Embed Size (px)
Citation preview
Minimally Invasive Therapies
for Achalasia
Siva Raja MD, PhD
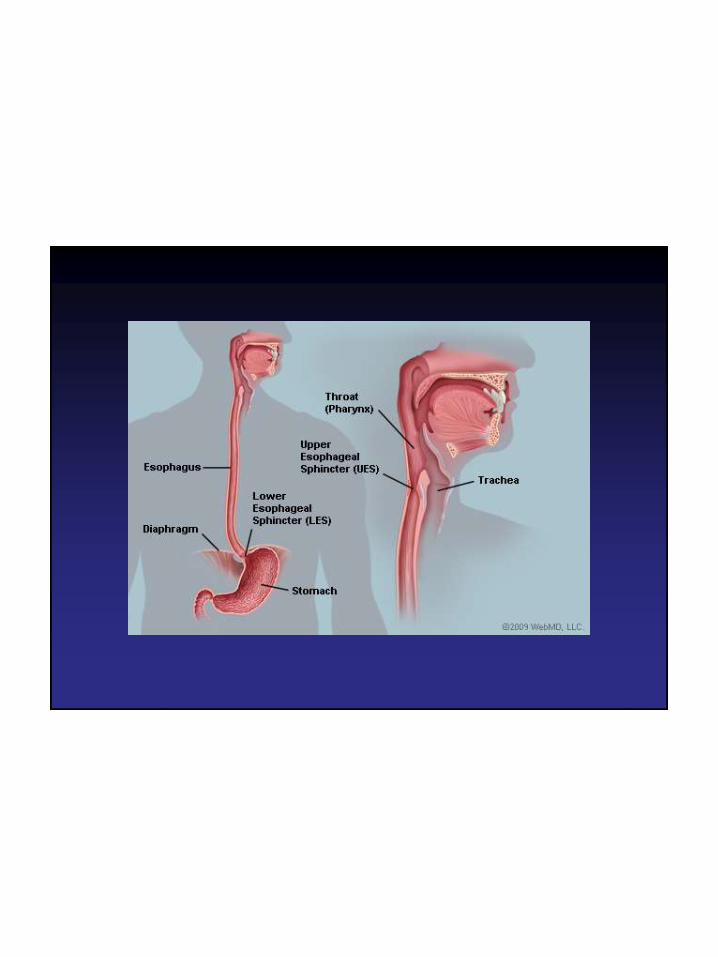

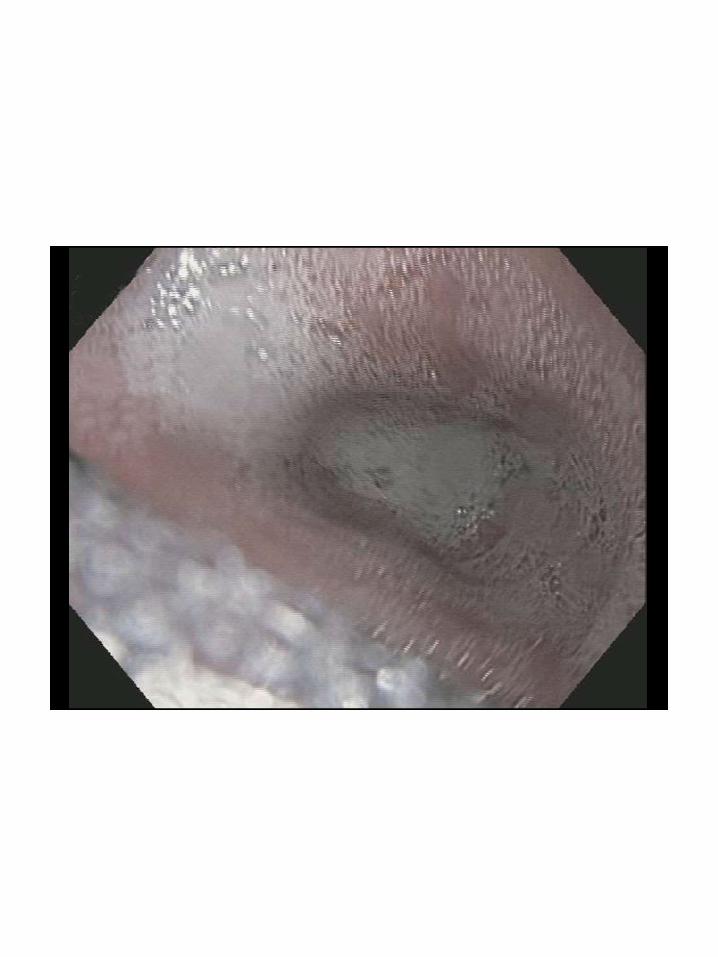
What is Achalasia?
• Achalasia (a- and -chalasia "no
relaxation") is a failure of smooth
muscle fibers (at the end of the
esophagus) to relax, which can cause a
sphincter to remain closed…
Wikipedia, 2014
What is Achalasia?
• Achalasia – failure to relax
- Lower esophageal sphincter (LES) has
impaired relaxation and dysregulation of
esophageal peristalsis
• Sir Thomas Willis 17th century treated
starving patient with a sponge-tipped
whale bone
• Rare – annual incidence 1/100,000
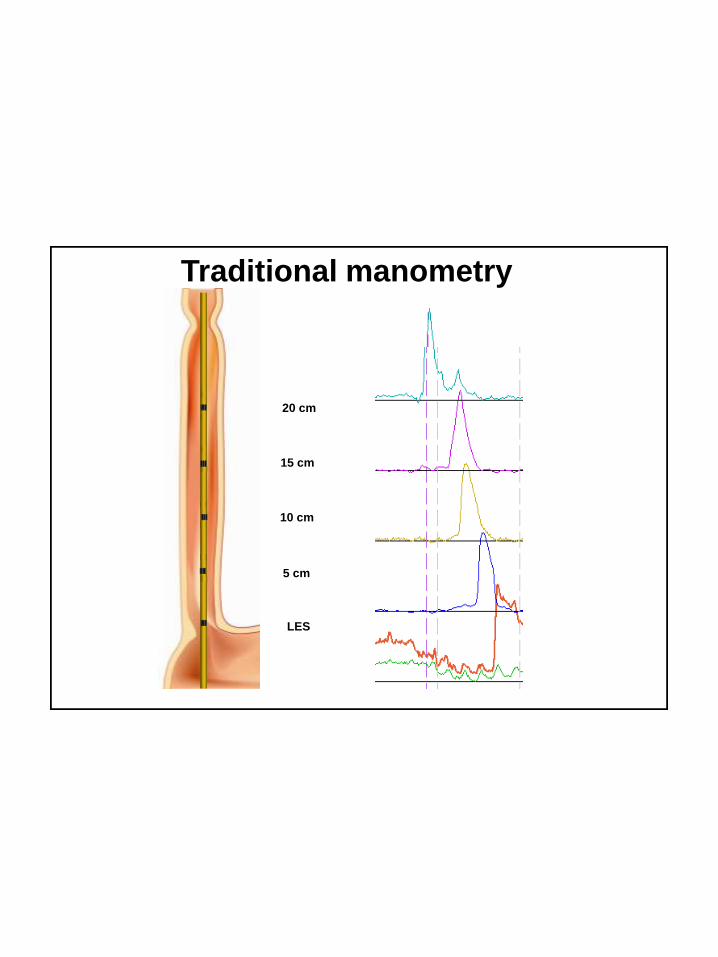
Traditional manometry
LES
20 cm
15 cm
10 cm
5 cm
-6
-5
-4
-3
-2
-1
0
1
2
3
4
5
6
7
8
9
10
11
12
13
15
14
16
18
17
20
19
22
21
24
23
25
27
26
28
30
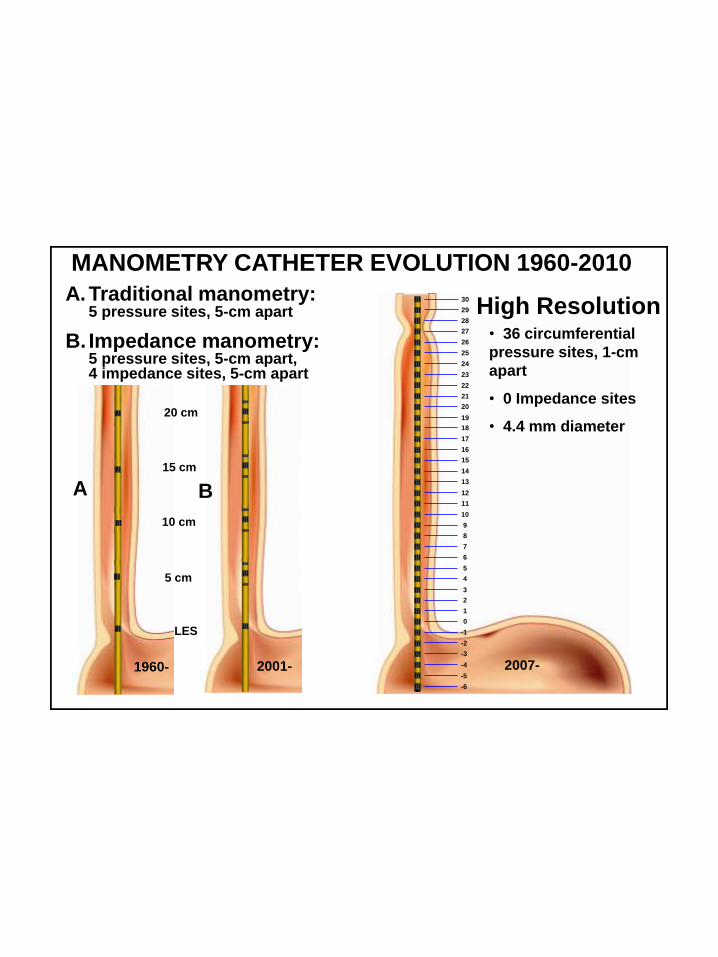
29 High Resolution • 36 circumferential
pressure sites, 1-cm
