Embed Size (px)
Citation preview
Adult Congenital Heart Disease
Howard Sacher, D.O.
Long Island Cardiology and Internal Medicine
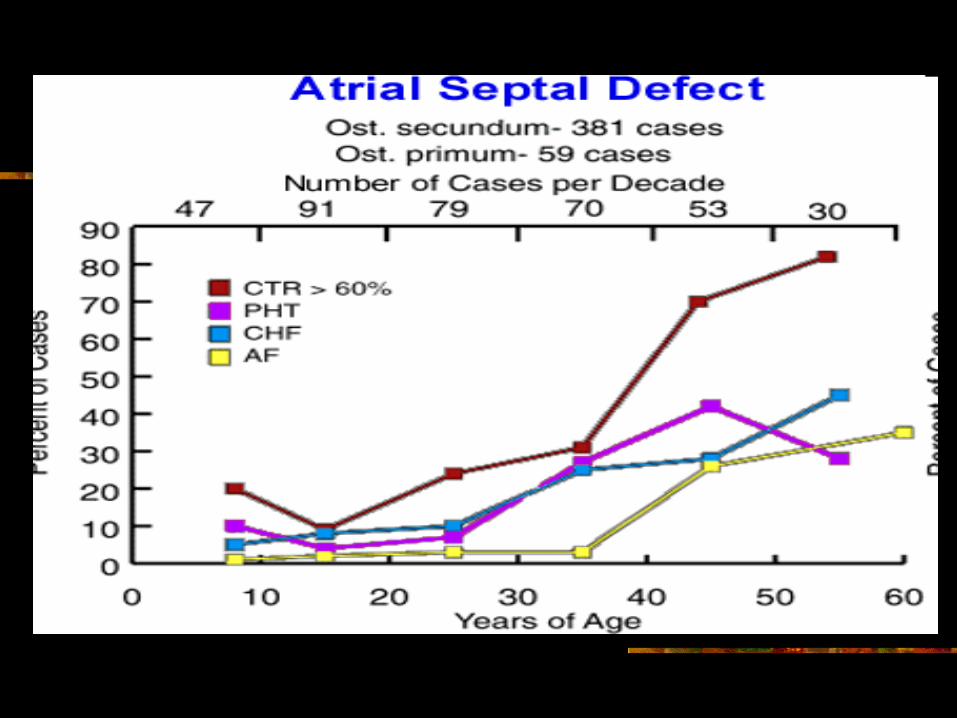
Atrial septal defect (ASD) constitutes 22% to 25% of all adult congenital cases.
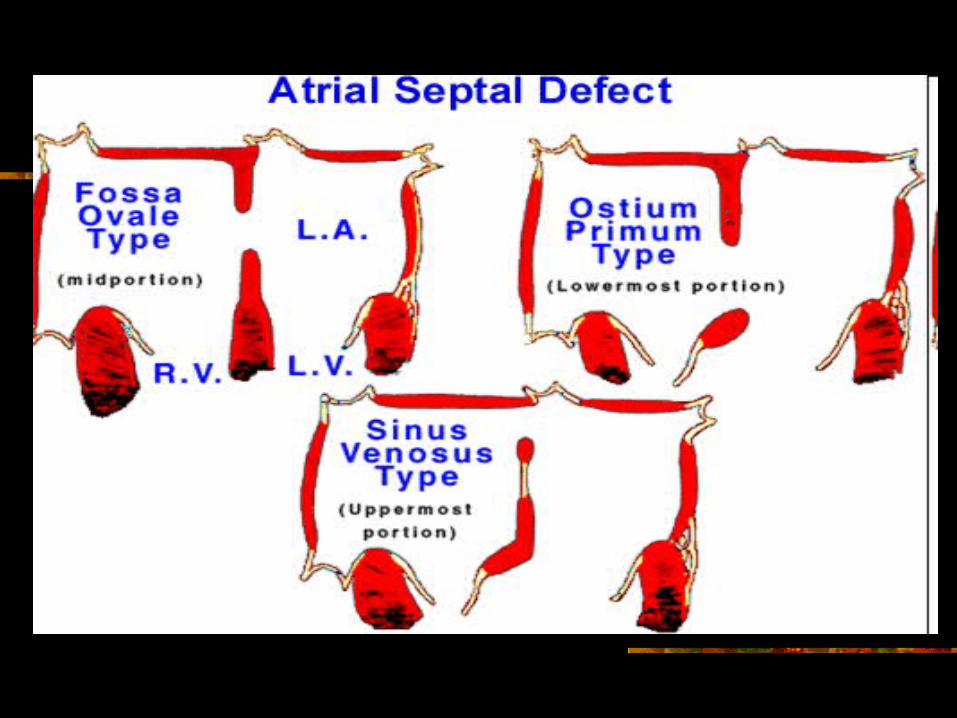
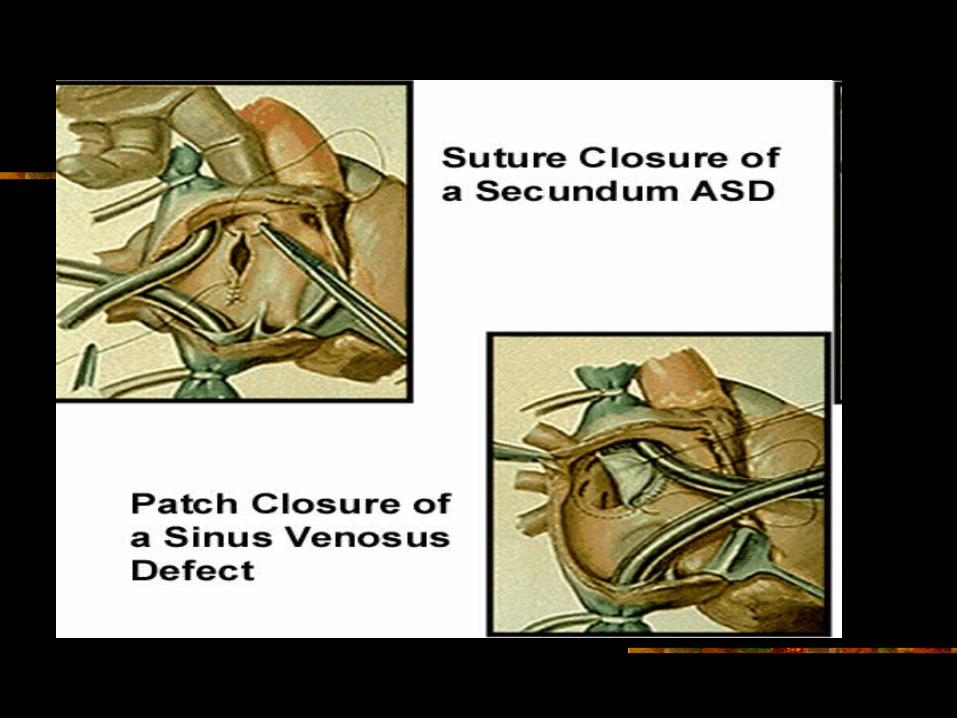
The secundum ASD is a defect of the mid-portion of the atrial septum.
The ostium primum defect is low in the atrial septum, almost always associated with a cleft in the anterior leaflet of the mitral valve
Sinus Venosus Defects Are Often Missed Sinus venosus defects lie high in the atrial septum
and are almost always associated with partial anomalous pulmonary venous return. These defects are commonly missed with transthoracic echocardiography--transesophageal echo is required.
Clinical Features Presenting symptoms include shortness of
breath, easy fatigability, palpitations and preoperative atrial fibrillation.
The hallmark is a Grade II - III/VI systolic murmur localized at the left mid, left upper sternal border radiating to the back.
