Embed Size (px)
Citation preview

Pediatric Pulmonology 15:28-35 (1993)
Acoustic vs. Spirometric Assessment of Bronchial Responsiveness to Methacholine in Children
lgnacio Sanchez, MD, Avi Avital, MD, Isaac Wong, MD, Asher Tal, MD, and Hans Pasterkamp, MD
Summary. To study wheezing as an indicator of bronchial responsiveness during methacholine challenge (MC) in children, we used computer analysis of respiratory sounds and compared wheeze measurements to routine spirometry. MC was performed in 30 symptomatic subjects (sympt), age 11 * 3.1 years (mean f SD), with suspected asthma and in 12 controls (contr), age 10 f 3.4 years. Respiratory rate (FIR), spirometry, arterial oxygen saturation (Sa,-+), and cough were registered until the concentration provoking a 220% fall in forced expiratory flow in 1 second (FEV,; PC,,), or the end point (8 mg/mL) was reached. For 1 min after each inhalation, sounds over the trachea and posterior right lower lobe were recorded together with calibrated airflow. Computer analysis of respiratory sounds was used for objective wheeze quantification. Wheezing was measured as its duration relative to inspiration (Tfl,) and expiration (T,TT,). Seventeen of the sympt group developed wheezing (sympVVV) with 85% Tfl, or 25% Tfl,. Thirteen of the sympt did not wheeze (symptho W). Three contr developed wheeze (contrw) while 9 did not (contrho W). In sympVVV, RR increased from 20 * 6.2 per min at baseline to 25 i 9.2 (P < 0.05) at the MC concentration provoking wheeze (PC,), and S k , decreased from 97.4 f 1.2% to 95.3 * 2.4 (P < 0.05). In contrW, RR did not change, but Sao, decreased from 97.3 f 1.5% to 95.7% 2 1.2% (P < 0.05). Wheezing occurred at both recording sites and was as common during inspiration as during expiration. In subjects who had both PC, and PC,,, these variables correlated well (r = 0.82, P < 0.0001). Three SW did not reach PC,, (maximum fall in FEV, 870, 1270, and 18%). On the other hand, 6 of 13 symptho W and 2 of 12 contrho W had a positive MC. Thus, wheezing during MC had a sensitivity of 68% and a specificity of 82%. Acoustic measurements were reproducible in 14 subjects who performed a second MC within 2-10 months. We conclude that wheezing during MC in children strongly suggests airway hyperresponsiveness; however, wheeze detection cannot fully replace spirometry in bronchial provocation testing. Pediatr Pulmonol. 1993; 15:28-35. !CI 1993 Wiley-Liss. Inc.
Key words: Wheezing; respiratory sounds; tracheal; lung sounds; symptomatic vs. non- symptomatic; wheezers vs. nonwheezers; sensitivity; specificity of wheeze sounds.
INTRODUCTION
Bronchial provocation challenge is a well-known tool for assessing bronchial responsiveness in adults and chil- dren. Significant flow obstruction develops in hyperre- sponsive subjects and presents as a critical reduction in forced expiratory flows. However, tests that require cooperation for active forced expiratory maneuvers can- not be used in infants and young children. Wheezing is commonly noticed in children with airflow obstruction. Lately, there has been an increased interest in using breath sounds as a measurement of airflow obstruction in
Avital and colleagues4 have compared the concentration of methacholine that produces wheezing (PC,) and the concentration that produces a 220% fall in forced expiratory volume in 1 second (FEV,; PC,,,). They found a positive correlation between PC, and PC2<). Howcver, they assessed wheezing only by subjective tra- cheal auscultation. 0 1993 Wiley-Liss, Inc.
From the Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, Manitoba, Canada.
Received January 20. 1992; (revision) accepted for publication July 29, 1992.
Supported by Childrcn’s Hospital Rescarch Foundation, Winnipeg. Canada.
Presentcd in part at the Annual Meeting of the American Thoracic Society. May 1991, Anaheim, California.
Address correspondence and reprint requests to Dr. H. Pasterkamp. Pediatric Respirology, AE103-67 I William Avcnue, Winnipeg, Man- itoba, R3E 022, Canada.
I.S. and A.A. were recipients of a fellowship from thc Manitoba Lung Association.
I.W. was thc rccipicnt of a fellowship from the Chang Cung Memorial Hospital, Taiwan, R.O.C.
A.T. was Visiting Professor from Ben Gurion University, Bccr Shew, Israel.

