Embed Size (px)
Citation preview

DOI: 10.2298/CSIS120405055G
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
Rupesh Ghyar1, Karupppasamy Subburaj
2, B. Ravi
1, and Manish Agarwal
3
1 OrthoCAD Network Research Centre Indian Institute of Technology Bombay, Powai, Mumbai, 400076, India
{r.ghyar, b.ravi}@iitb.ac.in 2 Department of Radiology and Biomedical Imaging
University of California San Francisco, San Francisco, CA 94158, USA [email protected]
3 Department of Surgical Oncology Hinduja Hospital and Medical Research Centre, Mahim, Mumbai, 400016, India
Abstract. Tumour knee prostheses reconstruct bone gaps, left after resecting the tumour affected tissues, in limb salvage surgeries of bone cancer patients. They typically comprise of 6-12 different components chosen from a family of components that are manufactured in discrete variations (intended to cater to a wide range of patient conditions including gender, tumour position, leg (left/right), and resection length). These variations generate numerous combinations and selecting a correct set of components from a family of 100 or more total components has made the process difficult for a given patient. This article describes an adaptive probabilistic approach developed for selection of tumour knee prosthesis components, driven by geometric details. These details were extracted from the 3D virtual anatomical model, reconstructed from set of CT scan images of patients. The selection was performed in two steps. First, the grossly undersized and oversized components were eliminated. Then the geometric details of components were mapped, with the measured anatomical parameters of the patient, to form a fuzzy-logic based decision tree. This was based on pre-defined rules compiled from surgeons' experience. A set of measures (geometric difference, bone curvature, knee centre shift, and reconstruction length) were used to evaluate the selected prosthesis components. Evaluation was based on their suitability with respect to the patient's anatomy, and classified with a qualitative tag: ‘most suitable’, ‘probably suitable’, or ‘not suitable’. A case study of distal femur replacement is presented to explain the proposed methodology. This approach eliminates the risk of over and under sizing of the prosthesis components and reduces the average inventory to be maintained for each patient.
Keywords: tumour knee prosthesis, prosthesis selection, 3D anatomical models, preoperative planning.

Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1408 ComSIS Vol. 10, No. 3, June 2013
1. Introduction
Modular endoprostheses, introduced in 1980s with the intent of replacing custom-made implants, had limitations such as lack of intra-operative flexibility, high lead time and cost [1]. The advent of superior diagnostic medical imaging, improved surgical techniques, effective adjuvant therapy, advanced biomaterials, and manufacturing processes has made endoprosthetic reconstruction a preferred method of treatment [2]. These treatments are widely used for skeletally immature individuals who undergo resection of a juxta-articular tumour. However, postoperative complications such as infection, mechanical failure, bone fracture, and aseptic loosening, have lead to a high rate of failure [3]. At present, surgeons select prosthesis components based on (i) reasonable track record of their use (5-10 years), (ii) prior experience of the surgeon with the prosthesis, and (iii) suitability to the patient’s anatomy [4]. The last criterion is the most critical one in selecting prosthesis components. A typical modular prosthesis set comprises of 100 to 200 components, manufactured in an assortment of sizes, which has made it difficult to select the most appropriate combination of components in intra-operative stage. Occasionally, surgeons have been forced to make assumptions about selection which eventually turned out to be unsuitable [5]. The implantation of an over-sized or an under-sized component has increased the risk of postoperative complications in multi-fold. Clinical studies have shown that such variances resulted in soft-tissue irritation [6], inequality in leg length, back pain [7], abnormal gait [8], and sciatic nerve palsy [3]. It has been a challenging problem to restore the position of the prosthetic joint line to the same level as the natural joint line ([9] and [10]). Any excessive deformation of bone also has to be considered while selecting prosthesis components to eliminate issues in orientation and alignment. Understanding the influence of rotational position of the leg and deformities on the radiological measurement of the distal femur and proximal tibia may improve component selection [11]. The best prosthesis components would offer a stable fixation of the prosthesis to host bone, restore the preoperative height of the joint line, to obtain a stable range of motion compatible with the patient’s activities of daily living, and to obtain the least degree of prosthetic constraint so that soft tissues may share in load transfer. As prosthetic constraint increases, the soft tissues participate in less load-sharing and stresses on the prosthesis-bone interface increase, with the attendant possibility of early loosening of the implant [12]. Selection of the best set of prosthesis components and their accurate placement has been important factors for increased durability and success rate ([13] and [14]). Strategic preoperative planning and prosthesis components selection may prevent use of under-sized and over-sized prosthesis components.

Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1409
2. Related Work
The use of templates, applied to radiographs before surgery, allows determining the most appropriate size of prosthesis to be used by the surgeon. Both Charnley
[15] and Muller
[16] had emphasised the importance of
preoperative radiographs in deciding the type and size of prosthesis, achieving the correct position and orientation of the components, equalising leg length and reducing intra-operative complications. For the pre-operative assessment of component size, templates are generally used on anterior-posterior (AP) and medio-lateral (ML) radiographs. As templates have a standard magnification of 15% or 20%, it is important that the pre-operative radiographs show the same magnification, principally on the AP radiographs. Furthermore, many patients have little external rotation deformity; it is helpful to know if the rotational position of the femur may influence the radiological measurement of the size and the position of the prosthesis. In standard radiograph, it is difficult to estimate. Criteria such as age, weight, expected activity, general health, and bone stock have been used in selecting the best hip prosthesis and reducing its cost [17].
Recently, CT axial images were used for manual selection of components and visually evaluated by superimposing them in total knee arthroplasty (TKA). Harris et al.
[18] have used CT axial slices and X-ray images for
selecting good match prosthesis component for TKA reconstruction. After an initial estimate of the prosthesis position the surgeon can fine tune it by moving the prosthesis parts on the CT images, and selecting appropriately sized components to find a good match with the bone geometry. Finally 3D prosthesis model was superimposed on X-ray image for visual verification. This is however fully interactive from selecting prosthesis components into aligning prosthesis for verification. Successful preoperative planning can prevent use of under- and over-sized prosthesis components and can identify extremes of size and bony deformity/morphology, which may require nonstandard (custom-made) implants or components. Curran
[8] emphasised
on the use of anatomical landmarks, in preoperative planning, that eventually allowed intra-operative verification of the planned leg lengthening. Nelson et al.
[12] reviewed and discussed about the type of implants and their longevity in
revision surgery after failure. Most of earlier work focussed on TKA and consisted of posterior cruciate retained versus excised, fixed-bearing versus mobile-bearing, high-flex versus standard implants and patella resurfacing versus non-resurfacing [19]. There is no reported work on methodologically selecting prosthesis components for tumour knee reconstruction. The set of variability of modular prosthesis components has made the selection process more complex.
In view of the above mentioned factors, there is a need for semi-automated system which narrows the choice of prosthesis components, based on qualitative tags like ‘most suitable’, ‘probably suitable’, and ‘not suitable’. This will help surgeons to choose the final components from a limited number of possibilities without need to select, order, obtain and check a complete prosthesis set. This article describes a semi-automatic computer program
Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1410 ComSIS Vol. 10, No. 3, June 2013
based on an adaptive probabilistic approach for selecting tumour endoprosthesis components driven by the anatomical data of the patient (reconstructed 3D model). Such a computer program coupled with patient-prosthesis geometric data to determine suitable tumour knee prosthesis components does not appear to have been attempted so far. In 80% of osteosarcoma (bone cancer) patients, the tumour is found in a long bone of the extremity, knee being the commonest [20]. Since distal femur experiences the highest incidence of bone tumour, the system was developed to illustrate with distal femur reconstruction example.
