-
8/11/2019 ADHD Web
1/68
ATTENTION DEFICIT
HYPERACTIVITY DISORDERIn Chi ldren & Ado lescents
-
8/11/2019 ADHD Web
2/68
What is ADHD?The Current Clinical View
A disorder featuring age-inappropriate : Inattention
Poor persistence of responding Impaired resistance to
distraction, Deficient task re-engagement following disruption
Hyperactivity-Impulsivity(Disinhibition) Impaired motor
inhibition, Poor sustained inhibition Excessive and often
task-irrelevant motor and verbal behavior Restlessness decreases
with age, becoming more internal, subjective by
adulthood
Most cases are developmental and involve delays in therate at
which these two traits are maturing
Some cases are acquired (20%+; mainly males) These may represent
pathology and may differ in severity, recovery, &
possibly treatment response
-
8/11/2019 ADHD Web
3/68
Essential Features
ADHD presents as impairment in:
Persistence
Resistance to distraction Working memory
-
8/11/2019 ADHD Web
4/68
Persistence
ADHD Individuals do not have problems withsuch perceptual
aspects of attention as:
arousal or alertness
focus or selective attention
span of apprehension or divided attention
Rather have an inability to sustain actiontoward a goal for an
adequate period of timewhich is a motor problem
Persistence is on the motor side of attention, itis an output
disorder.
Output is the problem
Most people think of attention as an inputproblem: how you
perceive, select filter andprocess information
-
8/11/2019 ADHD Web
5/68
Resistance to Distraction Related to persistence: opposite sides
of the
same coin.
If you can persist it is because you can resist
distraction; If you can resist distraction you
can persist: One requires the other
Not a perception problem, ADHD kids are notoverly perceptive
they do not perceive
distractions any better the difference is that
they respond to the distracting events
Most of us are able to inhibit our responses todistracting
events, ignore them even though
we detect them.
ADHD is not a problem of perception but
inhibition
-
8/11/2019 ADHD Web
6/68
Working Memory
Once distracted ADHD individuals are far lesslikely to return to
the original goal or task
task re-engagement is a major problem for
this population
This is modulated by working memory:information held in mind
that guides us toward
a goal.
People with ADHD are likely to have serious
difficulties with working memory. Once distracted they are gone,
off on another
task
-
8/11/2019 ADHD Web
7/68
Inattention Symptoms (DSM-IV)Failure to give close attention to
details
Difficulty sustaining attention
Does not seem to listen
Does not follow through on instructions
Difficulty organizing tasks or activitiesAvoids tasks requiring
sustained mental effort
Loses things necessary for tasks
Easily distractedForgetful in daily activities
Symptoms must occur Often or more frequently
-
8/11/2019 ADHD Web
8/68
Hyperactive-Impulsive SymptomsFidgets with hands or feet or
squirms in seat
Leaves seat in classroom inappropriately
Runs about or climbs excessively
Has difficulty playing quietly
Is on the go or driven by a motorTalks excessively
Blurts out answers before questions arecompleted
Has difficulty awaiting turn
Interrupts or intrudes on others
Symptoms must occur Often or more frequently
-
8/11/2019 ADHD Web
9/68
DSM-IV Criteria for ADHD Manifests 6+ symptoms of either
inattention or
hyperactive-impulsive behavior
Symptoms are developmentally inappropriate
Have existed for at least 6 months
Occur across settings (2 or more) Result in impairment in major
life activities
Developed by age 7 years
Are not better explained by another disorder,e.g. Severe MR,
PDD, Psychosis
3 Types: Inattentive, Hyperactive, or Combined
-
8/11/2019 ADHD Web
10/68
ADHD Varies by SettingBetter Here: Worse Here:
Fun Boring
Immediate Delayed Consequences
Frequent Infrequent Feedback
High Low Salience
Early Late in the Day
Supervised Unsupervised
One-to-one Group Situations
Novelty Familiarity
Fathers Mothers
Strangers Parents
Clinic Exam Room Waiting Room
-
8/11/2019 ADHD Web
11/68
Prevalence (United States) 7-8% of children (using DSM-IV) (~3-4
million) Varies by sex, age, social class, & urban-rural
3:1 Males to females in children (5:1 in clinical samples)
Somewhat more common in middle to lower-middle classes More common
in population dense areas
No evidence for ethnic differences to date that areindependent
of social class and urban-rural
-
8/11/2019 ADHD Web
12/68
Co-Occurring DSM-IV Disorders More than 80% have one additional
disorder
More than 60% have two additional disorders Oppositional Defiant
Disorder (Average of 55%) Conduct Disorder (Average of 45%) Anxiety
Disorders (20-35%) Major Depression (25-35%) Bipolar Disorder
(0-27%; likely 6-10% max.)