Acoustic vs. Spirometric Assessment During Methacholine Challenge 29
When airways are obstructed an increase in driving pressure may not increase airflow because of so-called flow limitation.x Gavriely and co-workers have demon- strated in healthy volunteers that a wheeze occurs at flow limitation during forced expiration, provided that suffi- cient transpulmonary pressure is generated.' During tidal breathing, flows are normally not limited. If wheezing occurred during tidal breathing, this would therefore indi- cate flow limitation. Another mechanism for generation of wheezes may be vortex shedding." Objective mea- surement of wheezing is possible by spectral analysis of tracheal and lung sounds. Baughman et a1.I' introduced computerized wheeze quantification and showed that the proportion of the respiratory cycle occupied by wheeze (Tw/Tlc,,) relates to the severity of airflow obstruction. We hypothesized that objective wheeze quantification by computer might substitute for spirometric tests com- monly used to document airway obstruction. This would be of great value for the assessment of infants and young children with suspected asthma. The objective of the present study was, therefore, to characterize wheezes during MC in children and to relate wheezing to airflow obstruction.
MATERIALS AND METHODS
We studied 30 symptomatic subjects (sympt), I9 males and 1 I females, aged 1 1 2 3. I years (mean * SD; range 6- I6 years). These children were referred because of asthma suspected by their pediatricians. They were not on regular treatment with inhaled steroids or sodium cro- moglycate, and they did not use bronchodilator therapy within 12 hours prior to the study. All subjects had nor- mal spirometry and no wheezing at baseline.
The control group (contr) consisted of 12 normal sub- jects, 6 males and 6 females, aged 10 * 3.4 years (range, 6-16 years). They were recruited from healthy relatives of hospital workers and colleagues. Their personal and family histories were negative for asthma and hay fever. All participants had been free of upper or lower respira- tory tract illness during 4 weeks prior to the test. The study subjects or their parents completed a questionnaire regarding respiratory symptoms, l 2 and informed consent was obtained. The study was approved by the University of Manitoba Ethics Committee for the Use of Human Subjects.
All children were evaluated at the Pulmonary Function Laboratory of Winnipeg Children's Hospital. A respira- tory technician and a physician were always present dur- ing the test. Baseline spirometry (Spirovit, SP-200 Schiller AG, Switzerland) was obtained after inhalation of normal saline. This was followed by inhalations of doubling concentrations of methacholine, nebulized with a Wright nebulizer (10.9 L/min) for 2 minutes each, starting with 0.25 mg/mL. The response was measured as
a change in FEV, I minute after the end of each inhala- tion. The test was terminated when a concentration of drug had provoked a fall of 220% from baseline FEV, (PC,,) or when the maximum dose of 8 mg/mL was reached. In addition to spirometry, we measured heart rate (HR), respiratory rite (RR), arterial oxygen satura- tion (Ohmeda Biox 3700, USA), rcspiratory system re- sistance by the forced oscillation technique (Rr,), and ventilatory timing components (T,/Tl,,,). The presence or absence of cough was noted after each inhalation of meth- acholine. For 1 minute after each dose, sounds over the trachea and posterior right lower lobe were recorded si- multaneously using piezoelectric accelerometers (EMT 25C contact transducer, Siemens, Iselin, NJ). These were attached to the skin with 2-sided adhesive tape rings. At the same time, airflow was recorded from a calibrated pneumotachograph (Fleisch no. 3) and a differential pres- sure transducer (Validyne, 2 2 cm H20, Northridge, CA). These signals were stored on videotape (Model SVO- 150, Sony , Japan), using pulse code modulation (PCM 8 Medical Systems Corp., Greenvale, NY). Sub- sequently, the sounds were played back through anti- aliasing filters (1,200 Hz low-pass, sixth order Butter- worth) before analog-to-digital conversion (Model 2801, Data-Translation, Marlboro, MA). The sampling rate was 5.12 kHz per sound channel and 80 Hz for the flow signal.
We analyzed the data on an IBM-compatible personal computer. A customized computer program was used for data acquisition, analysis, and display. l 3 Power spectra computation of the acoustic signals was performed, using a 1,024-point fast Fourier transform (FFI'). The FFTs were applied to consecutive 100 ms intervals, resulting in 50% overlap into adjacent segments. This allowed the use of a Hanning window for digital signal processing without loss of information. All recordings were ana- lyzed by automated wheeze quantification, based on peak frequency,I4 and by assessment of the sound wave in the time domain. In addition, we used auditory verification on digital-to-analog playback. This was done by 2 physi- cians who were not involved in the recordings and test procedures.