3. Methodology
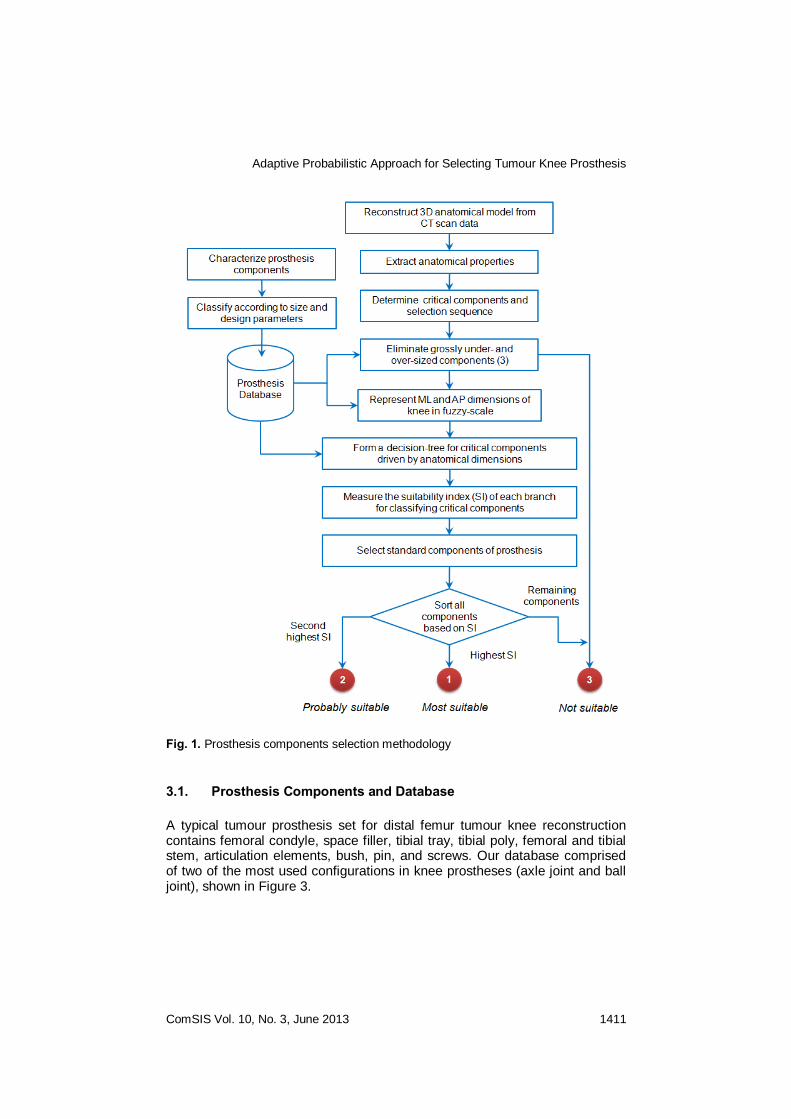
The approach starts with 3D anatomical model reconstruction from CT scan images of the knee joint. The steps followed in prosthesis components selection are illustrated in Figure 1.
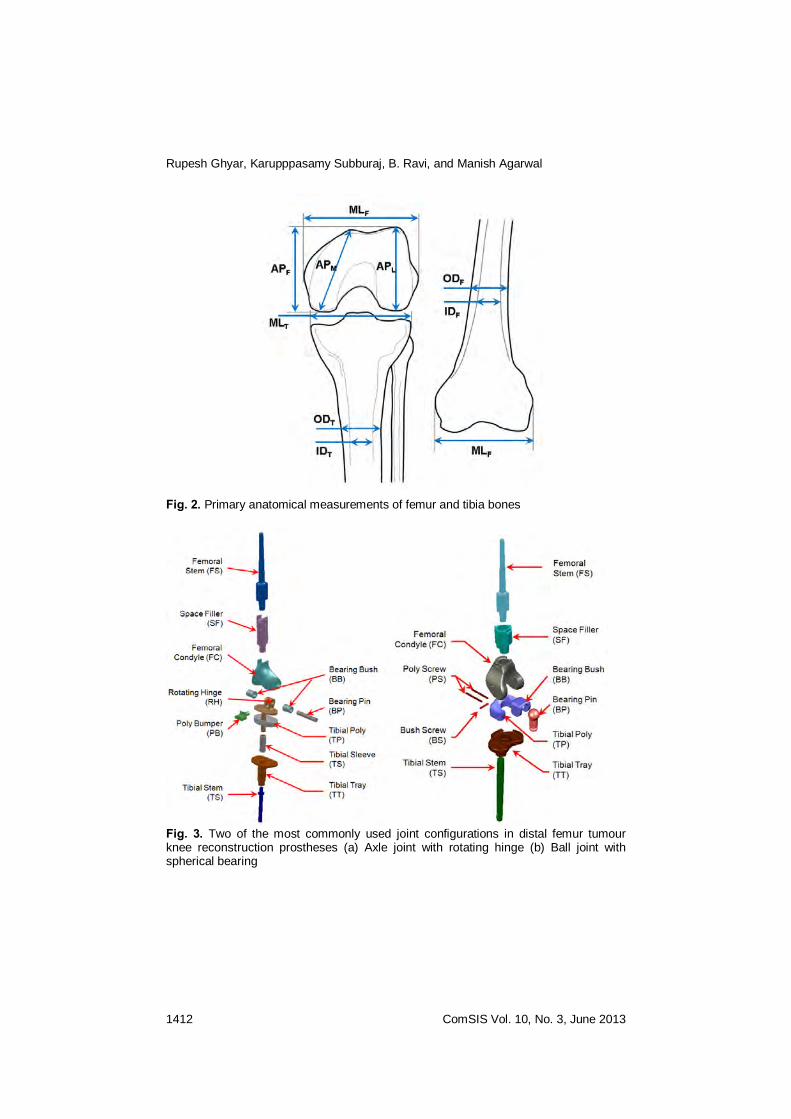
Primary anatomical measurements required for selecting the prosthesis components were semi-automatically extracted from the 3D anatomical model. These included epicondylar/plateau distance (ML), anterio-posterior distance (AP), inner diameter (ID), and outer diameter (OD) of the distal femur (MLF, APF, IDF, and ODF) and of the proximal tibia (MLT, APT, IDT, and ODT), as shown in Figure 2.
Valgus/varus angle of the leg (VA) and curvature of the femur and tibia (CVF and CVT) were also measured by referencing virtual anatomical landmarks. In prosthesis selection, AP dimension is an important factor in maintaining flexion-extension gap. Similarly, the ML dimension determines adequate coverage of the resected bone surface, which is required for even distribution of stress and tension-free wound closure. The properties of bone stock remaining after resection needs to be considered in selection. The bone resection length (RL) decision, usually taken by the operating surgeon, was finalised by a surgeon manually according to spread of the tumour. Since selection of a component is influenced by preceding and succeeding components in the selection process, a better approach would be to use hierarchical decision making tools that are driven by anatomical data of the patient. Functional or knee score has been used to evaluate the patients post-surgical outcome in terms of functional capability when compared to normal subject. But the cause of functional disability can be quantified in terms of geometry and alignment of prosthesis compared to the patient’s anatomy using some metrics. These need to be given true consideration during implantation. The detailed steps of this selection procedure are described in this section.
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1411
Fig. 1. Prosthesis components selection methodology
3.1. Prosthesis Components and Database
A typical tumour prosthesis set for distal femur tumour knee reconstruction contains femoral condyle, space filler, tibial tray, tibial poly, femoral and tibial stem, articulation elements, bush, pin, and screws. Our database comprised of two of the most used configurations in knee prostheses (axle joint and ball joint), shown in Figure 3.
Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1412 ComSIS Vol. 10, No. 3, June 2013
Fig. 2. Primary anatomical measurements of femur and tibia bones
Fig. 3. Two of the most commonly used joint configurations in distal femur tumour knee reconstruction prostheses (a) Axle joint with rotating hinge (b) Ball joint with spherical bearing
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1413
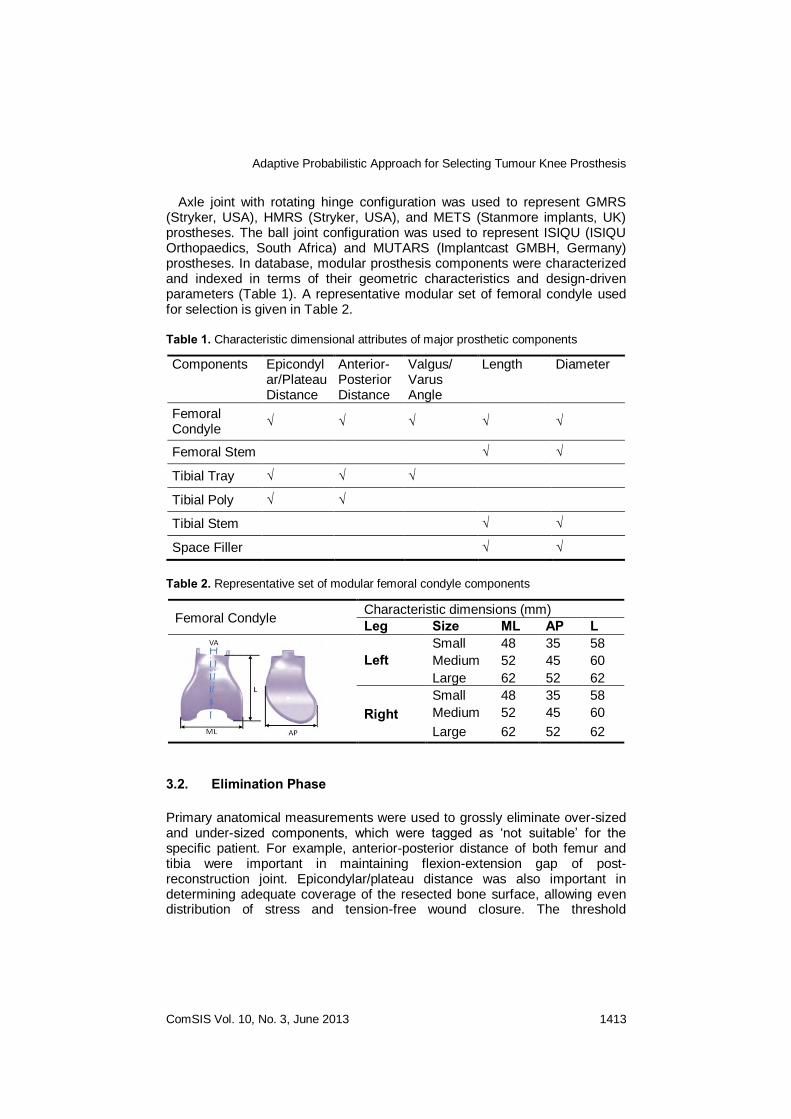
Axle joint with rotating hinge configuration was used to represent GMRS (Stryker, USA), HMRS (Stryker, USA), and METS (Stanmore implants, UK) prostheses. The ball joint configuration was used to represent ISIQU (ISIQU Orthopaedics, South Africa) and MUTARS (Implantcast GMBH, Germany) prostheses. In database, modular prosthesis components were characterized and indexed in terms of their geometric characteristics and design-driven parameters (Table 1). A representative modular set of femoral condyle used for selection is given in Table 2.
Table 1. Characteristic dimensional attributes of major prosthetic components
Components Epicondylar/Plateau Distance
Anterior-Posterior Distance
Valgus/ Varus Angle
Length Diameter
Femoral Condyle
√ √ √ √ √
Femoral Stem √ √
Tibial Tray √ √ √
Tibial Poly √ √
Tibial Stem √ √
Space Filler √ √
Table 2. Representative set of modular femoral condyle components
Femoral Condyle Characteristic dimensions (mm)
Leg Size ML AP L
Left Small 48 35 58
Medium 52 45 60
Large 62 52 62
Right Small 48 35 58
Medium 52 45 60
Large 62 52 62
3.2. Elimination Phase
Primary anatomical measurements were used to grossly eliminate over-sized and under-sized components, which were tagged as ‘not suitable’ for the specific patient. For example, anterior-posterior distance of both femur and tibia were important in maintaining flexion-extension gap of post-reconstruction joint. Epicondylar/plateau distance was also important in determining adequate coverage of the resected bone surface, allowing even distribution of stress and tension-free wound closure. The threshold

Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1414 ComSIS Vol. 10, No. 3, June 2013
dimensional values for Small (S), Medium (M), and Large (L) components were derived from morphometric studies on the knee of Indian population ([21] and [22]). Table 3 gives the optimized threshold values for these three sizes where, ML and AP represent measured length of distal femur (femoral condyle) and proximal tibia (tibial plateau) in medio-lateral and anterior-posterior directions, respectively.
Table 3. Optimized median values for dimensions in three ranges for Indian population
Size Femur Tibia
ML (mm) AP (mm) ML (mm) AP (mm)
Small 60.40 41.88 63.39 43.95
Medium 71.01 56.88 72.30 57.91
Large 77.09 66.68 80.90 63.37
The interrelationship between prosthesis components also affects the
sequence of the selection. Hence, critical components were selected first based on the measured anatomical measurements then the complimentary remaining components were chosen. The critical components of the distal femur tumour knee prosthesis were femoral condyle, tibial tray, tibial poly, and femoral and tibial stems. The remaining components (space filler, bearing bush, bearing pin, axle, and standard pins and screws) were selected based on both anatomical measurements and the previous selected critical components.
Selection of tibial tray was driven by anterior-posterior distance of the tibial plateau. The anterior-posterior dimension of tibial tray was ensuring not be larger than or smaller than the tibial plateau to eliminate the possibility of impingement during squatting and compromise the bearing strength required, respectively. Selection of femoral condyle component was influenced by the dimensions of the selected tibial tray. Femoral condyle component was selected based on epicondylar and anterior-posterior distance of the femur bone. The ratio of both these distances was used to reduce the femoral impingement. The size of the tibial poly component was chosen based on the constraints offered by the chosen femoral condylar and tibial tray components. The stems can be cemented or cementless and straight or curved. In straight stems, the length was decided by the amount of bone stock remaining after tumour excision while the diameter of the stem was chosen based on the diameter of the intramedullary canal of the femur bone. In curved stems, the curvature of bone stock after resection was also considered. If the measured radius was lower than an acceptable range allowed for straight stems, then a curved stem was chosen. The choice of cemented vs. cementless was decided based on the age of the patient. Due consideration of space for cement (typically 1-2 mm over diameter) was given before deciding the dimensions, if a cemented stem was preferred. More than 95% of stems were considered to be in the range of 8-14 mm. Space fillers or extension pieces were considered to be unnecessary when a minimum resection was performed (resection length ≤ length of femoral condylar
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1415
component). In such cases, femoral stems were directly inserted into the femoral condylar component. Selection of the femoral condylar component affected the diameter of space fillers, due to mating pair constraint. The mating part of the condylar component was cylindrical in shape, which was the default size (diameter) of the space filler component. The length of space filler was LSF = CL – LFC; where, LFC = length of femoral condylar component and CL = Reconstruction length (Resection length + tibial cut).
3.3. Selection Phase
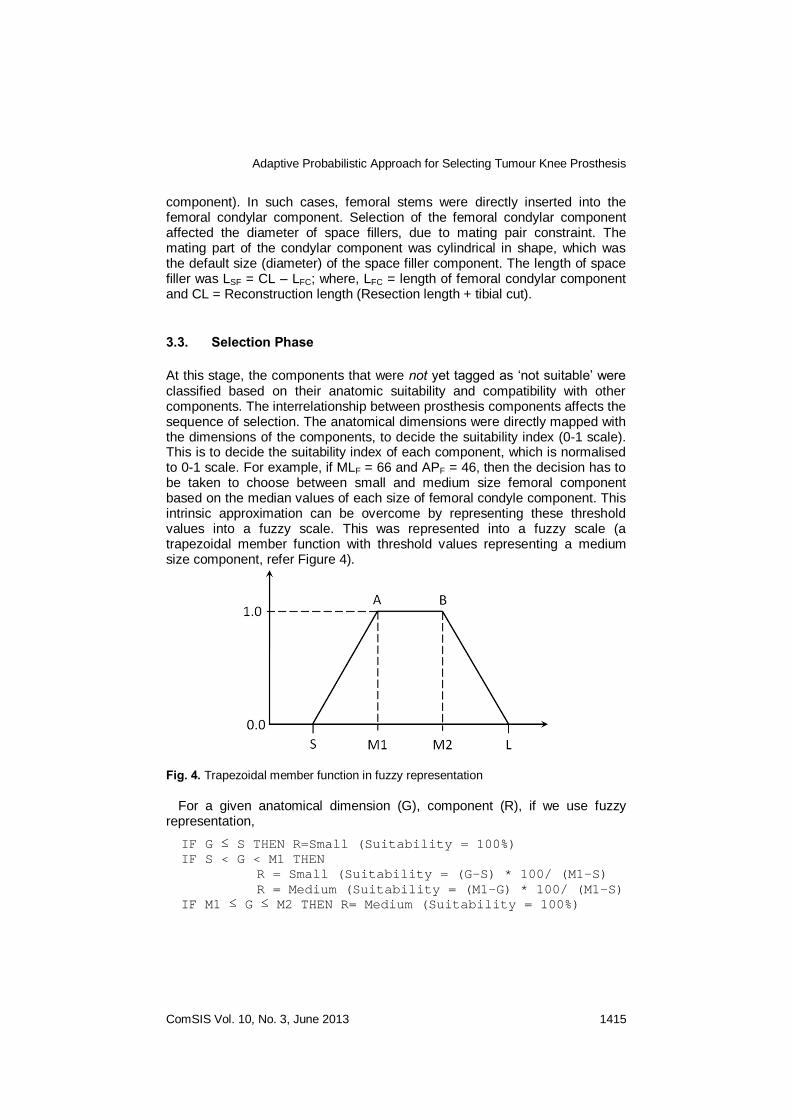
At this stage, the components that were not yet tagged as ‘not suitable’ were classified based on their anatomic suitability and compatibility with other components. The interrelationship between prosthesis components affects the sequence of selection. The anatomical dimensions were directly mapped with the dimensions of the components, to decide the suitability index (0-1 scale). This is to decide the suitability index of each component, which is normalised to 0-1 scale. For example, if MLF = 66 and APF = 46, then the decision has to be taken to choose between small and medium size femoral component based on the median values of each size of femoral condyle component. This intrinsic approximation can be overcome by representing these threshold values into a fuzzy scale. This was represented into a fuzzy scale (a trapezoidal member function with threshold values representing a medium size component, refer Figure 4).
