Embed Size (px)
Citation preview

REVIEWARTICLE
Adaptation, perceptual learning, and plasticity of brain functions
Jonathan C. Horton1& Manfred Fahle2 & Theo Mulder3 &
Susanne Trauzettel-Klosinski4
Received: 2 August 2016 /Revised: 6 December 2016 /Accepted: 28 December 2016 /Published online: 14 January 2017# The Author(s) 2017. This article is published with open access at Springerlink.com
Abstract The capacity for functional restitution after braindamage is quite different in the sensory and motor systems.This series of presentations highlights the potential for adap-tation, plasticity, and perceptual learning from an interdisci-plinary perspective. The chances for restitution in the primaryvisual cortex are limited. Some patterns of visual field loss andrecovery after stroke are common, whereas others are impos-sible, which can be explained by the arrangement and plastic-ity of the cortical map. On the other hand, compensatorymechanisms are effective, can occur spontaneously, and canbe enhanced by training. In contrast to the human visual sys-tem, the motor system is highly flexible. This is based onspecial relationships between perception and action and be-tween cognition and action. In addition, the healthy adult braincan learn new functions, e.g. increasing resolution above theretinal one. The significance of these studies for rehabilitationafter brain damage will be discussed.
Keywords Brain plasticity . Adaptation . Perceptuallearning . Visual cortex .Motor cortex . Rehabilitation
Introduction by S. Trauzettel-Klosinski
This symposium highlighted the potential for learning and re-learning after visual and motor cortex lesions in the adult brainfrom an interdisciplinary perspective. We considered mecha-nisms such as adaptation, plasticity, and perceptual learning ofdifferent brain functions, as well as their applications for re-habilitation in patients with brain damage. Additionally, thepotential for visual learning in the normal human brain wasdemonstrated.
In the visual system, the potential for recovery in the pri-mary visual cortex is limited (part 1 by Jonathan Horton).Visual field defects caused by embolic stroke are constrainedby the organization of the blood supply of the occipital lobewith respect to the retinotopic map. In terms of the arrange-ment and plasticity of the cortical map, it will be explainedwhy some patterns of visual field loss and recovery followingstroke are common, whereas others are essentially impossible.This is especially true along a visual field strip of constantwidth along the vertical meridian.
While the restitutive capacities of the primary visual cortexare limited, compensatory mechanisms can be very effective(part 2 by Susanne Trauzettel-Klosinski). They can occurspontaneously and can further be enhanced by training. Inhemianopia, for example, fixational eye movements and scan-ning saccades can shift the visual field border towards thehemianopic side and improve spatial orientation and mobility.
In contrast to the visual system, the human motor system ishighly flexible (part 3 by Theo Mulder). It is updated contin-uously by itself on the basis of sensory input and activity. Theplasticity of the motor system is based on a special
Synopsis of the Symposium BAdaptation, perceptual learning andplasticity of brain functions^ at the Meeting of the GermanOphthalmological Society 2015 in Berlin October 1–4, 2015
* Susanne Trauzettel-Klosinskisusanne.trauzettel-klosinski@uni-tuebingen.de
1 Beckman Vision Center, University of California, SanFrancisco, USA
2 Center for Cognitive Sciences, University of Bremen,Bremen, Germany
3 Royal Netherlands Academy of Arts and Sciences,Amsterdam, The Netherlands
4 Vision Rehabilitation Research Unit, Center for Ophthalmology,University of Tübingen, Tübingen, Germany
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447DOI 10.1007/s00417-016-3580-y

relationship between perception and action, as well as be-tween cognition and action. New approaches to rehabilitation,for example by motor imagery, give an outlook on futurepossibilities.
Additionally, the healthy adult brain can learn new visualfunctions (part 4 byManfred Fahle), for example the enhance-ment of resolution, which is higher than that of the retina.These functions, especially hyperacuity, can also be trained.
The authors will present a summary for each of the fourtalks.
Part 1: visual field recovery after lesionsof the occipital lobe by Jonathan C. Horton
Recently, I attended a 60-year-old woman who had a sponta-neous left parietal hemorrhage (Fig. 1). She underwent anemergency craniotomy to evacuate the hematoma. Her maindeficit was a severe aphasia, which improved slowly. Onceshe regained sufficient ability to communicate, shecomplained about her vision on the right side. Her examina-tion showed a total, macula-splitting right homonymoushemianopia. She has made nearly a complete recovery fromher stroke, except for this devastating visual field cut. It hasmade reading a chore, forced her to give up driving, and willprevent her from returning to her job. This is a common sce-nario: after surviving a neurological disaster, patients discoverthat vision loss represents their most serious and enduringdeficit. Why does central vision loss persist, and remain sostubbornly resistant to treatment?
The answer lies in the organization of the visual pathwayfrom eye to cortex. Retinal ganglion cell axons that are re-sponsible for conscious perception project to the lateral genic-ulate nucleus. It serves as a relay station, boosting the infor-mation content of outgoing spikes compared with incomingspikes by integrating and filtering retinal signals [1].Geniculate neurons send their projection to layer 4 of theprimary visual cortex. Simply by crossing a single synapsein the thalamus, retinal output is conveyed directly to theprimary visual cortex. In a sense, the retino-geniculo-corticalpathway is the aorta of our visual system (Fig. 2). After initialprocessing in the primary visual cortex, signals are analyzed insurrounding cortical areas that are specialized for differentattributes, allowing us to perceive the images that impingeupon our retinae.
Sprawling across the brain from eyes to occipital lobe, theretino-geniculo-cortical pathway is vulnerable to a multitudeof neurological insults. As every ophthalmologist knows, in-jury to the optic nerve, chiasm, or tract causes retrograde de-generation of ganglion cells in the retina. Downstream fromthe site of injury, retinal ganglion cell axons undergo antero-grade degeneration. Their terminals disintegrate in the lateralgeniculate nucleus. At present, there is no way to regenerate
lost retinal ganglion cells, and even if there were, there is noway to guide their axons to terminate in the correct location inthe lateral geniculate nucleus.
By the same token, injury to the visual cortex or opticradiations causes retrograde degeneration of neurons in thelateral geniculate nucleus. An example of a lesion in the pri-mary visual cortex of a monkey is shown in Fig. 3. It produceda zone of cell loss running through all the layers of the lateralgeniculate nucleus. It is important to bear in mind that a lesionof the calcarine fissure not only destroys cortical neurons, butamputates visual signals emanating from the lateral geniculatenucleus. Even if one could repair the cortical damage, loss ofinput from the lateral geniculate would be enough to shutdown vision.