The approach to ASD is surgical or closure of the defect in the catheterization laboratory. Operative mortality is extremely low
Complicated by cardiac enlargement and atrial fibrillation
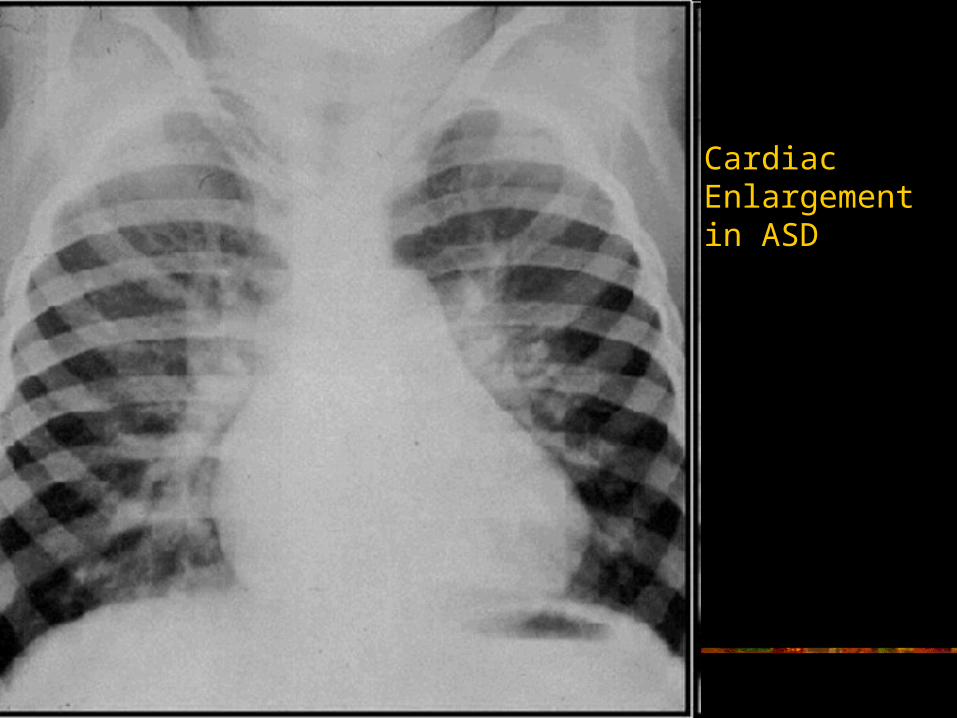
Cardiac Enlargement in ASD
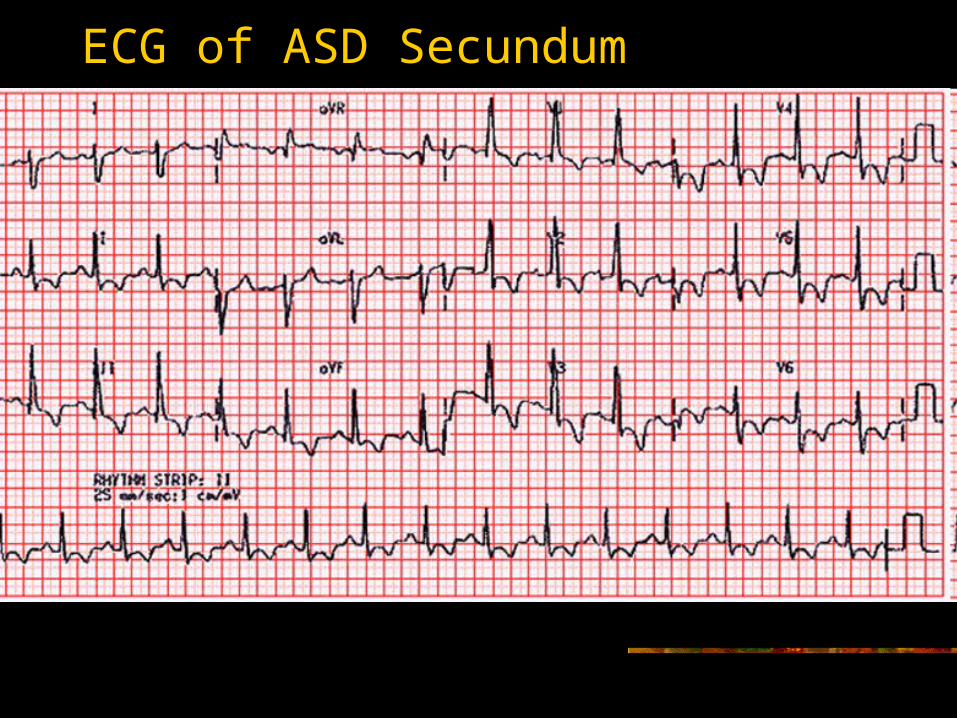
ECG of ASD Secundum
Ventricular Septal Defect
Ventricular septal defect (VSD) is found in approximately 10% of adult patients with congenital heart disease.
Clinical Features
The most common symptoms in adult patients with VSD are dyspnea on exertion, exercise intolerance, and shortness of breath. Findings include holosystolic murmurs and left heart enlargement.
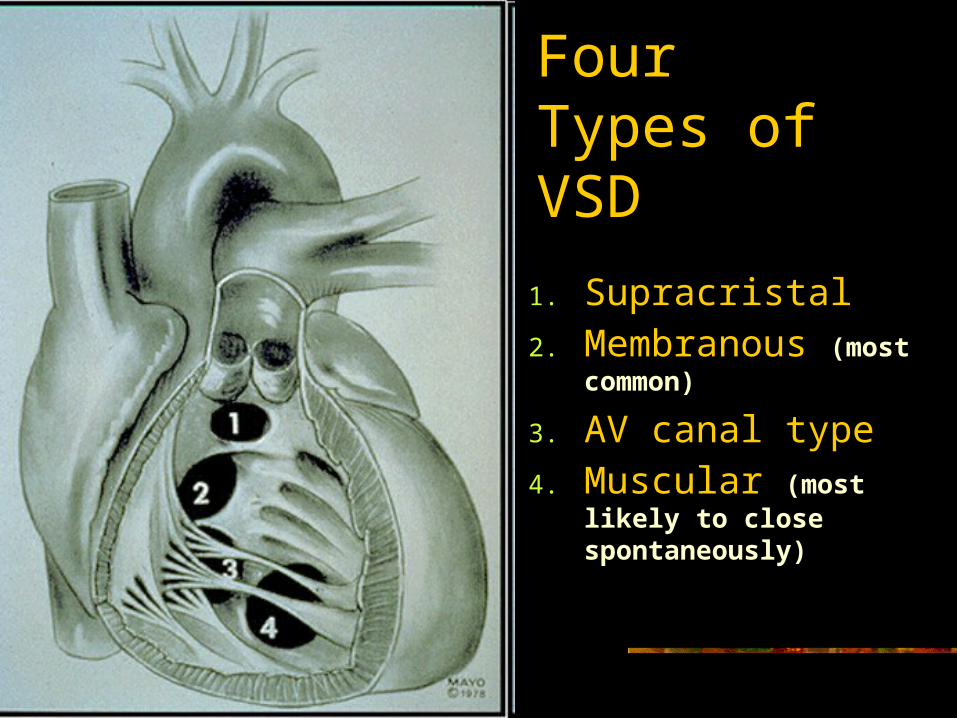