(97% of those Diagnosed w/ Bipolar also haveADHD)
-
8/11/2019 ADHD Web
13/68
Medical Risks Sleep problems (39-56%); mainly delayed
onset and greater night waking leading toshorter sleep time
Developmental Coordination Disorder (50+%) Reduced Physical
Fitness, Strength, &
Stamina (using physical fitness tests) Accident Proneness
57%+
1.5 to 4x risk of injuries (greater in ODD) 3x risk for
accidental poisonings
Due to Impulsivity, risk-taking, impaired coordination,
oppositionality, and poor parental monitoring
-
8/11/2019 ADHD Web
14/68
Causes of ADHD
Disorder arises from multiple causes All currently recognized
causes fall in the
realm of biology (neurology, genetics)
Causes may compound each other
Common neurological pathway for ADHDappears to be the areas of
the braincontrolling Executive Functions and
Physical Activity (Smaller / LessDeveloped)
Social causes have poor evidence
-
8/11/2019 ADHD Web
15/68
Acquired Cases: Prenatal
Maternal smoking in pregnancy (odds 2.5) Maternal alcohol
drinking in pregnancy (same)
Prematurity of birth, especially if brain bleeds(45%+ have
ADHD)
Total increased pregnancy complications
Maternal high phenylalanine levels in blood (?)
High maternal anxiety in second trimester (?)
Cocaine/crack exposure not a risk factor aftercontrolling for
the above factors
-
8/11/2019 ADHD Web
16/68
Acquired Cases: Post-Natal (7-10%)
Head trauma, brain hypoxia, tumors, or infection
Lead poisoning in preschool years (0-3 yrs.)
Survival from acute leukemia (ALL)
Treatments for ALL cause brain damage
Post-natal Streptococcal Bacterial Infection triggers
auto-immune antibody attack of basal ganglia
Post-natal elevated phenylalanine (dietary amino
acid related to PKU) Prenatalhyperactivity
Post-natalinattention
-
8/11/2019 ADHD Web
17/68
HeredityFamily Studies
Familial Expression of ADHD:
- 25-35% of siblings
- 78-92% of identical twins- 15-20% of mothers- 25-30% of
fathers
- If parent is ADHD, 20-54% of offspring
(odds 8+)
-
8/11/2019 ADHD Web
18/68
HeredityTwin Studies Heritability (Genetic contribution)
57-97% of individual differences (Mean 80%+)
(91-95%+ using DSM criteria)
Shared Environment (common to all siblings)
0-6% (Not significant in any study to date)
Unique Environment (events that happenonly to one person in a
family)
15-20% of individual differences
(but includes unreliability of measure used toassess ADHD)
-
8/11/2019 ADHD Web
19/68
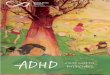
Etiologies of ADHDFrom Joel Nigg (2006), What Causes ADHD?
HeritableLBW
FASD
Lead (high)
Smoking
Perinatal
Other (Toxins)
LBW
FASDLead
Smoking
Perinatal
Other
Heritable (Genetics)
ADHD E l ti C
-
8/11/2019 ADHD Web
20/68
ADHD Evaluation: CoreConsiderations
Are the symptoms of inattention, impulsiveness, and
overactivity, present. MOST Importantly Is there clearevidence
of an impulsive style?
Is there evidence that these symptoms significantlyinterfere
with the childs functioning both at school and athome?
Did these symptoms have a reasonably early onset? (Ifnot, is
there a good explanation?).