apart
• 0 Impedance sites
• 4.4 mm diameter
LES
A. Traditional manometry:5 pressure sites, 5-cm apart
B. Impedance manometry:5 pressure sites, 5-cm apart, 4 impedance sites, 5-cm apart
A B
20 cm
15 cm
10 cm
5 cm
MANOMETRY CATHETER EVOLUTION 1960-2010
1960- 2001- 2007-
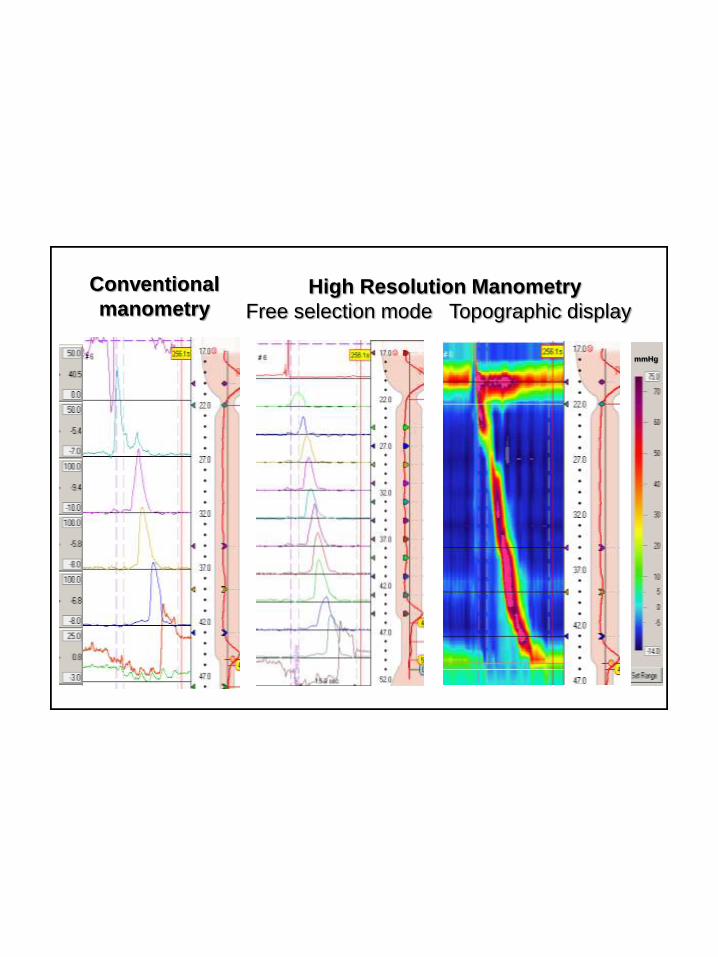
Conventional
manometry
mmHg
High Resolution Manometry
Free selection mode Topographic display
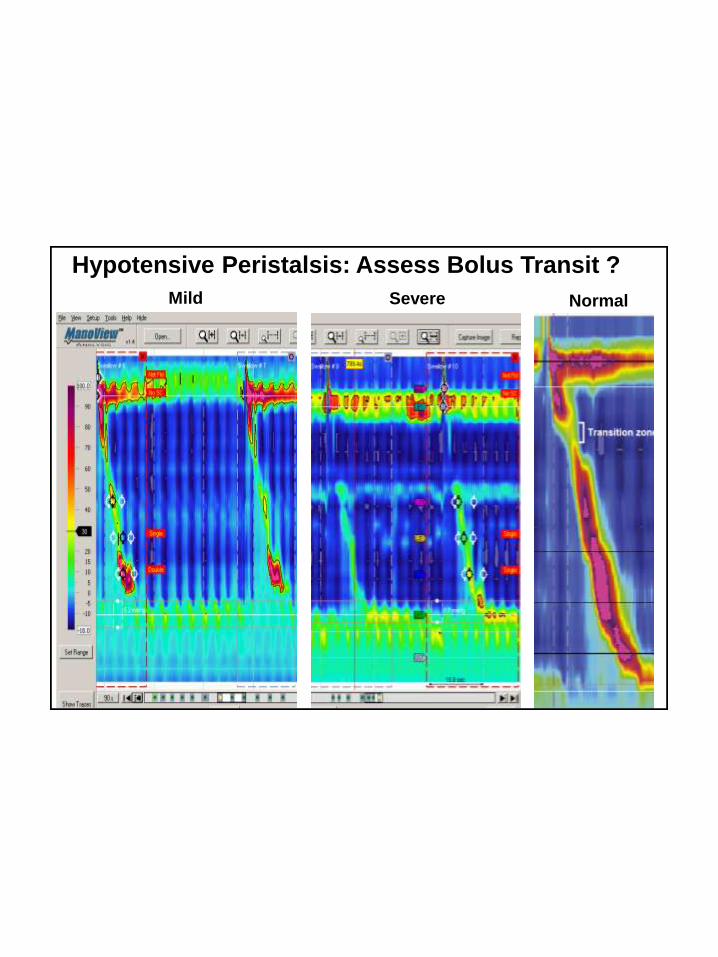
Hypotensive Peristalsis: Assess Bolus Transit ?
Mild Severe Normal
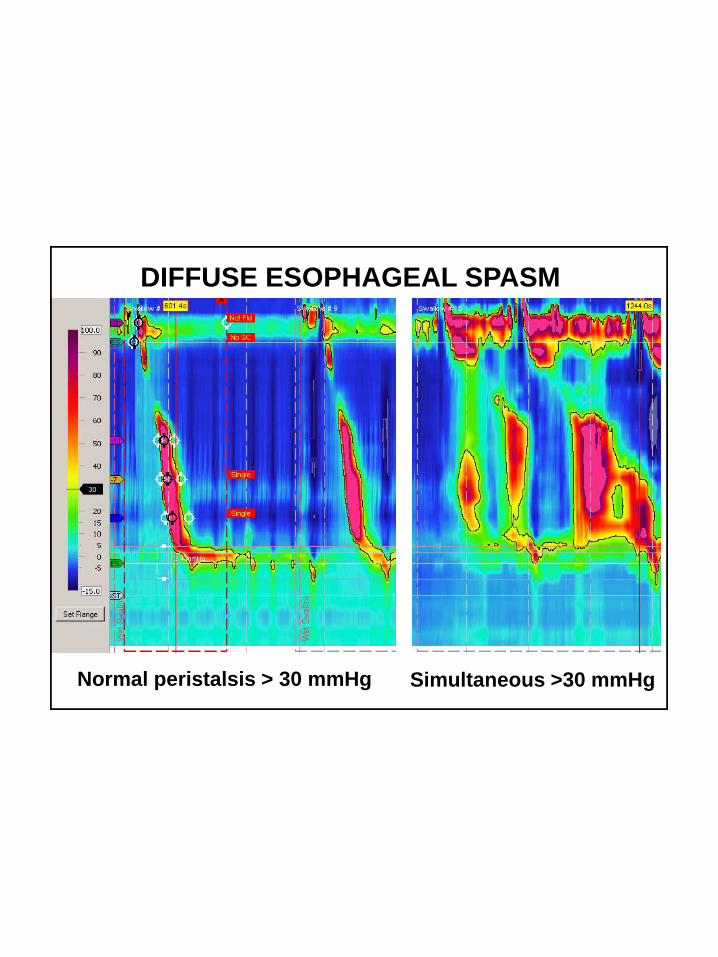
Normal peristalsis > 30 mmHg Simultaneous >30 mmHg
DIFFUSE ESOPHAGEAL SPASM
Type I
Phary
nxPressure
Scale
UE
S13-c
m8-c
m3-c
mLE
SG
astr
ic
75
25
50
75
25
50
75
25
50
75
25
50
75
25
50
75
25
50
75
25
50
Type 2
Pressure
Scale
Phary
nx
UE
S13-c
m8-c
m3-c
mLE
SG
astr
ic
100
75
25
50
100
75
25
50
100
75
25
50
100
75
25
50
100
75
25
50
100
75
25
50
100
75
25
50
Type 3
PressureScale
CCF © 2009