Four Types of VSD
1. Supracristal 2. Membranous (most
common)
3. AV canal type4. Muscular (most likely to
close spontaneously)
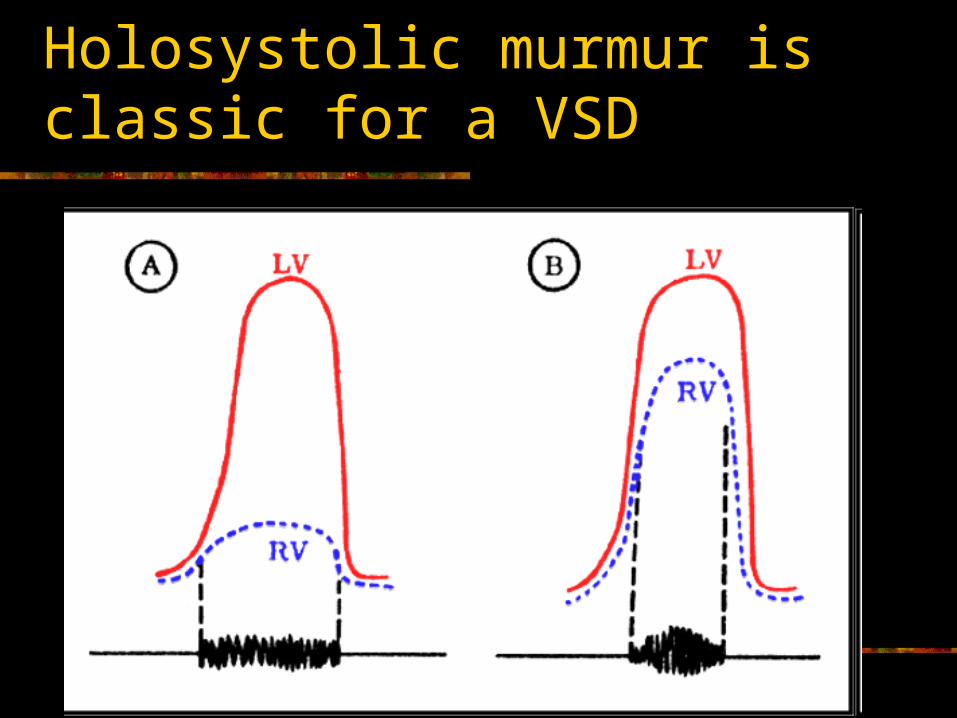
Holosystolic murmur is classic for a VSD
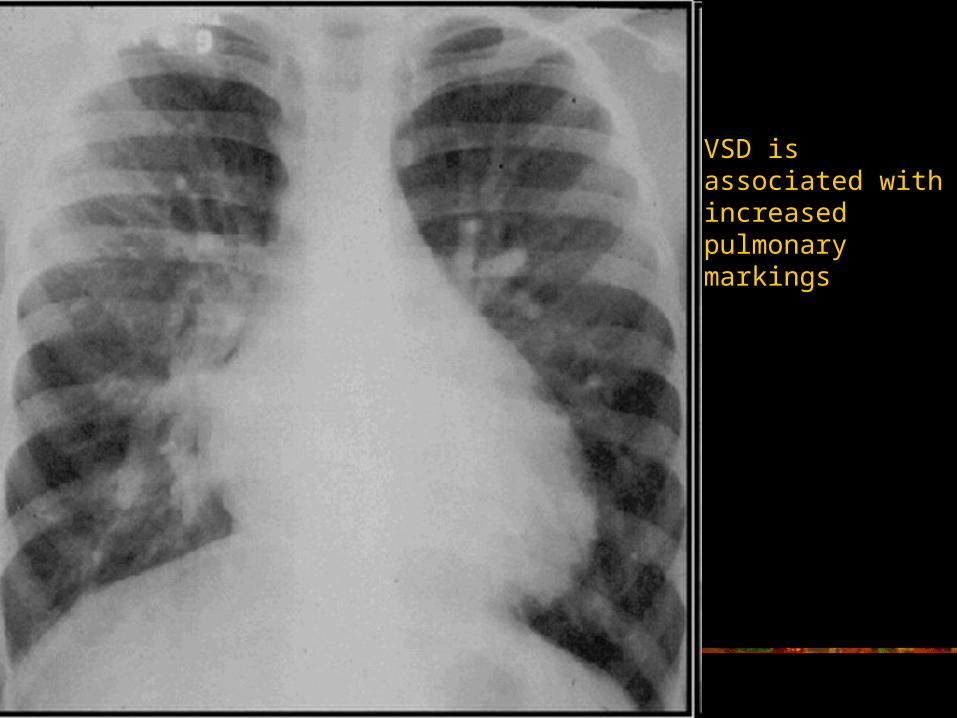
VSD is associated with increased pulmonary markings
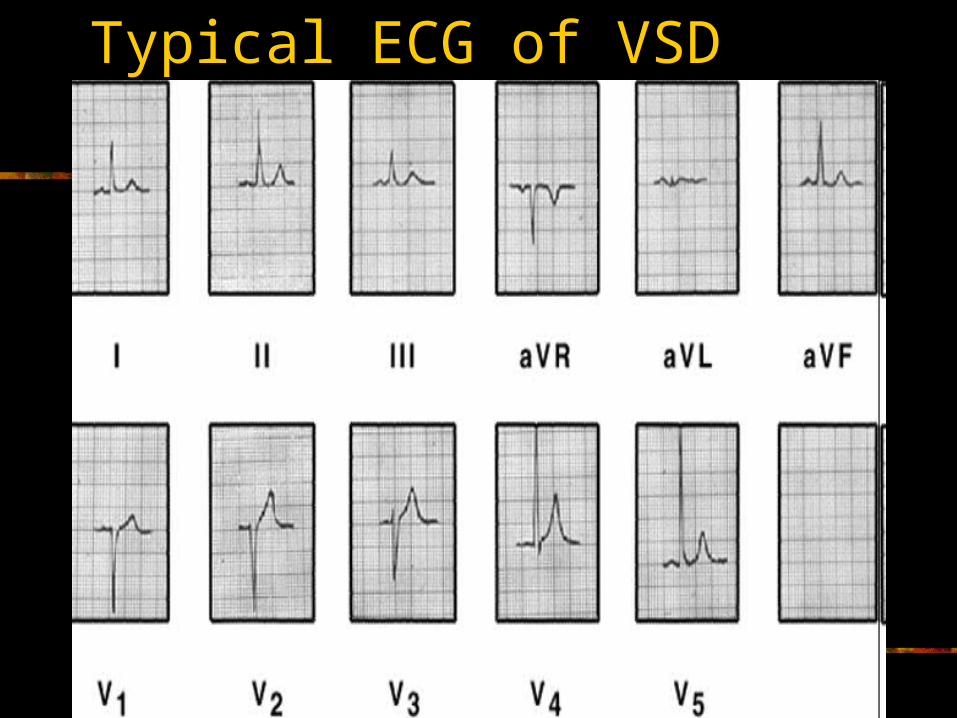
Typical ECG of VSD
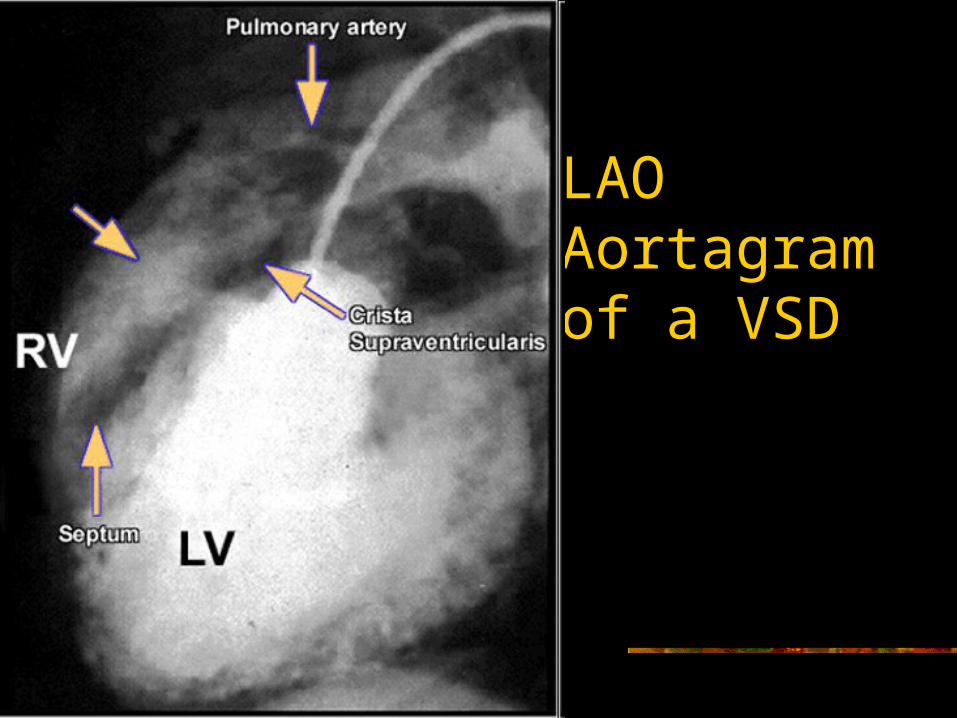
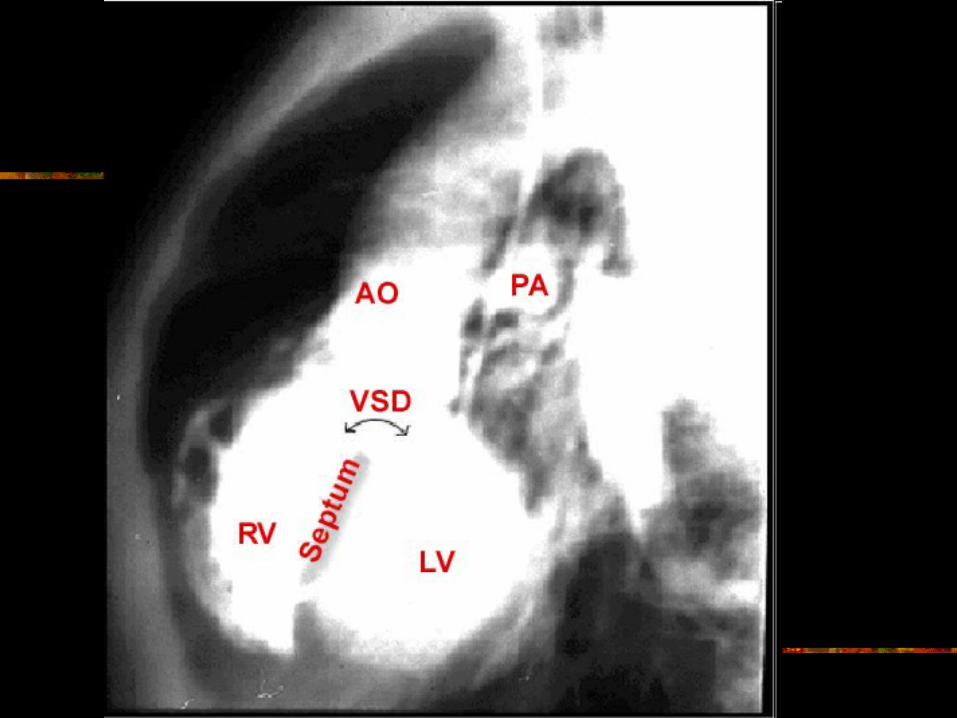
LAO Aortagram of a VSD
Treatment and Follow-up
Treatment of VSD may be surgical, with patch closure, or nonsurgical.
A large VSD in a child may lead to pulmonary vascular disease and eventually an Eisenmenger's physiology complex.
