Embed Size (px)
Citation preview

ADRENAL ADRENAL DISORDERSDISORDERS
Dr. Atallah Al-RuhailyDr. Atallah Al-Ruhaily
Conultant EndocrinolgistConultant Endocrinolgist

Adult Adrenal GlandsAdult Adrenal Glands Each gland weighs 4-5 g. Each gland weighs 4-5 g.
Location: in the retroperitoneum above or medial to Location: in the retroperitoneum above or medial to the upper poles of the kidneys.the upper poles of the kidneys.
Surrounded by a fibrous capsule.Surrounded by a fibrous capsule.
The yellowish outer cortex comprises 90% of The yellowish outer cortex comprises 90% of adrenal weight.adrenal weight.
The inner medulla 10% of adrenal weight.The inner medulla 10% of adrenal weight.

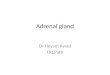
A normal right adrenal gland is shown here positioned between the liver and the kidney in the retroperitoneum. Note the amount of adipose tissue, some of which has been reflected to
reveal the upper pole of the kidney and the adrenal.
A normal right adrenal gland is shown here positioned between the liver and the kidney in the retroperitoneum. Note the amount of adipose tissue, some of which has been reflected to
reveal the upper pole of the kidney and the adrenal.

Each adult adrenal gland weighs from 4 to 6 grams.Each adult adrenal gland weighs from 4 to 6 grams.
Normal Adrenal Glands

Arterial SupplyArterial Supply
AdrenalAdrenal cortex iscortex is richly vascularised.richly vascularised.
Main arterial supply from branches of:Main arterial supply from branches of:
Inferior phrenic arteryInferior phrenic artery
Renal arteriesRenal arteries
Aorta.Aorta.

Venous DrainageVenous Drainage Rt. adrenal vein drains directly in Rt. adrenal vein drains directly in
the posterior aspect of I.V.C.the posterior aspect of I.V.C.
Lt. adrenal vein into Lt. Renal Lt. adrenal vein into Lt. Renal vein.vein.

Embryology of Adrenal Cortex
Adrenal Cortex is of mesodermal origin. Identifiable as a separate organ at the 2 month-old-fetus.
At this stage, composed of: Fetal zone
o additional zone in fetuso makes up the main bulk of weight at this time.o lost in the 1st year (usually within 3 months after birth).
Definitive zone o The origin of the adrenal cortex.

Embryology of Adrenal Cortex
Fetal adrenal increases rapidly in size (Larger than the kidney at mid gestation & much larger than adult gland in relation to total body mass).
Fetal adrenal produces mainly DHEA & DHEA-S (precursors of maternal-placental estrogen).
Definitive zone synthesizes many steroids mainly cortisol.

The anatomic relationship of fetal and definitive zones is maintained until birth.
Adrenocortical weight decreases gradually until the fetal zone disappears 3 months after delivery.
During the first 3 years, the adult adrenal cortex develops and differentiates into 3 adult zones:
GlomerulosaFasciculataReticularis
Embryology of Adrenal Cortex

Medullary chromaffin cells (the principal cells of adrenal medulla) are from the neural crest.
During development the medullary cells migrate and lie surrounded by the cortex.
Embryology of Adrenal Medulla

Adrenal gland is composed of Adrenal gland is composed of 2 distinct compartments2 distinct compartments
Adrenal cortex
produces many steroid hormones; the most important of which are:
Cortisol Aldosterone Adrenal androgens
Adrenal MedullaProduces Catecholamines: Adrenaline (Epinephrine) Noradrenaline (Norepinephrine)

Sectioning across the adrenals reveals:
• a golden yellow outer cortex; and
• an inner red to grey medulla.
Sectioning across the adrenals reveals:
• a golden yellow outer cortex; and
• an inner red to grey medulla.

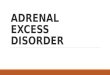
Microscopic Anatomy of Adrenal Gland
Remember “GFR”
Microscopic Anatomy of Adrenal Gland
Remember “GFR”
Periadrenal FattFibrous
CapsuleZona GlomerulsaZona Fasciculata
Zona ReticularisMedulla

Zona Glomerulosa Zona Fasciculata Zona Reticularis
The outermost. the thickest The innermost
Cells are small & lipid-poor &
scattered beneath the adrenal capsule.
Cells are larger, contain more lipid & termed “clear
cells”
“Compact” lipid-poor cells but
contain lipofuscin granules.
Aldosterone(Cannot produce
cortisol & Androgens)
Cortisol & Androgens
Cortisol & Androgens
Regulated by Renin-Angiotensin
System & K
Both structure and function are
regulated by ACTH
Both structure and function are
regulated by ACTH
Zones of Adrenal Cortex
Functionally considered as one unit.

