Embed Size (px)
Citation preview
Rev. 01/05/2017
02663
Adair County SB40 Temporary Residential Support Self-Directed Option
INDIVIDUAL DATA FORM
Individual Receiving Services (Minor Child)
Name in Payer Program First Middle Last
Street Address (Physical address where services will be provided, No PO Box)
City State Zip County
Gender Male Female Date of Birth ____/____/_______ Social Security # _____ -___-______
Parent/Guardian Information (FEIN Holder)
Name on Social Security Card First Middle Last
Street Address
City State Zip County
Phone ( ) ( ) ( ) Email Home Cell Fax
Date of Birth ____/____/_______ Social Security # _____-___-______
Support Coordinator Contact Information
Name Agency
Phone Email
Prior Relationships/Business Accounts
1. Yes No – Has the Individual ever received services through another Fiscal Provider? If yes, Provider name:
2. Yes No – Is the Individual switching FEIN holders? If yes, previous FEIN holder name:
3. Yes No - Are Prior Business Accounts established? If yes, enter account information below:
____-______________ FEIN State Unemployment Tax Account # SUTA Rate Business Tax Withholding Account #
Yes No - If previous FEIN, does FEIN holder have employees other than caregivers?
4. Budget/Auth Start Date _________________
Rev. 01/05/2017
05088
Adair County SB40 Temporary Residential Support Self-Directed Option
INDIVIDUAL DATA FORM
Enrollment Questions The Consumer Direct representative responsible for assisting the Individual with enrollment must complete the questions below by interviewing the Individual and/or FEIN holder. If Individual Receiving Service/FEIN holder does not know the answer to a question, please write “Individual doesn’t know” on the line next to the question. Questions for the FEIN holder named on page 1 of this form.
1. What name is shown on your most recently received Social Security Card?
2. What number is shown on your most recently received Social Security Card?
3. Have you gone by any other name(s) in the past which aren’t shown on your most recently received Social Security Card?
Yes No
a. If yes, please list your other name(s):
b. Please list when your other name(s) were used:
4. Were you ever previously assigned an FEIN by the IRS for any business previously operated/owned?
Yes No
a. If yes and known:
i. Please list the previously assigned FEIN:
ii. What was the business for?
iii. Is the business still active? Yes No
Question for the Individual Receiving Service named on page 1 of this form.
1. Were you ever previously enrolled with another Fiscal Agent/Provider?
Yes No
a. If yes and known:
i. Please list the name of the Fiscal Agent/Provider:
ii. Please list when you were with the Fiscal Agent/Provider:
Consumer Direct Representative Name:
Consumer Direct Representative Signature: Date:
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 1 of 8
02776
This Fiscal Employer Agent Services Agreement (Agreement) is made and entered into as of
(Start Date) between Missouri Consumer Direct, LLC doing business as Consumer Direct
Care Network Missouri (Consumer Direct) and ___________________________ Individual, and/or
___________________________________________________ their Guardian and/or ___________________________ Designated
Representative, if appointed by the Individual or Guardian.
DEFINITIONS 1. The “Employer” is the Individual who has a disability and who receives services through the Adair
County SB40 Developmental Disability Board, herein referred to as Adair Co SB40. A Designated Representative (DR) may be authorized by the Individual/Guardian to manage day-to-day employee activities on the Individual’s behalf. In the case of a minor child the “Employer” is the parent/guardian of the Individual receiving services. The Federal Employer Identification Number (FEIN) Holder will be the Employer (of Record and of Fact) and can employ persons to provide services to the Individual.
2. Missouri Consumer Direct, LLC is the “Fiscal Employer Agent” (F/EA). As authorized under IRS Revenue Procedure 70-6 for the purpose of payroll and payroll reporting services, the F/EA will file on behalf of the Employer/FEIN Holder.
3. Adair Co SB40 and its agents associated with the Temporary Residential Support Self-Directed Option is the entity that governs services and authorizes the Individual Service Plan (ISP) and budget. Adair Co SB40 recognizes that Consumer Direct, acting as the F/EA, will provide Fiscal Management Service (FMS) to the Employer/DR.
SERVICE TO BE PROVIDED The Employer/DR agrees to hire employee(s) to provide services as described in the ISP and consistent with Adair Co SB40’s policies and procedures. The hourly wage will be set as indicated in the Budget Authorization and approved by Adair Co SB40. Self-Directed Services include: Procedure Code Temporary Residential Support TRS - SD As defined in the Individual’s ISP PAYMENT FOR SERVICES
The Employer/DR acknowledges that Adair Co SB40 has contracted with an F/EA and that entity is responsible for: (a) providing employee(s) with a time sheet to be completed each pay period; (b) calculating, withholding, filing and paying all applicable Federal, State and local withholding and payroll taxes and other deductions, if any; (c) paying the balance to the Employee(s) by direct deposit or paycard; and (d) preparing standard payroll reports including monthly reports of balances.
The Employer/DR shall be responsible for ensuring employees accurately record the hours worked and services performed on the approved time sheet. This time sheet, once approved by the Employer/DR, becomes the basis for payment to the Employee. Any falsification or other misrepresentation of the information on this record will constitute fraud. All payments made as a result of inaccurate time sheet
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 2 of 8
02777
information will be recouped from the Employer/DR and/or Employee. Any evidence of fraud may be referred to law enforcement agencies. Payment will be made only for services described and authorized in an Individual Service Plan agreed to by the Employer/DR and Adair Co SB40. The Employer/DR will be given a budget summary as part of the Individual’s service plan, authorizing payment of the services. These documents will specify the maximum authorization and rates for payment and the time frames to which these maximums apply. Any services provided beyond the authorization will not be payable under this Agreement and shall be the responsibility of the Employer/DR. CONDITIONS
The quality, appropriateness and timeliness of services reimbursed through this Agreement shall be subject to evaluation and thorough inspection by Adair Co SB40. Services paid to the Employee and approved by the Employer/DR shall be submitted to the Adair Co SB40 for reimbursement when the services are authorized. The Support Coordinator shall monitor all services on at least a quarterly basis. The Employer/DR is responsible for ensuring that documentation of delivered services is maintained for a period of no less than six years from the date of service. These records will be made available to the Support Coordinator for monitoring. Additionally, these records must be produced for auditing purposes through Adair Co SB40. Any discrepancies in records and claims for reimbursement from Adair Co SB40 are subject to recoupment from the Employer/DR. Documentation requirements are:
Attendance or census records (time sheets, etc) documenting days of service signed by the Employee. Employee time sheets to be reviewed, signed and submitted to the F/EA by the Individual/DR. Time sheet information should include the dates and times of services (clock time and hours worked), records of which Employee provided each unit of service, signature of Employee who provided the services, and Employer/DR signature;
Daily activity records that describe various covered activities (services) in which the Individual receiving services participated.
The Employer/DR understands and agrees that they are the Employer and that the Employee is not, under any circumstances, an employee of MO Consumer Direct or Adair Co SB40. An Employee may work for more than one Individual receiving services. Information shared with the Employee by the Employer/DR or Adair Co SB40 and affiliated agencies regarding the Individual receiving services shall be confidential, as specified in HIPAA. The Employer/DR shall ensure the Employee meets the qualifications as specified in this agreement and trainings specified in the Individual’s ISP and training checklist.
