Embed Size (px)
Citation preview

CASE CONFERENCE addisonian crisis
Addisonian Crisis: Emergency Presentation of Primary Adrenal Insufficiency
[Frederick R, Brown C, Renusch J, Turner L: Addisonian crisis: Emergency presentation of primary adrenal insufficiency. Ann Emerg Med July 1991;20:802~806.]
INTRODUCTION Today's case involves a young man with severe vomiting and diarrhea
presenting with profound hypotension, tachycardia, and fever. Discussants are Richard Frederick, MD, Craig Brown, MD, Joseph Renusch, MD, and Lanny Turner, MD, from the Division of Emergency Medicine of the Uni- versity of Illinois College of Medicine at Peoria -- Saint Francis Medical Center.
CASE PRESENTATION Joseph Renusch, MD: A 21-year-old man developed vomiting, diarrhea, fe- ver, and rigors three days before admission. His appetite was poor, and had a decreased urine output. He had been taking two to four aspirins a day and a total of two to four 25-mg diphenhydramine capsules for the symptoms.
The patient became progressively weaker during the course of the illness and presented to the emergency department after a brief syncopal episode he experienced while attempting to rise to a standing position at home. He sustained no injuries.
His medical history was remarkable only for meningoencephalitis at age 11. His social history was negative for alcohol and drug use and homosex- ual contact. There was no recent travel and no exposure to chemicals, toxins, or persons with a similar illness. Initial family history from parents and a brother revealed no familial illnesses.
On arrival at the ED, the patient was alert and oriented but slow to answer questions. He had constant rigors and was incontinent of stool. Vital signs were blood pressure of 92/60 mm Hg; pulse, 160 and regular; respirations, 32; and rectal temperature, 40.5 C.
The patient's skin was hot and dry. His mucous membranes were dry, and he had bilateral conjunctival injection. Neck and chest examinations were unremarkable. There was no costovertebral angle tenderness to per- cussion. The abdomen was soft and diffusely tender with absent bowel sounds, but no other signs of peritoneal irritation were present. Examina- tion of the genitalia revealed a 1-cm-diameter ulcer with eschar on the dorsum of the right hemiscrotum. Rectal examination revealed liquid, green, guiac-negative stool. The prostate was normal. The extremities were cool and pale distally with poor capillary refill and thready pulses. There were no needle tracks. Neurologic examination was unremarkable. Initial laboratory values are shown (Figure 1). ECG showed sinus tachycardia without any sign of acute injury.
'Fluid resuscitation was begun with IV crystalloid. Vital signs after 6 L of fluid were systolic blood pressure of 82 mm Hg by Doppler; pulse, 140; and respirations, 20. No urine was obtained on bladder catheterization, and subsequent urine output was 8 mL/hr. IV antibiotic therapy was begun with ceftazidime, clindamycin, and ampicillin after cultures.
Question: What was the differential diagnosis at this point?
Richard Frederick, MD, FACEP Craig Brown, MD Joseph Renusch, MD Lanny Turner, MD Peoria, Illinois
From the Division of Emergency Medicine, University of Illinois College of Medicine at Peoria -- Saint Francis Medical Center, Peoria, Illinois.
Received for publication April 19, 1990. Revision received December 3, 1990. Accepted for publication January 7, 1991.
Address for reprints: Richard C Frederick, MD, FACER Emergency Medicine Residency Program, Saint Francis Medical Center, University of Illinois College of Medicine at Peoria, 530 Northeast Glen Oak Avenue, Peoria, Illinois 61637.
20:7 July 1991 Annals of Emergency Medicine 802/147

ADDISONIAN CRISIS Frederick et al
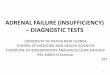
FIGURE 1. Initial laboratory values.
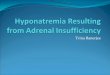
Richard Frederick, MD: The patient presented in frank clinical shock, and all etiologies of shock had to be con- sidered. Shock has traditionally been classified into three major categories: hypovolemic, cardiogenic, and vaso- genic {Figure 2). Although it is essen- tial to identify the initial insulting event causing the shock state, one needs to be aware that there is signif- icant overlap in the various classi- fications of shock. ~ For example, hy- povolemic shock and septic shock will reach a point at which signifi- cant negative inotropic function ex- ists. Also, at least 20% of people wi th acute myocardial infarctions and cardiogenic shock present ini- tially with hypovolemia. Thus, we must be cognizant of the fact that these divisions are somewhat artifi- cial in nature, t
Regarding the case under discus- sion, let us f irst cons ider hypo- volemic shock. There was no direct evidence of hemorrhagic shock in that the patient had a heme-negative stool. The nasogastric aspirate was also negative. The nasogastric tube should have been placed quite early in the course of the resusci ta t ion rather than when the patient arrived in the ICU. However, the patient still could have had an intraperitoneal or retroperitoneal bleed, perhaps from a ruptured great vessel or hemorrhagic pancreatitis. Plasma loss was much more likely.