A positive response to methacholine by spirometry was defined as a fall in FEV, of 320% from baseline at a concentration of S 8 mg/mL. A positive response to methacholine by acoustic measurements was defined as the presence of wheeze for at least 3% of the time during inspiration (T,/T, 2 0.03) or during expiration (TJ T, 5 0.03) at a concentration of <8 mg/mL. In our labo- ratory, automatic characterization of wheeze in older sub- jects has resulted in <3% of both false-positive and false- negative detection. l4
In order to evaluate the reproducibility of the test, MC with sound recording was repeated in 14 subjects (12 symptomatic and 2 control), 2-10 months after the first

30 Sanchez et al.
TABLE 1-Measurements at Baseline in Symptomatic and Control Subjects (mean * S.D.)
Sympt. Contr. (n = 30) (n = 12)
Heart rate (bpm) 95 2 11.2 21 f 5.8 91 t 1.4
Respiratory rate (cyclcs/min) Oxygen saturation (5%) Ti/Ttot 0.41 2 0.05 Presence of cough Nonc FEV, (Yo predicted) 99 2 4. I FEF,,, (% predicted) 100 f 12.5 R, (cmH,O)/L/s) 1 f 2.3
9 0 k 11.3 22 f 8.4 91 * 1.1
0.43 t 0.04 None
104 t 10.0 103 * 7.7 1 t 2.4
FEV, , forced expiratory volume in I second; FEF,,,, forced expir-flow at 508 of forced vital capacity; R,. respiratory system rcsistance.
test. The selection of these subjects was based on their availability and agreement to return for repeat testing. The patients had been free of lower respiratory illnesses or episodes of wheezing for at least 4 weeks before the second test. The geometric means for PC,,, and PC, in each subgroup were calculated and compared using the unpaired Student’s t-test. Correlations were calculated by linear regression analysis. Changes in oxygen saturation (Sa,,), RR, HR, T,/T,,,t, and R,, from bascline to the final dose-of methacholine were calculated. In addition, the occurrence of cough during the test was noted. Values in each subgroup were compared using the paired Student’s t-test. We considered P < 0.05 as statistically signifi- cant.
RESULTS
Thc condition at bascline of the 30 symptomatic and 12 contrd subjects is shown in Table 1 . There was no signif- icant difference between the 2 groups. Information col- lected from the questionnaire showed that 20 symptom- atic subjects (sympt) had wheezed before the test and had the diagnosis of asthma, and 25 had previously taken anti-asthmatic medication. Sixteen had a history of hay fever or eczema, and in 5 subjects one or both parents had asthma. In concordance with the inclusion criteria, none of the subjects in the control group (contr) had either a personal or family history of asthma.
Seven of 30 sympt had neither PC, or PC,,,, and 7 of I2 contr were negative for both wheeze and fall in FEV I .
The majority of all syrnpt who responded to MC with a significant fall in FEV, ( 14 of 23) also developed wheeze (sympVW), compared to 3 of 5 in the contr group (contr/ W). Six symptomatic subjects had only PC,,, without wheeze (symptho W) (PC,, 0.48-1.7 mg/mL; change in FEV, , 23-56%) compared to 2 of 5 in the control group (contrho W) (PC,(, 3.5 and 6.5 mg/mL). Interestingly, 3 patients of the sympt had only wheeze, with no signifi- cant fall in lung function (change in FEV,, 8%, 12%, and 18%). No wheeze at C20% fall in FEV, was seen in contr.
TABLE 2-Characteristics of Symptomatic Subjects With a Positive Methacholine Challenge at the Final Concentration of Methacholine (mean ? S.D.)
Symptomatic Symptomatic with wheeze without wheeze
( n = 14)
10.2 -c 3 .1 (n = 6)
8.6 t 2.1 Age (yearb) Heart rate (bpm) 89 t 10.4 83 f 9.6 Respiratory rate (cycleshin) 26 ? 9.4 29 * 3.4
TJT,,,, 0.41 k 0.04 0.39 k 0.03 Oxygen saturation (8) 95 f 2.5 9 6 2 1.4
Presence of cough 12/14 516 FEV, (96 prcdicted) 12 * 18.4 61 -C 15.2 FEF,,, (% predicted) 56 2 23.1 49 * 15.0
10 f 2.0 R,, (cm H20/L/s) PG, , (mg/mL) 3.1 2 2.1 1.28 ? 0.45
11 f 3.5
Max FEV, change 35 t 16.2 35 t 13.8
Abbreviations as in Table I .
