Embed Size (px)
Citation preview

Acute local inflammation after blunt trauma

The publication of this thesis was financially supported by:
Groningen University Institute for drug Exploration (GUIDE)Faculteit der Medische Wetenschappen RuGMathysDr. Ir. van de Laar StichtingStichting Ontwikkeling Klinische Immunologie
Cover: skin upper leg NamkjePicture page 5: St.Maartenszee, NL (picture made by Henk van der Laan)
Acute local inflammation after traumaNamkje van der LaanThesis University GroningenISBN 90-367-1515-6
Namkje van der LaanAll rights reserved
Printed by Ridderprint B.V., Ridderkerk

RIJKSUNIVERSITEIT GRONINGEN
Acute local inflammation after blunt trauma
Proefschrift
ter verkrijging van het doctoraat in deMedische Wetenschappen
aan de Rijksuniversiteit Groningenop gezag van de
Rector Magnificus, dr. D.F.J. Bosscher,in het openbaar te verdedigen op
woensdag 21 november 2001om 14.15 uur
door
Namkje van der Laan
geboren op 7 maart 1973te Groningen

Promotores: Prof. dr. H.J. ten DuisProf. dr. L.F.M.H de Leij
Beoordelingscommissie: Prof. dr. R.J.A. GorisProf. dr. R. van SchilfgaardeProf. dr. T.H. The

Ter nagedachtenis aan mijn lieve tante Nam
Voor Henk & Wil


Contents
Chapter I Introduction 9
Chapter II Tumor necrosis factor alpha (TNFα) in human skin: acomparison of different antibodies for immunohistochemistry 23
Chapter III Local cellular inflammation as a result of elective standardizedvascular surgery 41
Chapter IV Immunohistopathological appearance of three different typesof injury in human skin 59
Chapter V Is human skin activated by blunt trauma? 77
Chapter VI Production of pro-inflammatory cytokines by adipose tissueafter blunt trauma. 95
Chapter VII Discussion 111
Chapter VIII Summary 123
Chapter IX Samenvatting 127Dankwoord 133


Chapter I
Introduction

Chapter 1
10
Local inflammation
Injury induces a cascade of events which eventually leads to repair andhomeostasis. This repair or wound healing involves three phases. The first phase,inflammation is followed by tissue regeneration and tissue remodeling. Theinflammatory response is primarily intended to be a local response and providesprotection for the host. It is characterized by classical clinical features such asrubor (redness), tumor (swelling), calor (heat), dolor (pain) and functio laesa(loss of function).
In general, it is accepted that injury like tissue damage leads toinflammation. Tissue damage will lead to disruption of blood vessels, therebyactivating the coagulation cascade. Besides clot formation, coagulation inducesthe production of vasoactive, pro-inflammatory agents and activation of thecomplement cascade. In the damaged tissue, the fibrinolytic, and kinin-kallikreincascades are activated. Activation of the different cascade systems results ingeneration of bradykinin, the anaphylatoxins C3a and C5a and the expression ofpro-inflammatory cytokines such as tumor necrosis factor alpha (TNFα),interleukin-1 (IL1), interleukin-6 (IL6) and interleukin-8 (IL8). Production of thesemediators leads in turn to increased blood vessel permeability, local increasedblood flow, induction of the expression of adhesion molecules and recruitmentof cells into the site of inflammation. Of the various types of leukocytes thatappear in the injured area, neutrophils (granulocytes) are the first, followed bymonocytes and lymphocytes. Monocytes, macrophages produce cytokines andgrowth factors and play an important role in the transition from inflammation towound healing (1-4).
Systemic inflammation
Inflammation can be restricted to the site of tissue damage, but if theimpact is large enough, the local inflammatory response is accompanied to someextent by a systemic response. This response includes the induction of fever,increased synthesis of hormones, white blood cells and acute phase proteinssuch as C-reactive protein (CRP), serum amyloid A (SAA) and fibrinogen (5-7).
Acute versus chronic inflammation
Besides the discrimination between local and systemic inflammation,inflammation can be defined as acute and chronic inflammation. Acute andchronic inflammation can both consist of a local as well as a systemic response.Acute inflammation is, in contrast to chronic inflammation, self-limiting and willresolve. In general, inflammation is a strictly controlled system, but in some casessuch as major trauma or extensive tissue damage (burns, bacterial infection),

Introduction
11
persistent activation can result in chronic inflammation or an unregulatedinflammatory response.
Definitions
Unregulated systemic inflammation can be observed in multi-traumapatients, patients with severe burns and patients with otherwise devitalized tissues(bacterial infection). Depending on the cause and the clinical manifestation of theunderlying systemic inflammatory response, different definitions are used (8-10).
The systemic inflammatory response syndrome (SIRS) has been definedas a response characterized by two or more defined variables as described inTable 1. This response is not necessarily the result of an infection but can becaused by a variety of insults such as injuries, burns and pancreatitis (non-bacterial). If proven infection is the underlying cause of systemic inflammation,the response is defined as sepsis. SIRS and sepsis can, but do not necessarilylead to organ failure (MODS). The sequential organ failure of patients withMODS usually occurs after a lag period of days to weeks after the initial insult.MODS frequently starts with circulatory, respiratory or renal failure, with hepatic,intestinal or hematologic failure usually being later manifestations of the syndrome(11;12). Despite the fact that similar organs are involved in a certain sequence, thepathophysiology of the unregulated systemic response is largely unknown.
Table 1: Criteria for different systemic inflammatory responsesTerm Cause Definitions and variablesSIRS Trauma, burns,
hemorrhage,pancreatitis, other
Temperature >38°C, or <36°CHeart rate > 90 b/minRespiratory rate >20 b/min, or PaCO2 < 4,3 kPaWBC > 12000/mm3, or < 4000/mm3, or >10% bandforms
Sepsis Infection SIRS with a documented infectionSeveresepsis
Infection Sepsis and organ dysfunction, hypoperfusion orhypotension
MODS Consequence ofhost response
Sequential failure of one or more organ systems as aresult of a generalized persistent inflammatoryreaction
Generalized inflammation in SIRS/MODS
That patients with SIRS, sepsis and, or MODS have a generalized wholebody inflammation is indicated by the fact that the characteristic clinical featuresof inflammation are not only present in the involved areas, but are observed overthe whole body: generalized vasodilatation is evidenced by pink warm skin

Chapter 1
12
(rubor), fever (calor), generalized edema (tumor) and loss of function of one ormore remote organ systems (functio laesa).
The presence of a generalized whole body inflammation or systemicinflammatory response in these patients is underscored by elevated levels of pro-inflammatory mediators such as TNFα, IL1 and IL6. IL6 levels are foundelevated shortly after the accident and are a clear marker of injury: IL6 correlateswith the severity of injury and with outcome in multi-trauma patients (13-20).Also patients with burns or sepsis have high IL6 levels in the circulation (21-24).Results for TNFα and IL1 are less clear, conflicting results about their levels inthe circulation have been reported (15;25-27). This can be explained by the shortcirculation half life of these cytokines (respectively 20 and 6 minutes): TNFαbinds to its receptor and IL1 to the IL1 receptor antagonist (28). Elevated IL6levels are followed in general by an increase in procalcitonin, CRP, SAA,fibrinogen, and many other acute phase proteins (29-32).
Except for cytokines and acute phase proteins, increases in a wide varietyof inflammatory mediators have been reported, such as cytokine receptors(33;34), soluble adhesion molecules (35-37), nitric oxide (38;39), complementproducts (40;41), oxygen radicals and elastase (42). Although many dataconcerning circulating markers in relation to SIRS, sepsis and MODS have beenobtained, the underlying mechanisms leading to the production of thesemediators are largely unknown (43-45).
Hypotheses about origin of SIRS/MODS
To have the greatest chance to treat patients successfully and in order torecognize related signs and symptoms as early as possible, it is important tounderstand the underlying mechanisms leading to SIRS, sepsis and MODS. Thefact that organs that fail are not necessarily injured by the primary disease andthat there is a lag period between the initial cause and final onset of MODShampers the understanding and treatment of the syndrome.
Since MODS was generally observed in relation with infection (46-48), itwas thought that the clinical expression of a whole body inflammation was theresult of infection or the presence of significant levels of endotoxin in thecirculation. Although infection can induce SIRS, sepsis and MODS, it hasbecome clear that patients with MODS can but not necessarily are septic. Goriset al. (49-51), pointed out that in the majority of multi-trauma patients, MODSdevelops in the absence of infection.
Multiple hypotheses have been proposed about the events leading toMODS such as the “macrophage theory”, the “microcirculatory hypothesis”, the“gut hypothesis” and the “two hit theory”. Although these hypotheses offer anincomplete overview and they are partly overlapping, sometimes contradictoryand lack evidence, the mechanisms and systems proposed may be important in

Introduction
13
understanding MODS. Therefore the four above mentioned hypotheses areshortly described (11;12;52).
Macrophage theory
The macrophage theory is based on the assumption that as a result oftissue injury macrophages produce abundant amounts of cytokines such asTNFα, IL1, IL6 and other pro-inflammatory products which eventually lead tolocal and distant tissue injury. Local activation of macrophages as a result oftissue injury or infection is normally protective. However, when generalizedactivation of macrophages occurs, excessive amounts of pro-inflammatorymediators will be produced. As a result, a self-activation loop can be preservedthrough involvement of additional systems and cells, like the coagulation andcomplement system, fibroblasts and endothelial cells. Excessive amounts of pro-inflammatory mediators can be produced, reinforcing local injury. Furthermore,locally produced inflammatory mediators can ‘leak’ into the circulation, therebycontributing to systemic levels and distant organ injury. Support for the“macrophage theory” has its origin in the finding that pro-inflammatory cytokinesare present in multi-trauma and sepsis patients and that administration of TNFαor IL1 induces a response similar to SIRS or sepsis (53). The question remainswhat the exact and continuum trigger mechanism for the macrophage activationis.
Microcirculatory hypothesis
The microcirculatory hypothesis suggests that ischemia and reperfusioninjury play an important role in the development of MODS. It is known thatischemia or inadequate oxygen delivery can lead to organ damage, includingdamage of vascular endothelial cells, thereby inducing inflammation. Ischemia,followed by reperfusion injury, when circulation is restored, enhances celldamage, cell death and eventually organ dysfunction (54;55). Activatedendothelial cells can rapidly express adhesion molecules, produce cytokines andchemoattractants leading to leukocyte activation and adhesion (56). Theinteraction between activated endothelial cells and leukocytes is an important stepin maintaining the inflammatory state which can lead to excessive production ofpro-inflammatory mediators and cytokines. Tissue injury and organ damage isalso a secondary effect of toxic oxygen metabolites that are generated during thereperfusion period (57).This can finally lead to a self activation loop similar asdescribed for the macrophage theory leading to excessive production of pro-inflammatory mediators and possible distant organ injury.

Chapter 1
14
Gut hypothesis
In the gut hypothesis, bacteria and endotoxin derived from the gut initiateinflammation leading to MODS. Physiological stress such as trauma and shockmay cause failure of the gut mucosal barrier, with translocation of bacteria intomesenteric lymph nodes and systemic circulation. This bacterial and endotoxintranslocation can induce cytokine expression by monocytes, macrophages,activate endothelial cells and leukocytes, thereby activating a self-sustainingactivation loop resulting in the production of pro-inflammatory mediators.Bacterial translocation and the presence of endotoxin in the portal circulation hasbeen demonstrated in several animal models, although the clinical relevance of theintestinal barrier function in contributing to systemic inflammation in multi-traumapatients is controversial (58-64).
Two hit theory
The two hit theory proposes that MODS occurs as a result of two or moreinsults. The initial hit primes the immune system in such manner that a secondaryinsult amplifies the host’s response. In this way, an injury that is primarily not lifethreatening can indeed lead to a severe response and eventually MODS. Thismodel is a possible explanation for the fact that patients survive the first insult butdo not survive a subsequent infection. Mechanisms as described in the“macrophage theory”, the “microcirculatory hypothesis” and the “guthypothesis” may all be involved in the “two hit theory”.
Pathophysiology
Although the different theories regarding the pathophysiology of SIRS andMODS are still not sufficient to explain all underlying mechanisms, it is clear thatlocal inflammation plays an important role. Local inflammation in general isimportant in triggering the systemic response. From the described theories it canbe hypothesized that SIRS or MODS originate from an ongoing local activationin the damaged tissues. That indeed local inflammation in the damaged tissues isimportant in initiating the unregulated systemic response is supported byadditional findings. First, it has been reported that severity of the systemicreaction is related to the extent of the injuries, indicating that there is a connectionbetween the local and systemic response (20;65-67). Second, early fixation oflong bone fractures increases survival of multi-trauma patients. This can beexplained by the fact that early fixation leads to reduction of local tissue damage,thereby decreasing the ongoing local inflammatory response and risk for MODS(52;68-70). Third, cytokines are usually produced within tissues. They exert theireffects by direct cell-cell contact and are mainly locally biologically effective.

Introduction
15
Therefore the increased levels present in the circulation are probably derivedfrom locally produced cytokines in the tissues (71;72).
Altogether, this indicates that local inflammation and especially theproduction of pro-inflammatory cytokines is important in triggering a systemicresponse.
Pro-inflammatory cytokines
During local inflammation, production of pro-inflammatory cytokines isinitiated in the tissue.
As earlier described, cytokines are small regulatory proteins that functionmainly by paracrine and autocrine mechanisms. By binding to a cellular receptorthey can influence diverse biological activities such as cell activation, immunefunctions, proliferation, survival, production of other cytokines, etc. Cytokinescan be pleiotropic, redundant, synergistic and antagonistic, which makes thecytokine network a complex system.
In response to injury, pro-inflammatory cytokines such as TNFα, IL1, IL6and IL8 are thought to be important players.
TNFα is one of the earliest cytokines that is secreted during inflammation.It is mainly produced by monocytes / macrophages but there are many other celltypes that can secrete TNFα (neutrophils, mast cells, keratinocytes, endothelialcells, adipocytes). Effects of TNFα include activation of coagulation, inductionof the expression of adhesion molecules, prostaglandins and other cytokines.
IL1 is also released in the early phase of inflammation, acts together withTNFα and is also mainly produced by monocytes, macrophages and endothelialcells. TNFα and IL1 can both induce IL6 and IL8 production.
IL6 is produced by many cell types such as monocytes, macrophages,endothelial cells, adipocytes, fibroblasts and mast cells. IL6 is considered to be apro-inflammatory cytokine, but it is recently described to have anti-inflammatoryproperties as well. Pro-inflammatory properties include the induction of theproduction of acute phase proteins, fever, adhesion molecules and promotingcell differentiation. It may exert its anti-inflammatory properties by attenuatingTNFα and IL1 activity by induction of the release of soluble TNF-receptor andIL1-receptor antagonist.
IL8 is a potent neutrophil chemoattractant and activator. It is produced inresponse to TNFα and IL1 and is secreted by monocytes, macrophages, mastcells, epithelial cells and fibroblasts among other cell types (25;28;73-77).

Chapter 1
16
Outline of this thesis
To understand what induces the systemic inflammatory response that canlead to MODS, it is important to know where this response originates from.Based on the above described hypotheses and the important role for cytokines inthe onset of inflammation, we hypothesize that local inflammation and especiallycytokine production in tissues being part of the initial damaged areas initiate thesystemic inflammatory response. Therefore, we studied whether soft tissuessurrounding a fracture may be activated and produce cytokines to contribute toan unregulated systemic response.
As a model, trauma patients with a femoral fracture were studied. Theclosed femoral fracture served as a “standardized” mechanical injury. Femoralfractures are normally treated by direct closed reduction and (intramedullary nail)osteosynthesis. This treatment offers the possibility to study early localinflammation (within 12 hours post-injury) in tissues at the site of the fracture andcompare it with tissues taken from a non-injured area in the same patient. Tissueconsidered to be activated was taken near the femoral fracture, in the regionwhere the femoral nail was locked (Figure 1, A) and compared with controltissue, taken at the introduction place of the for stabilization used intramedullarynail (Figure 1, B).
Figure 1. Skin considered to be activated (A) was taken near the site of the femoral fracture, wherethe femoral nail is locked. The remote skin biopsy (B) was taken at the place where the femoral nailis introduced.

Introduction
17
First, different anti-TNFα antibodies were tested in Chapter 2, to obtain avalid method for the detection of cytokines and especially TNFα locally inhuman skin. Then, local inflammation in human skin as a result of injury wasstudied in detail. Not only the local pro-inflammatory response after a closedfemoral fracture, but also other types of local inflammation in human skin werestudied. The effects of disruption of the epithelial barrier by simple incision ofthe skin (Chapter 3) and of bacterial infection due to a penetrating injury of theskin were studied and compared with possible inflammation in human skin after aclosed femoral fracture (Chapter 4). Possible skin activation and cytokineproduction as a result of a closed femoral fracture was studied and describedextensively in Chapter 5. In addition, local inflammation and especially cytokineproduction was studied in muscle and adipose tissue, tissues more closer to thefractured bone (Chapter 6). In Chapter 7, in a general overview, localinflammation as a result of injury in general and specifically as a result of blunttrauma is discussed. Finally, Chapter 8, gives a summary of this thesis.

Chapter 1
18
References
1. Ross, R. Inflammation, cell proliferation, and connective tissue formation in wound repair. Hunt,T. K. Wound healing and wound infection: theory and surgical practice.1980. pp.1-8.
2. Kuby, J. Cytokines. Immunology. Second ed.W.H. Freeman and Company, New York; 1994.
3. Witte, M. B. and Barbul, A. General Principles of Wound Healing. Surg.Clin.North Am.1997;77(3):509-28.
4. Singer, A. J. and Clark, R. A. Cutaneous Wound Healing. N.Engl.J.Med. 2-9-1999;341(10):738-46.
5. Kushner, I. and Rzewnicki, D. L. The Acute Phase Response: General Aspects. BaillieresClin.Rheumatol. 1994;8(3):513-30.
6. Baumann, H. and Gauldie, J. The Acute Phase Response. Immunol.Today 1994;15(2):74-80.
7. Gabay, C. and Kushner, I. Acute-Phase Proteins and Other Systemic Responses toInflammation. N.Engl.J.Med. 11-2-1999;340(6):448-54.
8. Beal, A. L. and Cerra, F. B. Multiple Organ Failure Syndrome in the 1990s. SystemicInflammatory Response and Organ Dysfunction. JAMA 19-1-1994;271(3):226-33.
9. Davies, M. G. and Hagen, P. O. Systemic Inflammatory Response Syndrome. Br.J.Surg.1997;84(7):920-35.
10. Brun-Buisson, C. The Epidemiology of the Systemic Inflammatory Response. Intensive CareMed. 2000;26 Suppl 1:S64-S74.
11. Deitch, E. A. Multiple Organ Failure. Pathophysiology and Potential Future Therapy. Ann.Surg.1992;216(2):117-34.
12. Deitch, E. A. and Goodman, E. R. Prevention of Multiple Organ Failure. Surg.Clin.North Am.1999;79(6):1471-88.
13. Pullicino, E. A., Carli, F., Poole, S., Rafferty, B., Malik, S. T., and Elia, M. The RelationshipBetween the Circulating Concentrations of Interleukin 6 (IL-6), Tumor Necrosis Factor (TNF)and the Acute Phase Response to Elective Surgery and Accidental Injury. Lymphokine Res.1990;9(2):231-8.
14. Ayala, A., Wang, P., Ba, Z. F., Perrin, M. M., Ertel, W., and Chaudry, I. H. DifferentialAlterations in Plasma IL-6 and TNF Levels After Trauma and Hemorrhage. Am.J.Physiol1991;260(1 Pt 2):R167-R171.
15. Hoch, R. C., Rodriguez, R., Manning, T., Bishop, M., Mead, P., Shoemaker, W. C., andAbraham, E. Effects of Accidental Trauma on Cytokine and Endotoxin Production. Crit.CareMed. 1993;21(6):839-45.
16. Meade, P., Shoemaker, W. C., Donnelly, T. J., Abraham, E., Jagels, M. A., Cryer, H. G., Hugli,T. E., Bishop, M. H., and Wo, C. C. Temporal Patterns of Hemodynamics, Oxygen Transport,Cytokine Activity, and Complement Activity in the Development of Adult Respiratory DistressSyndrome After Severe Injury. J.Trauma. 1994;36(5):651-7.

Introduction
19
17. Svoboda, P., Kantorova, I., and Ochmann, J. Dynamics of Interleukin 1, 2, and 6 and TumorNecrosis Factor Alpha in Multiple Trauma Patients. J.Trauma. 1994;36(3):336-40.
18. Biffl, W. L., Moore, E. E., Moore, F. A., and Peterson, V. M. Interleukin-6 in the InjuredPatient. Marker of Injury or Mediator of Inflammation? Ann.Surg. 1996;224(5):647-64.
19. Nast, Kolb D., Waydhas, C., Gippner, Steppert C., Schneider, I., Trupka, A., Ruchholtz, S., Zettl,R., Schweiberer, L., and Jochum, M. Indicators of the Posttraumatic Inflammatory ResponseCorrelate With Organ Failure in Patients With Multiple Injuries. J.Trauma. 1997;42(3):446-54.
20. Gebhard, F., Pfetsch, H., Steinbach, G., Strecker, W., Kinzl, L., and Bruckner, U. B. IsInterleukin 6 an Early Marker of Injury Severity Following Major Trauma in Humans?Arch.Surg. 2000;135(3):291-5.
21. Nijsten, M. W., de-Groot, E. R., ten-Duis, H. J., Klasen, H. J., Hack, C. E., and Aarden, L. A.Serum Levels of Interleukin-6 and Acute Phase Responses. Lancet 17-10-1987;2(8564):921.
22. Damas, P., Canivet, J. L., de-Groote, D., Vrindts, Y., Albert, A., Franchimont, P., and Lamy, M.Sepsis and Serum Cytokine Concentrations. Crit.Care Med. 1997;25(3):405-12.
23. Kowal, Vern A., Sharp, Pucci MM, Walenga, J. M., Dries, D. J., and Gamelli, R. L. Trauma andThermal Injury: Comparison of Hemostatic and Cytokine Changes in the Acute Phase of Injury.J.Trauma. 1998;44(2):325-9.
24. Martin, C., Boisson, C., Haccoun, M., Thomachot, L., and Mege, J. L. Patterns of CytokineEvolution (Tumor Necrosis Factor-Alpha and Interleukin-6) After Septic Shock, HemorrhagicShock, and Severe Trauma. Crit Care Med. 1997;25(11):1813-9.
25. Bellomo, R. The Cytokine Network in the Critically Ill. Anaesth.Intensive Care 1992;20(3):288-302.
26. Rabinovici, R., John, R., Esser, K. M., Vernick, J., and Feuerstein, G. Serum Tumor NecrosisFactor-Alpha Profile in Trauma Patients. J.Trauma. 1993;35(5):698-702.
27. Keel, M., Ecknauer, E., Stocker, R., Ungethum, U., Steckholzer, U., Kenney, J., Gallati, H.,Trentz, O., and Ertel, W. Different Pattern of Local and Systemic Release of Proinflammatoryand Anti-Inflammatory Mediators in Severely Injured Patients With Chest Trauma. J.Trauma.1996;40(6):907-12.
28. Lin, E., Calvano, S. E., and Lowry, S. F. Inflammatory Cytokines and Cell Response in Surgery.Surgery 2000;127(2):117-26.
29. Gosling, P. and Dickson, G. R. Serum C-Reactive Protein in Patients With Serious Trauma.Injury 1992;23(7):483-6.
30. Ensenauer, R., Puttmann, M., Quintel, M., Kattermann, R., and Aufenanger, J. Comparison ofSerum Phospholipase A2, Polymorphonuclear Granulocyte Elastase, C-Reactive Protein andSerum Amyloid A With the APACHE II Score in the Prognosis of Multiple Injured Patients.Clin.Investig. 1994;72(11):843-9.
31. Petersen, S. R., Jeevanandam, M., Shahbazian, L. M., and Holaday, N. J. Reprioritization ofLiver Protein Synthesis Resulting From Recombinant Human Growth Hormone Supplementation

Chapter 1
20
in Parenterally Fed Trauma Patients: the Effect of Growth Hormone on the Acute-PhaseResponse. J.Trauma 1997;42(6):987-95.
32. Mimoz, O., Benoist, J. F., Edouard, A. R., Assicot, M., Bohuon, C., and Samii, K. Procalcitoninand C-Reactive Protein During the Early Posttraumatic Systemic Inflammatory ResponseSyndrome. Intensive.Care Med. 1998;24(2):185-8.
33. Tan, L. R., Waxman, K., Scannell, G., Ioli, G., and Granger, G. A. Trauma Causes Early Releaseof Soluble Receptors for Tumor Necrosis Factor. J.Trauma 1993;34(5):634-8.
34. Cinat, M., Waxman, K., Vaziri, N. D., Daughters, K., Yousefi, S., Scannell, G., and Tominaga,G. T. Soluble Cytokine Receptors and Receptor Antagonists Are Sequentially Released AfterTrauma. J.Trauma 1995;39(1):112-8.
35. Law, M. M., Cryer, H. G., and Abraham, E. Elevated Levels of Soluble ICAM-1 Correlate Withthe Development of Multiple Organ Failure in Severely Injured Trauma Patients. J.Trauma.1994;37(1):100-9.
36. Simons, R. K., Hoyt, D. B., Winchell, R. J., Rose, R. M., and Holbrook, T. Elevated SelectinLevels After Severe Trauma: a Marker for Sepsis and Organ Failure and a Potential Target forImmunomodulatory Therapy. J.Trauma 1996;41(4):653-62.
37. Schinkel, C., Faist, E., Zimmer, S., Piltz, S., Walz, A., Rose, R., Hocherl, E., Herndon, D., andSchildberg, F. W. Kinetics of Circulating Adhesion Molecules and Chemokines After MechanicalTrauma and Burns. Eur.J.Surg. 1996;162(10):763-8.
38. Ochoa, J. B., Udekwu, A. O., Billiar, T. R., Curran, R. D., Cerra, F. B., Simmons, R. L., andPeitzman, A. B. Nitrogen Oxide Levels in Patients After Trauma and During Sepsis. Ann.Surg.1991;214(5):621-6.
39. Nussler, A. K. and Billiar, T. R. Inflammation, Immunoregulation, and Inducible Nitric OxideSynthase. J.Leukoc.Biol. 1993;54(2):171-8.
40. Kapur, M. M., Jain, P., and Gidh, M. The Effect of Trauma on Serum C3 Activation and ItsCorrelation With Injury Severity Score in Man. J.Trauma 1986;26(5):464-6.
41. Gallinaro, R., Cheadle, W. G., Applegate, K., and Polk, H. C., Jr. The Role of the ComplementSystem in Trauma and Infection. Surg.Gynecol.Obstet. 1992;174(5):435-40.
42. Yao, Y. M., Redl, H., Bahrami, S., and Schlag, G. The Inflammatory Basis of Trauma/Shock-Associated Multiple Organ Failure. Inflamm.Res. 1998;47(5):201-10.
43. Schlag, G. and Redl, H. Mediators of Injury and Inflammation. World J.Surg. 1996;20(4):406-10.
44. Baue, A. E. Multiple Organ Failure, Multiple Organ Dysfunction Syndrome, and SystemicInflammatory Response Syndrome. Why No Magic Bullets? Arch.Surg. 1997;132(7):703-7.
45. Kim, P. K. and Deutschman, C. S. Inflammatory Responses and Mediators. Surg.Clin.NorthAm. 2000;80(3):885-94.
46. Polk, H. C., Jr. and Shields, C. L. Remote Organ Failure: a Valid Sign of Occult Intra-AbdominalInfection. Surgery 1977;81(3):310-3.