The most obvious source for the patient's plasma loss was the hyper- emesis and diarrhea, which was re- vealed by history. However, other causes were excluded, including peri- tonitis from the various causes that can lead to a ruptured viscus. The ab- domen did not have signs of peri- toneal irritation. There was diffuse tenderness, and in the patient with some degree of lethargy, physica l findings can be somewhat blunted.
Endocrine causes for severe hypo- volemia include diabetes mell i tus, thyroid storm, and adrenal insuffi- ciency. Our patient was neither ac- idotic nor hyperglycemic, thus ruling out diabet ic ketoacidosis . He did have a fever, tachycardia, vomiting, and diarrhea, which are seen in thy- roid storm; however, this pat ient ' s tachycardia was not out of propor- tion to either his fever or his hypo- volemia. He also had no clinical find-
CBC White blood cells (differential: 32 ]ymphocytes,
12 monocytes, 33 bands, 22 segmented neutrophils) Hemoglobin Platelets
Electrolytes
18,700 x 109/L 14.7 g/dL 196,000 x 109/L
Sodium Potassium Chloride
CO 2
Arterial Blood Gases
140 mEq/L 4.7 mEq/L 99 mEq/L
15 mEq/L
Po2 Pco 2 pH
Serum Chemistry
84 rnm Hg
25 mm Hg 7.33
Glucose BUN Creatinine
CPK LDH SGOT (AST) Alkaline phosphatase Total bilirubin
Uric acid Serum myoglobin Serum ammonia Serum amylase
Urinalysis
83 mg/dL 34 mg/dL 6.5 mg/dL
1,918 units/L 366 units/L 84 units/L
99 units/L 0.6 mg/dL 10.8 mg/dL 2,285 ng/mL
.42 mol/L 48 units/L
Specific gravity
pH Protein Glucose WBC RBC Occult blood Bacteria
Casts
Stool leukocytes Stool ova and parasites
RPR ECG
1.019
5.0 500 mg/dL (3 +) Negative
10 to 50/high-power field 10 to 50/high-power field Large amount Large amount
1 to 5 coarse granular/high-power field
Positive Negative Nonreactive
Sinus tachycardia
ings of Graves' disease. These are not invariably present. Acute adrenal in- sufficiency or addisonian crisis can certainly present with fever, chills, headache, severe vomiting, and diar- rhea as well as marked orthostatic hypotension.
Let us also consider other causes of shock that should be at least briefly considered in this, pat ient . .When a patient presents acutely with shock,
rul ing out the obs t ruc t ive causes should be done in the initial primary survey. This patient's physical exam- inat ion revealed no ev idence for a tension pneumothorax, pericardial tamponade, or aortic dissection. Pul- monary embolus is always a possi- bility; however, a febrile presentation would be quite unusual. Regarding primary causes for cardiogenic shock, the pat ient did not have any ECG
1481803 Annals of Emergency Medicine 20:7 July 1991

ADDISONIAN CRISIS Freder ick et al
Hypovolemic Hemorrhagic
Trauma Gastrointestinal bleed Ruptured aortic aneurysm Obstetric bleed Hemorrhagic pancreatitis
Plasma loss Burns Peritonitis Pancreatitis Diarrhea Hyperemesis Diabetes mellifus Adrenal insufficiency
Cardiogenic Primary
Acute myocardial infarction Dysrhythmias Congestive heart failure Cardiomyopathies Congenital or valvular heart disease
Secondary (obstructive) Pericardial tamponade Pulmonary embolus Tension pneumothorax Aortic dissection
Vasogeoic (maldistribution) Septic shock Neurogenic shock Anaphylactic shock Drug overdose
changes cons i s ten t wi th an acute myocardial infarction. Although the creatinine kinase, LDH, and SGOT were elevated, the isoenzyme results were not available in the ED. The pa- tient was monitored on arrival, and no dysrhythmias were noted. Neither the physical examination, chest ra- diograph, nor ECG revealed any evi- dence that would be consistent with c o n g e s t i v e h e a r t fa i lure , cardio- myopathies , or valvular heart dis- ease.