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 3 of 8
02778
The Employer/DR shall ensure that the Employee has a successful background screening prior to the Employee working with the Individual receiving services. This Agreement does not allow for payment of non-qualified employees. If an Employee is deemed to be non-qualified, payment for services rendered will be the responsibility of the Employer/DR. The Employer/DR shall set the conditions of employment. Termination of employment shall be the prerogative of the Employer. All employee hiring and firing practices exercised by the Employer/DR must be in accordance with the Missouri Department of Labor and Industrial Relations fair hiring and firing practices. Repeated terminations by the Employer/DR, however, if done without cause, may make replacing staff more difficult and result in increased state unemployment tax rates (SUTA) that must be paid. Finding replacement staff in this situation shall not be the responsibility of Adair Co SB40. The Employer/DR must inform the F/EA when an Employee has been terminated and the reason for termination in order for the F/EA to submit the required notice separation, if received from the Division of Employment Security. This information will be documented in the F/EA Employee’s file. RESPONSIBILITIES OF THE EMPLOYER/DESIGNATED REPRESENTATIVE
1. Complete all of the forms required by Consumer Direct for its F/EA FMS services. This includes accurately filling out required IRS and Missouri State tax forms (e.g. exempt status, Unemployment, etc.).
2. Obtain a Federal Employer Identification Number in the name of the Individual, with the assistance of Consumer Direct.
3. Follow all Federal and State employment laws, regulations, and rules; including:
a. Recruiting, interviewing, checking references, hiring, training, scheduling, managing, and terminating their Employee(s). This includes directing the day-to-day care of the Individual and addressing conflicts between Employees.
b. Employee must be at least 17 years old and cannot be the Individual's parent, step parent, guardian, spouse or any other family member or person who resides in the home with the Individual. In addition, the Designated Representative may not be an employee.
c. Submit all new Employee paperwork to Consumer Direct prior to the initiation of service. All required documents must be completed, submitted and approved as a complete packet in order for them to be processed timely. Incomplete documents may delay an Employee’s start date.
d. Provide equal employment opportunities to all Employees and interested Employees without discrimination as to race, creed, color, national origin, gender, age, disability, marital status, sexual orientation, or any other legally protected status in all employment decisions, including recruitment, hiring, changing schedules and number of hours worked, layoffs, and termina-tions, and all other terms and conditions of employment. The Employer/DR accepts full and specific responsibility for following Equal Opportunity laws and requirements regarding Employees. Each Employee is to be treated fairly and consistently, e.g., if the Employer/DR decides to check references on one Employee, it must be done for all Employees.
e. Review and approve time worked, which authorizes Adair Co SB40 to be billed. Submit time worked in a timely manner in accordance with the Consumer Direct payroll schedule. The
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 4 of 8
02779
Employer/DR and Employee signatures/approval, on the time sheet (or Web Portal), mean that the information submitted is accurate and true. If the Employer/DR signs/approves and the hours have not been worked, it is considered fraud. The Employer/DR can be held accountable for approving time entered that contains fraudulent information that results in over-billing Adair Co SB40.
f. The Employer/DR is responsible for monitoring the monthly Spending Summary Report provided by Consumer Direct and for keeping all expenditures within the Individual's Service Plan budget amount. The Employer/DR agrees to monitor their monthly service usage in order to stay within the annual authorization as specified in this agreement. The Employer/DR agrees to reimburse Consumer Direct for any payment of wages and expenses that exceed the amount in the Individual’s Service Plan budget. Payment to the Employee will be made only for services actually delivered by the Employee.
g. If the Employer authorizes use of all funds/hours before the end of the period, the Employer/DR will need to make other service arrangements, e.g. use non-paid support staff, etc. The Employer is responsible for the payment of any wages and expenses that exceed the amount in the Individual's Service Plan budget. If an employee works, they must be paid.
h. Inform Consumer Direct, within one working day, of any changes in the Individuals’ status, e.g., name, address, telephone number, hospitalization, terminations, etc.
i. Inform Consumer Direct of the standard rate of pay for the Employee, including timely notification of any changes in the rate. Change in pay rates must occur at the beginning of a pay period.
j. Maintain compliance with Adair Co SB40’s approved utilization amounts for the Individual's Service Plan budget.
4. The employer/DR will set the rate of pay for employees. It must be reasonably justified by the care needs of the individual, as established in their ISP, but it must be at least minimum wage and is capped at $10.00/hour.
5. Immediately Report:
a. Any possible fraud to Consumer Direct.
b. Abuse, neglect, misuse of property or funds, health risk or other reportable event to the appropriate authorities, i.e., Dept. of Health and Senior Services, DMH-DD, Support Coordinator or Adair Co SB40.
c. Employee changes, including name, address, contact number, and/or employment status to Consumer Direct.
6. Appoint a temporary representative if the Employer/Designated Representative is not capable or available to manage Employees and contact Support Coordinator to evaluate if a new representative must be appointed.
7. The Individual and/or Employer/DR agree to accept and allow Consumer Direct to transmit information electronically pursuant to the Uniform Electronic Transfer Act and HIPAA.
8. The Employer/DR agrees to the terms and conditions for payment set forth by the F/EA and approved by Adair Co SB40.
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 5 of 8
02780
9. If the Individual’s service needs exceed the monthly estimated authorization, the Support Coordinator must be informed. Approval from Adair Co SB40 is required to authorize any increase in the annual budget.
10. The Employer/DR shall not schedule Employees to work more than 40 hours in a work week without prior authorization. Exemptions to scheduling Employees over 40 hours per week must be approved by the Adair Co SB40, the need must be justified in the ISP, and the needs must be reviewed quarterly. Employees of the Individual/Guardian or Designated Representative fall within the category of domestic service workers. Domestic service workers may be exempt from overtime, when performing as a companion, providing care, fellowship and protection to persons with disabilities. Services may include general household work related to the Individual’s care as long as such work does not exceed 20 percent of total weekly hours worked.
11. The Employer/DR must not supplement wages to the Employee outside of this agreement. Records maintained by the F/EA will be the official records of the Employer’s wages to workers, which will be reported to State and Federal tax authorities. The Employer/DR understands all earnings and taxes for Employees must be accurately reported to these taxing authorities.
12. Any service hours provided before all requirements of this Agreement and applicable agreement(s) with Employee(s) are completed will not be payable by this Agreement and shall be the responsibility of the Employer/DR. Consumer Direct will issue an "Okay to Work" approval form to the Employer/DR upon receipt and approval of all Employee paperwork and receipt of a successful Family Care Safety Registry background screening for the prospective Employee. This will serve as the Employee's authorization to begin working. Consumer Direct cannot pay for time worked prior to the start date listed on the Okay to Work form.
13. The Employer/DR does not offer Employee fringe benefits such as long-term disability, paid holidays, sick leave, or vacation days.
RESPONSIBILITIES OF CONSUMER DIRECT
1. Provide the Employer/Designated Representative with an Enrollment Packet, Employee Packet(s) and Employee training materials.
