Embed Size (px)
Citation preview
Addiction Resource Center’s
Experience 2005-2010
Marketing and Finding/Maximizing
Revenue Sources for your Evidence Based Practices
November 2005November 2005NIATxNIATx
ARC receives a PI Grant from the Maine ARC receives a PI Grant from the Maine Office of Substance Abuse (OSA)Office of Substance Abuse (OSA)
Objectives: Objectives: Learn Rapid Cycle Process Improvement.Learn Rapid Cycle Process Improvement. Use these tools to decrease client wait times Use these tools to decrease client wait times
and increase client retention in treatment.and increase client retention in treatment. Report your data and share your experiences.Report your data and share your experiences.
Pt. Access is a Program’s Pt. Access is a Program’s Best Marketing ToolBest Marketing Tool
Long wait-times. High demand Long wait-times. High demand characteristic access systems, and a characteristic access systems, and a generalized acceptance of the term generalized acceptance of the term “hard to place clients” have become the “hard to place clients” have become the status quo in public behavioral health.status quo in public behavioral health.
Immediate access to services is such an Immediate access to services is such an anomaly, optimizing access and anomaly, optimizing access and promoting it will be your agencies’ best promoting it will be your agencies’ best social marketing strategy.social marketing strategy.
Social Marketing: What Social Marketing: What We DidWe Did
Product = MATProduct = MAT Behavior Change=Behavior Change=ReferentsReferents
ExpectExpect immediate access and immediate access and relevant treatment services.relevant treatment services.
Population segments= Payers, Population segments= Payers, referring systems (DOC, Judicial, referring systems (DOC, Judicial, Child Protective, Detox, current Child Protective, Detox, current abusers of chemicals and other abusers of chemicals and other agencies).agencies).
Indicators of Successful Indicators of Successful Social Marketing Social Marketing