The next major category is that of vasogenic shock or maldistr ibutive shock. The patient certainly demon- strated a clinical picture consistent with septic shock. The most likely focus for infection with his present- ing history was the gastrointestinal tract, a l though pyelonephri t is pro- ceeding to sepsis should also have been considered. The pat ient , al- though profoundly oliguric, did have p y u r i a , h e m a t u r i a , and a la rge amount of bacteria in the initial uri- nalysis. Appropriate cultures were done, and the patient was started on t r ip le -an t ib io t ic therapy. A severe
FIGURE 2. Classifications of shock.
bacterial gastroenteri t is leading to septic shock was high on the list of suspicious etiologies. Bacterial patho- gens that can present with severe hy- povolemia, fever, and rigors include Escherichia coli, Shigella, cholera, and occasionally Salmonella.
Anot he r t ox in -p roduc ing infec- tious syndrome to be considered is toxic shock syndrome, which could present with severe nausea and vom- iting, profound hypotension, fever, and rigors. Toxic shock syndrome would be u n u s u a l in a m a n and highly unusual without a history of nasal packing or antecedent staphy- lococcal infection.
In concentrating on the gastroin- t e s t i n a l and u r i n a r y t rac t s , one should not forget to look further for sites of infection, notably pulmonary and central nervous system. Initial chest radiography did not show pneu- monia. However, the patient was sig- nificantly dehydrated, and we have all seen cases in which pneumonia did not show up unt i l the pat ient was rehydrated. A spinal tap and blood cultures were done in the ICU to complete the septic workup. Ana- phylactic shock could present with a s imi l a r p ic ture , a l t hough hyper- pyrexia is usual ly not part of that presenting picture, and the history of a three-day antecedent illness would not usually be associated with ana- phylactic shock.
Last to be considered under the heading of vasogenic shock is drug overdose. A host of drugs can cause fever, in therapeutic doses as well as in overdoses, z A large number of drugs can cause hypotension, includ- ing barbiturates, chlorohydrate, alka- loids, ni t ra tes , ni t r i tes , iron, phe- nothiazines, tricyclics, and salicy- lates. Phenothiazine overdoses and salicylism, which can cause both hy- perpyrexia and hypotension, must be ruled out.
Mushroom poisoning can present wi th s imilar symptoms and some- what prolonged delayed course, al- t hough to m y knowledge , hyper- pyrexia is not a common finding in mush room poisonings. One might also anticipate an intervening latent period in the history, which we did not find. In addition, we had no his- tory of exposure or ingestion of any such toxin in a mushroom. Also, the patient presented on the last day of
March, which precedes mush room season in central Illinois by a full month.
Question: Please commen t on the initial management of this case in the ED.
Lanny Turner, MD: Given the sce- nario of a young man with severe gastrointestinal symptoms, fever, and syncope, the differential possibilities are vast. Dr Frederick has alluded to some likely possibilities for consid- eration, with which I concur. I be- lieve further possibilities with this patient might include heavy metal poisoning and in f lammatory bowel disease.
The generally aggressive approach taken with the patient, including vol- ume resuscitation, initiation of tri- valent antibiotic therapy, and a thor- ough search for metabolic etiologies, was appropriate. The patient's clini- cal picture was consistent with sep- tic shock. Although one could argue both for and against the early use of steroids, I agree with the empiric use of hydroeortisone phosphate 100 mg as was done in the ICU. Although at present corticosteroids are controver- sial, one could make an argument for their use in refractory shock.
Question: Describe the classic pre- sentation of addisonian crisis.
Craig Brown, MD: Addisonian crisis is usually precipitated by the addi- tion of a stressful event, usually in- fection or surgery, in someone whose cortisol output is low and who is un- able to increase output to meet the additional demand. 3 Other causes in- clude hemorrhagic or malignant de- struction of the adrenal glands and the abrupt t e rmina t ion of steroid therapy. Typical precipitating factors are t rauma, surgery, infection, alco- hol withdrawal, and excessive fluid and sodium loss through sweating or diarrhea.
