Embed Size (px)
Citation preview
Acute Myocardial Infarctions
Howard L. Sacher, D.O.Chief, Division of Cardiology
Adjunct Clinical Associate Professor of MedicineNew York College of Osteopathic Medicine
Learning Objectives
• To understand current concepts of the pathophysiology of acute myocardial infarction (AMI).
• To understand and apply current strategies in the evaluation of patients with AMI.
• To understand and apply current strategies in the management of patients with uncomplicated AMI.
• To understand and apply current strategies in the evaluation and management of patients with complications of AMI.
Acute Myocardial Infarction Acute Myocardial infarction
A. usually caused by sudden thrombotic occulusion of a coronary artery at the site of an atherosclerotic plaque that has become unstable due to a combination of ulceration, fissuring and rupture.
B. CHF if 25% of the left ventricle is infarcted C. Cardiogenic shock if 40% of left ventricle
is infarcted D. Right ventricular ischemia or infarction
occurs in up to ½ of inferior wall infarctions.
E. EKG 1.inferior wall myocardial infarction
changes leads II, III and aVF. 2. Anterior septal MI-V1, V2, V3 3. Anterior wall MI- V2, V3, V4 4. Lateral wall MI-V5,V6, I, aVLST segment elevation and T wave
changes occur first, then Q waves form
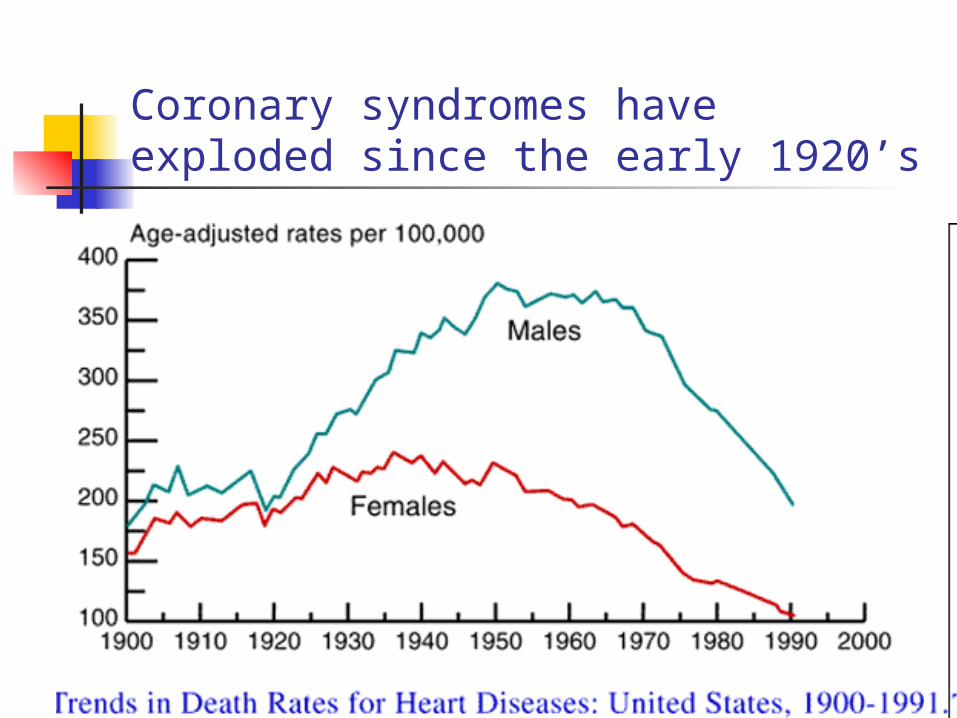
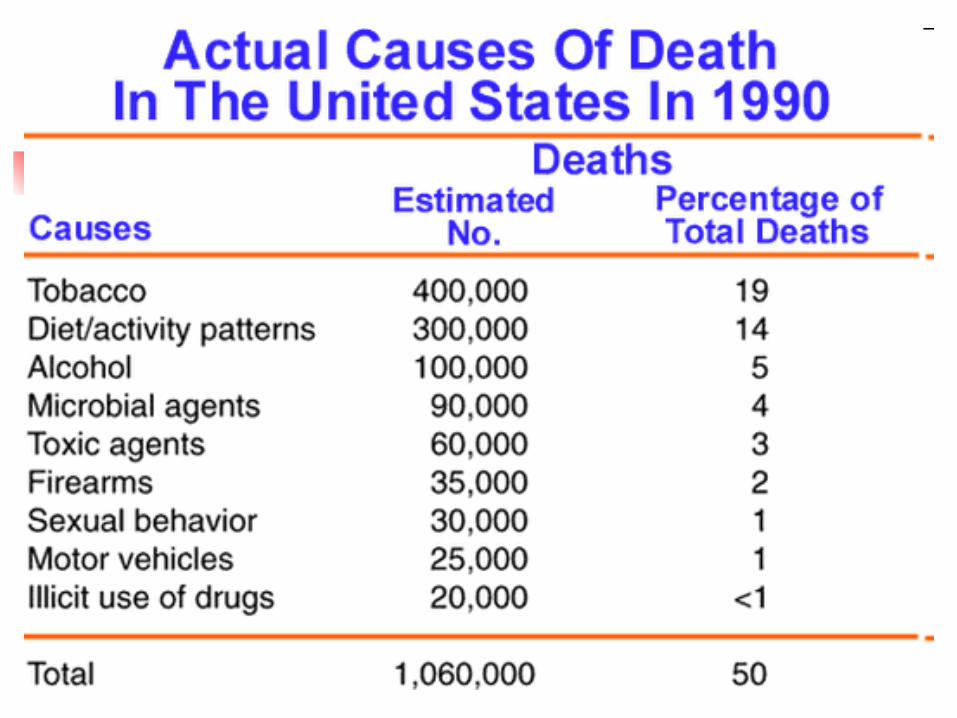
Coronary syndromes have exploded since the early 1920’s
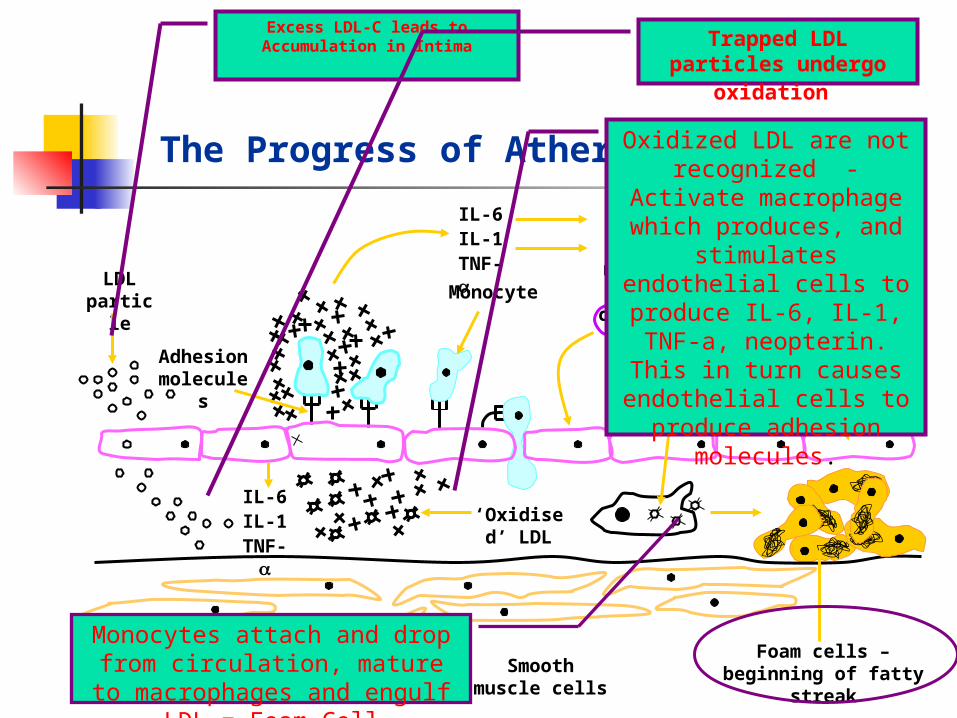
The Progress of Atherosclerosis
Foam cells – beginning of fatty streak
Endothelial cell
Activated macrophage
T-cell
Adhesion molecules
LDL particle
IL-6IL-1
TNF-
Smooth muscle cells
‘Oxidised’ LDL
Monocyte
IL-6IL-1TNF-
LiverBone marrow
Excess LDL-C leads to Accumulation in Intima Trapped LDL
particles undergo oxidation
Oxidized LDL are not recognized - Activate
macrophage which produces, and
stimulates endothelial cells to produce IL-6, IL-1, TNF-a, neopterin. This
in turn causes endothelial cells to produce adhesion
molecules.
Monocytes attach and drop from circulation, mature to
macrophages and engulf LDL = Foam Cell
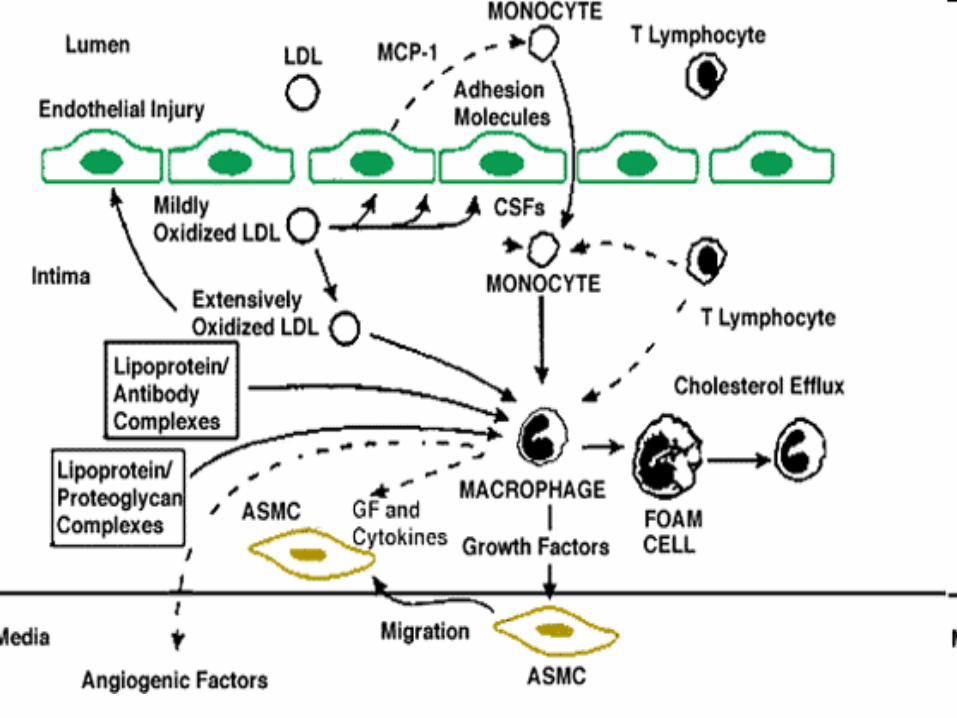
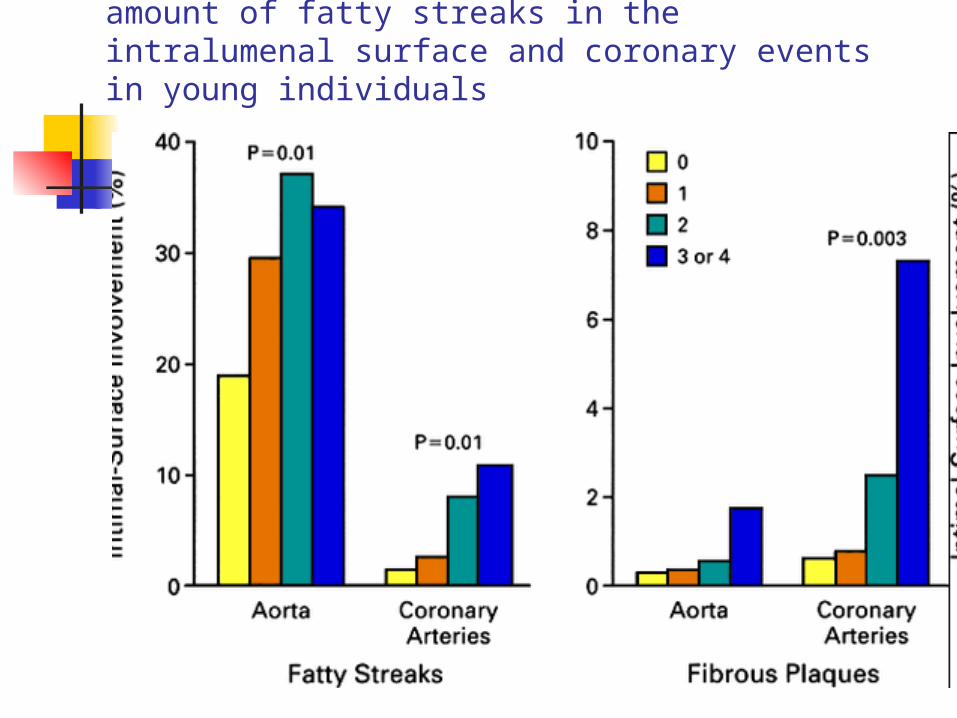
There is a direct correlation between the amount of fatty streaks in the intralumenal surface and coronary events in young individuals
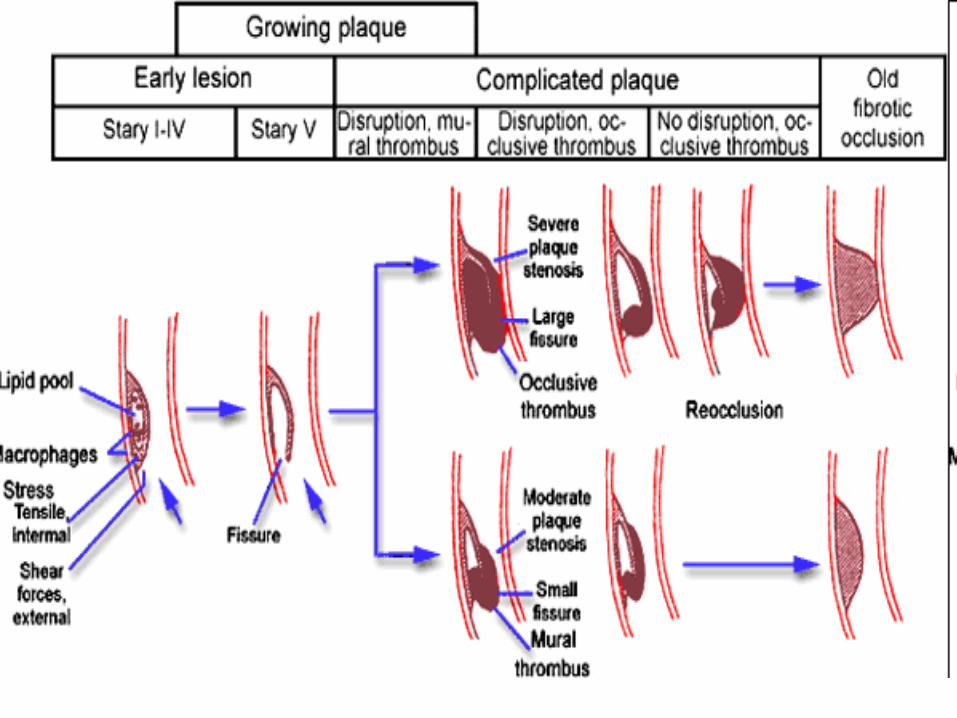
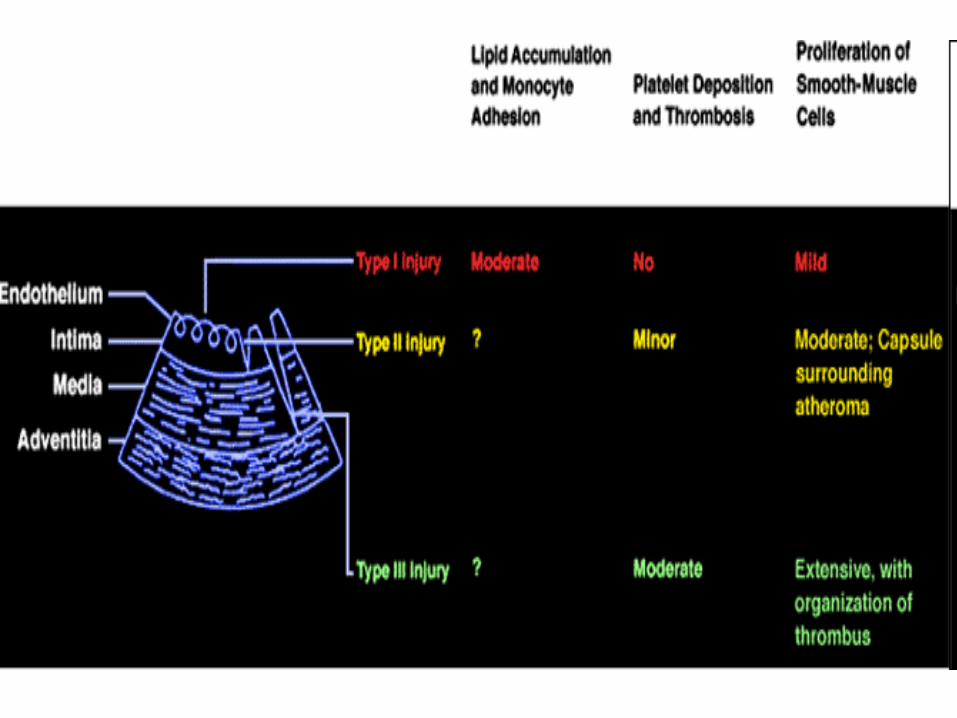
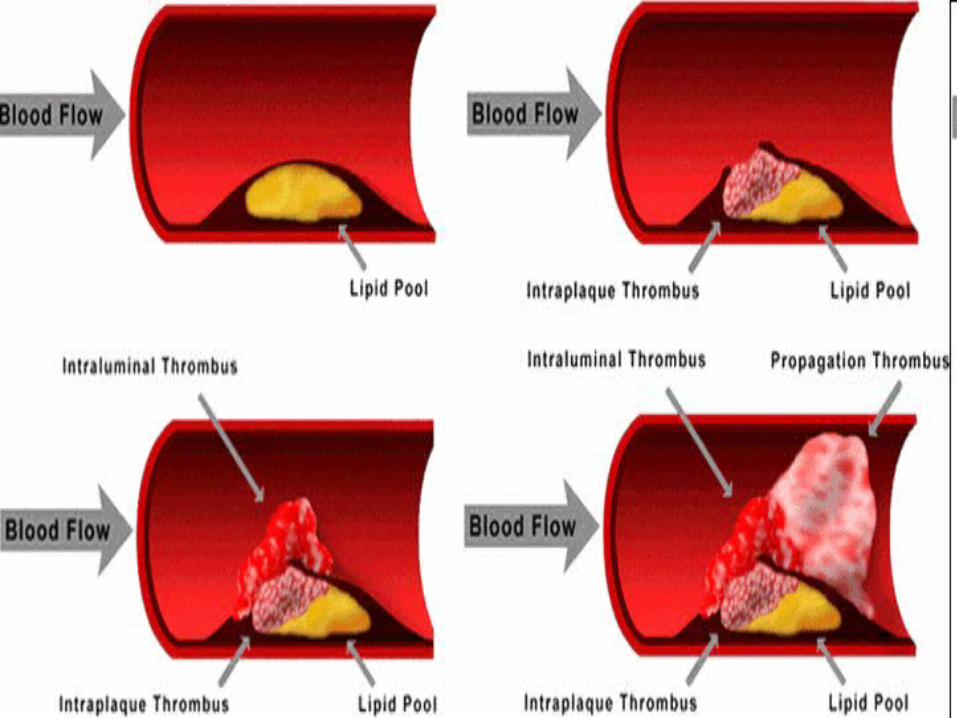
Pathophysiology Atherosclerotic plaques rich in foam cells
that are susceptible to sudden plaque rupture and hemorrhage into the vessel wall, which may result in the sudden partial or total occlusion of the coronary artery.