2. Pay wages to Employees on a bi-weekly schedule, in accordance with the time sheets approved, in writing (or electronically through the Web Portal), by the Employer/DR. All money due to the Employee at the time of termination will be paid by the F/EA if the Employee has submitted proper documentation which the Employer/DR has approved.
3. Deposit Employer-related taxes, in the aggregate, using the F/EA’s designated FEIN.
4. Follow all IRS and State reporting guidelines. This will begin with the Individual’s Start Date even though this date is prior to the formal IRS authorization.
5. Obtain Fiscal Employer Agency authorization pursuant to IRS Revenue Procedure 70-6 and follow all IRS guidelines including obtaining all proper Federal and State authorizations.
6. Follow all tax exemptions and withholdings as stated on Employee’s W-4, and process all tax withholdings & filings including Federal and State income taxes, FICA, Medicare tax, FUTA, and SUTA, and any other mandated withholdings, as appropriate, on behalf of the Individual. Consumer Direct will maintain records of all withholdings, filings and payments. The F/EA will provide the
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 6 of 8
02781
Employee with Federal and State tax withholding information on his or her paystub for each pay period and will furnish the Employee with end of year statements for filing Federal, State and local income tax returns.
7. Track expenditures and maintain this spending information on the Web-Portal. The Employer/DR is responsible for monitoring the spending reports and not using more service hours or budget amounts than approved.
8. Submit all claims for services to Adair Co SB40 on behalf of the Individual.
9. Upon termination of this Agreement, Consumer Direct will complete all required Federal and State filing requirements related to services rendered from the Start Date to the Date of Termination, even though these filings are made subsequent to the termination date, pursuant to Federal and State laws.
10. Consumer Direct will adjust payroll deductions to reflect that the State of Missouri exempts an FEIN Holder, designated as a “Household Employer,” from the State requirement for employers to maintain Workers’ Compensation and Unemployment Insurance. The F/EA will make contributions to the workers’ Compensation Insurance carrier on behalf of the Employer.
Additional Agreement Terms and Conditions
Indemnification: Consumer Direct is in no position to monitor, supervise and watch over the Employees in the performance of their duties; therefore, the Employer/DR agrees to indemnify, which means to repay, defend and hold harmless Consumer Direct from any claims, causes of actions, complaints, lawsuits claiming any damages or liability against Consumer Direct, as the result of any actions, inactions, or any conduct by the Employee, while employed by the Employer/DR. This Indemnification Agreement includes any claims for damage to the Individual’s property or person, or the property or person of any third party. The Employer/DR understands that this means that the Employer/DR will be required to pay for all claims of damages caused by their Employee(s) while employed by the Employer/DR, made against Consumer Direct, including the costs that Consumer Direct incurs in defending itself against such claims. Hold Harmless Provision: In determining Employee’s pay, Adair Co SB40 and its F/EA shall have the right to rely, without further inquiry or substantiation, on the time sheets presented by the Employee and approved by the Employer/DR. Adair Co and its F/EA shall not be responsible for any errors in any payments consistent with such approved time sheets. Partial Invalidity: If something in this Agreement does not apply or changes with time, it does not mean the rest of the Agreement does not apply. If one part of this Agreement is determined to be invalid, the rest of the Agreement remains in place. Arbitration: Consumer Direct and the Employer/DR agree that they will attempt to resolve any complaints, misunderstandings and other issues between themselves. If Consumer Direct or the Employer/DR decides that they cannot settle a disagreement by working together, they will choose someone together to work out the disagreement. This is called arbitration. The cost of arbitration will be paid equally between Consumer Direct and the Employer/DR. The decision of the Arbitrator may be given to a judge, in the event the decision is not accepted by either party.
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 7 of 8
02782
State Law: If the Employer/DR cannot solve a problem through negotiation or talking about the problem, then State laws will apply. Any legal action related to this Agreement will be conducted in the County where the Individual resides. Duration and Modification of Agreement: This Agreement will go into effect on the date indicated on the first page of this Agreement. Services may not begin until approved by Adair Co SB40 (“Start Date”). Any changes to this Agreement must be in writing, signed and dated by both the Employer, (or Designated Representative, if applicable) and Consumer Direct. The Agreement may be terminated as described in the Termination section. Timely Notification: The Employer/DR and Consumer Direct agree that all contact should occur in a timely manner. Any notice will be given immediately, so that the Employer/DR or Consumer Direct is not hurt by a delay. Entire Agreement: This Agreement and other written materials provided by Consumer Direct to the Employer/DR describe the complete understanding between Consumer Direct and Employer/DR. Any verbal agreements do not apply. All Agreements must be in writing. Termination: This Agreement can be terminated in three ways:
a. Mutual Agreement* - At any time, with written documentation.
b. Termination Without Cause* - Involuntary termination of TRS Self-Directed option: i. If the planning team determines the health and safety of the Individual receiving
services is at risk, the option of receiving Temporary Residential Support Self-Directed Option may be terminated. Further, termination could occur if there are concerns regarding the Individual’s ability to stay within budgeted authorization, or if the Employer/DR is unwilling to supervise Employees to receive services according to his or her service plan. The Employer/DR must ensure that proper documentation of services is maintained. Before terminating Temporary Residential Support Self-Directed Option, the Support Coordinator and other appropriate staff will first counsel the Employer/DR receiving services to assist them in understanding the issues, let them know what corrective action is needed, and offer assistance in making changes. If they refuse to cooperate, the option may be terminated. However, the same level of services would be offered to the Individual through an agency model.
ii. The Party wishing to terminate must give written notice of its decision to terminate this Agreement.
c. Termination for Cause* - Voluntary termination of TRS Self-Directed option:
i. For voluntary termination of TRS, the Support Coordinator will work with the Individual receiving services to select a provider agency and transition services to the agency model. The Support Coordinator and other Adair Co SB40 staff will make every effort for the transition to be smooth and to ensure the Individual is not without services during the transition.
Adair County SB40 Temporary Residential Support Self-Directed Option
FISCAL EMPLOYER AGENT SERVICES AGREEMENT
Rev. 01/04/2017 Page 8 of 8
02783
ii. If any Party to this Agreement does not comply with the terms of this Agreement or follow the policies and procedures established by Adair Co SB40, the other Party may provide written notice of the non-compliance and terminate this Agreement.
Assignment: Neither this Agreement nor any of the rights, benefits, duties or obligations provided for in this Agreement may be assigned by the Employer/DR to someone else without the prior, written consent of Consumer Direct. HIPAA Consent: The Employer/DR authorizes Consumer Direct to submit Personal Healthcare Information (“PHI”) to: Adair Co SB40, entities that Consumer Direct has a Referral Source Agreement with, and contractors in order to facilitate access to services and secure an authorization needed to initiate services. Consumer Direct will handle PHI in accordance with their published Privacy Practices – a copy of which is included in the enrollment materials.