Have these symptoms been an enduring and consistentfeature of
the childs behavior throughout theirdevelopment and in the majority
of contexts?
Is there evidence that the child wishes to perform well
butcannot?
Are there better explanations for the underachievement?
Is there a pattern or specific triggers to the
problembehaviors?
-
8/11/2019 ADHD Web
21/68
-
8/11/2019 ADHD Web
22/68
Psychodiagnostic Evaluation A psychodiagnostic Evaluation may be
necessary if the
assessment produces mixed/inconsistent results or hasuncovered
possible evidence of any of the following:
Suicidality
Significant Developmental Delays
Intellectual limitations
Learning disabilities
Serious Psychiatric disturbance
Significant family problems
Other reasons to refer for testing:
Child was moderately to severely premature
Prenatal exposure to toxins especially ETOH & Nicotine
Low birth weight Complicated pregnancy and/or birth
Reports that child had trouble grasping concepts/acquiring
newskills
Reports that child has trouble with major academic subjects
evenwhen attentive.
-
8/11/2019 ADHD Web
23/68
Ruling out Depression
Later onset than ADHD
Usually preceded by excessive anxiety
Not uncommon to have both as a result of thenegative outcomes
due to ADHD behaviors.
Must treat both
When comorbid, associated with a 4x increasein suicidal ideation
and 2x increase in attempts
Appears to be connected to same genesassociated with ADHD.
Best differential: EARLY HISTORY
-
8/11/2019 ADHD Web
24/68
Ruling Out Anxiety
Onset later than ADHD
Associated with a particular event or inaccordance with a time
pattern (anniversary).
Restlessness is not a primary manifestation ofAnxiety (usually a
habit, style, or boredom)
Usually characterized by panic or dread alongwith worry.
Best measure for presence of anxiety is childsreport (parents
and teachers under report).
-
8/11/2019 ADHD Web
25/68
Ruling Out PTSD
Must look closely at developmental and earlyschool history.
PTSD will stem from a specific event
Children with ADHD are at greater risk forPTSD from abuse and
risky behaviors.
-
8/11/2019 ADHD Web
26/68
Ruling Out Bipolar Disorder
Childhood BPD manifests as severe andchronic irritability
(rather than episodic mania)
Also characterized by Disjointed thinking,
capricious mood, destructiveness, anddysphoria.
BPD usually starts as ADHD in childhood
ADHD itself does not develop into BPD
One-way Comorbidity
3-6% of ADHD have BPD 80-97% of BPD have ADHD
-
8/11/2019 ADHD Web
27/68
Ruling Out ODD
In many cases ADHD is at the root of ODD
There is a high degree of co-occurrence
Early onset of ADHD symptoms is thedifferential
-
8/11/2019 ADHD Web
28/68
Treating
ATTENTION DEFICIT HYPERACTIVITYDISORDER
In Chi ldren & Ado lescents
-
8/11/2019 ADHD Web
29/68
Current Perspective
ADHD creates a kind of Myopia for future eventsor Time
Blindness.
ADHD individuals live in the Moment
ADHD is a Disorder of: Performance, not skill Doing what is
known, not knowing what to do
The when & where, not the how or what
Using representations of the past at the appropriateplace &
time (Point of Performance)
ADHD is better characterized as an IntentionDeficit
-
8/11/2019 ADHD Web
30/68
ADHD & Executive Functioning
Executive Functioning is responsible for twotypes of sustained
attention (SA): Contingency-shaped (Externally maintained)
Video Games
Goal-directed (Internally guided & motivated)
Homework Goal-directed (SA) is impaired in ADHD
individuals which creates problems with: Delayed responding
& intrinsic motivation Doing the opposite of what is suggested
in sensory
fields Time, waiting, delays, and future orientation Problem
solving, strategy development, & flexibility
Increases in complexity with age & development
-
8/11/2019 ADHD Web
31/68
Treatment Implications
Teaching skills is ineffective (As is insight) Treatment must
occur at the point of performance.
Medications are likely to be essential for most butnot all
cases.
Diminished capacity does not excuse accountability(The problem
is time and timing not consequences).