The data obtained at the PC,,, are shown in Table 2. There were no significant differences between those sub- jects who developed wheeze and those who did not. In sympVW, RR increased from 20 2 6.2 per minute at baseline to 25 2 9.2 per minute at the final concentration (P < 0.05), and Sa,, decreased from 97.4 2 1.2% to 95.3 2 2.4% ( P < 0.05). In contr/W, RR did not change, but Sac,, decreased from 97.3 * 1.5% to 95.7 -+ 1.2% ( P i O . 0 5 ) . HR and T,/T,,,, did not change in either group. Sympt/no W and contr/no W had no significant change in any of these parameters. Neither sympt or contr coughed at baseline, but I2 sympt/W and 2 contr/W coughed at PC2{), while 5 symptho W and one contr/no W coughed at the final concentration of meth- acholine.
In the 17 subjects (sympt and contr) with both PC, and PC2[), there was a significant correlation between the concentration of methacholine associated with wheeze and that causing a 220% fall in FEV, (r = 0.82, P < 0.OOOI).
Six subjects who were moderately to severely sensitive to MC (PC?,, below 2.0 mg/mL and changes of FEV, up to 56%) did not wheeze. Three of those who wheezed but had no significant fall in FEV, had PC, at 4, 8, and 8 mg/mL. Of the 42 children studied, 25 had a positive spirometric response and 17 of these developed whcez- ing. Thus, the sensitivity of wheeze detection as an indi- cator of bronchial hyperreactivity in our subjects was 68%. Fourteen of the 17 spirometric nonresponders to methacholine did not develop wheezing as assessed by acoustic measurements; this yields a specificity of 82%. Acoustic assessment revealed 3 of 17 false-positive tests ( 18%) and 8 of 25 (32%) false-negative tests.
The wheeze pattern was quite variable between sub- jects, and wheezing was as common during inspiration as it was during expiration (Table 3) . Two of 17 sympt had wheeze only over the lung and not over the trachea.

Acoustic vs. Spirometric Assessment During Methacholine Challenge 31
TABLE %Wheeze Patterns Among Subjects (Percent of the Time With Wheeze)
Trachcal wheeze Lung wheeze
Symptomatic Inspiration Expiration Inspiration Expiration
Subject no. I 2 3 4 5 6 7 8 9
10 II 12 13 14 15 16 17
Control no. 18 19 20
1 76
6 15 47
0 28 0
17 0 0 8 3 2
38 1
56
0 63 38
6 71 10 25 53
I 24
5 16 0
27 4 5
18 21
8 47
17 54 62
1 59 17 73 29 20 0 0
14 0 0
44 I 0
17 0 5
0 28 28
26 61 12 43 45 0 0 6 0 6
37 I 2 0 0 0
20
I 48
9
Digital respirosonograms of wheezes from the trachea and lung are presented in Figs. 1 and 2, and show typical acoustic characteristics of musical adventitious sounds. The respirosonograms illustrate how wheeze is quantified by its duration during the respiratory cycle and is charac- terized by its frequency components and its intensity.
In 14 subjects who returned for a second MC 2-10 months after the initial test, there was a good reproduc- ibility of the maximum fall in FEV, and of acoustic measurements, while PCza was variable (Table 4).
DISCUSSION
The majority of children with suspected asthma who responded to methacholine challenge with significant air- flow obstruction also developed wheezing. The sensitiv- ity of wheezing for detecting bronchial hyperresponsive- ness was 68%, with a specificity of 82%. This is different from findings of Baumann et a]., who did not detect wheezing by subjective auscultation in more than 60% of adult asthmatic subjects after histamine challenge. I 5 Most of the responders in our study had wheeze onset within one concentration of the provocative dose that produced a 220% fall in FEV, from baseline. It is note- worthy that 7 of the symptomatic children (23%) had no bronchial hyperresponsiveness on MC and they also did not wheeze. We could, therefore, not substantiate their presumed diagnosis of asthma. This discrepancy may be explained by the referral criteria and by the sensitivity of MC per se.