CONCLUSION
The FEIN Holder is the Employer (of Fact and of Record). The Employer/DR understands and accepts responsibility for recruiting, hiring, training, supervising and terminating their Employee(s). The Employer/DR is responsible for the actions of their Employees while they are providing services. Acceptance of this Agreement is shown by signing below. Missouri Consumer Direct Representative, Signature Date Printed Name Individual or Guardian, Printed Name Signature Date Designated Representative, Printed Name Signature Date
Form SS-4(Rev. December 2017)
Department of the Treasury Internal Revenue Service
Application for Employer Identification Number(For use by employers, corporations, partnerships, trusts, estates, churches, government agencies, Indian tribal entities, certain individuals, and others.)
Go to www.irs.gov/FormSS4 for instructions and the latest information.
See separate instructions for each line. Keep a copy for your records.
OMB No. 1545-0003
EINT
yp
e o
r p
rin
t c
lea
rly.
1 Legal name of entity (or individual) for whom the EIN is being requested
2 Trade name of business (if different from name on line 1) 3 Executor, administrator, trustee, “care of” name
4a Mailing address (room, apt., suite no. and street, or P.O. box) 5a Street address (if different) (Do not enter a P.O. box.)
4b City, state, and ZIP code (if foreign, see instructions) 5b City, state, and ZIP code (if foreign, see instructions)
6 County and state where principal business is located
7a Name of responsible party 7b SSN, ITIN, or EIN
8a
Is this application for a limited liability company (LLC) (or a foreign equivalent)? . . . . . . . . Yes No
8b If 8a is “Yes,” enter the number of LLC members . . . . . .
8c If 8a is “Yes,” was the LLC organized in the United States? . . . . . . . . . . . . . . . . . . Yes No
9a Type of entity (check only one box). Caution. If 8a is “Yes,” see the instructions for the correct box to check.
Sole proprietor (SSN) Estate (SSN of decedent)
Partnership Plan administrator (TIN)
Corporation (enter form number to be filed) Trust (TIN of grantor)
Personal service corporation Military/National Guard State/local government
Church or church-controlled organization Farmers’ cooperative Federal government
Other nonprofit organization (specify) REMIC Indian tribal governments/enterprises
Other (specify) Group Exemption Number (GEN) if any 9b
If a corporation, name the state or foreign country (if applicable) where incorporated
State Foreign country
10 Reason for applying (check only one box) Banking purpose (specify purpose)
Started new business (specify type) Changed type of organization (specify new type)
Purchased going business
Hired employees (Check the box and see line 13.) Created a trust (specify type)
Compliance with IRS withholding regulations Created a pension plan (specify type)
Other (specify) 11 Date business started or acquired (month, day, year). See instructions. 12 Closing month of accounting year
13
Highest number of employees expected in the next 12 months (enter -0- if none). If no employees expected, skip line 14.
Agricultural Household Other
14 If you expect your employment tax liability to be $1,000 or less in a full calendar year and want to file Form 944 annually instead of Forms 941 quarterly, check here. (Your employment tax liability generally will be $1,000 or less if you expect to pay $4,000 or less in total wages.) If you do not check this box, you must file Form 941 for every quarter.
15 First date wages or annuities were paid (month, day, year). Note: If applicant is a withholding agent, enter date income will first be paid to nonresident alien (month, day, year) . . . . . . . . . . . . . . . . .
16 Check one box that best describes the principal activity of your business. Health care & social assistance Wholesale-agent/broker
Construction Rental & leasing Transportation & warehousing Accommodation & food service Wholesale-other Retail
Real estate Manufacturing Finance & insurance Other (specify)
17 Indicate principal line of merchandise sold, specific construction work done, products produced, or services provided.
18 Has the applicant entity shown on line 1 ever applied for and received an EIN? Yes No
If “Yes,” write previous EIN here
Third
Party
Designee
Complete this section only if you want to authorize the named individual to receive the entity’s EIN and answer questions about the completion of this form.
Designee’s name Designee’s telephone number (include area code)
Address and ZIP code Designee’s fax number (include area code)
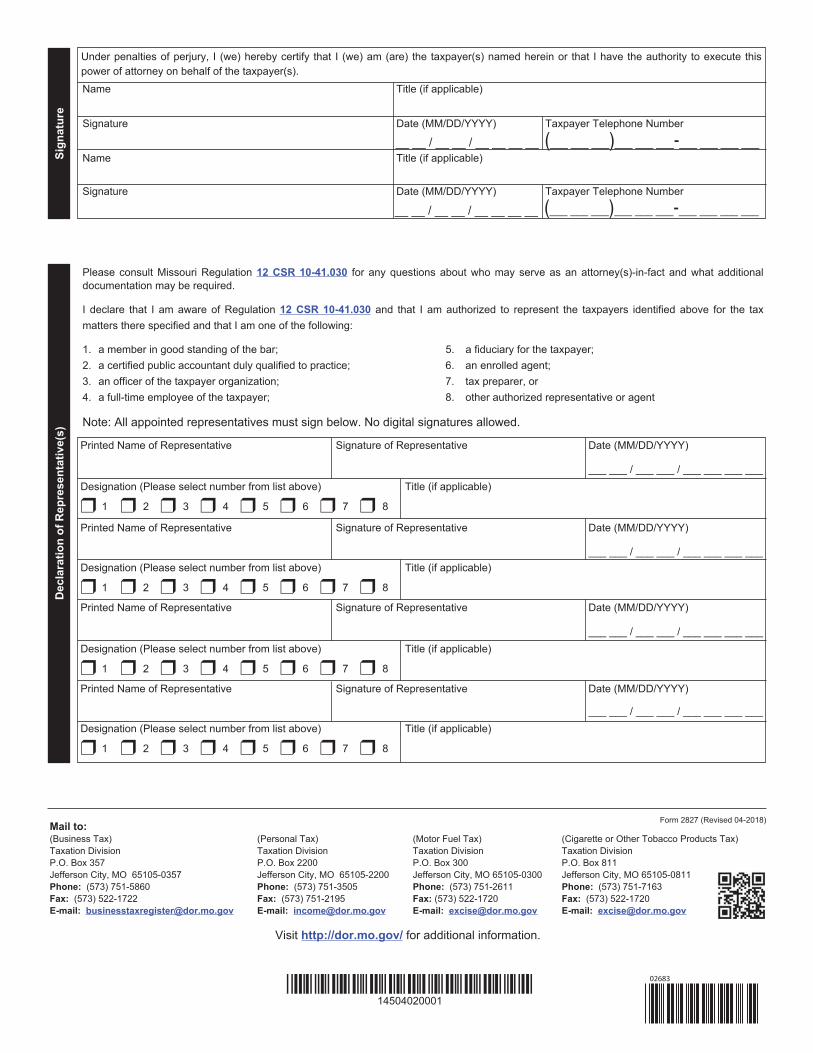
Under penalties of perjury, I declare that I have examined this application, and to the best of my knowledge and belief, it is true, correct, and complete.