After total occlusion myocardial necrosis is complete in 4-6 hours. Flow to ischemic area must remain above 40% of pre-occlusion levels for that area to survive.
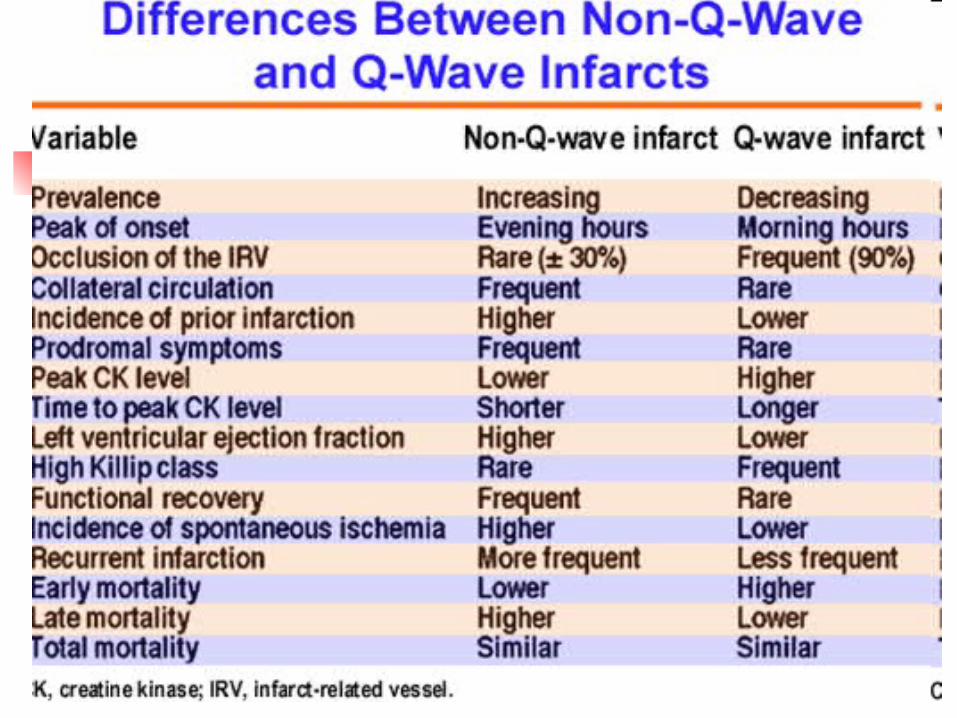
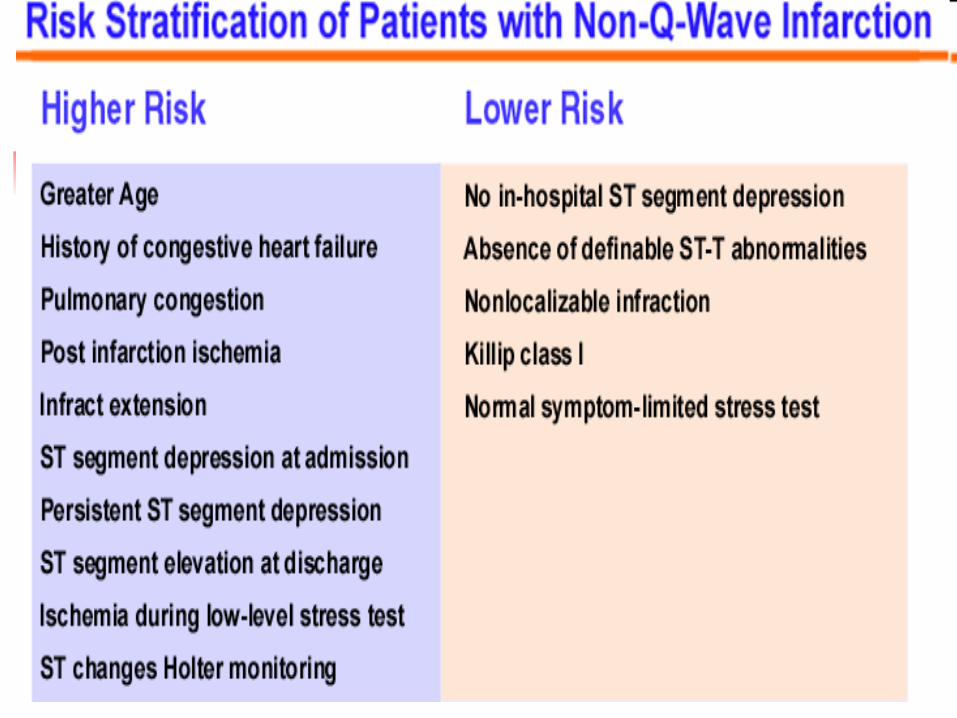
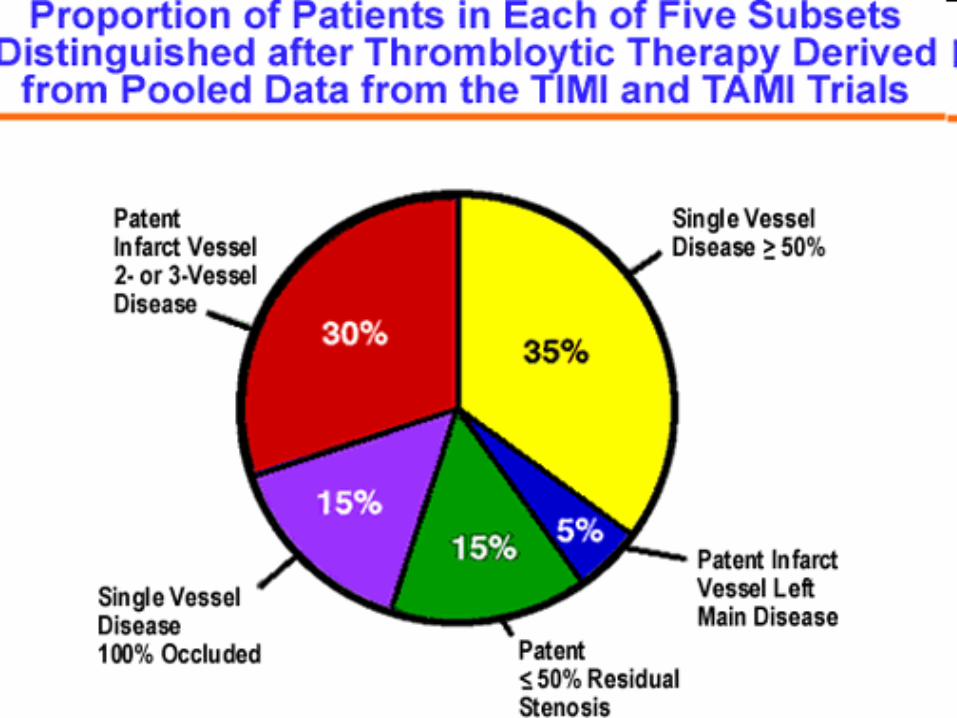
The infarctions can be divided into Q-wave and non Q-wave, with the former being transmural and associated with totally obstructed infarct-related artery and the latter being non-transmural and associated with patent
Total occlusion of the left main coronary artery which usually supplies 70% of the LV mass is catastrophic and results in death in minutes.
Common Signs/Symptoms
Pain - arm, back, jaw, epigastrium, neck, chest
AnxietyLightheadedness, pallor, weakness, syncopeNausea, vomiting, diaphoresisChest heaviness, tightness Cough, diaphoresis, dyspnea, rales, wheezing
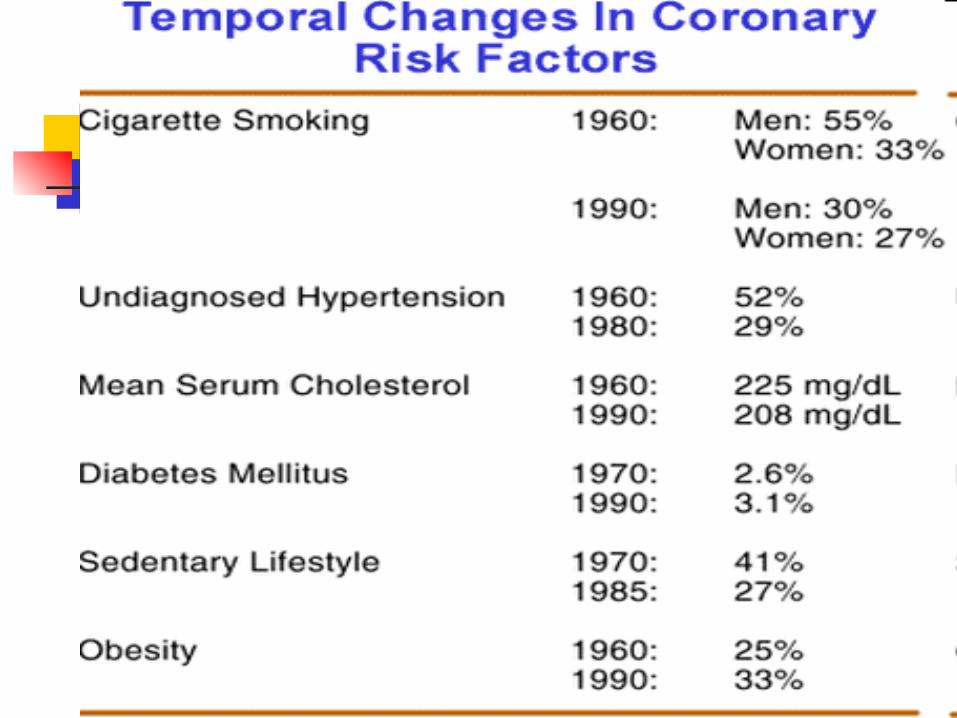
Pertinent Risk Factors Hypercholesterole
mia (increased LDL; decreased HDL)
Premature (<55) familial onset of coronary disease
Smoking Diabetes mellitus
Hypertension Sedentary life
style Aging Hostile, frustrated
personality Hypertriglyceride
mia Obesity
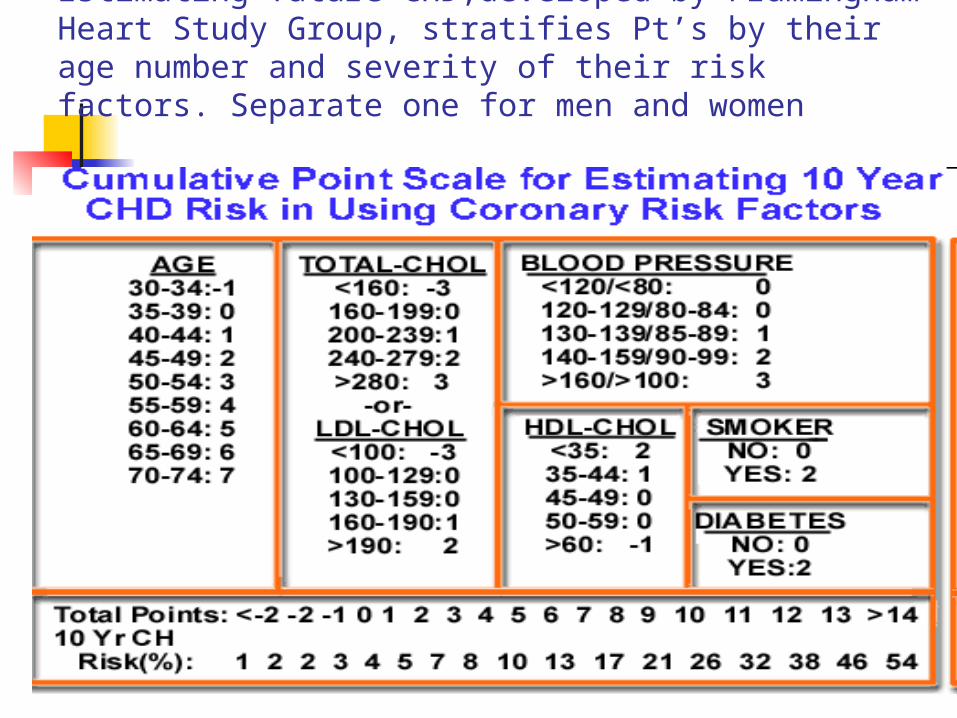
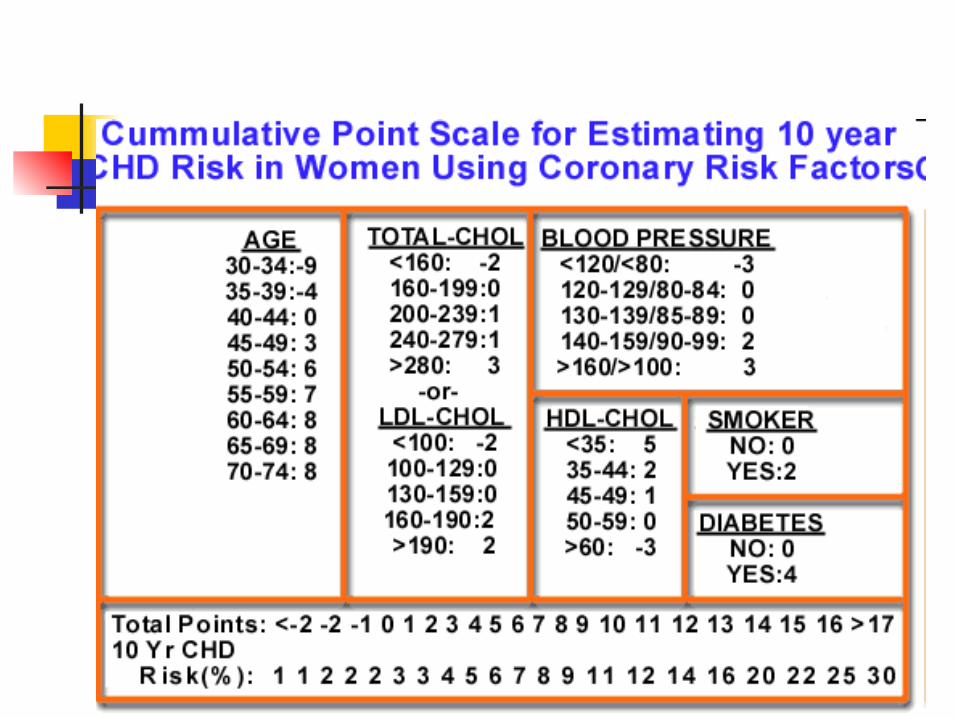
Estimating future CHD,developed by Framingham Heart Study Group, stratifies Pt’s by their age number and severity of their risk factors. Separate one for men and women
Physical Exam
S4/S3 heart sound
Arrhythmias Hypertension,
hypotension Levine’s sign Jugular venous
distention
Diaphoresis Pallor Bradycardia,
tachycardia, or irregular pulses
Fourth heart sound
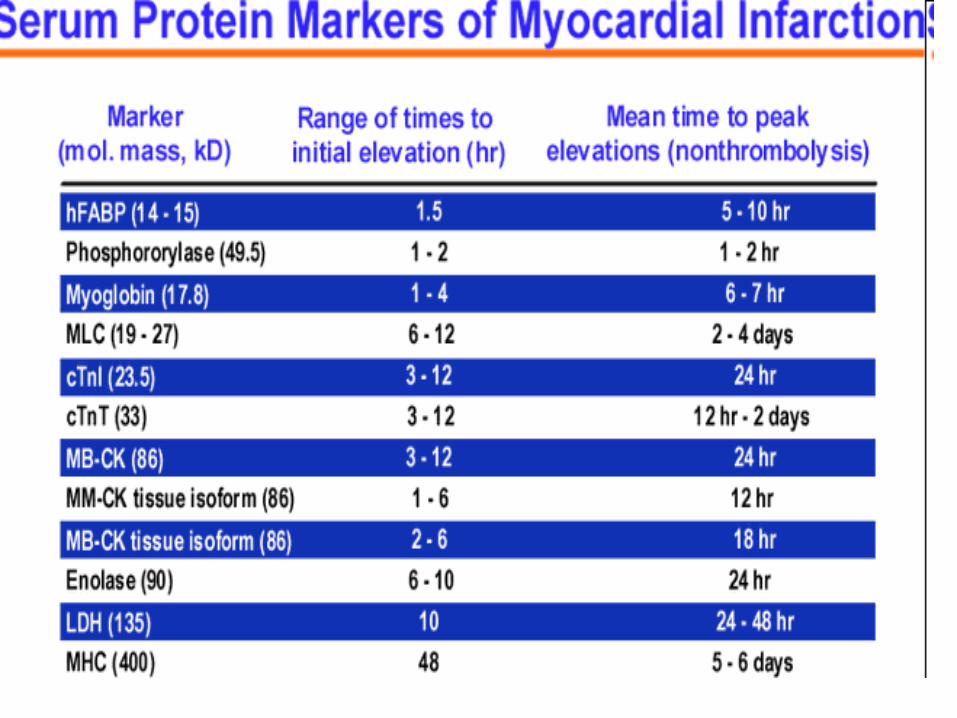
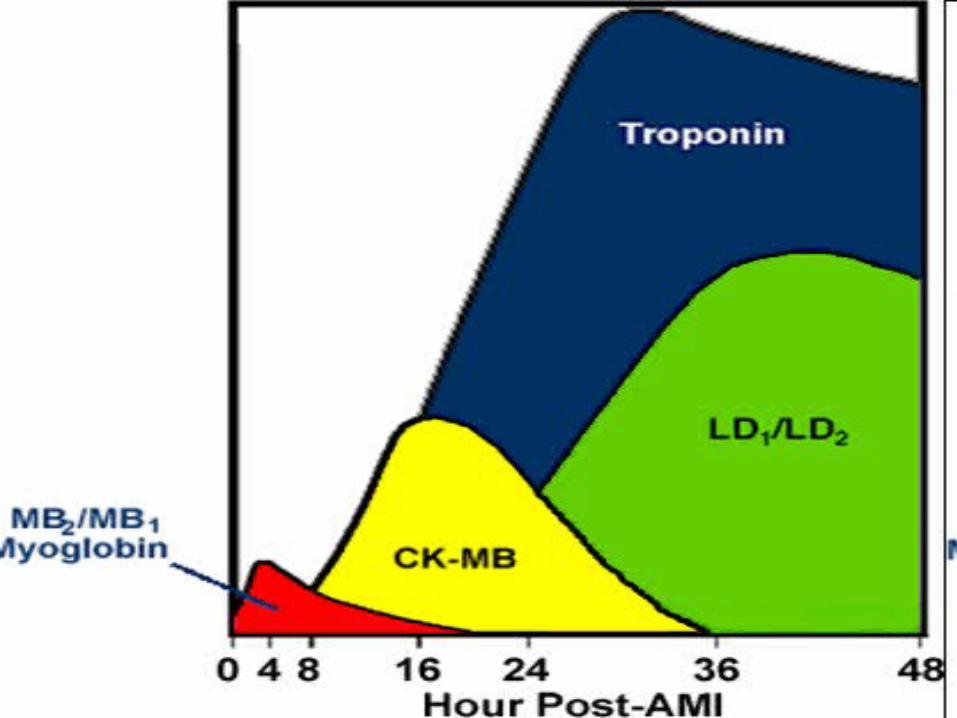
Serum Cardiac Markers A. cTnI/Troponin I
1.Becomes positive in 3-12 hours 2. Peaks at 24 hours 3. Remains elevated for 4-10 days 4. Highly sensitive for early detection of
myocardial injury 5. Can be used to help decide whether it
is safe to discharge patients who present to the emergency room with acute chest pain
Cont’d 6. Patients without ST segment
elevations during pain and 2 negative troponin I determinations (one at least 6 hours after the onset of symptoms) have a low risk of death or fatal acute MI (.3%) during the next 30 days.