Pa t i en t s w i th addisonian crisis (acute adrenal insufficiency) usually present with nonspecific complaints but with a rapid and nonspecific de- terioration that may lack an obvious underlying etiology. The nonspecific nature of the symptoms frequently causes the diagnosis to be missed or delayed. 4 Symptoms include leth- argy, weakness, and weight loss in more than 90% of cases. Fever, diar- rhea, nausea, and vomiting, which
20:7: July 1991 Annals of Emergency Medicine 804/149

ADDISONIAN CRISIS Frederick et al
may be intractable, are almost al- ways present. Abdominal pain is common and may be so severe as to be confused with an acute abdomen. Flank and epigastric pain may be present with an acute abdomen, and also may be present with acute adre- nal hemorrhage.
Hypotension varying from mild or- thostasis to frank shock is usually present and may be intractable. Hy- potension is due to volume depletion secondary to aldosterone deficiency. Occasional ly , pa t ients in adrenal crisis are normotensive because their precrisis blood pressure was ele- vated.~ Tachycardia is usually pres- ent, as are or thostat ic changes in blood pressure and heart rate. Confu- sion, stupor, or even coma may be present. Evidence of intercurrent in- fection is common. Cutaneous and/ or mucosal hyperpigmentation may be present if the adrenal crisis is an exacerbation of an Underlying pri- mary chronic insufficiency. This oc- curs in approximately 50% of pa- tients. 4
Question: What are the causes of acute adrenal insufficiency in Ad- dison's disease?
Dr Frederick: There are several causes of Addison's disease, includ- ing auto immune adrenalitis, infec- tion, metastatic disease, drugs, and hemorrhage. 6
The last cause, hemorrhage, is rare but well known as Waterhouse-Frid- erichsen syndrome, which is second- ary to sepsis and presents wi th a t r iad of h y p o t e n s i o n leading to shock, hemorrhagic diathesis with purpura, and complete adrenal fail- ure. H e m o r r h a g e of the adrenal glands can also occur wi th anti- coagulant therapy and secondary to direct trauma of the adrenal glands. The most common cause of adrenal insufficiency today is autoimmune adrenalitis, accounting for 66% of pa- tients in one series. 7 This can be spo- radic or familial in occurrence, and it can involve other endocrine organs such as thyroids, parathyroids, islet cells, and ovaries. There is a pro- cedure available to test the serum for au to immune antibodies, and it is positive in approximately 70% of the cases. 6
In fec t ions are sti l l a c o m m o n cause. However, tuberculosis, which in 1930 accounted for 70% of the
cases of Addison's disease, is much less common today. Fungal diseases, especially histoplasmosis, are the other main infectious etiologies. Re- cently, there have been reports of in- creased adrenal insufficiency in AIDS patients probably secondary to cyto- megalovi rus infect ions, a l though other authors believe that the inci- dence of clinically significant adrenal insufficiency in AIDS is quite un- common, s
Metas tases is the other major cause. 9 One study found involve- ment of the adrenal glands in meta- static cancers in 27% of the patients autopsied. It is, however, very rare for the signs and symptoms of adre- nal insufficiency to precede the dis- covery of the primary malignancy. Drugs are a rare cause, as with hem- orrhage, but four drugs - keto- conazole, a broad-spectrum antifun- gal agent; etomidate, an IV anes- thetic; rifampin, and cyproterone acetate - are particularly suspect. 6
Question: How do you make the di- agnosis of Addison's disease?
Dr Brown: The most important as- pect of diagnosing addisonian crisis is a thorough history and physical ex- amination plus a high index of suspi- cion of Addison's disease. The classic laboratory findings in adrenal insuffi- ciency are hyponatremia {seldom less than 120 mEq/dL), hyperkalemia {sel- dom more than 7 mEq/dL), hyper- calcemia, azotemia, and a mild meta- bolic acidosis. 4 A random serum cor- tisol level of less than 10 >g/dL during stress is suggestive of Ad- dison's disease, and less than 5 btg/dL is virtually diagnostic. Twenty-four- hour urine cortisol and 17 hydroxy- corticoids are also depressed. Plasma ACTH levels are elevated in primary adrenal insufficiency but depressed in secondary adrenal insufficiency and steroid therapy. 5
The hyponatremia is secondary to cortisol deficiency, which results in increased secretion of antidiuretic hormone with consequent inability to excrete free water. Mineralocorti- cal deficiency results in decreased al- dosterone production, which causes sodium depletion and potassium and hydrogen ion retention. The hema- tocrit and blood urea nitrogen are in- creased secondary to volume deple- tion.