Name and title (type or print clearly)
Applicant’s telephone number (include area code)
Signature Date
Applicant’s fax number (include area code)
For Privacy Act and Paperwork Reduction Act Notice, see separate instructions. Cat. No. 16055N Form SS-4 (Rev. 12-2017) 05151

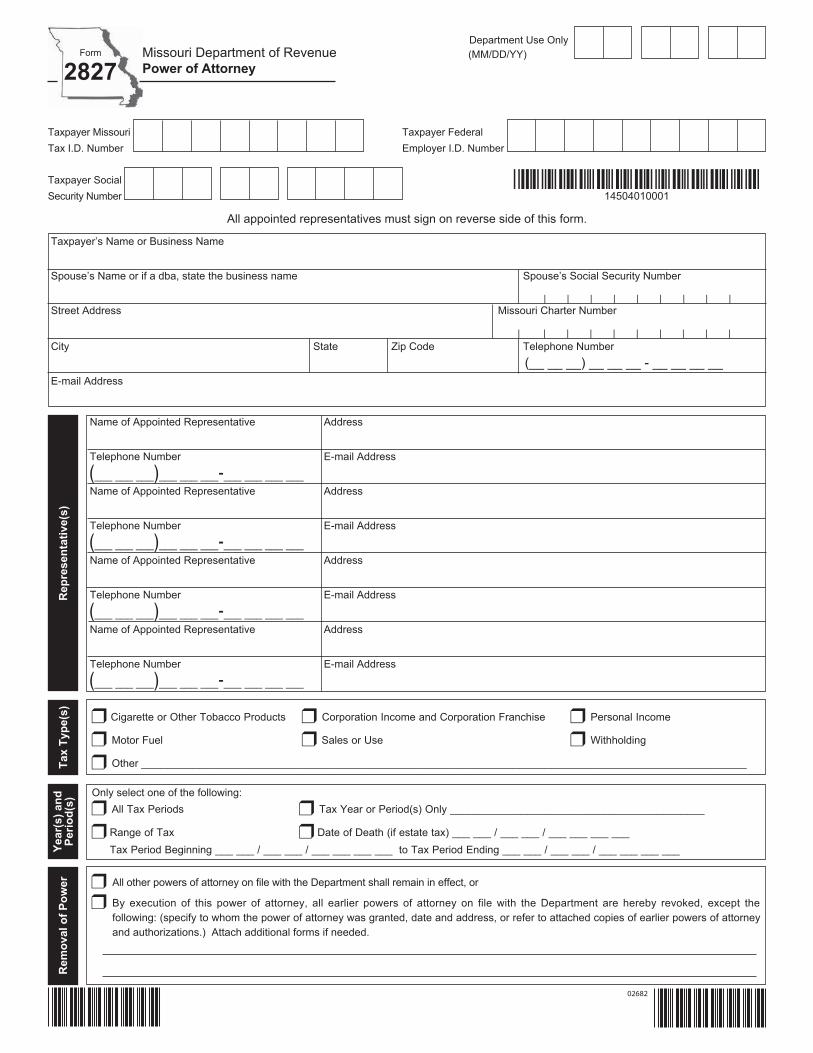
Form 2678(Rev. August 2014)
Employer/Payer Appointment of AgentDepartment of the Treasury — Internal Revenue Service
OMB No. 1545-0748
Use this form if you want to request approval to have an agent file returns and make
deposits or payments of employment or other withholding taxes or if you want to
revoke an existing appointment.
• If you are an employer or payer who wants to request approval, complete Parts 1 and 2 and sign Part 2. Then give it to the agent. Have the agent complete Part 3 and sign it.
Note. This appointment is not effective until we approve your request. See the instructionsfor filing Form 2678 on page 3.
• If you are an employer, payer, or agent who wants to revoke an existing appointment, complete all three parts. In this case, only one signature is required.
For IRS use:
Part 1: Why you are filing this form...
(Check one) You want to appoint an agent for tax reporting, depositing, and paying. You want to revoke an existing appointment.
Part 2: Employer or Payer Information: Complete this part if you want to appoint an agent or revoke an appointment.
1 Employer identification number (EIN) —
2 Employer’s or payer’s name (not your trade name)
3 Trade name (if any)
4 Address
Number Street Suite or room number
City State ZIP code
Foreign country name Foreign province/county Foreign postal code
5 Forms for which you want to appoint an agent or revoke the agent’s
appointment to file. (Check all that apply.) For ALL
employees/ payees/payments
For SOME employees/
payees/payments
Form 940, 940-PR (Employer's Annual Federal Unemployment (FUTA) Tax Return)*Form 941, 941-PR, 941-SS (Employer’s QUARTERLY Federal Tax Return) Form 943, 943-PR (Employer’s Annual Federal Tax Return for Agricultural Employees) Form 944, 944(SP) (Employer’s ANNUAL Federal Tax Return) Form 945 (Annual Return of Withheld Federal Income Tax) Form CT-1 (Employer’s Annual Railroad Retirement Tax Return) Form CT-2 (Employee Representative's Quarterly Railroad Tax Return)
*Generally you cannot appoint an agent to report, deposit, and pay tax reported on Form 940, Employer's Annual Federal Unemployment (FUTA) Tax Return, unless you are a home care service recipient.
Check here if you are a home care service recipient, and you want to appoint the agent to report, deposit, and pay FUTA tax for you. See the instructions.
I am authorizing the IRS to disclose otherwise confidential tax information to the agent relating to the authority granted under this appointment, including disclosures required to process Form 2678. The agent may contract with a third party, such as a reporting agent or certified public accountant, to prepare or file the returns covered by this appointment, or to make any required deposits and payments. Such contract may authorize the IRS to disclose confidential tax information of the employer/payer and agent to such third party. If a third party fails to file the returns or make the deposits and payments, the agent and employer/payer remain liable.
Sign your
name here
Date / /
Print your name here
Print your title here
Best daytime phone
Now give this form to the agent to complete. ■
For Privacy Act and Paperwork Reduction Act Notice, see the instructions. IRS.gov/form2678 Cat. No. 18770D Form 2678 (Rev. 8-2014)05152

5. Ownership Type Sole Proprietor Partnership Government TrustAll ownership types listed below, unless specifically exempted, are required to be registered with the Missouri Secretary of State’s Office (register at sos.mo.gov or call (866) 223-6535). Your application will not be complete without providing the charter number issued to you by their office.
Limited Partnership - LP Number __________________________________
Limited Liability Partnership - LLP Number ___________________________
Limited Liability Company - LLC Number ____________________________
Taxed as a Disregarded Entity Partnership Corporation
Missouri Corporation - Missouri Charter No. _________________________ Date Incorporated (MM/DD/YYYY) ___ ___ / ___ ___ / ___ ___ ___ ___
Non-Missouri Corporation - Missouri Charter No. ______________________State of Incorporation _________________________ Date Registered in Missouri (MM/DD/YYYY) ___ ___ / ___ ___ / ___ ___ ___ ___
3. Select all tax types for which you are applying:Sales from a Missouri business location
Retail Sales*
Temporary Retail Sales* (Less than 191 days)
Retail Liquor or Alcohol Sales*
Sales or Purchases from an out-of-state location
Vendor’s Use*
Consumer’s Use (Missouri purchases where tax is not collected.)
