Embed Size (px)
Citation preview
ACCURACY OF EXHALED TIDAL VOLUME (MEASURED AND ESTIMATED) OF TWO SUBACUTE/HOME CARE VENTILATORS IN A SIMULATED NEONATE/INFANT MODEL
Gerald Moody, RRT-‐NPS, Andre Finely, RRT-‐NPS -‐ Children’s Medical Center Dallas, TX
IntroducLon
When transi+oning ven+lator dependent pa+ents to home care ven+lators we commonly place pa+ents in PC-‐SIMV mode using +dal volumes (VT) as a parameter for seBng pressures. Pa+ents ven+lator seBngs are first established on cri+cal care ven+lators and then transposed to their subacute/home care ven+lators. Some pa+ents don’t tolerate the transi+on and are placed back on a cri+cal care ven+lator, delaying transfer out of the ICU. There has been some ques+on as to the accuracy of exhaled VT readings on our subacute/home care ven+lators, especially on smaller pa+ents (around 5 kg) when using a passive circuit with no proximal flow sensor at the pa+ent airway. We conducted tests of two brands of subacute/home care ven+lators used in our hospital to determine accuracy of exhaled VT readings with passive circuits and ac+ve circuits with proximal flow sensors. We hypothesized there would be no difference in accuracy between the LTV 1200 (Carefusion, Yorba Linda, CA) and the Trilogy 202 (Phillips Healthcare, Andover, MA) when using each manufacturers’ proprietary ac+ve circuits with proximal flow sensors; there would be a difference in VT accuracy when using the Trilogy 202’s passive circuit.
Methods The Trilogy 202 and LTV 1200 were tested with their respec+ve ac+ve and passive (Trilogy) circuits. Each vent/circuit configura+on was aZached to a test lung (Ingmar ASL 5000) using the neonate/apneic model with a C: 7 mL/cmH2O and R: 10 cm H2O/L/s. 10 Vent breaths were read for each configura+on and compared to the ASL 5000 readings at 3 different pressure levels using the following seBngs: PC-‐SIMV mode, PIP of (12,15 & 20 cmH2O), PEEP 5 cmH20, RR 25 breaths/min, Ti .5, rise of 1 on Trilogy rise of 3 on LTV (typical rise +mes for each vent used in our prac+ce), leak compensa+on “on”, all configura+ons were tested with no leaks.