Behavioral treatment is essential but doesgeneralize or endure
after removal.
Treatment success depends on the compassion andwillingness of
others to make accommodations.
Maintaining a Chronic Disability perspective ismost
effective.
-
8/11/2019 ADHD Web
32/68
Unproven / Disproved Therapies
Elimination Diets: Sugar, Additives, etc. (Weak
Evidence) Megavitamins, Anti-oxidants, Minerals: (No strong
evidence or disproved)
Sensory Integration Training (Disproved)
Chiropractic Skull Manipulation (No Evidence) Play /
Psychotherapy (Disproved)
Neurofeedback (Experimental)
Cognitive Self-Control Therapies (Effective in Clinic)
Social Skills Training (Effective in Clinic Setting) Better for
Inattentive (SCT) Type and anxious cases
-
8/11/2019 ADHD Web
33/68
Empirically Proven Treatments Parent Education
Psychopharmacology Parent Training in Child Management
65-75% of Children under 11 respond
25-30% of Adolescents show reliable changes
Family Therapy for Adolescents:
Problem-Solving and Communication Training
30% show change (best combined with BMT)
Teacher Education
Train Teachers in Classroom Bx Management
Special Ed (IDEA, 504) Regular Physical Exercise
Residential Treatment (5-8%)
Parent Family Services (25+%)
Parent/Patient Support Groups
-
8/11/2019 ADHD Web
34/68
Managing ADHD
Time is critical: reduce delays Externalize a many processes as
possible:
Time (Clocks, Timers, Calendars, PDAs etc.)
Important information (Lists, reminders, instruction
cards, etc.) Motivation (Token economy, tangible rewards)
Problem Solving (use paper and pencil or dry eraseboard)
Give immediate feedback Increase frequency of consequences
Increase accountability to others
Use salient & artificial rewards
-
8/11/2019 ADHD Web
35/68
General Recommendations
Change rewards periodically Minimize talking, maximize
communicative
touch Corollary: Act dont Yak
Maintain a sense of humor Emphasize rewards over punishments
(reward
first)
Anticipate problem situations and make a plan Keep a sense of
priorities (pick your battles)
Hold to the perspective of ADHD as a Disability
Be forgiving (of child, self, and others)
-
8/11/2019 ADHD Web
36/68
Give Effective Commands Initially give heavy praise to high
compliance commands
Dont use questions, use Imperatives Use eye contact and
touch
Have child recite request
Break complex tasks into simpler ones
Make chore cards for Multi-Step tasks List all steps involved on
a 3x5 card
Stipulate the time period on the card
Reduce time delays for consequences
Make use of Timers at the Point of Performance
Avoid assignment of multiple tasks all at once
Praise initiation of compliance
Provide rewards throughout the task
Have child evaluate their performance at the end
-
8/11/2019 ADHD Web
37/68
Time-Out Target time-out to focus on one problem
Act quickly after infractions Violations of household rules get
instant time out
Immediate commands: Give Command ( count backwards from 5)
Give Warning with raised voice (repeat count of 5) Initiate
time-out
Release from time-out contingent on: Completion of minimum time
period (1-2 minutes/year of age)
Becoming quiet
Consenting to command
Reward next good behavior
Best to use Bedroom for Time-out Remove all major play
activities (Sanitize)
-
8/11/2019 ADHD Web
38/68
Psychopharmacology
-
8/11/2019 ADHD Web
39/68
Stimulant Medications These are the most well studied drugs in
psychiatry
In use for over 40 years Over 350 studies
Thousands of cases
Stimulant Response Rate
Ritalin (Methylphenidate) 77%
Adderall (Amphetamine) 74%
Dexedrine
(Dextroamphetamime)73%
Trying All 90%
Stimulants:
-
8/11/2019 ADHD Web
40/68
Stimulants:Behavioral Effects
Increased concentration and persistence
Decreased Impulsivity & hyperactivity
Increased work productivity
Better emotional control
Decreased aggression and defiance
Improved compliance
Better working memory & internalized language
Improved handwriting and motor coordination
Improved self-esteem
Decreased punishment
Improved peer acceptance and interactions