We also found 40% of control subjects to respond positively to the bronchial provocation. Others have re- ported bronchial hyperresponsiveness in over 50% of normal children. This large proportion of hyperrespon- sive normal subjects may be related to age. ''-I'' Actually, the 5 normal subjects in this study who responded posi- tively to methacholine were less than 10 years old, and they presented mild nonspecific airway hyperresponsive- ness (PC,,, 2.0-6.5 mg/mL). Clifford et al.'" found atopy in otherwise normal children to be closely related to methacholine hyperresponsiveness, but we did not in- clude atopic individuals in the control group. Our obser- vation of a positive methacholine challenge in 76% of symptomatic subjects is in accordance with published data. * '
Any comparison of acoustic measurements and spirometry during bronchial provocation challenge has to take into account that the occurrence of wheeze may be a local event reflecting critical flow and pressure condi- tions in one or more airways, compared to the flows measured at the mouth. We included only those patients with baseline spirometry within a normal range (380% in expiratory flows). Since we do not know the normal best value for each individual, a 20% fall in FEV, from base- line could have reflected different decrease in airway diameter, which might have had an effect on the site of wheeze generation. It is also important to note that the acoustic measurements were obtained during tidal breath- ing, while forced expiratory maneuvers were required during spirometry . Thus, transpulmonary pressure and airway configuration during wheeze recording and spirometry will be quite different.
Our observations demonstrate a subgroup of subjccts who do not wheeze despite significant airflow obstruc- tion. While a silent chest is well recognized as an omi- nous finding in patients with extremely severe asthma, the range of fall in FEV, in this subgroup was moderate (23-5696) and breath sounds were clearly present. Avital and co-workers also found 3 of 15 subjects who did not wheeze despite a 220% fall in FEV, during meth- acholine ~ h a l l e n g e . ~ Two of their 3 subjects had moder- ate to severe hyperresponsiveness (PC,,, G 2.0 mg/mL), while all 6 subjects in our study had a PCzO =s 2.0 mgl mL. It is interesting to note, in this context, that 2 of our control subjects also developed flow obstruction without wheeze. However, their PC2{] showed only mild hyperre- sponsiveness ( 2 2 . 0 mg/mL) and their maximum fall in FEV, was less than 24% from baseline.
Since we used only 2 microphones located over the trachea and right posterior lower lobe, it is possible that wheezing was missed over other sites of the chest. Wheezing could also have been missed by Avital et al., who only listened to the trachea, whereas the present study demonstrates that wheezing may be limited to the chest. The presence of a negative wheeze response in

32 Sanchez et al.
Fig. 1. Left panel: digital respirosonogram of tracheal sounds over 6 seconds. Calibrated flow is plotted at the top, and the raw sound signal is displayed below. The respirosonogram shows time on the horizontal and frequencies on the vertical axes. Sound intensity is indicated on a black-to-white scale. Right
panel: Details of a selected 100 ms segment between vertical double bar of lefl panel at 5.3 sec. The signal waveform is dis- played at the top and the Fourier spectrum of this segment at the bottom. Squares filled on the x-axis indicate wheeze. Note both inspiratory and expiratory wheeze.
subjects with significant airflow obstruction was repro- ducible in all 4 symptomatic subjects who returned for a second challenge. This preliminary observation needs to be confirmed in a larger group of subjects. Recently, Avital and co-workers” have shown in a group of asth- matic children that the concentration that produced wheeze corresponded closely with the concentration that produced a 27% fall in FEV,. In our study, 5 of 8 non- wheeze responders had maximum fall in FEV, of less than 27%, and it is possible that these subjects did not reach the severity of airflow obstruction where wheezing would have occurred.
We can only speculate on mechanisms for the absence of wheezing in the presence of significant airflow ob- struction. Gavriely and co-workers showed in normal subjects that flow limitation alone during forced expira- tion did not produce a wheeze unless transpulmonary pressures reached a critical level.’ They speculate that this pressure is needed to flatten and deform airways into a shape that facilitates oscillations. lnvasive measure- ments, such as esophageal pressure monitoring, were not
part of our study, therefore, we cannot comment on transpulmonary pressures in our subjects.
Since only dynamic but not static pulmonary function was measured and compared to acoustic data, we do not know whether those who responded to methacholine but did not wheeze might have had more severe hyperinfla- tion than those who wheezed. Greatly increased lung volumes could tether airways to a degree that would prevent wheeze generation. Also, increased airway clo- sure and air trapping may reduce regional airflow to less than required for wheeze production. Standard spiromet- ric measurements, however, could not detect a difference between those who wheezed and those who did not. Fi- nally, methacholine provocation not only causes a de- crease in the diameter of the airways but may also make them more rigid. Thus, the oscillation characteristics of the airway wall itself may change significantly during the course of a MC.