The exquisite preservation of topographic order in the vi-sual system compounds the functional impairment wreakedby lesions of the retino-geniculo-cortical pathway. Each loca-tion in the visual field is represented serially at precise ana-tomical sites along the pathway, with no redundancy. Once asite is destroyed, vision is cut off, because there is no otherway around the choke point. In this respect, the visual systemis quite different from the auditory system. VIIIth nerve outputis supplied to the dorsal cochlear nucleus, ventral cochlearnucleus, medial accessory nucleus, and superior olivary nu-cleus on each side of the medulla. From the medulla, auditorysignals are fed to the nucleus of the lateral lemniscus and theinferior colliculus, again on both sides of the brainstem. Theyultimately reach the temporal lobes via the medial geniculatebodies. The crucial point is that information can reach theauditory cortex via several routes, because there exist multipledecussations and parallel relay streams. Moreover, the cortexin each hemisphere contains a representation of all frequenciesand all locations in space. Consequently, no deficit ensuesafter a unilateral lesion of primary auditory cortex. Clearly,different rules pertain in auditory, visual, motor, and languagecortex (see Mulder T, part 3 below).
Years ago, excitement followed reports that topographicmaps are plastic in the visual cortex, even in adults [2, 3]. Inexperimental animals, lesions were made in the retina with a
Fig. 1 CT scan showing an acute left parietal hematoma, causing a righthomonymous hemianopia. A CT scan performed 5 months later showsdamage to the left optic radiations. The visual field cut never recovered
436 Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447

laser, silencing a corresponding zone in the cortex. Afterwardsit was observed that the silent cortical zone eventually be-comes responsive to stimulation from surrounding, healthyretina. This result was surprising, because it was thought thatanatomical connections in the mature cortex lack the capacityto fill in large gaps created by deafferentation. Unfortunately,the phenomenonwas not replicable in other laboratories [4, 5].Even if real, it is hard to see how filling in could benefit visualfunction. The scotoma from the retinal laser burn remains,regardless of what happens in the cortex.
After a stroke, physical therapy can help patients recovermotor function. Can vision therapy do the same for the visualsystem, by shrinking field defects? Sabel and colleagues havedescribed partial recovery of homonymous hemianopiathrough computer-based rehabilitation therapy [6]. Subjectsundergo a daily training regimen, detecting stimuli presentedon a computer screen while they maintain fixation. The hopeis that stimulation of visual field represented by partially dam-aged brain tissue at the fringe of a stroke can promote recov-ery. Data have shown that improvement is particularly apt tooccur along the vertical meridian. In the occipital lobe, thevertical meridian corresponds to the perimeter of the primaryvisual cortex (Fig. 4). Strokes extend far beyond this frontier,but they produce a field cut that respects the vertical meridian.The sharp vertical edge to the hemianopia is because the intactvisual hemifield is represented in the other hemisphere of thebrain. It is remote from the stroke responsible for thehemianopia. This fact vitiates the theory that visual field re-covery along the vertical meridian is due to resuscitation ofdamaged, but viable cortex at the fringes of the lesion.
After onset of a hemianopia, patients learn to make fre-quent saccades towards their blind side, perhaps as a compen-satory mechanism [7]. This behavior is so powerful that pa-tients have trouble maintaining prolonged fixation on a
Fig. 2 Retinal input is conveyedto the primary (striate) cortex by atwo-neuron chain, crossing asingle relay in the lateralgeniculate nucleus. Injury at anypoint cuts off visual perception,although a small projection (greenshading) from the lateralgeniculate to area MT allowsBblindsight^ in patients withhomonymous hemianopia causedby a post-chiasmal lesion (pinkshading). After Polyak (1957)
Fig. 3 (Top) Flattened tissue section reacted for cytochrome oxidaseshowing a large lesion (arrow) of the primary visual cortex in amonkey. (Bottom) The lesion produced a swath of cell loss, visible in aNissl-stained section, running through all layers of the lateral geniculatenucleus (arrows). Relay neurons in the lateral geniculate die because theiraxon terminals are destroyed in the cortex
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447 437

stationary target. The strip of Brecovered^ visual field alongthe vertical meridian occurs because patients sneak frequentglances to the blind side. When testing is done by controllingfixation rigorously during perimetry, no significant benefit canbe detected from vision restoration therapy [8]. In other words,field improvement from vision therapy is an artifact of sloppypsychophysical testing.
Even in patients with infarction of calcarine cortex from aposterior cerebral artery occlusion, a crude ability to localizelarge moving objects is sometimes preserved. This residualvisual capacity has been given the catchy name Bblindsight^[9]. It may be due to a small projection from the lateral genic-ulate nucleus to a region in the parietal lobe known as BareaMT^ [10]. This region was discovered because it stains prom-inently for myelin, just like the primary visual cortex. It can bethought of as a small, accessory region of primary visual cor-tex, hanging like Tasmania off the Australian continent.Silencing the projection from the lateral geniculate nucleusto Area MT abolishes blindsight in monkeys [11]. Area MTlies outside the vascular territory of the posterior cerebral ar-tery, so it remains functional after occipital lobe stroke.Nonetheless, blindsight is too weak to provide much help topatients with hemianopia. One must concede that the goal ofrestoring sight after damage to the retino-geniculo-corticalpathway remains a profound challenge for scientists and cli-nicians. Ultimately, success will require gaining the ability toregenerate damaged neuronal tissue, learning how to graft itonto the patient’s brain, and then hooking it up properly toallow useful function.
Part 2: compensatory adaptation to visual field lossafter brain damage by Susanne Trauzettel-Klosinski
Hemianopia leads to orientation disorder, indicated bybumping into objects or persons, problems with route findingand impaired communication. In addition, if the visual fielddefect includes the visual field center, reading is severely im-paired. These impairments result in restricted participation insociety and a severe reduction of quality of life.
Spontaneous adaptive mechanisms
For rehabilitation of hemianopia, the investigation of sponta-neous adaptive mechanisms is crucial: Are these mechanismshelpful? Which patients have the potential to develop them?Can they be trained?
Fixational eye movements occur as a physiological phe-nomenon in healthy subjects to prevent fading and to maintain
�Fig. 4 a Right occipital lobe, with red shading to indicate the primaryvisual cortex. A large stroke (blue shading) from occlusion of theposterior cerebral artery is shown. b The calcarine fissure is opened toreveal the primary visual cortex. The stroke extends even beyond the edgeof the semi-flattened cortex, except posteriorly, where cortex is suppliedby the middle cerebral artery. c Flattened sheet of cortex, marking theboundaries of the stroke in (b) with a dashed line. Months after stroke,some recovery may occur at the fringes of the infarct, reducing theamount of cortical damage (shown schematically by shrinkage of theblue shading). However, the stroke still extends far beyond the bordersof the primary visual cortex, so no recovery of visual field along thevertical meridian should be expected
438 Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447

constant vision during fixation (for references see [12]). Inhemianopia, the fixational eye movements are asymmetrictowards the blind side, which causes a shift of the visual fieldborder to the blind side [12, 13]. This shift of the vertical fieldborder can be misinterpreted as an enlargement of the visualfield (Fig. 5).