Cont’d B.CKMB subforms, 1. CKMB1 (plasma) and CKMB2 (tissue)-
myocardial necrosis can be detected earlier with subform analysis then with traditional CKMB measurement.
2.Within 6 hours CKMB2 greater than 1.0 U/L with a ratio of CKMB2/CKMB1 greater than 1.5 is more sensitive and specific than CKMB for diagnosis of MI
Cont’d 3. If a patient presents more than
24 hours after a presumed MI, and the CK isoenzymes are inconclusive, troponin I is now preferred over LDH.
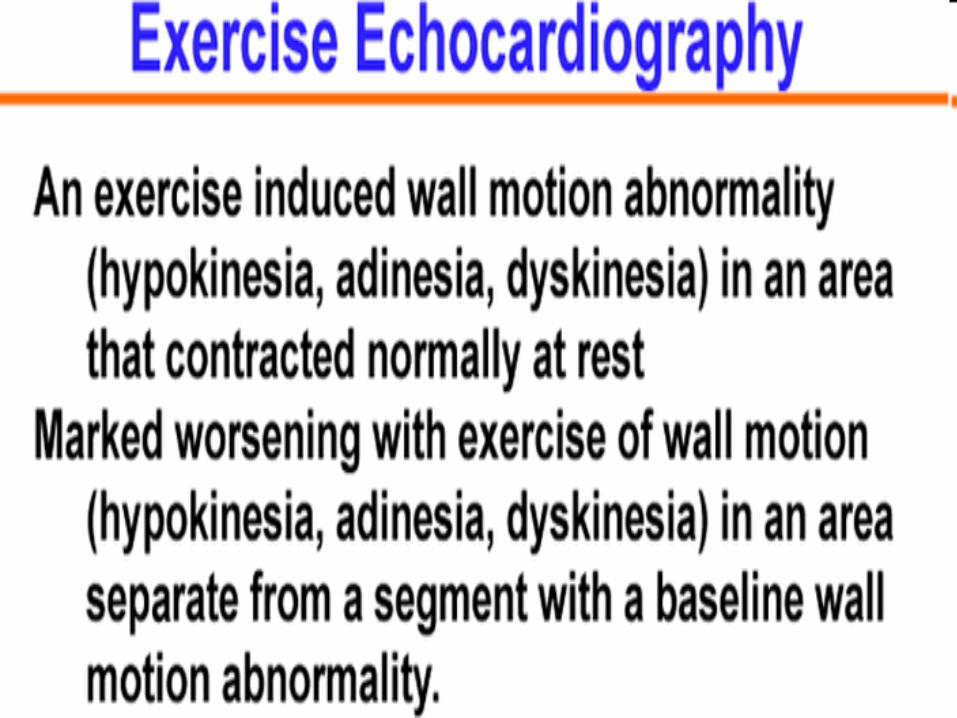
Early Assessment of Infarct Size A. Currently two dimensional echocardiography
is the technique used most frequently in the hospital course to evaluate acute MI infarction size.
B. Echo reveals 1. Extent and location of ventricular wall
abnormalities 2. Provides an assessment of overall ventricular
function 3. Demonstrates left ventricular thrombus 4. Color flow doppler provides information about the
extent of valvular disease and mechanical complications of acute MI.
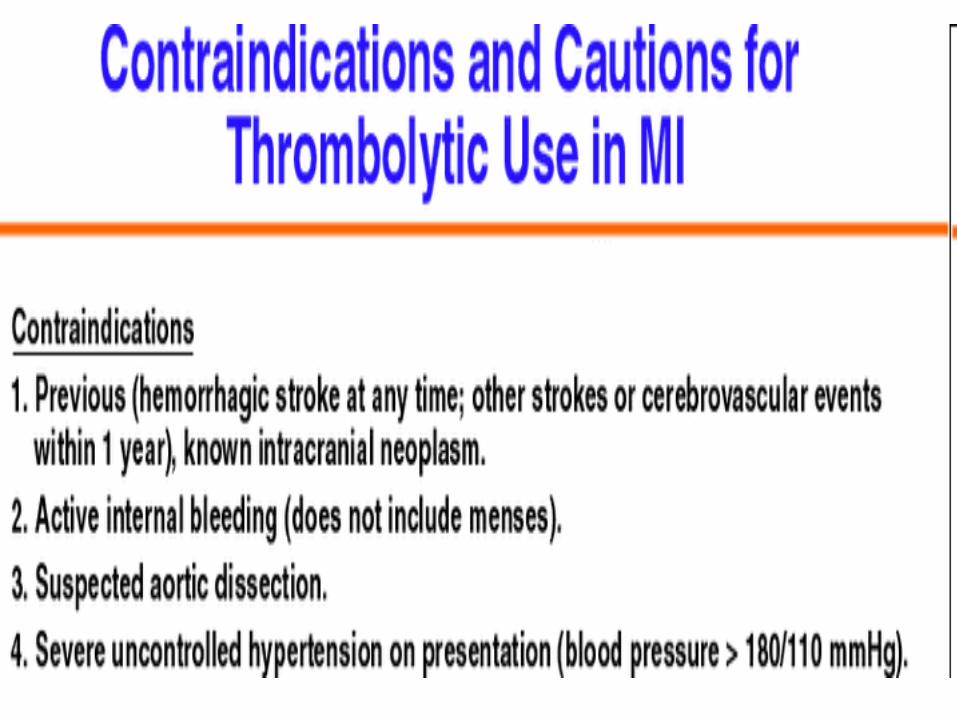
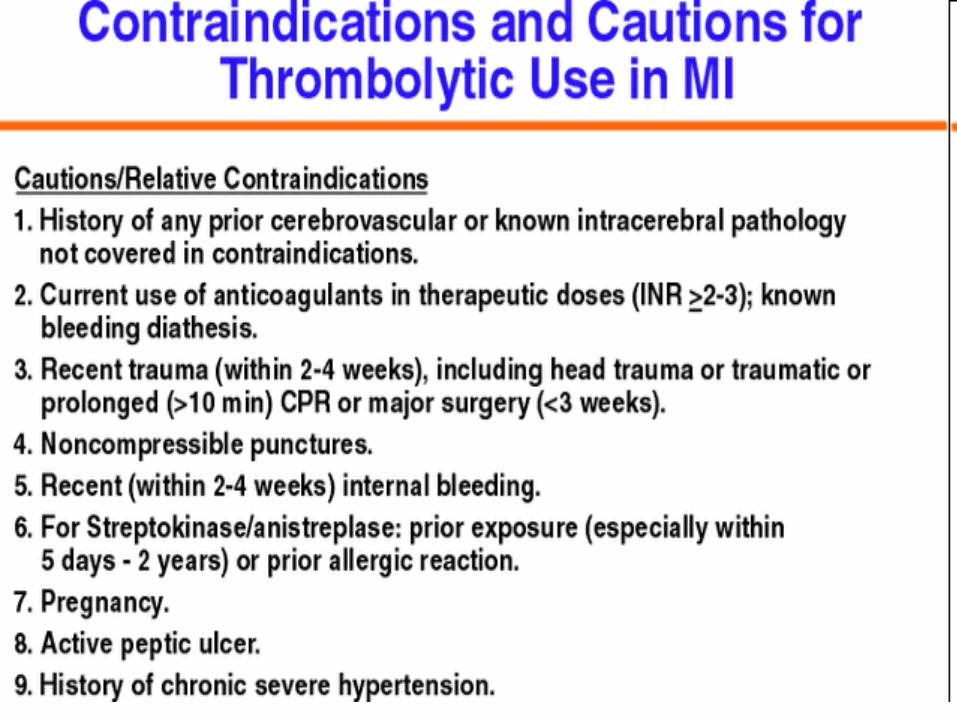
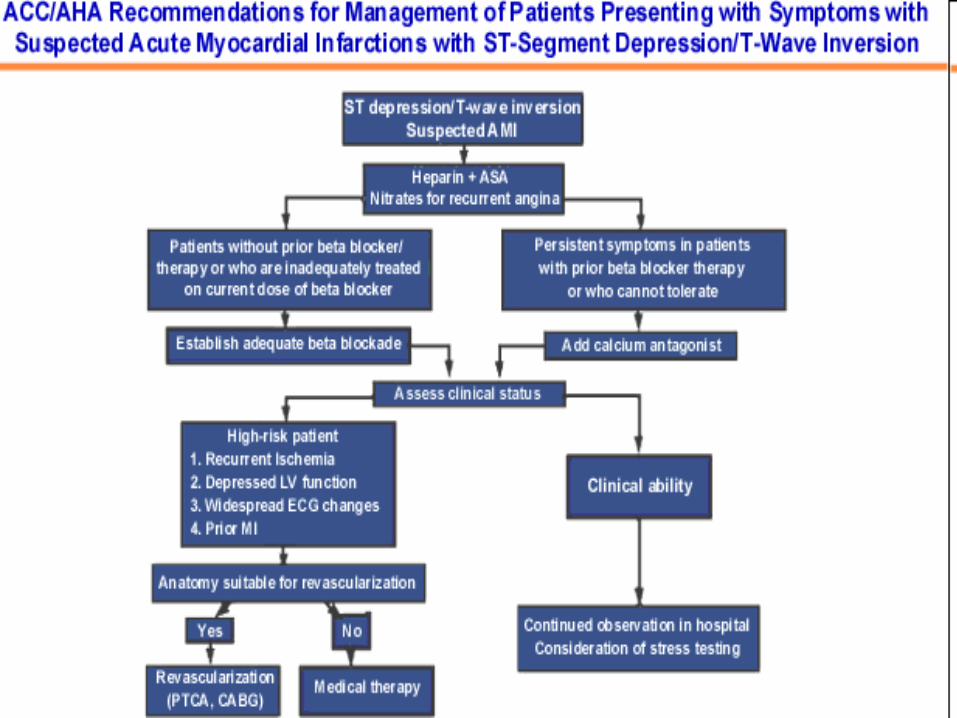
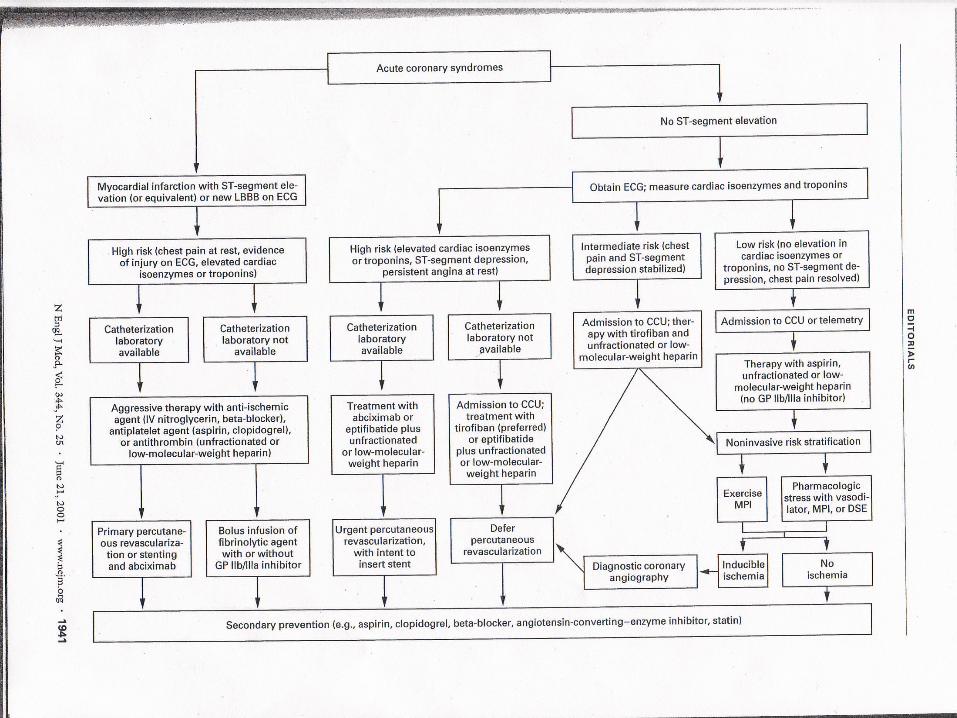
Approach to the patient with Acute MI A. History I. Aspirin B. Physical J. O2 C. EKG K. Thrombolytic
Therapy D. Enzymes L. Heparin E. Chest X-Ray M. Angiography F. Nitrates N. PTCA with stenting G. Beta-Blockers O. CABG H. Morphine P. GPIIB/IIIA
antagonists
Acute Reperfusion Therapy A. Rapid reperfusion of the infarct related
artery with IV thrombolytic therapy or primary PTCA is the main treatment strategy for acute MI. The main goal is to improve survival and outcome(decrease incidence of CHF). The benefit of reperfusion therapy are time dependent, the sooner the blood flow is restored to the ischemic zone, the greater the advantage in terms of survival and functional recovery.