There were also 3 symptomatic subjects but none among controls who wheezed with <20% fall in FEV, . These 3 had only mild degrees of hyperresponsivcncss,

Acoustic vs. Spirometric Assessment During Methacholine Challenge 33
UI I
Fig. 2. Respirosonogram of lung sounds over the right posterior lower lobe during 6 seconds. Note a loud inspiratory wheeze and a faint expiratory wheeze. For details see the legend to Fig. 1.
with PC2(, a4.0 mg/mL. We could not reproduce this finding on a second test in 1 of the 3 subjects who initially had an expiratory wheeze (5% over trachea and 6% over the lung, with a maximum fall in FEV, of 8%). Another subject in this group did reach PC,, on a second test and wheezed with a fall in FEV, of 23%, while the maximal fall had been 18% on the first test (Table 4, subject 5). If* we include this patient, the sensitivity of wheeze as an indicator of bronchial hyperresponsiveness increases to 70% and the specificity to 88%. The third subject has not returned for repeat testing. He was quite wheezy on the initial test (T,/T, 20% over the lung), with a drop in FEV , of only 12%. We assume that local airway obstruc- tion occurred but was not sufficient to produce a 20% fall in FEV, in these 3 subjects during the initial challenge. Thus, we speculate that wheezing during methacholine challenge may in some children be more sensitive than spirometry to indicate bronchial hyperresponsiveness. This would require further study, since spirometry is the gold standard for the assessment of bronchial obstruction.
The pattern of wheezing was quite variable between the subjects in our study. There were those who wheezed during expiration or inspiration only, and others who had wheezing only over I of the 2 recording sites. While
textbooks often describe wheezing in asthma as an expi- ratory phenomenon, published data on clinical observa- tions,2' as well as actual wheeze m e a s ~ r e m e n t s , ~ ~ have documented that wheezing occurs during both respiratory phases. There was no correlation between pulmonary function and the pattern of wheezing in our subjects.
Anderson and c o - ~ o r k e r s ~ ~ have postulated that lung sound characteristics other than wheeze could help in the detection of flow destruction. They found in adults with mild asthma that the fall in FEV, from baseline during histamine challenge correlated with an upward shift of the median frequency in the power spectrum of the breath sounds. They speculate that the spectrum of breath sounds during inspiration could reflect airway diameter and could therefore indicate airway obstruction, even in the absence of wheeze. However, we believe that power spectra of respiratory sounds which do not contain wheeze should only be compared at similar flows. The subjects in our study were not instructed to breathe at standardized flows during the recording of respiratory sounds. Since their mean inspiratory flows were lower at baseline than at the end point of the inhalation challenge, we did not analyze for changes in the median frequency. Further studies using standardized flows and measure-
