Embed Size (px)
Citation preview
Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
February 2018
We support providers to give patients
safe, high quality, compassionate care
within local health systems that are
financially sustainable.
1 | > Contents
Contents
1. Activity plans: overview .............................................................. 2
2. Summary of changes ................................................................. 3
3. Assurance statements ............................................................... 3
4. Support ...................................................................................... 4
5. Guidance ................................................................................... 6
Annex A: Ambulances – count of incidents by category ................ 7
Annex B: Total non-elective admissions with a zero length of stay and non-elective admissions with a length of stay of one day or longer (Specific Acute) ................................................................. 10
Annex C: Total elective spells (specific acute) ............................. 12
Annex D: Average number of G&A beds open per day (specific acute) ........................................................................................... 14
Annex E: Incomplete RTT pathways (specific acute) ................... 16
Annex F: Acute provider template ................................................ 18
Annex G: Ambulance provider template ...................................... 19
2 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
1. Activity plans: overview
This is supplementary information relating to the draft operational plan submission
process for February 2018, following publication of the NHS shared planning
guidance, NHS operational planning and contracting guidance 2017/18 and
2018/19 on 22 September 2016, we are now sharing additional information relating
to the draft operational plan submission process for 2018/19.
This document updates trusts on the planning process and contains extra reporting
guidance for acute trusts and guidance for the new ambulance activity plan lines for
2018/19.
The template has a tab for the trust’s planned activity that includes: referrals, bed
numbers, outpatients, inpatients, accident and emergency and referral to treatment.
This year there are new activity lines for ambulance trusts. Only the lines applicable
to the reporting organisation will be visible on the template.
The pre-populated template will be posted on your Sharepoint portal on the
afternoon of Thursday 8 February 2018. There are examples of the templates in
annex F and annex G.
The templates will be accessible via your trust SharePoint portal. To access this
you will need navigate to the URL for your trust portal (if you do not know this,
please contact [email protected]). You also need to have a user
name and password, which if you don’t already have, you can e-mail the same
address to obtain one. Full user guidance for SharePoint is available here:
SharePoint user guide.
The acute trust template posted on your SharePoint site will have the forecast
outturn (FOT) using M8 SUS data, as well as the activity lines with the reporting
trust’s final submission from the 2016/17 activity planning round. The template
figures will be editable, but we will expect you to comment on any changes to the
FOT.
There are validations built into the template to help your submissions. Activity plans
with more than 5% growth in activity will require you to explain the change.
3 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Draft and finalised operational activity planning submissions should be submitted in
accordance with the timescales set out in the joint planning letter guidance.
2. Summary of changes
There are extra lines to be collected in the template for acute providers and a new
set of activity lines for ambulance trusts.
There are four new lines and four additional activity existing plan line splits. The
new lines for acute trust submission are number of incomplete referral to treatment
(RTT) pathways and number of general and acute (G&A) beds open per day on a
quarterly basis. The RTT lines will consist of incomplete waits where patients have
waited 18 weeks or less, those who have waited over 18 weeks and patients
waiting over 52 weeks. Bed data submissions should be consistent with the KH03
guidance for average number of G&A overnight beds open per day during the
quarter.
The plan lines that acute trusts have provided during the initial planning process will
this year be expected to submit a breakdown of the ‘Total elective admission spells’
line. They will be broken down into separate lines for ordinary elective admissions
and day case elective admissions.
There is also a breakdown of the ‘Total non-elective admissions’ line. The
expectation is that there will be separate lines for non-elective patients with a zero
length of stay and non-elective admissions with a length of stay of one or more
days.
Ambulance trusts will be expected to submit 2018/19 monthly plan figures for
responses to incidents by category. There will not be a pre-populated FOT as the
volumes of activity in the current reporting format have not been running for long
enough for NHS Improvement to produce an accurate forecast.
3. Assurance statements
Access to up to 30% of a trust’s Sustainability and Transformation Fund (STF)
allocation depends on it maintaining delivery of core access standards through
2018/19. Where trusts do not have an STF trajectory to deliver the four-hour
4 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
accident and emergency (A&E) waits, referral to treatment (RTT) 18-week
incomplete pathways and 62-day cancer waits for patients by March 2019. These
will form part of the NHS standard contract for 2018/19 and show how the trust will
achieve this national standard by March 2019 at the latest.
In line with the planning process last year, trusts will need to submit signed
assurance statements for trusts that have agreed their control total. Assurance
statements will be posted on trust SharePoint portals and will be required for the
final submission only.