Missouri Employer Withholding Tax
Regular Withholding
Domestic or Household Employee
Transient Employer*
Corporate Tax
Corporate Income
Corporate FranchiseRea
son
for A
pplic
atio
n
New MO Registration
Purchase of Existing Business
Reinstating Old BusinessConverted (must have convertedthrough the Missouri Secretary ofState’s office)
Court Appointed Receiver
Other:Rea
son
for A
pply
ing
*Bond Required
Answer all questions completely. Incomplete and unsigned applications will delay processing..
Form
2643Missouri Department of RevenueMissouri Tax Registration Application
Missouri Tax I.D. Number(Optional)
Federal EmployerI.D. Number
Department Use Only(MM/DD/YY)
4. Owner Name (Enter Corporation, LLC or Partnership Name, if applicable)
Address E-mail Address
City State ZIP Code County
If an individual is listed as the owner, you must also provide the following: Social Security Number Date of Birth (MM/DD/YYYY) Telephone Number | | | | | | | |
Ow
ner I
nfor
mat
ion
___ ___ / ___ ___ / ___ ___ ___ ___ (___ ___ ___)___ ___ ___-___ ___ ___ ___
Ow
ners
hip
Type Not Required to register with Missouri Secretary
of State
Other
Prev
ious
Ow
ner I
nfor
mat
ion
6. Is there a previous owner or operator for the business? Yes* No *If yes, the following section must be completed.
Name of Previous Owner or Operator
Physical Location of Previous Business City State ZIP Code
Address of Previous Business City State ZIP Code
Select any of the following that you purchased from the previous owner: Inventory Fixtures Equipment Real Estate
Other __________________________________________________________________________________________________________
_____________________________________________________________________
Missouri Tax Identification Number | | | | | | |
Purchase Price
*14605010001*14605010001
3
02848
4
*14605020001*14605020001
8. Physical Address City State ZIP CodeAddress where you will store your tax records (do not use a P.O. Box for record storage).
Mai
ling
and
Stor
age
Addr
ess
Which forms do you want mailed to this address?All Tax Types Sales and Use Tax Corporate Income Tax Employer Withholding Tax
Reporting forms and notices will be mailed to this address.7. Address (street, rural route or P.O. Box) City State ZIP Code
Company Name if different than owner
Offi
cers
, Par
tner
s, o
r Mem
bers
9. Provide the officers, partners, or members (L.L.C.) of your business who are responsible for the collection and remittance of tax.Listing individuals or entities here indicates they have direct supervision or control over tax matters. Attach list if needed.
Name (Last, First, Middle Initial) Title
Social Security Number Federal Employer ID Number (FEIN) Date of Birth (MM/DD/YYYY)
Home Address City
State ZIP Code County Title Begin Date (MM/DD/YYYY)
| | | | | | | | ___ ___/___ ___/___ ___ ___ ___ | | | | | | | |
___ ___/___ ___/___ ___ ___ ___Name (Last, First, Middle Initial) Title
Social Security Number Federal Employer ID Number (FEIN) Date of Birth (MM/DD/YYYY)
Home Address City
State ZIP Code County Title Begin Date (MM/DD/YYYY)
| | | | | | | | ___ ___/___ ___/___ ___ ___ ___ | | | | | | | |
___ ___/___ ___/___ ___ ___ ___
Rep
rese
ntat
ives
10. Business Tax Accounts: control over tax matters whom you authorize the Department to discuss your tax matters. Attach list if needed.
Title Begin or End Date (MM/DD/YYYY) Name (Last, First, Middle Initial)
Title Social Security Number Birthdate (MM/DD/YYYY)
Home Address
City State ZIP Code County
| | | | | | | | __ __ / __ __ / __ __ __ __
__ __ / __ __ / __ __ __ __
Ret
ail S
ales
, Con
sum
er’s
or V
endo
r’s U
se T
ax
11. Taxable Sales or Purchases Begin Date (MM/DD/YYYY) ___ ___/___ ___/___ ___ ___ ___
12. Temporary License (Less than 191 days) (MM/DD/YYYY)(Example: fireworks, temporary event, etc.) Begins ___ ___/___ ___/___ ___ ___ ___ Ends ___ ___/___ ___/___ ___ ___ ___
13. Seasonal Business: If you do not make taxable sales year round, please check the months that you do.
January February March April May June July August September October November December
Monthly (over $500 a month) Quarterly ($500 or less a month) Annually (less than $100 a quarter)
15. Compute the amount of bond Estimated Monthly Taxable Sales Tax Rate Monthly Tax Liability Amount of Bond*
___________________________ X ___________________ = ___________________________ X 2 = _______________________Visit https://mytax.mo.gov/rptp/portal/home/business/salesUseTaxRateInformation/ to obtain your tax rate. *If you calculate the amount of bond to be less than $500, you are only required to submit a $25 bond. If you calculate your bond to be $500 or greater, you should submit the amount of bond figured. If the Department determines the bond is insufficient to cover your tax liability, the Director of Revenue may require you to adjust the bond amount to a level satisfactory to cover your tax liabilities or if returns are not filed timely and the taxes fully paid (see 12 CSR 10-104.020). Attach the appropriate bond form to your registration based on the type of bond checked.Visit http://dor.mo.gov/faq/business/register.php to access frequently asked questions.
16. Type of bond (no personal or company checks) Visit http://dor.mo.gov/forms/index.php?category=13 to access bond forms.
Cash Bond (Form 332) Irrevocable Letter of Credit (Form 2879) Surety Bond (Form 331)
02849
5
*14605030001*14605030001
17. Business Name (DBA name: attach list if necessary for additional locations)
Street, Highway (Do not use P.O. Box Number or Rural Route Number) City
County State ZIP Code Business Telephone Number
Retail _____% Wholesale _____% Service _____% Manufacturer Contractor Other _______________
19. Is this business located inside the city limits of any city or municipality in Missouri? To verify go to https://mytax.mo.gov/rptp/portal/home/business/salesUseTaxRateInformation
No Yes — Specify the city: _________________________________________________________________________20. Is this business located inside a district(s)? For example, ambulance, fire, tourism, community or transportation development.
No Yes — Specify the district name(s): ________________________________________________________________21. Describe the business activity, stating the major products sold and services provided. ___________________________________________
________________________________________________________________________________________________________________
18. Will sales be made at various temporary locations in Missouri?
No Yes—Attach a list of all known locations. If no Missouri location is given during initial registration, a general location will be used.
Bus
ines
s N
ame
and
Phys
ical
Loc
atio
n
(___ ___ ___)___ ___ ___-___ ___ ___ ___
Bus
ines
s A
ctiv
ity
22. Do you make retail sales of the following items? Select all that apply.
Alcoholic Beverages Alternative Nicotine Cigarettes or Other Tobacco Products Domestic Utilities
E-Cigarettes or Vapor Products Food Subject to Reduced State Food Tax Rate Items Qualifying for Show Me Green Sales Tax Holiday
Items Qualifying for Back-To-School Sales Tax Holiday http://dor.mo.gov/business/sales/taxholiday/ Lead-Acid Batteries
New Tires Post-Secondary Educational Textbooks Telecommunication Services
Qualifying Utilities or Items Used or Consumed in Manufacturing or Mining, Research and Development, or Processing Recovered Materials.