34 Sanchez et al.
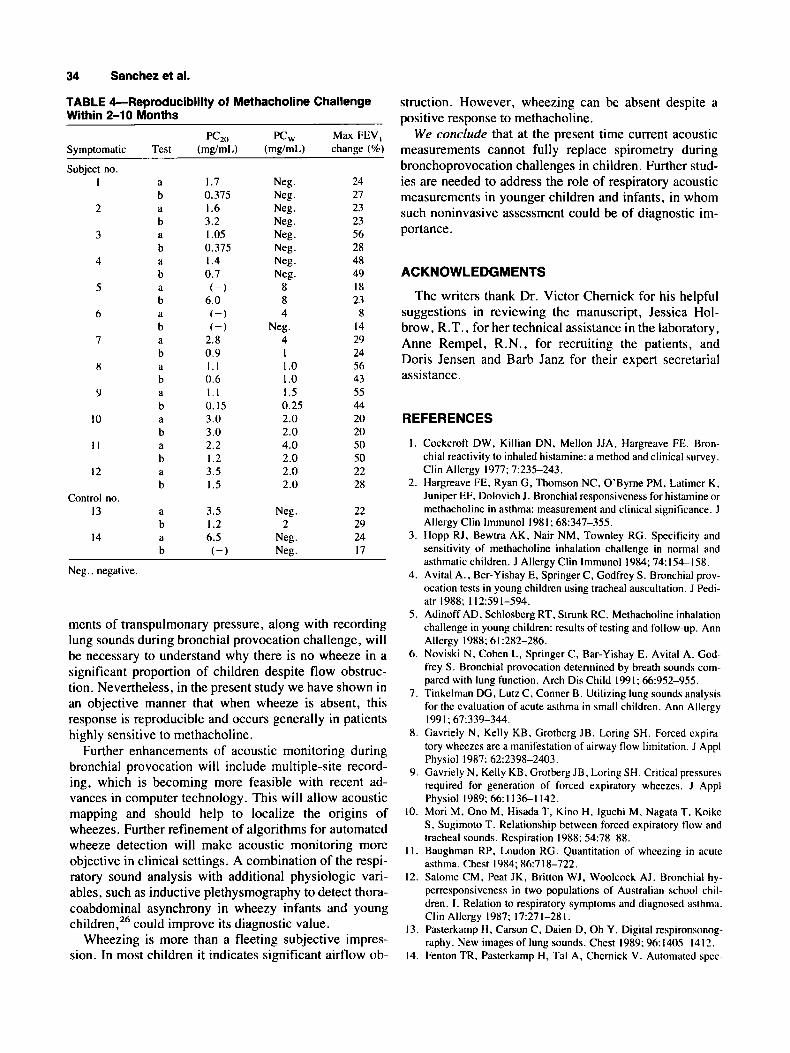
TABLE 4-Reproducibility of Methacholine Challenge Within 2-10 Months
PC20 PCW Max FEV, Symptomatic Test (mg/mL) (mg/mL) change (%)
Subject no. I
2
3
4
5
6
7
8
9
10
I 1
12
Control no. 13
14
a b
b a b
b a b
b a b
b
b
b a h a b
a b a b
a
d
d
a
a
a
1.7 0.375 I .6 3.2 I .05 0.375 I .4 0.7 (-)
6.0 ( - 1 ( - )
2.8 0.9 1 . 1 0 . 6 1.1 0.15 3.0 3.0 2.2 I .2 3.5 1.5
3.5 I .2 6.5 ( - )
Neg. 24
Neg . 23 Neg. 23 Neg . 56 Neg. 28 Neg . 48
8 I X 8 23 4 8
Neg . 14 4 29 I 24 I .o 56 I .o 43 I .5 55 0.25 44 2.0 20 2.0 20 4.0 50 2.0 50 2.0 22 2.0 28
Neg. 21
Neg . 49
Neg. 22 2 29
Neg. 24 Neg. 17
Neg.. negative.
ments of transpulmonary pressure, along with recording lung sounds during bronchial provocation challenge, will be necessary to understand why there is no wheeze in a significant proportion of children despite flow obstruc- tion. Nevertheless, in the present study we have shown in an objective manner that when wheeze is absent, this response is reproducible and occurs generally in patients highly sensitive to methacholine.
Further enhancements of acoustic monitoring during bronchial provocation will include multiple-site record- ing, which is becoming more feasible with recent ad- vances in computer technology. This will allow acoustic mapping and should help to localize the origins of wheezes. Further refinement of algorithms for automated wheeze detection will make acoustic monitoring more objective in clinical settings. A combination of the respi- ratory sound analysis with additional physiologic vari- ables, such as inductive plethysmography to detect thora- coabdominal asynchrony in wheezy infants and young children,26 could improve its diagnostic value.
Wheezing is more than a fleeting subjective impres- sion. In most children it indicates significant airflow ob-
struction. However, wheezing can be absent despite a positive response to methacholine.
We conclude that at the present time current acoustic measurements cannot fully replace spirometry during bronchoprovocation challenges in children. Further stud- ies are needed to address the role of respiratory acoustic measurements in younger children and infants, in whom such noninvasive assessment could be of diagnostic im- portance.
ACKNOWLEDGMENTS
The writers thank Dr. Victor Chernick for his helpful suggestions in reviewing the manuscript, Jessica Hol- brow, R.T., for her technical assistance in the laboratory, Anne Rempel, R.N., for recruiting the patients, and Doris Jensen and Barb Janz for their expert secretarial assistance.
REFERENCES
1.
2.
3.
4.
5 .
6 .
7.
8.
9.
10.
1 I .
12.
13.
14.