4. Support
To help trusts submitting the most accurate activity plans, we will be providing web
conferences and Excel with modelled forecasts for each provider.
The web conferences will run in February, from the week starting 12 February
2018, to help you complete the templates and answer any queries. There will be
three web conferences for acute providers which will run for two hours and a web
conference for ambulance trusts which will run for an hour. The web conferences
will include:
• what we expect of the trust returns and timetable
• guidance for each activity line
• methodology presentation on the profiling by our analytics team
• feedback/queries session from trusts.
Each acute trust will can get an Excel file containing activity profiles produced by
the analytics team by e-mailing: [email protected]. Each of the activity lines
have been profiled in the statistical modelling software R by using SUS data for
trust’s previous four years activity. You can use these to compare with/validate
against your planning submission.
To attend the web conferences dial into one of the session. Dates and times are on
the next page.
5 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Use the details listed below for the web conference you intend to join. (You should
use Internet Explorer to enter the meeting)
Acute trusts web conference dates:
Friday 16 February; 10am–12.00pm
Meeting number: 951 156 836
Meeting password: 12345
Join the meeting
Friday 16 February; 1:30pm– 3.30pm
Meeting number: 954 307 281
Meeting password: 12345
Join the meeting
Monday 19 February; 10am – 12pm
Meeting number: 957 512 506
Meeting password: 12345
Join the meeting
Ambulance trust web conference date:
Monday 19 February; 1pm – 2pm.
Meeting number: 956 998 073
Meeting password: 12345
Join this meeting
6 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
5. Guidance
A link to the full list of activity guidance (excluding the new lines in this document) is
available in the joint technical guidance:
www.england.nhs.uk/wp-content/uploads/2015/12/joint-technical-definitions-
performance-activity.pdf
There is extra guidance for the new lines for 2018-19 plans in the following
annexes:
• Ambulance activity line has been added as Annex A
• Non-elective activity lines as Annex B
• Elective activity lines as Annex C
• Beds collection lines have been added to this document as Annex D
• Referral to treatment lines have been added to this document as Annex E.
We have also published the trust portal submission instructions on the shared
planning guidance site on our website: https://improvement.nhs.uk/resources/nhs-
shared-planning-guidance
If you have any questions about completing the template, please email:
7 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex A: Ambulances – count of incidents by category
Definitions – detailed descriptor
Category 1 (C1)
C1 covers a wider range of conditions than the former Red 1 category. For this
reason, the attendance of a bystander with a defibrillator will no longer be regarded
as a response that stops the ambulance response time clock. However, first
responder schemes, through which the trust actively deploys volunteers and staff
from other agencies who have additional training and capabilities in airway
management and oxygen therapy, are deemed to be an appropriate resource to
stop the response time clock for C1 patients. It continues to be the policy that the
deployment of a first responder must not delay the deployment of a trust response
vehicle. A healthcare professional on scene with a C1 patient, who has access to a
defibrillator, is the only example where a resource that has not been deployed by
the trust can stop the clock.
We recognise the importance of early defibrillation and cardiopulmonary
resuscitation (CPR), and the positive impact that these interventions have on
patient outcomes. Bystander defibrillation and CPR will be encouraged through the
introduction of a new measure from the time of the call to the time of
commencement of CPR.
We have encouraged the rapid provision of transportation for C1 patients by
retaining a measure for the arrival of the conveying resource, C1T. We have
tightened the clock start for this measure by aligning the C1T clock start to the C1
clock start, rather than giving the option to start the clock at the point that the first
clinician on scene requests conveyance. We have not specified what type of vehicle
counts as a conveying resource in recognition of innovations such as advanced
paramedics operating in cars adapted for the transportation of suitable patients.
The intent is to measure the arrival of the vehicle that was able to convey the
patient. For example, a car would not stop the C1T response time clock if it is not
the vehicle that conveys the patient. Category 2, 3 and 4 (C2, C3 and C4)
The intent is to ensure that patients in these categories who require transportation
receive a conveying resource in a timeframe appropriate to their clinical needs. The
8 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
technical guidance is intended to prevent situations where a patient is attended by
an ambulance solo responder simply to stop the response time clock, but who is not
able to convey the patient to a place of definitive care.