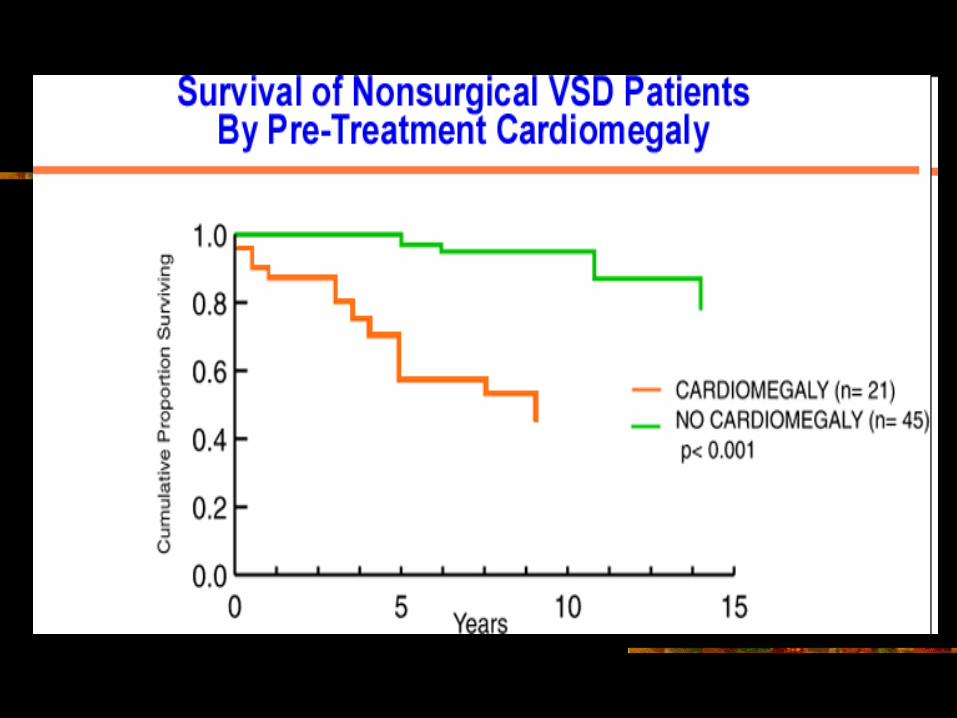
In all the studies done in adult congenital heart patients followed over time, cardiomegaly at the time of diagnosis has been a significant independent risk factor for survival.
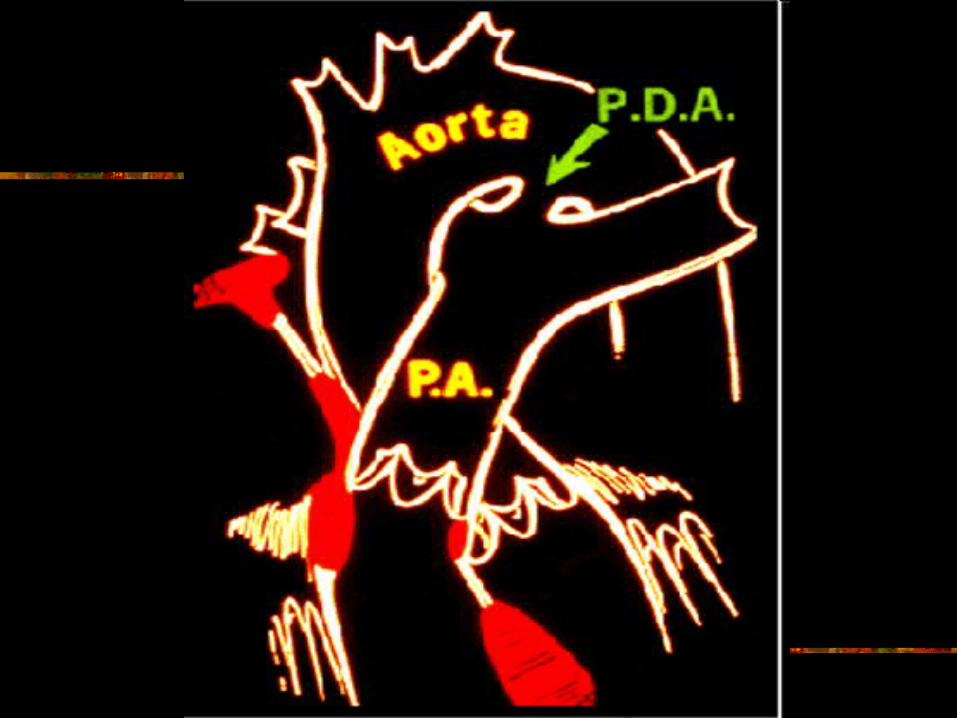
Patent Ductus Arteriosus
Patent ductus arteriosus (PDA) occurs in one case every 2,500 to 5,000 births.
Clinical Features The most common symptoms are exercise
intolerance, dyspnea, and shortness of breath. As the pulmonary artery pressure becomes elevated,
the murmur of the PDA gets shorter and softer. As the patent ductus places a volume load on the left
heart, the chest x-ray may demonstrate left ventricular and left atrial enlargement, with increased pulmonary vascularity.
Treatment
Surgical Closure The surgical approach is ligation and
suture closure of the duct. The calcified ductus needs to be handled carefully, and most of these patients will require cardiopulmonary bypass.
Coarctation of the Aorta
Coarctation of the aorta has been estimated to occur with a frequency of 7.5%.
Life expectancy is severely shortened in coarctation patients who do not undergo operations.
Death is due most commonly to congestive heart failure, aortic rupture, intracranial hemorrhage, or infective endocarditis. System hypertension is the most deleterious component of this anomaly.
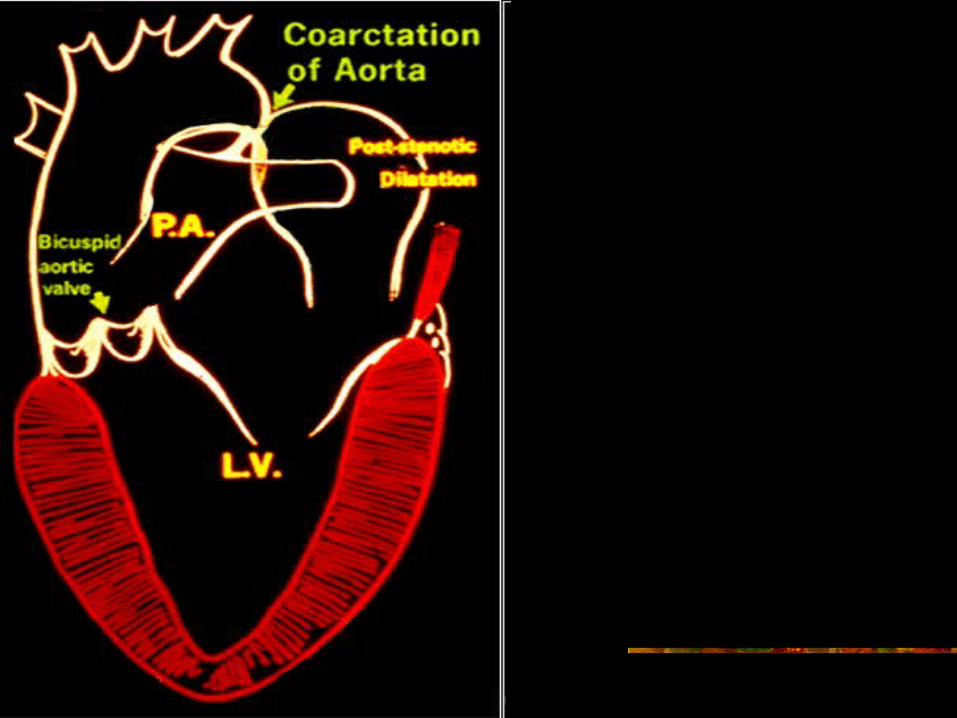
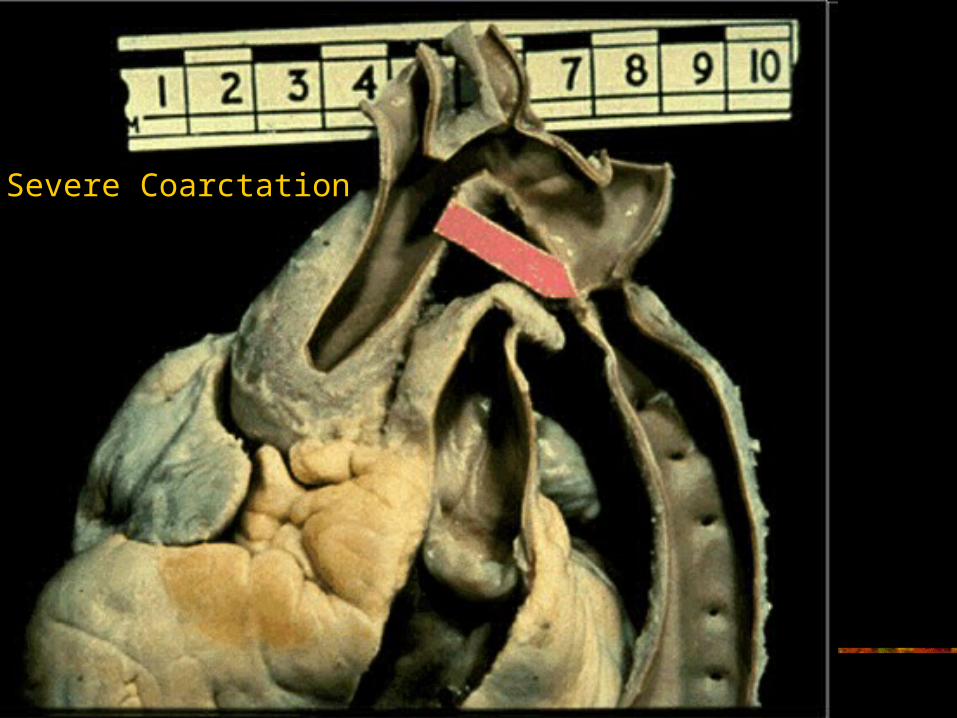
Severe Coarctation
Clinical Features The most common clinical finding is systolic
hypertension. Some patients may have claudication. A systolic murmur may be noted at the site of the
coarctation, or secondary to a bicuspid aortic valve.