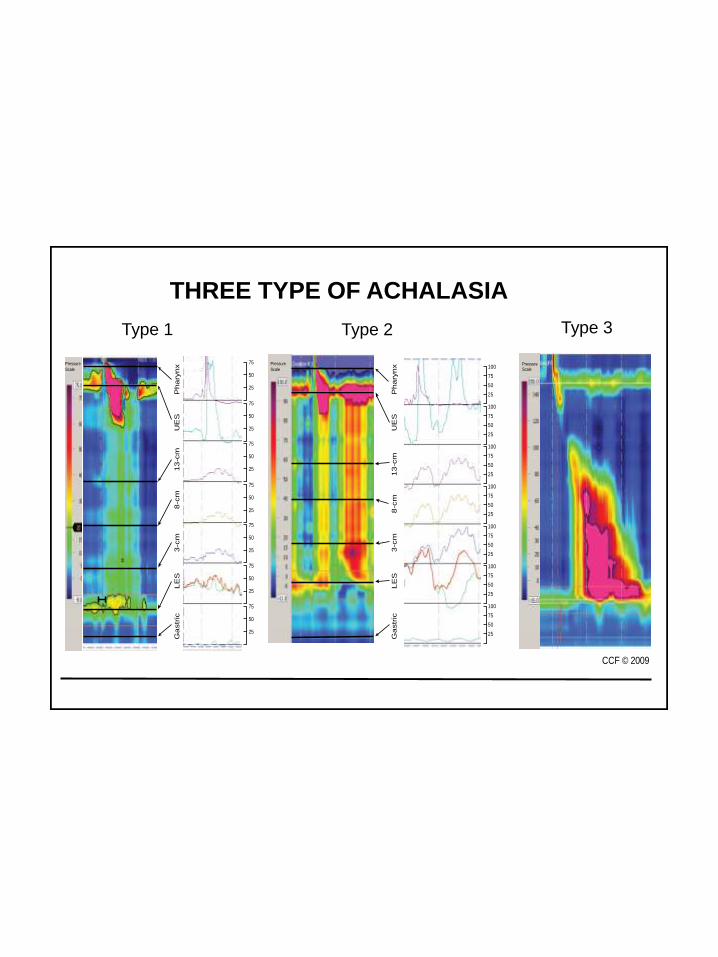
Type 1 Type 2 Type 3
THREE TYPE OF ACHALASIA
Motiltiy Disorders
Disorders of EGJ Relaxation
Achalasia
Type I Classic
Type II Esophageal compression
Type III Spastic
Functional Obstruction
Normal propagation (CFV)
Intrabolus pressure > 15 mmHg
≥ 30% of swallows compartmentalized
Pandolfino JE, et al. Neurogast & Mot 2009;21:796
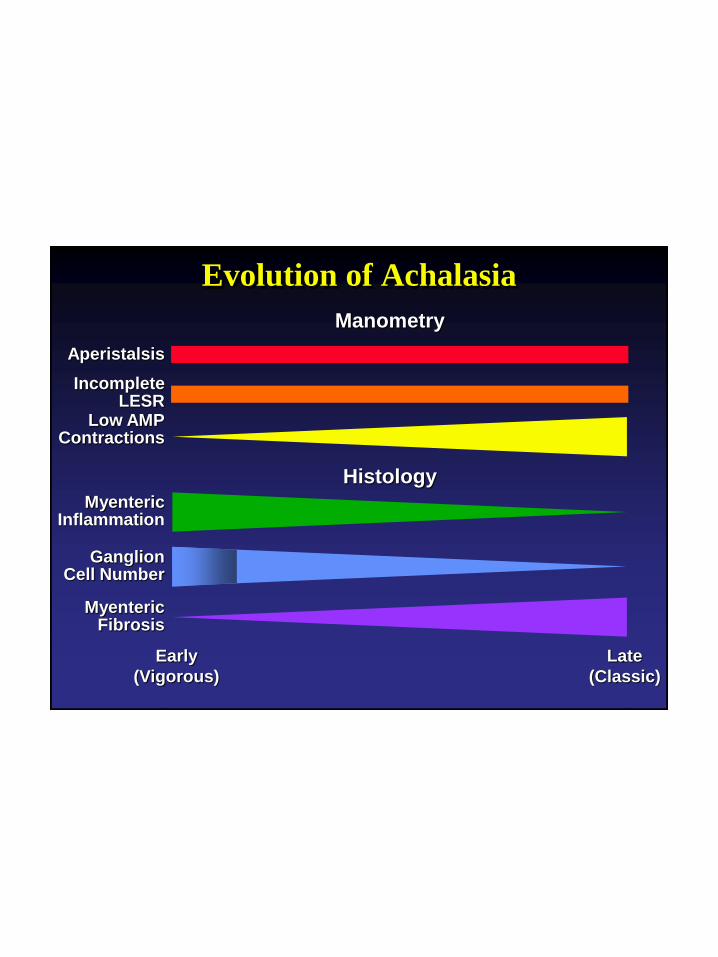
Evolution of Achalasia
Aperistalsis
IncompleteLESR
Low AMPContractions
MyentericInflammation
GanglionCell Number
MyentericFibrosis
Manometry
Histology
Early
(Vigorous)
Late
(Classic)


Goals of Therapy
Symptom relief
Palliation
Esophageal empting
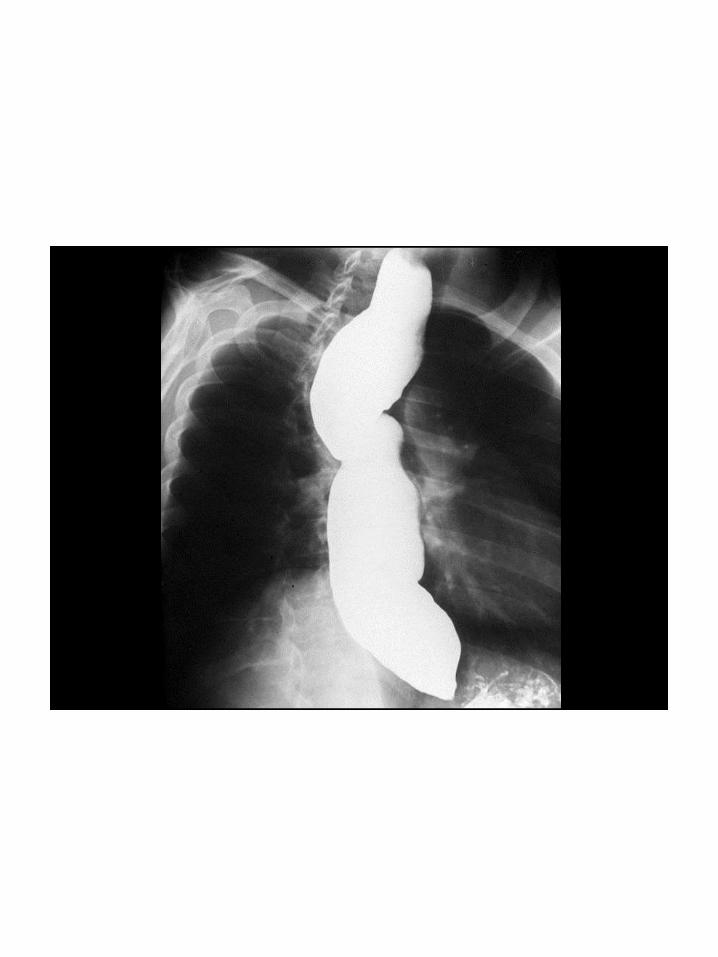
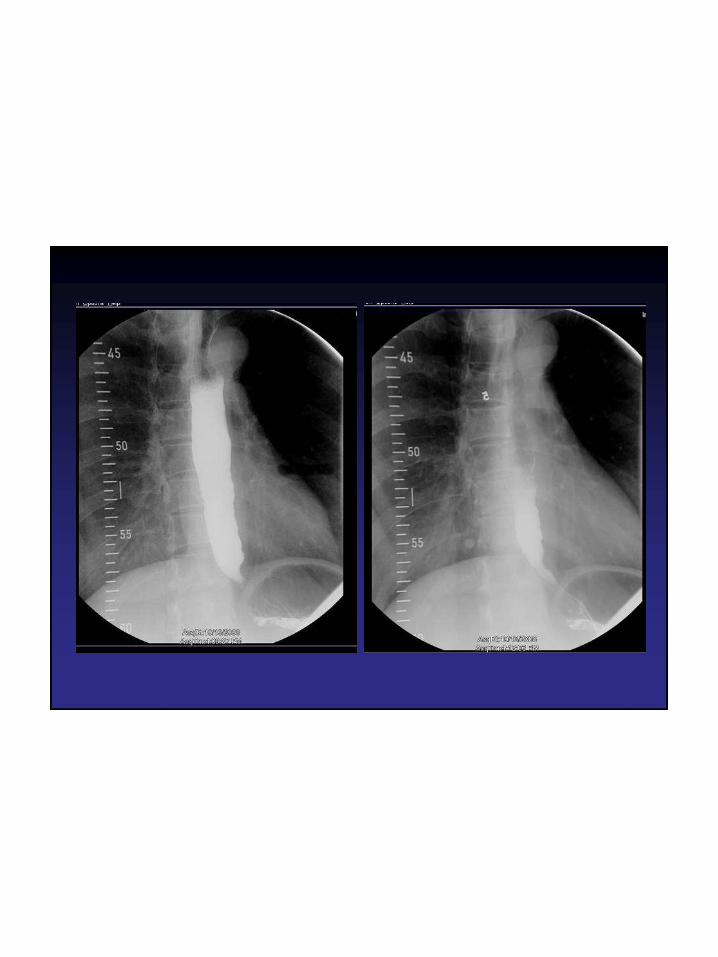
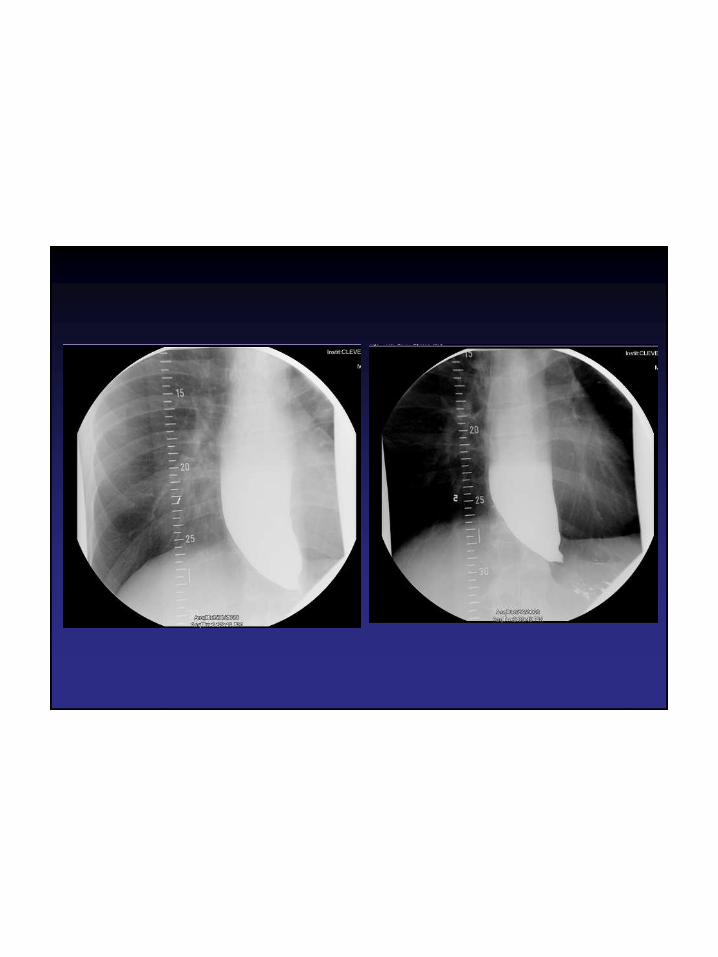
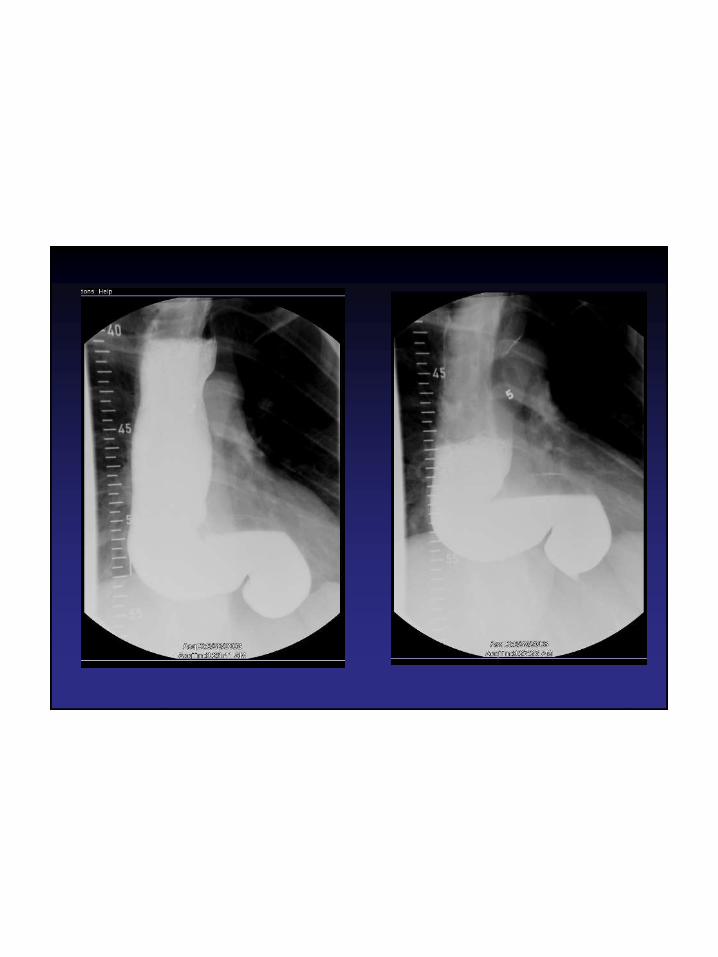
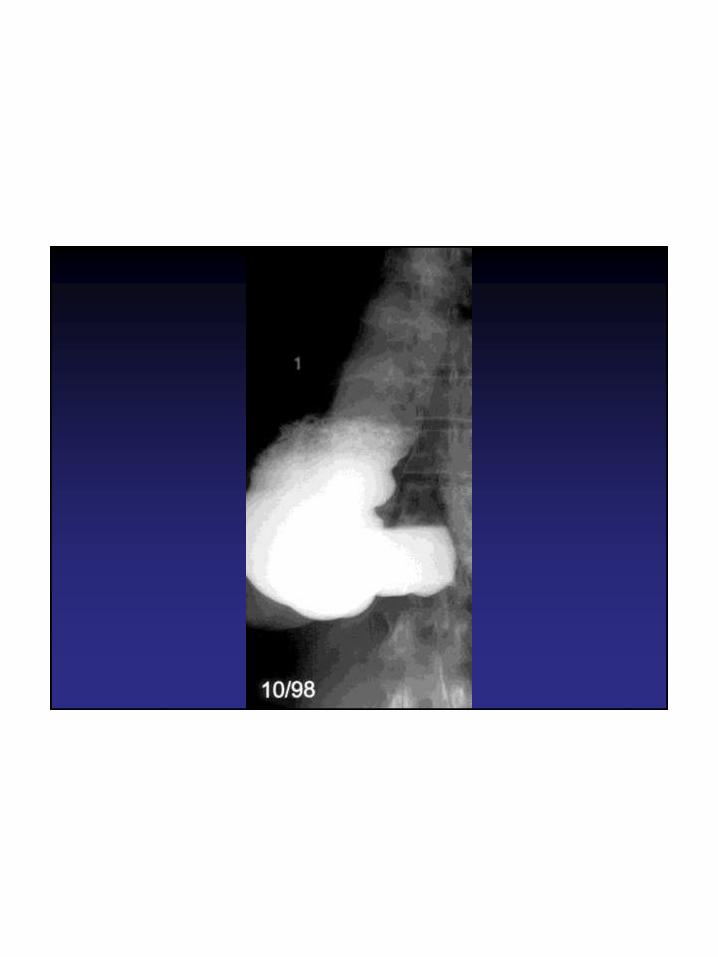
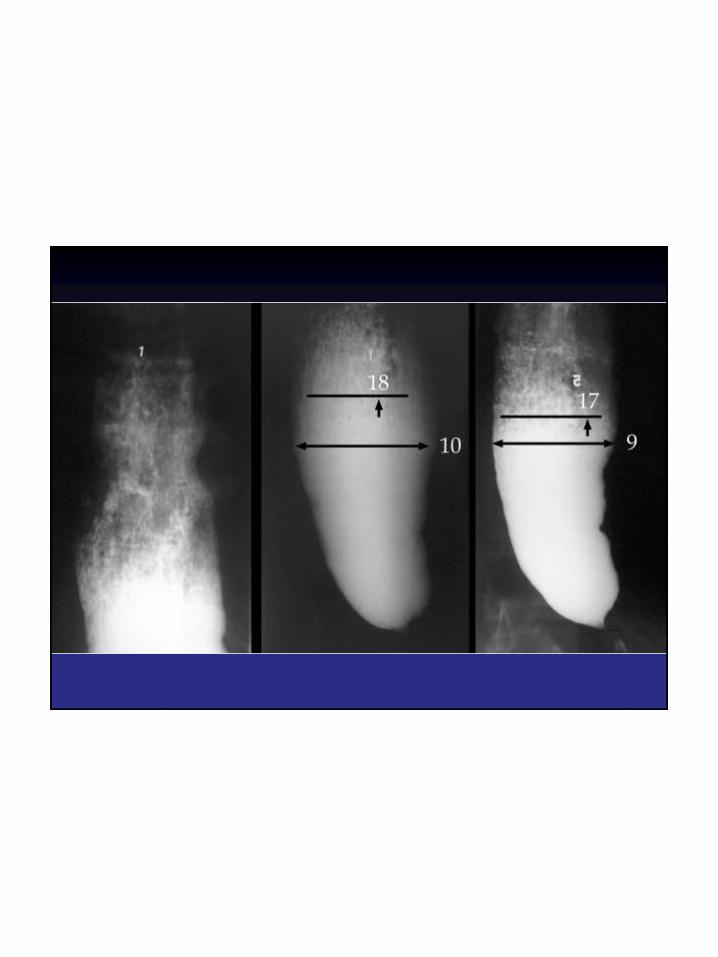
Timed Barium Esophagram
• 250 ml low density barium
