypothesis is the detection of circulat-ing LPS will facilitate the early diagnosis of sepsis.
Molecular imprinting describes the generation of synthetic,polymeric receptors through the polymerization of monomersaround a template molecule (Fig. 12). The resultant polymerspossess recognition properties akin to an antibody with theability to recognize the original target molecule and relatedspecies. Efficient molecularly imprinted polymers rely onstrong interactions between the target, in this case, LPS,and the functional monomers that form the polymer matrix.Polymyxin B (PMB), a peptide antibiotic, has high affinity for
LPS and is utilized in this study as a functional monomer. LPSis not a suitable template for conventional imprinting techni-ques; therefore, techniques that circumvent problems asso-ciated with the imprinting of biological macromolecules areneeded and modified approaches that localize LPS at asurface via chemical immobilization at a solid–solvent inter-face (surface imprinting on a solid support) or via self-assemblyat a solvent–solvent interface (suspension polymerization/microfluidic techniques) have been investigated.
Microfluidics (MF) describes the science and technologythat manipulates very small (10–9 to 10–18 litre) volumesof fluid. A system that generates segmented flow within poly-tetrafluoroethylene (PTFE) tubing has been constructed, pro-viding small pockets of an aqueous monomer solutiontravelling in an organic solvent continuous phase. Using abespoke cavity resonator, the in situ polymerization of the‘beads’ of aqueous monomer solution in this MF system hasbeen achieved using microwaves. Furthermore, the processof polymerization can be monitored by sensing the changesin resonant frequency imposed by the changing monomer so-lution as it polymerizes. Continued troubleshooting of sus-pension polymerization and microfluidic processes formsthe foundation of ongoing work as the successful imprintingof LPS in polymer beads with integrated PMB becomes apossibility.
Functional monomer
Template
Polymerization
Self assembly Imprinted material
Removalof
template
Polymer matrix
Fig 12 Schematic representation of traditional molecular imprinting method. A solution phase complex of the template molecule (LPS) and func-tional monomers (polymerizable PMB and acrylamide) forms, which is ‘locked’ in place during polymerization. Following removal of the templatespecies, an imprint of the template within the polymer matrix remains; this imprinted material demonstrates a natural affinity for the templatemolecule.
Abstracts of the Anaesthetic Research Society Meeting BJA
199P
Downloaded from https://academic.oup.com/bja/article-abstract/112/1/181P/243486by gueston 20 February 2018