ECG abnormalities are seen in ap-
proximately 50% of patients with p r imary adrenal insuf f ic iency , lo These abnormalities, which occur more frequently in women, include sinus bradycardia; low voltage, low, or inverted T waves; prolonged QT c i n t e r v a l s ; and s igns of h y p e r - kalemia.4, lo
Plain radiographs and computed tomography may show calcifications in one or both adrenals. Adrenal cal- cifications strongly suggest adrenal tuberculosis and exclude idiopathic adrenal atrophy.
The diagnosis of acute adrenal in- suff ic iency is mos t l ikely to be missed when the disorder occurs in association with trauma and alcohol withdrawal and in the postoperative period.
In the stable patient who is not in crisis, additional tests may be run to document adrenal insufficiency and determine if it is primary or second- ary. An ACTH stimulation test may be run in which a baseline cortisol level is drawn 30 and 60 minutes later. In a pat ient with normal ly funct ioning adrenals, the cortisol leve l s h o u l d r i se by 16 to 18 ixg/dL.3,~ 1 With adrenal insufficiency, the baseline levels fail to rise. Once primary adrenal insufficiency has been ruled out, secondary adrenal in- sufficiency can be diagnosed using the insulin hyperglycemia test or the metyrapone test. Both these tests should be done only after primary in- sufficiency has been ruled out.
In insulin-induced hypoglycemia, insulin is given to make the patient s y m p t o m a t i c a l l y h y p o g l y c e m i c (blood glucose, less than 40}. In a nor- mal person, the plasma cortisol will rise to more than 18 ~g/dL. This test is contraindicated in the elderly, in patients with cerebrovascular or car- diovascular disease, and in those w i t h s e i z u r e d i so rde r s . In the metyrapone test, patients are given 2 to 3 g metyrapone orally at midnight; the following morning, the plasma ll-deoxycortisol level is determined. A level of more than 7 btg/dL is a nor- Inal r e s p o n s e . 11
Question: What is the emergency treatment of addisonian crisis?
Dr Turner: The mainstay of treat- ment is the administration of cor- tisol (hydrocortisone) because of its mineralocorticoid and glutocorticoid effects, which are both critical in the
150/805 Annals of Emergency Medicine 20:7 July 1991

ADDISONIAN CRISIS Frederick et al
treatment of this disease. 12 This is accomplished by giving hydrocor- tisone sodium phosphate in an initial dose of 100 mg IV, which is repeated every six hours for 24 hours. If at that point progress is satisfactory, the dose is reduced to 50 mg every six hours on the second day and then tapered as an oral dose thereafter. 13
Other measures are more general and supportive, including the inser- tion of large-bore IV catheters and the early initiation of central venous moni tor ing to assess true volume status. A blood sample should be drawn for glucose, cortisol, and elec- trolyte determinations as well as re- nal function test, CBC, and plasma ACTH measurements. In addition, wi th rep lacement of vo lume and electrolyte deficits, hypoglycemia should be corrected if present, and the level of dehydration should be determined carefully because fluid deficits can exceed 20% of total body weight in the acute setting. 14 Ini- tially, this could be approached by using 5% dextrose in normal saline at a rate of 500 mL/hr for the first four hours.
Subsequent therapy should be de- termined by blood pressure, serum electrolytes, and urinary output. Se- rum potassium may be increased ini- tially, but there frequently is a deficit of total body potassium; replacement of therapy should be started shortly after reh3rdration and cortisol admin- istration is initiated. It is worth not- ing that vasopressors are frequently ineffective unless they are preceded by adequate glucocorticoid and fluid therapy.It A careful search should be made for underlying problems, which most frequently are of an infectious nature. The concomitant endocrine problems of hypothyroidism or pan- hypopituitarism should be searched for carefully as well.
When one is in a subacute setting and resuscitative efforts are well un- der way, it would be ideal to do an ACTH stimulation test before glu- cocorticoid therapy is begun. This is
frequently not possible, as was the case with this patient.
HOSPITAL COURSE The patient was admitted directly
to the medical ICU, fluid resuscita- tion was begun and a Swan-Ganz catheter was placed. Shortly after ad- mission, old records on microfilm re- vealed that the patient's brother had an admission for schizophrenia and primary Addison's disease.