To that end an ambulance solo responder will only stop the clock where no patient
is conveyed. For all incidents that require transportation in an emergency timescale,
it is the arrival of the conveying resource that will stop the clock. In addition, we
have introduced clinical measures (not included in this technical guidance) to
ensure the rapid response of a conveying resource to stroke and ST-elevated
myocardial infarction (STEMI) patients.
Lines within indicator (units)
A8 C1 incidents
The count of incidents coded as C1 that received a response on scene.
A9 C1T incidents
The count of C1 incidents where any patients were transported by an ambulance
service emergency vehicle.
Do not include incidents where an ambulance clinician on scene determines that no
conveyance is necessary, or incidents with non-emergency conveyance.
A10 C2 incidents
The count of incidents coded as C2 that received a response on scene.
A11 C3 incidents
The count of incidents coded as C3 that received a response on scene.
A12 C4 incidents
The count of incidents coded as C4 that received a response on scene.
(Reference codes A8-A12 correspond with NHS England’s ambulance quality
indicator guidance.)
9 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Rationale
A new series of standards, indicators and measures has been introduced through
the Ambulance Response Programme for publication in NHS England’s ambulance
quality indicators.
Monitoring
Monitoring frequency:
Monthly
Monitoring data source:
NHS England ambulance quality indicators
Further information
Further information on data available to support this metric can be found on the
ambulance quality indicators landing page:
www.england.nhs.uk/statistics/statistical-work-areas/ambulance-quality-indicators/
10 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex B: Total non-elective admissions with a zero length of stay and non-elective admissions with a length of stay of one day or longer (Specific Acute)
Definitions
Detailed descriptor:
Total number of specific acute (replaces G&A) non-elective spells with a zero length
of stay and with a stay of 1 day or more in a month.
Lines within indicator (units):
Number of specific acute non-elective spells in the period.
Data definition:
A non-elective admission is one that has not been arranged in advance. Specific
acute non-elective admissions may be an emergency admission or a transfer from
a hospital bed in another healthcare provider other than in an emergency.
Number of specific acute hospital provider spells for which:
• • Der_Management_Type is ‘EM’ and ‘NE’
Use criteria for either the zero or 1 or more days length of stay case lines:
• Hospital Provider Spell LOS <1 (non-elective admissions with a zero length
of stay)
• Hospital Provider Spell LOS >=1 (non-elective admissions with a length of
stay of one or more days)
Where ‘EM’ = Emergency and ‘NE’ = Non-Elective
11 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Monitoring
Monitoring frequency:
Monthly
Monitoring data source:
Secondary Uses Service tNR (SEM) - SUS tNR is derived from SUS (SEM) and not
the SUS PbR Mart.
Planning requirements
Are plans required and if so, at what frequency?
Yes. Provider plans, monthly 2018/19 via NHS Improvement Portal
12 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex C: Total elective spells (specific acute)
Definitions
Detailed descriptor:
Number of specific acute elective spells.
Lines within indicator (units):
Total number of specific acute day case and ordinary elective spells in the period.
Total elective spells (specific acute) is calculated directly from SUS using the
definition below.
Data definition
An elective admission is one that has been arranged in advance. It is not an
emergency admission, a maternity admission or a transfer from a hospital bed in
another healthcare provider. The period that the patient has to wait for admission
depends on the demand on hospital resources and the facilities available to meet
this demand.
A day case admission must be an elective admission, for which a ‘decision to admit’
has been made by someone with the ‘right of admission’. Any patient admitted
electively during the course of a day with the intention of receiving care, who does
not require the use of a hospital bed overnight and who returns home as scheduled,
should be counted as a day case. If this original intention is not fulfilled and the
patient stays overnight, such a patient should be counted as an ordinary admission.
Any patient admitted electively with the expectation that they will remain in hospital
for at least one night, including a patient admitted with this intention who leaves
hospital for any reason without staying overnight, should be counted as an ordinary
admission. A patient admitted electively with the intent of not staying overnight, but
who does not return home as scheduled, should also be counted as an ordinary
admission.
13 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
It is the number of specific acute day case and ordinary (as defined above) elective
spells relating to hospital provider spells for which:
• Treatment function = Specific Acute
Use criteria for either the Elective or Day case lines:
• Der_Management_Type is: ‘DC’ (Day case patients line)
• Der_Management_Type is: ‘EL’ (Ordinary elective patients line)
Monitoring
Monitoring frequency:
Monthly
Monitoring data source:
Secondary Uses Service tNR (SEM) - SUS tNR is derived from SUS (SEM) and not
the SUS PbR Mart.