23. Do you make retail sales of aviation jet fuel to Missouri customers? ........................................................................................... Yes NoIf yes, are your sales made at:
A Missouri airport? A location outside Missouri and the fuel is transported into Missouri?................ Yes No
If yes, provide a list of applicable locations. _____________________________________________________________________________
24. Do you use, store, or consume aviation jet fuel in Missouri where the seller does not collect tax? ............................................. Yes No......................................................... Yes No
If yes, provide a list of applicable locations: _____________________________________________________________________________
25. Do you lease or rent motor vehicles that were purchased sales tax exempt, to Missouri customers? ........................................ Yes NoIf you are an out-of-state company, will you lease motor vehicles to a Missouri resident where the lease is entered intooutside Missouri and the motor vehicle is delivered outside Missouri?........................................................................................ Yes No
Out
-of-S
tate
Com
pany
26. Do you have a location or job site in Missouri? .......................................................................................................................... Yes NoIf yes, attach a list of your locations including address, city, state, zip code and indicate if the location is inside or outsidethe city limits. ____________________________________________________________________________________________________
27. Are orders taken from your Missouri customers by telephone, non-resident salesmen, etc.? If resident salesmen, attacha list where they live and indicate if they are inside or outside the city limits............................................................................. Yes No
28. Do your representatives who reside in Missouri:A. Approve customer orders?..................................................................................................................................................... Yes NoB. Make on the spot sales?........................................................................................................................................................ Yes NoC. Maintain an inventory?........................................................................................................................................................... Yes NoD. Deliver merchandise to the customer? .................................................................................................................................. Yes No
29. Do you have non-resident representatives, agents, or temporary employees coming into Missouri on a regular basis? ......... Yes No
If yes, define the activities performed while in Missouri. ______________________________________________________________________________________________________________________________________________________________________
30. Do you have real or tangible personal property in Missouri? ..................................................................................................... Yes NoIf yes, please describe: ___________________________________________________________________________________
If you are an out-of-state entity doing business in Missouri, please answer the following questions. .
02850
6
Corp
orat
e In
com
e Ta
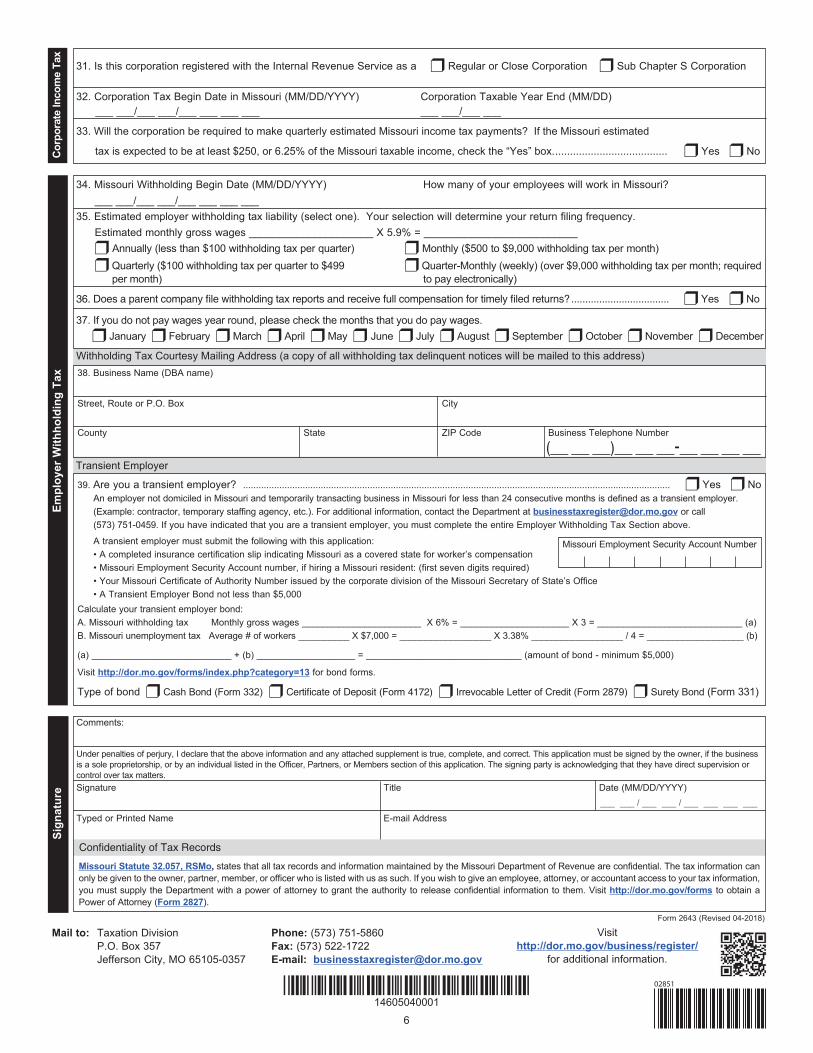
x31. Is this corporation registered with the Internal Revenue Service as a Regular or Close Corporation Sub Chapter S Corporation
32. Corporation Tax Begin Date in Missouri (MM/DD/YYYY) Corporation Taxable Year End (MM/DD) ___ ___/___ ___/___ ___ ___ ___ ___ ___/___ ___
33. Will the corporation be required to make quarterly estimated Missouri income tax payments? If the Missouri estimated
tax is expected to be at least $250, or 6.25% of the Missouri taxable income, check the “Yes” box....................................... Yes No
Mail to: Taxation Division Phone: (573) 751-5860 P.O. Box 357 Fax: (573) 522-1722Jefferson City, MO 65105-0357 E-mail: [email protected]
Visithttp://dor.mo.gov/business/register/
for additional information.
39. Are you a transient employer? ..................................................................................................................................................................... Yes NoAn employer not domiciled in Missouri and temporarily transacting business in Missouri for less than 24 consecutive months is defined as a transient employer. (Example: contractor, temporary staffing agency, etc.). For additional information, contact the Department at [email protected] or call(573) 751-0459. If you have indicated that you are a transient employer, you must complete the entire Employer Withholding Tax Section above.
A transient employer must submit the following with this application:• A completed insurance certification slip indicating Missouri as a covered state for worker’s compensation• Missouri Employment Security Account number, if hiring a Missouri resident: (first seven digits required)• Your Missouri Certificate of Authority Number issued by the corporate division of the Missouri Secretary of State’s Office• A Transient Employer Bond not less than $5,000
Calculate your transient employer bond:A. Missouri withholding tax Monthly gross wages _______________________ X 6% = _____________________ X 3 = ____________________________ (a)B. Missouri unemployment tax Average # of workers __________ X $7,000 = __________________ X 3.38% __________________ / 4 = ___________________ (b)
(a) ___________________________ + (b) ___________________ = ______________________________ (amount of bond - minimum $5,000)
Visit http://dor.mo.gov/forms/index.php?category=13 for bond forms.