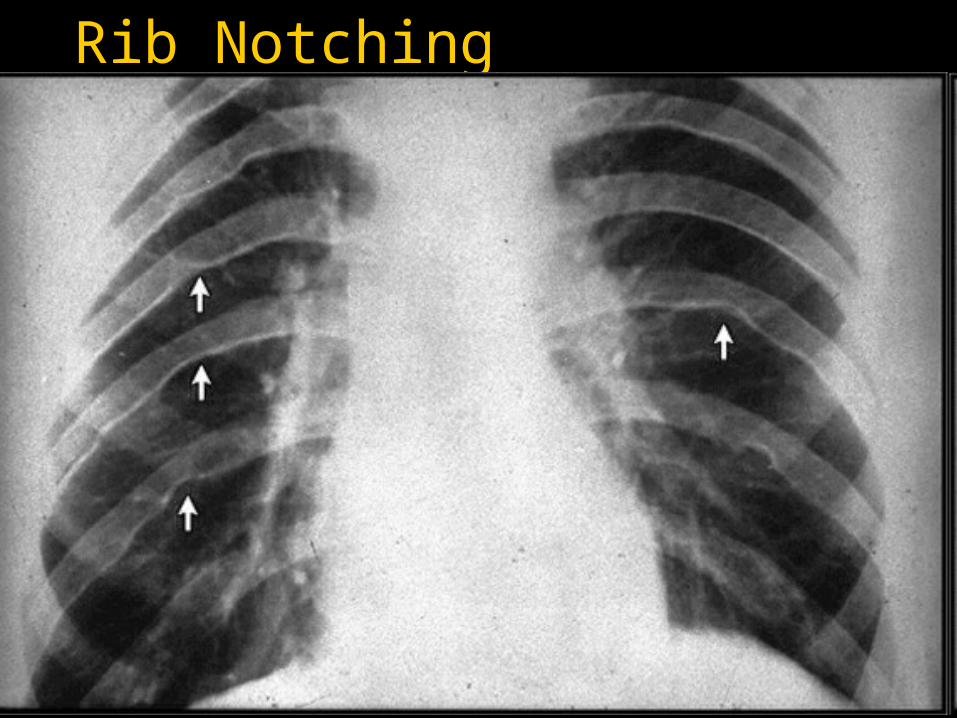
CXR reveals rib notching Stress exercise tests in adults usually
demonstrate marked systolic hypertension. Doppler echocardiographic signals from the aorta
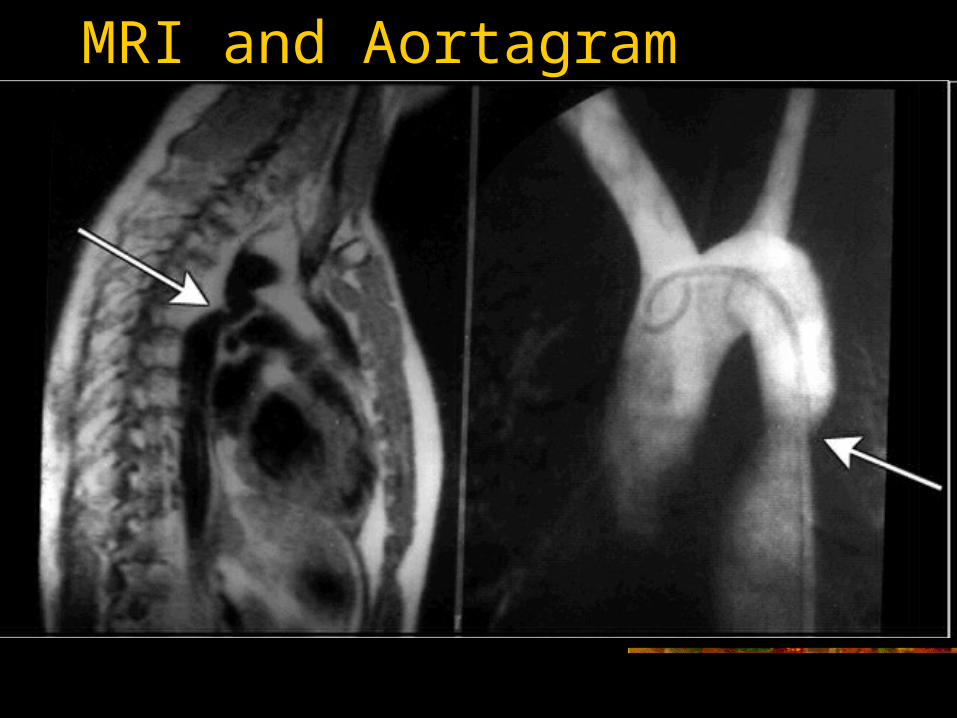
can show a pattern specific to coarctation Magnetic resonance imaging may be required to
find the true anatomy of the coarctation
Rib Notching
MRI and Aortagram
Treatment with Surgery and Postoperative Problems
The surgical approach to this lesion is end-to-end anastomosis, although a patch graft may be necessary in the adult.
Immediately after surgery, most patients will be hypertensive and will require sedation and medication. It is important to monitor blood pressure after coarctation repair in the adult.
Late complications can include aneurysm formation and dissection of the ascending aorta rather than the region of the previous coarctation.
Tetralogy of Fallot (TOF)
Most common form of cyanotic heart disease in adults. It is estimated that without surgical intervention, only about 10%
of patients survive beyond age 21.