Fig. 4. Trapezoidal member function in fuzzy representation
For a given anatomical dimension (G), component (R), if we use fuzzy representation,
IF G ≤ S THEN R=Small (Suitability = 100%)
IF S < G < M1 THEN
R = Small (Suitability = (G-S) * 100/ (M1-S)
R = Medium (Suitability = (M1-G) * 100/ (M1-S)
IF M1 ≤ G ≤ M2 THEN R= Medium (Suitability = 100%)
Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1416 ComSIS Vol. 10, No. 3, June 2013
IF M2 < G < L THEN
R = Medium (Suitability = (G-M2) * 100/ (L-M2)
R = Large (Suitability = (L-G) * 100/ (L-M2)
IF G ≥ L THEN R=Large (Suitability = 100%)
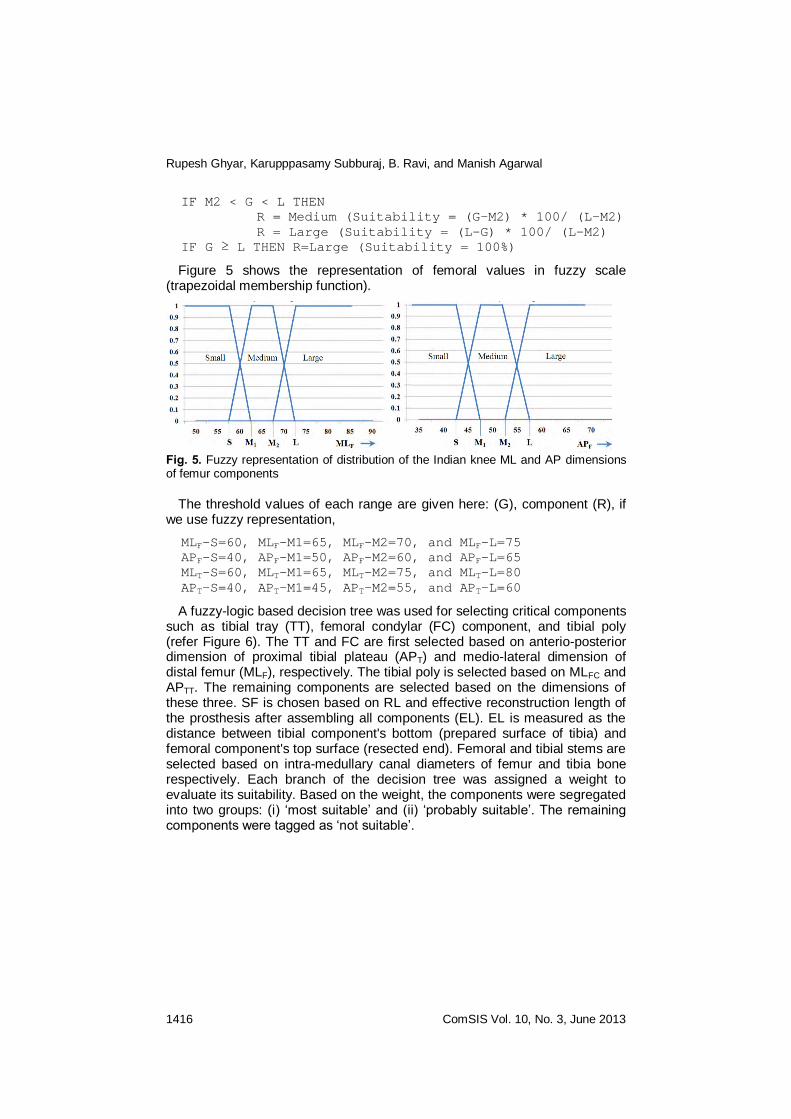
Figure 5 shows the representation of femoral values in fuzzy scale (trapezoidal membership function).
Fig. 5. Fuzzy representation of distribution of the Indian knee ML and AP dimensions of femur components
The threshold values of each range are given here: (G), component (R), if we use fuzzy representation,
MLF-S=60, MLF-M1=65, MLF-M2=70, and MLF-L=75
APF-S=40, APF-M1=50, APF-M2=60, and APF-L=65
MLT-S=60, MLT-M1=65, MLT-M2=75, and MLT-L=80
APT-S=40, APT-M1=45, APT-M2=55, and APT-L=60
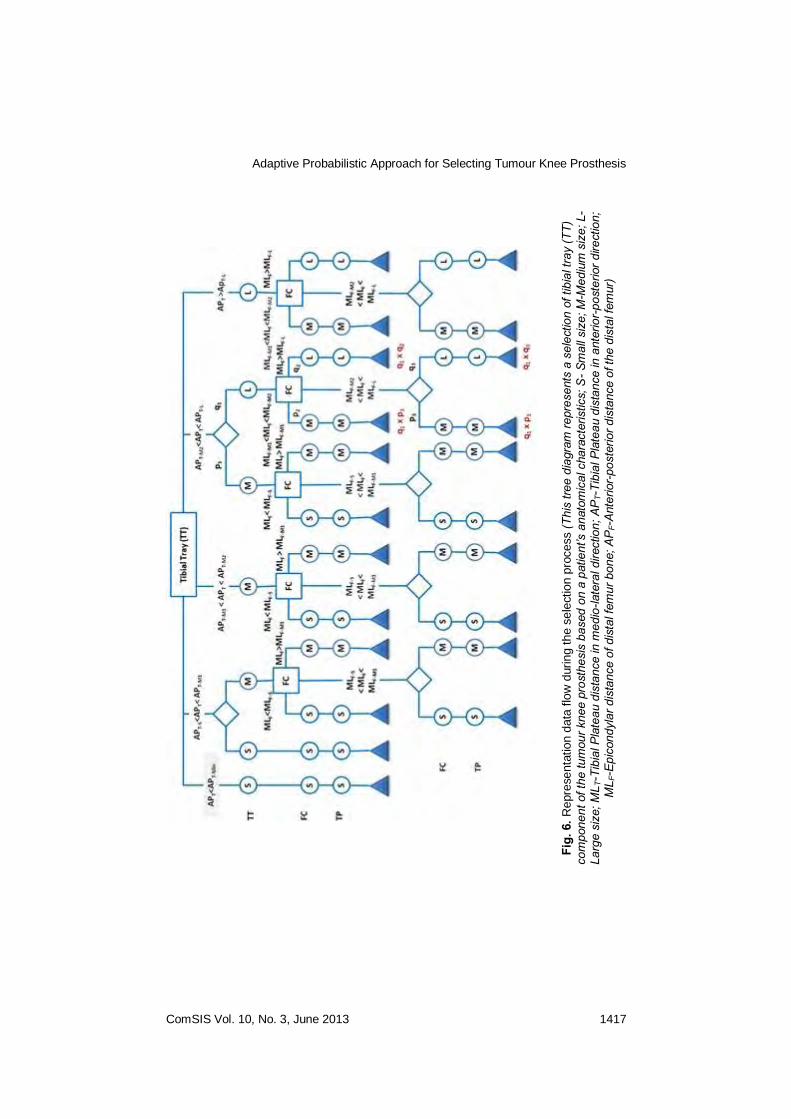
A fuzzy-logic based decision tree was used for selecting critical components such as tibial tray (TT), femoral condylar (FC) component, and tibial poly (refer Figure 6). The TT and FC are first selected based on anterio-posterior dimension of proximal tibial plateau (APT) and medio-lateral dimension of distal femur (MLF), respectively. The tibial poly is selected based on MLFC and APTT. The remaining components are selected based on the dimensions of these three. SF is chosen based on RL and effective reconstruction length of the prosthesis after assembling all components (EL). EL is measured as the distance between tibial component's bottom (prepared surface of tibia) and femoral component's top surface (resected end). Femoral and tibial stems are selected based on intra-medullary canal diameters of femur and tibia bone respectively. Each branch of the decision tree was assigned a weight to evaluate its suitability. Based on the weight, the components were segregated into two groups: (i) ‘most suitable’ and (ii) ‘probably suitable’. The remaining components were tagged as ‘not suitable’.