Results
Table 1 shows results for each vent/circuit configura+on. The LTV 1200 was the most accurate, followed by the Trilogy with ac+ve circuit. As hypothesized the Trilogy with the passive circuit was least accurate, but provided the most consistent VT’s at lower PIP’s, at a PIP of 20 the Trilogy with ac+ve circuit had the most consistent VT readings. The Trilogy with passive circuit also delivered less VT's compared to each ac+ve circuit configura+on.
Table 1: Results
PIP 12 +/-‐ SD Mean Vt Vt
(% Error) PIP 15 +/-‐ SD Mean Vt Vt
(% Error) PIP 20 +/-‐ SD Mean Vt Vt (% Error)
Trilogy Passive circuit
12.19 50.2
+ 28%
Trilogy Passive circuit
11.61 74.3
+ 25%
Trilogy Passive circuit
10.80 110.5
+ 19%
ASL 5000 2.11 36 ASL 5000 2.69 55.9 ASL 5000 2.27 89.6
Trilogy Active circuit
11.65 80.8
+ 11%
Trilogy Active circuit 8.95 100.6
+ 10%
Trilogy Active circuit
0.67 138.7
+ 9%
ASL 5000 13.86 72 ASL 5000 10.01 91 ASL 5000 0.42 126.2
LTV 1200 13.16 47.5
+ 3%
LTV 1200 14.01 106.9
+ 5%
LTV 1200 22.97 156.5
+ 5%
ASL 5000 12.70 45.9 ASL 5000 11.83 101.3 ASL 5000 16.11 148.2
50.2 74.3
110.5
36 55.9
89.6 80.8 100.6
138.7
72 91
126.2
47.5
106.9
156.5
45.9
101.3
148.2
PIP 12 PIP 15 PIP 20
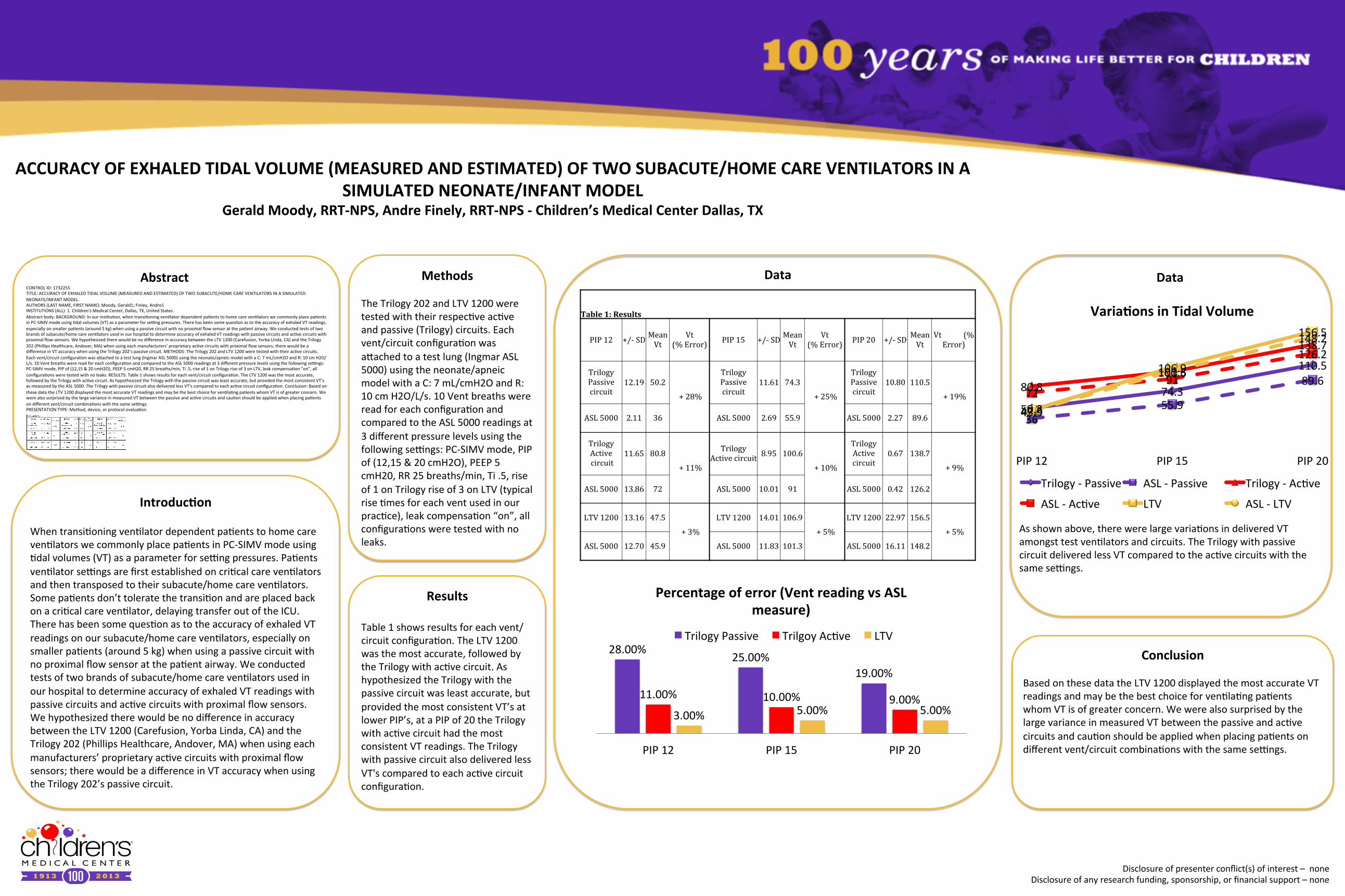
VariaLons in Tidal Volume
Trilogy -‐ Passive ASL -‐ Passive Trilogy -‐ Ac+ve
ASL -‐ Ac+ve LTV ASL -‐ LTV
Conclusion
Based on these data the LTV 1200 displayed the most accurate VT readings and may be the best choice for ven+la+ng pa+ents whom VT is of greater concern. We were also surprised by the large variance in measured VT between the passive and ac+ve circuits and cau+on should be applied when placing pa+ents on different vent/circuit combina+ons with the same seBngs.