• Upright
• Drink the volume they can tolerate without regurgitation (recorded for future testing) in 30-60 seconds
• Left posterior oblique position
• 3 on 1 spot films (35 cm x 35 cm) at 1, 2 and 5 minutes
De Olivera JAM et al. AJR 1997;169:473


Therapy
• Medical
- Calcium channel blockers, nitrates
• Interventional
- Botox
- Pneumatic Dilation
• Surgical
- Heller Myotomy
- Per Oral Endoscopic Myotomy

Medical Therapy

Medical Therapy
• • Calcium channel blockers
- nifedipine 10 – 20 mg sublingual before meals
compared to PD in 30 patients over mean
21months provided good or excellent response
in77% and 75%, respectively
- LES pressure reduced by 28%
• Oral nitrates
- isosorbide dinitrate 5 mg sublingual before meals
- May be more potent than nifedipine
Coccia Gut 1991;32604-6
Traube Am J Gastroenterol 1989;84:1259-62
Gelfond Gastroenterology 1982;83:963-9

Interventional Therapy
Botulinum Toxin (BT)
• Inhibitor of acetylcholine release from neurons
promoting LES contraction
• 80 u injected into LES with sclerotherapy needle
- 20 units / cc into 4 quadrants
- High safety profile - mild chest pain
- BT retreatment possible after BT, PD, myotomy
- Negative predictors – age <55 or LESP >50
mmHg
Pasricha Ann Intern Med 1994;121:590-1
Storr BMC Gastroenterol 2002;Aug 13;2:19
Neubrand Endoscopy 2002;34:519-23
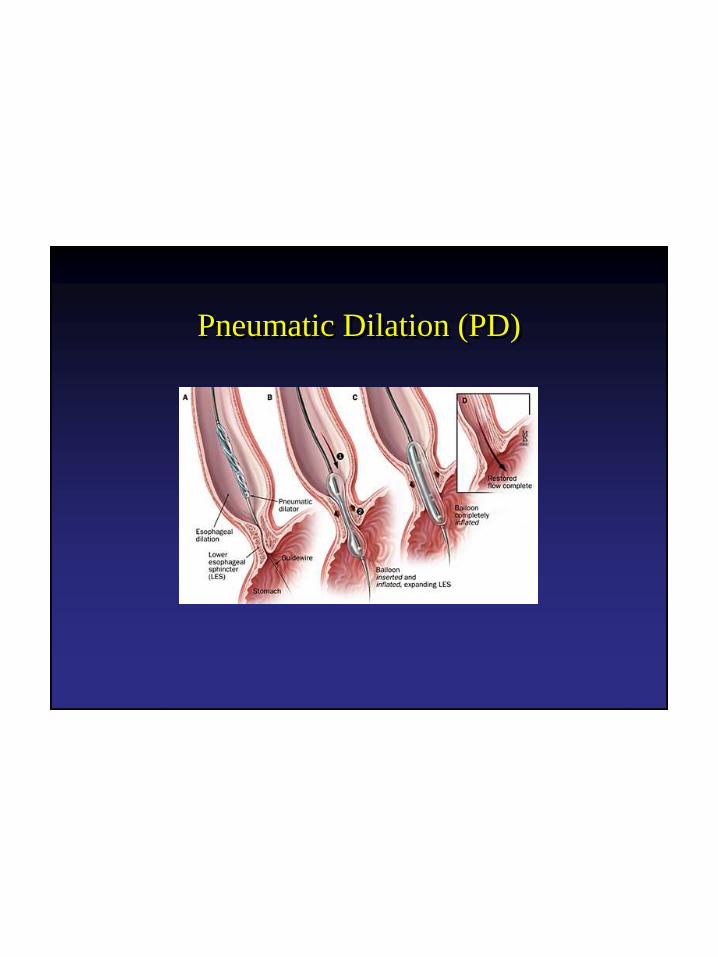
Pneumatic Dilation (PD)
Pneumatic Dilation (PD)
• Per-oral balloon disruption of the LES
- High pressure 5 – 12 psi to obliterate waist
- Large diameter 30, 35 and 40 mm
- Repeated sessions 1 day – 3 weeks apart
with size progression
• Negative predictors
- Age <40 years
- Higher LES pressures after treatment
- Pretreatment chest painHulselmans Clin Gastro Hepatol 2010;8:30-5
Eckart Gut 2004;53:629-33
Pneumatic Dilation (PD)
• Perforation 3 – 7%
• Severe chest pain 15%
• Fever
• Intramural hematoma
• Bleeding
• GERD 15%