Introduction
21
47. Fry, D. E., Pearlstein, L., Fulton, R. L., and Polk, H. C., Jr. Multiple System Organ Failure. TheRole of Uncontrolled Infection. Arch.Surg. 1980;115(2):136-40.
48. Bell, R. C., Coalson, J. J., Smith, J. D., and Johanson, W. G., Jr. Multiple Organ System Failureand Infection in Adult Respiratory Distress Syndrome. Ann.Intern.Med. 1983;99(3):293-8.
49. Goris, R. J., te-Boekhorst, T. P., Nuytinck, J. K., and Gimbrere, J. S. Multiple-Organ Failure.Generalized Autodestructive Inflammation? Arch.Surg. 1985;120(10):1109-15.
50. Goris, R. J., Boekholtz, W. K., van Bebber, I. P., Nuytinck, J. K., and Schillings, P. H. Multiple-Organ Failure and Sepsis Without Bacteria. An Experimental Model. Arch.Surg.1986;121(8):897-901.
51. Goris, R. J. Mediators of Multiple Organ Failure. Intensive Care Med. 1990;16 Suppl 3:S192-S196.
52. Livingston, D. H. and Deitch, E. A. Multiple Organ Failure: a Common Problem in SurgicalIntensive Care Unit Patients. Ann.Med. 1995;27(1):13-20.
53. Michie, H. R., Spriggs, D. R., Manogue, K. R., Sherman, M. L., Revhaug, A., O'Dwyer, S. T.,Arthur, K., Dinarello, C. A., Cerami, A., Wolff, S. M., and . Tumor Necrosis Factor andEndotoxin Induce Similar Metabolic Responses in Human Beings. Surgery 1988;104(2):280-6.
54. Seekamp, A., Till, G. O., Mulligan, M. S., Paulson, J. C., Anderson, D. C., Miyasaka, M., andWard, P. A. Role of Selectins in Local and Remote Tissue Injury Following Ischemia andReperfusion. Am.J.Pathol. 1994;144(3):592-8.
55. Verrier, E. The Microvascular Cell and Ischemia-Reperfusion Injury. J.Cardiovasc.Pharmacol.1996;27 Suppl 1:S26-S30.
56. Osborn, L. Leukocyte Adhesion to Endothelium in Inflammation. Cell 13-7-1990;62(1):3-6.
57. Inauen, W., Granger, D. N., Meininger, C. J., Schelling, M. E., Granger, H. J., and Kvietys, P. R.Anoxia-Reoxygenation-Induced, Neutrophil-Mediated Endothelial Cell Injury: Role of Elastase.Am.J.Physiol 1990;259(3 Pt 2):H925-H931.
58. Baker, J. W., Deitch, E. A., Li, M., Berg, R. D., and Specian, R. D. Hemorrhagic Shock InducesBacterial Translocation From the Gut. J.Trauma 1988;28(7):896-906.
59. Rush-BF, Jr, Redan, J. A., Flanagan-JJ, Jr, Heneghan, J. B., Hsieh, J., Murphy, T. F., Smith, S.,and Machiedo, G. W. Does the Bacteremia Observed in Hemorrhagic Shock Have ClinicalSignificance? A Study in Germ-Free Animals. Ann.Surg. 1989;210(3):342-5.
60. Moore, F. A., Moore, E. E., Poggetti, R., McAnena, O. J., Peterson, V. M., Abernathy, C. M.,and Parsons, P. E. Gut Bacterial Translocation Via the Portal Vein: a Clinical Perspective WithMajor Torso Trauma. J.Trauma 1991;31(5):629-36.
61. Peitzman, A. B., Udekwu, A. O., Ochoa, J., and Smith, S. Bacterial Translocation in TraumaPatients. J.Trauma 1991;31(8):1083-6.
62. Yao, Y. M., Bahrami, S., Leichtfried, G., Redl, H., and Schlag, G. Pathogenesis of Hemorrhage-Induced Bacteria/Endotoxin Translocation in Rats. Effects of RecombinantBactericidal/Permeability-Increasing Protein. Ann.Surg. 1995;221(4):398-405.

Chapter 1
22
63. Faries, P. L., Simon, R. J., Martella, A. T., Lee, M. J., and Machiedo, G. W. IntestinalPermeability Correlates With Severity of Injury in Trauma Patients. J.Trauma. 1998;44(6):1031-5.
64. Ramsay, G. and van-Saene, R. H. Selective Gut Decontamination in Intensive Care and SurgicalPractice: Where Are We? World J.Surg. 1998;22(2):164-70.
65. Bitterman, H., Kinarty, A., Lazarovich, H., and Lahat, N. Acute Release of Cytokines IsProportional to Tissue Injury Induced by Surgical Trauma and Shock in Rats. J.Clin.Immunol.1991;11(4):184-92.
66. Baigrie, R. J., Lamont, P. M., Kwiatkowski, D., Dallman, M. J., and Morris, P. J. SystemicCytokine Response After Major Surgery. Br.J.Surg. 1992;79(8):757-60.
67. Moore, F. A. and Moore, E. E. Evolving Concepts in the Pathogenesis of Postinjury MultipleOrgan Failure. Surg.Clin.North Am. 1995;75(2):257-77.
68. Bone, L. B., Johnson, K. D., Weigelt, J., and Scheinberg, R. Early Versus Delayed Stabilizationof Femoral Fractures. A Prospective Randomized Study. J.Bone Joint Surg.Am. 1989;71(3):336-40.
69. Pape, H. C., Auf'm'Kolk, M., Paffrath, T., Regel, G., Sturm, J. A., and Tscherne, H. PrimaryIntramedullary Femur Fixation in Multiple Trauma Patients With Associated Lung Contusion--aCause of Posttraumatic ARDS? J.Trauma 1993;34(4):540-7.
70. Livingston, D. H. Management of the Surgical Patient With Multiple System Organ Failure.Am.J.Surg. 1993;165(2A Suppl):8S-13S.
71. Deitch, E. A. Cytokines Yes, Cytokines No, Cytokines Maybe? Crit.Care Med. 1993;21(6):817-9.
72. Bone, R. C. Toward a Theory Regarding the Pathogenesis of the Systemic InflammatoryResponse Syndrome: What We Do and Do Not Know About Cytokine Regulation. Crit.CareMed. 1996;24(1):163-72.
73. Akira, S., Hirano, T., Taga, T., and Kishimoto, T. Biology of Multifunctional Cytokines: IL 6 andRelated Molecules (IL 1 and TNF). FASEB J. 1990;4(11):2860-7.
74. Mannel, D., Murray, C., Risau, W., and Clauss, M. Tumor Necrosis: Factors and Principles.Immunol.Today 1996;17(6):254-6.
75. Barton, B. E. IL-6: Insights into Novel Biological Activities. Clin.Immunol.Immunopathol.1997;85(1):16-20.
76. The Cytokine Handbook. Third ed.Academic Press; 1998. Thomson, A. W.
77. Dinarello, C. A. Proinflammatory Cytokines. Chest 2000;118(2):503-8.

Chapter II
Tumor necrosis factor alpha (TNFα) in human skin: a comparison ofdifferent antibodies for immunohistochemistry
Namkje van der Laan 1
Lou de Leij PhD 2
Wim Buurman PhD 3
Wim Timens PhD 2
Henk Jan ten Duis MD, PhD 1
1 Department of SurgeryUniversity Hospital GroningenThe Netherlands
2 Department of Pathology Laboratory medicine, section Medical BiologyUniversity Hospital GroningenThe Netherlands
3 Department of SurgeryUniversity Hospital MaastrichtThe Netherlands
Archives of Dermatological Research (2001) 293:226-232

Chapter 2
24
Summary
Conflicting results have been reported regarding the localization andpresence of TNFα in normal human skin. To study TNFα expression, we havetested a panel of antibodies directed against human TNFα. First, antibodies weretested for immunoreactivity on cytospots of isolated, LPS stimulated peripheralblood mononuclear cells. Second, antibodies were tested to detect recombinantTNFα on Western blot. Some antibodies were found to be unable to detectrecombinant TNFα on blot. Most antibodies were able however to bind TNFαprotein, whereas they did not bind to other irrelevant proteins that were alsopresent on blot. Finally, antibodies were tested on cryosections of normal humanskin. Antibodies that not reacted with TNFα on blot were incubated with TNFαbefore the staining procedure to see whether these antibodies specifically bindTNFα.
We found that although the antibodies all bind TNFα clear differences instaining patterns are observed. This indicates that these antibodies may recognizedistinct epitopes or different forms of TNFα. Differences found here, but alsothose reported in literature can be the result of the concentration of the antibodyused, the staining procedure or specificity of the antibody itself. So, forunambiguous interpretation of data, it is important to know the characterization ofthe antibodies used.

TNFα in human skin
25
Introduction
Many in vitro experiments have been performed to investigate theproperties of different cells of the skin immune system (SIS), especiallyconcerning their ability to produce cytokines (1). Epidermal keratinocytes havebeen shown to be able to produce a number of cytokines such as interleukin 1, 6and tumor necrosis factor alpha (TNFα) when cultured in the presence of avariety of stimuli. Also other cells of the SIS are able to produce cytokines asshown in in vitro experiments (2-4). About cytokine production of cells of theskin in in vivo situations, much remains unclear. It would be of interest to knowwhich cells produce cytokines such as TNFα under different conditions, sincethis could give information on the role of TNFα in physiological circumstancesand during inflammatory or systemic disease processes. For detection of TNFαmRNA in human skin, in situ hybridization or RT-PCR experiments can beperformed. The data from such experiments does not, however, give informationabout the presence of TNFα at the protein level. Protein can be detected usingWestern blotting, but this technique has the disadvantage that localization of theprotein is unknown. Therefore immunohistochemistry is a useful technique tolocalize cells that contain TNFα protein. Several studies concerning the presenceof TNFα in human skin cryostat sections have been published. These studieshave shown conflicting results regarding the presence and localization of TNFα.Oxholm et al.(5) were the first to detect TNFα in cryosections of normal humanskin. They showed that TNFα staining was localized in cells found in the upperlayers of the epidermis, stratum granulosum, stratum spinosum and stratumcorneum. No staining was observed in the basal cell layer of the epidermis, thestratum basale. In the dermis, only hair follicles were found positive for TNFα.This same pattern has been described by different authors (5-11). In contrast,others have described positive staining only in the basal cell layer (12-14),whereas others reported the absence of TNFα staining of epidermal cells ofnormal human skin (15-20).
Positive staining in the dermal compartment is described for different cells,eccrine sweat ducts, hair follicles and sebaceous glands. To study the role ofTNFα in skin under different pathological conditions (psoriasis, lepra, UVBradiation, trauma), the presence of the cytokine TNFα in the normal ‘resting’state should be well defined. To this end, we determined the specificity andstaining pattern of a panel of different TNFα antibodies in human skin.

Chapter 2
26
Materials and methods
Antibodies
The anti-TNFα antibodies used in this study are summarized in Table 1.Antibodies MR1-2 and MR2-1 (Hbt, Uden, the Netherlands) were used to detectrespectively TNFα receptor I (p55) and II (p75). Both antibodies were used at aconcentration of 25 µg/ml.
Table 1: Anti-TNFα antibodies used in this studyAntibody, clone Subclass Source10F Mouse IgG1 Dr. W. Buurman4H31 Mouse IgG1 Dr. W. Buurman, Hbt, Uden, The Netherlands52B83 Mouse IgG1 Dr. W. Buurman, Hbt, Uden, The Netherlands61E71 Mouse IgG1 Dr. W. Buurman, Hbt, Uden, The NetherlandsD9D10 Mouse IgG1 Eurogenetics, E. Bosman, Tessenderlo, Belgium35G10F3 Mouse IgG1 Genzyme Diagnostics, Abingdon, UKIP-300 Rabbit
polyclonalGenzyme Diagnostics, Abingdon, UK
199 Mouse IgG1 Boehringer Mannheim, Roche, Almere,The Netherlands
J1D9 Mouse IgG1 Ancell, Kordia, Leiden, The Netherlands28401.111 Mouse IgG1 R&D systems, Abingdon, UK
Western blotting
Recombinant TNFα (Boehringer Ingelheim, Germany) diluted indenaturation buffer and mixed with a crude cell extract (21) as a source ofirrelevant proteins, was used to determine the specificity of the antibodies.Samples were heated for 5 minutes at 57°C and loaded on a 15% SDS-polyacrylamide gel. After electrophoresis, the proteins were transferred ontonitrocellulose membranes (Schleicher & Schuell, Keene, NH) using semi-dry blotsystem. After blocking with 4% skimmed milk powder in 0.01 M phosphatebuffered saline (PBS), antibodies were tested at different concentrations in PBScontaining 1% skimmed milk powder and 0.1% Tween-20 (Sigma Chemicals, St.Louis, MO). Different concentrations of the antibodies were tested, ranging from0.125-2 µg/ml. Antibodies were detected with rabbit anti-mouse peroxidase(RαM-PO, P260, Dako, Glostrup, Denmark) diluted 1:5000 in PBS containing1% skimmed milk powder and 0.1% Tween-20 with 5% normal human serum toprevent non specific binding of the conjugate. Antibody IP-300 was detectedwith swine anti-rabbit peroxidase, 1:10.000 (SαR-PO, P217, Dako). Bound

TNFα in human skin
27
antibody was visualized using para-hydroxy-coumaric acid (Sigma) as enhancerand sodium-luminol (Sigma) 1.25 mM in 0.1M Tris-HCl, pH 8.6, as a substrate.Rainbow colored protein molecular weight marker (RPN 756, Amersham,Buckinghamshire, UK) with a molecular weight range of 14300-220000 was usedas a reference.
Preparation of LPS stimulated cells
For use in immunohistochemical staining, peripheral blood mononuclearcells (PBMC) were isolated from heparinized peripheral human blood. Blood wasdiluted with PBS (1:1) and cells were isolated by density centrifugation onlymphoprep (Nycomed, Oslo, Norway) at 2400 rpm for 20 minutes. The PBMCfraction was washed twice in RPMI-1640 (Gibco, Grand Island, N.Y.). Cellswere stimulated with 1 µg/ml LPS (L9143, Sigma) in complete medium, RPMI-1640 supplemented with 2 mM glutamine and 15% normal human serum, for 3hours at 37°C, 5% CO2 in humidified atmosphere. After stimulation, the cellswere washed with phosphate buffered saline (PBS) and 100 µl of the cellsuspension was centrifuged (5 min, 500 rpm) on glass slides using acytocentrifuge apparatus (Shandon, Runcorn, Cheshire, UK). Also nonstimulated cells, incubated for 3 hours in complete medium without LPS werecentrifuged on glass slides. The cytospots were air dried for at least 30 minutes,fixed with acetone for 10 minutes and stored at -20°C until use.
Skin biopsies
Normal skin was obtained from healthy patients undergoing electivesurgery. Informed consent was given and this study was approved by the localethics committee. Biopsies taken at first incision were immediately snap frozen inliquid nitrogen. Skin was obtained from different parts of the body (Table 2). Allbiopsies were immediately snap frozen in liquid nitrogen and stored at -80°C untiluse.

Chapter 2
28
Table 2: Description of patients skin biopsiesPlace of the body Age SexThigh 15 FemaleHip 22 MaleJust below knee 40 MaleUpperleg 48 FemaleHip 55 Male
Immunostaining of cytospins and sections
For immunohistochemistry, 6 µm sections of human skin were cut, airdried and fixed for 10 minutes with acetone.
Single step detection
This protocol was used for detection of TNFα on cytospots with alltested antibodies and for antibodies (4H31, 52B83, 35G10F3 and IP-300) thatcould be used at relatively low concentrations on human skin cryosections(respectively 2, 5, 2 µg/ml and 1:100) . First, sections were incubated for onehour with the different TNFα antibodies diluted in PBS. After washing with PBSfor 5 minutes, slides were incubated for 30 minutes with RαM-PO or SαR-PO(DAKO) for IP-300 at a respectively 1: 40 and 1:50 dilution in PBS supplementedwith 1% normal human serum. After washing with PBS, peroxidase reactivitywas visualized using amino-ethylcarbazole (AEC, Sigma) as a substrate. Slideswere counterstained with hematoxylin and mounted in Kaiser’s glycerin.
ABC
This protocol was used for antibodies (10F, 61E71, D9D10, 199, J1D9and 28401.111) that were used at a concentration of 10 or 25 µg/ml on humanskin cryosections. Sections were incubated for one hour with the different TNFαantibodies diluted in PBS. After washing with PBS for 5 minutes, slides wereincubated for 30 minutes with biotinylated goat anti-mouse conjugate (GαM-Ig(H+L)-bio, Southern Biotechnology Associates, Birmingham, Ala.) at a 1:200dilution in PBS supplemented with 1% normal human serum, washed with PBSand subsequently incubated for 30 minutes with streptavidine ABComplex (ABC,Dako). Streptavidine and biotinylated horseradishperoxidase were diluted 1:100in PBS. After washing with PBS, peroxidase reactivity was visualized usingamino-ethylcarbazole (AEC, Sigma) as a substrate. Slides were counterstainedwith hematoxylin and mounted in Kaiser’s glycerin.

TNFα in human skin
29
Immunofluorescence double staining
Antibodies IP-300 and 35G10F3 were used together with antibodiesagainst monocyte / macrophages (CD14 1:40, CD68 1:40, Dako) or endothelialcells (CD31 1:100, vWillebrand factor 1:200, Dako). Sections were incubated forone hour with a mixture of anti-TNFα and a cell specific antibody. After washingwith PBS for 5 minutes, slides were incubated for 30 minutes with a mixture of aFITC and TRITC labeled conjugate (GαM-IgG1-FITC, GαM-IgG2b-FITC,GαM-IgG1-TRITC, Southern Biotechnology Associates or SαR-FITC, SαR-TRITC, Dako) in PBS supplemented with 1% normal human serum. Afterwashing with PBS, sections were incubated for 15 minutes with DAPI(Boehringer Mannheim, 1:200.000) to stain nuclei. Sections were mounted incitifluor and analyzed for double positive cells.
Pre incubation of TNFα antibodies with recombinant TNFα
Three antibodies that were not reactive on Western blot (4H31, D9D10 and61E71) and three antibodies (4H31, 35G10F3 and IP-300) with a distinctivestaining pattern were tested for their TNFα specificity. Before the stainingprocedure, antibody was mixed with an excess (10x, 5x and equal amounts) ofrecombinant TNFα (Boehringer Ingelheim). This mixture was incubated for onehour at room temperature to allow binding of the antibody to TNFα. Then, themixture was applied to the section, for one hour, as antibody incubation.Furthermore, detection of TNFα expression was performed as described above.

Chapter 2
30
Results
Distribution of TNFα in stimulated cells
All selected antibodies stained LPS stimulated peripheral bloodmononuclear cells, whereas they were all negative when applied to unstimulatedcells. The concentrations of the antibodies used, to optimally detect TNFα instimulated cells, differed substantially between the antibodies: 10F, 4H31,35G10F3 and 28401.111 stained faintly positive at a concentration of 1 µg/ml,whereas 52B83, 61E71, 199, J1D9 stained at a concentration of 2 µg/ml andD9D10 needed 10 µg/ml. The concentration of IP-300 was not known and wasused at a dilution of 1:100. With the use of polyclonal antibody IP-300 differentcell types were found to be positive.
Specificity on Western blot
All antibodies were tested for specificity by their ability to detect recombinantTNFα added to a mixture of irrelevant human proteins (crude granulocyteextract) separated by SDS PAGE and analyzed by Western blotting. A maximumconcentration of 20 ng of recombinant TNFα was added, to be detected by theantibodies at a concentration of maximal 2 µg/ml. Several antibodies (4H31,61E71, D9D10 and 199) did not react with any protein present on Western blotunder these conditions. The other antibodies were able to detect TNFα on blot,as indicated by a positive staining of the added recombinant TNFα i.e. as a bandwith an apparent Mw of 17 kD. Three of these antibodies: 52B83, J1D9 and28401.111 show one specific band on Western blot at 17 kD (Fig.1).
Figure 1. Detection of TNFα protein on Western blotting using enhanced chemoluminescence.Lane 1+2, 5+6, 11+12, 13+14, 17+18, 19+20: 2.5 and 5 ng TNFα detected with 1 µg/ml 10F, 1µg/ml 52B83, 0.25 µg/ml 35G10F3, IP-300 1:400, 2 µg/ml J1D9 and 0.5 µg/ml 28401.111. Lane3+4, 7+8, 9+10, 15+16:10 and 20 ng TNFα detected with 2 µg/ml 4H31, 61E71, D9D10 and199.

TNFα in human skin
31
So they bind specifically to the monomeric form of TNFα protein (17kD). After longer exposure of the film 10F, 35G10F3 and IP-300 also seemed tobind to the TNFα dimer and tetramer protein, since a faint positively stainedband at 34 kD and 68 kD could be observed.
Distribution of TNFα in normal human skin
All antibodies were tested on cryosections of normal human skin. First,concentrations as used for detecting TNFα in cytospots and up to 5 µg/ml wereused to detect TNFα in human skin. With these concentrations, 10F, 61E71,199, J1D9 and 28401.111 did not stain any cell type in normal human skin,whereas 4H31, 52B83, D9D10, 35G10F3 and IP-300 showed positive staining innormal human skin. The pattern of staining of these latter antibodies wasdifferent. Also 10 µg/ml and 25 µg/ml of 10F, 61E71, 199, J1D9 and 28401.111were tested on skin, also in combination with the ABC protocol, to see whetherthese antibodies could detect TNFα in human skin at higher concentrations or adifferent protocol than were used for cytospots. Except for 199, all antibodiesstained positive on human skin using higher concentration antibody incombination with a different protocol. In Table 3 results of the detection ofTNFα using the different antibodies are summarized. Most of the antibodiesrevealed a diffuse granular staining pattern of the epidermis. 4H31 showed adifferent, very pronounced staining, only of the basal cell layer (Fig.4b).
Regarding staining of cells and structures in the dermis, most antibodiesdetected TNFα in endothelial cells, perivascular cells and cells scattered throughthe dermis.10F, D9D10, IP-300, J1D9 and 28401.111 reveal diffuse staining(Fig.2a,e. Fig .4f), whereas 52B83, 61E71 and 35G10F3 (Fig. 2b,c,d, Fig. 4d)stain more distinct cells. Different dermal structures like hair follicles, sweatglands and muscle are found positive with most tested antibodies (Table 3 andFig.3). Furthermore, no differences in immunoreactivity were seen betweennormal skin of different parts of the body. Skin was considered normal sinceonly biopsies were taken from healthy skin. Histologically the epidermal anddermal layer looked normal and contained no cellular infiltrates. The epidermallayer contains normal stratified keratinocytes and the dermal layer contains anormal pattern of connective tissue, resting endothelial cells and fibroblasts.

Chapter 2
32
Table 3: An overview of the results, using different antibodies to detect TNFα in normal humanskin.Antibody Concen-
trationDescription
10F 10 µg/ml Some epidermal cells positive; perivascular cells andscattered dermal cells diffusely positive; hair folliclespositive.
4H31 2 µg/ml Only basal cell layer of epidermis positive; no positivecells in the dermal cell layer; hair follicles and sweatglands positive.
52B83 5 µg/ml Faint granular-like staining in the epidermis, few cellsintensely positive; cells in dermis diffusely positive, withsome cells intensely positive; hair follicles, sweat glandsand muscle positive.
61E71 25 µg/ml Diffuse, granular-like staining through different layers ofepidermis, strongest in stratum basale; cells in dermisdiffusely positive, with some cells intensely positive; hairfollicles, sweat glands and muscle positive.
D9D10 10 µg/ml Diffuse, granular-like staining through different layers ofepidermis, strongest in stratum basale; diffuse positivitymainly in cells surrounding vessels; hair follicles, sweatglands positive.
35G10F3 2 µg/ml Diffuse, granular-like staining through different layers ofepidermis; strongest in stratum basale, some scatteredcells intensely positive; vascular and perivascular cells inthe dermis distinctly positive; hair follicles, sweat glandsand muscle (diffusely) positive.
IP-300 1:100 Diffuse granular-like staining through different layers ofepidermis, strongest in stratum basale; cells in thedermis, (peri)vascular and scattered, positive; hairfollicles, sweat glands and muscle positive.
199 25 µg/ml No staining observed.J1D9 10 µg/ml Diffuse, granular-like staining through different layers of
epidermis, strongest in stratum basale; cells in the dermisdiffusely positive; hair follicles faintly positive.
28401.111 25 µg/ml Epidermal and dermal cells faintly positive; hair folliclesand muscle diffusely positive.

TNFα in human skin
33
Distribution of TNF receptors p55 and p75 in normal human skin
The staining pattern of p55 in normal human skin was similar to the stainingpattern we observed with 4H31. Using anti-p55, we observed a clear staining ofthe basal cell layer of the epidermis (Fig.2f). Staining with anti-p75 antibody didnot lead to staining of cells of the epidermis and dermis.
Immunofluorescence double staining
To compare different staining patterns in more detail and identify the cellsthat stain positive for TNFα, double immunofluorescence staining wasperformed. 35G10F3 and IP-300 were used in combination with a cell specificantibody to see which cells are positive for TNFα. Both antibodies showed thatendothelial cells, but also other cells are TNFα positive. Furthermore, 35G10F3and IP-300 both showed that some but not all monocyte / macrophage like cellsare TNFα positive.
Pre incubation of TNFα antibodies with recombinant TNFα
In order to determine the specificity of the three antibodies with a cleardifferent staining pattern and of the antibodies that did not react with TNFα onblot, these antibodies were pre incubated with recombinant TNFα. After preincubation with TNFα, staining of 4H31, 61E71, D9D0, 35G10F3 or IP-300 wasabolished (Fig.4a, c, e).

Chapter 2
34
Figure 2. Staining patterns of TNFα using different TNFα antibodies (a-e) and the TNF receptor I,p55 (f) on cryosections of normal human skin. a) Antibody 10F: diffuse staining in the epidermallayer, b) Antibody 52B83: diffuse staining in the epidermal layer, clear staining of endothelial cells inthe dermal layer c) Antibody 61E71: diffuse staining in the epidermal layer, strongest in stratumbasale, d) Antibody 35G10F3: staining of endothelial cells in the dermal layer, e) Antibody28401.111: faint staining in the epidermal layer, f) Antibody MR1-2.
Figure 3. Positive staining of dermal structures a) Hair follicle - 10F, b) Muscle - 61E71 c) Sweatglands - 35G10F3.

TNFα in human skin
35
Figure 4. TNFα detection with (a, c, e) and without (b, d, f) preincubation of recombinant TNFαprotein, using (a, b ) 4H31, (c, d) 35G10F3 and (e, f) IP-300 (a-f 400x).

Chapter 2
36
Discussion
This study shows that TNFα is present in normal human skin, but thatdepending on which TNFα antibody is used, different staining patterns arefound. Furthermore, we found that although the tested antibodies are able todetect TNFα they are not necessarily useful for detecting TNFα in human skin.
Cryosections of normal human skin stained positively with all antibodies,except 199. Although TNFα antibodies 10F, 4H31, 52B83, 61E71, D9D10,35G10F3, IP-300, J1D9 and 28401.111 are able to detect TNFα in human skin,the staining pattern of these antibodies is different (Table 3 and Fig. 2, 3 and 4).35G10F3 and 4H31 revealed a clear distinct staining pattern, at a lowconcentration (2 µg/ml), which might imply that these antibodies have a highaffinity for TNFα. Antibodies 52B83, 61E71 and IP-300 are able to detectdistinct positive cells, but 10F, D9D10, J1D9 and 28401.111 reveal a diffusestaining pattern which is rather difficult to interpret.
In this study, we determined that although the antibodies reveal verydifferent staining patterns they all bind to TNFα. From the experiments with LPSstimulated PBMCs, in which we demonstrated that all antibodies reacted withstimulated, but not with unstimulated cells, we concluded that all antibodies areprobably reactive to TNFα protein. To confirm that the antibodies reactspecifically with TNFα and not with other proteins, Western blotting wasperformed. The antibodies 10F, 52B83, 35G10F3, IP-300, J1D9 and 28401.111detected only TNFα and none of the other proteins present. Therefore theseantibodies are judged to be specific for TNFα. Antibodies 4H31, 61E71, D9D10and 199 turned out not to be suitable for TNFα detection on blot. This may bedue to the changed availability of epitopes on blot. Conditions such as heating at57°C, although rather mild as compared to the usually used 100°C, and thepresence of SDS is known to induce conformational changes of the TNFαprotein, which may not be reversed during the rest of the procedure leading todestruction of epitopes.
Because specific reactivity for TNFα could not be confirmed for 4H31,61E71 and D9D10 on Western blot, an additional experiment with pre incubationof recombinant TNFα was performed. Abolishment of TNFα staining after thepre incubation confirmed that the antibodies are specific for TNFα. In addition,pre incubation of the antibodies 35G10F3 and IP-300 with recombinant TNFαand the double immunofluorescence experiments showed that although theseantibodies specifically bind TNFα and detect TNFα in endothelial cells andmonocytes, still different staining patterns are found.
These different staining patterns and differences as observed by using theother antibodies may be due to the fact that the antibodies recognize different

TNFα in human skin
37
epitopes or different forms of the TNFα protein. TNFα is synthesized as a pro-protein of 26 kD that is cleaved at the membrane by a metalloproteinase to a 17kD monomeric form (22;23) (24). The biological active TNFα is a homotrimerthat can mediate its effects after binding the membrane bound receptor TNF RI(p55) and TNF RII (p75) (25-27). Some antibodies may stain accumulation ofthe TNFα pro-protein, but also other forms such as membrane or receptorbound TNFα may be recognized by antibodies.
In this study, binding to mono, dimer or tetramer protein on Western blotdoes not correspond with a specific staining pattern on cryosections and can notexplain the different TNFα staining patterns on human skin. The staining patternof TNF receptor p55 was very similar to the pattern of 4H31.This may indicatethat 4H31 recognizes TNFα bound to its receptor and explain the staining patternof this antibody.
A staining pattern, similar to the one found by us, was described by Orteuet al. (28) for 35G10F3. Using the polyclonal antibody IP-300, Pierard et al. (11)showed positive staining of the upper layers, Terajima et al. (20) did not detectpositive staining in the epidermis, whereas we found staining in especially thebasal layer of the epidermis. So, even with the use of the same antibody differentstaining patterns are described. Discrepancies between our and earlier findingsusing 52B83 (19), 61E71 (9), D9D10 (29) and between our results and literaturein general may be explained by different concentrations of the antibody used, useof different protocols or different specificity of the antibodies used.
Our results confirm the conflicting results found in literature regarding thelocalization of TNFα in normal human skin using different antibodies. Therefore,the immunohistochemical approach should be used with care for studying TNFαproduction in human skin. It is not clear what underlies differences in stainingpattern of the different antibodies, and this makes comparison between studiesdifficult. Clear descriptions of the concentrations, protocols, and controls maymake it possible to compare different studies, but even then, for unambiguousinterpretation of data, it is important to know the characterization of theantibodies used. Elucidation of origin of differences in staining patterns maycontribute to interpretation of data.
In summary, we have shown that TNFα is present in normal human skin,but that depending on which TNFα antibody is used, different staining patternsare found. Furthermore, we found that although the tested antibodies are able todetect TNFα they are not necessarily useful for detecting TNFα in human skin.