Cont’d B. Risk of hemorrhage
1. Age greater than 65 2. Weight less than 70 kg. 3. Female 4. HypertensionAlthough patients greater than 75 years have
a greater risk of hemorrhage and stroke with thrombolytic therapy, they have a net benefit in overall outcome because of a significant mortality reduction with thrombolytic therapy.
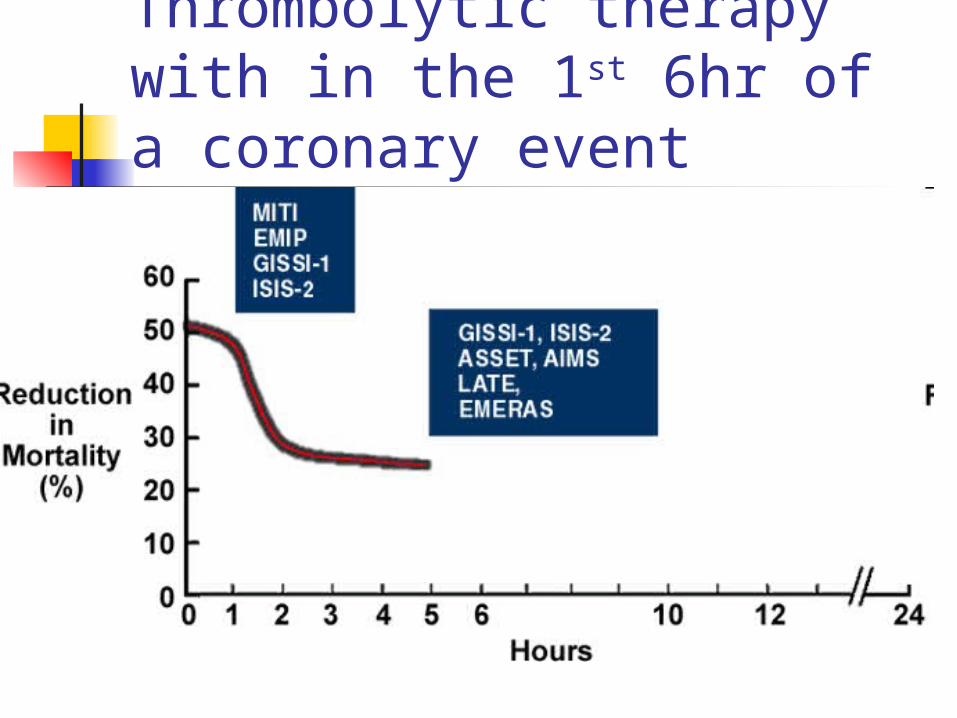
Thrombolytic therapy with in the 1st 6hr of a coronary event
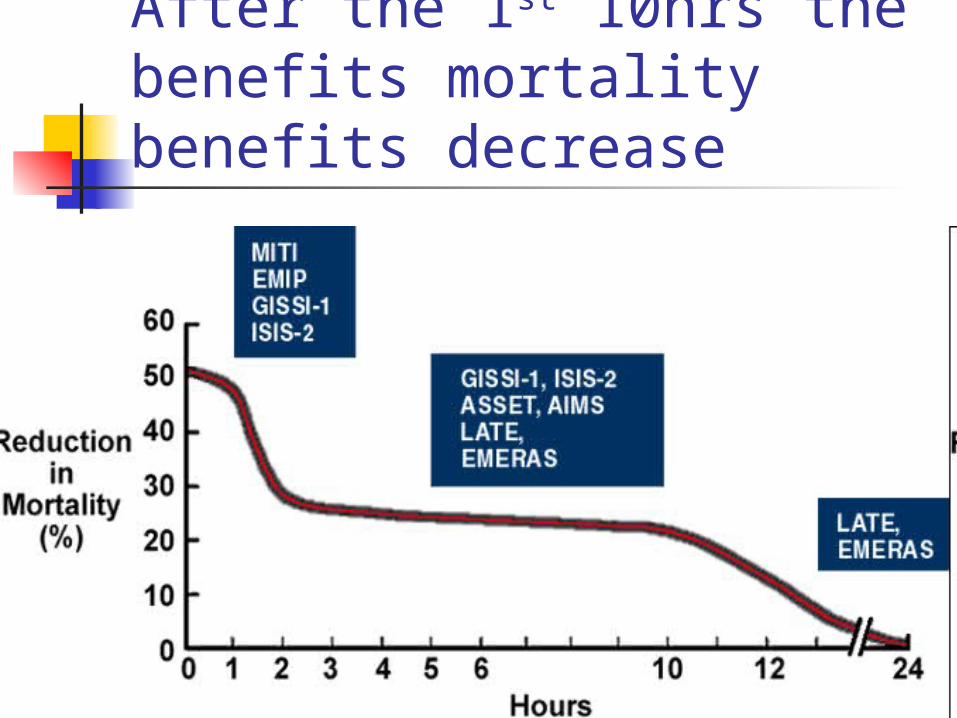
After the 1st 10hrs the benefits mortality benefits decrease
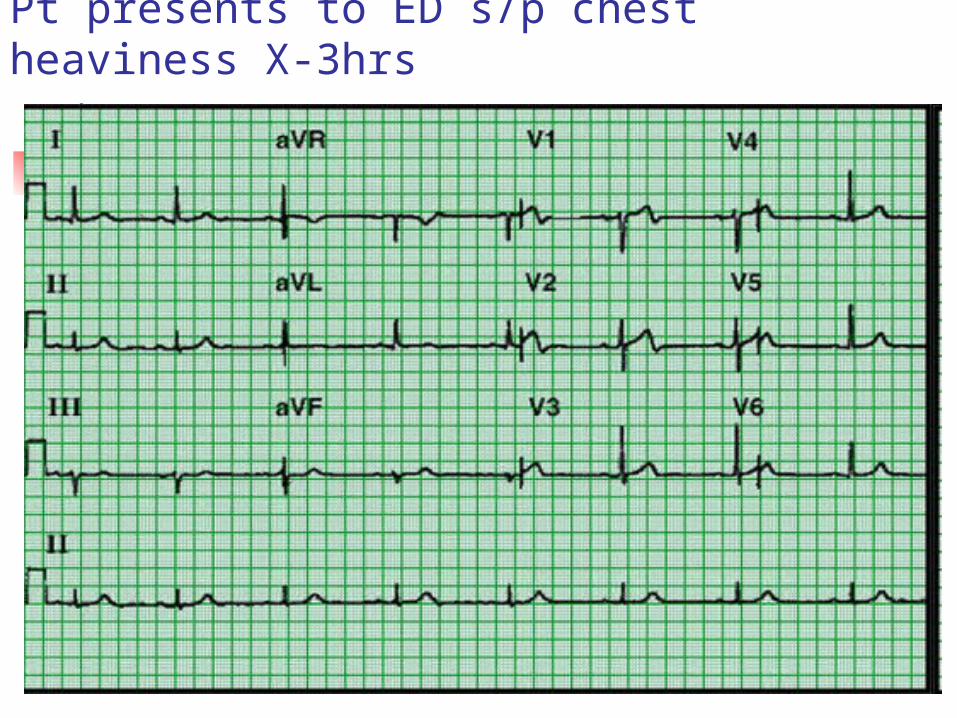
Pt presents to ED s/p chest heaviness X-3hrs
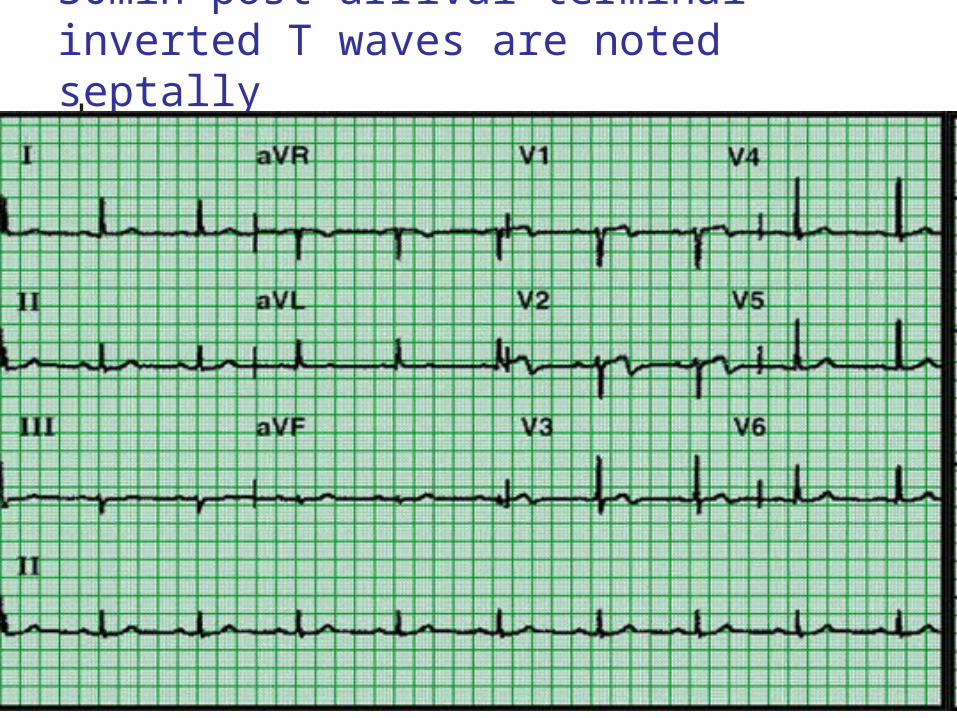
30min post arrival terminal inverted T waves are noted septally
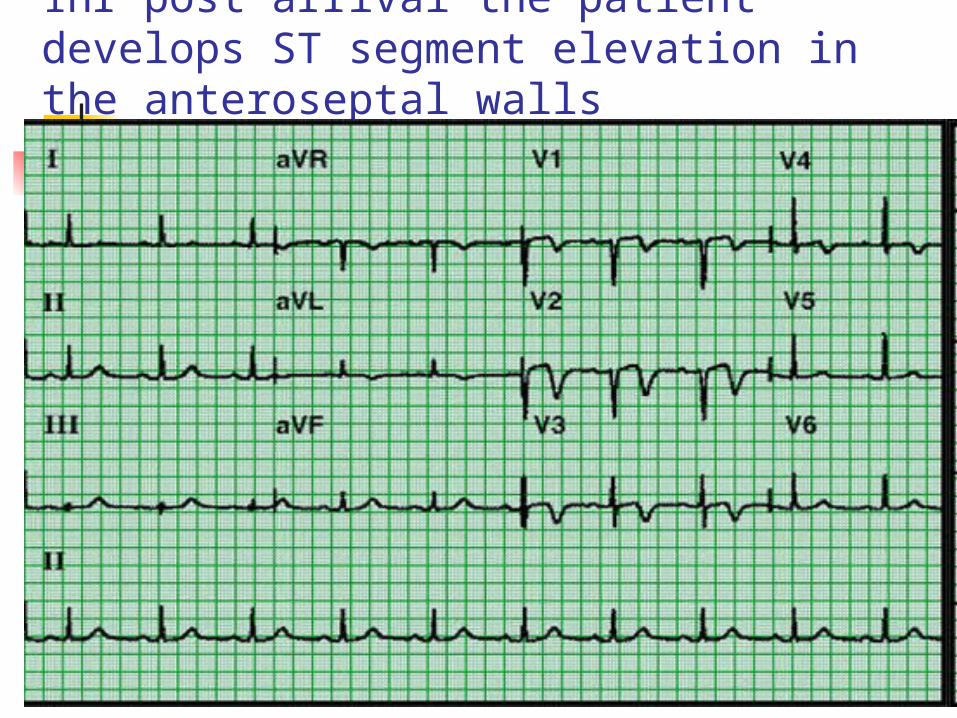
1hr post arrival the patient develops ST segment elevation in the anteroseptal walls
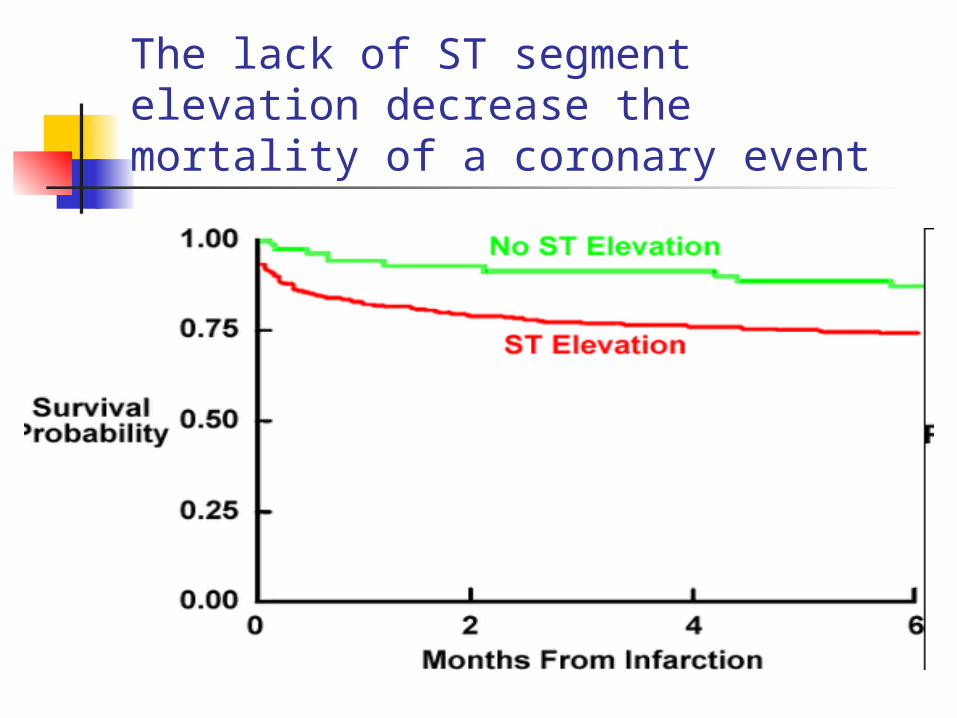