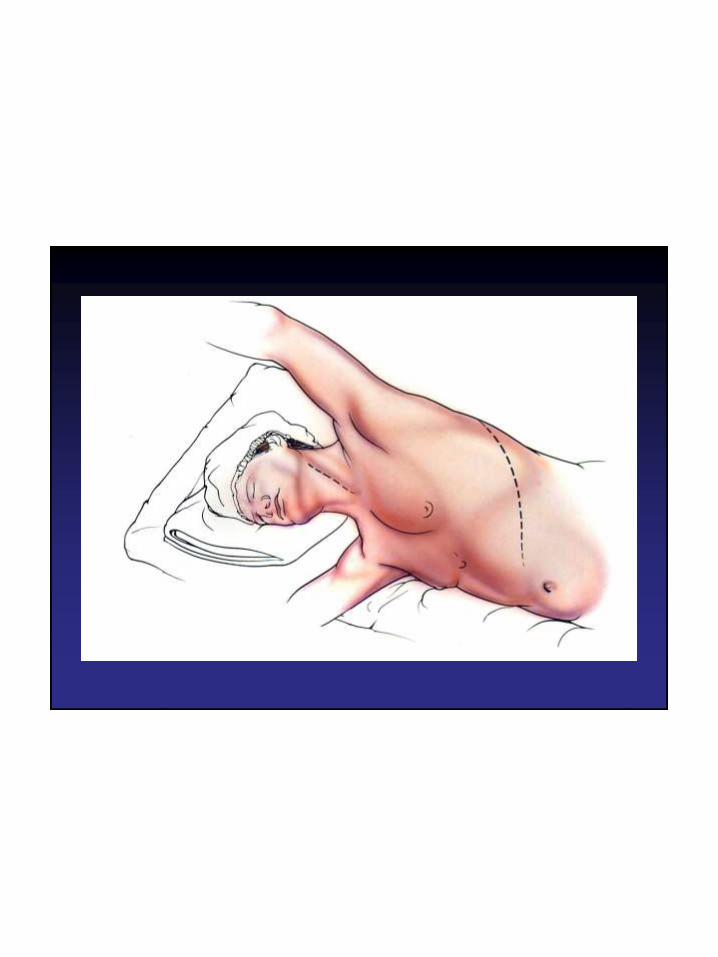
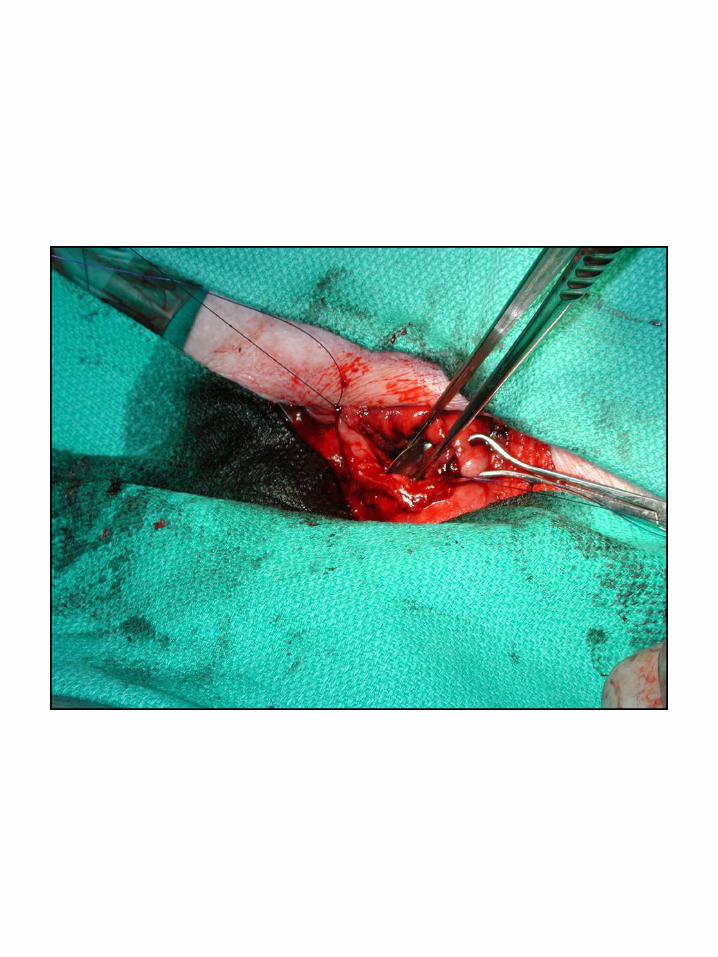
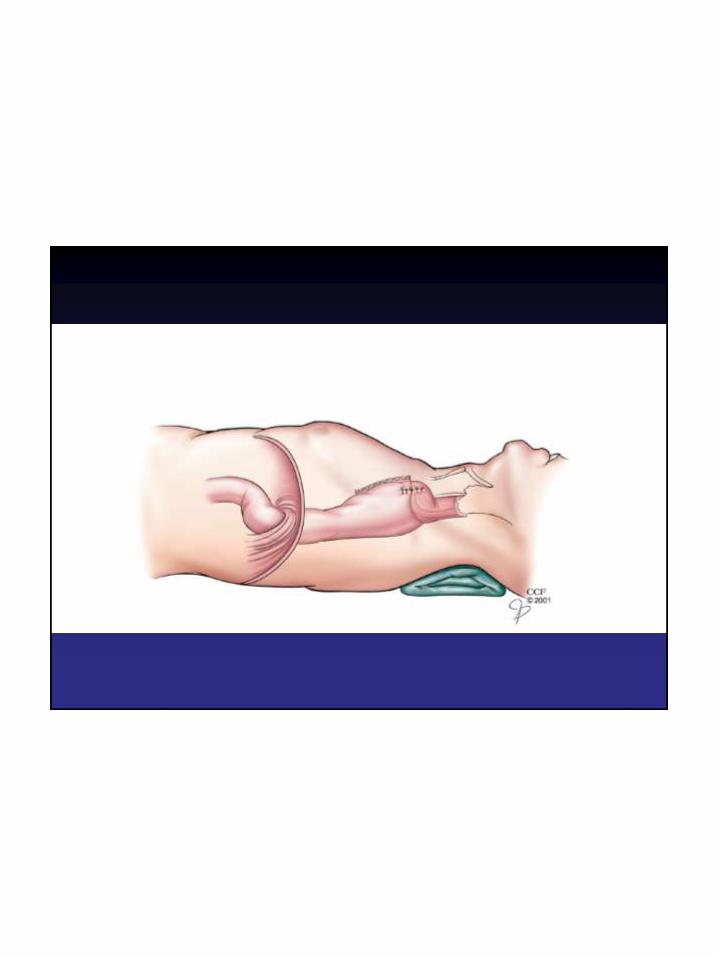
Surgical Therapy
Robotic Heller
Narration


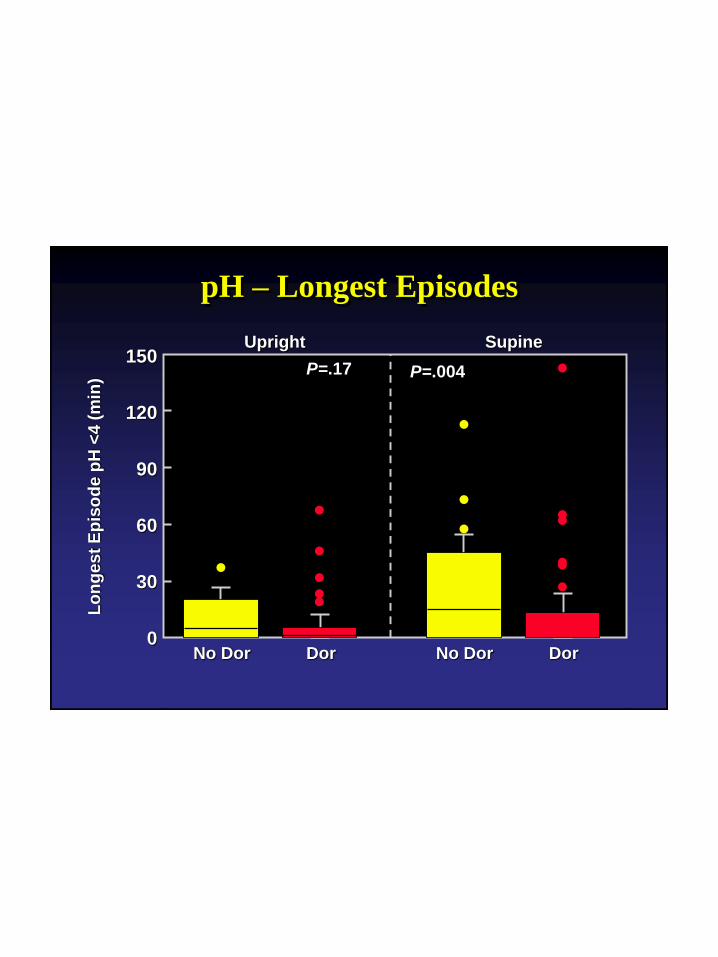
Best Operation
• Heller/Dor is obstructive decreasing the
adequacy of myotomy
• Heller/Dor does not adversely effect
esophageal emptying as assessed by
TBE
• Heller/Dor decreases reflux (?Normal)
150
120
90
60
30
0
Lo
ng
es
t E
pis
od
e p
H <
4 (
min
)
Upright Supine
No Dor Dor No Dor Dor
pH – Longest Episodes
P=.17 P=.004
Clinical Experiences
of
Per-Oral Endoscopic Myotomy
POEM
Inoue H, et al. Endoscopy 2010;42:265
Details of the Cases
Sex male: female = 15: 15
Age 18~75y.o. (mean 46.2 y.o.)
History 1~23years
Type Spindle 13 cases, Flask 9 cases
Sigmoid 8 cases
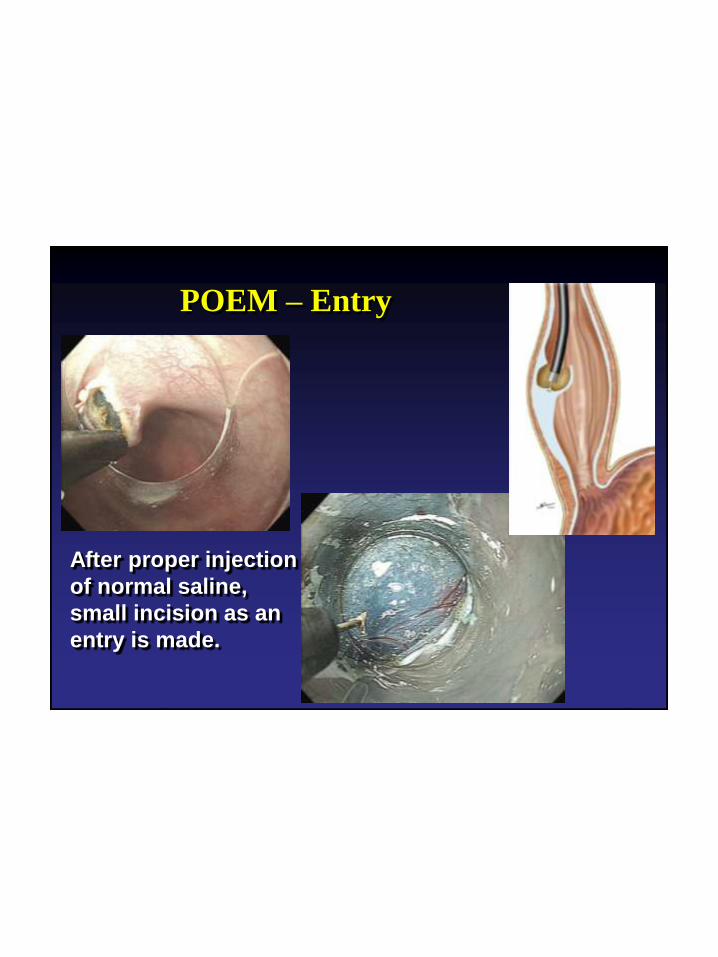
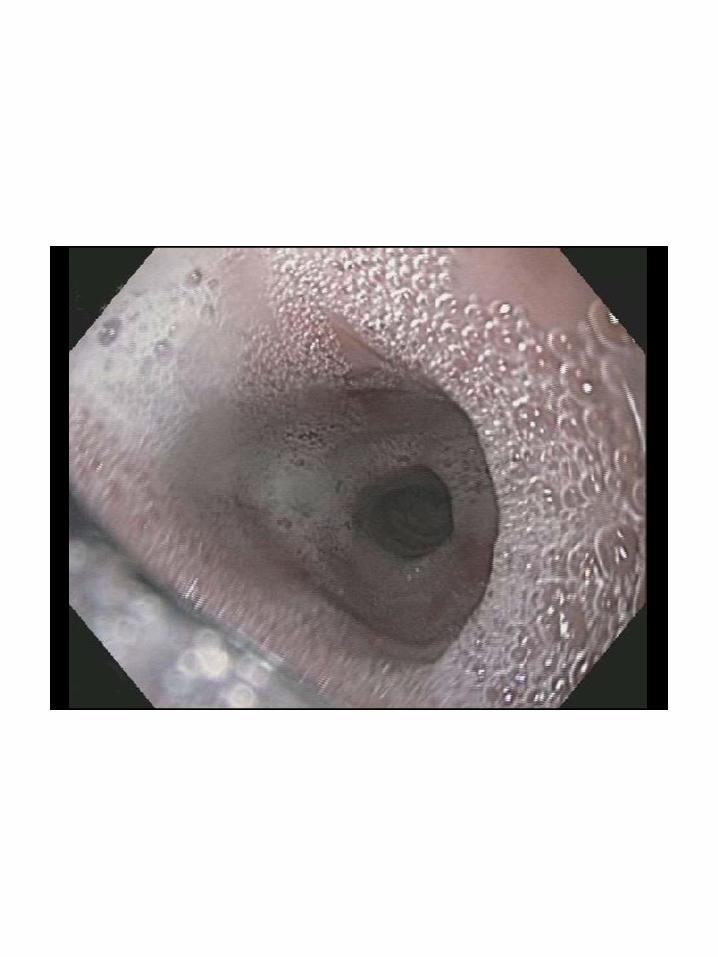
POEM – Entry
After proper injection
of normal saline,
small incision as an
entry is made.