Chapter 2
38
References
1. Luger, T. A. Epidermal Cytokines. Acta Derm.Venereol.Suppl.Stockh. 1989;151:61-76.
2. Kock, A., Schwarz, T., Kirnbauer, R., Urbanski, A., Perry, P., Ansel, J. C., and Luger, T. A.Human Keratinocytes Are a Source for Tumor Necrosis Factor Alpha: Evidence for Synthesisand Release Upon Stimulation With Endotoxin or Ultraviolet Light. J.Exp.Med. 1-12-1990;172(6):1609-14.
3. Ansel, J., Perry, P., Brown, J., Damm, D., Phan, T., Hart, C., Luger, T., and Hefeneider, S.Cytokine Modulation of Keratinocyte Cytokines. J.Invest.Dermatol. 1990;94(6 Suppl):101S-7S.
4. Bos, J. D. and Kapsenberg, M. L. The Skin Immune System: Progress in Cutaneous Biology.Immunol.Today 1993;14(2):75-8.
5. Oxholm, A., Oxholm, P., Staberg, B., and Bendtzen, K. Immunohistological Detection ofInterleukin I-Like Molecules and Tumour Necrosis Factor in Human Epidermis Before and AfterUVB-Irradiation in Vivo. Br.J.Dermatol. 1988;118(3):369-76.
6. Oxholm, A., Diamant, M., Oxholm, P., and Bendtzen, K. Interleukin-6 and Tumour NecrosisFactor Alpha Are Expressed by Keratinocytes but Not by Langerhans Cells. APMIS1991;99(1):58-64.
7. Oxholm, A. Epidermal Expression of Interleukin-6 and Tumour Necrosis Factor-Alpha in Normaland Immunoinflammatory Skin States in Humans. APMIS Suppl. 1992;24:1-32.
8. Kolde, G., Schulze, Osthoff K., Meyer, H., and Knop, J. Immunohistological and ImmunoelectronMicroscopic Identification of TNF Alpha in Normal Human and Murine Epidermis.Arch.Dermatol.Res. 1992;284(3):154-8.
9. Hoefakker, S., Caubo, M., van-'t-Erve, E. H., Roggeveen, M. J., Boersma, W. J., van-Joost, T.,Notten, W. R., and Claassen, E. In Vivo Cytokine Profiles in Allergic and Irritant ContactDermatitis. Contact.Dermatitis. 1995;33(4):258-66.
10. Paquet, P., Nikkels, A., Arrese, J. E., Vanderkelen, A., and Pierard, G. E. Macrophages andTumor Necrosis Factor Alpha in Toxic Epidermal Necrolysis. Arch.Dermatol. 1994;130(5):605-8.
11. Pierard, G. E., Nikkels, Tassoudji N., Arrese, J. E., Pierard, Franchimont C., and Leveque, J. L.Dermo-Epidermal Stimulation Elicited by a Beta-Lipohydroxyacid: a Comparison With SalicylicAcid and All-Trans-Retinoic Acid. Dermatology. 1997;194(4):398-401.
12. Walsh, L. J., Trinchieri, G., Waldorf, H. A., Whitaker, D., and Murphy, G. F. Human DermalMast Cells Contain and Release Tumor Necrosis Factor Alpha, Which Induces EndothelialLeukocyte Adhesion Molecule 1. Proc.Natl.Acad.Sci.U.S.A. 15-5-1991;88(10):4220-4.
13. Chu, C. Q., Field, M., Andrew, E., Haskard, D., Feldmann, M., and Maini, R. N. Detection ofCytokines at the Site of Tuberculin-Induced Delayed-Type Hypersensitivity in Man.Clin.Exp.Immunol. 1992;90(3):522-9.
14. Kristensen, M., Chu, C. Q., Eedy, D. J., Feldmann, M., Brennan, F. M., and Breathnach, S. M.Localization of Tumour Necrosis Factor-Alpha (TNF-Alpha) and Its Receptors in Normal and

TNFα in human skin
39
Psoriatic Skin: Epidermal Cells Express the 55-KD but Not the 75-KD TNF Receptor.Clin.Exp.Immunol. 1993;94(2):354-62.
15. Ruco, L. P., Stoppacciaro, A., Pomponi, D., Boraschi, D., Santoni, A., Tagliabue, A., Uccini, S.,and Baroni, C. D. Immunoreactivity for IL-1 Beta and TNF Alpha in Human Lymphoid andNonlymphoid Tissues. Am.J.Pathol. 1989;135(5):889-97.
16. Griffiths, C. E., Barker, J. N., Kunkel, S., and Nickoloff, B. J. Modulation of LeucocyteAdhesion Molecules, a T-Cell Chemotaxin (IL-8) and a Regulatory Cytokine (TNF-Alpha) inAllergic Contact Dermatitis (Rhus Dermatitis). Br.J.Dermatol. 1991;124(6):519-26.
17. Nickoloff, B. J., Karabin, G. D., Barker, J. N., Griffiths, C. E., Sarma, V., Mitra, R. S., Elder, J.T., Kunkel, S. L., and Dixit, V. M. Cellular Localization of Interleukin-8 and Its Inducer, TumorNecrosis Factor-Alpha in Psoriasis. Am.J.Pathol. 1991;138(1):129-40.
18. Castagnoli, C., Stella, M., Berthod, C., Magliacani, G., and Richiardi, P. M. TNF Production andHypertrophic Scarring. Cell Immunol. 1993;147(1):51-63.
19. Turner, G. D., Ly, V. C., Nguyen, T. H., Tran, T. H., Nguyen, H. P., Bethell, D., Wyllie, S.,Louwrier, K., Fox, S. B., Gatter, K. C., Day, N. P., White, N. J., and Berendt, A. R. SystemicEndothelial Activation Occurs in Both Mild and Severe Malaria. Correlating DermalMicrovascular Endothelial Cell Phenotype and Soluble Cell Adhesion Molecules With DiseaseSeverity. Am.J.Pathol. 1998;152(6):1477-87.
20. Terajima, S., Higaki, M., Igarashi, Y., Nogita, T., and Kawashima, M. An Important Role ofTumor Necrosis Factor-Alpha in the Induction of Adhesion Molecules in Psoriasis.Arch.Dermatol.Res. 1998;290(5):246-52.
21. Roozendaal, C., Zhao, M. H., Horst, G., Lockwood, C. M., Kleibeuker, J. H., Limburg, P. C.,Nelis, G. F., and Kallenberg, C. G. Catalase and Alpha-Enolase: Two Novel GranulocyteAutoantigens in Inflammatory Bowel Disease (IBD). Clin.Exp.Immunol. 1998;112(1):10-6.
22. Pennica, D., Nedwin, G. E., Hayflick, J. S., Seeburg, P. H., Derynck, R., Palladino, M. A., Kohr,W. J., Aggarwal, B. B., and Goeddel, D. V. Human Tumour Necrosis Factor: PrecursorStructure, Expression and Homology to Lymphotoxin. Nature 20-12-1984;312(5996):724-9.
23. Kriegler, M., Perez, C., DeFay, K., Albert, I., and Lu, S. D. A Novel Form of TNF/Cachectin Isa Cell Surface Cytotoxic Transmembrane Protein: Ramifications for the Complex Physiology ofTNF. Cell 8-4-1988;53(1):45-53.
24. Gearing, A. J., Beckett, P., Christodoulou, M., Churchill, M., Clements, J., Davidson, A. H.,Drummond, A. H., Galloway, W. A., Gilbert, R., Gordon, J. L., and et, al. Processing of TumourNecrosis Factor-Alpha Precursor by Metalloproteinases. Nature 18-8-1994;370(6490):555-7.
25. Smith, R. A. and Baglioni, C. The Active Form of Tumor Necrosis Factor Is a Trimer.J.Biol.Chem. 25-5-1987;262(15):6951-4.
26. Jones, E. Y., Stuart, D. I., and Walker, N. P. Structure of Tumour Necrosis Factor. Nature 16-3-1989;338(6212):225-8.
27. Bazzoni, F. and Beutler, B. The Tumor Necrosis Factor Ligand and Receptor Families.N.Engl.J.Med. 27-6-1996;334(26):1717-25.

Chapter 2
40
28. Orteu, C. H., Poulter, L. W., Rustin, M. H., Sabin, C. A., Salmon, M., and Akbar, A. N. TheRole of Apoptosis in the Resolution of T Cell-Mediated Cutaneous Inflammation. J.Immunol. 15-8-1998;161(4):1619-29.
29. de-Graaf, J. H., Tamminga, R. Y., Dam, Meiring A., Kamps, W. A., and Timens, W. ThePresence of Cytokines in Langerhans' Cell Histiocytosis. J.Pathol. 1996;180(4):400-6.

Chapter III
Local cellular inflammation as a result of elective standardized vascularsurgery
Namkje van der Laan 1
Lou de Leij PhD 2
Henk Jan ten Duis MD, PhD 1
1 Department of SurgeryUniversity Hospital GroningenThe Netherlands
2 Department of Pathology Laboratory medicine, section Medical BiologyUniversity Hospital GroningenThe Netherlands
Acta Histochemica 2001 103(2):139-149

Chapter 3
42
Summary
During surgery, incision of the skin under aseptic conditions is performed.Despite the absence of noxious agents, an inflammatory response may beinduced. We studied the local inflammatory response in human skin as a result ofsurgical intervention, under aseptic conditions. Elective standardized vascularsurgery served as a model. A series of skin biopsies was taken from the woundedge at different time points after first incision. Biopsies, directly taken at firstincision were considered to represent normal skin. Additional biopsies weretaken at 30 min after the start of surgery and just before closure of the wound,maximally 270 min after surgery. Kinetics of recruitment of cells, expression ofadhesion molecules and the presence of pro-inflammatory cytokines was studied.Granulocytes were observed at first at 30 min after incision of the skin and theirnumber increased in time. This granulocyte infiltration is paralleled by E-selectinexpression on endothelial cells, which also was observed at first at 30 min aftersurgery with a further increase in number in time. Incision of the skin did notchange P-selectin, ICAM-1, VCAM-1, TNFα, IL1α, IL1β, IL6 and IL8expression. These results show that incision of the skin under aseptic conditionsduring elective standardized vascular surgery induces local nonspecific cellularinflammation.

Local skin inflammation as a result of elective surgery
43
Introduction
Inflammatory responses can be initiated by a variety of stimuli likeinfection, implantation of foreign body substances or transplantation. Also blunttrauma and surgical intervention, stimuli in the absence of noxious substances,may induce such a response. Different types of stimuli may lead to differentinflammatory responses in vivo, for example in human skin.
The local inflammatory response is characterized, in part, by recruitment ofleukocytes into the site of inflammation (1-3). Granulocytes are the first cells thatmigrate into injured tissue. Recruitment of granulocytes and leukocytes in generalis mediated by the presence of adhesion molecules, which are expressed by bothendothelial cells and leukocytes (4;5). In vitro data show that E-selectin, VCAM-1 and ICAM-1 bind different types of leukocytes (6) (7-11). So, expression ofspecific adhesion molecules can influence the spectrum of leukocytes thatmigrate into the tissue.Besides expression of adhesion molecules, migration of leukocytes is influencedby the presence of chemotactic factors. These chemotactic factors includechemokines, anaphylatoxins and cytokines (12;13). Cytokines regulate inductionand kinetic expression of adhesion molecules (14). Incubation of culturedendothelial cells with pro-inflammatory cytokines such as TNFα, IL1α or IL1βleads to expression of E-selectin and VCAM-1, which are both not present onresting endothelial cells. Endothelial cells constitutively express ICAM-1, butafter stimulation with pro-inflammatory cytokines, expression is upregulated(15;16).
There are many in vitro data concerning the production of cytokines bycells of the skin immune system (SIS)(17-20), induction of expression ofadhesion molecules on endothelial cells by cytokines and binding of differentleukocyte cell types to endothelial cells (21). However, the relation betweenrecruitment of cells, expression of adhesion molecules and cytokine production,as a result of different stimuli -such as injury or tissue damage- in the in vivosituation in human skin, needs further documentation.
During surgery, incision of the skin is performed under aseptic conditionsand an inflammatory response may be induced despite the absence of noxiousagents. To obtain more insight in local inflammatory responses as a result ofinjury, we investigated the relation between recruitment of cells, expression ofadhesion molecules and pro-inflammatory cytokines in human skin as a result ofincision. In this study, surgical intervention in an elective standardized vascularsurgical procedure served as a model for the induction of an asepticinflammatory response.

Chapter 3
44
Material and methods
Skin biopsies
Six patients (3 male, 3 female) with a median age of 60 (44-76) years wereincluded in this study. Written informed consent was given and this study wasapproved by the local ethics committee (MEC 99/04/064). Biopsies were takenfrom apparently normal skin of healthy patients undergoing elective vascularsurgery. During surgery, skin biopsies were taken from the wound edge at firstincision using a scalpel. Biopsies were cut along the edge of the wound with alength of approximately 1 cm and a maximum thickness of 5 mm. Great care wastaken not to touch the skin during incision with tweezers to prevent damage ofthe skin biopsy. The first biopsy taken at the start of surgery was considered tobe normal skin. The second biopsy was taken after an interval of 30 min, thethird biopsy at the end of the operative procedure at 135, 140, 145, 155, 215 or270 min after start of surgery, just before closure of the wound. All biopsies wereimmediately snap frozen in liquid nitrogen and stored at -80°C until use.
Antibodies
Antibodies that were used for immunohistochemical staining are listed inTable 1.
Immunohistochemistry
For immunohistochemistry, sections of human skin (6 µm thick) were cutusing a cryostat, air dried and fixed for 10 min using acetone. Sections wereincubated for 1 h with antibodies in the appropriate concentration diluted in PBS(see Table 1). After washing with 0.01M Phosphate Buffered Saline (PBS) for 5min, sections were incubated for 30 min with horseradish peroxidase rabbit anti-mouse conjugate (RαM-PO; P260; Dako) in a 1:40 dilution in PBS supplementedwith 1% normal human serum. After washing with PBS, peroxidase activity wasvisualized using amino-ethylcarbazole (AEC; Sigma, St. Louis MO, USA) assubstrate. Sections were counterstained with hematoxylin and mounted inKaiser’s glycerin. As a control, the first antibody was omitted or an isotypematched, irrelevant antibody was used. In both cases, staining was not observedin human skin cryostat sections.

Local skin inflammation as a result of elective surgery
45
Table 1: Antibodies used for immunohistochemistryAntibody Antigen Source Used dilutionNA1/34 CD1a Dako, Glostrup, Denmark 1:100WT32 CD3 Gift of W. Tax SupernatantMy4 CD14 Coulter, Hialeah FL, USA 1:405D2 CD16 CLB, Amsterdam, The Netherlands SupernatantMOC1 CD56 In house produced antibody SupernatantCLB-B13.9 CD66b CLB 1:400EBM-1 CD68 Dako 1:40S12(C50) P-selectin Centocor, Malvern PA, USA 1:4000H18/7 acb E-selectin Gift of M.A. Gimbrone SupernatantHu 5/3-2.1 ICAM-1 Gift of M.A. Gimbrone SupernatantE 1/6 aa2 VCAM-1 Gift of M.A. Gimbrone SupernatantHECA-452 SHR Gift of A. Duijvestijn 1:104H31 TNFα Gift of W. Buurman 2 µg/ml35G10F3 TNFα Genzyme, Cambridge MA, USA 2 µg/ml1277-89-71277-82-291279-143-4
Interleukin 1α Gift of H. Towbin 10 µg/ml
2D8 Interleukin 1β Immunokontact, Brussel, Belgium 1:20IL6-16 Interleukin 6 CLB 1:201618-01 Interleukin 6 Genzyme 1:2052E8 Interleukin 8 Gift of M. Sticherling Sup 1:40134P HLA-DR IQP, Groningen, The Netherlands 1:15
Quantification of number of cells
Numbers of positive granulocytes, monocytes, macrophages, Langerhanscells, and HLA-DR-positive cells were determined using a Quantimet 600 (Q600;Leica, Cambridge, UK). The baseline level for positive cells was determined foreach marker and positive cells within one area (0.3 mm2) were measured aspercentage area of the total skin area. In each single skin section of each patientat each time point studied, 4 areas were measured and the mean of these areaswas determined. This resulted in 6 values (each for one patient) for each of thestudied time points. Finally, the mean values of all patients for each time pointwere determined, resulting in a mean and standard deviation for elastase, CD14,CD68, CD1a and HLA-DR surface area expression at start of surgery, 30 minafter and at the end of surgery.
Total numbers of CD3-positive cells for each skin biopsy were countedunder the microscope for each patient and mean numbers of cells at each timepoint were determined.

Chapter 3
46
ELISA
Supernatants of skin biopsies were used for TNFα ELISA. The methodfor skin lysis as described by Terajima et al.(22) with some modifications wasused: skin biopsies were weighed (30-100 mg), cut with a scalpel and suspendedin PBS (5 µg/ml) containing 1% Tween-20 (Sigma) and 1% human serumalbumin (CLB). Skin was repeatedly frozen in liquid nitrogen and thawed at 37°Cfor 5 times. Samples were centrifuged for 20 min at 18000g at 4°C, collected andstored at -80°C until measurement. The presence of TNFα in the undilutedsupernatant was established using a sandwich ELISA as described previously(23). Briefly, anti-TNFα in a dilution of 1:1000 (MAB 610; R&D Systems,Abingdon, UK) was used as primary antibody and biotin-labeled goat anti-humanTNFα (AB-210-NA; R&D Systems) as secondary antibody. Recombinanthuman TNFα (Boehringer, Ingelheim, Germany) served as standard.

Local skin inflammation as a result of elective surgery
47
Results
Cells
During the surgical procedure, granulocytes positive for elastase, CD16and CD66b infiltrated into the human skin at the wound edge. To exclude thepossibility that CD16 was expressed by NK cells, we studied CD56 expressionas well, which turned out to be negative in all skin biopsies studied. Verycomparable results were obtained when sections were stained for elastase, CD16or CD66b to detect granulocytes. A few more cells were found positive forelastase, when compared with CD16 and/or CD66b expression, but the patternsof granulocyte infiltrate were similar.
In the first biopsy, taken at the start of surgery, granulocytes were notpresent (Fig. 1a). After an interval of 30 min, the presence of scatteredgranulocytes was observed (Fig. 1b). These cells were located in close proximityto vessels. At later time points, the amount of granulocytes increased markedly,cells migrated into the dermal layer of the skin and distribution patterns ofgranulocytes were more diffuse (Fig. 1c). The amount of granulocytes thatinfiltrated into the skin varied between persons, but overall the pattern ofrecruitment over time showed a marked uniformity (Fig. 2, Table 2).
Figure 1. Granulocytes (CD66b positive cells) in human skin after surgical incision, a) at the start ofsurgery; b) at 30 min after first incision; and c) at 215 min after first incision. Original magnification,x127.

Chapter 3
48
Figure 2. Percentage (%) area of infiltrating granulocytes (elastase-positive cells) in time asmeasured with image analysis.
Table 2: Mean percentage (%) areas of positive cells of total skin surfaceCell type % area at start of
surgery *% area at 30 minafter surgery *
% area at end ofsurgery *
Elastase 0 ± 0 0.14 ± 0.10 5.91 ± 1.58CD14 1.17 ± 0.13 1.34 ± 0.25 1.22 ± 0.18CD68 1.16 ± 0.11 1.25 ± 0.14 1.23 ± 0.15CD1a 1.60 ± 0.15 1.69 ± 0.24 1.63 ± 0.12HLA-DR 4.91 ± 0.47 4.51 ± 0.35 4.68 ± 0.40* Mean values ± standard deviations
The increase in granulocyte numbers coincided with an increase in sialylLewis x, which is a ligand for E-selectin and can be recognized by HECA-452. Innormal skin, HECA-452 reacted with a few scattered mononuclear cells locatedin the dermis, but not with cells in the epidermis. At later time points afterincision, infiltrating granulocytes stained HECA-452 positive. Therefore, theincrease in numbers of granulocytes was accompanied by an increase in numberof HECA-452-positive cells.
The mean number of monocyte and macrophage-like cells (cells positivefor CD14 and/or CD68), Langerhans cells (CD1a-positive cells) and HLA-DR-positive cells, measured as percentage of the total skin surface area did notchange in time (Table 2). Numbers of T cells (CD3-positive cells) also did notchange during the observation period. Mean total numbers of T cells per sectionwere 42 at the start of surgery, 38 after 30 min and 40 at the end of surgery.
Granulocyte infiltrate
Time in minutes
0 50 100 150 200 250 300
% A
rea
of e
last
ase-
posi
tive
cells
of t
otal
ski
n su
rfac
e0
2
4
6
8

Local skin inflammation as a result of elective surgery
49
Furthermore, the distribution patterns of cells positive for CD14, CD68,CD1a, CD3 and HLA-DR did not change over time. In the biopsy, that wastaken at the start of surgery and is considered to be normal skin, CD14-positiveand CD68-positive cells were found scattered throughout the upper dermis.CD1a-positive cells were distributed in the epidermis, CD3-positive cells weredetected in small groups throughout the dermis and HLA-DR expression wasobserved on monocytes, Langerhans cells and endothelial cells.
Adhesion molecules
E-selectin expression was induced in human skin during surgical incisionwhereas expression of P-selectin, ICAM-1 and VCAM-1 did not change. In thefirst biopsy, E-selectin expression was absent (Fig. 3a) and at 30 min after thefirst incision, E-selectin expression was observed in some, but not all of thevessels. Numbers of positive vessels increased over time (Fig. 3b). Localizationof E-selectin positivity corresponded with the presence of infiltratedgranulocytes.
P-selectin is present on endothelial cells of normal human skin. In thepresent study, P-selectin expression was observed at all time points. Intensity ofexpression did not change over time. In normal human skin, ICAM-1 isconstitutively expressed by dermal endothelial cells and changes in intensity ofICAM-1 expression were hard to detect (Fig. 3c,d). VCAM-1 expression isabsent in normal human skin. During period of time of the present investigation,VCAM-1 expression was not induced.
Cytokines
We did not observe significant changes in TNFα, IL1α, IL1β, IL6 or IL8expression as a result of incision in human skin. We used 2 anti-TNFαantibodies and expression was observed in normal skin with both antibodies.Antibody 35G10F3 gives a diffuse granular staining of different layers of theepidermis, with strongest expression in stratum basale. Vascular and perivascularcells, hair follicles and glands in the dermis stained positive. With antibody 4H31,TNFα expression was found in the epidermis, only in the stratum basale (Fig.4a). With the use of an antibody mixture, IL1α expression was observed innormal skin in the epidermal cell layer with strongest expression in the stratumbasale. In the dermal layer, endothelial cells, hair follicles and glands expressedIL1α. Patients were not similar with respect to expression levels of TNFα andIL1α. Because of positivity in normal skin and because of the intra-individualdifferences, determination of induction of the expression of TNFα and IL1α was

Chapter 3
50
not possible. In none of the skin biopsies expression of IL1β or IL6 wasobserved.
Figure 3. a) Lack of E-selectin expression in normal skin; b) E-selectin expression at 155 min afterfirst incision (note that some but not all vessels are positive); c) ICAM-1 expression in normal skin;and d) ICAM-1 expression at 30 min after first incision. Original magnification, x127.
From the first incision up to the latest biopsy at 270 min, IL8 expressionwas observed. IL8 was present in the suprabasal cell layers of the epidermis andin hair follicles in the dermis (Fig. 4b). We did not observe significant changes inintensity of staining over time.

Local skin inflammation as a result of elective surgery
51
Figure 4. a) Expression of TNFα as demonstrated with antibody 4H31 and b) IL8 in human skin at30 min after first incision. Original magnification, x127.
ELISA
We were not able to detect TNFα in the undiluted supernatant of the skinbiopsies, as TNFα levels were under the detection limit (20 pg/ml).

Chapter 3
52
Discussion
The present study shows that incision of the skin under aseptic conditionsduring elective standardized vascular surgery induces local nonspecific cellularinflammation. Local cellular inflammation was demonstrated by infiltration ofgranulocytes in combination with E-selectin expression.
Granulocytes were observed already at 30 min after incision and theirnumbers increased subsequently over time. Our results are in agreement withprevious studies indicating that granulocytes are the first cells migrating intotissue during inflammation (1;2;24). Cell types other than granulocytes did notmigrate into the skin as a result of skin incision, which can be explained by theshort study period, the limited extent of tissue damage and the type of stimulus.Tissue damage as a result of incision in combination with the absence of noxioussubstances induces a nonspecific immune response. That indeed a nonspecificimmune response is induced, was confirmed by the fact that there was not anincrease in numbers of T cells and expression of HLA-DR.
Furthermore, local inflammation was characterized in this study by E-selectin expression on endothelial cells. Incision of the skin did not result indistinct changes in expression of the other adhesion molecules studied, P-selectin, ICAM-1 and VCAM-1. The absence of VCAM-1 expression may beexplained by the short study period in combination with the type of stimulus.
E-selectin expression and infiltration of granulocytes in skin occurredsimultaneously. This is in agreement with in vitro and in vivo studies showing thatneutrophils can bind to E-selectin (8). Furthermore, we observed that sialyl Lewisx, which is a ligand for E-selectin and is recognized by HECA-452, wasexpressed by the infiltrating granulocytes. It has been shown that the HECA-452antigen is involved in adhesion of neutrophils (25;26). Therefore, we concludethat granulocyte migration into the dermal layer is mediated by binding to E-selectin (27;28).
Skin is always in contact with the environment and therefore de novoadhesion molecules are expressed constitutively to sustain recirculation ofimmune cells for immune surveillance. This prone state enables the skin torespond with a very rapid inflammatory reaction as we indeed observed. Soalthough the intensity of P-selectin and ICAM-1 was not significantly altered,they may play a role in granulocyte migration (29;30).
There was virtually no TNFα, IL1α, IL1β, IL6 and/or IL8 production inskin as a result of incision. We tried to detect TNFα expression with ELISA, butTNFα levels in supernatant of these skin biopsies were below the detection limit.IL1β and IL6 expression was not observed in any of the skin sections, butadditional experiments (not shown) showed that these antibodies did not result in

Local skin inflammation as a result of elective surgery
53
detection of ILβ and IL6 in cryostat sections of human skin. Therefore, we cannot exclude that IL1β and, or IL6 are involved in early inflammatory responses.
The absence of a clear TNFα upregulation in our experiments is inagreement with the data presented by Strickland et al. (31). Instead, they andothers (32); (33) (24) have shown that IL8 and not TNFα plays an important rolein the early inflammatory response in human skin. IL8 is known to be achemoattractant for neutrophils and already at 30 min after IL8 injection inhuman skin, neutrophils are found in close proximity of vessels (34;35). In thepresent study, IL8 expression was observed in the suprabasal layers of theepidermis (Fig. 4b). With the use of antibody 52E8 an intracellular stored form ofIL8 was detected. This stored form of IL8 is secreted by cells in its active form.Skin biopsies of patients with psoriasis, acute and delayed pressure or chronicurticaria showed decreased IL8 expression using this antibody (36-38).Therefore, we expected to find decreased IL8 expression as a result of skinincision. The fact that there were no distinct differences in IL8 expressionbetween the biopsies may be explained by the relative short study period, thelimited extent of tissue damage and the relative small cell infiltrates as observedhere as compared with chronic skin disorders.
Other chemotactic factors besides IL8 may be involved in local cellularinflammation in skin. Factors such as the anaphylatoxins C3a and C5a can attractgranulocytes (1). It has been shown that at 30 min after injection of C5a in humanskin, neutrophil infiltrates are located around vessels (34). Measurements ofcomplement in serum samples have shown that vascular surgery activatescomplement and induces neutrophil recruitment and degranulation (39). Westudied C3c (data not shown), which is a C3b component. However, there wasno C3c present in any of the skin biopsies.
In summary, our data show that aseptic incision of the skin during electivestandardized vascular surgery induces local nonspecific cellular inflammation.The tissue damage as a result of incision leads to a nonspecific inflammatoryresponse which is characterized by granulocyte infiltration into the skin, incombination with E-selectin expression.

Chapter 3
54
Acknowledgements
We would like to thank W. Buurman, A. Duijvestijn, M. Sticherling and H.Towbin for providing us with the monoclonal antibodies.