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1417
Fig.
6. R
epre
senta
tion d
ata
flo
w d
uring the s
ele
ction p
rocess (T
his
tree
diag
ram
repr
esen
ts a
sel
ectio
n of
tibi
al tr
ay (T
T)
com
pone
nt o
f the
tum
our k
nee
pros
thes
is b
ased
on
a pa
tient
’s a
nato
mic
al c
hara
cter
istic
s; S
- Sm
all s
ize;
M-M
ediu
m s
ize;
L-
Larg
e si
ze; M
L T-T
ibia
l Pla
teau
dis
tanc
e in
med
io-la
tera
l dire
ctio
n; A
PT-
Tibi
al P
late
au d
ista
nce
in a
nter
ior-
post
erio
r dire
ctio
n;
ML F
-Epi
cond
ylar
dis
tanc
e of
dis
tal f
emur
bon
e; A
PF-
Ante
rior-
post
erio
r dis
tanc
e of
the
dist
al fe
mur
)
Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1418 ComSIS Vol. 10, No. 3, June 2013
3.4. Anatomical Suitability Metrics
A set of geometry-based metrics, described below, was developed to quantify the suitability of the selected prosthesis components by positioning them inside patient’s bone model.
1) geometric conformity of every component with respect to the corresponding portion of bone (geometric difference)
2) length difference of leg before and after implantation (reconstruction length difference)
3) difference in curvature of bone and selected prosthesis set (bone curvature difference)
4) shift in articulation centre of the knee joint before and after surgery (knee centre shift)
If the value of one or more metric was lower or higher than the acceptable limit, then the surgeon was given flexibility to decide for a custom-made component.
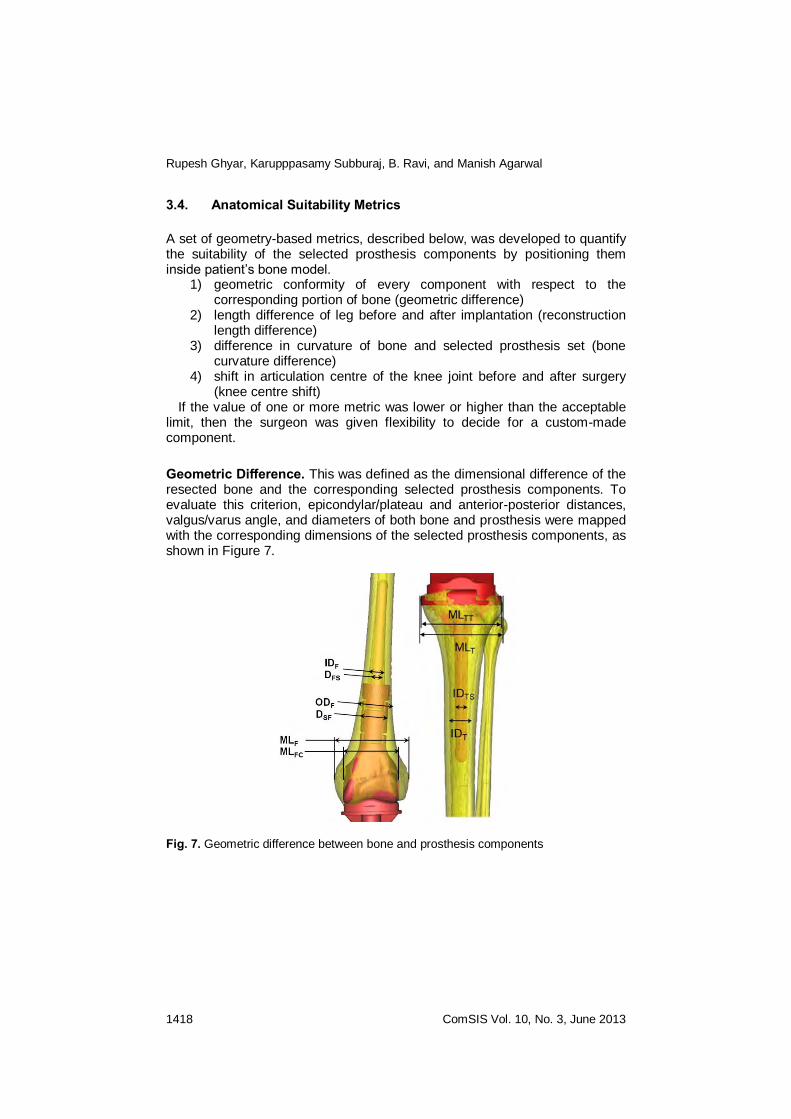
Geometric Difference. This was defined as the dimensional difference of the resected bone and the corresponding selected prosthesis components. To evaluate this criterion, epicondylar/plateau and anterior-posterior distances, valgus/varus angle, and diameters of both bone and prosthesis were mapped with the corresponding dimensions of the selected prosthesis components, as shown in Figure 7.
Fig. 7. Geometric difference between bone and prosthesis components
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1419
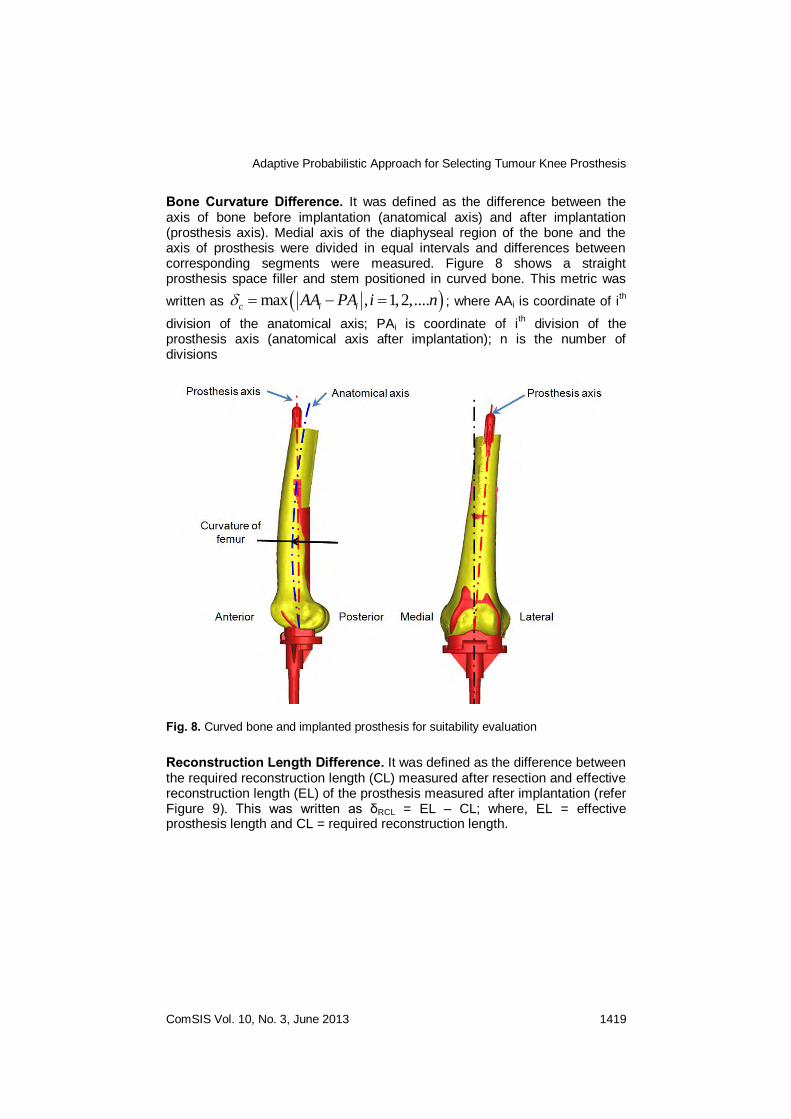
Bone Curvature Difference. It was defined as the difference between the axis of bone before implantation (anatomical axis) and after implantation (prosthesis axis). Medial axis of the diaphyseal region of the bone and the axis of prosthesis were divided in equal intervals and differences between corresponding segments were measured. Figure 8 shows a straight prosthesis space filler and stem positioned in curved bone. This metric was
written as max , 1,2,....c i iAA PA i n ; where AAi is coordinate of ith
division of the anatomical axis; PAi is coordinate of ith division of the
prosthesis axis (anatomical axis after implantation); n is the number of divisions
Fig. 8. Curved bone and implanted prosthesis for suitability evaluation
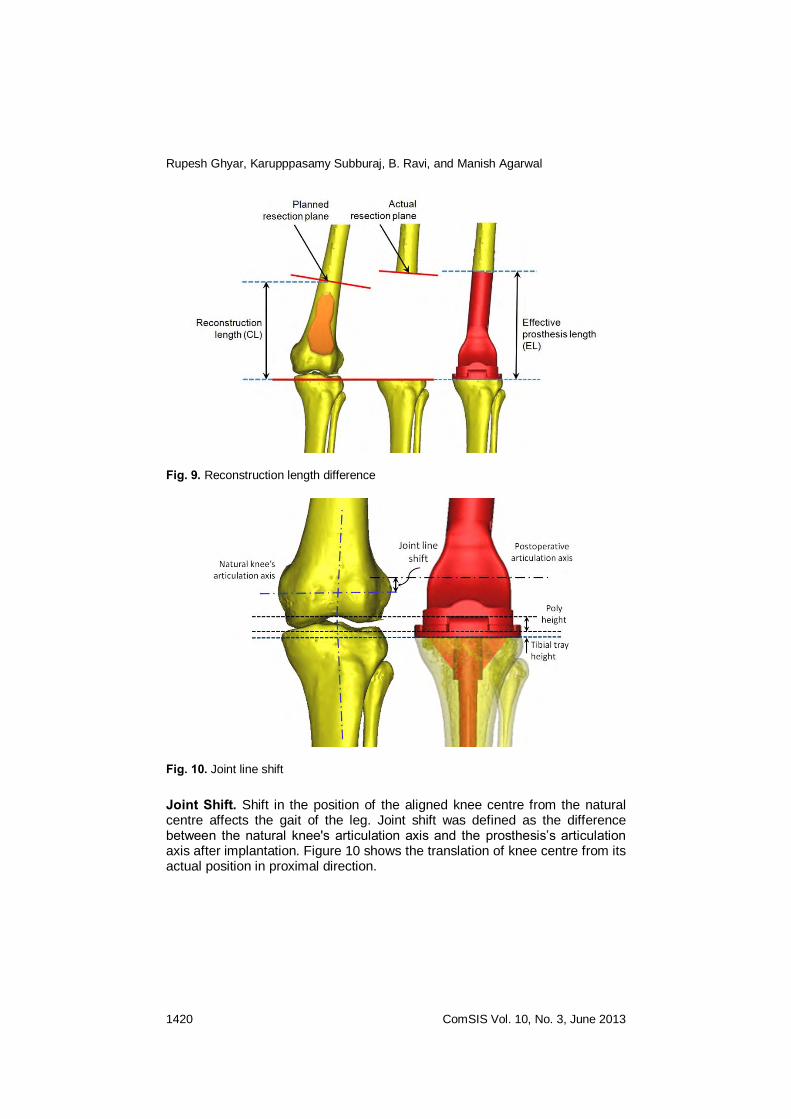
Reconstruction Length Difference. It was defined as the difference between the required reconstruction length (CL) measured after resection and effective reconstruction length (EL) of the prosthesis measured after implantation (refer Figure 9). This was written as δRCL = EL – CL; where, EL = effective prosthesis length and CL = required reconstruction length.
Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1420 ComSIS Vol. 10, No. 3, June 2013
Fig. 9. Reconstruction length difference
Fig. 10. Joint line shift
Joint Shift. Shift in the position of the aligned knee centre from the natural centre affects the gait of the leg. Joint shift was defined as the difference between the natural knee's articulation axis and the prosthesis’s articulation axis after implantation. Figure 10 shows the translation of knee centre from its actual position in proximal direction.

Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1421
3.5. Implementation
The proposed methodology for selection tumour knee prosthesis components was implemented and integrated as a module in an orthopaedic surgery planning system (OrthoSYS). It is an integrated system consisting of a set of three-dimensional geometric methods for effective planning of tumour resection, prosthesis selection and positioning in tumour joint reconstructive surgery (refer Figure 11). The system relied on automating related geometric operations, including identification of anatomical landmarks, quantitative evaluation of bone deformities, and thickness analysis of bone stock. Virtual anatomical model was reconstructed by stacking and segmenting CT scan image data set. A neighbourhood configuration based 3D visualisation algorithm was used for fast rendering of the volumetric data, enabling a quick understanding of anatomical structures [23]. Anatomical landmarks on reconstructed 3D volume model of bone were localised and labelled without user intervention by utilizing their unique geometric characteristics and spatial adjacency relations [24]. Excessive anatomical deformations of the lower limb were automatically measured by referencing the medial axes and anatomical landmarks of femur and tibia bones [25]. The bone stock remaining after tumour resection was analysed in terms of thickness distribution for correctly selecting and fixing the prosthesis [26].