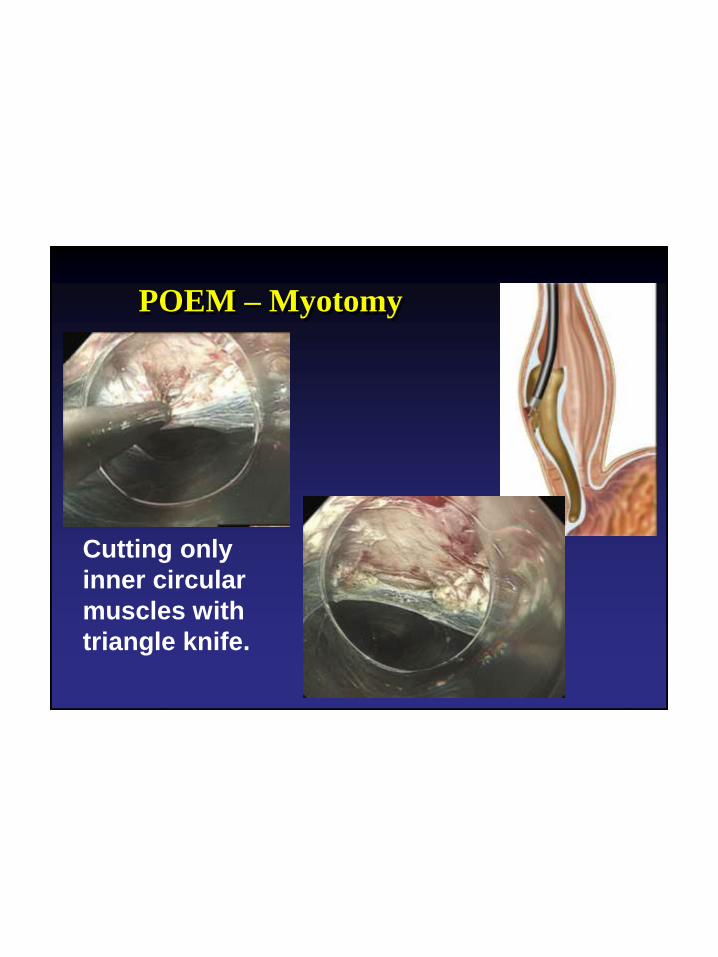
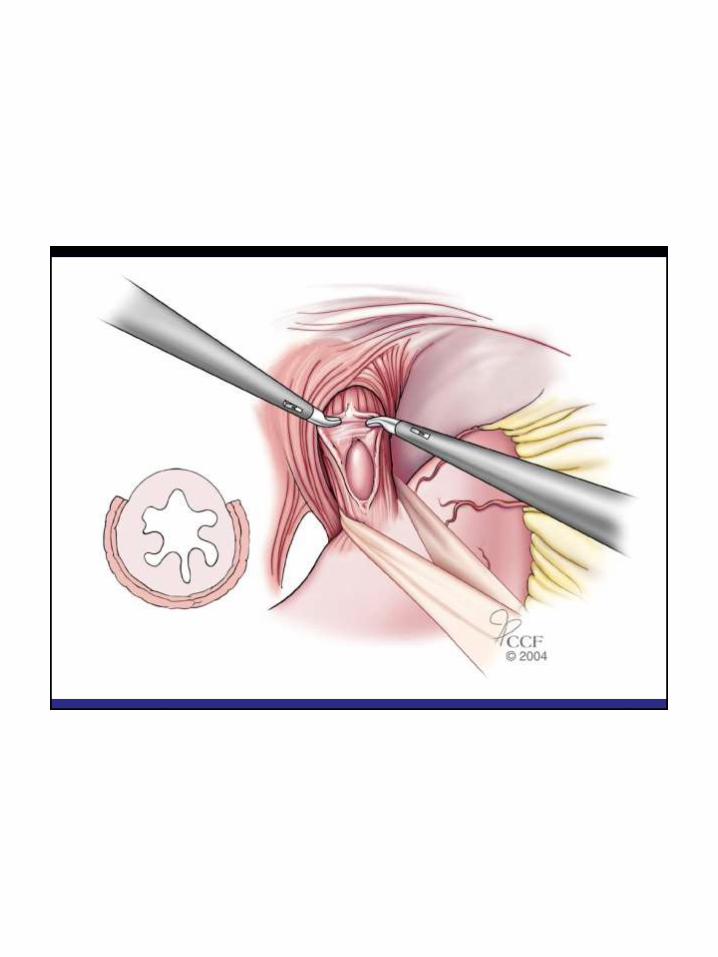
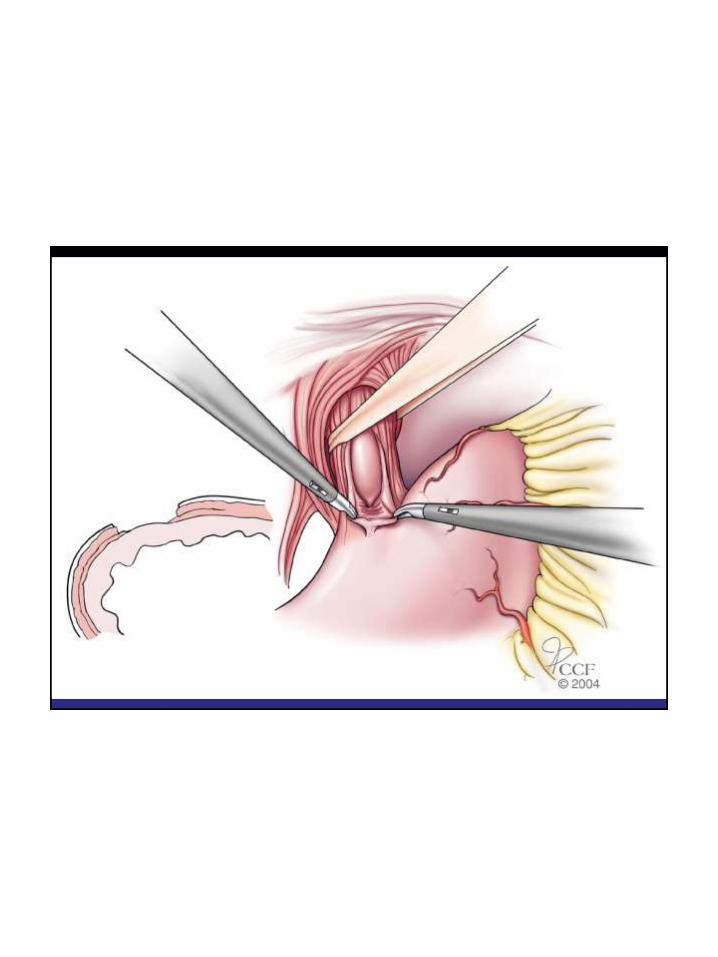
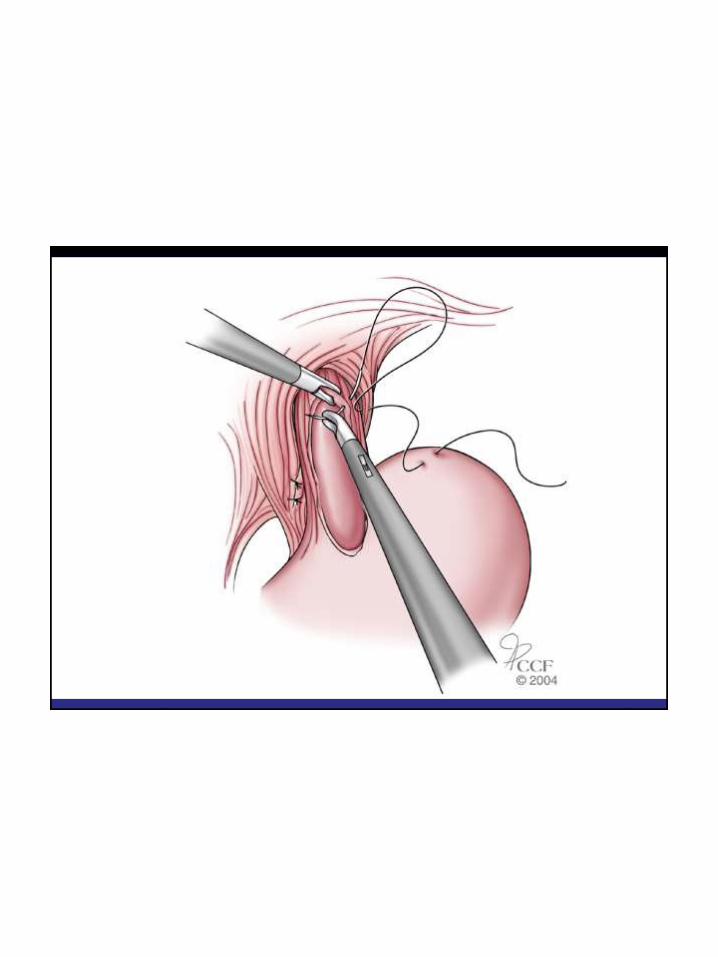
POEM – Myotomy
Cutting only
inner circular
muscles with
triangle knife.