““I always get my clients in at ARC.” I always get my clients in at ARC.” ““You guys don’t believe in You guys don’t believe in
impossible clients” impossible clients” “ “I knew you’d know what to do.” I knew you’d know what to do.” ““I just texted 40 of my friends.”I just texted 40 of my friends.” ““We need more chairs, parking We need more chairs, parking
spaces, staff…”spaces, staff…”
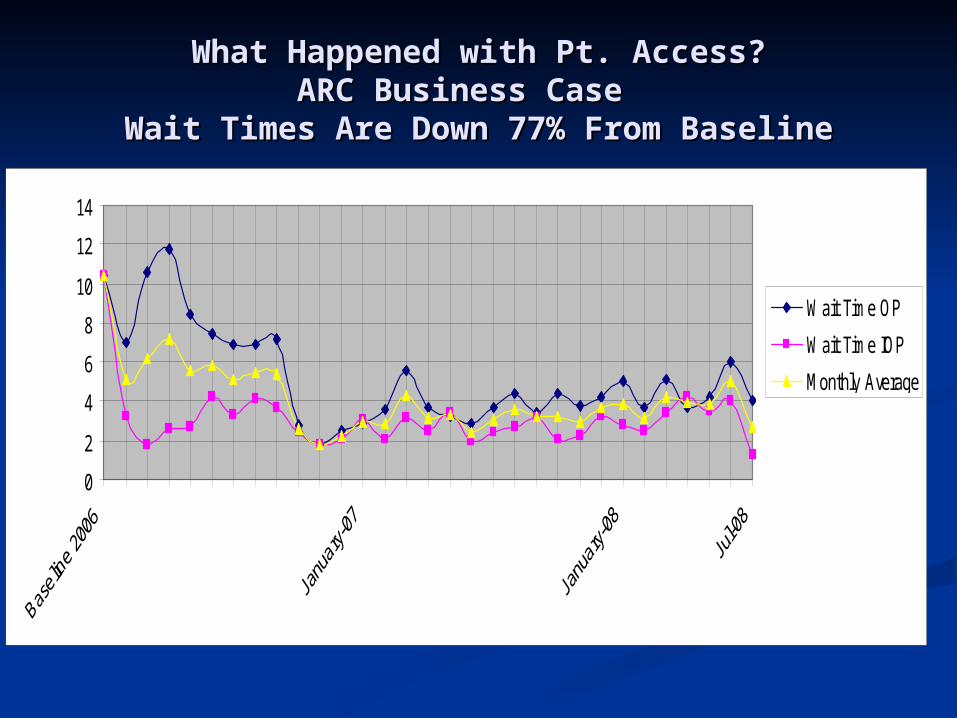
What Happened with Pt. Access?What Happened with Pt. Access?ARC Business Case ARC Business Case
Wait Times Are Down 77% From BaselineWait Times Are Down 77% From Baseline
0
2
4
6
8
10
12
14
Wait Time OP
Wait Time IOP
Monthly Average
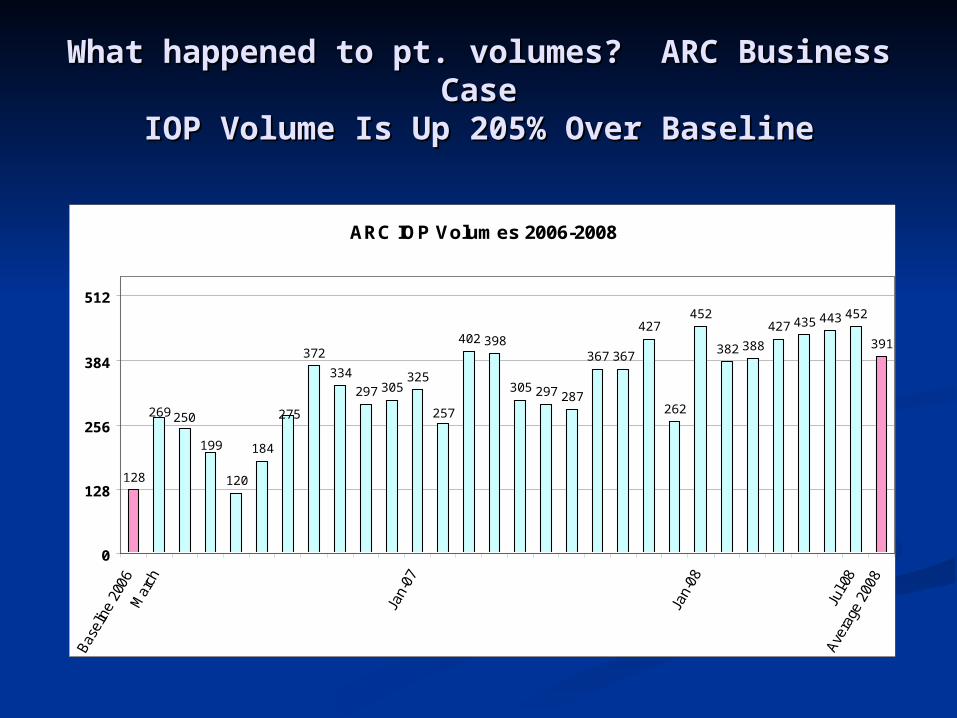
What happened to pt. volumes? ARC Business What happened to pt. volumes? ARC Business CaseCase
IOP Volume Is Up 205% Over BaselineIOP Volume Is Up 205% Over Baseline
ARC IOP Volumes 2006-2008
120
184
372
334
297 305325
402 398
305 297 287
367 367
427
262
452
382 388
427 435 443 452
391
275 257
199
128
269 250
0
128
256
384
512
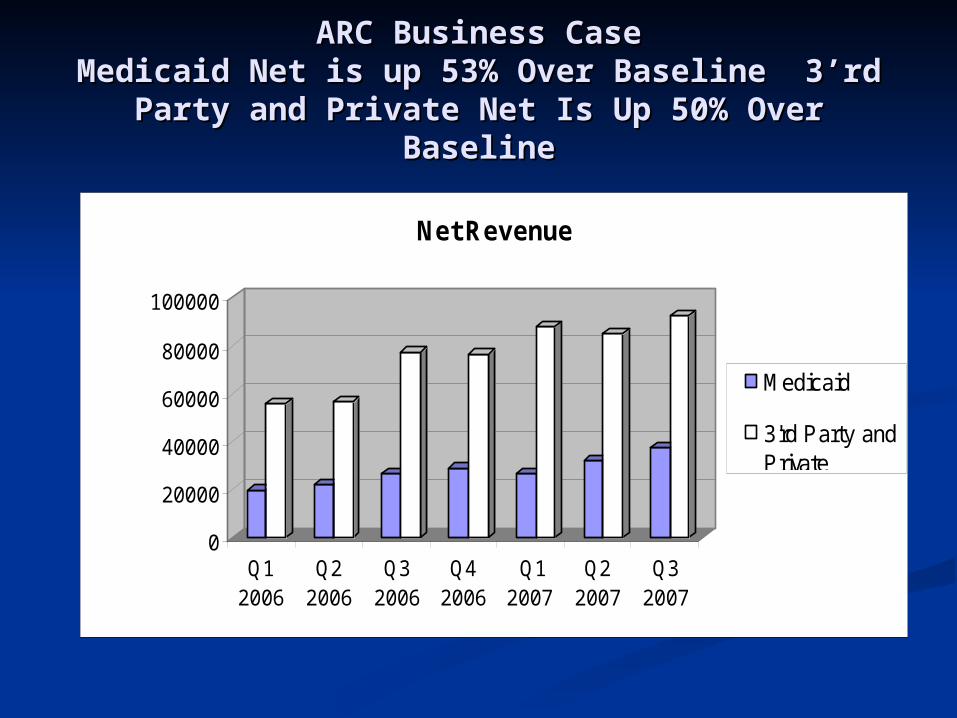
ARC Business CaseARC Business CaseMedicaid Net is up 53% Over Baseline 3’rd Medicaid Net is up 53% Over Baseline 3’rd
Party and Private Net Is Up 50% Over BaselineParty and Private Net Is Up 50% Over Baseline
0
20000
40000
60000
80000
100000
Q12006
Q22006
Q32006
Q42006
Q12007
Q22007
Q32007
Net Revenue
Medicaid
3'rd Party andPrivate
A Model for ChangeA Model for Change
The NIATx Way: The NIATx Way: Performance/Process Improvement Performance/Process Improvement has provided ARC three key assets has provided ARC three key assets which enable larger systems change:which enable larger systems change:1. Tools to manage change.1. Tools to manage change.
2. Experience being successful. (Access 2. Experience being successful. (Access and and Retention)Retention)
3. Institutional Credibility3. Institutional Credibility (budget (budget neutrality or better)neutrality or better)
November 2006November 2006
We still had an opiate problem!We still had an opiate problem!