Planning requirements
Are plans required and if so, at what frequency?
Yes. Provider plans, monthly 2018/19 via NHS Improvement Portal
14 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex D: Average number of G&A beds open per day (specific acute)
Definitions
Detailed descriptor:
Average number of G&A beds open per day (quarterly)
Lines within indicator (units):
Average number of general and acute beds open per day during the quarter
Data definition:
This plan is required to be submitted in line with the monthly NHS England KH03
publication on available beds,
This data line identifies the average number of bed days for each NHS healthcare
provider which are available for patients to have treatment or care. It must only
include beds in units managed by the provider, not beds commissioned from other
providers. Exclude from the bed days available totals any beds designated solely
for the use of well babies. Exclude from the bed days occupied totals any bed days
of occupation by well babies.
Monitoring
Monitoring frequency:
Quarterly
Monitoring data source:
KH03 Quarterly Bed Availability and Occupancy
15 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Planning requirements
Are plans required and if so, at what frequency?
Yes. Provider plans, monthly 2018/19 via NHS Improvement Portal
Further information
Further information on data available to support this metric can be found on the
beds availability and occupancy landing page:
www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-
occupancy/
16 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex E: Incomplete RTT pathways (specific acute)
Definitions
Detailed descriptor:
Number of incomplete RTT pathways by specified waiting time
Lines within indicator (units):
Number of incomplete RTT pathways <=18 weeks
Number of incomplete RTT pathways >18 weeks