Scanning eye movements: While viewing naturalisticscenes, patients were described to show increasingly differentfixation patterns from normal subjects, which indicates a com-pensating strategy [14].
Asymmetric eye movements towards the hemianopic side,which are small during fixation, occur as larger saccades toscan the blind hemifield by using the full field of gaze, i.e. toenlarge their Bfunctional visual field^ (for details see [15, 16]).
Regarding saccadic accuracy, short-term adaptation hasbeen described [7], but insufficient long-term adaptation[12], which is indicated by the increased number of dysmetricsaccades during gaze shift to the blind side.
Furthermore, a shift of attention to the blind side can behelpful to promote scanning saccades, because they are pre-ceded by movements of attention. A head turn alone does notchange the visual fields. However, a head turn in combinationwith scanning eye movements leads to an extension of thefunctional visual field by using the full field of gaze.
Exotropia with anomalous retinal correspondence can ex-tend the binocular visual field, which is then a contraindica-tion for strabismus surgery [17].
Rehabilitation of the hemianopic orientation disorder
For intervention studies the following general aspects have tobe considered:
1) Specificity:
– spontaneous recovery has to be excluded– a placebo effect has to be ruled out by use of a control
group
2) Quality of testing methods for assessing the effect :
– objectivity– validity (e.g. can the test show causal connections?)– reliability (e.g. exactness, repeatability)
3) Aim of the intervention
– Is the effect clinically relevant?– Is the effect persistent after training?
The main approaches in recent years were substitutive,restitutive, and compensatory.
Literature research regarding rehabilitation in hemianopiawas performed using Cochrane Reviews and randomized con-trolled trials (RCTs) in Cochrane and Pubmed for the period1990 – April 2016. The reference list of part 2 is restrictedmainly to overview articles and RCTs. Those after 2010 arecited directly in the list below, the majority of those publishedbefore 2010 are listed in the overview articles [15, 16].
The substitutive approach
The use of peripheral prisms to expand the functional visualfield without central diplopia yielded positive subjective
Fig. 5 Fixational eye movementsduring fixation of a cross areasymmetric towards the blindside, shown for right hemianopia:a assessment by scanning laserophthalmoscope (SLO), exampleof one patient. b in conventionalperimetry (schematic), the visualfield defect and the blind spot areshifted towards the blind side. cdistribution of fixational eyemovements in 25 patients withright hemianopia with absent orsmall (<4°) macular sparingassessed by SLO (based on 1000video fields per patient): the meanis shifted to 2.6 degrees to theright and is significantly differentfrom normal distributionmodified after [12]
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447 439

reports by the patients, but a conclusive judgment of the ben-efit is not possible at present.
The restitutive approach
The aim of restitutive training is to enlarge the visual fields byreactivating incompletely damaged neurons in the blindhemifield by visual stimulation. Earlier studies using visualstimulation along the vertical border of the field defect report-ed visual field enlargement [6], but it was later shown byfundus-controlled perimetry that fixational eye movementsshift the field defect towards the hemianopic side, which canbe misinterpreted as an enlargement of the visual field [8, 18].At present, there are no evidence-based studies available thatshow an effect of training to restitute the visual field.(Cochrane review [19]; for a recent review see [20] andHorton Part 1 in this article).
Regeneration of neurons in the primary visual cortex (V1)should be distinguished from extrastriate activation, alsocalled the Bblind-sight phenomenon^ (see Horton part 1above). BPhylogenetically old^ pathways via the lateral genic-ulate nucleus that bypass area V1, can be partly re-activatedby intense training. In some patients, this can lead to mostlyunconscious perception [20]. It is still an open question,whether residual vision of this kind can be improved to a levelthat is relevant to daily life.
The compensatory approach
The spontaneous mechanism of generating scanning eyemovements towards the hemianopic side is used and enhancedby compensatory saccadic training. Earlier non-controlledstudies reported positive effects, but the specificity of themethod was not proven. The specific positive effects of ex-plorative saccadic training was proven in the first randomizedand controlled trial by our group [21]: It selectively improvedsaccadic behavior, performance in an everyday search task(searching objects on a table) and natural scene exploration.The effects were also present in patients with longstandinghemianopia. The new saccadic strategy could be applied toeveryday life and the training effect remained stable after theend of the training. Quality of life in the social domainimproved.
Figure 6 shows the functional visual field for ahemianopic patient viewing the scene without eye move-ments (a) and with scanning eye movements (b). The de-tection of obstacles, here the baby stroller, is especiallyvaluable for avoiding collisions.
In the meantime, several randomized controlled trials(RCTs) have been performed (for an overview see [15, 16])that showed improvement of exploration and orientation byways of audio-visual stimulation, attentional training, a com-bined reading and exploration training [22], and a purely hor-izontal saccadic training task [23]. A systematic review onmultisensory stimulation did not allow a valid conclusionabout the effectiveness of this intervention [24]. Another in-teresting approach was reported using anti-saccadic training[25].
In summary, it is evident that after brain damage regenera-tion of the occipital cortex is quite limited, whereas compen-satory plasticity by extrastriate activation can lead to changesin gaze strategy with an improved adaptation to the demandsof everyday life.
The hemianopic reading disorder
Reading performance in hemianopia depends highly on itsconfiguration: In macular splitting, half of the reading visualfield is covered by the scotoma and is dysfunctional (Fig. 7a).In patients with macular sparing, the reading visual field (per-ceptual span during one fixation) can be fully spared andreading is not impaired (Fig. 7b). On the other hand, a smallparacentral homonymous scotoma can cover half of the read-ing visual field and lead to severe reading impairment(Fig. 7c).
Furthermore, the reading performance depends on theside of the field defect in regard to the reading direction[15, 16]: In languages that require moving the eyes fromleft to right along the line, patients are much more im-paired by a right hemianopia, indicated by an increasednumber of saccades and regressions and a severely re-duced reading speed. If a left hemianopia is present, pa-tients have the problem of finding the beginning of thenext line, indicated by several hypometric saccades duringthe return sweep.
Fig. 6 Exploration of a naturalscene in right hemianopia: a)without eye movements, b) withscanning eye movements the fieldof gaze is utilized and obstacles,here the baby stroller, can be seenin time
440 Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447

Spontaneous adaptive mechanisms for reading
A promising adaptive mechanism is eccentric fixation: a mi-nority of patients (approximately 20%) are able to use a slight-ly eccentric fixation locus, which shifts their visual field bor-der towards the hemianopic side and creates a narrow seeingstrip along the vertical field border (Fig. 7d). They can use thismechanism by sacrificing a bit of visual acuity and gaining aslightly enlarged reading visual field, which leads to homon-ymous eccentric fixation [15, 16]. Another favorable adaptivemechanism is making predictive saccades, especially in pa-tients with left hemianopia, who can learn to apply a singlehypermetric predictive saccade to find the beginning of thenew line.