Type of bond Cash Bond (Form 332) Irrevocable Letter of Credit (Form 2879) Surety Bond (Form 331)
Withholding Tax Courtesy Mailing Address (a copy of all withholding tax delinquent notices will be mailed to this address)
Transient Employer
Empl
oyer
With
hold
ing
Tax
34. Missouri Withholding Begin Date (MM/DD/YYYY) How many of your employees will work in Missouri?___ ___/___ ___/___ ___ ___ ___
35. Estimated employer withholding tax liability (select one). Your selection will determine your return filing frequency.Estimated monthly gross wages _____________________ X 5.9% = __________________________
Annually (less than $100 withholding tax per quarter) Monthly ($500 to $9,000 withholding tax per month) Quarterly ($100 withholding tax per quarter to $499 Quarter-Monthly (weekly) (over $9,000 withholding tax per month; required
per month) to pay electronically)
................................... Yes No
37. If you do not pay wages year round, please check the months that you do pay wages. January February March April May June July August September October November December
38. Business Name (DBA name)
Street, Route or P.O. Box City
County State ZIP Code Business Telephone Number
(___ ___ ___)___ ___ ___-___ ___ ___ ___
Sign
atur
e
Missouri Statute 32.057, RSMo, states that all tax records and information maintained by the Missouri Department of Revenue are confidential. The tax information canonly be given to the owner, partner, member, or officer who is listed with us as such. If you wish to give an employee, attorney, or accountant access to your tax information, you must supply the Department with a power of attorney to grant the authority to release confidential information to them. Visit http://dor.mo.gov/forms to obtain a Power of Attorney (Form 2827).
Signature Title Date (MM/DD/YYYY)
Typed or Printed Name E-mail Address___ ___ / ___ ___ / ___ ___ ___ ___
Under penalties of perjury, I declare that the above information and any attached supplement is true, complete, and correct. This application must be signed by the owner, if the business is a sole proprietorship, or by an individual listed in the Officer, Partners, or Members section of this application. The signing party is acknowledging that they have direct supervision or control over tax matters.
Comments:
Form 2643 (Revised 04-2018)
*14605040001*14605040001
Missouri Employment Security Account Number
02851
( ) -
( ) -
( ) -
( ) -
*14504010001*
02682
( ) -
( ) -
*14504020001*02683
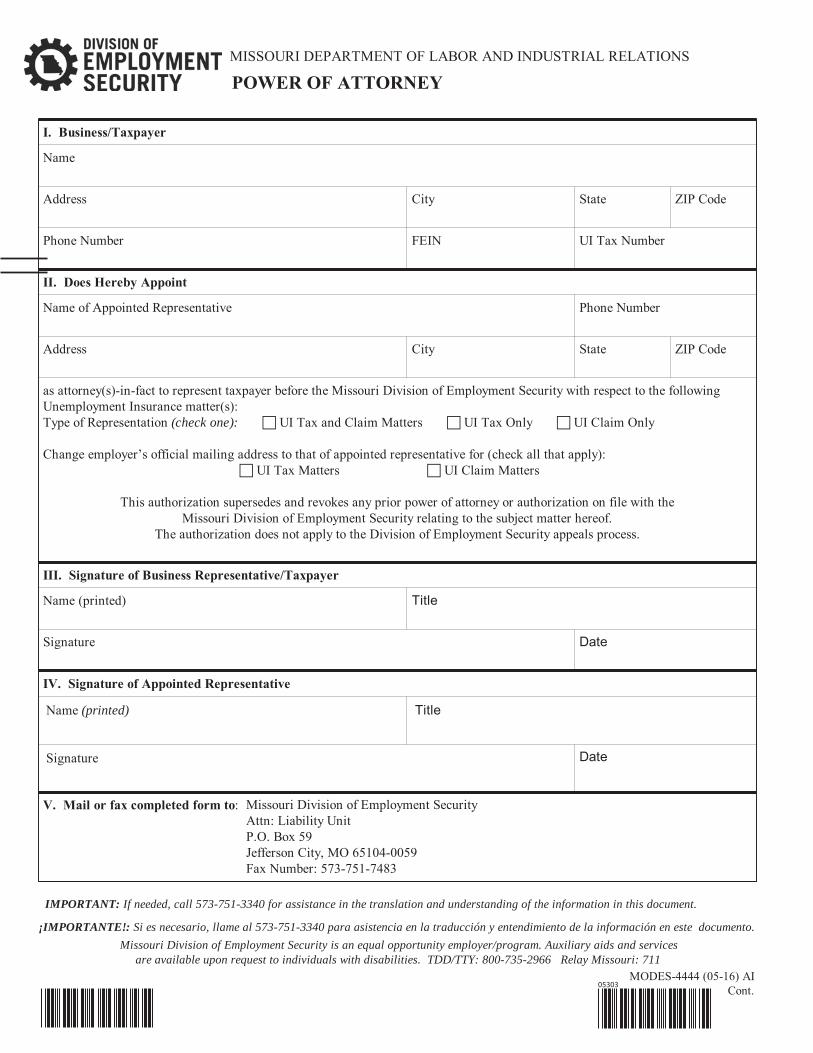
MISSOURI DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS
I. Business/Taxpayer
Name
Address City State ZIP Code
Phone Number FEIN UI Tax Number
II. Does Hereby Appoint
Name of Appointed Representative Phone Number
Address City State ZIP Code
as attorney(s)-in-fact to represent taxpayer before the Missouri Division of Employment Security with respect to the followingUnemployment Insurance matter(s):Type of Representation (check one): UI Tax and Claim Matters UI Tax Only UI Claim Only
Change employer’s official mailing address to that of appointed representative for (check all that apply):UI Tax Matters UI Claim Matters
This authorization supersedes and revokes any prior power of attorney or authorization on file with theMissouri Division of Employment Security relating to the subject matter hereof.
The authorization does not apply to the Division of Employment Security appeals process.
III. Signature of Business Representative/Taxpayer
Name (printed) Title
Signature Date
IV. Signature of Appointed Representative
Name (printed) Title
Signature Date
V. Mail or fax completed form to:
POWER OF ATTORNEY
IMPORTANT: If needed, call 573-751-3340 for assistance in the translation and understanding of the information in this document.
¡IMPORTANTE!: Si es necesario, llame al 573-751-3340 para asistencia en la traducción y entendimiento de la información en este documento.
Missouri Division of Employment Security is an equal opportunity employer/program. Auxiliary aids and servicesare available upon request to individuals with disabilities. TDD/TTY: 800-735-2966 Relay Missouri: 711
MODES-4444 (05-16) AICont.
Missouri Division of Employment SecurityAttn: Liability UnitP.O. Box 59Jefferson City, MO 65104-0059Fax Number: 573-751-7483
05303

![Names indexed from the Tithe Applotment Books …billmacafee.com/182030stithe/tithenorthantrim.pdf1851 Adair Adair James 1826 Cary Billy Clogher Lower [Low Clogher] 3867 Adair Adair](https://img.pdfslide.net/doc/110x75/5b3339c77f8b9a81728d252d/names-indexed-from-the-tithe-applotment-books-adair-adair-james-1826-cary-billy.jpg)