Better awareness in sports
Improved driving performance
Sti l t Sid Eff t
-
8/11/2019 ADHD Web
41/68
Stimulants: Side Effects Most tolerate well
5% discontinue due to negative effects
Side effects are dose dependent Most common side effects:
Insomnia (50% +) Loss of Appetite (50% +) Headaches (20-40%)
Stomach Aches (20-40%)
Irritability, tearfulness (
-
8/11/2019 ADHD Web
42/68
Stimulants:Common Myths
Addictive when used as prescribed No, Must be inhaled or
injected
Over Prescribed 7.8% prevalence rate, only 4.3% on
stimulants
Creates Aggressive, Assaultive Behavior
No, decreases aggression and antisocial actions
Increases the likelihood of Seizures Only at very very high
doses
Causes Tourettes Syndrome
Can increase tics in 30%; decreases it in 35% Increases risk of
later substance abuse
No, 14 studies have found no such result, some found that
itdecreased risk if continued throughout teens
St tt
-
8/11/2019 ADHD Web
43/68
Strattera
Selective Norepinepherine reuptake inhibitor Not Schedule II; no
abuse potential
Effective for children, adolescents, and adults
Equal efficacy with Methylphenidate with
previously unmedicated cases (75% positiveresponse)
Slightly lower efficacy with those previously onstimulants (55%
positive response)
Sustained response for up to 3 years Increasing improvement over
time
Can be given once daily (morning) or split
(am/pm)
-
8/11/2019 ADHD Web
44/68
Benefits of Strattera
Reduces ADHD, ODD, & aggression
Reduces internalizing symptoms
Increases school productivity
Improved peer social behavior
Improved self-esteem Improved parent-child relations
Improved dry nights among bed-wetters
Better morning after behavior Less insomnia and faster onset of
sleep thanMethylphenidate
No emotional blunting
-
8/11/2019 ADHD Web
45/68
Academ ic and Occupat ional
In tervent ions fo r theTreatment o f ADHD
-
8/11/2019 ADHD Web
46/68
Classroom Management:Basic Considerations
One of the major impairments of children withADHD is functioning
in the educational setting.
More children with ADHD are receiving services inpublic schools
now than at any other time in
history. Despite the success of medication management
and parent training, psychoeducationalinterventions are needed
to ensure academic
success and maintain positive behavior in childrenwith ADHD.
-
8/11/2019 ADHD Web
47/68
Classroom Management:Basic Considerations
The first goal of school-based interventions is toimprove basic
knowledgeamong educatorsabout the nature, causes, course and
treatmentof ADHD.
The second goal is to increase home andschool col laborat ionto
ensure that thetreatment plan is consistent, and effectiveacross
settings.
Third, effective intervent ionsshould includestrategies to
improve academic and socialfunctioning in children and adolescents
and
occupational functioning in adults.
-
8/11/2019 ADHD Web
48/68
ADHD Basics:Training for Educators
ADHD is biological lybased and is treatable butnot curable. Goal
is to manage symptoms andreduce secondary harm (e.g., grade
retention,peer rejection, disciplinary actions).
ADHD is not due to a lack of skill or knowledge,but is a problem
of sustaining attention, effort,and motivation and of inhibiting
behavior. It is adisorder of performing what one knows, not of
knowing what to do. Treatment is most effective when
appliedconsis tent lyat the place and time where abehavior is
expected to be performed (e.g., at
school).
ADHD B i
-
8/11/2019 ADHD Web
49/68
ADHD Basics:Training for Educators
It is harder for students with ADHD to do thesame academic work
and exhibit the socialbehavior expected of other students. Thus,
thesestudents need more st ruc ture, frequent positive
consequences, consistent negativeconsequences, and
accommodations to assignedwork.
To maximize behavior change: proact ive
interventions involve manipulating antecedentevents to prevent
challenging behaviors fromoccurring; reactive interventions
involveimplementing consequences following a target
behavior.