Number of incomplete RTT pathways >52 weeks
Data definition:
Once a referral to treatment (RTT) waiting time clock has started it continues to tick
until:
• the patient starts first definitive treatment or
• clinical decision is made that stops the clock.
Trusts should ensure that all clock stops without treatment are made in the best
clinical interest of the patient and are not influenced by the impact on incomplete
pathway waiting time performance.
Patients should be allowed to choose their time of treatment taking account of
clinical advice where undue delay may present a risk to them.
Monitoring
Monitoring frequency:
Monthly
Monitoring data source:
NHS England consultant-led referral to treatment waiting times monthly published
report
17 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Planning requirements
Are plans required and if so, at what frequency?
Yes, Provider plans, monthly 2018/19 via NHS Improvement Portal
Further information
Further information on data available to support this metric can be found on the
referral to treatment indicators landing page:
www.england.nhs.uk/statistics/statistical-work-areas/rtt-waiting-
times/https://www.england.nhs.uk/statistics/statistical-work-areas/rtt-waiting-times/
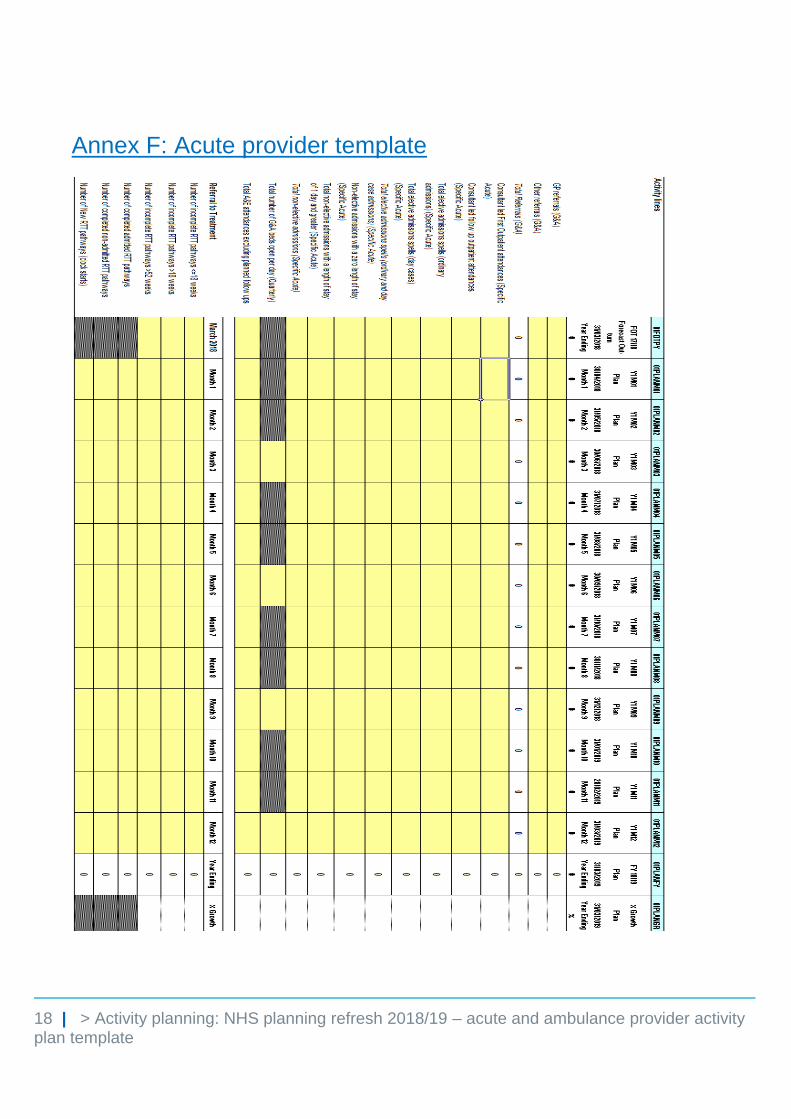
18 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex F: Acute provider template
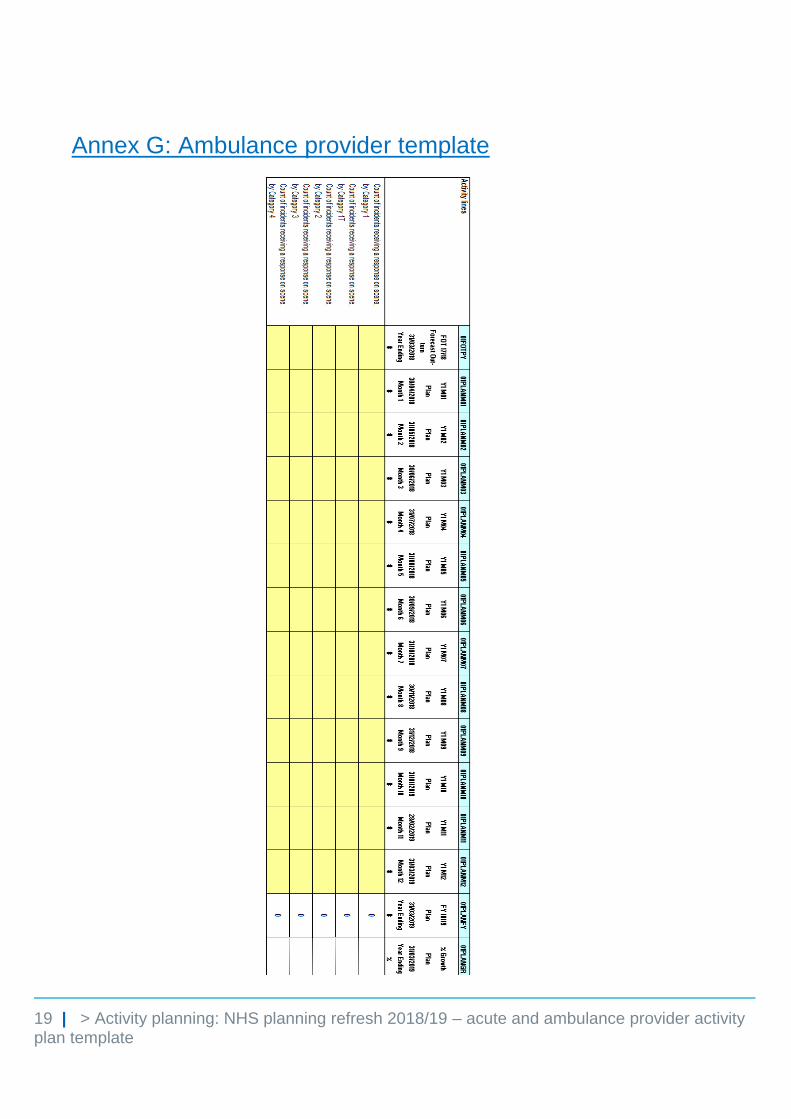
19 | > Activity planning: NHS planning refresh 2018/19 – acute and ambulance provider activity plan template
Annex G: Ambulance provider template
© NHS Improvement February 2018 Publication code: CG 40/18
Contact us:
NHS Improvement
Wellington House
133-155 Waterloo Road
London
SE1 8UG
0300 123 2257
improvement.nhs.uk
Follow us on Twitter @NHSImprovement
This publication can be made available in a number of other formats on request.