The lack of ST segment elevation decrease the mortality of a coronary event
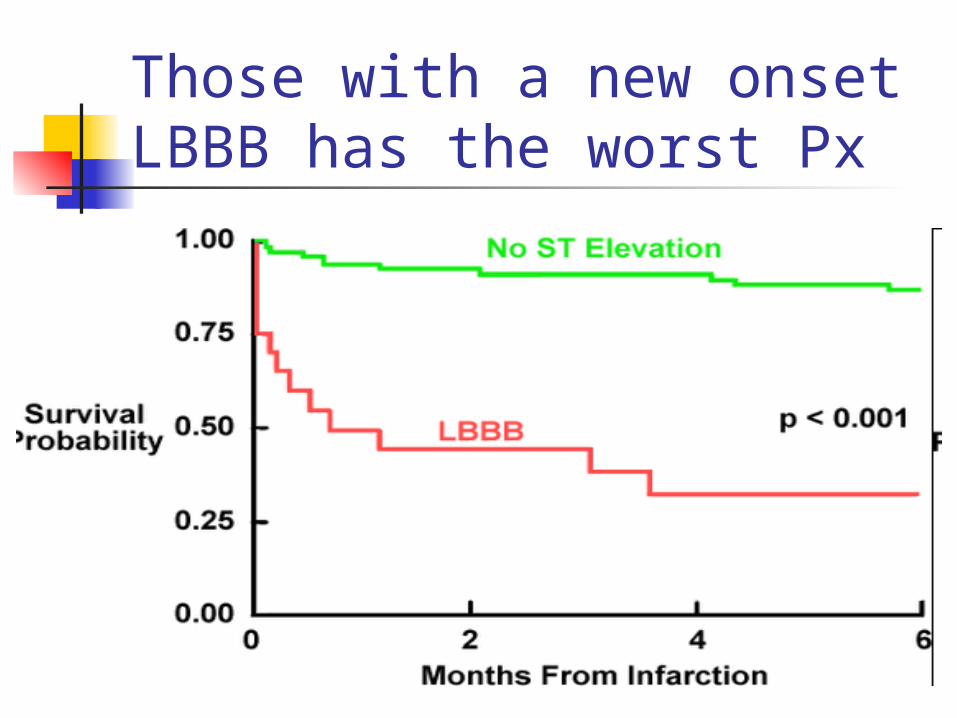
Those with a new onset LBBB has the worst Px
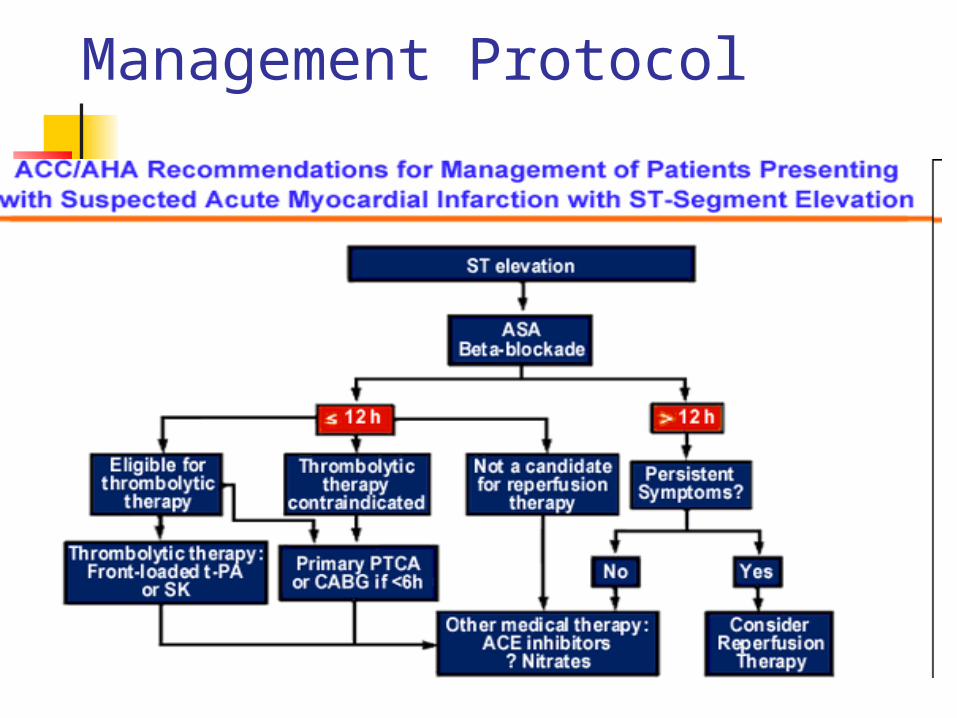
Management Protocol
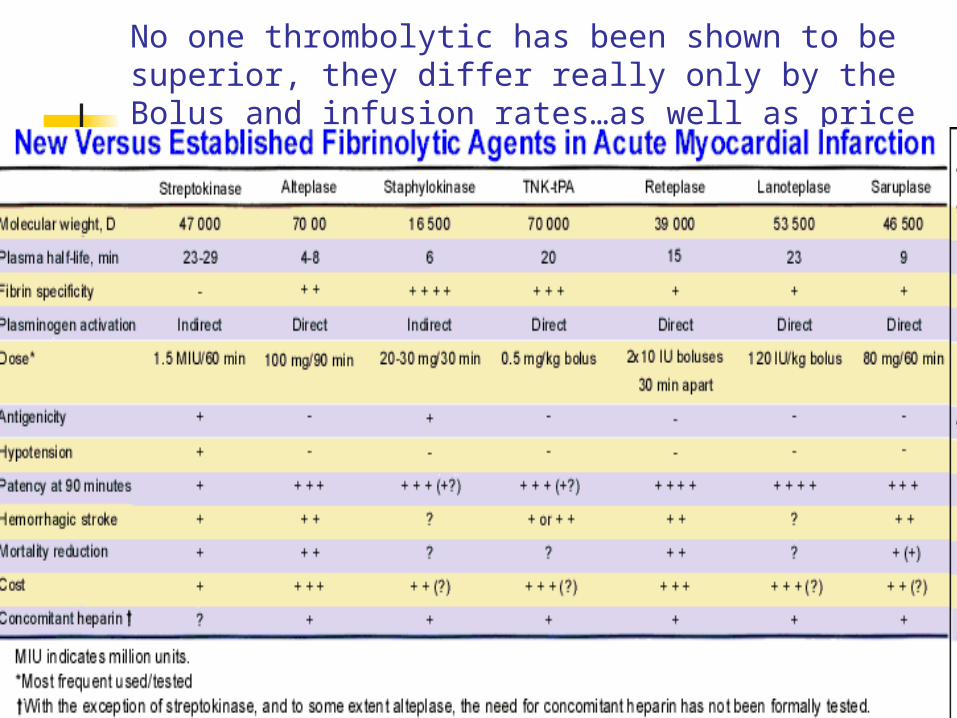
No one thrombolytic has been shown to be superior, they differ really only by the Bolus and infusion rates…as well as price
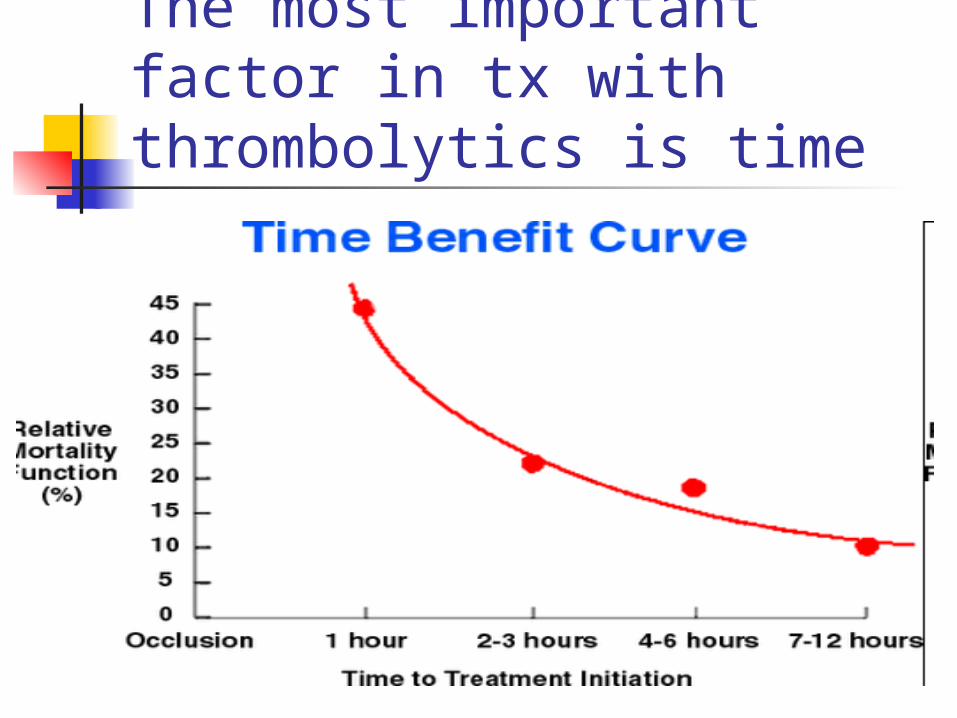
The most important factor in tx with thrombolytics is time
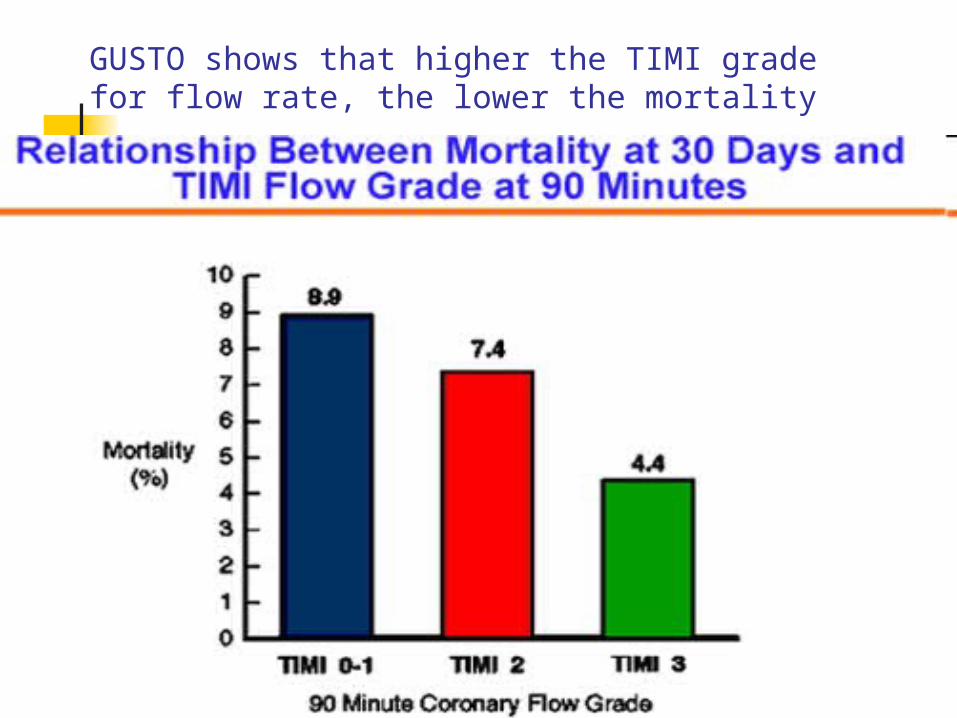
GUSTO shows that higher the TIMI grade for flow rate, the lower the mortality
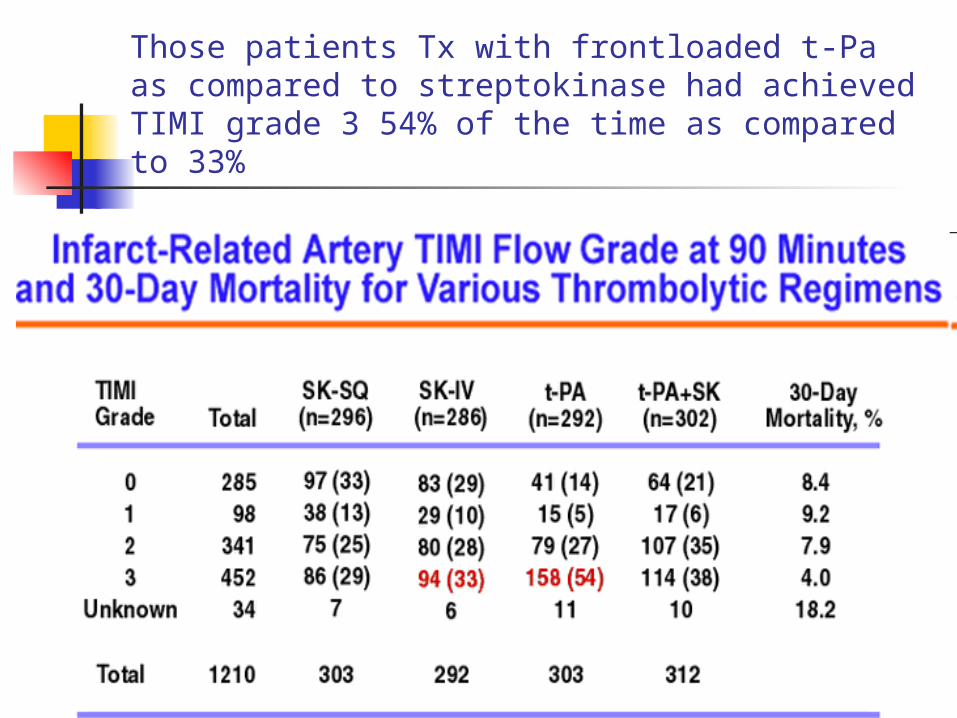
Those patients Tx with frontloaded t-Pa as compared to streptokinase had achieved TIMI grade 3 54% of the time as compared to 33%
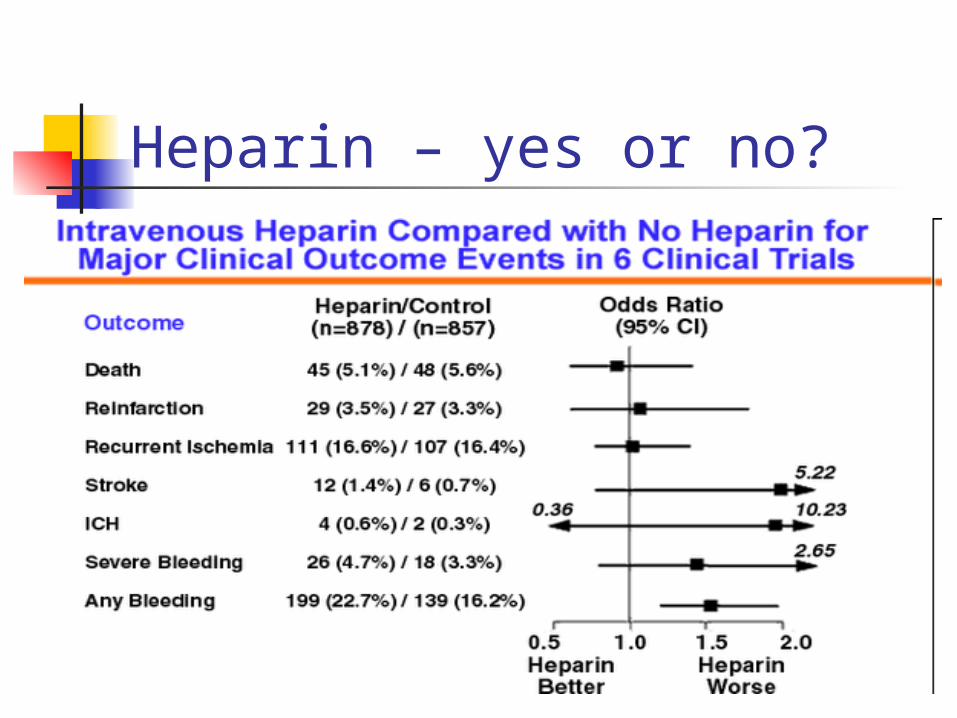
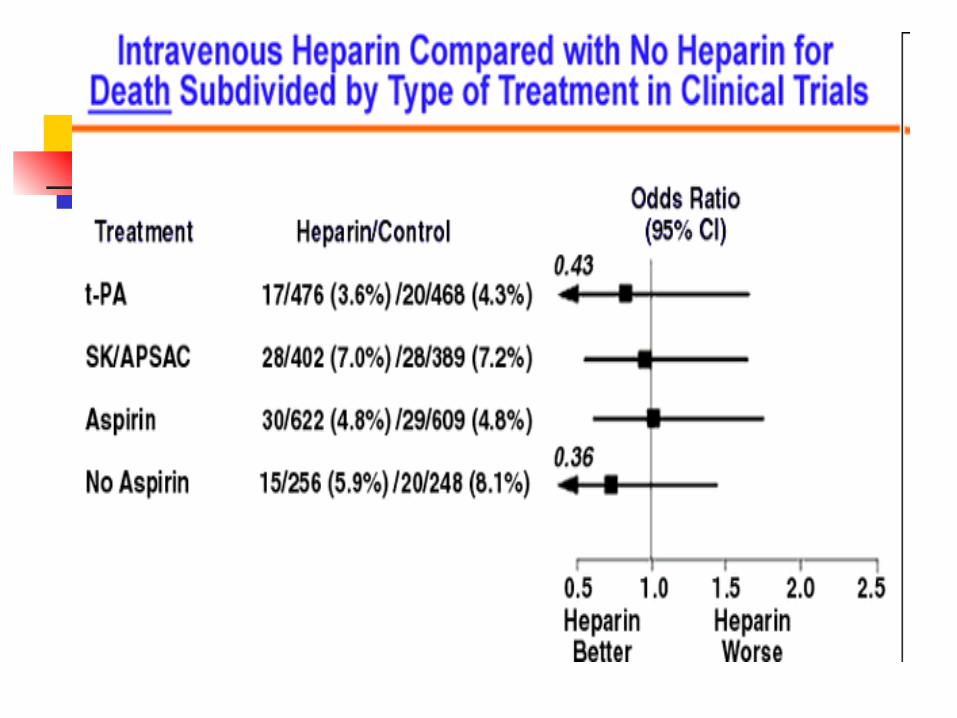
Heparin – yes or no?