Fig. 11. GUI showing selected prosthesis implantation in 3D bone model

Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1422 ComSIS Vol. 10, No. 3, June 2013
4. Case Study
The distal femur knee replacement of a patient (35/M) was taken as an example to illustrate the entire methodology. The 3D anatomical model of the knee joint was reconstructed from 720 CT axial slices in DICOM format, acquired with the following parameters: pixel width = 0.697 mm, slice thickness = 0.625 mm, and inter-slice distance = 0.7 mm. The anatomical landmarks were located and the anatomical dimensions required for selecting prosthesis components were measured using these anatomical landmarks. Curvature of the femur bone was also calculated automatically from the reconstructed 3D model. Femur bone dimensions were: MLF = 72 mm, and APF = 65 mm. The intra-medullary canal sites were ODF = 28-25 mm and IDF = 16-13 mm at three difference zones of equal intervals from distal femur (condyle) to the middle of femur bone. Tibial bone dimensions were: MLT = 78 mm, APT = 58 mm, ODT = 28-24 mm and IDT = 14-17 mm from proximal tibia to the middle of tibial bone. Femur valgus angle VAF = 4.6
o. Resection length,
after analyzing spread of tumour region, was RL= 120 mm which included about 30 mm margin.
In the elimination phase, over-sized and under-sized components were discarded based on the measured anatomical dimensions and the modular prosthesis components available in the database. As the anterior-posterior dimension of tibia (APT) was considered to be between APT-M2 < APT < APT-L, the suitability factor of medium and large size tibial tray were 0.19 (p1) and 0.81 (q1), respectively. In the decision-tree, the branch attached to Large size component was chosen due to its higher value of suitability factor. Since the chosen tibial tray based on suitability was LARGE, the femoral condyle and tibial poly sizes were constrained to Medium and Large (tree-branch restriction).
The medio-lateral dimension of femoral condyle (MLF) was considered to be between MLF-S < MLF < MLF-M1. Suitability factors of the Medium and Large size femoral condyle were 0.1 (p2) and 0.9 (q2). Large size femoral condyle is selected based on higher suitability factor. Since Large size tibial tray and femoral condylar component were selected, accordingly corresponding Large size tibial poly were also selected. Final cumulative suitability factor of the selected prosthesis components set was 0.54 (for Large) and 0.4 (for Medium). Thus the 'most suitable' set for this case was Large size TT, FC, and TP; the 'probably suitable' set was Medium size TT, FC, and TP. Total reconstruction length was 134 mm (RL=120 mm). Minimum length of large size femoral condyle was 62 mm. The femur bone space fill length (RCL-LFC) was 72 mm, which was compensated by two space filler components (40 mm and 35 mm).
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1423
5. Discussion
Due to discrete modularity in terms of size, the required size of a component may not be available readily. In such case, typically the nearest size component is chosen. Pre-operative planning reduces the need for intra-operative decisions and related risk of size mismatch. Custom-made component is used only when no available component matches the requirement. Tibial tray component is typically selected and implanted before femoral condylar component to ensure there is no mismatch between tibial tray and femoral condylar components. While selecting the tibial poly component, dimensions of the selected femoral condylar and tibial tray component are used as a reference. Tibial poly selection is important to ensure femoral condylar component does not impinge upon the tibial tray, which leads to wear particles. The size of condylar component of prosthesis is always chosen smaller than the corresponding bone (femoral condyle). This is due to massive amount of soft-tissue (near biopsy opening) excised along with tumour affected tissue to reduce contamination caused by biopsy, necessitating a smaller size of femoral condylar component to ensure tension-free wound closure and prevent arterial damage from traction on the vessel.