28.00% 25.00%
19.00%
11.00% 10.00% 9.00% 3.00% 5.00% 5.00%
PIP 12 PIP 15 PIP 20
Percentage of error (Vent reading vs ASL measure)
Trilogy Passive Trilgoy Ac+ve LTV
Data Data
As shown above, there were large varia+ons in delivered VT amongst test ven+lators and circuits. The Trilogy with passive circuit delivered less VT compared to the ac+ve circuits with the same seBngs.
CONTROL ID: 1732255 TITLE: ACCURACY OF EXHALED TIDAL VOLUME (MEASURED AND ESTIMATED) OF TWO SUBACUTE/HOME CARE VENTILATORS IN A SIMULATED NEONATE/INFANT MODEL. AUTHORS (LAST NAME, FIRST NAME): Moody, Gerald1; Finley, Andre1 INSTITUTIONS (ALL): 1. Children's Medical Center, Dallas, TX, United States. Abstract body: BACKGROUND: In our ins+tu+on, when transi+oning ven+lator dependent pa+ents to home care ven+lators we commonly place pa+ents in PC-‐SIMV mode using +dal volumes (VT) as a parameter for seBng pressures. There has been some ques+on as to the accuracy of exhaled VT readings, especially on smaller pa+ents (around 5 kg) when using a passive circuit with no proximal flow sensor at the pa+ent airway. We conducted tests of two brands of subacute/home care ven+lators used in our hospital to determine accuracy of exhaled VT readings with passive circuits and ac+ve circuits with proximal flow sensors. We hypothesized there would be no difference in accuracy between the LTV 1200 (Carefusion, Yorba Linda, CA) and the Trilogy 202 (Phillips Healthcare, Andover, MA) when using each manufacturers’ proprietary ac+ve circuits with proximal flow sensors; there would be a difference in VT accuracy when using the Trilogy 202’s passive circuit. METHODS: The Trilogy 202 and LTV 1200 were tested with their ac+ve circuits. Each vent/circuit configura+on was aZached to a test lung (Ingmar ASL 5000) using the neonate/apneic model with a C: 7 mL/cmH2O and R: 10 cm H2O/L/s. 10 Vent breaths were read for each configura+on and compared to the ASL 5000 readings at 3 different pressure levels using the following seBngs: PC-‐SIMV mode, PIP of (12,15 & 20 cmH2O), PEEP 5 cmH20, RR 25 breaths/min, Ti .5, rise of 1 on Trilogy rise of 3 on LTV, leak compensa+on “on”, all configura+ons were tested with no leaks. RESULTS: Table 1 shows results for each vent/circuit configura+on. The LTV 1200 was the most accurate, followed by the Trilogy with ac+ve circuit. As hypothesized the Trilogy with the passive circuit was least accurate, but provided the most consistent VT’s as measured by the ASL 5000. The Trilogy with passive circuit also delivered less VT's compared to each ac+ve circuit configura+on. Conclusion: Based on these data the LTV 1200 displayed the most accurate VT readings and may be the best choice for ven+la+ng pa+ents whom VT is of greater concern. We were also surprised by the large variance in measured VT between the passive and ac+ve circuits and cau+on should be applied when placing pa+ents on different vent/circuit combina+ons with the same seBngs. PRESENTATION TYPE: Method, device, or protocol evalua+on
Disclosure of presenter conflict(s) of interest – none Disclosure of any research funding, sponsorship, or financial support – none
Abstract





