Needed to make a big change!Needed to make a big change!
November 2006November 2006
Implement Medication Assisted Implement Medication Assisted Treatment (MAT) for opiate Treatment (MAT) for opiate addictionaddiction. (Service Gap). (Service Gap)
Not with 20 consumers, but 200Not with 20 consumers, but 200. . (Economies of Scale—Delivery Model)(Economies of Scale—Delivery Model)
We needed a PLAN!We needed a PLAN!
Key ActivitiesKey Activities Analyze relevance of current services and Analyze relevance of current services and
what gaps exist. Pt. Need, Payor Need.what gaps exist. Pt. Need, Payor Need. Analyze community demand for service. Analyze community demand for service.
Volumes.Volumes. Analyze Payer Mix for new and existing Analyze Payer Mix for new and existing
services.services. Complete draft of “Mission Fit” and Complete draft of “Mission Fit” and
“Business Case.”“Business Case.” Present business plan to Hospital Present business plan to Hospital
Administration/Board.Administration/Board.
Demand Analysis-Demand Analysis-Mission FitMission Fit
ARC took a 4 month snap shot to trend ARC took a 4 month snap shot to trend volumes of clients seeking treatment for volumes of clients seeking treatment for opiate dependence. opiate dependence. On average 15-20 callers per month request On average 15-20 callers per month request
Suboxone assisted treatment. Suboxone assisted treatment. Of 15 assessments Dx. with opioid Of 15 assessments Dx. with opioid
dependence in Jan. and Feb. 2007dependence in Jan. and Feb. 2007 Five have admitted to treatment programs and Five have admitted to treatment programs and
are involved in MAT. are involved in MAT. Those not admitted did not access MATThose not admitted did not access MAT
Anticipated volume of new ARC clients Anticipated volume of new ARC clients per year is 100-150 clients per year is 100-150 clients
Pt. Volumes AnalysisPt. Volumes Analysis
Obtained report from Maine Obtained report from Maine Hospital Association looking at Hospital Association looking at DRG’s of opiate DRG’s of opiate dependence/detoxification.dependence/detoxification.
Sorted data by zip code, then payer Sorted data by zip code, then payer source.source.
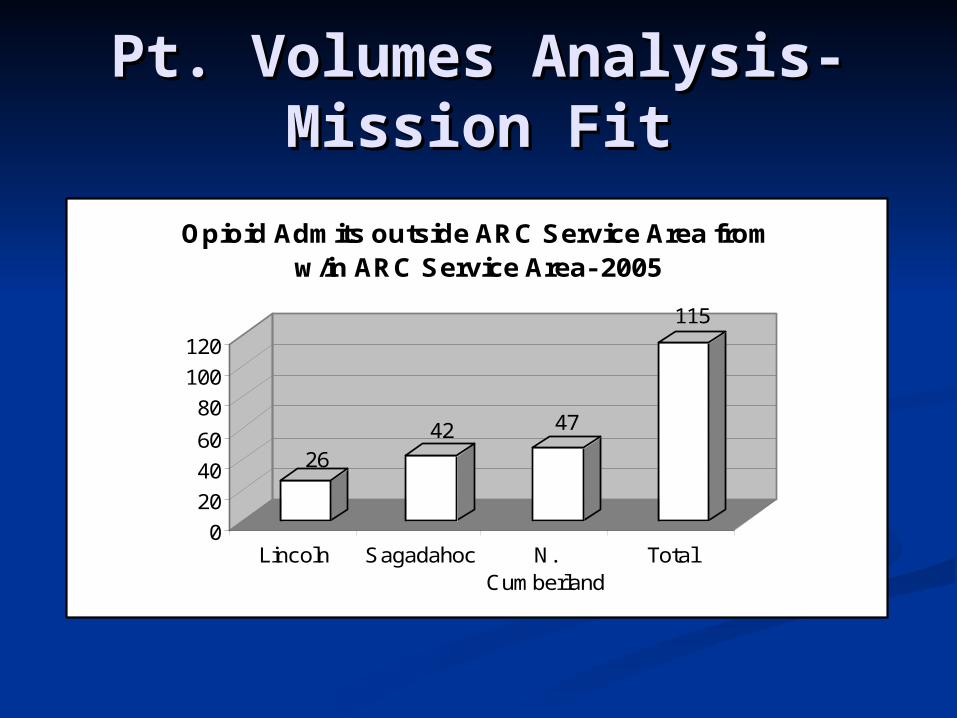
Pt. Volumes Analysis-Pt. Volumes Analysis-Mission FitMission Fit
2642 47
115
0
20
40
60
80
100
120
Lincoln Sagadahoc N.Cumberland
Total
Opioid Admits outside ARC Service Area from w/in ARC Service Area- 2005
Community Response-Community Response-Business CaseBusiness Case
The 115 patients treated by other programs The 115 patients treated by other programs equate to the current volume of ARC equate to the current volume of ARC Intensive Outpatient Programs (IOP).Intensive Outpatient Programs (IOP).
Absorbing this volume equates to an Absorbing this volume equates to an additional 2,300 IOP treatment days per additional 2,300 IOP treatment days per year for ARC.year for ARC.