Cockcroft DW, Killian DN, Mellon JJA. Hargreave FE. Bron- chial reactivity to inhaled histamine: a method and clinical survey. Clin Allcrgy 1977; 7:235-243. Hargreave FE. Ryan G, Thomson NC, O'Byrne PM. Latimcr K, Juniper EF, Dolovich J. Bronchial responsivcness for histamine or methacholinc in asthma: measurement and clinical significance. J Allergy Clin lmmunol 1981; 68:347-355. Hopp RJ. Bewtra AK, Nair NM. Townley RG. Specificity and sensitivity of methacholine inhalation challenge in normal and asthmatic children. J Allergy Clin lmmunol 1984; 74:154-158. Avital A., Ber-Yishay E, Springer C , Godfrcy S. Bronchial prov- ocation tests in young children using tracheal auscultation. J Pedi- atr 1988; II2:SY 1-594. Adinoff AD, Schlosbcrg RT, Strunk RC. Methacholine inhalation challenge in young children: rcsults of testing and follow-up. Ann Allergy 1988; 61:282-286. Noviski N, Cohen L, Springer C, Bar-Yishay E. Avital A. God- frey S. Bronchial provocation determincd by breath sounds com- pared with lung function. Arch Dis Child 1991; 66:952-955. Tinkelman DG, Lutz C , Conner B. Utilizing lung sounds analysis for the cvaluation of acute asthma in small children. Ann Allergy
Gavriely N . Kelly KB, Grotberg JB. Loring SH. Forced expira- tory wheezes are a manifestation of airway flow limitation. J Appl Physiol 19x7: 62:2398-2403. Gavriely N, Kelly KB, Grotberg JB. Loring SH. Critical pressures required for generation of forced expiratory wheezes. J Appl Physiol 1989; 66:1136--1142. Mori M, Ono M. Hisada T. Kino H, lguchi M, Nagata T. Koike S, Sugimoto T. Relationship between forced expiratory flow and tracheal sounds. Rcspiration 1988: 54:78-88. Baughman RP, Loudon RG. Quantitation of wheezing in acute asthma. Chest 1984; 86:7 18-722. Salome CM, Peat JK. Britton WJ, Woolcock AJ. Bronchial hy- perresponsiveness in two populations of Australian school chil- dren. I. Relation to respiratory symptoms and diagnosed asthma. Clin Allcrgy 1987: 17:271-281. Pasterkamp H, Carson C , Daien D, Oh Y. Digital respironsonog- raphy. New images of lung sounds. Chest 1989: 96:1405-1412. Fenton TR, Pasterkamp H, Tal A, Chcrnick V. Automated spcc-
1991; 671339-344.

Acoustic vs. Spirometric Assessment During Methacholine Challenge 35
tral characterization of wheezing in asthmatic children. IEEE Trans Biomed Eng 1985; 3250-55.
15. Baumann UA, Haerdi E, Keller R. Relations betwccn clinical signs and lung function in bronchial asthma: How is acute bron- chial obstruction reflected in dyspnea and wheezing? Respiration 1986; 50:294-300.
16. Pattemore PK, Asher MI, Harrison AC, Mitchell EA, Rea HH, Stewart AW. The interrelationship among bronchial hyperrespon- siveness, the diagnosis of asthma and asthma symptoms. Am Rev Respir Dis 1990; 142549-554.
17. Moreno R, Sanchez I, Leiva A, Corrales R. The shape and posi- tion of the airway dose-response curve to methacholine in non asthmatic children. Am Rev Resp Dis 1989; 139:A498 (abstract).
18. Northway WH, Moss RB, Carlisle KB, Parker BR. Popp RL, Pitlick FT, Eichler 1, Lamm RL, Brown BW. Late pulmonary sequelae of bronchopulmonary dysplasia. N Engl J Med 1990; 323~1793-1799.
19. Cockcroft DW, Hargreave FE. Airway hyperresponsiveness. Rel- evance of random population data to clinical usefulness. Am Rev Respir Dis 1990; 142:497-500.
20. Clifford RD, Radford M, Howell JB, Holgate ST. Prevalence of
atopy and range of bronchial response to methacholine in 7 and I I year old schoolchildren. Arch Dis Child 1989; 64:l 126-1 132.
21. Spiropoulos K, Stevens J , Eigen H, Spiropoulos A. Specificity and sensitivity of methacholine challcnge test in children with normal and hyperreactive airways. Acta Paediatr Scand 1986; 75:737-743.
22. Avital A, Noviski N, Bar-Yishay E, Springer C, Levy M, Godfrey S. Nonspecific bronchial reactivity in asthmatic children depends on severity but not on age. Am Rev Respir Dis 1991; 144:36-38.
23. Shim CS, Williams MH. Relationships of wheezing to thc severity of obstruction in asthma. Arch Intern Med 1983; 143:890-892.
24. Pasterkamp H, Tal A, Leahy F, Fenton R, Chernick V. The effect of anticholinergic treatment on postexertional wheezing in asthma studied by phonopneumography and spirometry . Am Rev Resp Dis 1985; 132:16-21.
25. Anderson K, Aitken S, Carter R, MacLeod JES, Moran F. Varia- tion of breath sound and airway caliber induced by histamine challenge. Am Rev Respir Dis 1990; 141:1147-1150.
26. Allen JL, Wolfson MR, McDowell K, Shaffer H. Thoracoabdom- inal asynchrony in infants with airflow obstruction. Am Rev Respir Dis 1990; 141337-342.