Classification of Adrenal Steroids
classified into 3 groups based on their predominant functions:1. Glucocorticoids2. Mineralocorticoids3. Androgens

Major Classes of Adrenal SteroidsMajor Classes of Adrenal Steroids
Steroid Class Androgens (C19)
Glucocorticoids (C21)
Mineralocorticoids (C21)
Main Hormones
DHEA, DHEA-SAndrostenidione
CortisolCorticosteron
e
Aldosterone
Predominant action
Androgenic activity metabolism of:• carbohydrates• and proteins
• metabolism of: Na & K•Maintain the ECV
Main Zone of production
Z. FasciculataZ. Reticularis
(functionally as one unit)
Z. Glomerulosa

Disorders of Adrenal glands
Adrenal Cortex
• Cushing’s syndrome• Addison’s disease• Hyperaldoteronism• Syndomes of congenital adrenal hyperplasia (CAH).• Hirsutism• Virilization
Adrenal MedullaPheochromocytoma

Adrenal InsufficiencyAdrenal Insufficiency
Adrenocortical insufficiency (hypofunction of the adrenal cortex) includes all conditions in which there is deficient production of:• adrenal glucocorticoid, and• mineralocorticoid hormones.

Types of adrenal insufficiency
These conditions are divided into 2 general groups according to the level of hypofunction:
1. Primary adrenal insufficiency (Addison’s diease)
due to primary hypofunction of the adrenal cortex.
2. Secondary adrenal insufficiency
adrenocortical failure secondary to a primary deficient secretion of ACTH from the pituitary gland.

Etiology of adrenal insufficiency
Primary Adrenal Insufficiency A. Anatomic destruction of gland (chronic & acute)
1. “Idiopathic” atrophy (autoimmune)2. Surgical removal3. Infection (Tb., fungal, viral-esp. AIDS)4. Adrenal Hemorrhage5. Invasion: metasteses, amyloidosis, sarcoidosis
B. Metabolic failure in hormone production
1. Congenital adrenal hyperplasia (CAH)2. Enzyme inhibitors: (metyrapone, ketoconazole, aminoglutethemide)1. Cytotoxic agents: (mitotane)
C. ACTH-blocking Antibodies

Etiology of adrenal insufficiency
Secondary Adrenal Insufficiency
A. Hypopituitarism due to hypothalamic-pituitary disease.
B. Suppresion of hypothalamic-pituitary axis.
1. Exogenous steroids (Iatrogenic)2. Endogenous steroids (from tumors)

Incidence
Primary adrenal insufficiency:relatively rare.Occurs at any age.affects both sexes equally.
Secondary adrenal insufficiency:
relatively common (because of common therapeutic use of steroids).

Addison’s disease results from progressive destruction of adrenal cortex.
At least 90% of gland is destroyed before signs of insufficiency appear.
Addison’s Disease
Etiology and Pathogenesis


50% of patients have +ve circulating adrenal Abs.Some Abs destroy the adrenal glands, others block the binding of ACTH to its receptors.
Some patients have +ve Abs to thyroid, parathyroid and/or gonadal tissues.
Polyglandular Autoimmune (PGA) syndromes
Addison’s Disease
Etiology and Pathogenesis

Associated Autoimmune DisordersAssociated Autoimmune Disorders
Endocrine DisordersEndocrine Disorders
• Chronic lymphocytic thyroiditis
• Premature ovarian failure• DM type 1• Primary hypothyroidism• Hyperthyroidism
Nonendocrine DisordersNonendocrine Disorders
• Pernicious anemia• Vitiligo• Alopecia• Chronic active hepatitis• Nontropical sprue• Myasthenia gravis

Common Symptoms in chronic primary adrenal insufficiency
SymptomsSymptoms FrequencyFrequency
Asthenia (weakness, tiredness, fatigue)Asthenia (weakness, tiredness, fatigue)
AnorexiaAnorexia
Gastrointestinal symptomsGastrointestinal symptoms•NauseaNausea•VomitingVomiting•ConstipationConstipation•Abdominal painAbdominal pain•DiarrheaDiarrhea•Salt cravingSalt craving•Postural dizzinessPostural dizziness•Muscular or joint painsMuscular or joint pains
100100
100100
9090
8585
7575
3030
3030
1515
1515
1010
1010