Rehabilitation of the hemianopic reading disorder
Only few RCTs are available: It has been shown that readingscrolled text for right hemianopia was effective to improvereading speed [26]. Furthermore, reading speed increased byperforming a search task in a line of words [22] and anti-saccade training [25]. Other approaches, based on clinical ex-perience, are to help orientation on the page by use of visualand tactile aids, for example the index finger, a ruler or aslightly vertically magnifying ruler with a red guideline.Turning the text into a vertical or diagonal orientation hasnot been studied systematically yet.
To summarize, to aid the rehabilitation of hemianopia, onlycompensatory methods have been shown to be effective inevidence-based studies to date: For general orientation, byapplying visual and audio-visual search tasks, attentional
training and saccadic/anti-saccadic tasks. For reading, scrolledtext for right hemianopia and search task in a line of words.
Part 3: brain plasticity and recovery of motorfunction by Theo Mulder
Human motor behavior is not the result of a series of detailedmuscle-specific central commands, but is characterized by anextreme flexibility. Almost without any effort we can pick upa cup with the right hand, with the left hand, we can even pickit up by using our feet as the main effector organs. We canwalk forward, backward, we can jump, dance, run, shuffle,and produce all sorts of silly walks. Without any problemwe are able to produce an almost infinite stream ofmovementsin order to reach goals in the environment.
For a large part, motor behavior can be seen as problemsolving. We are forced to find solutions for the problemswhich appear in a continuously changing environment. Theobtained solutions, however, are never static, but always tai-lored to the actual requirements. Indeed, when the environ-mental constraints are never the same, the solutions can alsonever be the same.
This is an important point since it indicates that motorcontrol cannot be the result of a rigid hierarchically organizedsystem, generating efferent commands to individual musclesand joints on basis of motor programs stored in a huge neuralwarehouse. The control is for a large part non-hierarchical,self-organizing, and driven by multisensory input.Furthermore, the organism never functions in vacuo, discon-nected from its history and without any knowledge. On the
Fig. 7 Reading in hemianopiadepends on the configuration ofthe field defect and the availableperceptual span during onefixation: a In macular splitting,half of the reading visual field iscovered and functionless,resulting in severe readingimpairment. b In macular sparing,the reading visual field can bespared and reading can be normal.c A paracentral homonymousscotoma leads to severe readingimpairment. d Eccentric fixationshifts the field defect towards thehemianopic side and creates asmall perceptual strip along thevertical field border, a favorableadaptive mechanism
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447 441

contrary, almost all actions are influenced by knowledge andexperience. We have learned how to handle a cup, toride a bicycle, to write, to play the violin, to dance.Even the most simple actions such as how to open adoor are influenced by learning. We know, for example,when to push and when to pull on basis of knowledgederived from experience. Hence, motor processes con-tinuously interact with cognitive and perceptual process-es. This interaction between perception, action, andknowledge forms the basis for human motor behavior.Only in this way we are able to cope with the environ-mental instability [27].
I will describe the human motor system with an em-phasis on flexibility and change. It will be shown thatthe human motor system is continuously updating itselfon the basis of sensory input and activity. The abovementioned intimate relationship between perception andaction, but also between cognition and action will bestressed.
The human brain is a biological system of ultimate com-plexity, consisting of 100 billion nerve cells (neurons), where-by each neuron is connected with thousands of other cellscreating an information processing network whose detailedfunction is still largely unknown. For a long time it wasthought that the adult brain was a fixed organ as is reflectedin the famous statement of Santiago Ramon y Cajal [28]: BInadult brain centers, the nerve paths are fixed, ended, immo-bile. Everythingmay die, nothing may be regenerated^. Whenwriting this, Cajal knew that the brain showed flexibility, buthe was more or less caught in the dominant paradigm.
Franz Joseph Gall
It was in Vienna in the early nineteenth century that FranzJoseph Gall (see [29]) presented a more optimistic viewon the human brain. In a way he was far ahead of his timewhen he argued that brain areas could increase in size as aresult of use. He claimed that the skull followed the sizeof the brain areas so that an increased area in the brain(reflecting a highly learned skill) could be palpated at thesurface of the skull as a bulb. Gall termed his systemOrganologie. Later his system became known as phrenol-ogy, a term never used by Gall himself. Phrenology,fiercely defended by Johann Gaspar Spurzheim (see[29]) derailed in a series of wrong assumptions and com-mercial interests.
Gall’s view on the brain was unorthodox since the prevail-ing view of brain function at the end of the eighteenth centuryin Vienna was that of Albrecht von Haller (1708–1777, see[29]) who argued that the brain functioned as a whole and didnot have areas where distinct faculties were localized. Gallwas right about the supposed flexibility of the brain, but helooked at the wrong side. He looked at the skull and there wasnothing to see, the skull does not expose what happens on theinside. After his death in 1828, Gall was slowly forgotten. Hewas buried in history, beside the remains of phrenology.
The landmark experiments of Michael Merzenich
More than 200 years later in the 1980s, Merzenich and co-workers showed that neural representations (maps) of the
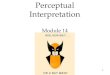
Fig. 8 Improvement of visualacuity (preferential looking upperleft, and VEP upper right), andvisual field size (bottom; isoptersshown for years) during earlyyears of life. Results ofpreferential looking and visualevoked potentials from [47]
442 Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447

limbs are flexible and continuously updated by our move-ments. Repetition of movement leads to the strengthen-ing of these representations (enlargement), whereas in-activity or non-use results in the shrinkage of theserepresentations. In a way we hear the echo of Gall. Ina landmark experiment Merzenich et al. [30] indicatedthat if a body part becomes less active, such as afterdeafferentation, its topographical representation in thesomatosensory cortex shrinks. He clearly showed thatthe adult human brain is not a rigid system, but a sys-tem that continuously undergoes plastic changes afteralterations in the sensory flow from peripheral receptorsand nerve fibers. The maps changed under the influenceof input. When input was withdrawn, the maps more orless shriveled up, whereas when input was increased,the maps extended in space. Furthermore, they showedthat previously existing synapses could be dramaticallymodified and that new synapses could be formed. Manyother studies showed that central sensory representationscould be reorganized, not only as a result of changes inthe peripheral input in an experimental context, but alsoafter amputation, spinal cord injury, deafferentation, af-ter ischaemic nerve block .