Cl I t ti
-
8/11/2019 ADHD Web
50/68
Classroom Interventions :9 Key Principles
Rules and instructions provided to childrenwith ADHD must be c
lear, b riefand oftendelivered through more vis ib leand
externalmodes of presentation than required for themanagement of
their peers.
Consequences used to manage the behaviorof those with ADHD must
be delivered more
swi f t ly (ideally, immediately) than with theirpeers.
Consequences must also be applied moref requent ly.
Cl I t ti
-
8/11/2019 ADHD Web
51/68
Classroom Interventions :9 Key Principles
Consequencesmust often be of a highermagnitude, or more
powerful, than thatneeded to manage the behavior of
typicalchildren.
An appropriate degree of incent ivesmustbe provided within a
setting or task toreinforce appropriate behavior before
punishment can be implemented. Reinforcers/rewards that are
employed must
be changed or rotated more frequently thantypical to avoid
habituation or satiation.
Cl I t ti
-
8/11/2019 ADHD Web
52/68
Classroom Interventions :9 Key Principles
Ant ic ipat ionis key. Thus, teachers mustplan ahead and ensure
that children with
ADHD are cognizant of an upcomingtransition or change in rules
or routine beforeit occurs. Think aloud, think ahead.
Children with ADHD must be held morepublicly accountable for
their behavior and
goal attainment than typical children. Behavioral interventions
only work while they
are being implemented and requiremodification over time for
effectiveness.
Cl M t
-
8/11/2019 ADHD Web
53/68
Classroom Management:Accommodations
10 core areas of intervention: Decrease workload to fit the
childs attentional capacity
Alter teaching style and curriculum
Make rules external
Increase frequency of rewards and fines Increase immediacy of
consequences
Increase the magnitude/power of rewards
Set time limits for work completion
Develop a hierarchy of classroom punishments Coordinate home and
school consequences
Modifications for teens & adults
Cl M t
-
8/11/2019 ADHD Web
54/68
Classroom Management:Accommodations
Decreasing the workload Give smaller quotas of work
Allow frequent, shorter work periods
Target productivity and effort first; accuracy and
completion of assignments later Post work instructions on the
board; provide a schedule
of assignments weekly and send home to parents.
Reduce the amount of homework to 10 mins. per gradelevel (e.g.,
1st grade= 10 mins.)
Cl M t
-
8/11/2019 ADHD Web
55/68
Classroom Management:Accommodations
Modifying the classroom and curriculum Be animated, flexible and
responsive
Reward incentive systems and clear
consequences for misbehavior are crucial Use participatory
teaching strategies: have child
write on board, point, use counters
Sit child close to the teachers areaAllow for restlessness,
short stretching and/or
exercise breaks
Intersperse low interest with high interest tasks
Cl M t
-
8/11/2019 ADHD Web
56/68
Classroom Management:Accommodations
Make rules external Post schedule and rules
Use color-coded materials for instructionsand organization
Have child re-state the instruction toensure understanding
Use verbal prompts such as stay in seat,keep on working,
etc.
Cl M t
-
8/11/2019 ADHD Web
57/68
Classroom Management:Accommodations
Use a reward incentive system
Combine positive consequences (praise,
rewards, token economies) and negativeconsequences (response
cost, time out),with positive consequences tending to
make the most impact Use strategic teacher attention:
smiles,
nods, pats on the back, active ignoring
Cl M t
-
8/11/2019 ADHD Web
58/68
Classroom Management:Accommodations
Consequences must be immediateAvoid lengthy reasoning over
misbehavior.
Simply state the misbehavior and theconsequence (should be
posted as a rule)
Use a daily report card or sticker chart.
Variations of time out: go to the chill area ofclassroom;
complete a given number of
worksheets (drills) depending on the severity ofthe
misbehavior
Use mild, private, specific reprimands althoughpunishment should
be used sparingly
Cl M t
-
8/11/2019 ADHD Web
59/68
Classroom Management:Accommodations
Rewards must be tangible and desirable
Vary rewards to keep interest high
A videogame (especially, educational type) orcomputer program
can be used as an incentive
Have parents donate preferred toys and games
Try group rewards
Use a home-school based reward program (e.g.good behavior points
from school transfer torewards at home)
Classroom Management
-
8/11/2019 ADHD Web
60/68
Classroom Management:Accommodations
Set time limits for work completion
Use timers or a bell to signify the end of a
work period; use a signal about fiveminutes before the end as
well
Generally, extra time is not beneficial.