The funding mix from this population is:The funding mix from this population is:34% private insurance34% private insurance28% Medicaid28% Medicaid17% Medicare17% Medicare16% Unfunded16% Unfunded
Payer PrioritiesPayer Priorities Cigna endorses Medication Assisted Cigna endorses Medication Assisted
Treatment.Treatment. Anthem puts out report on improved Anthem puts out report on improved
outcomes with MAT.outcomes with MAT. Cigna is largest payer in our service area. Cigna is largest payer in our service area.
Bath Iron Works. “The Shipyard”.Bath Iron Works. “The Shipyard”. Anthem is largest 3’rd party payer in Maine.Anthem is largest 3’rd party payer in Maine. Ambulatory detox is cheaper than IP.Ambulatory detox is cheaper than IP. 2011- ARC awarded Gold Card Status by 2011- ARC awarded Gold Card Status by
Anthem for IOP and PHP based upon low re-Anthem for IOP and PHP based upon low re-admission rates and lengths of stay. Auto admission rates and lengths of stay. Auto auth. initial 14 days of IOP and PHP as a auth. initial 14 days of IOP and PHP as a result.result.
Capacity PlanningCapacity Planning 20% attrition rate is factored for each change 20% attrition rate is factored for each change
in level of care. Induction to Med. in level of care. Induction to Med. Management, during IOP treatment, and from Management, during IOP treatment, and from IOP to Aftercare.IOP to Aftercare. Based on national models for suboxone assisted Based on national models for suboxone assisted
treatment and three years experience at other treatment and three years experience at other Maine Hospital-Based programs.Maine Hospital-Based programs.
Capacity exists for 832 Med. Management Capacity exists for 832 Med. Management visits in first 18 months. visits in first 18 months.
Based upon the data above, we expect to Based upon the data above, we expect to complete 532 Med. Management visits in first complete 532 Med. Management visits in first 18 months. 18 months.
This 300 patient buffer exists to assure optimal This 300 patient buffer exists to assure optimal pt. care and to avoid overwhelming resources.pt. care and to avoid overwhelming resources.
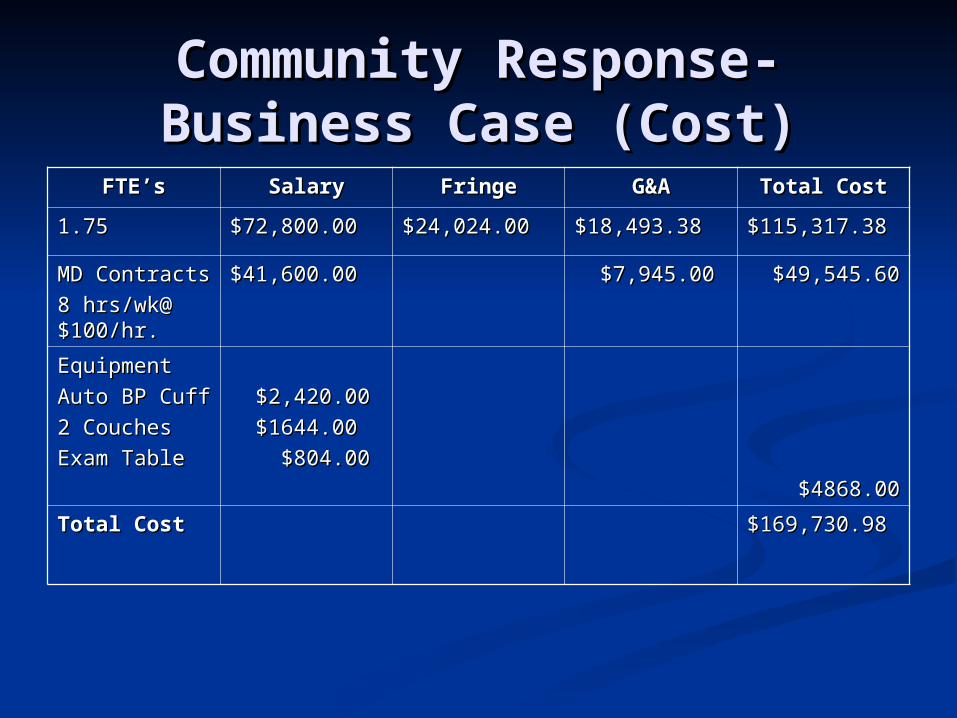
Community Response-Community Response-Business Case (Cost)Business Case (Cost)
FTE’sFTE’s SalarySalary FringeFringe G&AG&A Total CostTotal Cost
1.751.75 $72,800.00$72,800.00 $24,024.00$24,024.00 $18,493.38$18,493.38 $115,317.38$115,317.38
MD ContractsMD Contracts
8 hrs/wk@ 8 hrs/wk@ $100/hr.$100/hr.