In particular, the speed of these reorganization process-es was impressive, which indicated that reorganizationwithin the motor system is not an occasional state of thebrain, but rather the normal ongoing condition of the hu-man brain throughout the life span. The human motorsystem is reorganizing itself more or less permanentlyon the basis of input. In that way the motor system maydiffer from other systems such as the visual system. Thiscapacity to reorganize plays a crucial role not only inlearning but also in recovery of motor function after dam-age to the brain.
Motor imagery
The availability of multimodal response-related input forms acrucial factor not only for the intactness of motor representa-tions in the brain, but also for the intactness of body awarenessand for learning and recovery. Against this background, learn-ing can be seen as input-dependent plasticity that is reflectedin changes in the brain.
However, since recent studies show that brain activity dur-ing the actual performance of a movement is comparable tobrain activity in a task where the movement is imagined orobserved instead of performed, the question becomes relevantwhether for motor learning it is always necessary to actuallyexecute the movement. In other words would it be possible tolearn movements not by executing them but by imagining themovements or by observing the movements as performed byothers? Does the imagination (and/or observation) of a
movement result in a flow of information that is similar tothe flow that is generated by the actual execution of amovement?
On the basis of research performed during the last decade,the answer on the questions is affirmative. There is ampleevidence that both motor imagery and action observation in-deed, play a role in (re)learning motor skills since they share acommon neurophysiological basis with action execution[31–34].
It is argued that mirror neurons form a crucial factor in theexplanation of the role observation and imagination play inmotor learning. Mirror neurons, first identified in monkeypremotor area F5, discharge when an animal performs amovement, but also when the animal observes another indi-vidual performing the same or a related movement [35, 36],for a critical discussion on mirror neurons see [37].
Motor imagery seems to rely on a network involving motorrelated regions including frontoparietal areas and subcorticalstructures, which supports the view that motor imagery andmotor execution are very similar processes [38]. Motor imag-ery and action observation have been used in neurologicalrehabilitation [39], in sports [33], and in musical training [40].
Motor imagery can be described as the activation of a mo-tor representation or motor program, while Bblocking^ theoutput mode. This activation elicits an estimation of the sen-sory consequences that would have taken place when the ac-tion was actually performed. A clear relation exists betweenmotor imagery and memory. Movements stored in memorysystems of the brain form the input for the sensory estimation.From clinical studies it is, indeed, known that patients withsevere memory disorders show also difficulties in their abilityto imagine.
Action observation in human neonates
Human beings are excellent imitators. No other animal is moreable to do so thanman. Human imitation starts at a very youngage. In a series of very intriguing experiments Meltzoff &Moore [41] showed that infants between 12 and 21 days ofage are able to imitate both facial and manual gestures and thatthis behavior cannot be explained in terms of conditioning.The results implied that human neonates can equate theirown unseen behaviors with gestures they see others perform.A similar study with a group of 40 infants with a mean age of72 h (youngest 42 min) showed the same results, making itunlikely that intermodal mapping these infants displayed waslearned [42].
Conclusion
In this short paper it was attempted to show that the humanmotor system is a flexible non-hierarchical system, that almost
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447 443

literary Bruns on information^. It was argued that the abovecited statement of Cahal at the beginning of the twentiethcentury was too pessimistic, at least for the motor system.The motor system adapts and changes itself as a result ofactivity-driven input but also as a result of input that is gener-ated Boff-line^ as is the case in motor imagery. Action obser-vation forms a relevant additional source of sensory input.
Part 4: learning to see beyond visual resolutionby Manfred Fahle
Learning, according to Merriam-Webster [43], is the activityor process of gaining knowledge or skill by studying, practic-ing, being taught or experiencing something. In our case, thepracticing of certain visual tasks can improve the skill of de-tecting and discriminating certain visual features.
There exist quite a number of different types of learning.There is first short-term learning that leads to short-termmem-ory. Short-term learning enables us, for example, to memorizephone numbers that we hear until we are able to write themdown. Another type of short-term learning involves visualimpressions that we can store in short-term memory, for ex-ample when copying complex patterns.
In ophthalmology, we are more interested in the secondtype of learning, namely long-term learning and long-termmemory. In long-term learning and memory, again, there existtwo quite different types of learning. The first one deals withfacts and events that can be described with words. This part oflearning and memory is called explicit or declarative. Thebrain structure involved is mainly the medial temporal lobe;there we store facts and events from the past and learn aboutnew facts and new events. The second type of long-term learn-ing and memory cannot be communicated with words. It iscalled implicit or non-declarative learning and memory. Foursubtypes of long-term learning and memory are generally dis-criminated. The first one is non-associative learning, namelyhabituation and sensitization. This is not really a long-termtype of memory and learning because habituation and sensiti-zation usually last only a few days or weeks. Habituationmeans that we react less strongly to a stimulus that has beenpresented several times in a row. On the contrary, sensitizationmeans that we are reacting more strongly to a stimulus thatwas presented several times. Sensitization, of course, happensfar less often than habituation. The second type of mediumlong-term learning and memory is called priming. It relies onthe neocortex and means that a stimulus that we experiencedmay influence our behavior and reactions in ways that aremostly subconscious. Third, there is associative learning,namely classical and operant conditioning, as in the case ofPavlov’s dog. This type of learning and memory relies mainlyon the amygdala and the cerebellum. Finally, there are proce-dural forms of long-term learning and memory, and personally
I would count perceptual learning as one form of procedurallearning, which relies on the striatum and the neocortex.
When defining perceptual learning, we can follow Gibson[44] who stated, Bany relatively permanent and consistentchange in the perception of a stimulus following practice orexperience with this array will be considered perceptuallearning.^ The important points of this definition are, first,the part that perceptual learning means a relatively permanentand consistent change unlike, for example, dark adaptation.The second important point is that this improvement is theresult of an active process. In the case of perceptual visuallearning this improvement usually relies on training the per-ception and categorization of visual stimuli and often indeedvery extensive training. Work by myself and others indicatesthat perceptual learning is not just a better use of sensory dataon relatively Bhigh^ and complex levels of cortical processing,but that even early sensory and especially visual cortical areascan change their behavior as a result of training [45].
Fortunately, the processes on the cellular or neuronal levelthat underlie learning have been clarified by means of electro-physiological and biochemical investigations by Kandel andothers [46]. Today, we can be sure that plasticity in the ner-vous system relies on changes at the level of synapses.Synapses can learn, for example, to set transmitter free faster,to produce more transmitter or to set free additional secondmessengers. Moreover, neurons may produce additional syn-apses to influence other neurons better. While we do not haveto consider these changes here in detail, it is certainlyreassuring that the underlying mechanisms of perceptuallearning on the cellular level have been clarified.