Clinical Features Cyanosis and dyspnea on exertion are the most common
symptoms prior to total repair in tetralogy of Fallot. Most presenting adult patients are in functional class III. If echocardiography leaves any question about the anatomy or
the possibility that the patient may have an anomalous coronary artery, and should undergo catheterization
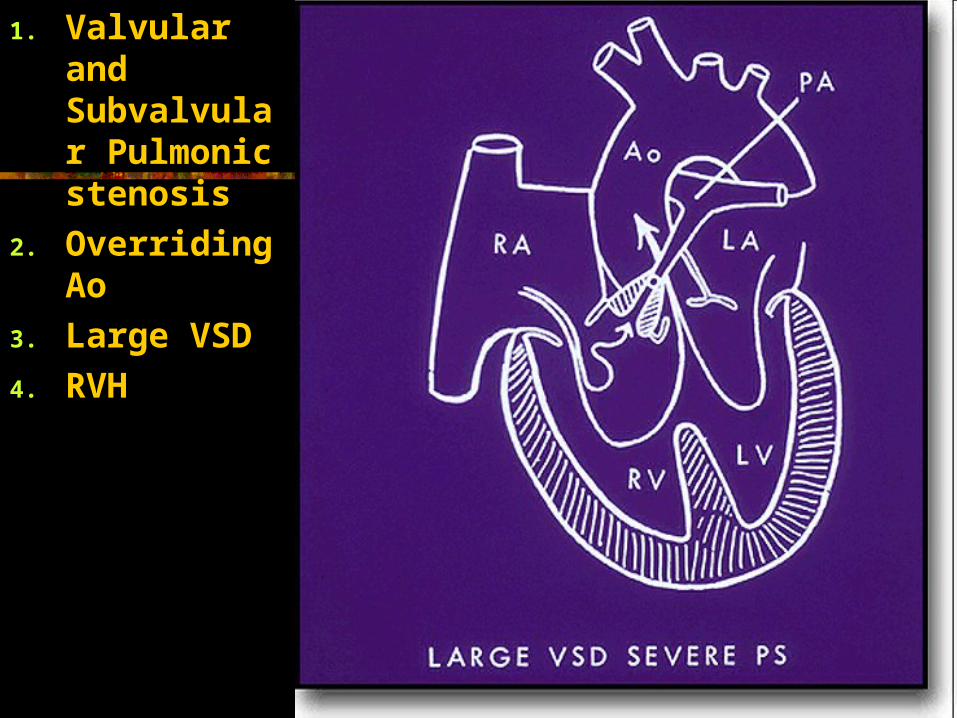
1. Valvular and Subvalvular Pulmonic stenosis
2. Overriding Ao
3. Large VSD
4. RVH
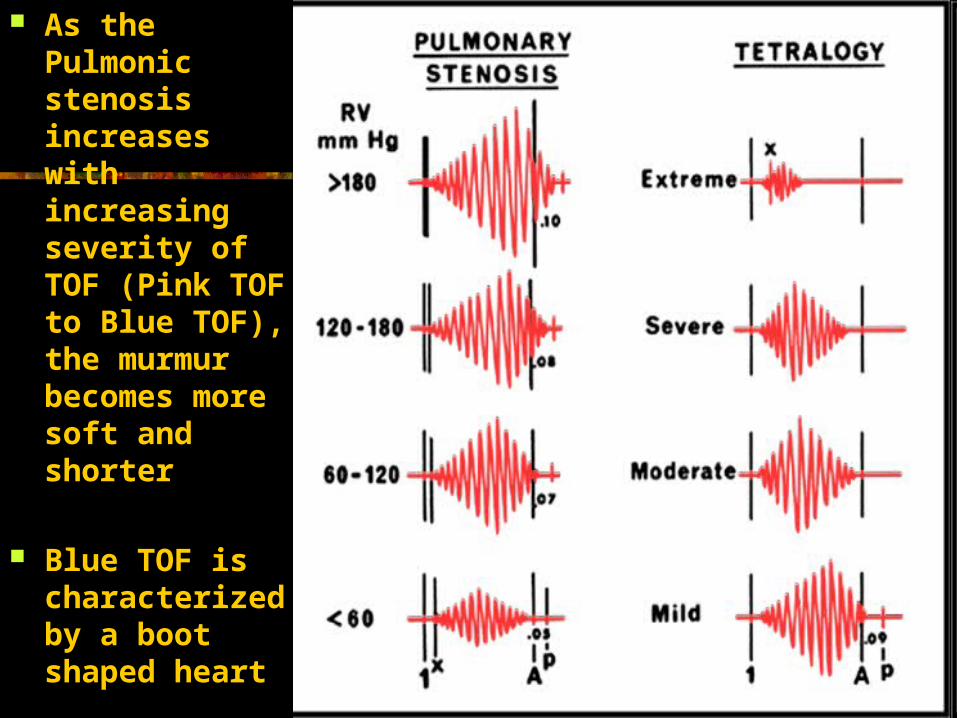
As the Pulmonic stenosis increases with increasing severity of TOF (Pink TOF to Blue TOF), the murmur becomes more soft and shorter
Blue TOF is characterized by a boot shaped heart
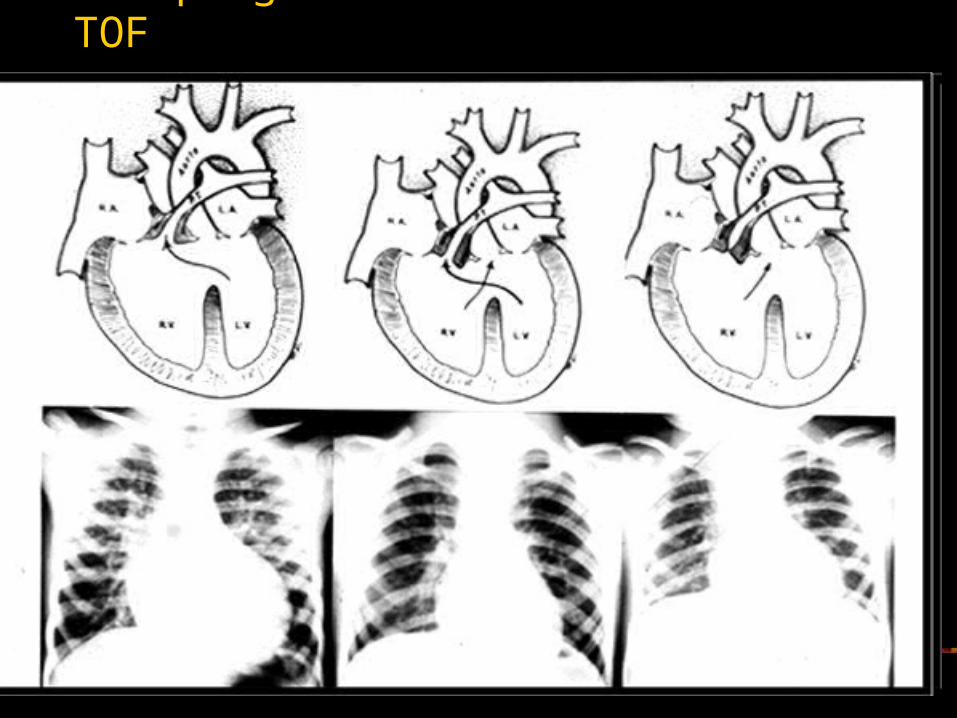
The progression of Pink to Blue TOF
Treatment with Surgery
Surgery involves closure of the VSD with a patch and relief of the right ventricular outflow tract obstruction.
Ebstein's Anomaly
Ebstein's anomaly is the congenital cardiac defect most associated with preexcitation WPW (Wolfe-Parkinson-White syndrome).
Hemodynamic abnormalities often result in: Severe tricuspid regurgitation Right ventricular dysfunction Decreased pulmonary blood flow.
A foramen ovale or ASD is present in approximately 50% of patients
Natural History
Patients with severe tricuspid regurgitation may have significant cyanosis as neonates.
Rapid improvement often occurs, and these patients may be asymptomatic for many years.
Adult patients present most commonly with easy fatigability and dyspnea on exertion—also rhythm disturbances
Clinical Examination
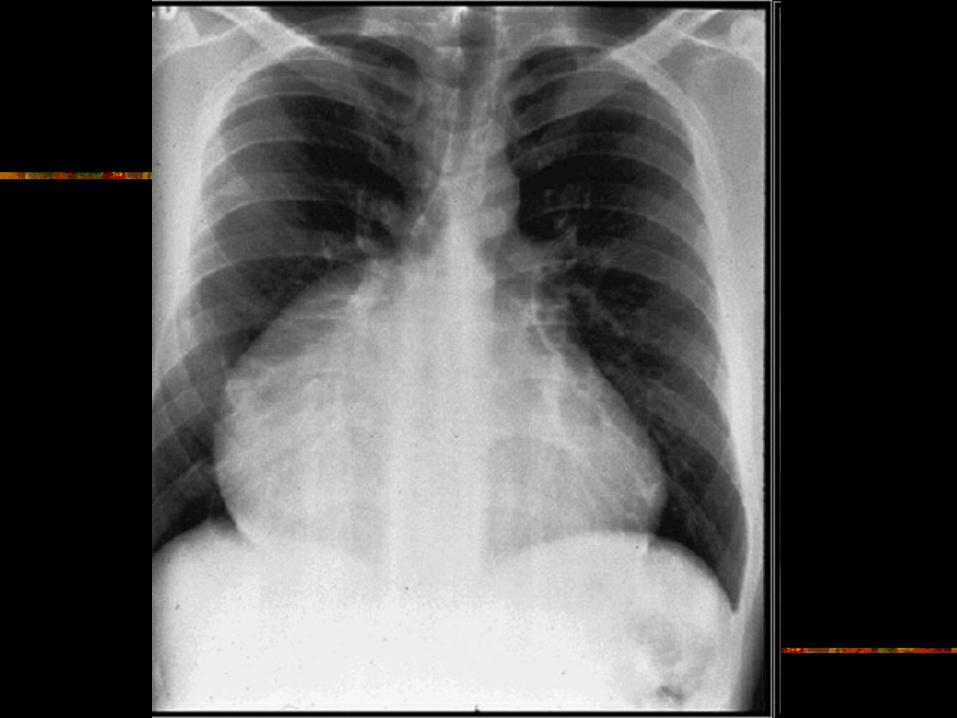
Quadruple cardiac rhythm Moderately severe tricuspid regurgitation Grade II to III/VI systolic murmur along the right mid, right
lower sternal border The ECG often shows first-degree AV block and
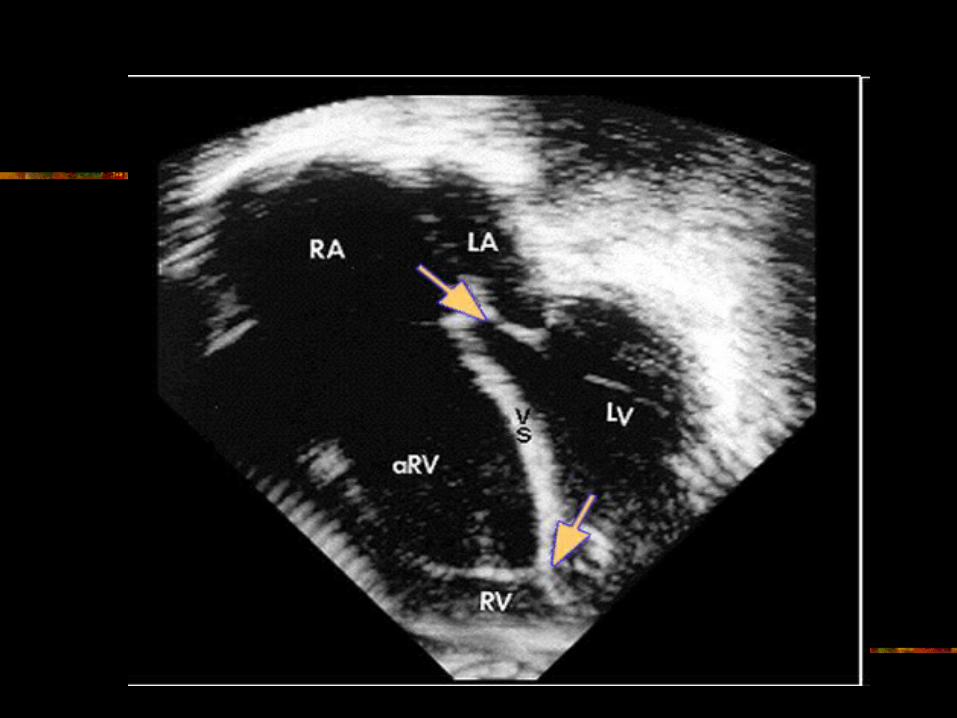
intraventricular conduction delay The chest x-ray shows a markedly enlarged heart The echo demonstrates a markedly enlarged right atrium and
downward displacement of the tricuspid valve (Atrialization of the Tricuspid Valve in the most severe cases)
Treatment
Surgical treatment involves either replacing the tricuspid valve or plastic repair on the atrium, with tricuspid valve repair.