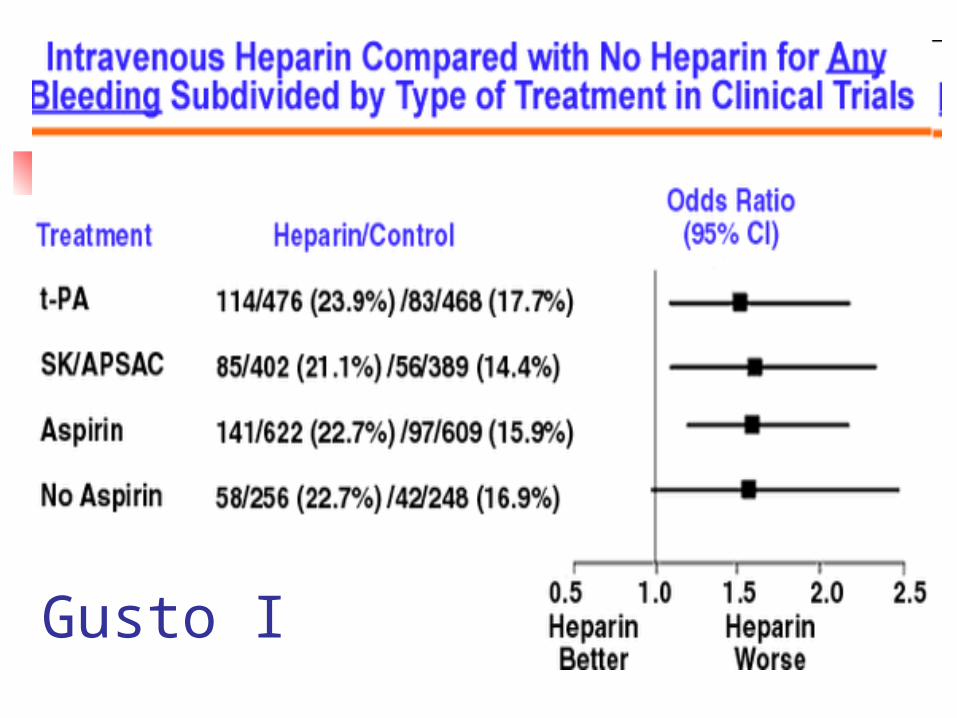
Gusto I
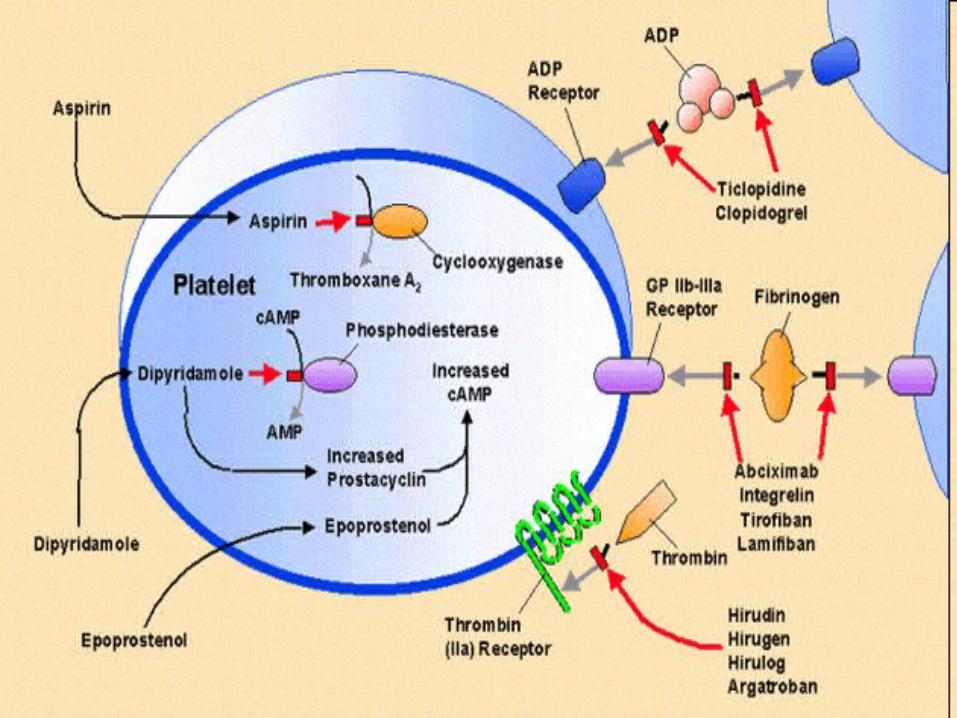
Pharmacokinetics ASA GP IIb IIIa Ticlopidine Anti-Thrombins Dipyridomol Epoprostenol
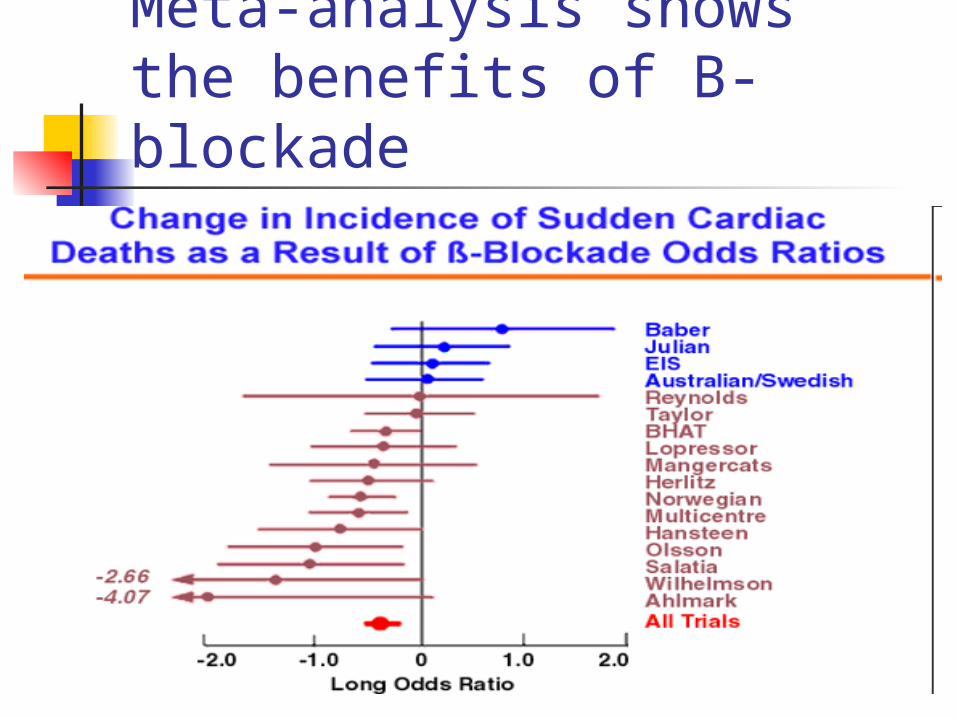
Meta-analysis shows the benefits of B-blockade
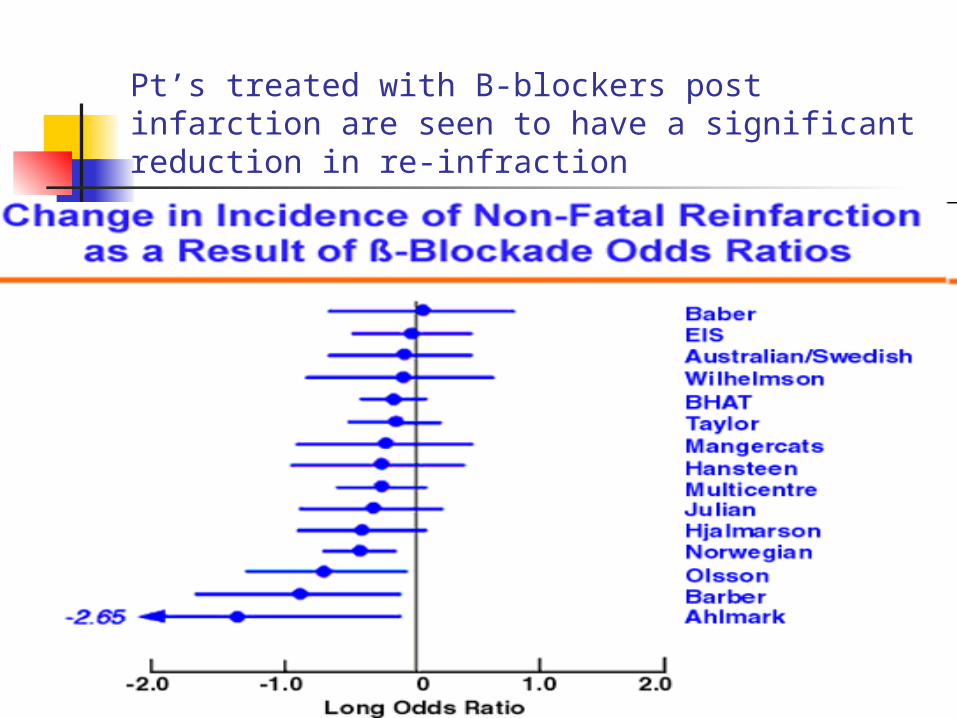
Pt’s treated with B-blockers post infarction are seen to have a significant reduction in re-infraction
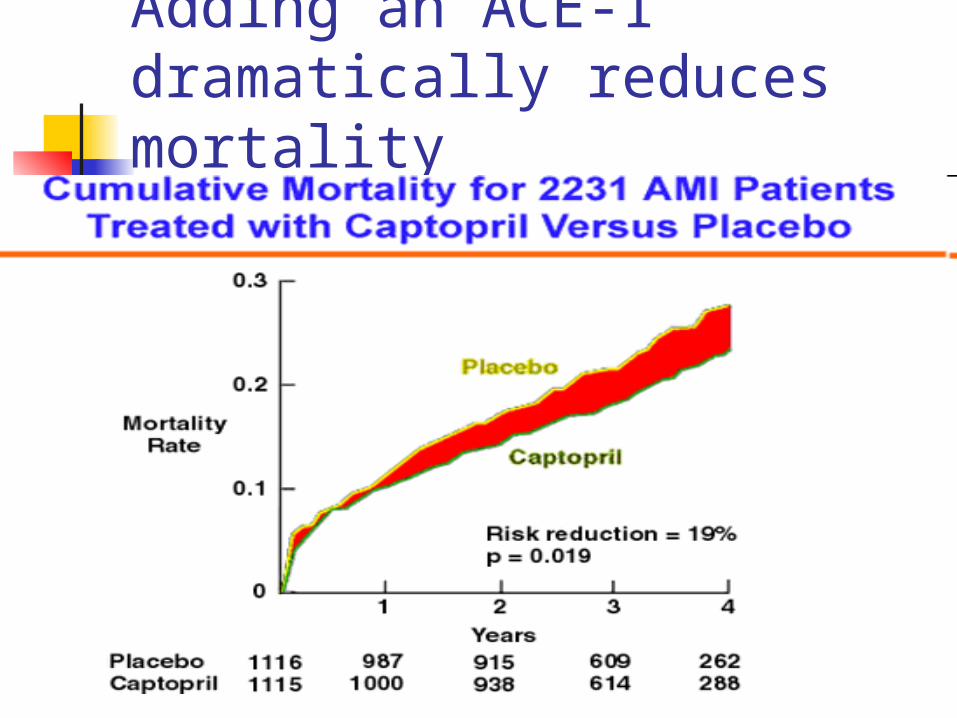
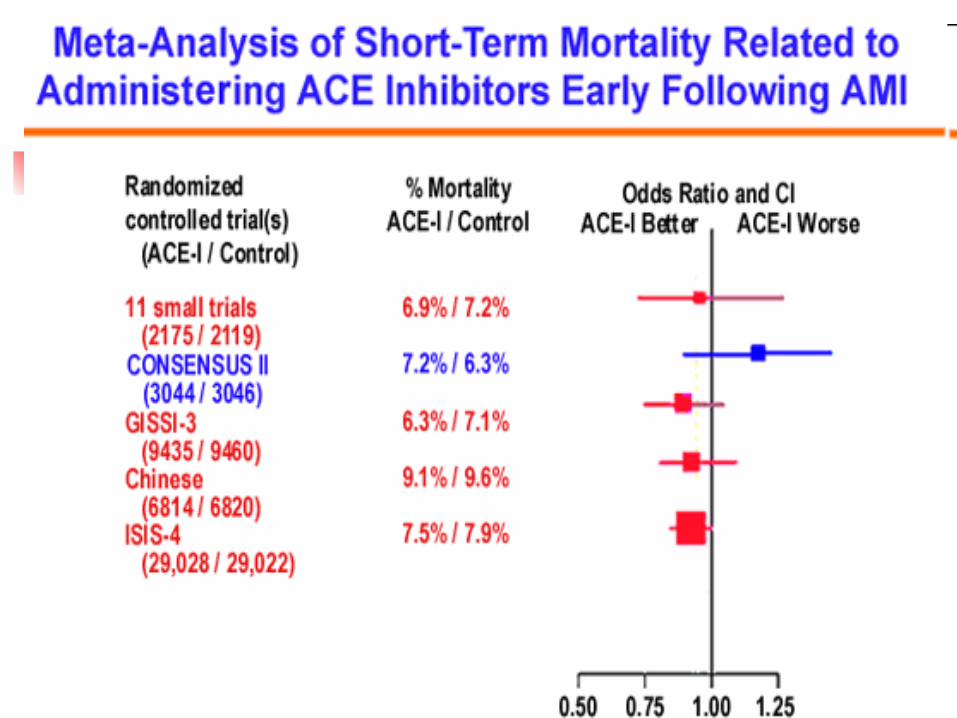
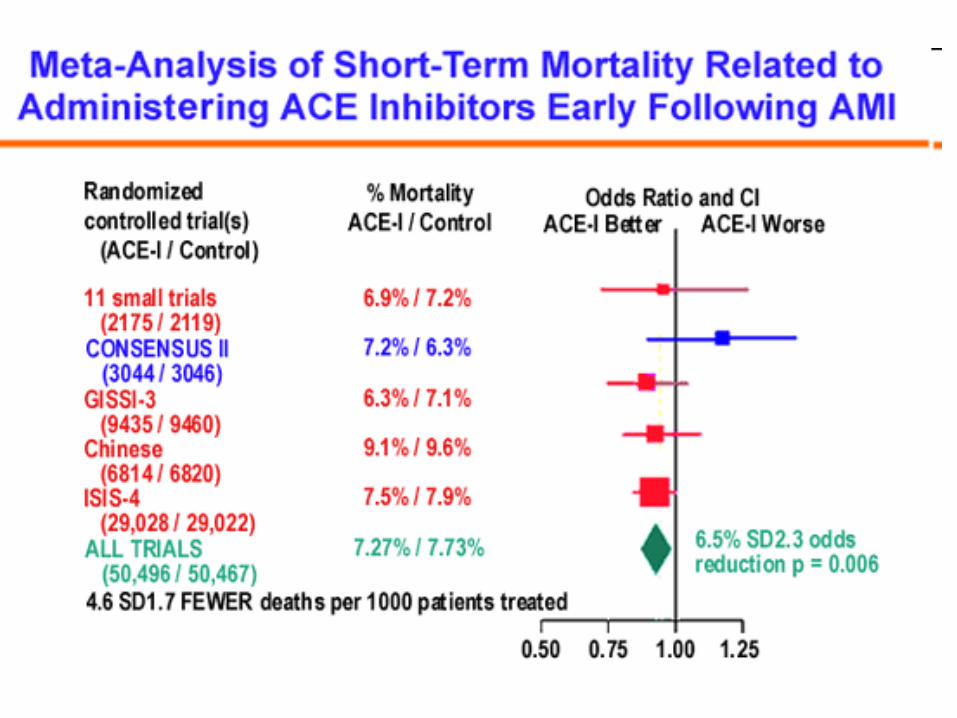
Adding an ACE-I dramatically reduces mortality
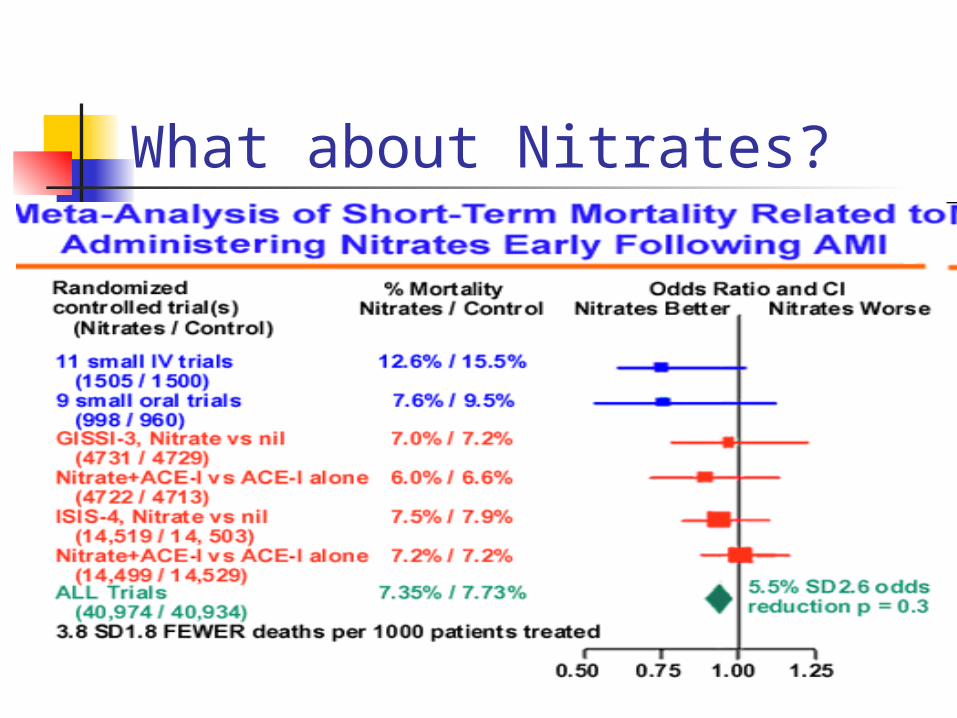
What about Nitrates?