Perceptual learning is a very important process during earlylife. Newborns have a visual acuity clearly below 1/20 (0.05).The fast improvement of visual acuity over the first monthsand years of life is not only due to maturation processes, butmainly due to active learning through something I would callearly perceptual learning. Both studies using visually evokedpotentials (VEP) and behavioral measures, such as preferen-tial looking, show fast improvement of visual acuity, and anincrease of the visual field size[47] (see Fig. 8). Perceptuallearning is not only happening during childhood, but also inadults. While most of my patients see me to get readingglasses around the age of 45 years, there are a few non-myopic ones who come up to me 10 years later. These patientsinsist that they are able to read or at least were able to readuntil recently. I tend to believe them. Perceptual learning canenable you to guess the correct letters even from rather blurredimages. And there are companies that sell apps, for examplefor smart phones, that enable people in this age range to readwithout reading spectacles by learning to decipher even ratherblurred letters and words.
We decided to investigate perceptual learning mainly bymeans of a phenomenon called visual hyperacuity. This termdenotes the fact that we as humans are able to detect features
444 Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447

that are clearly below the diameter of the photoreceptor spac-ing even in the foveola, for example in stereovision and whenreading a Vernier scale. The features that can be resolved arein the order of magnitude of 10 arcseconds, even forunexperienced observers, and down to 2 or 3 arcseconds forvery experienced observers. These low thresholds, for exam-ple when deciding whether the lower element of a Verniertarget is offset to the left or to the right relative to the upperone, is really amazing when we consider that photoreceptorshave a diameter of around 25 arcseconds.
When Wülfing in the nineteenth century first describedthese low thresholds, people concluded that the anatomistshad gotten it wrong when they calculated the size of photore-ceptors. At this time, the size of photoreceptors had been mea-sured and determined to be around 25 arcseconds when con-verted into an angular measure. So people reasoned that pho-toreceptors had to be much smaller than previously thought,due to the low thresholds measured by Wülfing [48]. But theanatomists had gotten it right: photoreceptors are indeedmuchwider and larger than hyperacuity thresholds. Hering [49, 50]tried to resolve this paradox by postulating that the low thresh-olds are because Vernier stimuli extend over hundreds andthousands of photoreceptors and that the brain is able to aver-age over these many photoreceptors. Unfortunately, this ex-planation was wrong as was shown by Ludvigh [51]. Whenthree dots are presented (almost aligned), then under optimalconditions, a lateral displacement of the middle dot can bedetected for deviations that are again below 10 arcseconds,i.e. clearly below the photoreceptor diameter.
Only at the end of the twentieth century, the puzzle ofhyperacuity has been resolved. The underlying cause for thisamazing spatial acuity lies in the fact that our optics is not atall optimal. The retinal image even of the smallest star that is alight source almost as small as a mathematical point extendson the retina over several photoreceptors. So while one pho-toreceptor will usually be most strongly activated, its neigh-bors are somewhat less strongly activated. Then, the brain isable to calculate the position of this star with a precision farbelow the photoreceptor diameter by comparing the relativeexcitations of these neighboring photoreceptors. As a conse-quence, the spatial resolution to pinpoint the exact position ofvisual features relative to each other is mainly limited bysignal-to-noise ratios, rather than by photoreceptor diameteror photoreceptor distance, as long as the conditions ofShannon’s sampling theorem are fulfilled [52]. This theorempostulates that any signal can be completely reconstructed, aslong as there are slightly more than two sampling points forthe highest frequency that is part of this signal, in this case theimage. And indeed, the density of foveal photoreceptors issufficient to sample at least twice the highest frequency thatcan be produced by the optics of the eye, that is, more than 30receptors per degree of visual angle. Hence, physics can showthat there is no magic in these low perceptual thresholds in
hyperacuity that enable us, for example, to detect a displace-ment between two lines at a distance of 100 km, once theoffset is above 1.5 m!
Over the last decade we have performed quite a num-ber of experiments on perceptual learning by using differ-ent hyperacuity tasks. Here, I will give the example ofVernier learning. As indicated above, we interpret ourdata as indicating that indeed to achieve the very highestperformance, i.e. the very lowest thresholds, learning can-not be exclusively on relatively high levels of corticalprocessing but has to involve already on the early sensorycortical areas. Let me try to convince you that this hy-pothesis is correct. In the first experiment we presentedVernier stimuli to 12 observers. In six observers theseVernier stimuli were oriented horizontally, for the othersix observers they were oriented vertically. Observerstrained with these stimuli for 1 h and improved detectionon average from around 50% to 70%. When we rotatedthe stimuli (the group that had trained with vertical stimulinow had to practice with horizontal stimuli and viceversa), the detection level dropped drastically, even slight-ly below 50%, and observers had to learn the new task,that only deviated from the previous task by stimulusorientation, completely from scratch, attaining 70% detec-tion only after about one additional hour of training. In acontrol group where we did not change stimulus orienta-tion no such drop of performance occurred.
We then repeated the experiment in a lengthier version,training observers for 5 h on five consecutive days. Thethresholds improved from around 13 arcseconds to aboutslightly below 10 arcseconds during that time. Then, again,we changed orientation by 90 degrees so that observers whohad trained with vertical Verniers now had to respond to hor-izontal Verniers. Thresholds increased strongly, to above 15arcseconds, that is, evenworse than in the untrained observers.This is to say that surprisingly, extensive training with onestimulus orientation improved performance for this orienta-tion, but decreased performance for the stimuli rotated by 90degrees. Again, performance improved over five additionalhours of additional training to achieve the level attained forthe first orientation only after these 5 h of training. This is tosay that perceptual learning in the hyperacuity range is highlyspecific for stimulus orientation.
In a second experiment, we trained observers with one eyepatched. Six observers started with the left eye patched whilesix further observers started with the right eye patched. Theimprovement was similar as in the experiment with stimulusrotation. After 1 h of training, the drop of performance afterchanging patch side was less pronounced than for the rotationof stimulus orientation, but for the companion experimentwith long-term learning of 5 h per observer, we again founda strong decrease of performance when observers switchedfrom seeing with one eye to the partner eye (even slightly)
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447 445

below the level of untrained observers. Please note that for allof these experiments, new observers were recruited for eachnew experiment.
These results and additional results we obtained, for exam-ple, by using visual evoked potentials that showed significantchange as a result of perceptual learning already over theoccipital pole [53], lead us to the conclusion already men-tioned above, that perceptual learning can change processingalready on a very early level of cortical computation before thethe inputs from the two eyes are combined. If perceptual learn-ing improved performance through better evaluation of sen-sory signals on higher levels of cortical processing, one wouldhave to expect that improvements generalize from one eye tothe other. One has to keep in mind that, due to tremor andsmall eye movements, stimuli will fall on different parts of theretina over the course of the experiment. Different parts of thesame retina will differ from each other as much or maybe evenmore than corresponding parts of both eyes. Hence, an im-provement that is specific for one eye strongly suggests thatthis improvement is mediated on very early levels of visualinformation processing that are still monocularly activated.This is to say that the old view of a hard-wired early visualcortex, as proposed for example by Marr and colleagues [54],does no longer hold true. Quite to the contrary, the early sen-sory cortical areas seem to keep some plasticity even in adults.