$41,600.00$41,600.00 $7,945.00$7,945.00 $49,545.60$49,545.60
EquipmentEquipment
Auto BP CuffAuto BP Cuff
2 Couches 2 Couches
Exam TableExam Table
$2,420.00$2,420.00
$1644.00$1644.00
$804.00$804.00
$4868.00$4868.00
Total CostTotal Cost $169,730.98$169,730.98
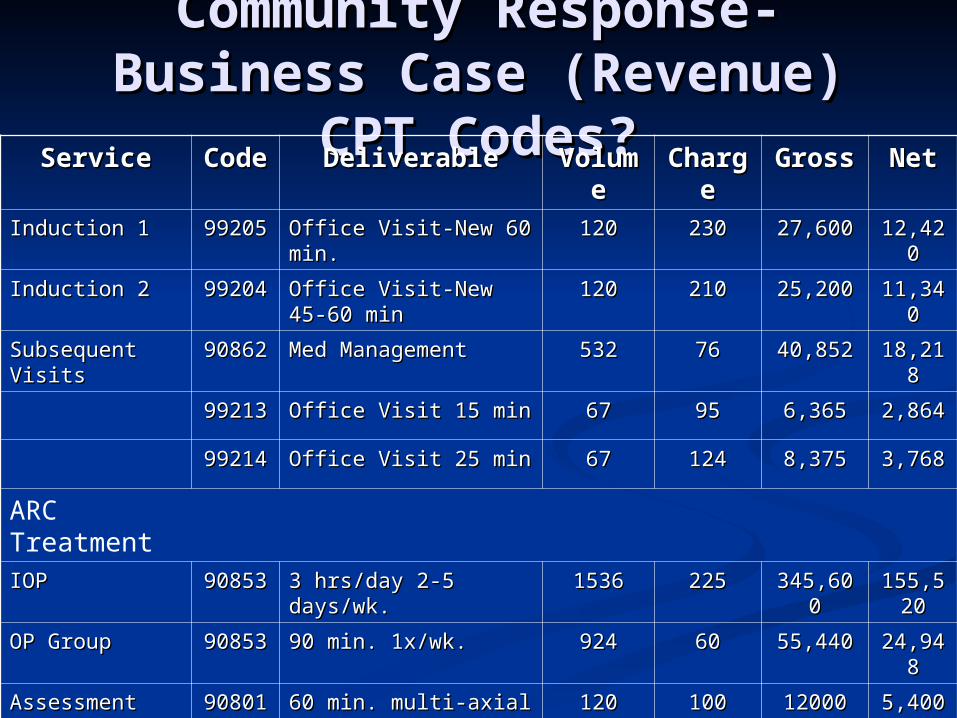
Community Response-Community Response-Business Case (Revenue) Business Case (Revenue)
CPT Codes?CPT Codes?ServiceService CodCodee
DeliverableDeliverable VoluVolumeme
CharChargege
GrossGross NetNet
Induction 1Induction 1 9920599205 Office Visit-New 60 Office Visit-New 60 min.min.
120120 230230 27,60027,600 12,4212,4200
Induction 2Induction 2 9920499204 Office Visit-New 45-60 Office Visit-New 45-60 minmin
120120 210210 25,20025,200 11,3411,3400
Subsequent Subsequent VisitsVisits
9086290862 Med ManagementMed Management 532532 7676 40,85240,852 18,2118,2188
9921399213 Office Visit 15 minOffice Visit 15 min 6767 9595 6,3656,365 2,8642,864
9921499214 Office Visit 25 minOffice Visit 25 min 6767 124124 8,3758,375 3,7683,768
ARC TreatmentIOPIOP 9085390853 3 hrs/day 2-5 days/wk.3 hrs/day 2-5 days/wk. 15361536 225225 345,600345,600 155,5155,5
2020
OP GroupOP Group 9085390853 90 min. 1x/wk.90 min. 1x/wk. 924924 6060 55,44055,440 24,9424,9488
AssessmentAssessment 9080190801 60 min. multi-axial60 min. multi-axial 120120 100100 1200012000 5,4005,400
Totals gross Totals gross * .45* .45
MeCare MeCare ContractsContracts
521,065521,065 234,4234,47979
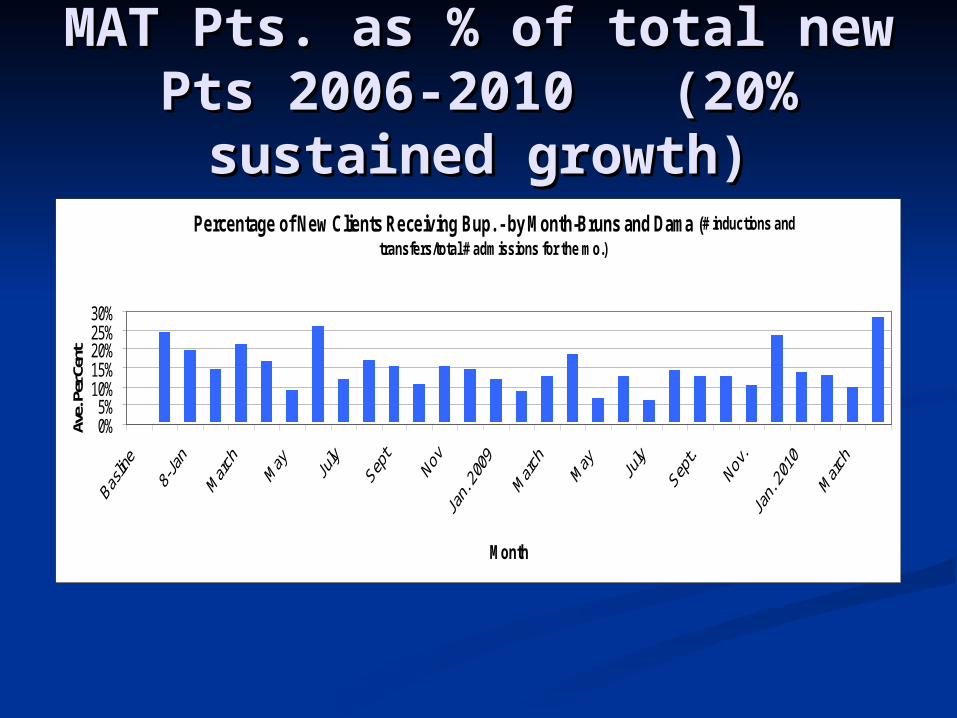
MAT Pts. as % of total new MAT Pts. as % of total new Pts 2006-2010 (20% Pts 2006-2010 (20%
sustained growth)sustained growth) Percentage of New Clients Receiving Bup. - by Month-Bruns and Dama (# inductions and
transfers/total # admissions for the mo.)