The thickness of the tibial poly component will be decided according to the knee centre measured between tibia and femoral condyle. Proximal shift of knee centre can be compromised only up to 3-5 mm; more than that will affect the gait of the patient. Hence, the thickness of the tibial poly is always decided according to the length of tibial tray. Knee centre shift is contributed by many factors, the main one being the thickness of tibial poly and tibial tray components. In distal femur tumour knee replacement cases, 3-4 mm slice of tibial surface may be resected to prepare it for fixing the tibial component of the prosthesis.
There are two ways to incorporate curvature of the bone in prosthetic replacement: (i) use of curved stem and (ii) osteotomy. If osteotomy is chosen, then it has to be performed on both legs to maintain the gait of the limb. This metric was designed to ensure that curvature of bone was considered and the difference does not affect the surgical outcomes. Standard modular prosthesis sets have a limited choice in size of modular components like space fillers and femoral and tibial stems, which lead to increase in effective prosthesis length than that the required. The difference δRCL occurs due to usage of fixed valgus prosthesis systems. Currently, no commercially available TKP system offers the commonly observed ≈2
o varus
in tibia, which also contributes to a shorter CL value. Further, the tibial cut is made with due consideration of visible bone curvature. If prosthesis with a straight stem is implanted, unconsidered bone curvature deformities add a certain length to reconstruction length. A stem is inserted in the bone to hold the prosthesis in position and transmit the load from bone to prosthesis and vice versa. One of the most common mechanical failures observed in prosthesis is fracture of stem due to inadequate size and overloading. A small stem may lead to collapse of the entire prosthesis. On the other hand, oversized stems may lead to fracture of bone. Cemented fixation uses a fast-

Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1424 ComSIS Vol. 10, No. 3, June 2013
curing bone cement (polymethylmethacrylate) to hold the prostheses in place. Cementless fixation relies on the in-growth of bone into the porous coated surface. To transmit and withstand the body weight, the maximum possible size of the stem that the bone can accommodate has to be selected.
In practice, the resection length is initially decided according to the spread of disease. After selecting prosthesis components, the effective prosthesis length is usually higher than the required reconstruction length. Hence the resection length must be revised by considering selected prosthesis components set. Also, most of the standard prostheses do not consider bone deformities (such as curved femur), which limits the selection of femoral and tibial stems. These unconsidered bone deformities affect the gait of limb after implantation. If the error measures are higher than acceptable for all combinations of prosthesis components, then the surgeon may decide to go for a patient-specific custom-made prosthesis. Space filler is an optional connective element between femoral condyle and stem. This is placed to adjust the reconstruction length. The interrelationship between prosthesis components affects the sequence of selection. Typically space filler is a cylindrical piece with diameter close to the outer diameter of the bone. So, we can eliminate unsuitable components by mapping outer diameter of the bone and diameter of the space filler.
The tibial tray and femoral condylar components were first selected based on anterio-posterior dimension of proximal tibial plateau and epicondylar distance of the distal femur, respectively. The remaining components were selected based on the dimensions of tibial tray, femoral condyle and tibial poly component. Space fillers were chosen based on the resection length and effective reconstruction length of the prosthesis after assembling all components (effective length). Effect length was measured as the distance between tibial component's bottom (prepared surface of tibia) and femoral component's top surface (resected end). Femoral and tibial stems were selected based on intra-medullary canal diameters of femur and tibia bone respectively.
Preliminary research findings of this work was reported in references ([27] and [28]) as a part of those articles describing overall system design, architecture, and validation. In those articles, we focused on describing usage of 3D computer graphics and geometric reasoning algorithms to aid surgeons in planning tumour knee replacement. The present study focussed specially on details of the algorithm, developed for selecting tumour knee prosthesis components, using fuzzy logic and decision tree along with anatomical suitability metrics to evaluate the suitability of the selected prosthesis components when compared with patient's anatomy. Detailed description on selection methodology, fuzzy representation of the sizes of different prosthesis components, development of prosthesis components database, two additional case studies, and in-depth discussion on clinical implications of the case study results were included in this manuscript. This is perhaps the first attempt of using a decision method driven by anatomical properties (including dimensions, deformities, and bone stock thickness) extracted from three-dimensional anatomical model for tumour knee prosthesis components

Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1425
selection. A set of anatomical suitability metrics to evaluate the geometric as well as alignment deviation of prosthesis from bone model have been developed. This is to ensure that the selected prosthesis components fit into the anatomical space left after resection, fulfil their function without interfering with the surrounding tissues (geometric suitability), and produce a normal pattern of gait (alignment). These metrics provide a numerical measure to surgeons, drawing their attention to any error-prone steps. There is no previous reported work on quantifying suitability of prosthesis components and alignment in tumour joint reconstructive surgery planning and the work fills this gap.
In summary, a geometry-driven, fuzzy-logic based decision method to systematically categorize the tumour knee prosthesis components (most suitable, probably suitable, and not suitable) based on anatomical dimensions extracted from the 3D bone models reconstructed from CT scan data of the specific patient, to assist surgeons in selecting the correct set, was described. Fuzzy representation of sizes of prosthesis components improved the adaptability of the approach and accommodates the approximation caused by modularity. Fuzzy-logic based decision tree effectively mapped the inter-dependency of the components. An XML based representation allowed easy incorporation of additional components and new prosthesis components without major changes in database structure. Anatomical suitability metrics along with 3D bone models allowed quantifying the suitability of prosthesis components accurately and quickly. Integrating 3D geometric reasoning algorithms with decision methods automated the approach and yielded consistent results with minimal human intervention.
Acknowledgements. This work was a part of a project on developing a Computer
Assisted Orthopaedic Surgery Planning and Navigation System at IIT Bombay in
collaboration with Tata Memorial Hospital, Mumbai. It was supported by the Office of
the Principal Scientific Adviser to the Government of India, New Delhi.
References
1. Ravi, B. and Agarwal, M.G., “Computer aided development of mega endo-prostheses,” in Bio-Materials and Prototyping Applications in Medicine, B. Bidanda and P. Bartolo (Eds.), Springer, USA, 2008, 191–207
2. Lewis, V.O., “What’s new in musculoskeletal oncology,” Journal of Bone and Joint Surgery, 91-A (6) (2009), 1546–1556
3. Sim, I.W., TSe, L.F., Ek, E.T., Powell, G.J., and Choong, P.F.M., “Salvaging the limb salvage: management of complications following endoprosthetic reconstruction for tumours around the knee,” European Journal of Surgical Oncology, 33 (6) (2007), 796–802
4. NICE, “Guidance on the selection of prostheses for primary total hip replacement,” National Institute for Clinical Excellence, London, UK, (2000), 1–12
Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1426 ComSIS Vol. 10, No. 3, June 2013
5. Bugbee, W.D., Ammeen, D.J., and Engh, G.A., “Does implant selection affect outcome of revision knee arthroplasty?,” Journal of Arthroplasty, 16 (5) (2001), 581–585
6. Chin, K.R., Dalury, D.F., Zurakowski, D., and Scott, R.D., “Intraoperative measurements of male and female distal femurs during primary total knee arthroplasty,” Journal of Knee Surgery, 15 (4) (2002), 213–217
7. Giles, L.G. and Taylor, J.R., “Low-back pain associated with leg length inequality,” Spine, 6 (5) (1981), 510–21
8. Curran, S., “Relationship of functional leg-length discrepancy to abnormal pronation: commentary,” Journal of American Podiatric Medical Association, 96 (6) (2006), 505–506
9. Rajagopal, T.S. and Nathwani, D., “Can interepicondylar distance predict joint line position in primary and revision knee arthroplasty?,” American Journal of Orthopedics, 40 (4) (2011), 175-178