Anticoagulation is mandatory if the tricuspid valve is replaced
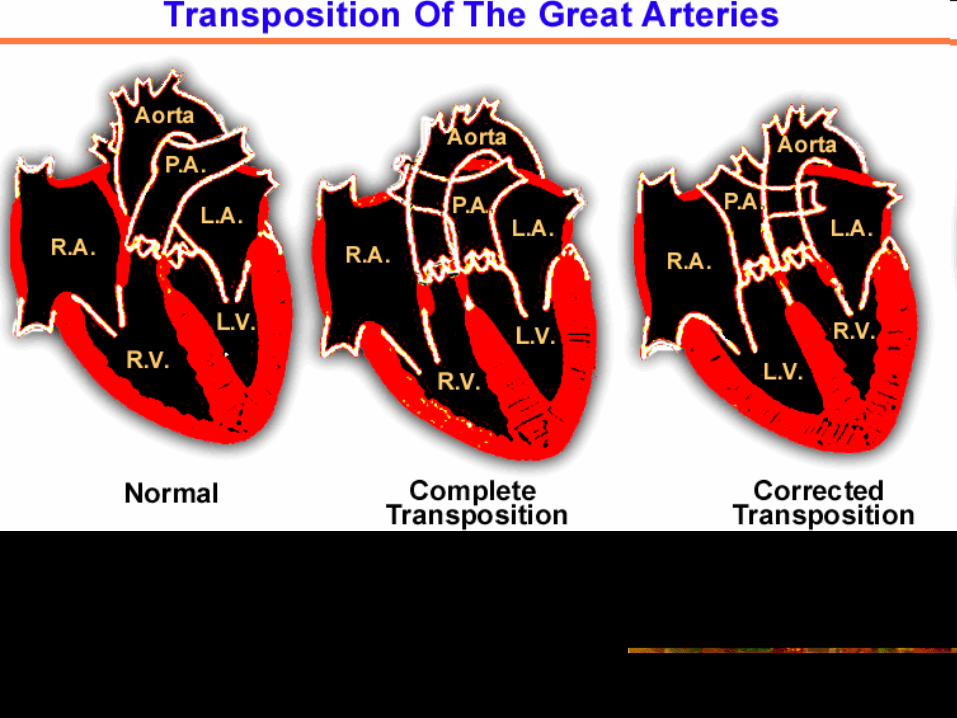
Transposition of the Great Vessels
Complete Transposition The right ventricle is directly connected to the
aorta, and the pulmonary artery is directly connected to the left ventricle, such that blood flow within the heart is in parallel rather than in series.
Patients will die in the early neonatal period unless there is some way to mix the oxygenated with deoxygenated blood.
A redirection procedure used in the late 1960s and early 1970s had low operative mortality, but late complications are common
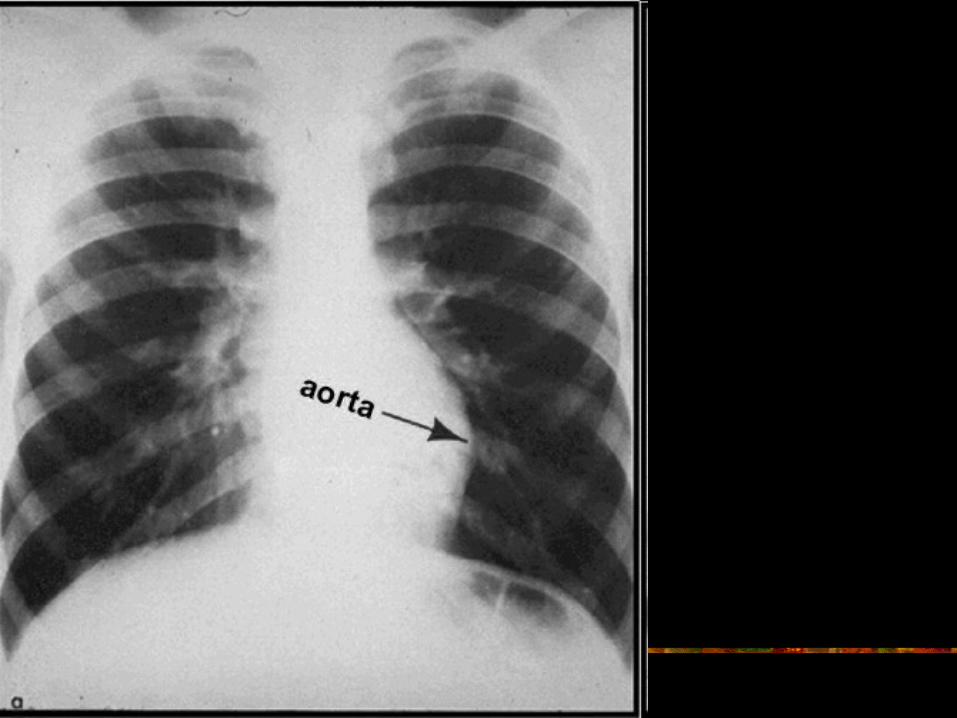
Corrected Transposition of the Great Vessels
The morphologic right atrium delivers blood across the mitral valve into a morphologic left ventricle, which is connected to a more medially placed pulmonary artery.
The pulmonary venous blood comes back into a morphologic left atrium, which empties across a morphologic tricuspid valve into the morphologic right ventricle,
Ventricle ejects blood into an aorta that is anterior and to the left.
Adult patients with corrected transposition commonly have VSDs Pulmonary valve stenosis, Ebstein's malformation of the tricuspid AV
valve, with resultant valve regurgitation. Patients with congenitally corrected
transposition and no other associated cardiac defects can remain free of symptoms until the 6th decade, when symptoms occur in more than 50% of patients.
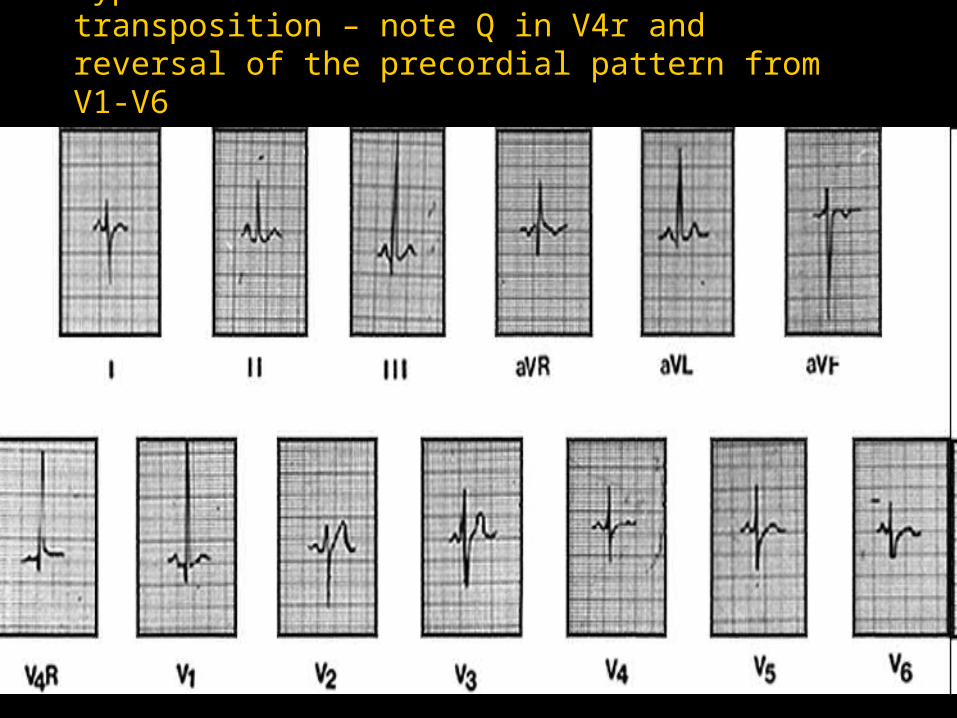
Typical ECG of an adult with transposition – note Q in V4r and reversal of the precordial pattern from V1-V6
Tricuspid Atresia and Double-Inlet Left
Ventricle
Patients with tricuspid atresia are generally cyanotic unless they have undergone systemic pulmonary artery shunts.