Local skin inflammation as a result of elective surgery
55
References
1. Clark, R. A. Basics of Cutaneous Wound Repair. J.Dermatol.Surg.Oncol. 1993;19(8):693-706.
2. Ross, R., Raines, E. W., and Bowen, Pope DF. The Biology of Platelet-Derived Growth Factor.Cell 18-7-1986;46(2):155-69.
3. Witte, M. B. and Barbul, A. General Principles of Wound Healing. Surg.Clin.North Am.1997;77(3):509-28.
4. Carlos, T. M. and Harlan, J. M. Leukocyte-Endothelial Adhesion Molecules. Blood 1-10-1994;84(7):2068-101.
5. Zimmerman, G. A., Prescott, S. M., and McIntyre, T. M. Endothelial Cell Interactions WithGranulocytes: Tethering and Signaling Molecules. Immunol.Today 1992;13(3):93-100.
6. Rothlein, R., Dustin, M. L., Marlin, S. D., and Springer, T. A. A Human Intercellular AdhesionMolecule (ICAM-1) Distinct From LFA-1. J.Immunol. 15-8-1986;137(4):1270-4.
7. Bevilacqua, M. P., Stengelin, S., Gimbrone-MA, Jr, and Seed, B. Endothelial LeukocyteAdhesion Molecule 1: an Inducible Receptor for Neutrophils Related to Complement RegulatoryProteins and Lectins. Science 3-3-1989;243(4895):1160-5.
8. Hession, C., Osborn, L., Goff, D., Chi, Rosso G., Vassallo, C., Pasek, M., Pittack, C., Tizard, R.,Goelz, S., McCarthy, K., and et, al. Endothelial Leukocyte Adhesion Molecule 1: DirectExpression Cloning and Functional Interactions. Proc.Natl.Acad.Sci.U.S.A. 1990;87(5):1673-7.
9. Elices, M. J., Osborn, L., Takada, Y., Crouse, C., Luhowskyj, S., Hemler, M. E., and Lobb, R. R.VCAM-1 on Activated Endothelium Interacts With the Leukocyte Integrin VLA-4 at a SiteDistinct From the VLA-4/Fibronectin Binding Site. Cell 23-2-1990;60(4):577-84.
10. Carlos, T., Kovach, N., Schwartz, B., Rosa, M., Newman, B., Wayner, E., Benjamin, C., Osborn,L., Lobb, R., and Harlan, J. Human Monocytes Bind to Two Cytokine-Induced AdhesiveLigands on Cultured Human Endothelial Cells: Endothelial-Leukocyte Adhesion Molecule-1 andVascular Cell Adhesion Molecule-1. Blood 15-5-1991;77(10):2266-71.
11. Dobrina, A., Menegazzi, R., Carlos, T. M., Nardon, E., Cramer, R., Zacchi, T., Harlan, J. M.,and Patriarca, P. Mechanisms of Eosinophil Adherence to Cultured Vascular Endothelial Cells.Eosinophils Bind to the Cytokine-Induced Ligand Vascular Cell Adhesion Molecule-1 Via theVery Late Activation Antigen-4 Integrin Receptor. J.Clin.Invest. 1991;88(1):20-6.
12. Ebnet, K. and Vestweber, D. Molecular Mechanisms That Control Leukocyte Extravasation: theSelectins and the Chemokines. Histochem.Cell Biol. 1999;112(1):1-23.
13. Osborn, L. Leukocyte Adhesion to Endothelium in Inflammation. Cell 13-7-1990;62(1):3-6.
14. Pober, J. S. Warner-Lambert/Parke-Davis Award Lecture. Cytokine-Mediated Activation ofVascular Endothelium. Physiology and Pathology. Am.J.Pathol. 1988;133(3):426-33.
15. Rice, G. E., Munro, J. M., Corless, C., and Bevilacqua, M. P. Vascular and NonvascularExpression of INCAM-110. A Target for Mononuclear Leukocyte Adhesion in Normal andInflamed Human Tissues. Am.J.Pathol. 1991;138(2):385-93.

Chapter 3
56
16. Pober, J. S. and Cotran, R. S. Cytokines and Endothelial Cell Biology. Physiol.Rev.1990;70(2):427-51.
17. Kupper, T. S. Immune and Inflammatory Processes in Cutaneous Tissues. Mechanisms andSpeculations [Published Erratum Appears in J Clin Invest 1991 Feb;87(2):753]. J.Clin.Invest.1990;86(6):1783-9.
18. Barker, J. N., Mitra, R. S., Griffiths, C. E., Dixit, V. M., and Nickoloff, B. J. Keratinocytes AsInitiators of Inflammation [See Comments]. Lancet 26-1-1991;337(8735):211-4.
19. Gordon, J. R., Burd, P. R., and Galli, S. J. Mast Cells As a Source of Multifunctional Cytokines.Immunol.Today 1990;11(12):458-64.
20. Matsue, H., Cruz-PD, Jr, Bergstresser, P. R., and Takashima, A. Cytokine Expression byEpidermal Cell Subpopulations. J.Invest.Dermatol. 1992;99(5):42S-5S.
21. Bos, J. D. The Skin As an Organ of Immunity. Clin.Exp.Immunol. 1997;107 Suppl 1:3-5.
22. Terajima, S., Higaki, M., Igarashi, Y., Nogita, T., and Kawashima, M. An Important Role ofTumor Necrosis Factor-Alpha in the Induction of Adhesion Molecules in Psoriasis.Arch.Dermatol.Res. 1998;290(5):246-52.
23. Kobold, A. C., van-Wijk, R. T., Franssen, C. F., Molema, G., Kallenberg, C. G., and Tervaert, J.W. In Vitro Up-Regulation of E-Selectin and Induction of Interleukin-6 in Endothelial Cells byAutoantibodies in Wegener's Granulomatosis and Microscopic Polyangiitis. Clin.Exp.Rheumatol.1999;17(4):433-40.
24. Engelhardt, E., Toksoy, A., Goebeler, M., Debus, S., Brocker, E. B., and Gillitzer, R. ChemokinesIL-8, GROalpha, MCP-1, IP-10, and Mig Are Sequentially and Differentially Expressed DuringPhase-Specific Infiltration of Leukocyte Subsets in Human Wound Healing. Am.J.Pathol.1998;153(6):1849-60.
25. De Boer, O. J., Horst, E., Pals, S. T., Bos, J. D., and Das, P. K. Functional Evidence That theHECA-452 Antigen Is Involved in the Adhesion of Human Neutrophils and Lymphocytes toTumour Necrosis Factor-Alpha-Stimulated Endothelial Cells. Immunology 1994;81(3):359-65.
26. Tu, L., Murphy, P. G., Li, X., and Tedder, T. F. L-Selectin Ligands Expressed by HumanLeukocytes Are HECA-452 Antibody-Defined Carbohydrate Epitopes Preferentially Displayedby P-Selectin Glycoprotein Ligand-1. J.Immunol. 1-11-1999;163(9):5070-8.
27. Springer, T. A. and Lasky, L. A. Cell Adhesion. Sticky Sugars for Selectins. Nature 17-1-1991;349(6306):196-7.
28. Silber, A., Newman, W., Reimann, K. A., Hendricks, E., Walsh, D., and Ringler, D. J. KineticExpression of Endothelial Adhesion Molecules and Relationship to Leukocyte Recruitment inTwo Cutaneous Models of Inflammation. Lab.Invest. 1994;70(2):163-75.
29. Burns, A. R., Bowden, R. A., Abe, Y., Walker, D. C., Simon, S. I., Entman, M. L., and Smith, C.W. P-Selectin Mediates Neutrophil Adhesion to Endothelial Cell Borders. J.Leukoc.Biol.1999;65(3):299-306.

Local skin inflammation as a result of elective surgery
57
30. Yeo, E. L., Sheppard, J. A., and Feuerstein, I. A. Role of P-Selectin and Leukocyte Activation inPolymorphonuclear Cell Adhesion to Surface Adherent Activated Platelets Under PhysiologicShear Conditions (an Injury Vessel Wall Model). Blood 1-5-1994;83(9):2498-507.
31. Strickland, I., Rhodes, L. E., Flanagan, B. F., and Friedmann, P. S. TNF-Alpha and IL-8 AreUpregulated in the Epidermis of Normal Human Skin After UVB Exposure: Correlation WithNeutrophil Accumulation and E-Selectin Expression. J.Invest.Dermatol. 1997;108(5):763-8.
32. Rot, A. Neutrophil Attractant/Activation Protein-1 (Interleukin-8) Induces in Vitro NeutrophilMigration by Haptotactic Mechanism. Eur.J.Immunol. 1993;23(1):303-6.
33. Garner, W. L., Rodriguez, J. L., Miller, C. G., Till, G. O., Rees, R. S., Smith, D. J., and Remick,D. G. Acute Skin Injury Releases Neutrophil Chemoattractants. Surgery 1994;116(1):42-8.
34. Schubert, C., Christophers, E., Swensson, O., and Isei, T. Transendothelial Cell Diapedesis ofNeutrophils in Inflamed Human Skin. Arch.Dermatol.Res. 1989;281(7):475-81.
35. Swensson, O., Schubert, C., Christophers, E., and Schroder, J. M. Inflammatory Properties ofNeutrophil-Activating Protein-1/Interleukin 8 (NAP-1/IL-8) in Human Skin: a Light- andElectronmicroscopic Study. J.Invest.Dermatol. 1991;96(5):682-9.
36. Sticherling, M., Bornscheuer, E., Schroder, J. M., and Christophers, E. Localization ofNeutrophil-Activating Peptide-1/Interleukin-8-Immunoreactivity in Normal and Psoriatic Skin.J.Invest.Dermatol. 1991;96(1):26-30.
37. Sticherling, M., Bornscheuer, E., Schroder, J. M., and Christophers, E. ImmunohistochemicalStudies on NAP-1/IL-8 in Contact Eczema and Atopic Dermatitis. Arch.Dermatol.Res.1992;284(2):82-5.
38. Hermes, B., Prochazka, A. K., Haas, N., Jurgovsky, K., Sticherling, M., and Henz, B. M.Upregulation of TNF-Alpha and IL-3 Expression in Lesional and Uninvolved Skin in DifferentTypes of Urticaria. J.Allergy Clin.Immunol. 1999;103(2 Pt 1):307-14.
39. Groeneveld, A. B., Raijmakers, P. G., Rauwerda, J. A., and Hack, C. E. The InflammatoryResponse to Vascular Surgery-Associated Ischaemia and Reperfusion in Man: Effect onPostoperative Pulmonary Function. Eur.J.Vasc.Endovasc.Surg. 1997;14(5):351-9.

Chapter 3
58

Chapter IV
Immunohistopathological appearance of three different types of injury inhuman skin
Namkje van der Laan 1
Lou de Leij PhD 2
Henk Jan ten Duis MD, PhD 1
1 Department of SurgeryUniversity Hospital GroningenThe Netherlands
2 Department of Pathology Laboratory medicine, section Medical BiologyUniversity Hospital GroningenThe Netherlands
Inflammation Research 50 (2001) 350-356

Chapter 4
60
Summary
To determine whether underlying mechanisms of inflammation, like cellularinfiltrates, expression of adhesion molecule and cytokine patterns are similarunder different conditions of injury. Skin biopsies were taken of three differentgroups of patients in which local inflammation of the skin might occur.
Skin activation was studied as a result of incision during surgery underaseptic conditions, as a result of a local bacterial infection and as a result of blunttrauma, resulting in a femoral fracture, without disruption of the epithelial barrier.
Skin biopsies were snap frozen for immunohistochemical analysis.Incision of the skin resulted in a granulocyte infiltrate, paralleled by E-
selectin expression. As a result of infection granulocytes were observed andmonocyte / macrophage and T cell numbers were increased. Furthermore, E-selectin, VCAM-1 and ICAM-1 expression increased and cytokine expressionmarkedly changed compared to normal skin. Skin taken at the site of the femoralfracture showed no signs of inflammation.
Different stimuli lead to different local inflammatory responses in humanskin.

Different inflammatory responses in human skin
61
Introduction
As the first barrier to the outside, skin is an important and immunologicallyactive organ. Skin damage caused by injury or an invading pathogen induces acascade of events, which eventually leads to removal of the pathogen, repair ofthe skin and restoring of homeostasis. This repair or wound healing processinvolves three phases. The first phase, inflammation, is followed by tissueregeneration and tissue remodeling. Inflammation is characterized by classicalclinical features such as redness, swelling, pain, warmth and loss of function (1-3). These effects follow a series of events such as vasodilatation, increasedvascular permeability and recruitment of cells. Recruitment of cells is mediatedby the interaction between vascular and leukocyte adhesion molecules (4), whichexpression is regulated by a variety of cytokines and chemokines (5-7).
There are many different circumstances under which local inflammation ofskin can be induced: applying of irritant substances, burns, a simple cut, blunttrauma or local infection as the result of the presence of a corpus alienum, e.g. asplinter. Despite the variety of stimuli, skin reveals classical clinical features ofinflammation under all these circumstances: it becomes red, swollen, painful andwarm. Although the presence of an actual local cellular response has not beendescribed for all these stimuli, it is assumed that, irrespective of the type ofstimulus, a local cellular inflammatory reaction is induced in the skin. Localcellular inflammation in skin is usually described in general terms, but previousstudies have shown, that different cellular infiltrates are associated with differentadhesion molecule and cytokine expression patterns in two models of skininflammation (8).
So, to see whether skin showing the classical clinical features ofinflammation is indeed imunologically active and to get more insight into theunderlying local inflammatory processes in human skin, we studied local cellularinflammation in skin as a result of different stimuli.
It is known that one day after a surgical procedure incised skin revealssigns of inflammation, the skin around the wound is red and swollen. So, in thefirst group, we studied activation of the skin as a result of incision as part of asurgical procedure under aseptic conditions. The second group consisted ofpatients with a red and swollen skin as a result of a local bacterial infection. Alsoan extremity in which a fracture is present shows signs of inflammation, itbecomes swollen and warm. Therefore, we suppose that serious blunt traumacan also induce an inflammatory response in the skin. Consequently, the lastgroup consisted of patients that had an femoral fracture, without disruption of theepithelial barrier. By taking skin biopsies, we studied the composition of theinflammatory infiltrate, expression of adhesion molecules and pro-inflammatorycytokines in three different types of inflammation in human skin.

Chapter 4
62
Materials and methods
Patients and skin biopsies
Three groups of patients were included in this study.
Group 1: Local inflammation as a result of incision of the skin
To study the local inflammatory response as a result of disruption of theepithelial barrier, incision of the skin during elective standardized vascular surgeryserved as a model. Six patients (3 male, 3 female) with a median age of 60 years(44-76) were included in this study. Biopsies were taken from apparently normalskin of healthy patients undergoing elective vascular surgery. During surgery, skinbiopsies were taken from the wound edge at first incision. Great care was takennot to touch the skin during incision with tweezers to prevent damage of the skinbiopsy. The first biopsy taken at the start of surgery was considered to representnormal skin. The second biopsy was taken after an interval of 30 minutes, thethird biopsy at the end of the operative procedure (135, 140, 145, 155, 215 and270 minutes after start of surgery), just before closure of the wound.
Group 2: Local inflammation as a result of infection
To study local inflammation as a result of infection, skin of an infectedarea was studied in five patients (4 male, 1 female) with a median age of 49 (35-53). The infections were caused by a splinter, a bite, an abscess (2x) andthromboflebitis surrounding an arterial line. All patients needed surgical treatment.During surgery, biopsies were taken from skin including the infected area.Cultures showed that Staphylococcus aureus was present in all skin biopsies.
Group 3: Local inflammation as a result of mechanical injury
To study the effects of mechanical injury to the skin, without disruption ofthe epithelial barrier, ten patients (7 male, 3 female) with a medium age of 29years (20-45) were included in this study. All patients had at least one femoralfracture. After diagnostic procedures, all patients underwent surgical treatment.The femoral fractures were treated by closed reduction and intramedullary nailosteosynthesis. During the surgical procedure, two skin biopsies were taken fromplaces indicated in Figure 1. The skin biopsy (A), considered to be activatedskin, was taken halfway the leg at the site of the femoral fracture at the placewhere the femoral nail was locked. The biopsy (B) taken at the place where thefemoral nail was introduced served as an internal control. Biopsies were taken

Different inflammatory responses in human skin
63
directly at first incision to exclude the effect of the surgical procedure itself.Mean time between accident and biopsy was 7.5 hours, range 3.5-12.5 hours.
Figure 1. Skin biopsies were taken from places where nail is introduced (B) and locked (A) inpatients with a femoral fracture as a result of blunt trauma.
Normal skin
As a control, skin biopsies were obtained from patients in the first group.In this group, first biopsy taken at the start of surgery was considered torepresent normal skin.
Skin biopsies from all patients were immediately snap frozen in liquidnitrogen and stored at -80°C until use. The local ethics committee (MEC99/04/064) approved this study and written informed consent was given.
Immunohistochemistry and antibodies
For immunohistochemistry, 6 µm sections of human skin were cut, airdried and fixed for 10 minutes with acetone. Sections were incubated for onehour with the different antibodies diluted in 0,01M Phosphate Buffered Saline(PBS) (see Table 1). After washing with PBS for 5 minutes, sections wereincubated for 30 minutes with horseradish peroxidase rabbit anti-mouseconjugate (RαM-PO, P260, Dako, Glostrup, Denmark) at a 1:40 dilution in PBSsupplemented with 1% normal human serum. After washing with PBS,peroxidase reactivity was visualized using amino-ethylcarbazole (AEC, St.LouisMO, USA, Sigma) as a substrate. Sections were counterstained with hematoxylinand mounted in Kaiser’s glycerin. As a control, the first antibody was omitted oran isotype matched, irrelevant antibody was used. In both cases no staining wasobserved.

Chapter 4
64
Table 1: Antibodies used for immunohistochemistryAntibody Antigen Source Used dilutionNA1/34 CD1a Dako, Glostrup, Denmark 1:100WT32 CD3 Gift of W.Tax SupernatantMy4 CD14 Coulter, Hialeah, Fla., USA 1:405D2 CD16 CLB, Amsterdam, The Netherlands SupernatantCLB-B13.9 CD66b CLB, Amsterdam, The Netherlands 1:400EBM-1 CD68 Dako, Glostrup, Denmark 1:40S12 (C50) P-selectin Centocor, Malvern, PA, USA 1:4000H18/7 acb E-selectin Gift of M.A. Gimbrone SupernatantHu 5/3-2.1 ICAM-1 Gift of M.A. Gimbrone SupernatantE 1/6 aa2 VCAM-1 Gift of M.A. Gimbrone Supernatant1277-89-71277-82-291279-143-4
Interleukin 1α Gift of H. Towbin 10 µg/ml
35G10F3 TNFα Genzyme, Cambridge, MA., USA 1:5001618-01 Interleukin 6 Genzyme, Cambridge, MA., USA 1:2052E8 Interleukin 8 Gift of M. Sticherling Supernatant
1:40
ELISA
Supernatant of normal skin and infected skin biopsies were measured in aninterleukin 6 ELISA. For this, skin biopsies were weighed (30-100 mg), cut anddissolved in PBS (5 µg/ml) containing 1% Tween-20 (Sigma) and 1% humanserum albumin (CLB, Amsterdam, the Netherlands). Skin was repeatedly frozenin liquid nitrogen and put in 37°C until ice was thawed for 5 times. Samples werecentrifuged for 20 minutes at 13000 rpm at 4°C, collected and stored at -80°Cuntil measurement. The presence of IL6 in the supernatant was established usinga sandwich ELISA as described (9). Briefly, anti IL6 1:1000 (CLB.MIL6/16,CLB) was used as the first capture antibody and the biotin labeled goat antihuman IL6 (CLB.SIL6-D, CLB) as the second capture antibody. Recombinanthuman IL6 (206-IL-050; R&D Systems, Abingdon, UK) served as a standard.

Different inflammatory responses in human skin
65
Results
Normal skin
In normal human skin, Langerhans cells (CD1a positive cells) aredistributed mainly in the epidermis with some CD1a positive cells found scatteredthrough the dermis. Few T cells (CD3 positive cells) are detected and found tobe present as small clusters through the dermis. Monocyte / macrophages(CD14, CD68 positive cells) are found scattered through the dermis.Granulocytes (CD16, CD66b positive cells) are not detected in normal humanskin. P-selectin and ICAM-1 expression is observed on endothelial cells, whereasE-selectin and VCAM-1 expression is not observed. Furthermore, we foundTNFα, IL1α and IL8 in normal skin, whereas IL6 expression is absent. TNFαand IL1α show a similar expression pattern: expression is found throughout theepidermis, with strongest expression in stratum basal. In the dermis endothelialcells, hair follicles and glands stain positive. IL8 is present in the suprabasal celllayers of the epidermis and in hair follicles in the dermis.
Group 1: Local inflammation as a result of incision in human skin
During surgery, granulocytes infiltrated into human skin of the woundedge. In the first biopsy, taken at the start of surgery, granulocytes were notpresent. After an interval of 30 minutes, the presence of scattered granulocyteswas observed. These cells were located in close proximity to vessels. At latertime points, the amount of granulocytes increased markedly, cells migratedfurther and distribution was more diffuse throughout the dermal layer of the skin(Fig.2).
Figure 2. Granulocyte infiltrate as a result of incision during surgery under aseptic conditions: a) atthe very start of surgery, b) 30 minutes after incision and c) 145 minutes after incision (A 250x, B, C400x).

Chapter 4
66
The amount of granulocytes that infiltrated into the skin varied betweenpersons, but over all the pattern of recruitment over time showed a markeduniformity. The number and distribution of CD1a, CD3, CD14 and CD68positive cells did not change during the observation period.
E-selectin expression is induced on endothelial cells in human skin duringsurgery whereas P-selectin, ICAM-1 and VCAM-1 expression did not change. Inthe first biopsy E-selectin expression is absent. 30 minutes after first incision E-selectin expression was observed in some, but not all of the vessels (Fig.3).Number of positive vessels increased during time. Localization of E-selectinexpression corresponded with the presence of infiltrated granulocytes. In thisstudy, from first incision until the latest biopsy at 270 minutes, intensity of P-selectin did not change. Furthermore, no increase in intensity of ICAM-1expression and no induction of VCAM-1 protein expression was found.
We did not observe visible changes in intensity of TNFα, IL1α, IL6 orIL8 expression as a result of incision in human skin.
Group 2: Local inflammation in human skin as a result of infection
In biopsies taken from the infected skin, showing clinical signs ofinflammation, it was found that leukocyte infiltrates were present. In contrast tonormal skin granulocytes were present in the dermal layer. In all biopsies T cellswere found, located in the dermal layer, in increased numbers as compared tonormal skin. Furthermore, a massive increase in monocyte / macrophage likecells was observed in infected skin. They were visible throughout the dermis(Fig.4).
Furthermore E-selectin and VCAM-1 expression was induced and ICAM-1 expression was markedly increased compared to normal skin, whereas P-selectin expression did not change. E-selectin and VCAM-1 expression wasobserved on some but not all vessels. In contrast, ICAM-1 expression was notonly found on endothelial cells but also cells scattered through the dermis and in3 of the 5 patients, keratinocytes strongly expressed ICAM-1 (Fig.5).
Cytokine expression in infected skin has markedly changed compared tonormal skin. TNFα and IL1α expression is induced in keratinocytes in theepidermal cell layer. In the dermal layer, some infiltrated, but mainly endothelialcells showed increased expression for both cytokines. Furthermore, IL8expression in the lower layers of the epidermis had decreased or disappeared(Fig.6) in all biopsies. We did not observe IL6 expression in the skin usingimmunohistochemistry. In contrast, using an ELISA, we found elevated levels ofIL6 in infected skin. IL6 levels of 785 pg/ml and 915 pg/ml were measured inbiopsies of respectively 75 mg and 31 mg. IL6 levels in normal skin biopsies(115,9 mg and 46,6 mg) were below the detection limit (20 pg/ml) of the ELISA.

Different inflammatory responses in human skin
67
Group 3: Local inflammation in human skin as a result of mechanical injury
Skin taken at the site of a femoral fracture showed no differences innumber or distribution of any of the studied cells. Langerhans cells, T cells andmonocyte / macrophage like cells are present in similar numbers and distributionis similar compared to control and normal skin. Granulocytes are not observed inskin adjacent to the femoral fracture and in control skin.
Furthermore, no differences in P-selectin, ICAM-1 and VCAM-1expression compared to control and normal skin were observed. Some skinbiopsies from both the place where the femoral nail was introduced and from theplace where the nail was locked, near the fracture, showed E-selectin expressionon a few endothelial cells.
We did not observe changes in cytokine expression as compared tonormal skin. (Fig.7).

Chapter 4
68
Figure 3. E-selectin expression 155 minutes after incision (400x).
Figure 4. CD68 positive cells a) in normal skin, b) two days and c) four days after infection (A250x, B, C 400x).
Figure 5. a) ICAM-1 expression on endothelial cells of normal skin. b) In infected skin ICAM-1expression is also found on scattered cells in the dermis and c) keratinocytes (A, B 400x, C 250x).

Different inflammatory responses in human skin
69
Figure 6. IL8 expression a) in normal skin, b) four days after infection (A 400x, B 250x).
Figure 7. Skin biopsies taken 4 hours after a fracture, showing: a) the absence of granulocytes, b)ICAM-1 expression, c) the absence of E-selectin expression (A 250x, B-C 400x).

Chapter 4
70
Discussion
We studied the course of local inflammation in human skin under differentconditions. Although all biopsies studied were taken from skin showing generalclinical features of inflammation, we observed clear differences in the underlyingmechanisms of inflammation.
Our results show that disruption of the epithelial barrier, by incision of theskin under aseptic conditions induces a limited, whereas infection induces apronounced inflammatory response. Mechanical injury without disruption of theepithelial barrier does not show signs of inflammation on the cellular level.
We think it is an important observation that inflammation in skin is onlyinduced after disruption of the epithelial barrier and by the presence of noxioussubstances like bacteria. Just mechanical injury or pressure as a result ofmechanical injury does not seem to induce an inflammatory response in the skin.So, it is not necessarily true that clinical signs of inflammation present on theoutside correlate with an actual local cellular response in the skin.
The limited inflammatory response, as a result of disruption of theepithelial barrier by incision of the skin, is only characterized by recruitment ofgranulocytes in combination with E-selectin expression. Our results are inagreement with previous studies indicating that granulocytes are the first cellsmigrating into the tissue during inflammation (1;10-12). Incision of the skin didnot induce cytokine expression. It may be that the stimulus is too small and thestudy period too short to reveal visible changes in cytokine expression.
We expected to find a more pronounced response and differentinflammatory pattern in infected skin compared to incised skin. Indeed, we didnot only observe granulocytes, but also a clear increase in monocyte /macrophage and T cell numbers. Furthermore, E-selectin, VCAM-1 andincreased ICAM-1 expression was observed. In contrast to incised skin, infectedskin showed a markedly changed cytokine pattern, using immunohistochemistry.Antibodies against TNFα, IL1α and IL8 have proven to be appropriate to detectcytokines in cryosections (13-15). TNFα and IL1α expression is increased,whereas IL8 expression was decreased in infected skin. With antibody 52E8 anintracellularly stored form of IL8 was detected. This stored form is secreted here,as is also seen in chronic skin disorders like psoriasis, acute, delayed pressure orchronic urticaria (15-17). IL8 is known to be a chemoattractant (18) and itsrelease may play an important role in attracting the observed granulocytes andmonocyte / macrophage like cells. We were not able to detect IL6 in the skinusing immunohistochemistry, but ELISA experiments showed a clear increasedIL6 protein concentration in infected skin compared to normal skin. Apparentlythe antibody, in combination with the protocol we used, was not appropriate todetect IL6 in cryostat sections of human skin.

Different inflammatory responses in human skin
71
The different and pronounced adhesion molecule expression in infectedskin compared to incised skin might be explained by locally produced andreleased cytokines or by bacteria that are present. E-selectin, P-selectin andICAM-1 are able to bind granulocytes (19-22) and can mediate granulocyterecruitment in both incised and infected skin. It is known that monocytes andlymphocytes can bind to VCAM-1 (23-25). So, monocyte / macrophage and Tcell recruitment in infected skin can be mediated by VCAM-1. Based on theseresults, we believe that the adhesion molecule expression patterns can be relatedto the observed different cellular infiltrates in the two inflammatory conditions.Although the different time points at which incised and infected skin were studiedcan explain differences in cellular infiltrates, magnitude and seriousness of theresponse is probably a result of the type of injury.
Skin adjacent to the fracture does not show signs of inflammation on thecellular level: we did not find cellular infiltrates or increased adhesion moleculeand cytokine expression. This is in contrast to what we expected, because on theouter side, the leg shows clinical signs of inflammation: it is swollen and warm.There is one study of skin activation after a fracture in mice. Catania et al.(26)described the effect of a closed tibial fracture on skin cytokine production andfound pro-inflammatory cytokine gene expression in injured and uninjured remoteskin. We were not able to observe a visible increase of pro-inflammatorycytokines on the protein level, using immunohistochemistry. There are manyreports about inflammation in human skin as a result of injury in general, e.g. burninjury, disruption of the skin, tape stripping and injection or applying of irritantsubstances(8;11;27-30) But, these are all kinds of stimuli that directly damage oractivate cells in the skin or interfere with the epithelial skin barrier, just as in thetwo other groups we studied. So, it seems that the absence of inflammation, inskin of patients with a severe blunt trauma to the upperleg inducing a femoralfracture, can be explained by the fact that the skin itself is intact and that there areno noxious substances present. Apparently the serious mechanical impact on theskin necessary to fracture the underlying long bone, does not result in anobservable damage at the skin level. That indeed the skin has the appearance ofan inflammatory response may be explained by the fact that damaged underlyingtissue such as subcutaneous adipose and muscle tissue may be activated. Thisinflamed tissue may lead to secondary endothelial activation (as observed by E-selectin expression), edema formation and subsequent swelling of the skin.
In summary, we have shown that although all biopsies were taken fromskin showing general clinical features of inflammation, the underlying mechanismsof inflammation differ. First, incision of the skin leads to a limited form ofinflammation, characterized by recruitment of granulocytes paralleled by E-selectin expression. Second, infection resulted in a pronounced inflammatoryresponse with granulocyte, monocyte /macrophage and T cell recruitment,increased E-selectin, ICAM-1, VCAM-1 expression and markedly changed

Chapter 4
72
cytokine expression. Last, mechanical injury without disruption of the epithelialbarrier does not show any signs of a local inflammatory response on the cellularlevel.