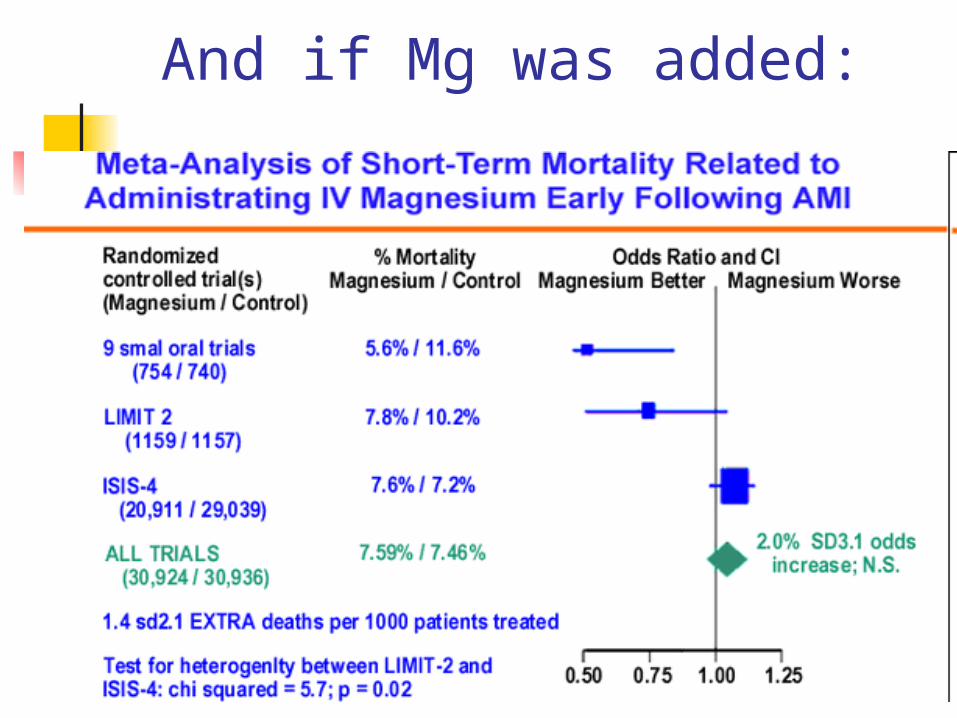
And if Mg was added:
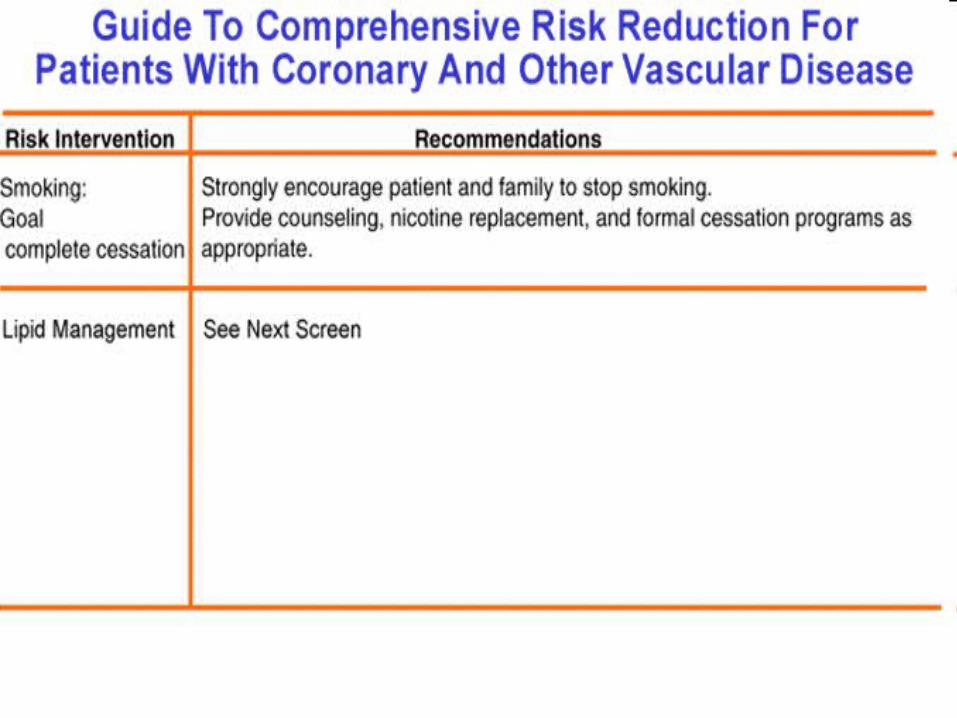
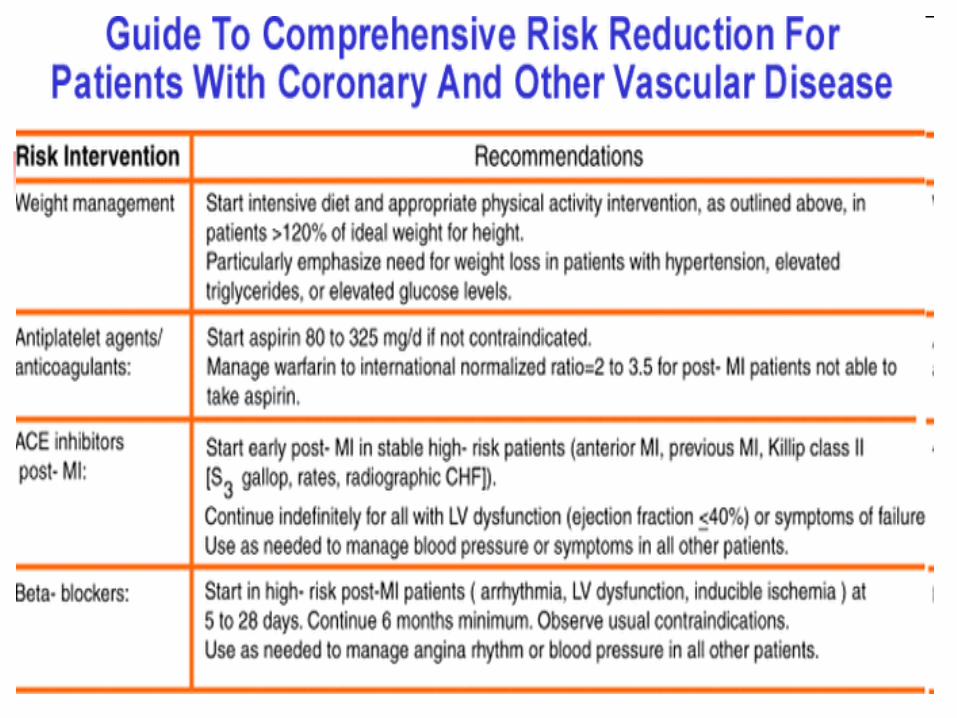
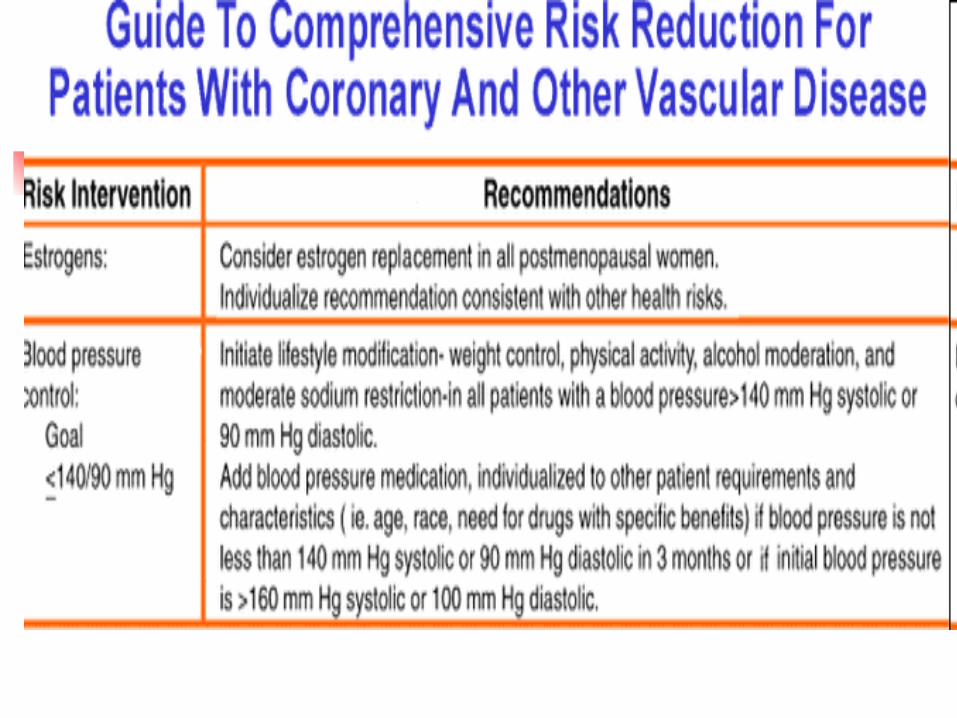
Rx d/c after MI
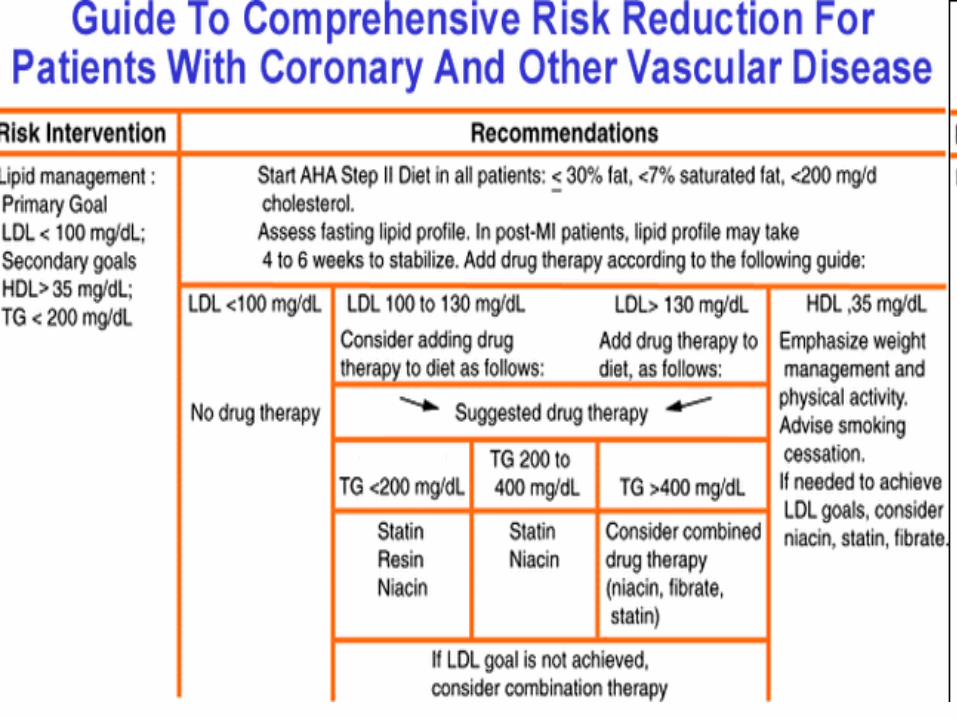
A. Beta-blocker B. ACE-Inhibitor or if not tolerated,
ARB C. Aspirin D. Lipid lowering drug- Statin E. Folic Acid, Vit B6, Vit B12 ? F. Clopidogrel
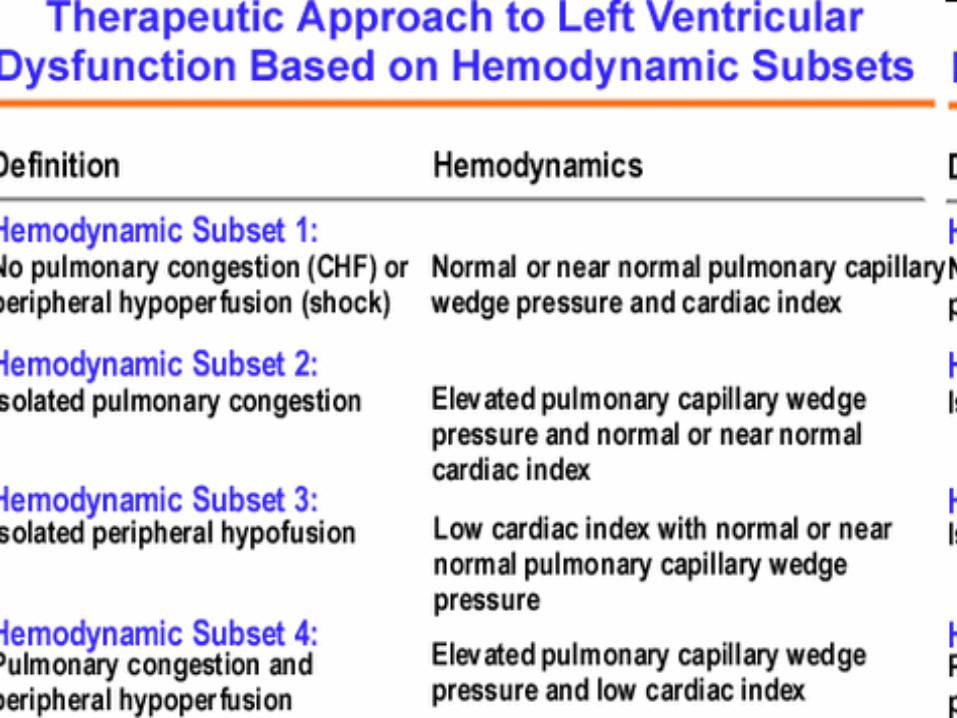
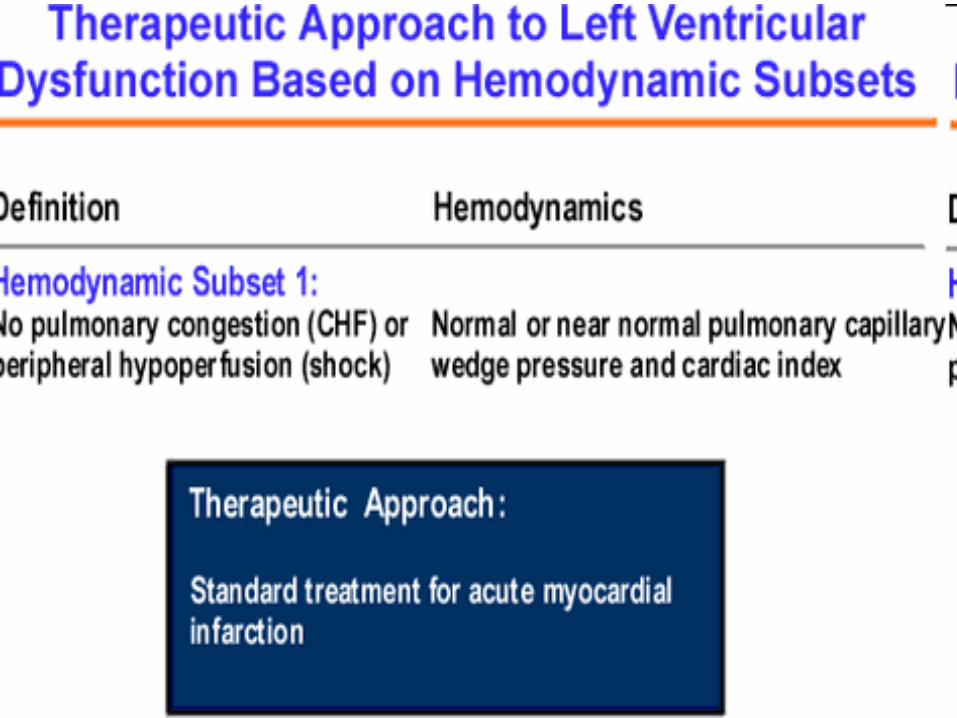
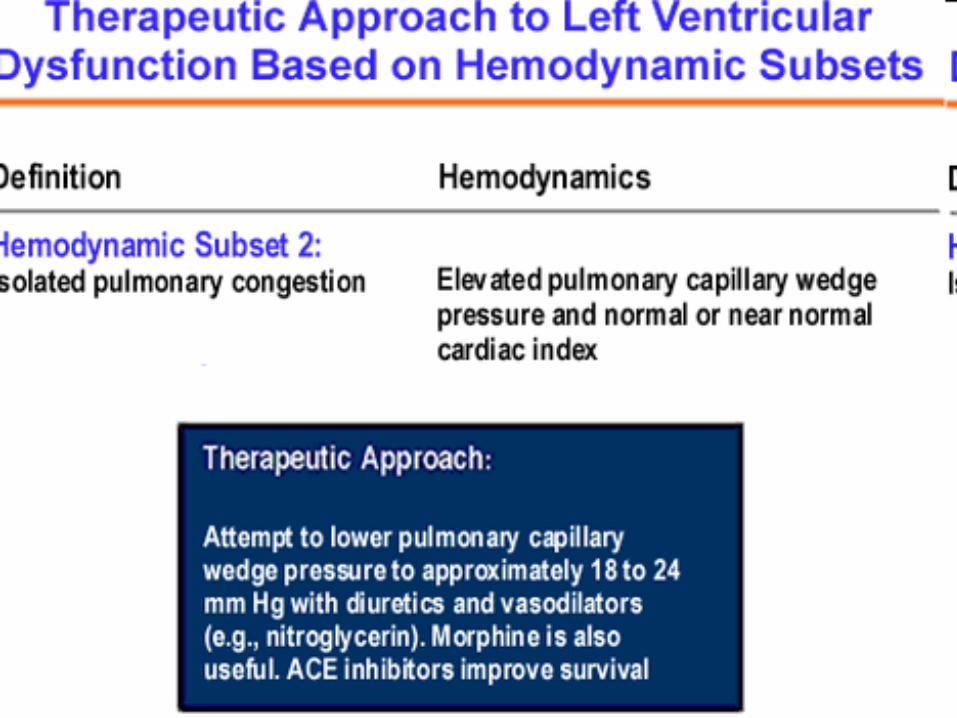
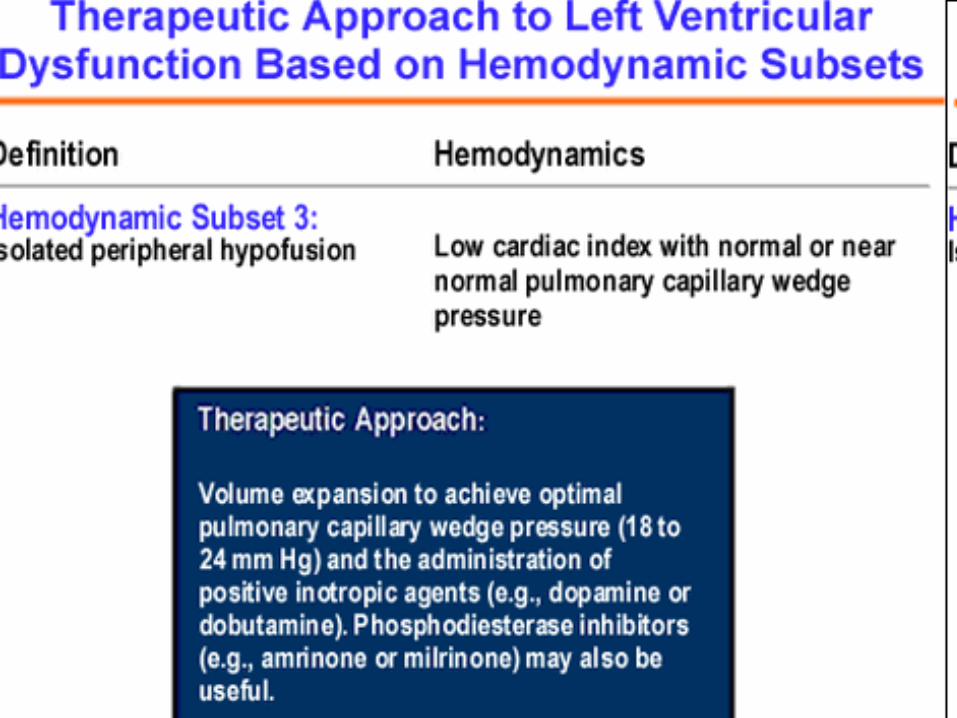
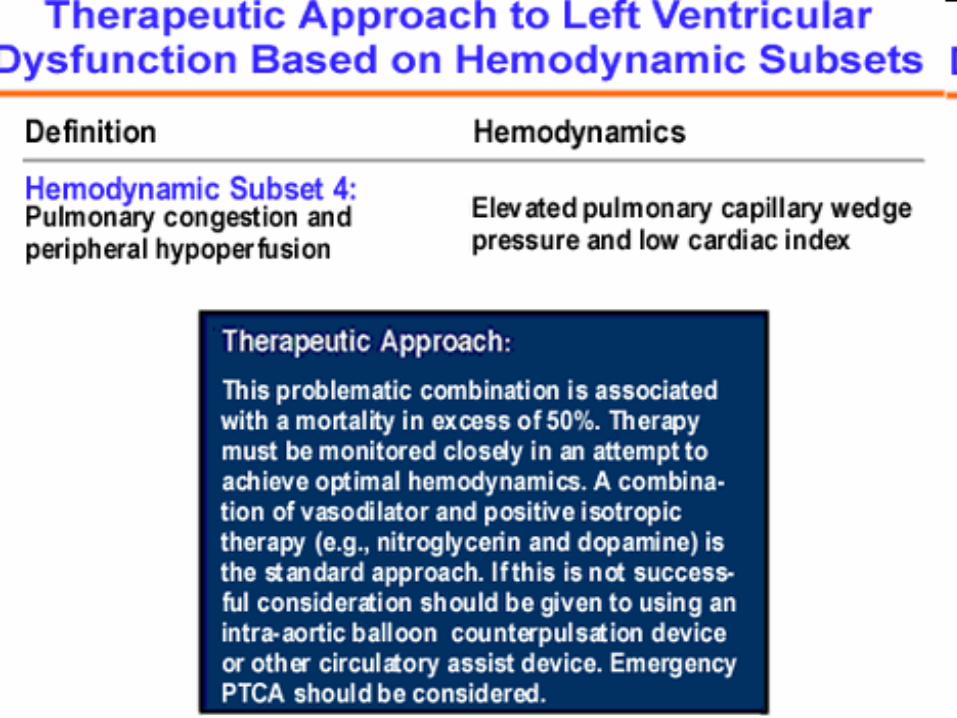
Hemodynamic Compromise A. Patients who develop hemodynamic
compromise (CHF, Hypotension, Cardiogenic shock) following AMI have a worse prognosis than those with little or no hemodynamic impairment.