This has consequences not only for the therapy of ambly-opia, but also for stroke patients. As long as signals reach thevisual cortex, learning and compensatory mechanisms areable to improve perception and discrimination of objects.The essential condition to keep in mind is that signals fromthe retina have to arrive at the brain. Phenomena such as blind-sight seem to indicate that these signals do not necessarilyhave to arrive in the primary visual cortex, but other parts ofthe cortex may also be able to subserve some type of rudimen-tary vision. If, on the other hand, fibers are destroyed, as is thecase in glaucoma or strokes on the level of the thalamus, thenthe resulting visual field defects cannot be made to disappearby means of perceptual learning. Training can improve theway that the visual cortex analyzes and categorizes visualstimuli, but can never compensate absolute visual field defectscaused by lesions on very early levels of the visual system.
To conclude, we find that there are a number of differentforms of learning and have reminded ourselves that learningdramatically improves seeing in infants and can improve vi-sual perception at least slightly in patients and in presbyopes.We also find that in several so-called hyperacuity tasks, suchas Vernier acuity and stereopsis, observers achieve spatial res-olution far below the photoreceptor diameter and photorecep-tor spacing even in the foveola and can thus, at least afterextensive training, attain thresholds that are far below photo-receptor diameters. But improvement in perceptual learningseems under most conditions to be very specific for the exacttask trained and therefore indicative of changes that involve
even the level of early sensory cortical areas. Extensive re-search is presently under way to find training procedures lead-ing to perceptual learning that generalizes to new tasks.
Acknowledgements Jonathan Horton: Funding Support: This workwas supported by grants EY10217 (J.C.H.), EY02162 (Beckman VisionCenter) from the National Eye Institute and a Physician-Scientist Awardfrom Research to Prevent Blindness. The sponsor or funding organizationhad no role in the design or conduct of this research. There are no conflictsof interest pertaining to this study.
Susanne Trauzettel-Klosinski: Funding support: Kerstan Foundation,Adolf Messer Foundation, Herbert Funke Foundation. The funding orga-nizations had no role in the design or conduct of this research.
Compliance with ethical standards
Conflict of interest All authors certify that they have no affiliationswith or involvement in any organization or entity with any financialinterest (such as honoraria; educational grants; participation in speakers’bureaus; membership, employment, consultancies, stock ownership, orother equity interest; and expert testimony or patent-licensing arrange-ments), or non-financial interest (such as personal or professional rela-tionships, affiliations, knowledge or beliefs) in the subject matter or ma-terials discussed in this manuscript.
Ethical statement For this type of study formal consent is not required.
Open Access This article is distributed under the terms of the CreativeCommons At t r ibut ion 4 .0 In te rna t ional License (h t tp : / /creativecommons.org/licenses/by/4.0/), which permits unrestricted use,distribution, and reproduction in any medium, provided you give appro-priate credit to the original author(s) and the source, provide a link to theCreative Commons license, and indicate if changes were made.
References
1. Sincich LC, Adams DL, Economides JR, Horton JC (2007)Transmission of spike trains at the retinogeniculate synapse. JNeurosci 27:2683–2692. doi:10.1523/JNEUROSCI.5077-06.2007
2. Gilbert CD, Wiesel TN (1992) Receptive field dynamics in adultprimary visual cortex. Nature 356:150–152
3. ChinoYM,Kaas JH, Smith EL III et al (1992) Rapid reorganizationof cortical maps in adult cats following restricted deafferentation inretina. Vision Res 32:789–796
4. Horton JC, Hocking DR (1998) Monocular core zones and binoc-ular border strips in primate striate cortex revealed by the contrast-ing effects of enucleation, eyelid suture, and retinal laser lesions oncytochrome oxidase activity. J Neurosci 18(14):5433–5455
5. Smirnakis SM, Brewer AA, Schmid MC et al (2005) Lack of long-term cortical reorganization after macaque retinal lesions. Nature435(7040):300–307
6. Kasten E, Wust S, Behrens-Baumann W, Sabel BA (1998)Computer-based training for the treatment of partial blindness.Nat Med 4(9):1083–1087
7. Meienberg O, Zangemeister WH, Rosenberg M et al (1981)Saccadic eye movement strategies in patients with homonymoushemianopia. Ann Neurol 9(6):537–544
8. Reinhard J, Schreiber A, Schiefer U et al (2005) Does visual resti-tution training change absolute homonymous visual field defects? afundus controlled study. Br J Ophthalmol 89(1):30–35. doi:10.1136/bjo.2003.040543
446 Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447

9. Leopold DA (2012) Primary visual cortex: awareness andblindsight. Annu Rev Neurosci 35:91–109
10. Sincich LC, Park KF, Wohlgemuth MJ, Horton JC (2004)Bypassing V1: a direct geniculate input to area MT. Nat Neurosci7(10):1123–1128. doi:10.1038/nn1318
11. SchmidMC,Mrowka SW, Turchi J et al (2010) Blindsight dependson the lateral geniculate nucleus. Nature 466(7304):373–377
12. Reinhard J, Damm I, Ivanov IV, Trauzettel-Klosinski S (2014) Eyemovements during saccadic and fixation tasks in patients withhemianopia. J Neuroophthalmol 34(4):354–361
13. Trauzettel-Klosinski S, Reinhard J (1998) The vertical field borderin human hemianopia and its significance for fixation behavior andreading. Invest Ophthalmol Vis Sci 39:2177–2186
14. Mannan SK, Pambakian ALM, Kennard C (2010) Compensatorystrategies following visual search training in patients with homon-ymous hemianopia: an eye movement study. J Neurol 257(11):1812–1821
15. Trauzettel-Klosinski S (2010) Rehabilitation for visual disorders. JNeuro-Ophthalmol 30(1):73–84. doi:10.1097/WNO.0b013e3181ce7e8f