Focus on developing a distraction-freework setting and provide
breaks after shortwork periods.
Classroom Management:
-
8/11/2019 ADHD Web
61/68
Classroom Management:Accommodations
Use a punishment hierarchy Head down on desk; quiet time
Response cost (loss of tokens) Time out in a corner/chill
location
Time out at school office where childs
behavior can be monitored Suspension to the office (in school,
not athome)--punishment is immediate and briefand does not include
rewarding activities
Classroom Management:
-
8/11/2019 ADHD Web
62/68
Classroom Management:Accommodations
Coordinate home and schoolconsequences
Daily school behavior report card/ratingform and point
system
Daily home-school journal to communicate
with parents and/or provide a reminder tochild when completing
homework
Gradually, move to weekly monitoring
Classroom Management:
-
8/11/2019 ADHD Web
63/68
Classroom Management:Accommodations
Specifically, for teens with ADHD: Use a daily assignment
notebook/planner with teacher
verification and cross-checking
Create a private, in-class cueing system for off-task
behavior and disruption Use a daily or weekly school report
card; coordinate w/
home rewards (e.g. $ for grades)
Assign a daily case manager or organizational coach to
help monitor, organize and motivate Permit music during
homework
Require note-taking to pay attention
Keep an extra set of books/materials at home
Classroom Management:
-
8/11/2019 ADHD Web
64/68
Classroom Management:Accommodations
More tips for teens: Learn SQ4R for reading comprehension:
Survey material, draft Questions, Read, Recite,
Write, Review
-- Study with buddy after school
-- Swap phone numbers and email addresses withclassmates to call
in the event of lost or missing
assignment sheets and instructions-- Attend after school
help/tutoring sessions
-- Schedule parent-teacher review meetings every6 weeks
Occupational:
-
8/11/2019 ADHD Web
65/68
Occupational:Accommodations
College-bound teens and young adults mayrequire assistance
with:
Employment Independent Living
Managing money
Organization
Time management
Accommodations/resources for college andoccupational success
Occupational:
-
8/11/2019 ADHD Web
66/68
Occupational:Accommodations
CHADD (Children and Adults with Attention-Deficit/Hyperactivity
Disorder) offers severalresources to assist adults in handling
theseand other important issues. Please visitwww.chadd.orgfor more
information.
http://www.chadd.org/http://www.chadd.org/
-
8/11/2019 ADHD Web
67/68
Summary Education of teachers and other professionals
working with children and adults with ADHD iscrucial to helping
these individuals receive theaccommodations needed to ensure
successacademically and occupationally.
Interventions are effective as long as they arebeing implemented
and must be maintained overextended time periods.
Collaboration between school and home appearsto ensure greater
success in the classroom.
There are many resources available offering awealth of advice to
professionals who help those
with ADHD.
Resources
-
8/11/2019 ADHD Web
68/68
Resources www.chadd.orgoffers scientifically reliable
information in English and
Spanish about ADD in children, adolescents, and adults.
Sponsored byChildren and Adults with ADHD (CHADD), the largest ADHD
support andadvocacy organization in the United States, it has
downloadable fact sheets ofscience-based information for parents,
educators, professionals, the media,and the general public. The
site also includes contact information for twohundred local
chapters of CHADD throughout the United States.
www.help4adhd.orgpresents evidence-based information in English
andSpanish about ADD in children, adolescents, and adults. This
national clearinghouse of downloadable information and resources
concerning many aspectsof ADHD is funded by the U.S. government's
Centers for Disease Control andPrevention and operated by CHADD.
New material is added frequently, andquestions directed to the site
are responded to by knowledgeable health-
information specialists. www.add.orgis a resource in English for
adults with ADD. Sponsored by
Attention Deficit Disorder Association (ADDA), the world's
largest organizationfor adults with ADHD, it provides information,
resources, and networkingopportunities.