0%5%
10%15%20%25%30%
Month
Ave.
Per
Cen
t
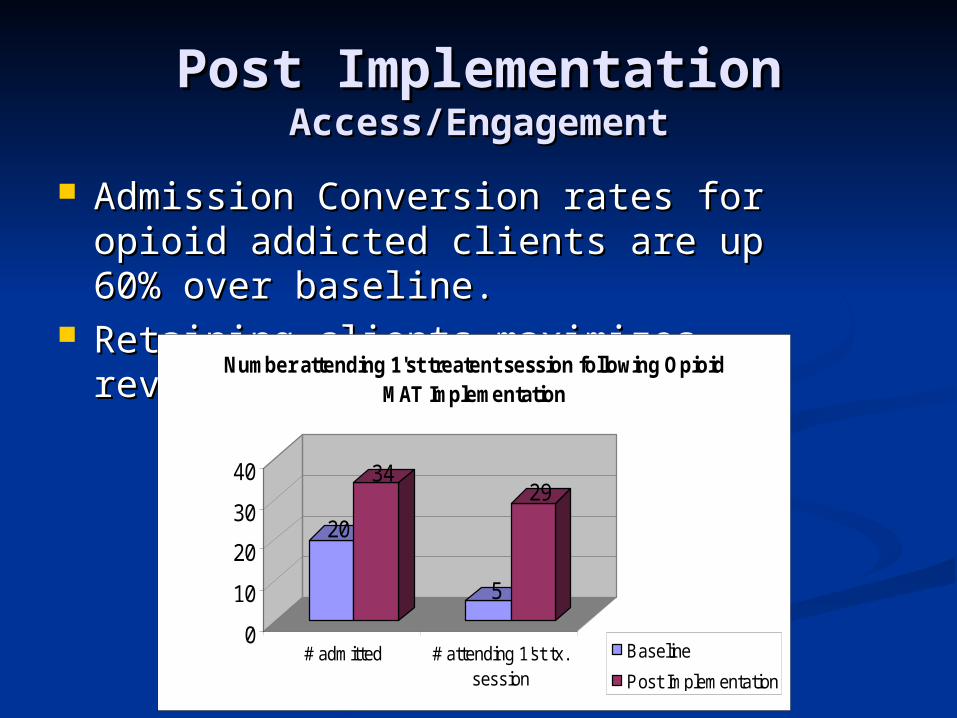
Post ImplementationPost ImplementationAccess/EngagementAccess/Engagement
Admission Conversion rates for opioid Admission Conversion rates for opioid addicted clients are up 60% over addicted clients are up 60% over baseline.baseline.
Retaining clients maximizes revenueRetaining clients maximizes revenue
20
34
5
29
0
10
20
30
40
# admitted # attending 1'st tx.session
Number attending 1'st treatent session following Opioid MAT Implementation
Baseline
Post Implementation
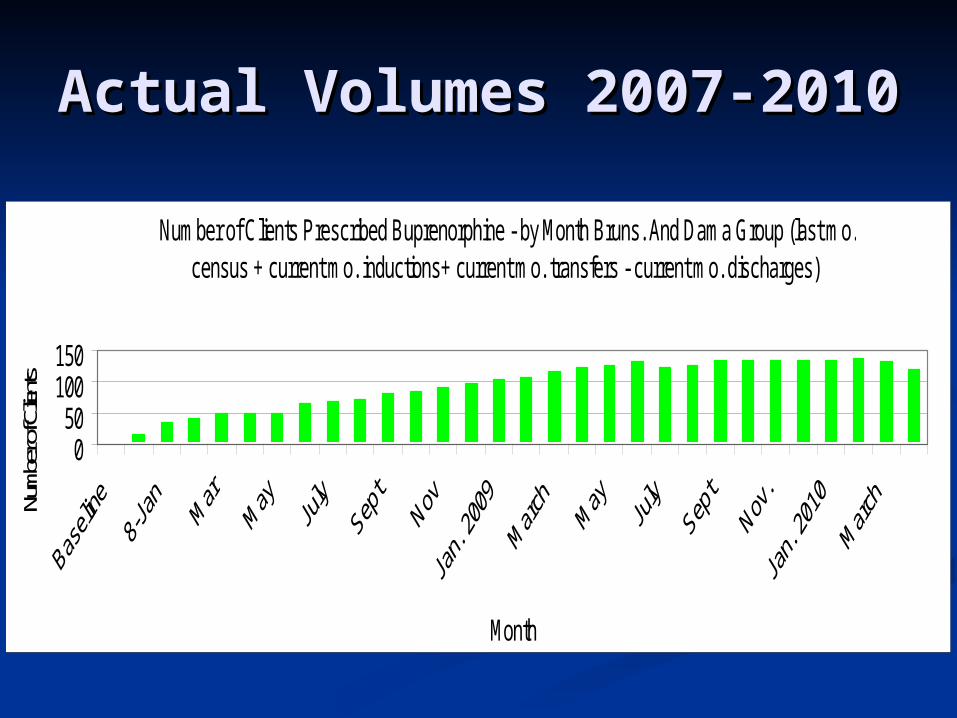
Actual Volumes 2007-Actual Volumes 2007-20102010
Number of Clients Prescribed Buprenorphine - by Month Bruns. And Dama Group (last mo. census + current mo. inductions+ current mo. transfers - current mo. discharges)
050
100150
Month
Numb
er of
Clien
ts
Post ImplementationPost ImplementationPit Falls (Keep workin’ it)Pit Falls (Keep workin’ it)
Access for new bup. pts. is decreasing Access for new bup. pts. is decreasing Bottlenecks in maintenance apt. Bottlenecks in maintenance apt.