16. Trauzettel-Klosinski S (2011) Current methods of visual rehabilita-tion. Dtsch Arztebl Int 108(51–52):871–878. doi:10.3238/arztebl.2011.0871
17. Van Waveren M, Jägle H, Besch D (2013) Management of strabis-mus with hemianopic visual field defects. Graefe’s Arch Clin Exp251:575–584. doi:10.1007/s00417-012-2045-1
18. Horton JC (2005) Disappointing results from Nova vision’s visualrestoration therapy. Br J Ophthalmol 89(1):1–2. doi:10.1136/bjo.2004.058214
19. Pollock A, HazeltonC, Henderson CA et al (2011) Interventions forvisual field defects in patients with stroke. Cochrane Database SystRev 5(10):CD008388. doi:10.1002/14651858.CD008388.pub2
20. Melnick MD, Tadin D, Huxlin KR (2016) Re-learning to see incortical blindness. Neuroscientist 22(2):199–212
21. Roth T, Sokolov AN, Messias A et al (2009) Comparing explor-ative saccade and flicker training in hemianopia: a randomized con-trolled study. Neurology 72(4):324–331
22. Aimola L, Lane AR, Smith DT, Kerkhoff G, Ford GA, Schenk T(2014) Efficacy and feasibility of home- based training for individ-uals with homonymous visual field defects. Neurorehab Neural Re28(3):207–218. doi:10.1177/1545968313503219
23. de Haan GA, Melis-Dankers BJM, Brouwer WH, Tucha O,Heutink J (2015) The effects of compensatory scanning trainingon mobility in patients with homonymous visual field defects: arandomized controlled trial. PLoS ONE 10(8):e0134459.doi:10.1371/journal.pone.0134459
24. Tinga AM, Visser-Meily JMA, van der Smagt MJ, van der StigchelSTCW, van Ee R, Nijboer TCW (2016)Multisensory stimulation toimprove low- and higher-level sensory deficits after stroke: a sys-tematic review. Neuropsychol Rev 26:73–91. doi:10.1007/s11065015-9301-1
25. Lévy-Bencheton D, Pélisson D, Prost M, Jacquin-Courtois S,Salemme R, Pisella L, Tilikete C (2016) The effects of short-lasting anti-saccade training in homonymous hemianopia withand without saccadic adaptation. Front Behav Neurosci 9:332.doi:10.3389/fnbeh.2015.00332, eCollection 2015
26. Spitzyna GA, Wise RJS, McDonald SA et al (2007) Optokinetictherapy improves text reading in patients with hemianopic alexia: acontrolled trial. Neurology 68(22):1922–1930
27. Mulder T, Hochstenbach J (2003) Motor control and learning: im-plications for neurological rehabilitation. In: GreenwoodRJ, BarnesMP, McMillan TM, Ward CD (eds) Handbook of neurological re-habilitation. Psychology Press, New York, pp 143–152
28. Cajal SRY (1928) Degeneration and regeneration of the nervoussystem. volume 2. Haffner Publishing Co, New York, p 750
29. Van Wyhe J (2002) The authority of human nature: theSchädellehre of Franz Joseph Gall. Br J Hist Sci 35(124 Pt 1):17–42. doi:10.1017/S0007087401004599
30. Merzenich MM, Kaas JH, Wall J, Nelson RJ, Sur M, Felleman D(1983) Topographic reorganization of somatosensory cortical areas3b and 1 in adult monkeys following restricted deafferentation.Neuroscience 8(1):33–55
31. Mulder T, Zijlstra S, Zijlstra W, Hochstenbach J (2004) The role ofmotor imagery in learning a totally novel movement. Exp Brain Res154(2):211–217. doi:10.1007/s00221-003-1647-6
32. Mulder T (2007) Motor imagery and action observation: cognitivetools for rehabilitation. J Neural Transm 114(10):1265–1279.doi:10.1007/s00702-007-0763-z
33. Vogt S, Thomaschke R (2007) From visuo-motor interactions toimitation learning: behavioral and brain imaging studies. J SportsSci 25(5):497–517. doi:10.1080/02640410600946779
34. Gatti R, Tettamanti A, Gough PM, Riboldi E, Marinoni L, BuccinoG (2013) Action observation versus motor imagery in learning acomplex motor task: a short review of literature and a kinematicstudy. Neuroscience 540:37–42. doi:10.1016/j.neulet.2012.11.039
35. Galese V, Fadiga L, Fogassi L, Rizzolatti G (1996) Action recog-nition in the premotor cortex. Brain 119(Pt 2):593–609
36. Rizzolatti G, Fadiga L, Fogassi L, Galese V (1996) Premotor cortexand the recognition of motor actions. Brain Res 3:131–141
37. Hickock G (2014) The myth of mirror neurons: the real neurosci-ence of communication and cognition. Norton Publ, New York
38. Hétua S, Grégoire M, Saimpont A, Coll MP, Eugènec F, MichonPE, Jacksonb PL (2013) The neural network of motor imagery: anALE meta-analysis. Neurosci Biobehav R 37(5):930–949.doi:10.1016/j.neubiorev.2013.03.017
39. Malouin F, Jackson PL, Richards CL (2013) Towards the integra-tion of mental practice in rehabilitation programs: s critical review.Front Hum Neurosci. doi:10.3389/fnhum.2013.00576
40. Keller PE (2012) Mental imagery in music performance: underly-ing mechanisms and potential benefits. Ann NY Acad Sciannals1252:206–213. doi:10.1111/j.1749-632.2011.06439.x
41. Meltzoff AN, Moore MK (1977) Imitation of facial and manualgestures by human neonates. Science 198:75–78
42. Meltzoff AN, Borton RW (1979) Intermodal matching by humanneonates. Nature 282:403–404
43. BLearning.^ /Merriam-Webster.com/.Dictionary (2016)http://www.merriam-webster.com. Accessed 15 July 2016
44. Gibson EJ (1963) Perceptual learning. AnnuRev Psychol 14:29–5645. Fahle M, Poggio T (eds) (2002) Perceptual learning. MIT-Press,
Cambridge46. Kandel ER, Schwartz JH, Jessell TM, Siegelbaum SA, Hudspeth
AJ (2013) Principles of neural sciences. McGraw-Hill, New York47. Mohn G, van Hof - van Duin J (1991) Development of Spatial
Vision. In: Regan D (ed) Spatial Vision. Vision and VisualDysfunction, Vol. 10, Macmillan Press, London, pp 179-211
48. Wülfing EA (1892) Über den kleinsten Gesichtswinkel. Z Biol-Munich 29:199–202
49. Hering E (1861) Zur Lehre vomOrtsinne der Netzhaut. In: Beiträgezur Physiologie. Engelmann, Leipzig
50. Hering E (1899) Über die Grenze der Sehschärfe. Ber. math.-phys.Cl. D. königl. Sächs. Gesell. Wiss. Leipzig; Naturwiss. Teil, 16–24
51. Ludvigh E (1953) Direction sense of the eye. Am J Ophthmalmol36:139–142
52. Shannon GE (1949) Communication in the presence of noise. Proc.IRE, 37(1)
53. Fahle M, Skrandies M (1994) An electrophysiological correlate oflearning in motion perception. Ger J Ophthalmol 3:427–432
54 Marr D (1982) Vision. MIT-Press, Cambridge
Graefes Arch Clin Exp Ophthalmol (2017) 255:435–447 447