Common Signs in chronic primary adrenal insufficiency
SignsSigns FrequencyFrequency
Weight lossWeight loss
Hyperpigmentation of skin Hyperpigmentation of skin
Pigmentation of mucous membranePigmentation of mucous membrane
Decreased axillary and pubic hair (in women Decreased axillary and pubic hair (in women only)only)
Hypotention (systolic BP <110 mm Hg) with Hypotention (systolic BP <110 mm Hg) with postural accentuationpostural accentuation
Vitiligo (with autoimmune)Vitiligo (with autoimmune)
100100
9595
8080
6060
1515
1010

Common Laboratory findings in chronic primary adrenal insufficiency
Laboratory FindingsLaboratory Findings FrequencyFrequency
Electrolytes disturbancesElectrolytes disturbances• HyponatremiaHyponatremia
• HyperkalemiaHyperkalemia
• HypercalcemiaHypercalcemia
AzotemiaAzotemia
AnemiaAnemia
EosinophiliaEosinophilia
9090
9090
6565
55
5555
4040
1515

HyperpigmentationHyperpigmentation
Generalized hyperpigmentation of skin & Generalized hyperpigmentation of skin & mucous membrane (the classical physical mucous membrane (the classical physical finding).finding).
Along with other features, suggests primary Along with other features, suggests primary adrenocortical insufficiency.adrenocortical insufficiency.
One of earliest manifestations of Addison’s One of earliest manifestations of Addison’s disease.disease.

HyperpigmentationHyperpigmentation Increased at exposed areas and accentuated at pressure areas Increased at exposed areas and accentuated at pressure areas
(knuckles, toes, elbows, knees)(knuckles, toes, elbows, knees)
Associated with black or dark brown freckles.Associated with black or dark brown freckles.
Hperpigmentation of buccal mucosa & gum is preceded by Hperpigmentation of buccal mucosa & gum is preceded by generalized hyperpigmentation of skin.generalized hyperpigmentation of skin.
Other areas: palmar creases, nail beds, nipples, areolae, Other areas: palmar creases, nail beds, nipples, areolae, perivaginal, perianal mucosa & scars that formed after onset perivaginal, perianal mucosa & scars that formed after onset of ACTH excess (but not older scars).of ACTH excess (but not older scars).

Adrenal ImagingAdrenal Imaging Abdominal x-raysAbdominal x-rays
– Adrenal calcificationAdrenal calcification in 50% tuberculous cases & some other invasive or in 50% tuberculous cases & some other invasive or
hemorrhagic causes.hemorrhagic causes.
CT ScanCT Scan more sensitive for adrenal calcification & enlargementmore sensitive for adrenal calcification & enlargement
Causes of bilateral adrenal enlargement:Causes of bilateral adrenal enlargement:» TbTb
» Fungal infectionFungal infection
» CMV infectionCMV infection
» Infiltrative diseases (malignant or nonmalignant)Infiltrative diseases (malignant or nonmalignant)
» Adrenal hemorrhageAdrenal hemorrhage

Rt Adrenal mass

Acute Adrenal CrisisAcute Adrenal Crisis
A state of acute adrenal insufficiency occuring in A state of acute adrenal insufficiency occuring in patients with Addison’s disease who are exposed to patients with Addison’s disease who are exposed to any form of stress.any form of stress.
Precipitating stress factors:Precipitating stress factors:
1. Infection
2. Trauma
3. Surgery
4. Dehydration (Salt deprivation, vomiting, diarrhea)
5. Discontinuation of steroids replacement therapy

Acute Adrenal CrisisCommon Clinical Features
• Hypotension & shock
• Fever (due to infection or hypoadrenalism per se)
• Dehydration, volume depletion
• Nausea, vomiting, anorexia
• Abdominal pain (may mimic acute abdomen)
• Weakness, apathy, depressed mentation
• Hypoglycemia (more in children)
Shock and coma may rapidly lead to death in untreated patients.

Acute Adrenal CrisisLaboratory Findings Suggestive of Diagnosis
• Hyponatremia & Hyperkalemia
(In a small number of acute cases).
• Azotemia (usual)
• Lymphocytosis
• Eosinophilia
• Hypoglycemia

Acute Adrenal HemorrhageAcute Adrenal Hemorrhage
A progressively deteriorating A progressively deteriorating condition resulting from bilateral condition resulting from bilateral adrenal hemorrhage and acute adrenal hemorrhage and acute adrenal destruction in an already adrenal destruction in an already compromised patient with major compromised patient with major illness.illness.