schedule begin drive access for new schedule begin drive access for new patients.patients.
Deviation from practice standards to Deviation from practice standards to accommodate rapid paceaccommodate rapid pace Work-arounds that compromise pt. and Work-arounds that compromise pt. and
public safety.public safety.
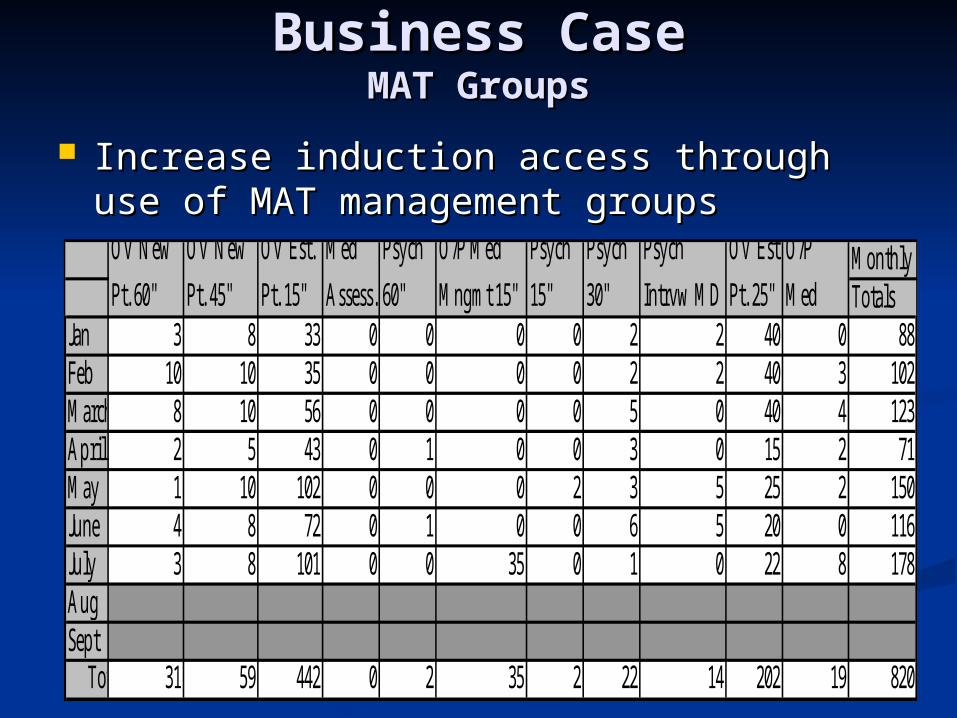
Business CaseBusiness CaseMAT GroupsMAT Groups
Increase induction access through use of Increase induction access through use of MAT management groupsMAT management groups
Monthly Totals
Jan 3 8 33 0 0 0 0 2 2 40 0 88Feb 10 10 35 0 0 0 0 2 2 40 3 102March 8 10 56 0 0 0 0 5 0 40 4 123April 2 5 43 0 1 0 0 3 0 15 2 71May 1 10 102 0 0 0 2 3 5 25 2 150June 4 8 72 0 1 0 0 6 5 20 0 116July 3 8 101 0 0 35 0 1 0 22 8 178AugSept Totals 31 59 442 0 2 35 2 22 14 202 19 820
Psych
30"
Psych
Intrvw MD
OV Est
Pt. 25"
O/P
Med
OV New
Pt. 60"
OV New
Pt. 45"
OV Est.
Pt. 15"
Med
Assess.
Psych
60"
O/P Med
Mngmt 15"
Psych
15"
Pt. Flow Analysis: Business Pt. Flow Analysis: Business CaseCase
for MAT Groupsfor MAT Groups Used PDCA cycles to pilot one group for 8 wks.Used PDCA cycles to pilot one group for 8 wks.
Better use of multidisciplinary team approachBetter use of multidisciplinary team approach Consistent application of standard of careConsistent application of standard of care
Replicate intervention with two 1.5 hour groups Replicate intervention with two 1.5 hour groups per week.per week. 2 groups per week takes 12 hours per month vs. 26.5 2 groups per week takes 12 hours per month vs. 26.5
hours per month for MD to see same case load hours per month for MD to see same case load individually.individually.
2 groups per week absorbs 112 encounters per 2 groups per week absorbs 112 encounters per month.month.