Different inflammatory responses in human skin
73
References
1. Clark, R. A. Basics of Cutaneous Wound Repair. J.Dermatol.Surg.Oncol. 1993;19(8):693-706.
2. Martin, P. Wound Healing--Aiming for Perfect Skin Regeneration. Science 4-4-1997;276(5309):75-81.
3. Singer, A. J. and Clark, R. A. Cutaneous Wound Healing. N.Engl.J.Med. 2-9-1999;341(10):738-46.
4. Carlos, T. M. and Harlan, J. M. Leukocyte-Endothelial Adhesion Molecules. Blood 1-10-1994;84(7):2068-101.
5. Ebnet, K. and Vestweber, D. Molecular Mechanisms That Control Leukocyte Extravasation: theSelectins and the Chemokines. Histochem.Cell Biol. 1999;112(1):1-23.
6. Adams, D. H. and Lloyd, A. R. Chemokines: Leucocyte Recruitment and Activation Cytokines.Lancet 15-2-1997;349(9050):490-5.
7. Pober, J. S. and Cotran, R. S. Cytokines and Endothelial Cell Biology. Physiol.Rev.1990;70(2):427-51.
8. Silber, A., Newman, W., Reimann, K. A., Hendricks, E., Walsh, D., and Ringler, D. J. KineticExpression of Endothelial Adhesion Molecules and Relationship to Leukocyte Recruitment inTwo Cutaneous Models of Inflammation. Lab.Invest. 1994;70(2):163-75.
9. Kobold, A. C., van-Wijk, R. T., Franssen, C. F., Molema, G., Kallenberg, C. G., and Tervaert, J.W. In Vitro Up-Regulation of E-Selectin and Induction of Interleukin-6 in Endothelial Cells byAutoantibodies in Wegener's Granulomatosis and Microscopic Polyangiitis. Clin.Exp.Rheumatol.1999;17(4):433-40.
10. Ross, R., Raines, E. W., and Bowen, Pope DF. The Biology of Platelet-Derived Growth Factor.Cell 18-7-1986;46(2):155-69.
11. Engelhardt, E., Toksoy, A., Goebeler, M., Debus, S., Brocker, E. B., and Gillitzer, R. ChemokinesIL-8, GROalpha, MCP-1, IP-10, and Mig Are Sequentially and Differentially Expressed DuringPhase-Specific Infiltration of Leukocyte Subsets in Human Wound Healing. Am.J.Pathol.1998;153(6):1849-60.
12. van der Laan, N., de Leij, L.F.M.H., ten Duis, H. J. Local Cellular Inflammation as a Result ofElective Standardized Vascular Surgery. Acta Histochemica 2001;103(2):139-149.
13. Orteu, C. H., Poulter, L. W., Rustin, M. H., Sabin, C. A., Salmon, M., and Akbar, A. N. TheRole of Apoptosis in the Resolution of T Cell-Mediated Cutaneous Inflammation. J.Immunol. 15-8-1998;161(4):1619-29.
14. Lundberg, I., Ulfgren, A. K., Nyberg, P., Andersson, U., and Klareskog, L. Cytokine Productionin Muscle Tissue of Patients With Idiopathic Inflammatory Myopathies. Arthritis Rheum.1997;40(5):865-74.
15. Sticherling, M., Bornscheuer, E., Schroder, J. M., and Christophers, E. Localization ofNeutrophil-Activating Peptide-1/Interleukin-8-Immunoreactivity in Normal and Psoriatic Skin.J.Invest.Dermatol. 1991;96(1):26-30.

Chapter 4
74
16. Sticherling, M., Bornscheuer, E., Schroder, J. M., and Christophers, E. ImmunohistochemicalStudies on NAP-1/IL-8 in Contact Eczema and Atopic Dermatitis. Arch.Dermatol.Res.1992;284(2):82-5.
17. Hermes, B., Prochazka, A. K., Haas, N., Jurgovsky, K., Sticherling, M., and Henz, B. M.Upregulation of TNF-Alpha and IL-3 Expression in Lesional and Uninvolved Skin in DifferentTypes of Urticaria. J.Allergy Clin.Immunol. 1999;103(2 Pt 1):307-14.
18. Rot, A. Neutrophil Attractant/Activation Protein-1 (Interleukin-8) Induces in Vitro NeutrophilMigration by Haptotactic Mechanism. Eur.J.Immunol. 1993;23(1):303-6.
19. Rothlein, R., Dustin, M. L., Marlin, S. D., and Springer, T. A. A Human Intercellular AdhesionMolecule (ICAM-1) Distinct From LFA-1. J.Immunol. 15-8-1986;137(4):1270-4.
20. Burns, A. R., Bowden, R. A., Abe, Y., Walker, D. C., Simon, S. I., Entman, M. L., and Smith, C.W. P-Selectin Mediates Neutrophil Adhesion to Endothelial Cell Borders. J.Leukoc.Biol.1999;65(3):299-306.
21. Hession, C., Osborn, L., Goff, D., Chi, Rosso G., Vassallo, C., Pasek, M., Pittack, C., Tizard, R.,Goelz, S., McCarthy, K., and et, al. Endothelial Leukocyte Adhesion Molecule 1: DirectExpression Cloning and Functional Interactions. Proc.Natl.Acad.Sci.U.S.A. 1990;87(5):1673-7.
22. Springer, T. A. and Lasky, L. A. Cell Adhesion. Sticky Sugars for Selectins [News]. Nature 17-1-1991;349(6306):196-7.
23. Elices, M. J., Osborn, L., Takada, Y., Crouse, C., Luhowskyj, S., Hemler, M. E., and Lobb, R. R.VCAM-1 on Activated Endothelium Interacts With the Leukocyte Integrin VLA-4 at a SiteDistinct From the VLA-4/Fibronectin Binding Site. Cell 23-2-1990;60(4):577-84.
24. Carlos, T., Kovach, N., Schwartz, B., Rosa, M., Newman, B., Wayner, E., Benjamin, C., Osborn,L., Lobb, R., and Harlan, J. Human Monocytes Bind to Two Cytokine-Induced AdhesiveLigands on Cultured Human Endothelial Cells: Endothelial-Leukocyte Adhesion Molecule-1 andVascular Cell Adhesion Molecule-1. Blood 15-5-1991;77(10):2266-71.
25. Dobrina, A., Menegazzi, R., Carlos, T. M., Nardon, E., Cramer, R., Zacchi, T., Harlan, J. M.,and Patriarca, P. Mechanisms of Eosinophil Adherence to Cultured Vascular Endothelial Cells.Eosinophils Bind to the Cytokine-Induced Ligand Vascular Cell Adhesion Molecule-1 Via theVery Late Activation Antigen-4 Integrin Receptor. J.Clin.Invest. 1991;88(1):20-6.
26. Catania, R. A., Schwacha, M. G., Cioffi, W. G., Bland, K. I., and Chaudry, I. H. Does UninjuredSkin Release Proinflammatory Cytokines Following Trauma and Hemorrhage? Arch.Surg.1999;134(4):368-73.
27. Garner, W. L., Rodriguez, J. L., Miller, C. G., Till, G. O., Rees, R. S., Smith, D. J., and Remick,D. G. Acute Skin Injury Releases Neutrophil Chemoattractants. Surgery 1994;116(1):42-8.
28. Reilly, D. M. and Green, M. R. Eicosanoid and Cytokine Levels in Acute Skin Irritation inResponse to Tape Stripping and Capsaicin. Acta Derm.Venereol. 1999;79(3):187-90.
29. Enk, A. H. and Katz, S. I. Early Events in the Induction Phase of Contact Sensitivity.J.Invest.Dermatol. 1992;99(5):39S-41S.

Different inflammatory responses in human skin
75
30. Boehm, K. D., Yun, J. K., Strohl, K. P., Trefzer, U., Haffner, A., and Elmets, C. A. In SituChanges in the Relative Abundance of Human Epidermal Cytokine Messenger RNA LevelsFollowing Exposure to the Poison Ivy/Oak Contact Allergen Urushiol. Exp.Dermatol.1996;5(3):150-60.

Chapter 4
76

Chapter V
Is human skin activated by blunt trauma?
Namkje van der Laan 1
Agnes Lesman 2
Marja van Luyn PhD 2
Lou de Leij PhD 2
Henk Jan ten Duis MD, PhD 1
1 Department of SurgeryUniversity Hospital GroningenThe Netherlands
2 Department of Pathology Laboratory medicine, section Medical BiologyUniversity Hospital GroningenThe Netherlands
Submitted for publication

Chapter 5
78
Summary
Local activation at the tissue level can initiate the onset of a systemicinflammatory response. Skin surrounding a long bone fracture may be damagedor activated shortly after the blunt trauma and contribute to the onset of systemicinflammation.
Trauma patients with at least one femoral fracture were studied. Skinsurrounding the fracture was compared with remote and normal skin. Biopsieswere analyzed using immunohistochemistry, electron microscopy, ELISA andRT-PCR.
Limited activation is observed in the form of E-selectin expression in somevessels of both skin near and remote from the fracture. In some cases, RT-PCRshowed expression of IL1β and IL6 mRNA and ELISA of TNFα and IL6protein in skin taken from the site of the femoral fracture and, or remote skin.Electron microscopy results confirmed that there is a large variation in activationstate of endothelial cells present in the different biopsies.
We conclude that human skin is not directly activated as a result of afemoral fracture. Local inflammation in skin as result of blunt trauma is limitedand does not contribute to a systemic inflammatory response in trauma patients.

Is human skin activated by blunt trauma?
79
Introduction
Severe injuries, like long bone fractures or burns and infections can all leadto a systemic inflammatory response syndrome, in some situations resulting in anunregulated systemic response which is called multiple organ dysfunctionsyndrome (MODS). There are different hypotheses about the origin of MODS,like the macrophage, microcirculatory and gut hypothesis (1;2). Thesehypotheses are partly overlapping and have general features. In all these theoriescytokines are thought to play a major role as they are known to be involved inresponse to injury in general (3). Therefore, various aspects of cytokineregulation e.g. expression of cytokines and related markers in the circulation havebeen studied extensively. There are conflicting results about TNFα and IL1βlevels in the circulation of trauma patients, but increased IL6 levels have beenreported several times, within hours after the accident (4-13). Also expression ofcytokine receptors, soluble adhesion molecules and acute phase proteins havebeen found to be elevated in blood of trauma patients (14-24). Although manydata concerning circulation markers in relation to MODS have been obtained,interpretation of these data remain difficult. High IL6 levels in the circulationappear to correlate e.g. with patients who are at risk to develop MODS, but it isstill unknown what initiates the IL6 production (25). Cytokines are locallyproduced and production is related to the degree of tissue damage (26-29).Therefore, production of cytokines at the tissue level seems to have an importantcontribution to the onset of the inflammatory response.
For a good interpretation of data, it is important to know what underliesthe increased cytokine levels in the circulation. We hypothesize that skin might bedamaged as a result of the mechanical impact necessary to fracture the underlyingbone, produce cytokines and contribute to the onset of a systemic inflammatoryresponse. Skin is a strong immunomodulator, containing many cells that arecapable of producing cytokines: keratinocytes, Langerhans cells, mast cells,fibroblasts, endothelial cells and monocytes (30-33). It is known that cytokineproduction locally in the skin can contribute to systemic levels (34-36).Therefore, early local inflammation in human skin as a result of “standardized”mechanical injury, a femoral fracture in young adolescent patients, was studied.Biopsies of skin surrounding the fracture were compared with remote skin andwith normal skin. Expression of pro-inflammatory cytokines was analyzed usingimmunohistochemistry, ELISA and RT-PCR. Furthermore, number anddistribution of cells and expression of adhesion molecules was studied. Byelectron microscopy, morphology and activation state of cells, especially ofendothelial cells, in the different skin biopsies was compared.

Chapter 5
80
Material and methods
Patients and skin biopsies
Eight patients (6 male, 2 female) with a medium age of 31 years (range 21-45) were included in this study. All patients had multiple injuries, including at leastone femoral fracture. After diagnostic procedures, patients underwent immediate(<12 hours) stabilization of their long bone fractures. The femoral fractures weretreated by closed reduction and intramedullary nail osteosynthesis. During thesurgical procedure, two skin biopsies were taken (as indicated in figure 1). Theskin biopsy (A), considered to be activated skin was taken near the site of thefemoral fracture at one of the places where the femoral nail was locked. Theremote skin biopsy (B), was taken from the upper hip region, the introductionplace of the intramedullary nail and served as an internal control.
Figure 1. Skin considered to be activated (A) was taken near the site of the femoral fracture, wherethe femoral nail was locked. The remote skin biopsy (B) was taken at the place where the femoralnail was introduced.
Biopsies were taken directly at first incision to exclude the effect of thesurgical procedure itself (disruption of the epithelial barrier) (37). Mean timebetween accident and biopsy was 6.5 hours, range 3.5-12 hours. As a control,skin biopsies were taken from eight healthy patients undergoing elective surgery.Here, first biopsy taken at the start of surgery was considered to representnormal skin.
Biopsies were immediately snap frozen in liquid nitrogen and stored at -80°C until use for immunohistochemistry and RT-PCR. For TEM, biopsies wereimmersion fixed in 2% (v/v) glutaraldehyde in Phosphate Buffered Saline (PBS).
Written informed consent was given and this study was approved by thelocal ethics committee (MEC 99/04/064).

Is human skin activated by blunt trauma?
81
Immunohistochemistry
For immunohistochemistry, 6 µm sections of human skin were cut, airdried and fixed for 10 minutes with acetone. Sections were incubated for onehour with the appropriate concentrations of antibodies diluted in 0,01M PBS(Table 1). After washing with PBS for 5 minutes, sections were incubated for 30minutes with horseradish peroxidase rabbit anti-mouse conjugate (RαM-PO,P260, Dako, Glostrup, Denmark) at a 1:40 dilution in PBS supplemented with 1%normal human serum. After washing with PBS, peroxidase reactivity wasvisualized using amino-ethylcarbazole (AEC, Sigma, St.Louis, MO, USA) as asubstrate.
Table 1: Antibodies used for immunohistochemistryAntibody Antigen Source Used dilutionNA1/34 CD1a Dako, Glostrup, Denmark 1:100WT32 CD3 Gift of W.Tax SupernatantMy4 CD14 Coulter, Hialeah, Fla., USA 1:405D2 CD16 CLB, Amsterdam, The Netherlands SupernatantCLB-B13.9 CD66b CLB 1:400EBM-1 CD68 Dako, Glostrup, Denmark 1:40S12(C50) P-selectin Centocor, Malvern, PA., USA 1:4000H18/7 acb E-selectin Gift of M.A. Gimbrone SupernatantHu 5/3-2.1 ICAM-1 Gift of M.A. Gimbrone SupernatantE 1/6 aa2 VCAM-1 Gift of M.A. Gimbrone Supernatant1277-89-71277-82-291279-143-4
Interleukin 1α Gift of H. Towbin 10 µg/ml
4H31 TNFα Gift of W. Buurman 2 µg/ml35G10F3 TNFα Genzyme, Cambridge, MA., USA 2 µg/ml1618-01 Interleukin 6 Genzyme 25 µg/ml52E8 Interleukin 8 Gift of M. Sticherling Supernatant
1:40
Sections were counterstained with hematoxylin and mounted in Kaiser’sglycerin. As a control, the first antibody was omitted or an isotype matched,irrelevant antibody was used. In both cases no staining was observed in humanskin cryostat sections (Fig.2 a).

Chapter 5
82
Transmission Electron Microscopy
After at least 24 hours of fixation at 4°C in 2% glutaraldehyde, skinbiopsies were cut into pieces, post fixed in 1% OsO4 for 1 hour, dehydratedthrough a series of ethanol and embedded in Epon 812. For Light Microscopy(LM) overview and Transmission Electron Microscopy (TEM), 1 µm sectionswere stained with toluidine blue. By LM vascularized areas, just under theepidermis, containing endothelial cells, were selected. Ultra thin sections (80 nm)of these areas were cut and stained with uranyl acetate and lead citrate. Sampleswere examined using a Philips EM 201 electron microscope at 60 kV.
ELISA
The TNFα and IL6 concentrations in the supernatant of skin biopsies offour patients were measured in an ELISA. Therefore, skin biopsies were weighed(30-100 mg), cut and dissolved (5 µl/mg) in PBS containing 1% Tween-20(Sigma) and 1% human serum albumine (CLB, Amsterdam, The Netherlands).Skin was repeatedly frozen in liquid nitrogen and thawed at 37°C for 5 times.Samples were centrifuged for 20 minutes at 13000 rpm at 4°C, collected andstored at -80°C until measurement. The presence of TNFα in the supernatantwas established using a sandwich ELISA as described previously (38). Briefly,anti TNFα 1:1000 (MAB610, R&D Systems, Abingdon, UK) was used as thefirst capture antibody and the biotin labeled goat anti-human TNFα (AB-210-NA,R&D Systems) as the second capture antibody. To detect IL6, anti-IL6 1:1000(CLB.MIL6/16, CLB) was used as the first capture antibody and the biotinlabeled goat anti-human IL6 (CLB.SIL6-D, CLB) as the second captureantibody. Recombinant human TNFα (Boehringer, Ingelheim, Germany) orhuman IL6 (206-IL-050, R&D Systems) served as a standard.
RT-PCR
Total RNA was isolated from 10-15 slices of 30 µm from skin biopsies offive patients, using guanidine thiocyanate as described before (39). RNA wasresuspended in diethylpyrocarbonate (DEPC) treated water and RNAconcentration was determined by spectroscopy at 260 nm. First strand cDNAwas prepared from 2 µg RNA using reverse transcriptase (Gibco-BRL),hexameer primers and 5 mM of each of the four dNTPs (Gibco-BRL, NY, USA)in a total volume of 50 µl. After reverse transcription, amplification was carriedout by PCR using 10 µl of cDNA. Each PCR reaction mixture contained 1 unitTaq polymerase (Gibco-BRL) and primers specific for β2- microglobulin,

Is human skin activated by blunt trauma?
83
TNFα, IL1β and IL6 (see Table 2). Amplification cycles were 1 min at 94°C, 1min at 57°C and 1 min at 72 °C during 35 cycles. β2-microglobulin PCRproducts of each sample were analyzed after 18 and 35 cycles to compareintensity of the gel bands, to make sure that the same amounts of cDNA wereused. Furthermore, β2-microglobulin primers were designed to distinguishbetween genomic and cDNA by length of the PCR product. The PCR productswere analyzed for the presence or absence of cytokine gene expression on a 1,5% agarose gel. As a positive control for the cytokine RT-PCR, RNA wasisolated of LPS stimulated monocytes.
Table 2:. Primer sequence and sizes of the resulting PCR productsAmplicon Primers Product size
β2-microglobulin
5’-CCAGCAGAGAATGGAAAGTC-3’5’-GATGCTGCTTACATGTCTCG-3’
cDNA 268Genomic DNA 900
TNFα 5’-TACAGCTTTGATCCCTGACATCT-3’5’-GTAGGCCGATTACAGACAACT-3’
509
IL-1β 5’-ATGTACCAGTTGGGGAACTG-3’5’-GGATATGGAGCAACAAGTGG-3’
263
IL6 5’-TCAATGAGGAGACTTGCCTG- 3’5’-GATGAGTTGTCATGTCCTGC -3’
260

Chapter 5
84
Results
Immunohistochemistry
Skin taken at the site of a femoral fracture show no differences in numberor distribution of any of the studied cells compared to remote and normal skin.Langerhans cells (CD1a) are found mainly in the epidermis and few positivescattered cells are present in the dermis. T cell (CD3) and monocyte,macrophage like cells (CD14, CD68) are solely observed in the dermal layer. Thefew observed T cells are found as clusters, whereas the monocyte, macrophagesare present scattered throughout the dermis. Granulocytes (CD16, CD66b) arenot present in any of the studied skin biopsies (Fig.2 b). Toluidine bluehistostaining confirms the immunohistochemical data: number and type of cells inthe different skin biopsies are comparable.
In five out of eight patients, E-selectin expression is induced: once in skinnear the fracture, three times only in remote skin and once in skin of both places.E-selectin expression is found on endothelial cells in some, but not all of thevessels. In normal skin biopsies, E-selectin expression is not observed (Table 3,Fig. 2 c, d).
Figure 2. a) No staining using isotype control, b) Lack of granulocytes in skin taken from the site ofthe femoral fracture, c) Faint E-selectin expression in remote skin of a patient with a femoral fracture,d) The absence of E-selectin on endothelial cells in remote skin of a patient with a femoral fracture.
No differences in P-selectin, ICAM-1 and VCAM-1 expression in skinfrom the site of the femoral fracture compared to remote and normal skin isfound. P-selectin and ICAM-1 are constitutively expressed on endothelial cells ofnormal skin and expression is not increased in skin taken near the fracture and

Is human skin activated by blunt trauma?
85
remote skin. In none of the studied skin biopsies VCAM-1 expression isobserved.
Furthermore, there is not a visible increase in intensity of cytokineexpression between skin taken from the site of the femoral fracture, remote andnormal skin. Similar intensity of expression for TNFα, IL1α and IL8 is presentin all studied skin biopsies, whereas IL6 expression is not found in any of thestudied biopsies. Intracellular TNFα (Fig. 3 a, b) and IL1α expression isobserved in the different layers of the epidermis, with strongest expression instratum basale. In the dermal layer, vascular and perivascular, hair follicles andglands stain positive. IL8 is present in the suprabasal cell layers of the epidermisand in hair follicles in the dermis.
Figure 3. No differences is observed in intensity and distribution of TNFα expression between skintaken from a) the site of the femoral fracture and b) normal skin.
Transmission Electron MicroscopyEndothelial cells in the upper dermis, just beneath the epidermis are studied
in detail. In both skin biopsies taken of the leg of a patient with a femoralfracture, but also in normal skin, vessels with activated endothelial cells aresometimes found (Fig. 4 a, b, c). Characteristics of endothelial cell activation thatwere observed are: swollen endothelial cells, nuclei with a uniform less electrondense gray pattern as a result of the euchromatin in active uncoiled configurationand an increased numbers of vesicles, mitochondria and Weibel Palade bodies inthe cytoplasm. There is a large variation in the presence of these characteristics inthe different skin biopsies, but they were found in all studied skin biopsies,including the normal tissue. Furthermore, electron microscopy confirmed theimmunohistochemical data since no cellular infiltrates such as granulocytes orother signs of cellular inflammation are observed.

Chapter 5
86
Figure 4. Transmission electron microscopy of endothelialcells from a) normal skin: in this case the nucleus is dark as aresult of many heterochromatin, coiled in tight helices, noWeibel Palade bodies or vesicles are observed, b) skin takenremote and c) near the fracture showing endothelial activationsince the nucleus has a uniform less gray pattern and manyWeibel Palade bodies – arrow- and vesicles –arrowhead-are present in the cytoplasm (original magnification a, c2400x, b 1600x).
ELISA
In three of the four studied patients either TNFα, IL6 or both is observedin supernatant of skin biopsies (Table 3). In normal skin supernatant, TNFα andIL6 levels are below the detection limit (< 20 pg/ml). In one patient, IL6 is foundin supernatant of skin taken from the site of the femoral fracture. Remote skin ofanother patient contains TNFα and in the third patient TNFα and IL6 is presentin both skin taken from the site of the femoral fracture and in remote skin.

Is human skin activated by blunt trauma?
87
Table 3: Partial list of resultsSkin E-selectin ELISA
(TNFα, IL6)RT-PCR
(TNFα, IL1β, IL6)Normal -(8 x)1 -(4 x) -(3 x)Near 2
Remote 3+-
++
ND4
NDNearRemote
-+
-+
NDND
NearRemote
-+
--
+-
NearRemote
--
+-
++
NearRemote
--
NDND
+-
NearRemote
++
NDND
+-
NearRemote
-+
NDND
-+
NearRemote
--
NDND
NDND
1 - number of biopsies that was studied2 - skin biopsy from place indicated in figure1A3 - skin biopsy from place indicated in figure1B4 - not done
RT-PCR
IL1β and, or IL6 mRNA expression is present in some of the skin biopsiestaken from the site of the femoral fracture and remote skin. Expression of IL1βand IL6 is not observed in normal skin, whereas TNFα expression is notobserved in any of the studied skin biopsies (Fig. 5). Also, no clear upregulationof cytokine mRNA is found in skin taken from the site of the femoral fracturecompared to remote skin. All patients show expression of at least one cytokine inone of the biopsies (Table 3). The same amount of isolated RNA is used for theRT-PCR and the intensity of β2-microglobulin DNA bands after 18 cycles ofPCR confirmed this. After PCR, only a 268 bp band is observed, which meansthat no genomic DNA was isolated during RNA isolation.

Chapter 5
88
Figure 5. A 1,5 % agarose gel showing the products of the RT-PCR reactions of RNA isolatedfrom skin biopsies of patient with a femoral fracture for a) β2 –microblobulin, b) TNFα, c) IL1βand d) IL6. M is marker (100 bp ladder), C is positive control, N is near skin biopsy taken fromplace indicated in Fig.1A, R is remote biopsy taken from place indicated in Fig.1B

Is human skin activated by blunt trauma?
89
Discussion
Multiple Organ Dysfunction Syndrome (MODS) is a serious complicationin severely injured patients. Many studies have shown that MODS is the result ofan unregulated systemic inflammatory response (2;40;41). High levels of IL6correlate with patients who develop complications or are at risk to developMODS. Furthermore, it has been shown that strongly elevated systemic IL6levels can already be measured at arrival of the patient in the hospital (4;6;8;9;11-13).The question arises, where this increased IL6 and the unregulated systemicresponse originates from. A possible explanation might be found in the fact thatlocal activation at the tissue level can initiate the onset of a systemic inflammatoryresponse. Therefore, possible early local inflammation in skin shortly aftermechanical injury, i.e. in patients with a femoral fracture, without disruption of theepithelial skin barrier, was studied and compared with normal skin.
We observed limited local inflammation in human skin as a result of themechanical injury. Not only skin surrounding the fracture, but also remote skinfrom the same leg showed limited activation compared to normal skin. E-selectinexpression was found on endothelial cells in some skin biopsies of patients witha femoral fracture. Increased cytokine protein levels and gene expression weredetected by ELISA and RT-PCR in some of the skin biopsies. None of thisactivation was found in normal human skin.
With respect to the blood vessels, E-selectin was expressed by someendothelial cells in skin biopsies of five patients. The absence of E-selectin inskin of the other three patients might be explained by the fact that a limitednumber of vessels were found positive. Sections of a certain skin biopsy can bychange only reveal E-selectin negative vessels. That there is indeed variation inactivation state of endothelial cells is confirmed by the electron microscopyresults. Characteristics of activated endothelial cells were observed in somevessels in all studied skin biopsies, also in normal skin. Since there is no clearincreased endothelial activation in skin covering the fracture compared to remoteand normal skin, we can conclude that the fracture itself does not enhanceendothelial cell activation.
In accordance with these results is the observation that the fracture doesnot induce local cellular inflammation, since we were not able to show localactivation in skin using various markers for immunohistochemistry. Number anddistribution of immune competent cells, P-selectin, ICAM-1 and VCAM-1expression were all similar to remote and normal skin. The absence of aninflammatory response locally, as characterized by cellular infiltrates, might beexplained by the fact that the skin itself -the epithelial barrier- is intact and thatthere are no noxious substances or bacteria present. Apparently the mechanicalimpact on the skin necessary to fracture the underlying bone does not result inobservable damage and corresponding inflammation.

Chapter 5
90
Furthermore, by immunohistochemistry, a similar intensity of TNFα,IL1α, IL6 and IL8 expression in the different skin cryostat sections wasobserved compared to normal skin. Additionally, ELISA experiments confirmedthat there was no clear increase in cytokine protein production. Only a slightincrease in TNFα and, or IL6, compared to normal skin, was detected in threepatients. This may indicate that the local increase in cytokine levels is too low todetect by immunohistochemistry. Increased cytokine gene expression as foundwith RT-PCR was present in both skin taken near the fracture and in remote skin.There was not always an increased cytokine gene expression in near and remotebiopsy of one patient, which might be explained by the fact that RNA wasisolated from skin sections, which may vary in cellular composition. Our resultsextend the findings of Catania et al.(42) who found cytokine gene expression ininjured and uninjured skin of mice after a closed tibial fracture. The mechanismsand cell types that are responsible for this increased cytokine production areunknown. Ischemia, hypoperfusion or hypoxia in the leg as a result of thefemoral fracture may activate endothelial cells not only in skin surrounding thefracture, but also further away from the fracture. This is in agreement with ourfindings that E-selectin expression, IL6 and TNFα protein and IL1β and IL6mRNA were found in both local and remote skin biopsies. So, in contrast towhat we expected, no differences in activation between skin surrounding thefracture and remote skin were found, but skin biopsies on both, i.e. local andremote, places were found to be slightly activated, as a result of mechanicalinjury compared to normal skin. Although ELISA and RT-PCR have shown aslight increase in cytokine levels, it is clear that cells present in the skinsurrounding the fracture do not produce remarkable amounts of cytokines, whichis confirmed by the immunohistochemical data.
In addition, no relation was observed between the amount of tissuedamage (ISS scores) or time of biopsy with respectively the cytokine levels,endothelial activation or the physiologic response of the different patients.
We conclude that human skin is not directly activated as a result of afemoral fracture. Local inflammation in human skin as a result of blunt trauma islimited and does probably not contribute to a systemic inflammatory response.Other soft tissues, like muscle or fat may be important in triggering the systemicresponse, but also mechanisms as described in the macrophage, microcirculatoryor gut hypothesis may play a role.