B. Management of hemodynamic compromise is aided by balloon flotation Swan-Ganz catheter. This catheter makes it possible to measure cardiac output and PCWP that reflect LVEDP and helps the physician adjust therapy according to the patients hemodynamic subset
Right Ventricular Infarction A. Nearly 50% of patients with inferior
wall MI have some evidence of right ventricular ischemia or infarction (It is hemodynamically significant in only about 10% of these patients).
B. Should be suspected with inferior MI when patient presents with a triad of hypotension, clear lung fields, and jugular venous distention (right atrial pressure greater than 10 mmHg).
Cont’d C. Right sided EKG should be done in
patients with inferior wall myocardial infarction.
D. Treatment 1. Reperfusion therapy 2. Increasing preload by volume expansion(1
or more Liters of normal saline) 3. Cautious administration of Dobutamine 4. Diuretics and Vasodilators should be
avoided
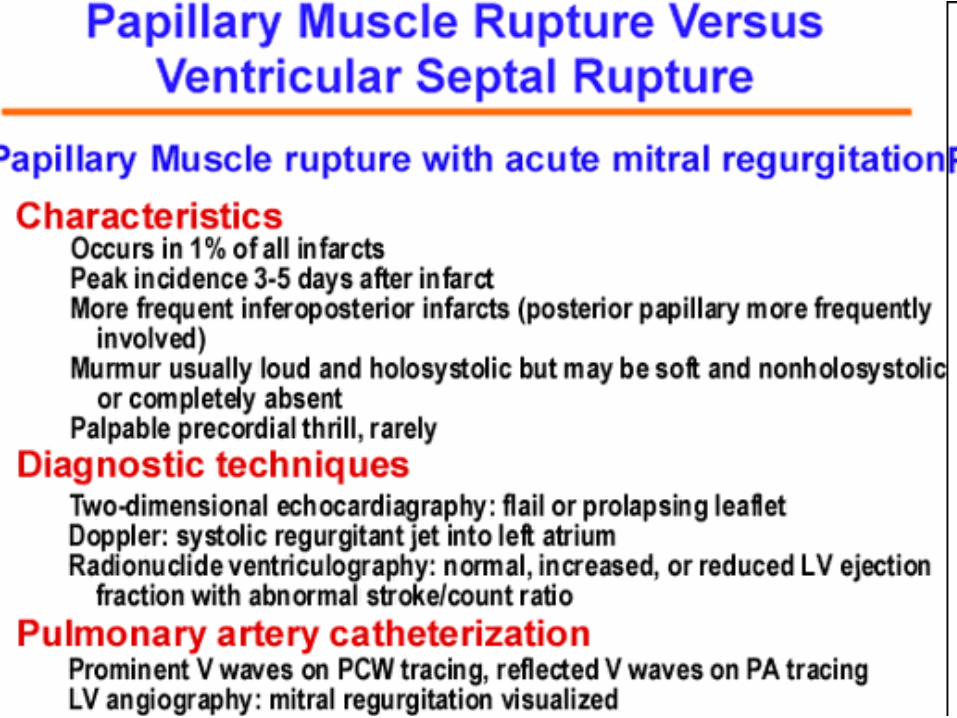
Papillary Muscle Rupture A. Has mortality of 80-90% with
medical therapy B. Prompt surgical therapy
indicated C. Intra-aortic balloon pump prior
to surgery
Ventricular Septal Defect A. Has mortality of 50% with
surgical treatment and at least 90% with medical treatment.
B. Surgical repair and CABG C. Intra-aortic balloon pump prior
to surgery
Rupture of LV free wall A. Occurs 10% of patients who die of an AMI B. Sudden hemodynamic collapse often
accompanied by severe chest pain suggests possibility of rupture of free wall
C. Echocardiogram diagnostic D. Emergency pericardiocentesis and use of
intra aortic balloon pump to stabilize E. Emergency surgery is definitive therapeutic
approach F. Event is almost always fatal even when
emergency surgery attempted
LV Aneurysm and Mural Thrombus A. Occurs 10% of AMI patients B. 80% located in anterior apical
segment and result from occlusion of LAD coronary artery
C. Mural thrombus develops in about 50% of patients with anterior apical Q wave MI usually during the first week after infarction
D. Thrombi are uncommon in inferior wall AMI and rare in non-Q wave infarctions
Cont’d E. Echocardiography useful for identifying
LV aneurysm and mural thrombi F. 4% of AMI patients have embolic events
during the first week after infarction G. There is a 5-fold increase in embolic
events in patients with anterior apical MI’s found to have a mural thrombus by echo
Cont’d Other complications of LV
aneurysms are CHF and ventricular aneurysms
H. Treatment- anticoagulation with Heparin followed by Warfarin for 3-6 months significantly decreases frequency of embolic events
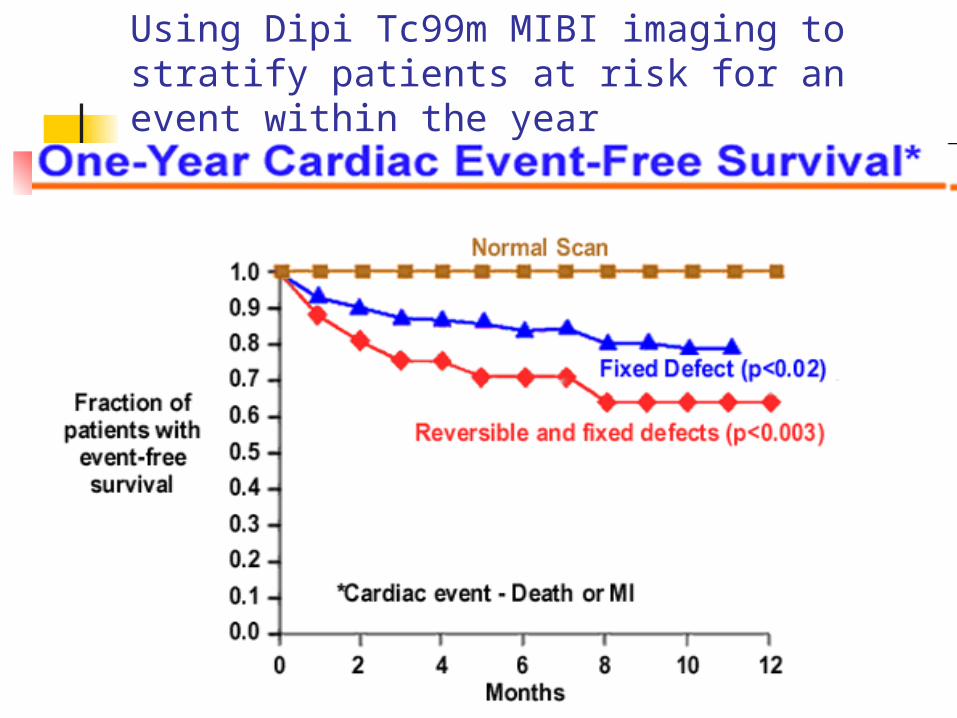
Using Dipi Tc99m MIBI imaging to stratify patients at risk for an event within the year
Assessment of Resting LV function A. Prognosis following AMI is
related to degree of LV disfunction. B. Evaluation is done by
echocardiogram, radionuclide imaging (MUGA study), positron emission tomography.
C. Identify stunned and hybernating myocardium
Non-Invasive Strategies for Identifying Risk of Sudden Death
A. Holter moniter- PVC’s, nonsustained ventricular tachycardia
B. Signal averaged EKG C. Heart rate variability D. Patients at high risk of non-sustained
V-tach, low EF(less than 40%) consider electrophysiologic testing and implantable cardioverter defibrillator (AICD)
Cont’d E. Multi-center automatic
defibrillator implantation trial revealed (MADIT trial) 1. LV dysfunction less than 35% 2. Asymptomatic non-sustained V-tach
(3 beats-30 beats) 3. Inducible, sustained, non-supressible
V-tachPatients with these criteria had improved
survival with AICD.
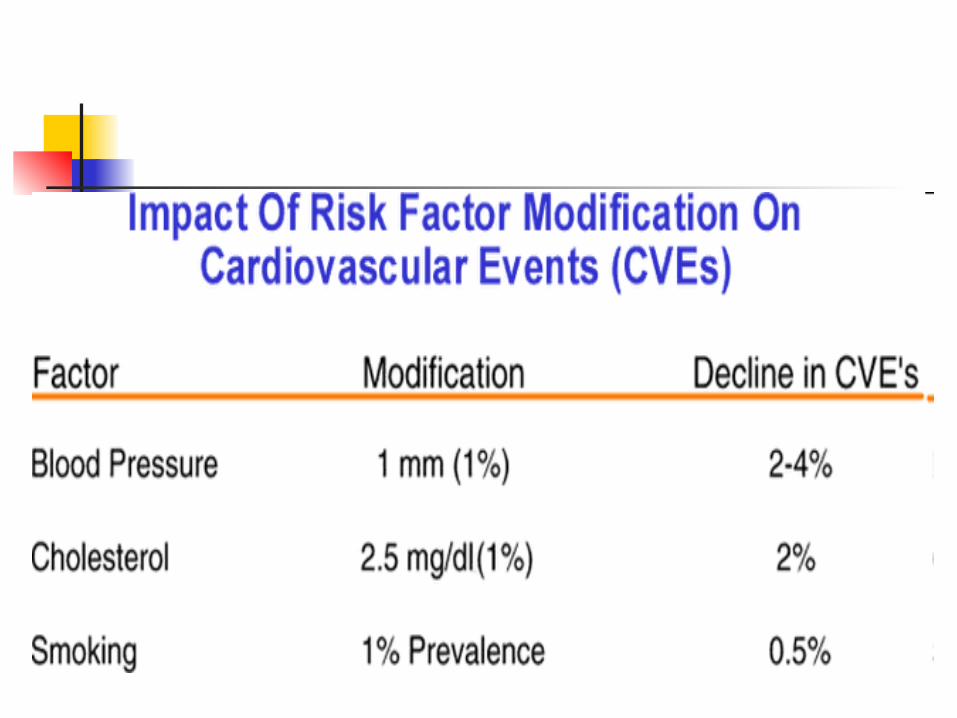
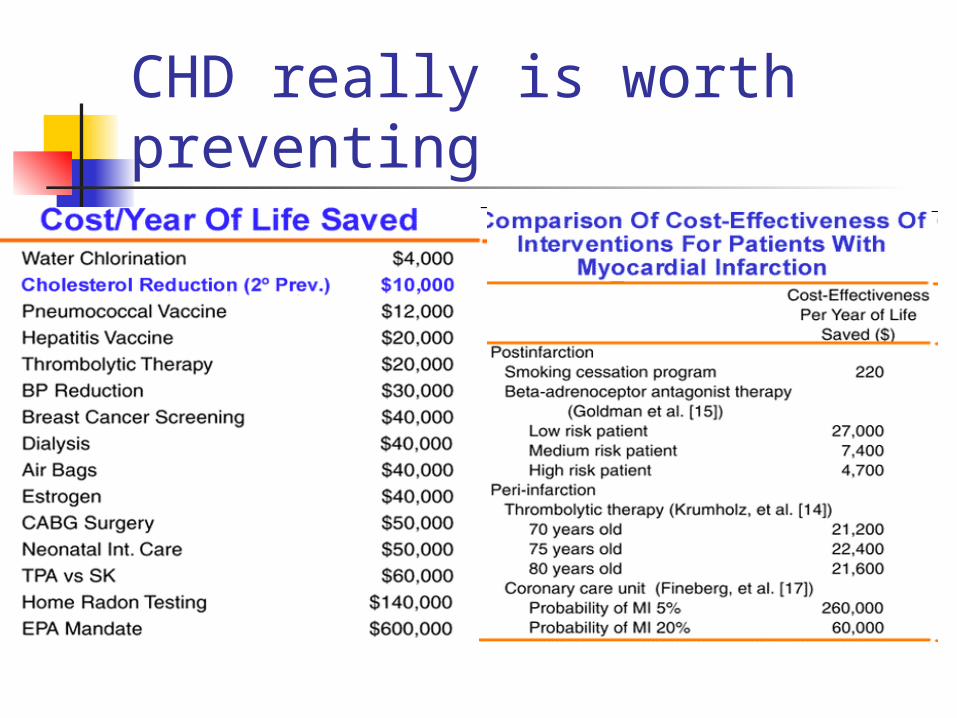
CHD really is worth preventing
At the end….. The acute coronary event (AMI)
can be devastating…as clinicians, let’s do our part to try and prevent these events from occurring.
Remember the old saying… “An once of prevention is worth a pound of cure”


























![Sacher-Masoch [ Deleuze ]](https://img.pdfslide.net/doc/110x75/577ccf461a28ab9e788f56ab/sacher-masoch-deleuze-.jpg)