They tend to have normal or small heart size, with significantly decreased pulmonary vascularity.
Their ECGs demonstrate lack of right ventricular voltages, with left ventricular hypertrophy, right atrial enlargement, and occasionally first-degree AV block
Patients with double-inlet left ventricle tend to have cardiomegaly on x-ray, with increased vascularity if there is no outflow tract obstruction.
They often have AV valve regurgitation. The ECGs tend to demonstrate first-degree AV block, intraventricular conduction delay, lack of septal Q waves, and frequently, biventricular hypertrophy
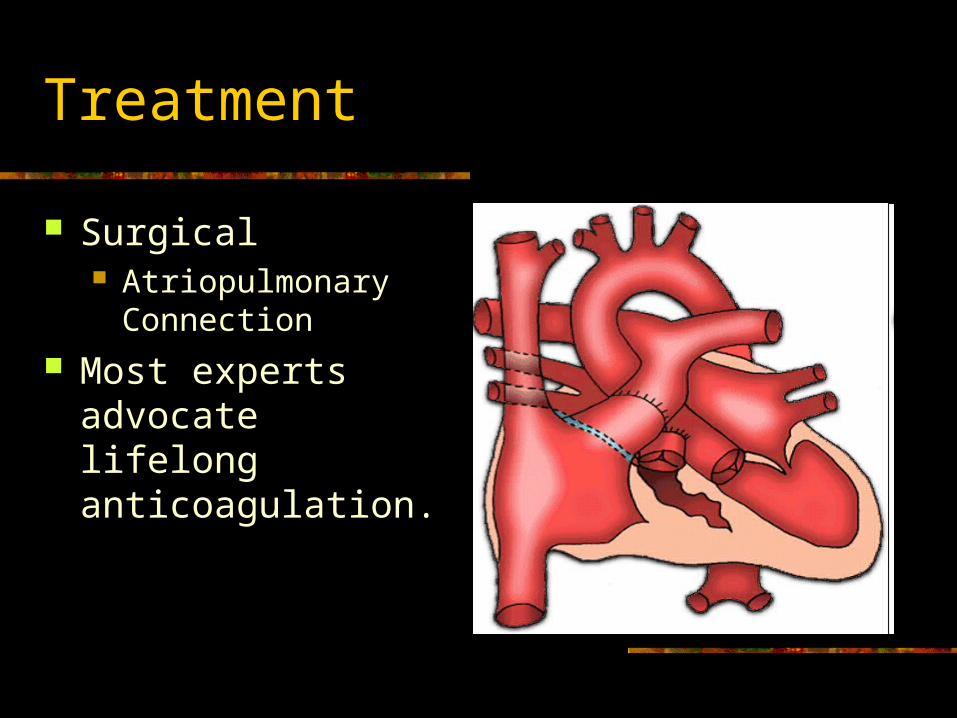
Treatment
Surgical Atriopulmonary
Connection Most experts
advocate lifelong anticoagulation.
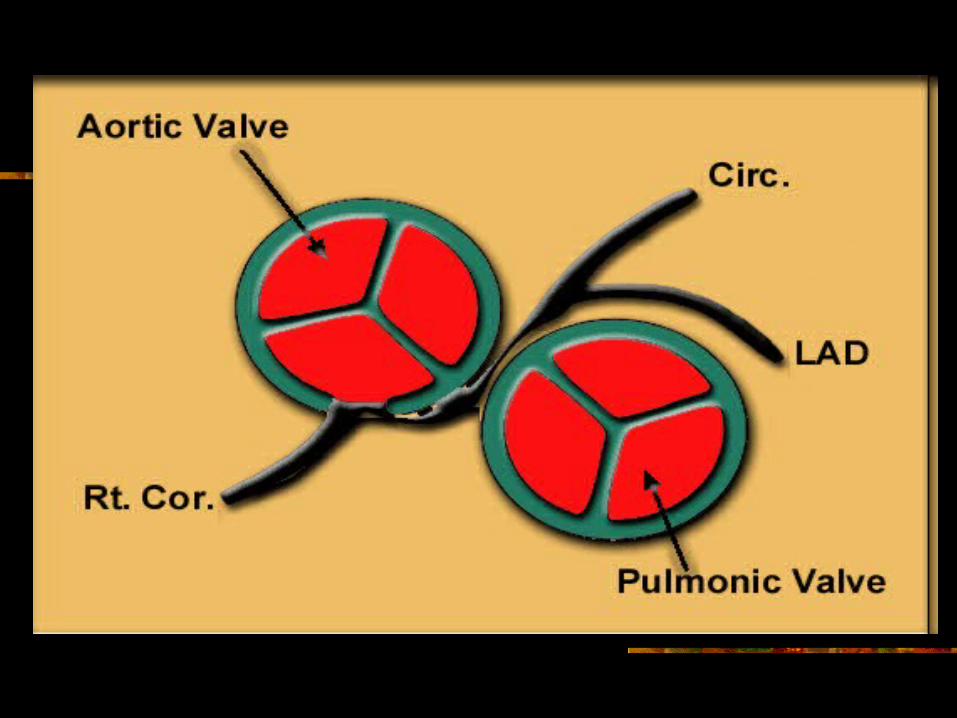
Congenital Coronary Anomalies
The right coronary artery may originate from the left sinus of Valsalva, both running in between the aorta and the pulmonary artery.
The left coronary artery may originate from the right sinus of Valsalva.
These 2 anomalies may be especially lethal in young males during exercise.
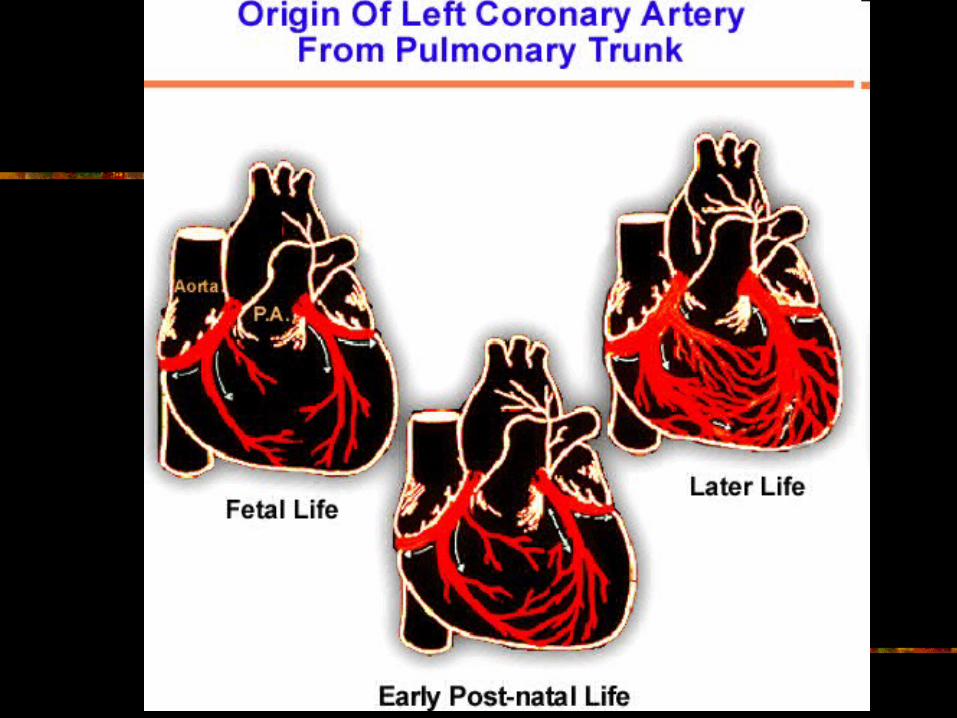
The left coronary artery may originate from the pulmonary artery, a rare condition known as Bland-White-Garland syndrome.
Bland-White-Garland Syndrome
Approximately 10% of patients with Bland-White-Garland syndrome present as adults.
Adult patients with this condition demonstrate large collaterals from the right coronary artery to the pulmonary artery.
Patients are managed surgically, generally with good results.