Is human skin activated by blunt trauma?
91
References
1. Deitch, E. A. Multiple Organ Failure. Pathophysiology and Potential Future Therapy. Ann.Surg.1992;216(2):117-34.
2. Livingston, D. H. and Deitch, E. A. Multiple Organ Failure: a Common Problem in SurgicalIntensive Care Unit Patients. Ann.Med. 1995;27(1):13-20.
3. Bellomo, R. The Cytokine Network in the Critically Ill. Anaesth.Intensive Care 1992;20(3):288-302.
4. Pullicino, E. A., Carli, F., Poole, S., Rafferty, B., Malik, S. T., and Elia, M. The RelationshipBetween the Circulating Concentrations of Interleukin 6 (IL-6), Tumor Necrosis Factor (TNF)and the Acute Phase Response to Elective Surgery and Accidental Injury. Lymphokine Res.1990;9(2):231-8.
5. Rabinovici, R., John, R., Esser, K. M., Vernick, J., and Feuerstein, G. Serum Tumor NecrosisFactor-Alpha Profile in Trauma Patients. J.Trauma. 1993;35(5):698-702.
6. Hoch, R. C., Rodriguez, R., Manning, T., Bishop, M., Mead, P., Shoemaker, W. C., andAbraham, E. Effects of Accidental Trauma on Cytokine and Endotoxin Production. Crit.CareMed. 1993;21(6):839-45.
7. Cipolle, M. D., Pasquale, M. D., Shearer, J., Caldwell, M., and Cerra, F. Blunt Injury AugmentsInterleukin-6 but Not Tumor Necrosis Factor in Isolated, Perfused Rat Hindlimbs. J.Trauma.1994;37(1):91-8.
8. Meade, P., Shoemaker, W. C., Donnelly, T. J., Abraham, E., Jagels, M. A., Cryer, H. G., Hugli,T. E., Bishop, M. H., and Wo, C. C. Temporal Patterns of Hemodynamics, Oxygen Transport,Cytokine Activity, and Complement Activity in the Development of Adult Respiratory DistressSyndrome After Severe Injury. J.Trauma. 1994;36(5):651-7.
9. Svoboda, P., Kantorova, I., and Ochmann, J. Dynamics of Interleukin 1, 2, and 6 and TumorNecrosis Factor Alpha in Multiple Trauma Patients. J.Trauma. 1994;36(3):336-40.
10. Keel, M., Ecknauer, E., Stocker, R., Ungethum, U., Steckholzer, U., Kenney, J., Gallati, H.,Trentz, O., and Ertel, W. Different Pattern of Local and Systemic Release of Proinflammatoryand Anti-Inflammatory Mediators in Severely Injured Patients With Chest Trauma. J.Trauma.1996;40(6):907-12.
11. Martin, C., Boisson, C., Haccoun, M., Thomachot, L., and Mege, J. L. Patterns of CytokineEvolution (Tumor Necrosis Factor-Alpha and Interleukin-6) After Septic Shock, HemorrhagicShock, and Severe Trauma. Crit Care Med. 1997;25(11):1813-9.
12. Nast, Kolb D., Waydhas, C., Gippner, Steppert C., Schneider, I., Trupka, A., Ruchholtz, S., Zettl,R., Schweiberer, L., and Jochum, M. Indicators of the Posttraumatic Inflammatory ResponseCorrelate With Organ Failure in Patients With Multiple Injuries. J.Trauma. 1997;42(3):446-54.
13. Gebhard, F., Pfetsch, H., Steinbach, G., Strecker, W., Kinzl, L., and Bruckner, U. B. IsInterleukin 6 an Early Marker of Injury Severity Following Major Trauma in Humans?Arch.Surg. 2000;135(3):291-5.

Chapter 5
92
14. Tan, L. R., Waxman, K., Scannell, G., Ioli, G., and Granger, G. A. Trauma Causes Early Releaseof Soluble Receptors for Tumor Necrosis Factor. J.Trauma 1993;34(5):634-8.
15. Cinat, M., Waxman, K., Vaziri, N. D., Daughters, K., Yousefi, S., Scannell, G., and Tominaga,G. T. Soluble Cytokine Receptors and Receptor Antagonists Are Sequentially Released AfterTrauma. J.Trauma 1995;39(1):112-8.
16. Law, M. M., Cryer, H. G., and Abraham, E. Elevated Levels of Soluble ICAM-1 Correlate Withthe Development of Multiple Organ Failure in Severely Injured Trauma Patients. J.Trauma.1994;37(1):100-9.
17. Simons, R. K., Hoyt, D. B., Winchell, R. J., Rose, R. M., and Holbrook, T. Elevated SelectinLevels After Severe Trauma: a Marker for Sepsis and Organ Failure and a Potential Target forImmunomodulatory Therapy. J.Trauma 1996;41(4):653-62.
18. Giannoudis, P. V., Smith, R. M., Banks, R. E., Windsor, A. C., Dickson, R. A., and Guillou, P. J.Stimulation of Inflammatory Markers After Blunt Trauma. Br.J.Surg. 1998;85(7):986-90.
19. Seekamp, A., Jochum, M., Ziegler, M., van-Griensven, M., Martin, M., and Regel, G. Cytokinesand Adhesion Molecules in Elective and Accidental Trauma-Related Ischemia/Reperfusion.J.Trauma. 1998;44(5):874-82.
20. Gosling, P. and Dickson, G. R. Serum C-Reactive Protein in Patients With Serious Trauma.Injury 1992;23(7):483-6.
21. Ensenauer, R., Puttmann, M., Quintel, M., Kattermann, R., and Aufenanger, J. Comparison ofSerum Phospholipase A2, Polymorphonuclear Granulocyte Elastase, C-Reactive Protein andSerum Amyloid A With the APACHE II Score in the Prognosis of Multiple Injured Patients.Clin.Investig. 1994;72(11):843-9.
22. Petersen, S. R., Jeevanandam, M., Shahbazian, L. M., and Holaday, N. J. Reprioritization ofLiver Protein Synthesis Resulting From Recombinant Human Growth Hormone Supplementationin Parenterally Fed Trauma Patients: the Effect of Growth Hormone on the Acute-PhaseResponse. J.Trauma 1997;42(6):987-95.
23. Mimoz, O., Benoist, J. F., Edouard, A. R., Assicot, M., Bohuon, C., and Samii, K. Procalcitoninand C-Reactive Protein During the Early Posttraumatic Systemic Inflammatory ResponseSyndrome. Intensive.Care Med. 1998;24(2):185-8.
24. Giannoudis, P. V., Smith, M. R., Evans, R. T., Bellamy, M. C., and Guillou, P. J. Serum CRP andIL-6 Levels After Trauma. Not Predictive of Septic Complications in 31 Patients. ActaOrthop.Scand. 1998;69(2):184-8.
25. Bone, R. C. Toward a Theory Regarding the Pathogenesis of the Systemic InflammatoryResponse Syndrome: What We Do and Do Not Know About Cytokine Regulation. Crit.CareMed. 1996;24(1):163-72.
26. Bitterman, H., Kinarty, A., Lazarovich, H., and Lahat, N. Acute Release of Cytokines IsProportional to Tissue Injury Induced by Surgical Trauma and Shock in Rats. J.Clin.Immunol.1991;11(4):184-92.
27. Baigrie, R. J., Lamont, P. M., Kwiatkowski, D., Dallman, M. J., and Morris, P. J. SystemicCytokine Response After Major Surgery. Br.J.Surg. 1992;79(8):757-60.

Is human skin activated by blunt trauma?
93
28. Biffl, W. L., Moore, E. E., Moore, F. A., and Peterson, V. M. Interleukin-6 in the InjuredPatient. Marker of Injury or Mediator of Inflammation? Ann.Surg. 1996;224(5):647-64.
29. Kolvenbach, R., Deling, O., Schwierz, E., and Landers, B. Reducing the Operative Trauma inAortoiliac Reconstructions--a Prospective Study to Evaluate the Role of Video-AssistedVascular Surgery. Eur.J.Vasc.Endovasc.Surg. 1998;15(6):483-8.
30. Kupper, T. S. Immune and Inflammatory Processes in Cutaneous Tissues. Mechanisms andSpeculations. J.Clin.Invest. 1990;86(6):1783-9.
31. Matsue, H., Cruz-PD, Jr, Bergstresser, P. R., and Takashima, A. Cytokine Expression byEpidermal Cell Subpopulations. J.Invest.Dermatol. 1992;99(5):42S-5S.
32. Schroder, J. M. Cytokine Networks in the Skin. J.Invest.Dermatol. 1995;105(1 Suppl):20S-4S.
33. Bos, J. D. The Skin As an Organ of Immunity. Clin.Exp.Immunol. 1997;107 Suppl 1:3-5.
34. Urbanski, A., Schwarz, T., Neuner, P., Krutmann, J., Kirnbauer, R., Kock, A., and Luger, T. A.Ultraviolet Light Induces Increased Circulating Interleukin-6 in Humans. J.Invest.Dermatol.1990;94(6):808-11.
35. Rodriguez, J. L., Miller, C. G., Garner, W. L., Till, G. O., Guerrero, P., Moore, N. P., Corridore,M., Normolle, D. P., Smith, D. J., and Remick, D. G. Correlation of the Local and SystemicCytokine Response With Clinical Outcome Following Thermal Injury. J.Trauma. 1993;34(5):684-94.
36. Kawakami, M., Kaneko, N., Anada, H., Terai, C., and Okada, Y. Measurement of Interleukin-6,Interleukin-10, and Tumor Necrosis Factor-Alpha Levels in Tissues and Plasma After ThermalInjury in Mice. Surgery 1997;121(4):440-8.
37. van der Laan, N., de Leij, L. and ten Duis, HJ. Local cellular inflammation as a result of electivestandardized vascular surgery. Acta Histochemica.2001;103(2):139-49.
38. Kobold, A. C., van-Wijk, R. T., Franssen, C. F., Molema, G., Kallenberg, C. G., and Tervaert, J.W. In Vitro Up-Regulation of E-Selectin and Induction of Interleukin-6 in Endothelial Cells byAutoantibodies in Wegener's Granulomatosis and Microscopic Polyangiitis. Clin.Exp.Rheumatol.1999;17(4):433-40.
39. Chomczynski, P. and Sacchi, N. Single-Step Method of RNA Isolation by Acid GuanidiniumThiocyanate-Phenol-Chloroform Extraction. Anal.Biochem. 1987;162(1):156-9.
40. Bone, R. C. Immunologic Dissonance: a Continuing Evolution in Our Understanding of theSystemic Inflammatory Response Syndrome (SIRS) and the Multiple Organ DysfunctionSyndrome (MODS). Ann.Intern.Med. 15-10-1996;125(8):680-7.
41. Yao, Y. M., Redl, H., Bahrami, S., and Schlag, G. The Inflammatory Basis of Trauma/Shock-Associated Multiple Organ Failure. Inflamm.Res. 1998;47(5):201-10.
42. Catania, R. A., Schwacha, M. G., Cioffi, W. G., Bland, K. I., and Chaudry, I. H. Does UninjuredSkin Release Proinflammatory Cytokines Following Trauma and Hemorrhage? Arch.Surg.1999;134(4):368-73.

Chapter 5
94

Chapter VI
Production of pro-inflammatory cytokines by adipose tissueafter blunt trauma
Namkje van der Laan 1
Sandra Henkelman 2
Elinda Bruin-van Dijk 2
Herbert Roerdink MD 1
Lou de Leij PhD 2
Henk Jan ten Duis MD, PhD 1
1 Department of SurgeryUniversity Hospital GroningenThe Netherlands
2 Department of Pathology Laboratory Medicine, section Medical BiologyUniversity Hospital GroningenThe Netherlands
Submitted for publication

Chapter 6
96
Summary
Multiple organ dysfunction syndrome (MODS) is a major complicationafter trauma. MODS is an unregulated systemic inflammatory responsecharacterized by an excessive release of pro-inflammatory mediators. Localactivation or a spill-over from locally produced mediators can be important intriggering a systemic response. We hypothesize that the mechanical impactnecessary to fracture an underlying bone will lead to soft tissue damage, localinflammation and cytokine production that may contribute to the onset of asystemic response.
Local activation as a result of “standardized” mechanical injury, i.e. aclosed femoral fracture was studied in muscle and subcutaneous adipose tissueby immunohistochemistry, RT-PCR and ELISA. Systemic inflammation wasconfirmed by the detection of pro-inflammatory cytokines in the circulation usingELISA.
No inflammatory reaction or clear cytokine production is observed inmuscle biopsies taken from patients with a femoral fracture. Increased levels ofcytokines are found in adipose tissue taken near the fracture compared to remoteadipose tissue.
Adipose tissue is activated and produce cytokines as a result of a femoralfracture and may contribute to elevated IL6 levels or systemic inflammation afterblunt trauma.

Cytokine production after blunt trauma
97
Introduction
Multiple Organ Dysfunction Syndrome (MODS) is a major complicationafter trauma. MODS is an unregulated systemic inflammatory responsecharacterized by an excessive release of pro-inflammatory mediators such as anumber of cytokines and acute phase proteins (1-4).
Although it has been demonstrated that elevated levels of e.g. interleukin 6(IL6) are associated with an increased risk to develop MODS after trauma,mechanisms underlying this unregulated systemic response are still unclear (5;6).
Systemic inflammation after trauma appears to be initiated by a localinflammatory response which starts in the tissues where the initial damage ispresent. It is assumed that due to tissue damage the complement and coagulationcascade are activated and cytokines are produced (7;8). Since cytokineproduction appears to be related to the degree of tissue damage (9-12), localinflammation and production of cytokines in the tissues may be important ininitiating systemic inflammation. In case of massive tissue damage, an ongoinglocal activation and, or a spill-over from locally produced inflammatorymediators may induce an unregulated systemic response.
We hypothesize that the mechanical impact necessary to fracture anunderlying bone will lead to soft tissue damage, local inflammation and cytokineproduction that may contribute to the onset of a systemic response.
Therefore, local tissue activation as result of a “standardized” mechanicalinjury, i.e. a closed femoral fracture was studied. Since we have shown beforethat skin surrounding a fracture is not activated as a result of the injury, tissuesmore close to the fractured bone were studied: muscle and subcutaneous adiposetissue. In muscle, expression of pro-inflammatory cytokines was analyzed usingimmunohistochemistry and RT-PCR. Furthermore, number and distribution ofinfiltrating leukocytes and expression of adhesion molecules was studied. Inadipose tissue cytokine levels were determined by ELISA and RT-PCR.Systemic inflammation was confirmed by the detection of pro-inflammatorycytokines in the circulation using ELISA.

Chapter 6
98
Materials and methods
Patients
Consecutive patients, from June 2000 to April 2001, with at least oneclosed femoral fracture were included in this study. 12 patients (10 male, 2female), mean age 29 years (range 16-66) and mean injury severity score (ISS) 12(range 9-22) met the criteria of the study. After diagnostic procedures, patientsunderwent immediate (<12 hours) stabilization of their long bone fractures. Thefemoral fractures were treated by closed reduction and intramedullary nailosteosynthesis. In principle, two subcutaneous adipose and muscle biopsieswere taken during surgery. In case of open reduction, tissue taken at the site ofthe femoral fracture was considered to be activated. In case of closed reduction,the site where the femoral nail was locked near to the femoral fracture wassupposed to be activated. The remote biopsy was taken from the upper hipregion, the introduction place of the used intramedullary nail, and served as aninternal control. It was not always possible to obtain both muscle and adiposetissue, and from both places of one patient (Table 1).
Table 1: List showing which biopsies or samples were taken from each patientPatient Muscle Adipose Plasma
1 Near Near 2x2 Remote Remote -1
3 Near and remote Remote 2x4 Near Near -5 Near and remote Near and remote 2x6 Remote Near and remote 2x7 Near and remote Near and remote 2x8 - Near -9 - Near and remote -
10 Near and remote Near and remote 2x11 Near 2x Near and remote -12 Near and remote Near and remote -
1 – no biopsy or sample was taken
Biopsies were taken directly at first incision to exclude the effect of thesurgical procedure itself (13). Mean time between accident and biopsy was 6.5hours (range 4-11.5). Muscle and adipose biopsies were immediately snap frozenin liquid nitrogen and stored at -80°C until use for immunohistochemistry, ELISAand RT-PCR.

Cytokine production after blunt trauma
99
To study systemic inflammation, blood samples were taken from 6 patientson arrival at the hospital and at least one additional sample was taken within 48 hrafter the accident. As a control, plasma was taken from 3 healthy volunteers.Samples were centrifuged (2700 rpm at 4ºC for 10 min) and plasma was storedat -80ºC until analysis.
Written informed consent was given and this study was approved by thelocal ethics committee (METc 00/01/011).
Immunohistochemistry
For immunohistochemistry, 6 µm sections of human muscle were cut andair dried. Sections were fixated in 2% formaldehyde in 0,01M PhosphateBuffered Saline (PBS) for 20 minutes. After washing with PBS, sections wereincubated overnight with the appropriate concentrations of antibody (Table 2)diluted in PBS supplemented with 0,1% saponine (PBS/sap). After incubationwith the primary antibody, sections were washed in PBS/sap for 5 minutes. Next,endogenous peroxidase activity of the sections was blocked with 0,03% H202
dissolved in PBS, for 10 minutes. After additional washing with PBS/sap for 5minutes, sections were incubated for 30 minutes with horseradish peroxidaserabbit anti-mouse conjugate (RαM-PO, P260, Dako, Glostrup, Denmark) at a1:40 dilution in PBS/sap supplemented with 1% normal human serum. Fordetection of von Willebrand Factor, swine anti-rabbit conjugate 1:50 (SαR-PO,P213, Dako) was used. After washing with PBS, peroxidase reactivity wasvisualized using amino-ethylcarbazole (AEC, Sigma, St.Louis, MO, USA) as asubstrate. Sections were counterstained with hematoxylin and mounted inKaiser’s glycerin. As a control, the first antibody was omitted or an isotypematched, irrelevant antibody was used. In both cases no staining was observed inhuman muscle cryostat sections.
RT-PCR
Total RNA was isolated from 20-40 mg muscle (10 patients, Table 1) andadipose tissue (last 4 patients, Table 1), using guanidine thiocyanate as describedbefore (14). RNA was resuspended in diethylpyrocarbonate (DEPC) treatedwater and RNA concentration was determined by spectroscopy at 260 nm. Firststrand cDNA was prepared from 2 µg RNA using reverse transcriptase (Gibco-BRL), poly-T primers and 1 mM of each of the four dNTPs (Gibco-BRL) in atotal volume of 25 µl. After reverse transcription, amplification was carried outby PCR using 2 µl of cDNA for β2-microglobulin and 3 µl cDNA for thecytokines. Each PCR reaction mixture contained 0,5 unit Taq polymerase(Gibco-BRL) and primers specific for β2-microglobulin, TNFα, IL1β, IL6 or

Chapter 6
100
IL8 (see Table 3). Amplification cycles were 1 min at 94°C, 1 min at 57°C (60°Cfor TNFα) and 1 min at 72°C during 35 cycles. β2-microglobulin primers weredesigned to distinguish between genomic and cDNA by length of the PCRproduct. The PCR products were analyzed for the presence or absence ofcytokine gene expression on a 1,5 % agarose gel. As a positive control for thecytokine RT-PCR, RNA was isolated of LPS stimulated monocytes.
Table 2: Antibodies used for immunohistochemistryAntibody Antigen Source Used dilutionWT32 CD3 Gift of W.Tax SupernatantMy4 CD14 Coulter, Hialeah, Fla., USA 1:405D2 CD16 CLB, Amsterdam, The
NetherlandsSupernatant
CLB-B13.9 CD66b CLB 1:400EBM-1 CD68 Dako, Glostrup, Denmark 1:40JC/76A CD31 Dako 1:100Polyclonal Von Willebrand
FactorDako 1:500
S12(C50) P-selectin Centocor, Malvern, PA., USA 1:4000H18/7 acb E-selectin Gift of M.A. Gimbrone SupernatantHu 5/3-2.1 ICAM-1 Gift of M.A. Gimbrone SupernatantE 1/6 aa2 VCAM-1 Gift of M.A. Gimbrone Supernatant1277-89-71277-82-291279-143-4
Interleukin 1α Gift of H. Towbin 10 µg/ml
2D8 Interleukin 1β Immunokontact, Brussel, Belgium 1:2035G10F3 TNFα Genzyme, Cambridge, MA., USA 2 µg/mlIL-6-16 Interleukin 6 CLB 1:2052E8 Interleukin 8 Gift of M. Sticherling Supernatant
1:40
ELISA
The TNFα, IL6 and IL8 concentrations of plasma and supernatant ofsubcutaneous adipose (see Table 1) were measured in an ELISA. Therefore,adipose tissue was weighed (100 - 500 mg), cut and dissolved (2 µl/mg) in lysisbuffer (50 mM Tris/HCl, pH 7.4, 600 mM NaCl, 0.2% Triton-X-100). Proteaseinhibitor mix (P8340, Sigma) was added (5 µl/100 mg) and tissue was vortexedand shaked overnight at 4ºC. Samples were centrifuged for 20 minutes at 13000rpm at 4°C and supernatant was collected using a needle and stored at -80°Cuntil measurement. The TNFα, IL6 and IL8 levels of supernatant and plasma

Cytokine production after blunt trauma
101
samples were established using a sandwich ELISA as described previously (15).Briefly, anti-TNFα 1:500 (MAB610, R&D Systems, Abingdon, UK), anti-IL61:1000 (CLB.MIL6/16, CLB) or anti-IL8 1:1000 (MAB208, R&D Systems) wasused as the first capture antibody and the biotin labeled goat anti-human TNFα(AB-210-NA, R&D systems), anti-human IL6 (CLB.SIL6-D, CLB) or anti-human IL8 (AB-208-NA, R&D Systems) as the second capture antibody.Recombinant TNFα (Boehringer Ingelheim, Germany), IL6 (206-IL-050, R&DSystems) and IL8 (1588-00, Genzyme) served as standards.
Table 3: Primer sequences and sizes of the resulting PCR productsAmplicon Primers Product size
β2-microglobulin
5’-CCAGCAGAGAATGGAAAGTC-3’5’-GATGCTGCTTACATGTCTCG-3’
cDNA 268Genomic DNA 900
TNFα 5’-AAGAATTCAAACTGGGGCCT-3’5’-GAGGAAGGCCTAAGGTCCAC-3’
174
IL-1β 5’-ATGTACCAGTTGGGGAACTG-3’5’-GGATATGGAGCAACAAGTGG-3’
263
IL6 5’-TCAATGAGGAGACTTGCCTG- 3’5’-GATGAGTTGTCATGTCCTGC -3’
260
IL8 5’-TTGGCAGCCTTCCTGATT-3’5’-AACTTCTCCACAACCCTCTG-3’
247
Statistical analysis
Levels of TNFα, IL6 and IL8 in adipose tissue biopsies were evaluated bycomparing the median level of all near biopsies (n=12) with the median of allremote biopsies (n=10) for each cytokine. Differences between the groups wereanalyzed by the Mann-Whitney test.
Increase in TNFα, IL6 or IL8 in the biopsy taken near compared to theremote biopsy within one patient was analyzed by the Wilcoxon signed rank test.

Chapter 6
102
Results
Muscle
Immunohistochemistry
No inflammatory reaction is observed in muscle biopsies taken frompatients with a femoral fracture. Sometimes bleeding and, or ruptured musclefibers are present in biopsies taken near the fracture, but no cellular infiltrates, noinduction of adhesion molecule expression nor induction of cytokines is found.Furthermore, there are no differences observed between muscle biopsies takenremote from or near the fracture.
Very few monocytes, macrophages (CD14, CD68 positive cells) andgranulocytes (CD16, CD66b positive cells) are detected in muscle biopsies ofboth places, whereas T cells (CD3 positive cells) are not found. Endothelial cellsare detected using CD31 and von Willebrand Factor. Many small capillaries andto a lesser extent bigger vessels are found located between the muscle cells. Thenumber of capillaries and vessels varied between different patients but is notrelated to the place where the biopsy was taken. In both remote and near musclebiopsies P-selectin and ICAM-1 expression is found in some, but not all of thevessels. E-selectin and VCAM-1 expression is not detected in any of the studiedbiopsies. Endothelial cells and a varying number of muscle cells in both remoteand near muscle biopsies express TNFα and IL1α. In general more cells expressTNFα than IL1α, but there is no correlation between number of cells that arepositive for TNFα or IL1α and the place where the biopsy was taken.Furthermore, the intensity of TNFα and IL1α expression is similar in remote andnear muscle biopsies (Figure 1). IL1β, IL6 and IL8 expression is not detected inany of the studied muscle biopsies.

Cytokine production after blunt trauma
103
Figure 1. Intensity of TNFα expression in capillaries and vessels is similar in both muscle taken a)near and b) remote from the femoral fracture. IL1α expression in muscle taken near the femoralfracture in c) capillaries and vessels, d) muscle cells.
RT-PCR
TNFα, IL1β, IL6 and IL8 mRNA expression is present in some but not allof the muscle biopsies, both remote from and near the fracture (Table 4). Thereis no clear upregulation of cytokine mRNA found in muscle taken from the siteof the femoral fracture compared to remote muscle, although biopsies taken nearthe fracture are more often positive than remote biopsies and intensity ofcytokine expression is in some cases higher near than remote from the fracture.Variation in expression levels of the cytokines is different between individualsand the intensity is low compared to β2-microglubulin expression. TNFα mRNAis detected in 15 out of 17 muscle biopsies , whereas IL1β mRNA is detected inonly 2 biopsies. IL6 mRNA expression is found in 8 and IL8 in 7 of the biopsies.Biopsies that are positive for IL1β mRNA are also IL6 and IL8 positive (seeTable 4).

Chapter 6
104
Table 4: List of RT-PCR results of muscleMuscle TNFα IL1β IL6 IL8
Near + 1 - 2 - +Remote + - - -
NearRemote
++
--
--
--
Near - - - +Near
Remote++
+-
++
++
Remote + - + -Near
Remote+-
--
-+
--
- ND3 ND ND ND- ND ND ND ND
NearRemote
++
--
++
--
NearNear
++
+-
++
++
NearRemote
++
--
--
+-
1 – positive PCR signal2 – no PCR signal3 – not done
Adipose tissue
Table 5: List of RT-PCR results of adipose tissueAdipose TNFα IL1β IL6 IL8
NearRemote
- 1
---
--
--
NearRemote
+ 2
-+-
+-
+-
NearRemote
++
-+
++
++
NearRemote
+-
--
+-
+-
1 – no PCR signal2 – positive PCR signal

Cytokine production after blunt trauma
105
RT-PCR
There is expression of TNFα, IL6 and IL8 mRNA in adipose tissue of 3of the 4 studied patients (Table 5) and adipose tissue taken near the fracture ismore often positive than remote from the fracture. Although there is somevariation in the expression of β2-microglobulin indicating that the startingamounts of RNA and the subsequently cDNA levels are not exactly similar, thereis clearly mRNA either present or absent in the adipose tissue.
ELISA
Increased levels of cytokines are found in adipose tissue of patients with afemoral fracture. The cytokine levels are more often and higher positive insupernatant from adipose tissue taken near the fracture than in adipose tissuetaken remote from the fracture (Figure 2). The increased levels in near comparedto remote is most pronounced for IL8 (p=0.0006), and to a lesser extent for IL6(p=0.06). There are no clear differences in TNFα levels. All 12 near adiposebiopsies were positive for at least one cytokine, whereas of the 10 remote studiedbiopsies, 6 were negative for all: TNFα, IL6 and IL8.
Figure 2. Levels of TNFα (left), IL6 (middle) and IL8 (right) in adipose tissue remote from or nearthe femoral fracture, * p = 0.06, # p = 0.0006.
Since there is a large variation in the levels of cytokines between patients,TNFα, IL6 and IL8 levels within one patient (remote and near) are alsocompared (7 patients, indicated in Figure 3). There is a clear increase in IL8levels (p=0.016) in adipose tissue near the fracture compared to remote adiposetissue within a patient. Although the increase in near compared to remote is notsignificant for IL6 (p=0.06), IL6 levels are more and higher positive in near than
remote near
IL6
(pg/
g)
0
20
40
60
80
100
120
140
remote near
IL8
(pg/
g)
0
100
200
300
400
remote near
TN
Fα (
pg/g
)
0
20
40
60
80
100
120
140
* #

Chapter 6
106
remote. Since in 2 of the 7 patients IL6 levels are unaltered, only 5 pairs of nearand remote are left for the Wilcoxon signed rank test, which makes statisticalanalysis difficult. As mentioned before, there are no clear differences in TNFαlevels and thus also no clear response is found between near and remote withinone patient.
Figure 3. Levels of TNFα (left), IL6 (middle) and IL8 (right) in adipose tissue, remote or near fromthe femoral fracture are compared within one patient (n=7).
Plasma
ELISA
In plasma of 5 of the 6 studied patients elevated IL6, and 3 of the 6 studiedpatients elevated IL8 levels are found. TNFα is not detected in plasma of any ofthe patients. No TNFα, IL6 and IL8 is detected in plasma of healthy controls.The observed levels range from 20 to120 pg/ml for IL6 and from 18 to 50 pg/mlfor IL8.
remote near
TN
Fα p
g/g
0
10
20
30
40
50
60
remote near
IL6
(pg/
g)0
40
80
120
160
200p=0.06
remote near
IL8
pg
/g
0
100
200
300
400p=0.016

Cytokine production after blunt trauma
107
Discussion
To understand what initiates the systemic inflammatory response that maylead to the development of MODS after severe trauma, local inflammation andespecially cytokine production in muscle and subcutaneous adipose tissue wasstudied in patients with a closed femoral fracture. Our findings indicate that aclosed femoral fracture cannot induce local activation in muscle or skin (previousresults), but induces cytokine production in adipose tissue.
Activation of subcutaneous adipose tissue near the fracture has beendemonstrated by an increase in IL6 and a clear increase in IL8 levels ascompared to remote adipose tissue (Figure 3). TNFα is also detected in adiposetissue, but its response is not as clear as for IL6 and IL8.
The increased cytokine levels that we measured in adipose tissue near thefracture, are the result of actual production of cytokines by the adipose tissueitself, since the RT-PCR experiments have shown that IL6 and IL8, but alsoTNFα and IL1β mRNA is present. It indicates that there is active transcriptionand cytokine production by cells of adipose tissue and not only release ofcytokines that are ‘stored’. It is known from literature that adipocytes canproduce TNFα, IL6 and IL8 (16-20). Production of TNFα and IL8 has onlybeen shown in vitro, IL6 production in vitro as well as in vivo. It is also knownthat besides adipocytes other cells present in the adipose tissue: endothelial cellsand fibroblasts, can be producers of pro-inflammatory cytokines. Regardless ofwhich cells produce the cytokines, these results show that adipose tissue is asource of IL6, IL8 and to a lesser extent of TNFα, in response to blunt trauma (afemoral fracture). In theory, pro-inflammatory cytokines derived from adiposetissue may constitute the link between local and systemic inflammation as it hasbeen described that IL6 produced in adipose tissue is released into the circulation(19;21). This finding is confirmed in our study in which a (moderate) systemicIL6 response was observed. The hypothesis that adipose tissue might be thesource of a systemic (non-bacterial) inflammation is further supported by thefinding that a positive association between body mass index (BMI) and acutephase protein CRP has been reported. This can be explained by increased IL6production in patients with obesity or overweight (22). Also, other studiesindicate that IL6 derived from adipose tissue may leak into the circulation andcontribute to a systemic inflammatory response (23;24).
As mentioned before, a moderate systemic cytokine response was found.The systemic response was relatively mild which can be explained by the lowseverity of tissue damage (mean ISS of 12). As could be expected, none of thestudied patients developed a serious systemic inflammatory response and, orMODS.
There seems to be a certain correlation between elevated IL6 and IL8levels in adipose tissue and the systemic response, although this could be studied

Chapter 6
108
in only six patients. In the patient that did not reveal elevated levels systemically,adipose tissue was negative for cytokines, whereas increased cytokines locallycorrelated with increased systemic levels. The absence of systemic TNFα intrauma patients is in agreement with previous studies (25;26) and is probably theresult of the short half life and possible binding to its soluble receptor. A clearTNFα response is difficult to show as we also observed in adipose tissue.
Cytokine levels in 3 bone marrow samples -derived from a fracturedfemur- were studied (data not shown) and found positive for IL6 and IL8(respectively 56, 487 and 1085 pg/g and IL8 is 168, 1764 and 592 pg/g), whereasTNFα is not detected. This finding is in accordance with the observation ofLaharrague et al. (27) who showed that adipocytes can secrete significant IL6levels. It is unknown if these bone marrow derived cytokines can contribute toinflammation, but in case of a fractured long bone, these cytokines may leak intothe circulation.
From clinical experience it is known that muscle often becomes edematousafter long bone fractures. In case a long bone fracture is attended by local muscleswelling, it is often necessary to perform a fasciotomy to prevent a compartmentsyndrome (28;29). Despite the fact that muscle was sometimes found to bedamaged and bleeding is present in some of the biopsies, there are no signs oflocal inflammation in muscle tissue. Using histochemistry, there are nodifferences between near and remote muscle biopsies observed. No infiltratingcells, no induction of adhesion molecule nor increased cytokine production isfound in any of the studied biopsies. The absence of local cytokine production isconfirmed by the RT-PCR experiments. There was no clear upregulation ofcytokine mRNA in muscle near the fracture compared to remote muscle,although it seemed that biopsies taken near were more often positive thanbiopsies remote from the fracture. Differences in cytokine mRNA intensitybetween patients can be explained by different individual baseline expressionlevels and the varying cellular composition of the sections that were used forRNA isolation. The absence of a clear local response and remarkable cytokineproduction suggests that muscle surrounding fractured bone does not contributeto a systemic response.
In summary, our results indicate that adipose tissue is activated andproduce pro-inflammatory cytokines as a result of a femoral fracture. As it isknown from literature that adipose tissue can produce and release cytokinesleading to increased systemic levels as well as systemic inflammation, weconclude that adipose tissue involved in an injury may contribute to elevated IL6levels and or systemic inflammation.