Increase monthly average from 8 to 16 inductions.Increase monthly average from 8 to 16 inductions. Increase monthly average from 2 to 7 psychiatric Increase monthly average from 2 to 7 psychiatric
evaluations.evaluations. Will result in increase revenues in the amount of Will result in increase revenues in the amount of
$41,000.00 per year-NET.$41,000.00 per year-NET.
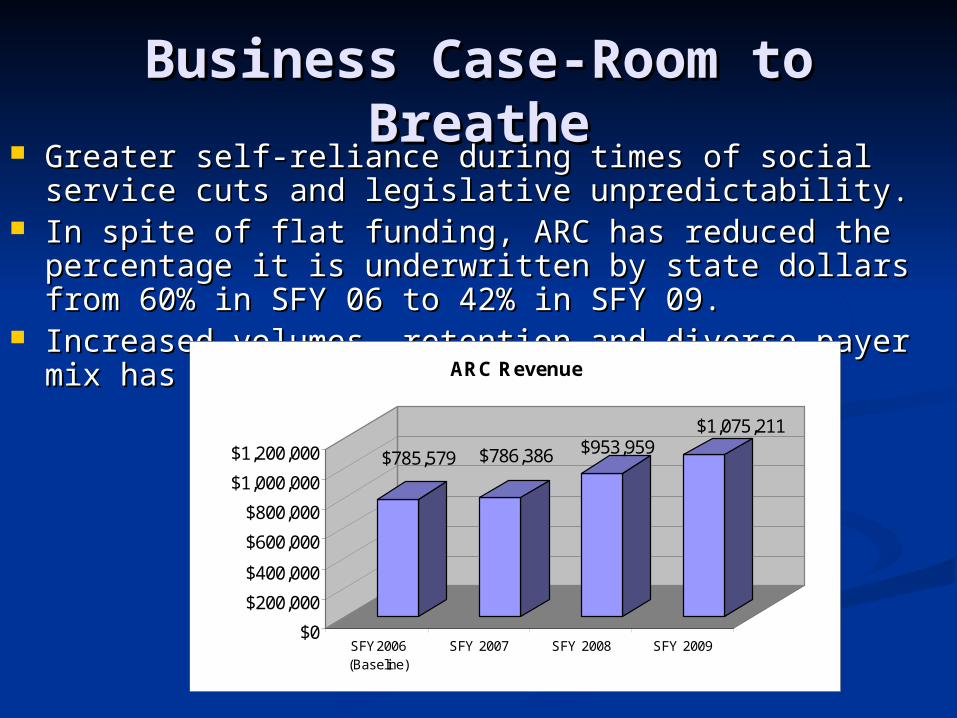
Business Case-Room to Business Case-Room to BreatheBreathe
Greater self-reliance during times of social service cuts Greater self-reliance during times of social service cuts and legislative unpredictability.and legislative unpredictability.
In spite of flat funding, ARC has reduced the In spite of flat funding, ARC has reduced the percentage it is underwritten by state dollars from percentage it is underwritten by state dollars from 60% in SFY 06 to 42% in SFY 09.60% in SFY 06 to 42% in SFY 09.
Increased volumes, retention and diverse payer mix Increased volumes, retention and diverse payer mix has dropped our cost 30%has dropped our cost 30%
$785,579 $786,386 $953,959$1,075,211
$0
$200,000
$400,000
$600,000
$800,000
$1,000,000
$1,200,000
SFY2006(Baseline)
SFY 2007 SFY 2008 SFY 2009
ARC Revenue
Marketing Through Leadership: Marketing Through Leadership: Community and Professional Community and Professional
EducationEducation Provided NIDA/CTN endorsed training Provided NIDA/CTN endorsed training
curricula to 125 participants in Maine curricula to 125 participants in Maine since 2009. (since 2009. (Rockland, Machias, Portland, Rockland, Machias, Portland, Lewiston) 8 hour training sponsored by Lewiston) 8 hour training sponsored by ATTC, Brown University and CCSME.ATTC, Brown University and CCSME.
Published Guide for the Published Guide for the Implementation of Medication Assisted Implementation of Medication Assisted Treatment. 2011 University of Treatment. 2011 University of Wisconsin–Madison, Center for Health Wisconsin–Madison, Center for Health Enhancement System Studies.Enhancement System Studies.
Marketing Through Leadership: Marketing Through Leadership: Community and Professional Community and Professional
EducationEducation Provided training for USM school of Provided training for USM school of
Nursing students. 2009, 2010, 2011Nursing students. 2009, 2010, 2011 Working actively with Maine DOC to Working actively with Maine DOC to
examine barriers to inmates’ access examine barriers to inmates’ access to FDA approved medications for to FDA approved medications for withdrawal and craving.withdrawal and craving.
CIT training annually. 40 hrs. CIT training annually. 40 hrs. training to local law enforcement.training to local law enforcement.
Payer/Provider Payer/Provider PartnershipsPartnerships
Support for rapid cycle change approach.Support for rapid cycle change approach. State and other payers want to know State and other payers want to know
barriers to MAT implementation.barriers to MAT implementation. AccessAccess FlexibilityFlexibility
Advocacy and CredibilityAdvocacy and Credibility Operational reliefOperational relief
Licensing regulationsLicensing regulations Incentives in Contracting are congruent with Incentives in Contracting are congruent with
4 AIMS4 AIMS Gold Status with Anthem, Diverse Payer MixGold Status with Anthem, Diverse Payer Mix





