10. Schwab, J.H., Agarwal, P., Boland, P.J., Kennedy, J.G., and Healey, J.H., “Patellar complications following distal femoral replacement after bone tumour resection,” Journal of Bone and Joint Surgery, 88A (10) (2006), 2225–2230
11. Healy, W.L., Kirven, F.M., Iorio, R., Patch, D.A., and Pfeifer, B.A., “Implant standardization for total hip arthroplasty: An implant selection and a cost reduction program,” The Journal of Arthroplasty, 10 (2) (1995), 177–183
12. Nelson, C.L., Gioe, T.J., Cheng, E.Y., Thompson, R.C., “Implant selection in revision total knee arthroplasty,” The Journal of Bone & Joint Surgery, 85-A (2003), 43-51
13. Hewitt, B. and Shakespeare, D., “A straightforward method of assessing the accuracy of implantation of knee prostheses,” The Knee, 8 (2) (2001), 139–144
14. Jeon, D.G., Lee, S.Y., and Kim, J.W., “Bone primary sarcomas undergone unplanned intralesional procedures – the possibility of limb salvage and their oncological results,” Journal of Surgical Oncology, 94 (7) (2006), 592–598
15. Charnley, J. “Low friction arthroplasty of the hip,” Springer Verlag, Berlin, 1979, 246
16. Muller, M.E., “Total hip replacement: planning, technique and complications,” In: Surgical Management of Degenerative Arthritis of the Lower Limb, Cruess, R.L. and Nelson, M.S. (Eds.), Lea and Faber, Philadelphia, (1975), 90–113
17. Ho, D.M. and Huo, M.H., “Are critical pathways and implant standardization programs effective in reducing costs in total knee replacement operations?,” Journal of the American College of Surgeons, 205 (1) (2007), 97–100
18. Harris, S.J, Jakopec, M., Hibberd, R.D., Cobb, J., and Davies, B.L., “Interactive pre-operative selection of cutting constraints, and interactive force controlled knee surgery by a surgical robot,” MICCAI’98, W.M. Wells et al. (Eds.), Lecture Notes in Computer Science, 1496 (1998), 996–1006
19. Anderson, J.A. and Sculco, T.P., “Implant Selection in Revision Total Knee Replacement,” Techniques in Orthopaedics, 26 (2) (2011), 94–98
20. Sundaram, M. and Rohren, E.M., “Primary bone tumours,” in Imaging on Oncology, J. Husband and R.H. Reznek (Eds.), Taylor and Francis, London, 2nd Edition, (2004), 515–536
21. Ravi, B., “OrthoCAD network centre for endoprosthetic skeletal reconstruction systems,” Project Report - PSA/OrthoCAD/2006-09, Indian Institute of Technology Bombay, INDIA, (2009), 1–29
22. Vaidya SV, Ranawat CS, Aroojis A, Laud NS. Anthropometric measurements to design total knee prostheses for the Indian population. J Arthroplasty. 2000 Jan;15(1):79-85
Adaptive Probabilistic Approach for Selecting Tumour Knee Prosthesis
ComSIS Vol. 10, No. 3, June 2013 1427
23. Subburaj, K. and Ravi, B., “High resolution medical modelling and geometric reasoning starting from CT/MR images,” in G. Wang, H. Li, H. Zha, and B. Zhou (Eds.), proceedings of IEEE 10th International Conference on CAD and Computer Graphics, IEEE Computer Society, Beijing, China, 2007, 441–444
24. Subburaj, K., Ravi, B., and Agarwal, M.G., “Automated identification of anatomical landmarks on bone models reconstructed from CT scan images,” Computerized Medical Imaging and Graphics, 33 (5) (2009), 359–368
25. Subburaj, K., Ravi, B., Agarwal, M.G., "Computer-Aided Methods for Assessing Lower Limb Deformities in Orthopaedic Surgery Planning," Computerized Medical Imaging and Graphics, 34(4), 2010, 277-288
26. Subburaj, K., Patil, S.S., Ravi, B., “Voxel-based thickness analysis of intricate objects,” International Journal of CAD/CAM, 6 (1) (2006), 105-115
27. Subburaj, K., Suresh Kumar, P., Anasane, S.S., Ravi, B., Agarwal, M.G., " Geometry driven decision support system for knee tumour mega endo‐prosthesis componenets selection ," ASME Frontiers of Biomedical Devices Conference, Irvine, California, USA, June 18‐20, 2008, Biomed-38035, 67-68
28. Subburaj, K., Ravi, B., and Agarwal, M.G., "Automated 3D geometric reasoning in computer assisted joint reconstructive surgery," in proceedings of IEEE Automation Science and Engineering, Bangalore, 22-25 Aug, (2009), 367–372 Rupesh Ghyar is a Senior Research Associate in OrthoCAD Network Research Laboratory at IIT Bombay since 2007. His research focuses on design, development and testing of Orthopaedic implants & instruments using CAD/CAM tools. Currently, he is writing his Ph.D thesis on integrated testing methodology for modular and custom implants, which involves standardization of FEA coupled with experimental evaluation, using photoelasticity and strain measurements on a UTM. He also holds two a patent for Apparatus and another patent for method for Orthopaedic surgery and Modular knee joint implant for anthropometric anatomical variation. He holds a Masters degree in Bioengineering, from University of Strathclyde, UK, completed in 2005 after his Bachelor's degree, in mechanical engineering, from Govt. College of Engineering Pune, in 2003. His Masters work focused on "Mathematical modelling of mechanical properties of human tendons". He has guided several M.Tech and B.Tech students at IIT Bombay in projects related to medical device development. He has also given talks in conferences like Biotribology (Xian, China), ASM Biomaterials and Medical Implants and Altair HyperWorks Technology Conference, invited lectures in courses like Magnetic Resonance Imaging - IIT Bombay, Medical Implants Innovation challenges - IIT Delhi and trained working professionals from Depuy on biomechanics. Dr. Karupppasamy Subburaj is a postdoctoral scholar in the Musculoskeletal Quantitative Imaging Research laboratory in the department of radiology and biomedical imaging at the University of California San Francisco (UCSF). He received his PhD degree in Mechanical Engineering from the Indian Institute Technology Bombay (IIT Bombay), India in 2009. His thesis work was focused on developing geometric reasoning algorithms for extracting geometric characteristics of bones and planning tumor knee reconstructive surgery. He worked as a Senior Research Associate in the OrthoCAD Network Research Laboratory at IIT Bombay before joining UCSF. Currently, at UCSF, he is focused on developing image-based modelling, analysis, and quantification methods to

Rupesh Ghyar, Karupppasamy Subburaj, B. Ravi, and Manish Agarwal
1428 ComSIS Vol. 10, No. 3, June 2013
study joint loading pattern and contact kinematics in young healthy adults and patients with osteoarthritis. He has edited a technical book on CT imaging techniques and applications, and published 20 journal papers in international journals and over 40 international conference papers. He is a regular manuscript reviewer for many international journals in the domain of medical image analysis, computer graphics, computer aided surgery, and medical imaging. His research interests are in the domain of 3D geometric processing, musculoskeletal biomechanics, medical image analysis, virtual surgery planning, and interactive computer graphics. Dr. B. Ravi is an Institute Chair Professor, working in Mechanical Engineering Department, IIT Bombay. He completed his BE from National Institute of Technology, Rourkela in 1986, followed by Masters and Ph.D. from Indian Institute of Science, Bangalore in 1992. He has held visiting appointments at West Virginia (in 1996) and Purdue University (in 2006). His research work focuses on the areas of casting design and simulation, CAD/ CAM and biomedical device development. He has guided 8 PhD and over 50 Master students. He has published over 200 technical papers, two books. He has conducted 10 certificate courses on Casting Design & Simulation, and 20 simulation clinics all over India. He is also heading the E-Foundry lab and OrthoCAD Network Research Laboratory at IIT Bombay. He is a member of the Program Advisory Committee of DST (Dept. of Science & Technology). He is a Fellow of the Institution of Engineers, and Vice President of the Governing Council of Central Manufacturing Technology Institute, Bangalore. He is the associate editor of Indian Foundry Journal, and review board member of International CAD, Rapid Prototyping, Bio Fabrication and manufacturing journals. Dr. Manish Agarwal is currently a Consultant Orthopaedic Oncologist at the Hinduja Hospital & Medical Research Centre, Mumbai. He did his M.B.B.S. from the University of Bombay and M.S. (Ortho) also from the University of Bombay. He is a member of the Musculoskeletal Tumor Society (North America), the Indian Orthopaedic Association, and the Indian Society of Oncology. He is teaching Faculty for Orthopaedics at the S.N.D.T. College of Nursing, Mumbai. He has been appointed on board as Independent Non Executive Director for Zee Learn, an education company of the reputed Zee Group which deals with education at various levels. He has been awarded Gold Medal for Orthopedic Surgery 2004 conference by Special Executive Magistrates Society. He has also been awarded Best Paper Award for his research papers presented in Annual Conference of Bombay Orthopaedic Society on 1998, 2002, 2004 and 2010. He has received S.S. Yadav Gold Medal for best paper in Oncology in 2009 at annual Conference of the Indian Orthopaedic Association. There are about 30 research papers and three books in the field of Orthopaedic Oncology, published on his name in last 5 years. Received: April 5, 2012; Accepted: December 13, 2012