Cytokine production after blunt trauma
109
References
1. Gosling, P. and Dickson, G. R. Serum C-Reactive Protein in Patients With Serious Trauma.Injury 1992;23(7):483-6.
2. Rabinovici, R., John, R., Esser, K. M., Vernick, J., and Feuerstein, G. Serum Tumor NecrosisFactor-Alpha Profile in Trauma Patients. J.Trauma. 1993;35(5):698-702.
3. Svoboda, P., Kantorova, I., and Ochmann, J. Dynamics of Interleukin 1, 2, and 6 and TumorNecrosis Factor Alpha in Multiple Trauma Patients. J.Trauma. 1994;36(3):336-40.
4. Goris, R. J. MODS/SIRS: Result of an Overwhelming Inflammatory Response?. World J.Surg.1996;20(4):418-21.
5. Baue, A. E. Multiple Organ Failure, Multiple Organ Dysfunction Syndrome, and SystemicInflammatory Response Syndrome. Why No Magic Bullets? Arch.Surg. 1997;132(7):703-7.
6. Davies, M. G. and Hagen, P. O. Systemic Inflammatory Response Syndrome. Br.J.Surg.1997;84(7):920-35.
7. Ross, R. Inflammation, cell proliferation, and connective tissue formation in wound repair. Hunt,T. K. Wound healing and wound infection: theory and surgical practice.1980. pp.1-8.
8. Hunt, T. K. Basic Principles of Wound Healing. J.Trauma. 1990;30(12 Suppl):S122-S128.
9. Bitterman, H., Kinarty, A., Lazarovich, H., and Lahat, N. Acute Release of Cytokines IsProportional to Tissue Injury Induced by Surgical Trauma and Shock in Rats. J.Clin.Immunol.1991;11(4):184-92.
10. Baigrie, R. J., Lamont, P. M., Kwiatkowski, D., Dallman, M. J., and Morris, P. J. SystemicCytokine Response After Major Surgery. Br.J.Surg. 1992;79(8):757-60.
11. Biffl, W. L., Moore, E. E., Moore, F. A., and Peterson, V. M. Interleukin-6 in the InjuredPatient. Marker of Injury or Mediator of Inflammation? Ann.Surg. 1996;224(5):647-64.
12. Gebhard, F., Pfetsch, H., Steinbach, G., Strecker, W., Kinzl, L., and Bruckner, U. B. IsInterleukin 6 an Early Marker of Injury Severity Following Major Trauma in Humans?Arch.Surg. 2000;135(3):291-5.
13. van der, Laan N., de Leij, L., and ten Duis, H. J. Local Cellular Inflammation As a Result ofElective Standardized Vascular Surgery. Acta Histochem. 2001;103(2):139-49.
14. Chomczynski, P. and Sacchi, N. Single-Step Method of RNA Isolation by Acid GuanidiniumThiocyanate-Phenol-Chloroform Extraction. Anal.Biochem. 1987;162(1):156-9.
15. Kobold, A. C., van-Wijk, R. T., Franssen, C. F., Molema, G., Kallenberg, C. G., and Tervaert, J.W. In Vitro Up-Regulation of E-Selectin and Induction of Interleukin-6 in Endothelial Cells byAutoantibodies in Wegener's Granulomatosis and Microscopic Polyangiitis. Clin.Exp.Rheumatol.1999;17(4):433-40.
16. Kern, P. A., Saghizadeh, M., Ong, J. M., Bosch, R. J., Deem, R., and Simsolo, R. B. TheExpression of Tumor Necrosis Factor in Human Adipose Tissue. Regulation by Obesity, WeightLoss, and Relationship to Lipoprotein Lipase. J.Clin.Invest 1995;95(5):2111-9.

Chapter 6
110
17. Sewter, C. P., Digby, J. E., Blows, F., Prins, J., and O'Rahilly, S. Regulation of Tumour NecrosisFactor-Alpha Release From Human Adipose Tissue in Vitro. J.Endocrinol. 1999;163(1):33-8.
18. Purohit, A., Ghilchik, M. W., Duncan, L., Wang, D. Y., Singh, A., Walker, M. M., and Reed, M.J. Aromatase Activity and Interleukin-6 Production by Normal and Malignant Breast Tissues.J.Clin.Endocrinol.Metab 1995;80(10):3052-8.
19. Fried, S. K., Bunkin, D. A., and Greenberg, A. S. Omental and Subcutaneous Adipose Tissues ofObese Subjects Release Interleukin-6: Depot Difference and Regulation by Glucocorticoid.J.Clin.Endocrinol.Metab 1998;83(3):847-50.
20. Bruun, J. M., Pedersen, S. B., and Richelsen, B. Regulation of Interleukin 8 Production and GeneExpression in Human Adipose Tissue in Vitro. J.Clin.Endocrinol.Metab 2001;86(3):1267-73.
21. Mohamed, Ali, V, Goodrick, S., Rawesh, A., Katz, D. R., Miles, J. M., Yudkin, J. S., Klein, S.,and Coppack, S. W. Subcutaneous Adipose Tissue Releases Interleukin-6, but Not TumorNecrosis Factor-Alpha, in Vivo. J.Clin.Endocrinol.Metab 1997;82(12):4196-200.
22. Visser, M., Bouter, L. M., McQuillan, G. M., Wener, M. H., and Harris, T. B. Elevated C-Reactive Protein Levels in Overweight and Obese Adults. JAMA 8-12-1999;282(22):2131-5.
23. Yudkin, J. S., Stehouwer, C. D., Emeis, J. J., and Coppack, S. W. C-Reactive Protein in HealthySubjects: Associations With Obesity, Insulin Resistance, and Endothelial Dysfunction: a PotentialRole for Cytokines Originating From Adipose Tissue? Arterioscler.Thromb.Vasc.Biol.1999;19(4):972-8.
24. Bastard, J. P., Jardel, C., Bruckert, E., Blondy, P., Capeau, J., Laville, M., Vidal, H., andHainque, B. Elevated Levels of Interleukin 6 Are Reduced in Serum and Subcutaneous AdiposeTissue of Obese Women After Weight Loss. J.Clin.Endocrinol.Metab 2000;85(9):3338-42.
25. Pullicino, E. A., Carli, F., Poole, S., Rafferty, B., Malik, S. T., and Elia, M. The RelationshipBetween the Circulating Concentrations of Interleukin 6 (IL-6), Tumor Necrosis Factor (TNF)and the Acute Phase Response to Elective Surgery and Accidental Injury. Lymphokine Res.1990;9(2):231-8.
26. Keel, M., Ecknauer, E., Stocker, R., Ungethum, U., Steckholzer, U., Kenney, J., Gallati, H.,Trentz, O., and Ertel, W. Different Pattern of Local and Systemic Release of Proinflammatoryand Anti-Inflammatory Mediators in Severely Injured Patients With Chest Trauma. J.Trauma.1996;40(6):907-12.
27. Laharrague, P., Fontanilles, A. M., Tkaczuk, J., Corberand, J. X., Penicaud, L., and Casteilla, L.Inflammatory/Haematopoietic Cytokine Production by Human Bone Marrow Adipocytes.Eur.Cytokine Netw. 2000;11(4):634-9.
28. Tarlow, S. D., Achterman, C. A., Hayhurst, J., and Ovadia, D. N. Acute CompartmentSyndrome in the Thigh Complicating Fracture of the Femur. A Report of Three Cases. J.BoneJoint Surg.Am. 1986;68(9):1439-43.
29. Heckman, M. M., Whitesides, T. E., Jr., Grewe, S. R., and Rooks, M. D. Compartment Pressurein Association With Closed Tibial Fractures. The Relationship Between Tissue Pressure,Compartment, and the Distance From the Site of the Fracture. J.Bone Joint Surg.Am.1994;76(9):1285-92.

Chapter VII
Discussion

Chapter 7
112
Inflammation
It is generally assumed that tissue injury leads to local inflammation, and ifthe extent is large enough, tissue injury also leads to systemic inflammation. Sucha “classical local inflammatory response” as reflected by an immediategranulocyte migration into the damaged tissue may result from a variety of stimulilike ischemia reperfusion injury (1-4), skin injury (5;6), infection (7) and mucosaldamage (8;9). Inflammation can be restricted to the site of tissue damage but isoften accompanied to some extent by a systemic response (10). In general,inflammation is a strictly controlled system: duration and intensity of theinflammatory response is carefully regulated in order to limit tissue damage as aresult of a too extensive reaction.
When the inflammatory response is large enough to cause systemic effects,like defined (11-13) changes in temperature, heart rate, respiratory rate or whiteblood cell count, we call it the systemic inflammatory response syndrome(SIRS). In case of persistent activation, the systemic inflammatory response canresult in a type of deleterious unregulated inflammation known as multiple organdysfunction syndrome (MODS).Unregulated inflammation as can be observed inmulti-trauma patients, burn patients or patients with otherwise devitalized tissues(abdominal abcesses, pancreatitis), is characterized by an excessive release ofpro-inflammatory mediators such as cytokines, acute phase proteins, solubleadhesion molecules and complement products (14-17).
Can a local trigger lead to systemic inflammation?
Although many data concerning the presence of circulating markers ofinflammation in relation to an unregulated systemic inflammation are available inmulti-trauma patients, underlying mechanisms are largely unknown. An obviousexplanation is, that the systemic response is induced by the local inflammatoryresponse. In the systemic circulation measured cytokines are quantitativelyrelated to the degree of tissue damage (18-21). If there is an ongoing localactivation in the damaged tissue with a spill-over of locally producedinflammatory mediators into the systemic circulation, an unregulated systemicresponse may be induced.
The importance of a local inflammatory response in initiating anunregulated systemic response is underscored by the finding that early fixation oflong bone fractures increases survival of multi-trauma patients (22-26). Immediatestabilization of long bone fractures prevents ongoing movement at the fracturesite. By this, repetitive local damage to the surrounding tissue is prevented.
There are similarities in the described systemic inflammatory response totrauma as indicated above and in the fat embolism syndrome. Marrow fatembolization occurs in almost all patients with long bone or pelvic fractures

Discussion
113
(27;28). Only a minority of these patients develop mental disturbances,pulmonary stress, petechiae and early fever, all symptoms related to the classicalfat embolism syndrome. The fat embolism syndrome develops more often inpatients with a closed fracture and, or delayed (i.e. after 24 hours) surgery than inpatients with an open fracture or early operation (27;29). This implies that inaddition to purely mechanical factors (embolization of fat) other factors possiblyplay a role in the development of systemic signs of fat embolism. Accompanyingsoft tissue injury surrounding the long bone fracture has been proposed to besuch an additional factor (30).
Since local inflammation seems important in response to injury and ininitiating the systemic response, it was studied whether indicators of an acutelocal inflammatory response (within 12 hours post-injury) could be found inlocally inflicted tissue in the case of blunt trauma. More specifically, localinflammation was studied in the light of the assumption that tissue damage intissues surrounding a fractured bone is followed by a local inflammatoryresponse.
Local inflammation in skin after blunt trauma
Local inflammation as a result of blunt trauma has first been studied inhuman skin. Skin is the largest “organ” of the body and represents the interfacebetween the internal and external environment. It is a “barrier” and therefore animportant protective organ. In addition, skin contains many immunocompetentcells such as Langerhans cells, keratinocytes, fibroblasts, mast cells, tissuemacrophages and lymphocytes. It is generally assumed that skin plays an activerole in inducing a local inflammatory response (31-33).
To assess this in trauma patients, we have compared skin surrounding aclosed femoral fracture with remote (in the same patient) and normal skin andbiopsies were analyzed using immunohistochemistry, electron microscopy,ELISA and RT-PCR. To our surprise, no signs of a local inflammatory responsewere observed in skin after blunt trauma. Using immunohistochemistry, noinfiltrating granulocytes were observed and there was no increase in pro-inflammatory cytokine expression. Skin surrounding the fracture, but also remoteskin showed limited activation as was apparent from low or absent E-selectinexpression in local endothelial cells, generally low IL1β and IL6 mRNAexpression and low TNFα and IL6 protein expression. Electron microscopyshowed that there is a wide variation in the morphology of endothelial cellsindicative for variations in activation status of endothelial cells. However also bythis method no clear signs of an inflammatory response were observed.Altogether, these data indicate that local inflammation as a result of blunt traumais limited in skin. Apparently, the mechanical impact, necessary to fracture the

Chapter 7
114
underlying bone does not result in damage of the skin and a subsequent localinflammatory response.
Local inflammation in muscle after blunt trauma
Since skeletal muscle is located more closely to a fractured bone than skin,it might become damaged more easily. From clinical experience we know thatmuscle often becomes edematous after long bone fractures. As with edema inother tissues, muscle swelling is considered to be part of an inflammatoryresponse. In case a long bone fracture is attended by serious local muscleswelling, it is often necessary to perform a fasciotomy to prevent a compartmentsyndrome (high pressure soft tissue ischemia) (34;35).
Although in our study muscle was found to be damaged and signs ofbleeding were present between muscle fibers as a result of blunt trauma, no signsof a local inflammatory response were observed. No infiltrating cells, noinduction of adhesion molecule expression nor induction of pro-inflammatorycytokines were found in muscle biopsies with immunohistochemistry. RT-PCRexperiments confirmed that there is no substantial increase in cytokine productionas a result of blunt trauma.
Since swelling of the muscle reaches maximum values after 24 to 48 hoursafter the initial injury, signs of local inflammation may be observed at later timepoints. But, based on the knowledge that granulocytes quickly enter damagedtissue, it is unlikely that these cells will be found later. Monocytes andmacrophages might be observed after one or two days. However, it remainsunclear if there is a direct relation between these cell types and the observedclinical picture. So, in conclusion, blunt trauma does not induce a “classical localinflammatory response” in muscle.
Local inflammation in adipose tissue after trauma
In addition to skin and muscle, subcutaneous adipose tissue was studiedfor the early production of pro-inflammatory cytokines as a result of blunttrauma. Blunt trauma induced local activation in adipose tissue which wasdemonstrated by a clear increase in IL6 and IL8 in adipose tissue near thefracture as compared to remote adipose tissue (from the same patient, but takenfrom the hip region). RT-PCR experiments, showing the presence of TNFα, IL6and IL8 mRNA in adipose tissue, indicate that the increased cytokine levels arethe result of actual production by adipose tissue itself. The observed pro-inflammatory cytokines can originate from adipocytes, but it can not be excludedthat these are produced by other cells present in adipose tissue, such asendothelial cells and fibroblasts. Since granulocytes are not present in skin andmuscle surrounding the fractured bone, it is unlikely to expect infiltrating

Discussion
115
granulocytes in subcutaneous adipose tissue which is located between skin andmuscle.
Thus although adipose tissue is clearly activated as opposed to skin andmuscle, a “classical local inflammatory response” with granulocyte infiltrates isprobably not induced.
Blunt trauma does not induce a “classical local inflammatory response”
Starting from the principle that every injury should lead to an inflammatoryresponse, we assumed that blunt trauma (a closed femoral fracture) would inducea “classical local inflammatory response” as characterized by infiltratinggranulocytes. In contrast to what we expected, no such reaction was observed inskin and muscle surrounding the fractured bone. Although there is a possibilitythat an inflammatory response occurs later, a granulocyte infiltrate more than 12hours post injury would not be expected. Remarkable is the fact that we didobserve “inflammation” in adipose tissue as a result of a femoral fracture. Yet,this does not mean that a “classical inflammatory response” with infiltrating cellswas induced.
Since in contrast to skin and muscle, there is cytokine production inadipose tissue, different activation signals and subsequent mechanisms areinduced in adipose tissue than in skin and muscle. So, the type of tissue that isinvolved seems to be an important factor in the subsequent response.
Local inflammation as a result of different injuries
Since no “classical inflammatory response” was observed in tissues afterblunt trauma, other kinds of injuries were studied: a simple skin incision and thelate effects (> 48 hours) of penetrating injuries, i.e. one which leads to infection,of the skin.
In contrast to blunt trauma, the other types of injury did indeed inducelocal inflammation that was accompanied by granulocyte infiltration.
First, local inflammation after disruption of the epithelial skin barrier wasstudied. Surgical incision under aseptic conditions was used as a model. Weobserved granulocyte infiltration at first at 30 minutes after incision of the skin,their number increasing with time. This granulocyte infiltration was paralleled byE-selectin expression on endothelial cells, whereas no P-selectin, ICAM-1 andVCAM-1 expression was induced. Comparable to what was observed after blunttrauma, incision of the skin did not result in observable changes in pro-inflammatory cytokines (TNFα, IL1α, IL1β, IL6, IL8). This is probably theresult of the limited extent of tissue damage and the relative short study period(up to 4.5 hours) (6).

Chapter 7
116
Second, local inflammation as the late result of a penetrating injury(splinter, bite, infectious arterial line) resulting in infection was studied. This timea more pronounced and different inflammatory pattern was observed. Not onlygranulocytes, but also a clear increase in monocyte /macrophages and T-cellswas found. Furthermore, E-selectin, VCAM-1 and increased ICAM-1 isobserved. In contrast to skin afflicted with a simple incision, infected skinshowed a markedly changed cytokine pattern. TNFα and IL1α expression isincreased, whereas IL8 expression was decreased. Although the different timepoints at which incised and infected skin were studied can explain the differentresponses, the magnitude and seriousness of the response is probably a result ofthe type of injury (36): sharp wound edges without a lot of clear tissue damageversus contused wound edges with much apparently non-vital tissue. These latterforming an ideal environment for bacterial outgrowth.
Different local inflammatory responses in skin, muscle and adiposetissue
Skin
Based on the findings that a penetrating injury and even aseptic incision ofthe skin does induce a “classical inflammatory response”, whereas blunt traumadoes not, we propose that disruption of the epithelial barrier is an importanttrigger for granulocyte infiltration in human skin. This is confirmed by the factthat an open fracture induces a local inflammatory response similar as isobserved in incised skin, namely recruitment of granulocytes in combination withE-selectin expression (unpublished results). Similar responses as seen in skin arealso observed in the mucosal barrier of the gastrointestinal tract. In ulcerformation, the initial trigger for inflammation is a broken mucosal epithelial barrieras a result of injury, chemicals, drugs or toxins (8;9;37). Apparently, disruptionof the epithelial barrier in general is an important trigger for the induction of localinflammation.
In addition to a disrupted epithelial barrier, the presence of noxioussubstances is also a trigger for the induction of a “classical local inflammatoryresponse”. This is in agreement with reports about inflammation in human skin asa result of injury: burns, disruption of the skin, tape stripping, and intra-dermalinjection or applying of irritant substances (7;38-42). These are all stimuli thatdirectly activate or damage cells in the skin or interfere with the epithelial skinbarrier. Our findings concerning the local response as a result of infection after apenetrating injury also indicated that the presence of dead tissue and subsequentgrow of bacteria had clearly pro-inflammatory effects in addition to the effectsobserved after disruption of the epithelial barrier under aseptic conditions (simpleskin incision).

Discussion
117
From the point of view that skin provides protection and epithelial cells ingeneral serve as a barrier, it is comprehensible that an inflammatory response witha granulocyte infiltrate is induced after incision of the skin or after an openfracture: when the epithelial barrier is broken, there is a clearly increased risk forinfection. In the case of a closed femoral fracture, the presence of only damagefrom inside without disruption of the epithelial barrier and the low risk forinfection might explain the absence of a “classical local inflammatory response”.
Muscle
The fact that muscle is swollen as a result of blunt trauma apparently doesnot mean that there is a “classical” local response with subsequent granulocyteinfiltrate, as we demonstrated. As muscle is damaged from inside, granulocytesare not necessary, because similar as in skin, there is no risk for infection. At latertime points, macrophages may be present in muscle to contribute to the repair ofthe damaged tissue. However they play as far as we know no distinct role in theinduction of the acute inflammatory response characterized by capillary leakageand soft tissue swelling. Since not any sign of an inflammatory response wasobserved in the studied muscle biopsies, the underlying pathophysiologicalprocess remains obscure.
Helliwell et al. (43) observed endothelial activation in muscle of patientswith multiple organ failure. The biopsies they studied were taken after at least oneday on the intensive care unit and thus also at least one day after the initial injury.They conclude that endothelial activation in muscle as a primary process and notmicrovascular damage and ischemia may be an important factor in pathogenesisof multiple organ failure. This observation points to a systemic response ratherthan a local response (like the swelling of a muscle compartment in case of abroken leg) and is of no help in the interpretation of our results.
Adipose tissue
Blunt trauma clearly induces IL6 and IL8 production in adipose tissue inthe early phase (within 12 hours) after blunt trauma. This indicates that in contrastto skin and muscle, blunt trauma has a direct effect on adipose tissue. Pro-inflammatory cytokines derived from adipose tissue may constitute the linkbetween local and systemic inflammation while it is known that adipose tissuederived IL6 can be released into the circulation (44;45). Also, a positiveassociation has been reported between body mass index (BMI) and elevatedCRP levels. CRP is one of the inflammatory parameters, which production isinduced by IL6. So, elevated CRP can be explained by increased IL6 productionin patients with obesity or overweight (46). These data indicate that pro-inflammatory cytokines produced by adipose tissue can contribute to a systemic

Chapter 7
118
inflammatory response (47;48). The same cytokines may also induce endothelialcell activation in tissues surrounding the fracture, such as muscle.
Concluding remarks
We did not observe an early “classical local inflammatory response” in ourmodel of blunt trauma - a closed femoral fracture. Since tissues surrounding thefractured bone do not come in contact with the “foreign” environment, there isno increased risk for infection. As a result of this, there is no need forgranulocyte infiltration.
It is concluded that the mechanical injury as a result of a femoral fractureonly induces cytokine production in adipose tissue and not in skin and muscletissue within the observation period. So, inflammation of adipose tissue may bethe main cause of elevated IL6 levels observed early after blunt trauma.

Discussion
119
References
1. Seekamp, A., Till, G. O., Mulligan, M. S., Paulson, J. C., Anderson, D. C., Miyasaka, M., andWard, P. A. Role of Selectins in Local and Remote Tissue Injury Following Ischemia andReperfusion. Am.J.Pathol. 1994;144(3):592-8.
2. Verrie r, E. The Microvascular Cell and Ischemia-Reperfusion Injury. J.Cardiovasc.Pharmacol.1996;27 Suppl 1:S26-S30.
3. Groeneveld, A. B., Raijmakers, P. G., Rauwerda, J. A., and Hack, C. E. The InflammatoryResponse to Vascular Surgery-Associated Ischaemia and Reperfusion in Man: Effect onPostoperative Pulmonary Function. Eur.J.Vasc.Endovasc.Surg. 1997;14(5):351-9.
4. Sullivan, G. W., Sarembock, I. J., and Linden, J. The Role of Inflammation in Vascular Diseases.J.Leukoc.Biol. 2000;67(5):591-602.
5. Singer, A. J. and Clark, R. A. Cutaneous Wound Healing. N.Engl.J.Med. 2-9-1999;341(10):738-46.
6. van der, Laan N., de Leij, L., and ten Duis, H. J. Local Cellular Inflammation As a Result ofElective Standardized Vascular Surgery. Acta Histochem. 2001;103(2):139-49.
7. Silber, A., Newman, W., Reimann, K. A., Hendricks, E., Walsh, D., and Ringler, D. J. KineticExpression of Endothelial Adhesion Molecules and Relationship to Leukocyte Recruitment inTwo Cutaneous Models of Inflammation. Lab.Invest. 1994;70(2):163-75.
8. Ernst, P. B., Crowe, S. E., and Reyes, V. E. How Does Helicobacter Pylori Cause MucosalDamage? The Inflammatory Response. Gastroenterology 1997;113(6 Suppl):S35-S42.
9. Podolsky, D. K. Mucosal Immunity and Inflammation. V. Innate Mechanisms of MucosalDefense and Repair: the Best Offense Is a Good Defense. Am.J.Physiol 1999;277(3 Pt 1):G495-G499.
10. Gabay, C. and Kushner, I. Acute-Phase Proteins and Other Systemic Responses toInflammation. N.Engl.J.Med. 11-2-1999;340(6):448-54.
11. Beal, A. L. and Cerra, F. B. Multiple Organ Failure Syndrome in the 1990s. SystemicInflammatory Response and Organ Dysfunction. JAMA 19-1-1994;271(3):226-33.
12. Davies, M. G. and Hagen, P. O. Systemic Inflammatory Response Syndrome. Br.J.Surg.1997;84(7):920-35.
13. Brun-Buisson, C. The Epidemiology of the Systemic Inflammatory Response. Intensive CareMed. 2000;26 Suppl 1:S64-S74.
14. Goris, R. J., te-Boekhorst, T. P., Nuytinck, J. K., and Gimbrere, J. S. Multiple-Organ Failure.Generalized Autodestructive Inflammation? Arch.Surg. 1985;120(10):1109-15.
15. Goris, R. J. MODS/SIRS: Result of an Overwhelming Inflammatory Response? World J.Surg.1996;20(4):418-21.
16. Yao, Y. M., Redl, H., Bahrami, S., and Schlag, G. The Inflammatory Basis of Trauma/Shock-Associated Multiple Organ Failure. Inflamm.Res. 1998;47(5):201-10.