After receiving 6 L of fluid, the pa- tient's pressure increased to 120/64 mm Hg. Over the next two hours, it dropped to 90 mm Hg. He developed increasing respira tory distress; a chest radiograph revealed bilateral pu lmona ry inf i l t ra tes cons i s ten t with. pulmonary edema or acute res- piratory distress syndrome. Fluids were discontinued; he was given fu- rosemide, but his systolic blood pres- sure dropped to 58 mm Hg. At this point, fluids were resumed, and the patient was started on dopamine and dobutamine.
The patient was given 100 mg hy- drocortisone IV, four hours after ad- mission. He also received additional doses every six hours during his hos- pital course.
The patient had continuing respi- ratory distress. During an attempt at intubation, he vomited and aspirated significant gastric contents; he sub- sequently became bradycardic and went into electromechanical disso- ciation followed by ventricular fi- brillation. He underwent prolonged CPR including manual compressions, and after 30 to 40 minutes normal si- nus rhy thm was restored. He re- mained hypotensive.
The patient was placed on a ven- tilator with 100% O2, but because of poor oxygenation, he required pro- gressively increasing peak end-expi- ratory pressure. He was treated with high-dose dopamine, dobutamine, and crystalloids as well as blood, al- bumin, and fresh-frozen plasma. De- spite this, his pressure remained low, and his hypoxia continued.
The patient's Swan-Ganz readings continued to show low wedge and pulmonary artery diastolic pressures. An echocardiogram ruled out cardiac tamponade and showed slightly de- pressed ventricular function. A lum- bar puncture was unremarkable. Se- rum myoglobin was 2,285 (normal, 6 to 85 ng/mL), creatinine phospho- kinase was 2,251 with an MB fraction of 2%, and the remainder of the labo- ratory values were unremarkable.
Ant ib io t ics were cont inued, as were high-dose dopamine and dobut- amine. The patient arrested again but could not be resuscitated despite a prolonged effort. Time from admis- sion to the medical ICU to death was approximately ten hours. The plasma cortisol level of 2 Ixg% (normal, 6 to 25 ~g%) was not known until the next day.
REFERENCES t. Kreis DJ, Bave AE: Clinical Management of Shock. Baltimore, University Press, 1984, p 39-83, 118.
2. Lipsky BA, Hi r schmann JV: Drug fever. JAMA 1981;245:851-854.
3. Tzagoumis M: Acute adrenal insufficiency. Heart Lung 1978;7:603 609.
4. Rusnok RA: Adrenal and pi tu i tary emergencies . Emerg Med Clin North Am 1989;7:903-925.
5. Gilliland PF: Endocrine emergencies. Postgrad Med 1983;74:215-2).7.
6. Kannan CR: Diseases of the adrenal cortex. Disease a Month 1988;34:604-673.
7. Nerup J: Addison's disease - Clinical studies, a re- port of 108 cases. Acta Endoerin 1974;76:127q41.
8. Hilton CW, Harrington PT, Prasad C, et al: Adrenal insufficiency in the acquired immunodefieiency syn- drome. South Med J 1988;81:1493-1495.
9. Kung AW, Pun KK, Lamb K, et al: Addisonian crisis as presenting factor in malignancies. Cancer 1990;65: 177-179.
10. Surawicz B, Mangiardi ML: Electrocardiogram in endocrine and metabolic disorders. Cardiovasc Clin 1977~8:243-266.
ll. Greenspan F8, £oshon PS: Basic and Clinical Endo- crinologJa Norwalk, Connecticut, Appleton & Lang, 1986, p 56-58.
12. Williams GH, Dluky RG: Diseases of the adrenal cortex, in Wilson GD, Braunwald E, Issdbacher KG, et al [edsJ: Harrison Principles of internal Medicine, ed 12. New York, McGraw-Hill, 1991, p 1713-1735.
13. Eisenberg MS, Copass MK: Endocrinologic disor- ders, in Emergency Medicine Therapy, ed 3. Phila- delphia, WB Saunders, 1988, p 83-85.
14. Ho MT, Saunders CE: Current Emergency Diagnosis and Treatment, ed 3. Norwalk, Connecticut, Appleton & Lang, 1990, p 573-575.
20:7: July 1991 Annals of Emergency Medicine 806/151