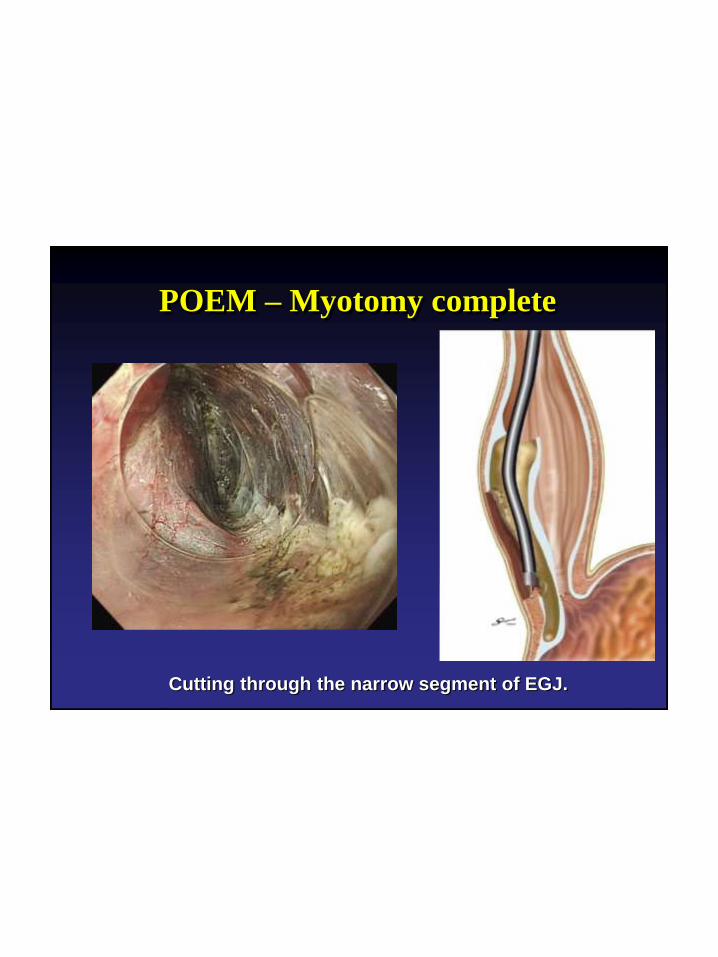
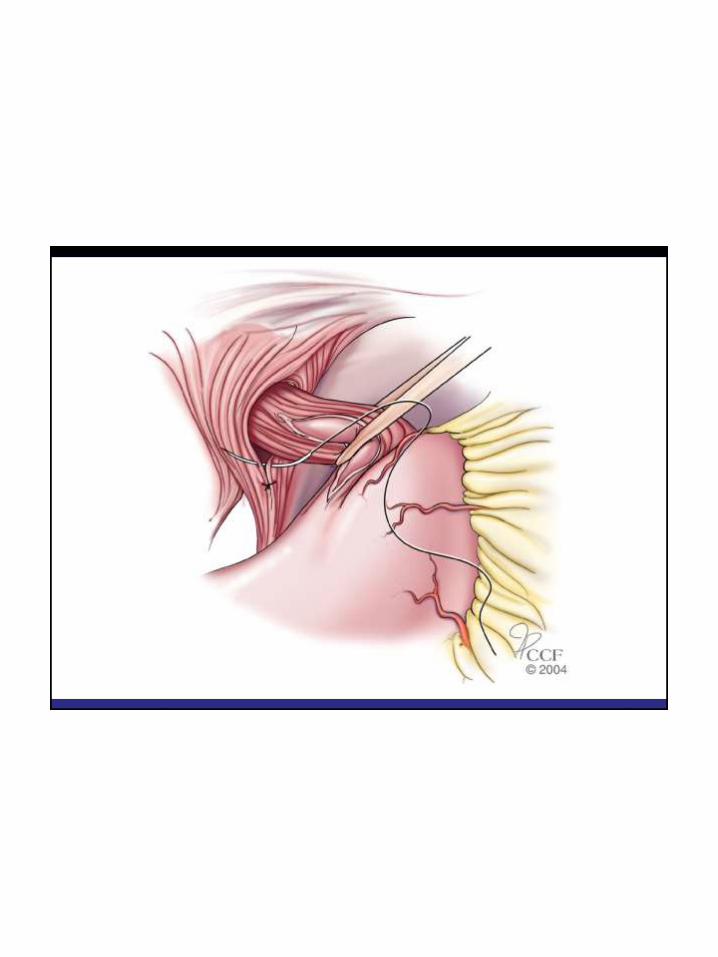
POEM – Myotomy complete
Cutting through the narrow segment of EGJ.
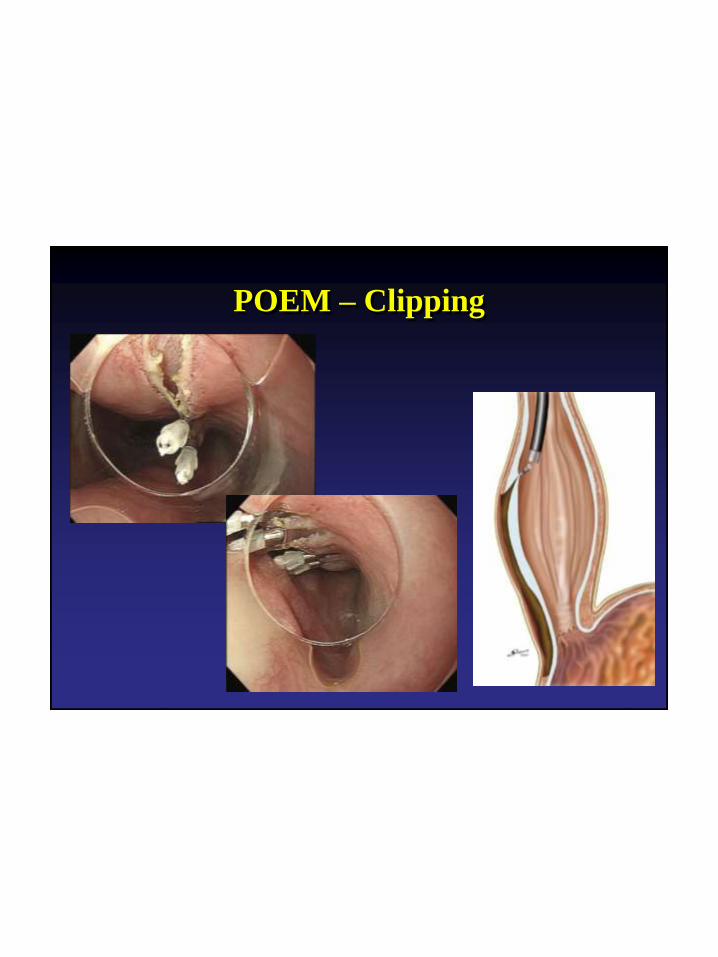
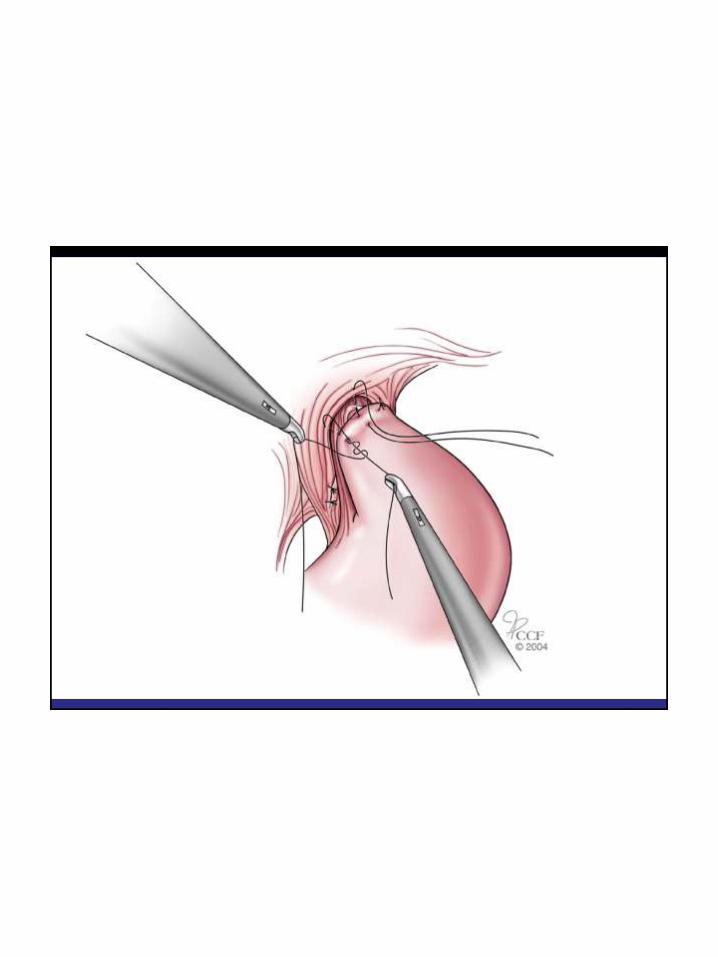
POEM – Clipping

S
before POEM after POEM
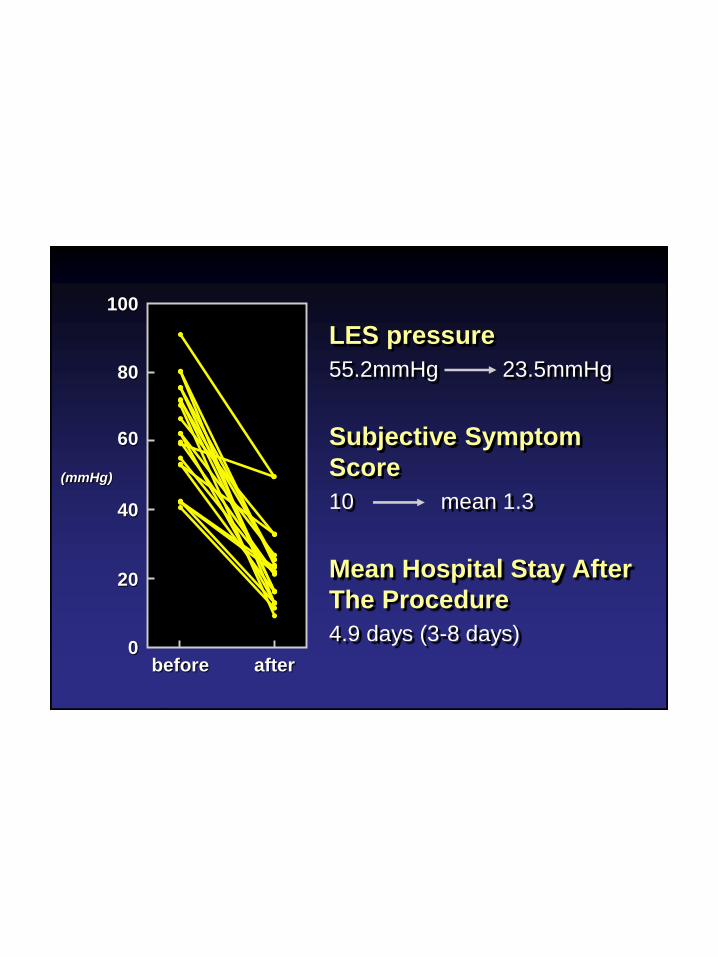
LES pressure
55.2mmHg 23.5mmHg
Subjective Symptom
Score
10 mean 1.3
Mean Hospital Stay After
The Procedure
4.9 days (3-8 days)
100
80
60
40
20
0before after
(mmHg)
When minimally invasive therapies fail,
there is maximally invasive therapy