Chapter 7
120
17. Kim, P. K. and Deutschman, C. S. Inflammatory Responses and Mediators. Surg.Clin.NorthAm. 2000;80(3):885-94.
18. Bitterman, H., Kinarty, A., Lazarovich, H., and Lahat, N. Acute Release of Cytokines IsProportional to Tissue Injury Induced by Surgical Trauma and Shock in Rats. J.Clin.Immunol.1991;11(4):184-92.
19. Baigrie, R. J., Lamont, P. M., Kwiatkowski, D., Dallman, M. J., and Morris, P. J. SystemicCytokine Response After Major Surgery. Br.J.Surg. 1992;79(8):757-60.
20. Moore, F. A. and Moore, E. E. Evolving Concepts in the Pathogenesis of Postinjury MultipleOrgan Failure. Surg.Clin.North Am. 1995;75(2):257-77.
21. Gebhard, F., Pfetsch, H., Steinbach, G., Strecker, W., Kinzl, L., and Bruckner, U. B. IsInterleukin 6 an Early Marker of Injury Severity Following Major Trauma in Humans?Arch.Surg. 2000;135(3):291-5.
22. Goris, R. J., Gimbrere, J. S., van Niekerk, J. L., Schoots, F. J., and Booy, L. H. EarlyOsteosynthesis and Prophylactic Mechanical Ventilation in the Multitrauma Patient. J.Trauma1982;22(11):895-903.
23. Bone, L. B., Johnson, K. D., Weigelt, J., and Scheinberg, R. Early Versus Delayed Stabilizationof Femoral Fractures. A Prospective Randomized Study. J.Bone Joint Surg.Am. 1989;71(3):336-40.
24. Pape, H. C., Auf'm'Kolk, M., Paffrath, T., Regel, G., Sturm, J. A., and Tscherne, H. PrimaryIntramedullary Femur Fixation in Multiple Trauma Patients With Associated Lung Contusion--aCause of Posttraumatic ARDS? J.Trauma 1993;34(4):540-7.
25. Livingston, D. H. Management of the Surgical Patient With Multiple System Organ Failure.Am.J.Surg. 1993;165(2A Suppl):8S-13S.
26. Livingston, D. H. and Deitch, E. A. Multiple Organ Failure: a Common Problem in SurgicalIntensive Care Unit Patients. Ann.Med. 1995;27(1):13-20.
27. ten-Duis, H. J., Nijsten, M. W., Klasen, H. J., and Binnendijk, B. Fat Embolism in Patients Withan Isolated Fracture of the Femoral Shaft. J.Trauma. 1988;28(3):383-90.
28. van den Brand, J. G., van der Hoeven, J. H., and Olsman, J. G. [Dyspnea or Confusion AfterTrauma? Consider Fat Embolism Syndrome]. Ned.Tijdschr.Geneeskd. 5-8-2000;144(32):1513-7.
29. Riska, E. B. and Myllynen, P. Fat Embolism in Patients With Multiple Injuries. J.Trauma1982;22(11):891-4.
30. ten-Duis, H. J. The Fat Embolism Syndrome. Injury. 1997;28(2):77-85.
31. Kupper, T. S. Immune and Inflammatory Processes in Cutaneous Tissues. Mechanisms andSpeculations. J.Clin.Invest. 1990;86(6):1783-9.
32. Bos, J. D. and Kapsenberg, M. L. The Skin Immune System: Progress in Cutaneous Biology.Immunol.Today 1993;14(2):75-8.
33. Bos, J. D. The Skin As an Organ of Immunity. Clin.Exp.Immunol. 1997;107 Suppl 1:3-5.

Discussion
121
34. Tarlow, S. D., Achterman, C. A., Hayhurst, J., and Ovadia, D. N. Acute CompartmentSyndrome in the Thigh Complicating Fracture of the Femur. A Report of Three Cases. J.BoneJoint Surg.Am. 1986;68(9):1439-43.
35. Heckman, M. M., Whitesides, T. E., Jr., Grewe, S. R., and Rooks, M. D. Compartment Pressurein Association With Closed Tibial Fractures. The Relationship Between Tissue Pressure,Compartment, and the Distance From the Site of the Fracture. J.Bone Joint Surg.Am.1994;76(9):1285-92.
36. van der, Laan N., de Leij, L., and ten-Duis, H. J. Immunohistopathological Appearance of ThreeDifferent Types of Injury in Human Skin. Inflamm.Res. 2001;50(7).
37. Blecker, U. and Gold, B. D. Gastritis and Peptic Ulcer Disease in Childhood. Eur.J.Pediatr.1999;158(7):541-6.
38. Enk, A. H. and Katz, S. I. Early Events in the Induction Phase of Contact Sensitivity.J.Invest.Dermatol. 1992;99(5):39S-41S.
39. Garner, W. L., Rodriguez, J. L., Miller, C. G., Till, G. O., Rees, R. S., Smith, D. J., and Remick,D. G. Acute Skin Injury Releases Neutrophil Chemoattractants. Surgery 1994;116(1):42-8.
40. Boehm, K. D., Yun, J. K., Strohl, K. P., Trefzer, U., Haffner, A., and Elmets, C. A. In SituChanges in the Relative Abundance of Human Epidermal Cytokine Messenger RNA LevelsFollowing Exposure to the Poison Ivy/Oak Contact Allergen Urushiol. Exp.Dermatol.1996;5(3):150-60.
41. Engelhardt, E., Toksoy, A., Goebeler, M., Debus, S., Brocker, E. B., and Gillitzer, R. ChemokinesIL-8, GROalpha, MCP-1, IP-10, and Mig Are Sequentially and Differentially Expressed DuringPhase-Specific Infiltration of Leukocyte Subsets in Human Wound Healing. Am.J.Pathol.1998;153(6):1849-60.
42. Reilly, D. M. and Green, M. R. Eicosanoid and Cytokine Levels in Acute Skin Irritation inResponse to Tape Stripping and Capsaicin. Acta Derm.Venereol. 1999;79(3):187-90.
43. Helliwell, T. R., Wilkinson, A., Griffiths, R. D., Palmer, T. E., McClelland, P., and Bone, J. M.Microvascular Endothelial Activation in the Skeletal Muscles of Patients With Multiple OrganFailure. J.Neurol.Sci. 21-1-1998;154(1):26-34.
44. Mohamed, Ali, V, Goodrick, S., Rawesh, A., Katz, D. R., Miles, J. M., Yudkin, J. S., Klein, S.,and Coppack, S. W. Subcutaneous Adipose Tissue Releases Interleukin-6, but Not TumorNecrosis Factor-Alpha, in Vivo. J.Clin.Endocrinol.Metab 1997;82(12):4196-200.
45. Fried, S. K., Bunkin, D. A., and Greenberg, A. S. Omental and Subcutaneous Adipose Tissues ofObese Subjects Release Interleukin-6: Depot Difference and Regulation by Glucocorticoid.J.Clin.Endocrinol.Metab 1998;83(3):847-50.
46. Visser, M., Bouter, L. M., McQuillan, G. M., Wener, M. H., and Harris, T. B. Elevated C-Reactive Protein Levels in Overweight and Obese Adults]. JAMA 8-12-1999;282(22):2131-5.
47. Yudkin, J. S., Stehouwer, C. D., Emeis, J. J., and Coppack, S. W. C-Reactive Protein in HealthySubjects: Associations With Obesity, Insulin Resistance, and Endothelial Dysfunction: a PotentialRole for Cytokines Originating From Adipose Tissue? Arterioscler.Thromb.Vasc.Biol.1999;19(4):972-8.

Chapter 7
122
48. Bastard, J. P., Jardel, C., Bruckert, E., Blondy, P., Capeau, J., Laville, M., Vidal, H., andHainque, B. Elevated Levels of Interleukin 6 Are Reduced in Serum and Subcutaneous AdiposeTissue of Obese Women After Weight Loss. J.Clin.Endocrinol.Metab 2000;85(9):3338-42.

Chapter VIII
Summary

Chapter 8
124
Introduction
Multiple Organ Dysfunction Syndrome (MODS) is a serious complicationin severely injured patients. It is accompanied by an extreme high mortality rate(40 to 60 %). MODS is the ultimate consequence of an ongoing systemicinflammatory response syndrome (SIRS). Clinically SIRS is characterized by thecombination of two or more of the following symptoms: fever or hypothermia,increased heart rate, increased respiratory rate or hypocapnia, and leukocytosesor leukopenia. SIRS is considered to be the first phase of a systemic response towhat has begun as a local inflammatory process. SIRS is often characterized byan excessive release of pro-inflammatory mediators. Persistent release ofexcessive amounts of these pro-inflammatory mediators, may turn the “normally”beneficial inflammatory response to injury, into an auto-destructive process thatmay lead to distant organ damage or failure.
Although many data concerning the behavior of certain circulating markersin relation to SIRS and MODS have been obtained, interpretation of these data isdifficult. For example, elevated IL6 levels in the circulation correlate withpatients’ risk to develop MODS, but it is still unknown what initiates the IL6production.
Since cytokine production appears to be related to the degree of tissuedamage, local inflammation and production of cytokines in the tissues may beimportant in initiating systemic inflammation. If local activation in the damagedtissue persists, with a spill-over of locally produced inflammatory mediators intothe rest of the body, an unregulated response may be induced, in some caseseventually resulting in MODS.
In this thesis, early local inflammation as a result of injury was studied intrauma patients. Local tissue activation as a result of a closed femoral fracturewas used as a model. The local inflammatory response in general and especiallythe production of pro-inflammatory cytokines was studied in tissues (skin,muscle and adipose tissue) surrounding the fractured bone and compared withtissues taken from a more remote site, which were not damaged by the trauma.
To be able to detect cytokines locally in tissues such as skin as a result ofinjury, it is important to use a validated method and to know baseline levels.From the literature, it is clear that there is no consensus about the presence ofTNFα in normal human skin. Therefore, in Chapter 2, we tested ten differentantibodies directed against human TNFα for suitability to detect this cytokine intissues. First, antibodies were tested for immunoreactivity on cytospots of LPSstimulated peripheral blood mononuclear cells. Second, they were tested todetect recombinant TNFα in Western blot. Third, antibodies were tested oncryosections of normal human skin. It was found that TNFα is present in normalhuman skin, but that different antibodies reveal different staining patterns.

Summary
125
Although some antibodies were able to detect TNFα, they are not necessarilyuseful for detecting TNFα in human skin. These results emphasize that forunambiguous interpretation of data, clear description of protocols,concentrations used and appropriate controls are important.
Local inflammation as a result of disruption of the epithelial barrier byincision of the skin was studied and described in Chapter 3. Since biopsieswere taken under standardized conditions, it is a reproducible model to study theearly local inflammatory response in vivo as a function of time. We found thatincision of the skin induced a local inflammatory response. Local inflammationwas demonstrated by infiltration of granulocytes paralleled by E-selectinexpression. So, even in the absence of noxious exogenous substances and underaseptic conditions, a mild inflammatory response is induced in human skin.Furthermore, the study underscores the importance of acquiring baselinebiopsies at timepoint zero, to avoid local inflammation as a result of the incisionitself.
In Chapter 4, the local inflammatory response as a result of disruption ofthe epithelial barrier by incision of the skin and of proven bacterial infection as aresult of a penetrating injury in the skin were compared with possibleinflammation in human skin after a closed femoral fracture. Incision of the skinresulted in a granulocyte infiltrate paralleled by E-selectin expression. In infectedskin, granulocytes were observed and monocyte/macrophage and T-cell numbersincreased. Also, E-selectin, VCAM-1, ICAM-1 and pro-inflammatory cytokineexpression changed. Skin biopsies taken at the site of the femoral fractureshowed no signs of inflammation. Thus different patterns of inflammationaccompany different types of injury in human skin.
In Chapter 5, the local inflammatory response and especially cytokineproduction as a result of blunt trauma, i.e. a closed femoral fracture, was studiedin detail. Skin surrounding a closed femoral fracture was compared with remote(in the same patient) and normal skin. Biopsies were analyzed usingimmunohistochemistry, electron microscopy, ELISA and RT-PCR. Skinsurrounding the fracture, but also remote skin showed only limited activation inthe form of E-selectin expression, IL1β and IL6 mRNA and TNFα and IL6protein expression. Electron microscopy indicated that there is a wide variation inactivation state of endothelial cells.
It was shown that human skin is not directly activated as a result of afemoral fracture. Local inflammation of the skin is limited and probably does notcontribute to a systemic inflammatory response in trauma patients.

Chapter 8
126
Since we found no clear activation in skin, signs of early local inflammationin tissues closer to the fractured bone, i.e. muscle and adipose tissue werestudied and described in Chapter 6. In addition to local inflammation, thepresence of a systemic inflammatory response was determined by detection ofpro-inflammatory cytokines in the circulation. Blunt trauma induces activation ofsubcutaneous adipose tissue as demonstrated by a clear increase in IL6 and IL8in the tissue near the fracture as compared to remote tissue. RT-PCRexperiments confirmed that the increase in cytokines is the result of an actualproduction by adipose tissue itself. In contrast, in muscle, immunohistochemistryand RT-PCR showed no signs of local inflammation or clear cytokineproduction. All, except for one patient, showed a moderate systemic response asreflected by elevated IL6 and IL8 levels. It is concluded that mechanical injury asa result of a closed femoral fracture only induces cytokine production in adiposetissue, but not in muscle tissue within the observation period. So, inflammation ofadipose tissue may be the main cause of elevated systemic IL6 levels observedearly after blunt trauma.
Chapter 7 attempts to integrate the results of the different studiesconcerning early local inflammation as a result of injury. The main conclusion isthat blunt trauma does not induce a “classical local inflammatory response” ascharacterized by infiltrating granulocytes. However, blunt trauma may result inlocal triggering of systemic signs of inflammation, since pro-inflammatorycytokines are mainly produced in the adipose tissue surrounding the fracture.Since adipose tissue is well known to be able to produce and release cytokines,we conclude that adipose tissue is the prime local trigger resulting in elevated IL6and systemic inflammation after blunt trauma.

Chapter IX
Samenvatting

Chapter 9
128
Inleiding
Multiple Organ Dysfunction Syndrome (MODS) is een ernstigecomplicatie bij zwaar gewonde patiënten. MODS gaat gepaard met een hoogsterftecijfer (40 tot 60 %) en is het uiteindelijke gevolg van een voortdurendealgehele (systemische) ontsteking, welke Systemic Inflammatory ResponseSyndrome (SIRS) wordt genoemd. Klinisch wordt SIRS gekarakteriseerd doorde combinatie van twee of meer van de volgende symptomen: koorts ofhypothermie (verlaagde temperatuur), versnelde hartslag, verhoogdeademhalingsfrequentie of hypocapnie (verlaagd CO2 gehalte in het bloed) enleukocytose of leukopenie (een tijdelijk toe -of afname van de hoeveelheid wittebloedcellen). SIRS wordt verondersteld de eerste fase te zijn van eensystemische respons als reactie op een plaatselijk ontstekingsproces. SIRS wordtin veel gevallen gekenmerkt door het vrijkomen van een overvloed aan ontstekinginducerende stoffen. Door het voortdurend vrijkomen van een overvloed vandeze stoffen, kan de normaal gesproken voordelige ontstekingsreactie als gevolgvan weefselschade, veranderen in een zelf-vernietigend proces. Dit kan uiteindelijktot schade aan organen en zelfs tot orgaanfalen leiden.
Hoewel er veel gegevens beschikbaar zijn met betrekking tot deaanwezigheid van bepaalde merkers (pro-ontstekingsmediatoren) in het bloed ende relatie tot SIRS en MODS, is de interpretatie van deze gegevens moeilijk.Verhoogde spiegels van het cytokine interleukine 6 (IL6) in het bloed correlerenbijvoorbeeld met het risico dat een patiënt loopt om multi-orgaanfalen teontwikkelen, maar het is nog steeds onbekend welke prikkel tot eenoverproductie van IL6 leidt.
Aangezien de hoogte van cytokine productie gerelateerd lijkt te zijn aan demate van weefselschade, zou een lokale ontsteking en de productie van cytokinesin de weefsels belangrijk kunnen zijn bij het initiëren van systemische ontsteking.Immers, wanneer plaatselijke activering in de beschadigde weefsels te langaanhoudt, kunnen lokaal geproduceerde ontstekingsmediatoren in het bloed endaarmee in de rest van het lichaam terechtkomen. Hierdoor zou eenongecontroleerde reactie in gang gezet kunnen worden, die in een aantal gevallenuiteindelijk tot multi-orgaanfalen leidt.
In dit proefschrift wordt de vroeg lokale ontstekingsreactie als gevolg vanweefselschade onderzocht bij trauma patiënten. Als “standaard” model werd deplaatselijke weefsel activatie als gevolg van een gesloten bovenbeenbreukgekozen. Niet alleen de lokale ontstekingsreactie in het algemeen, maar vooral deproductie van pro-ontstekingscytokines werd onderzocht in weefsels (huid, spieren vetweefsel) rondom de breuk en vergeleken met onbeschadigde weefsels dieverder van de breuk waren verwijderd.

Samenvatting
129
Om lokaal -in weefsels zoals huid-, cytokines aan te tonen, is het belangrijkom een gevalideerde methode te gebruiken en de basale cytokine niveaus tekennen. De literatuur is niet eenduidend over de aanwezigheid van het cytokineTNFα in normale humane huid. Daarom hebben we in Hoofdstuk 2, tienverschillende antilichamen, gericht tegen humaan TNFα, getest op hungeschiktheid om dit cytokine in weefsel aan te tonen. In de eerste plaats werdende antilichamen getest op immunoreactiviteit op geactiveerde monocyten (cellenwaarvan bekend is dat ze TNF aanmaken). Vervolgens werden ze met behulp vanWestern blot getest op binding aan recombinant TNFα. Tenslotte werden deantilichamen getest op vriescoupes van normale humane huid. TNFα bleekaanwezig te zijn in normale huid, echter de verschillende antilichamen lietenverschillende aankleuringspatronen zien. Hoewel sommige antilichamen in staatbleken TNFα aan te tonen, zijn ze niet per definitie geschikt om TNFα inmenselijke huid te bestuderen. De resultaten benadrukken dat voor hetondubbelzinnig interpreteren van gegevens, het belangrijk is dat duidelijk vermeldwordt welk protocol, welk antilichaam en welke concentratie van het antilichaamgebruikt is. Bovendien is het gebruik van de juiste controles essentieel.
De lokale ontsteking als gevolg van het doorbreken van de epitheelbarrière,zoals plaatsvindt bij incisie van de huid, is beschreven in Hoofdstuk 3. Bijvaatchirurgische patienten werd bij de aanvang van de operatie (onder aseptischeomstandigheden) in de lies op standaardwijze een huid biopsie genomen. Navaste tijden werd van de wondrand een nieuw biopt genomen om deontstekingsreactie in de tijd te kunnen volgen.
We vonden dat incisie van de huid inderdaad een lokale ontstekingsreactieveroorzaakt. Dit werd aangetoond door een in de tijd snelle toename van hetaantal infiltrerende granulocyten, parallel met de expressie van E-selectine opendotheel. Er kan geconcludeerd worden dat in afwezigheid van schadelijkeexogene stoffen en onder aseptische omstandigheden, een mildeontstekingsreactie opgewekt wordt in de huid.
In Hoofdstuk 4, werd de lokale ontstekingsreactie als gevolg van incisievan de huid vergeleken met een ontstekingsreactie die het gevolg is van eenbewezen bacteriële infectie en met een mogelijke ontstekingsreactie in humanehuid ten gevolge van een breuk van het bovenbeen. Zoals beschreven inhoofdstuk 3 leidde incisie van de huid tot het infiltreren van granulocyten en E-selectine expressie. In de geï nfecteerde huid werd naast granulocyten eentoename in het aantal monocyten/macrofagen en T-cellen waargenomen. Ookwerd een verhoogde expressie van E-selectine, VCAM-1, ICAM-1 en pro-ontstekingscytokines geconstateerd. Huidbiopten afkomstig van patienten meteen gesloten bovenbeenbreuk toonden geen tekenen van ontsteking. Uit deze

Chapter 9
130
resultaten kan geconcludeerd worden dat verschillende vormen van schade aande huid bestaan, die verschillende ontstekingspatronen induceren.
In Hoofdstuk 5, werd de lokale ontstekingsreactie en met name decytokine productie als gevolg van stomp letsel, d.w.z. een gesloten breuk van hetbovenbeen, in detail bestudeerd. Huid rondom de gesloten bovenbeenbreuk werdvergeleken met huid van dezelfde patiënt op een plaats waar geen letsel aanwezigwas. Biopten werden geanalyseerd met behulp van immunohistochemie,electronen microscopie, ELISA en RT-PCR. Huid rondom de breuk, maar ookde huid “op afstand” vertoonde slechts een geringe activatie, zoals afgeleid uit deaanwezigheid van IL1β en IL6 mRNA en E-selectine, TNFα en IL6 eiwitexpressie. Electronen miscroscopie liet zien dat er een grote variatie is in deactivatietoestand van endotheelcellen. Er werd aangetoond dat humane huid nietdirect geactiveerd wordt als gevolg van een breuk van het bovenbeen. Lokaleontsteking in de huid is beperkt en draagt waarschijnlijk niet bij aan desystemische ontstekingsreacties die vaak bij ongevalspatiënten worden gezien.
Aangezien we geen duidelijke activatie in huid konden aantonen, werdentekenen van een vroege plaatselijke ontstekingsreactie gezocht in weefsels dichterbij het gebroken bot, d.w.z. spier en vetweefsel. De resultaten zijn beschreven inHoofdstuk 6. Daarnaast werd naast een lokale ontstekingsreactie ook demogelijke aanwezigheid van een systemische ontstekingsreactie onderzocht doorpro-ontstekingscytokines in het bloed te bepalen van patiënten met een geslotenbreuk van het bovenbeen. Stomp letsel induceert de activatie van onderhuidsvetweefsel. Dit bleek uit een duidelijke toename van de gemeten IL6 en IL8niveaus in weefsel vlakbij de breuk in vergelijking met weefsel “op afstand”. RT-PCR experimenten bevestigen dat de toename van cytokines het resultaat is vandaadwerkelijke productie door vetweefsel zelf. In spierweefsel daarentegen wasmet behulp van immunohistochemie en RT-PCR geen lokale ontsteking ofcytokine productie zichtbaar. Op één patiënt na, vertoonden alle patiënten eenmatige systemische reactie zoals zichtbaar is door de verhoogde systemische IL6en IL8 spiegels. Mechanische schade als gevolg van een geslotenbovenbeenbreuk induceert alleen cytokine productie in vetweefsel en niet inspierweefsel. Als we deze resultaten doortrekken naar de situatie bij patiënten meternstige verwondingen, dan kan geconcludeerd worden dat een plaatselijke initiëleontstekingsreactie in vetweefsel een oorzaak kan zijn van de snelle verhoogdesystemische IL6 niveaus als gevolg van een ongeval.
Hoofdstuk 7 tracht de resultaten van de verschillende studies metbetrekking tot vroege lokale ontsteking als gevolg van weefselbeschadiging teintegreren. De belangrijkste conclusie is dat stomp letsel geen klassiekeontstekingsreactie in de huid en spier, zoals gekarakteriseerd door infiltrerende

Samenvatting
131
granulocyten, veroorzaakt. Echter, stomp letsel zou via het lokaal in werkingzetten van een ontstekingsreactie kunnen leiden tot systemische ontsteking.Aangedaan vetweefsel rondom de breuk lijkt hieraan de voornaamste bijdrage televeren.

Chapter 9
132

Dankwoord

Dankwoord
134
Uiteraard wil ik beginnen om mijn beide promotores te bedanken: Prof. dr.H.J ten Duis en Prof. dr. L.F.M.H de Leij.
Allereerst Professor ten Duis: dat u, ondanks al uw drukkewerkzaamheden, toch altijd tijd heeft vrijgemaakt voor het onderzoek, heb ik zeergewaardeerd. Mede dankzij uw enorme enthousiasme, steun en vertrouwen is ditproefschrift tot stand gekomen. Zo nu en dan zei u: “Je bent een beetje mijn AIO”en zo heb ik dat zelf ook altijd ervaren. Heel veel dank voor alles.
Dan natuurlijk Loe: Onze eerste kennismaking naar aanleiding van eeninterview in de UK zal ik nooit meer vergeten. Je was het -terecht- oneens metmijn (niet juist geciteerde) uitspraken over de immunologie cursus in Groningen.Na even praten was het al snel bijgelegd, typerend voor hoe je bent. Ook jijmaakte ondanks je drukke bezigheden tijd voor het onderzoek. Bedanktdaarvoor.
Het feit dat mijn onderzoek zich op twee totaal verschillende maar naarmijn idee mooi aanvullende vlakken afspeelde, namelijk de kliniek en hetlaboratorium, heb ik als heel waardevol ervaren. Wat mij betreft geldt datzelfdevoor jullie “Loe en ten Duis”: heel verschillend, elkaar aanvullend en daardoor eensterke combinatie. Ik ben blij dat ik de mogelijkheid heb gehad om met julliebeide gewerkt te hebben.
Naast mijn beide promotores zijn er natuurlijk een heleboel andere mensendie op wat voor manier dan ook een steentje hebben bijgedragen. Het isonmogelijk om iedereen te noemen, maar een paar mensen wil ik in ieder gevalbedanken.
Met name in de beginfase, bij het opzetten van de TNFα kleuringenhebben we regelmatig contact gehad met Wim Buurman. Uw enormeenthousiasme en vele ideeën hebben zeker bijgedragen aan het tot stand komenvan Hoofdstuk 2. Bedankt voor de discussies en natuurlijk het beschikbaarstellen van alle antilichamen.
Met ontzettend veel enthousiasme heeft Marja van Luyn meegedacht engewerkt op een moment dat het onderzoek vrij moeizaam verliep. Dankzij je hulphebben we een aantal belangrijke experimenten kunnen doen dat heeftgeresulteerd in Hoofdstuk 5. Veel dank voor je steun.
De leescommissie: Prof. dr. R.J.A. Goris, Prof. dr. R. van Schilfgaarde enProf. dr. T.H. The, bedankt dat u mijn proefschrift heeft willen beoordelen.
Zonder hulp vanuit de kliniek hadden we dit onderzoek nooit kunnen doen.In het bijzonder wil ik hierbij Herbert Roerdink noemen en vooral bedanken.Herbert is vanaf het allereerste begin bij het onderzoek betrokken geweest enheeft zich ingezet om mensen in de kliniek enthousiast te maken en bij hetonderzoek te betrekken. Natuurlijk wil ik ook alle chirurgen, en alle mensen op deOK’s, die dit onderzoek mede mogelijk gemaakt hebben, bedanken voor hunhulp!

Dankwoord
135
Ger: Fijn om een roommate te hebben die ook van snoepen houdt.Hopelijk heb ik je niet te veel van het werk gehouden met mijn geklets. Het wasleuk om een kamer met je te delen.
Er zijn nog een paar mensen van verschillende afdelingen die ik wilbedanken: Hendry Pas, Ingrid Molema, Johan Bijzet, Nieske Brouwer, Peter vander Sijde, alle secretaresses van de chirurgie en met name Riette, jullie hulp eninzet heeft zeker bijgedragen aan het tot standkomen van dit proefschrift!
Ik heb met heel veel plezier op het lab gewerkt (en gekletst), bijzondergezellig was het altijd, bedankt: Aalzen, Anita, Astrid, Bart-Jan, Berber, Coba,Daniel, Elinda, Ieneke, Ingrid M., Jelleke, Pamela, Wijnand, Sebo en Susan, enook (oud) AIO’s van de AIO kamer: Hilde, Ymke, Raoul, Diane, Anneke,Agnieszka en Caroline.
Conny, Ingrid v.V en Renske, jammer dat jullie al eerder van het lab warenvertrokken. Gelukkig zien we elkaar zo nu en dan nog eens.
Natuurlijk zijn er ook mensen van buiten het werk die ik wil bedanken. Deéén heb ik vaker gezien dan de ander: Barbara, Dietha, Fleur, Jolanda, Paula,Paulo, Ronald en Sanne, het is hartstikke leuk met jullie.
Roeien met de Wombats was altijd erg fanatiek en vooral ook heel gezellig.Dank Annemieke, Welmoed en Lucy (op volgorde van de boot) dat ik altijd opboeg mocht klooien en kletsen.
Speciaal wil ik mijn “paranimfjes” Astrid en Paula bedanken, fijn dat jullieme willen ‘bijstaan’ op deze voor mij speciale dag.
Dan uiteraard mijn familie: Allerliefste Henk en Wil, de onvoorwaardelijkesteun die ik altijd van jullie heb gehad is ook de afgelopen jaren ontzettendbelangrijk voor me geweest. Het letterlijk en figuurlijk thuiskomen bij jullie is zowaardevol. Mede dankzij jullie is het proefschrift nu af. Ik weet niet hoe ik jullieooit kan bedanken.
Het kleine zusje zijn is nog steeds heerlijk en ik heb nu ook eindelijk mijn‘broers’. Liesbeth, Arie, Sjoukje, Ton (en nichtje Mare): fijn dat we nu allemaalvlak bij elkaar wonen, maar ook als dat niet zo is blijf ik jullie opzoeken.
Tot slot: Bastiaan, lief, ik ben zo blij met je. Hoe kan ik je bedanken voor alje steun, niet alleen de afgelopen tijd, maar ook in het algemeen. Wat moet ik tochzonder je!! Just to be with you is giving me the best day of my life.
Namkje







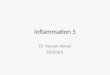





![Skin Inflammation, [Acute, Suppurative, Chronic, Chronic ... · Skin – Inflammation, [Acute, Suppurative, Chronic, Chronic Active, Granulomatous] presence of mononuclear cells (lymphocytes,](https://img.pdfslide.net/doc/110x75/5f0eb0c97e708231d44075f1/skin-inflammation-acute-suppurative-chronic-chronic-skin-a-inflammation.jpg)