Acute Adrenal HemorrhageAcute Adrenal Hemorrhage
Manifestations:Manifestations:– Abdominal, flank or back pain & abdominal Abdominal, flank or back pain & abdominal
tenderness (Less frequently, abdominal tenderness (Less frequently, abdominal distention, rigidity & rebound tenderness).distention, rigidity & rebound tenderness).
– Hypotension & shockHypotension & shock– FeverFever– Nausea & VomitingNausea & Vomiting– Confusion & disorientationConfusion & disorientation– tachycardiatachycardia

Acute Adrenal HemorrhageAcute Adrenal Hemorrhage
With progression, the following With progression, the following manifestations may ensue:manifestations may ensue:– severe hypotentionsevere hypotention– volume depletionvolume depletion– DehydrationDehydration– HyperpyrexiaHyperpyrexia– CynosisCynosis– HypoglycemiaHypoglycemia– ComaComa– deathdeath

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyCausesCauses
ACTH deficiency most commonly due ACTH deficiency most commonly due to exogenous glucocorticoid therapy.to exogenous glucocorticoid therapy.
Pituitary & Hypothalamus tumors the Pituitary & Hypothalamus tumors the most common causes of naturally most common causes of naturally occuring pituitary ACTH occuring pituitary ACTH hyposecretion.hyposecretion.

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyPathphysiologyPathphysiology
ACTH deficiency is the primary event.ACTH deficiency is the primary event.
This leads to: This leads to: – decreased cortisol & androgen secretion.decreased cortisol & androgen secretion.– But aldosterone secretion remains normal except in But aldosterone secretion remains normal except in
few cases.few cases.

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyPathphysiologyPathphysiology
In early stages, In early stages, – Basal ACTH & cortisol levels may be normal.Basal ACTH & cortisol levels may be normal.– ACTH reserve is impaired. Response of ACTH & ACTH reserve is impaired. Response of ACTH &
cortisol to stress is subnormal.cortisol to stress is subnormal. With further loss of basal ACTH secretion,With further loss of basal ACTH secretion,
– There is atrophy of Z. Fasciculata & Z. Reticularis.There is atrophy of Z. Fasciculata & Z. Reticularis.– Basal cortisol secretion is decreasedBasal cortisol secretion is decreased– The entire pituitary adrenal axis is impaired (i.e. The entire pituitary adrenal axis is impaired (i.e.
Decreased ACTH responsiveness to stress & decreased Decreased ACTH responsiveness to stress & decreased adrenal responsiveness to stimulation with exogenous adrenal responsiveness to stimulation with exogenous ACTH). ACTH).
In early stages, In early stages, – Basal ACTH & cortisol levels may be normal.Basal ACTH & cortisol levels may be normal.– ACTH reserve is impaired. Response of ACTH & ACTH reserve is impaired. Response of ACTH &
cortisol to stress is subnormal.cortisol to stress is subnormal. With further loss of basal ACTH secretion,With further loss of basal ACTH secretion,
– There is atrophy of Z. Fasciculata & Z. Reticularis.There is atrophy of Z. Fasciculata & Z. Reticularis.– Basal cortisol secretion is decreasedBasal cortisol secretion is decreased– The entire pituitary adrenal axis is impaired (i.e. The entire pituitary adrenal axis is impaired (i.e.
Decreased ACTH responsiveness to stress & decreased Decreased ACTH responsiveness to stress & decreased adrenal responsiveness to stimulation with exogenous adrenal responsiveness to stimulation with exogenous ACTH). ACTH).

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyClinical FeaturesClinical Features
Usually chronic nonspecific manifestations.Usually chronic nonspecific manifestations.
Acute crisis occurs in:Acute crisis occurs in:– Undiagnosed patientsUndiagnosed patients– Patients who do not receive increased steroid dosage Patients who do not receive increased steroid dosage
during periods of stress.during periods of stress.
Usually chronic nonspecific manifestations.Usually chronic nonspecific manifestations.
Acute crisis occurs in:Acute crisis occurs in:– Undiagnosed patientsUndiagnosed patients– Patients who do not receive increased steroid dosage Patients who do not receive increased steroid dosage
during periods of stress.during periods of stress.

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyClinical FeaturesClinical Features
Clinical features differ from primary in Clinical features differ from primary in that:that:
1.1. Hyperpigmentation does not occur (Because of Hyperpigmentation does not occur (Because of ACTH deficiency).ACTH deficiency).
2.2. Manifestations of mineralocorticoid deficiency are Manifestations of mineralocorticoid deficiency are usually absent (Because Aldosterone secretion by usually absent (Because Aldosterone secretion by Z. G. is usually preserved). Therefore:Z. G. is usually preserved). Therefore:
» Volume depletion, dehydration & hyperkalemia usually absent.Volume depletion, dehydration & hyperkalemia usually absent.
» Hypotention is usually absent except in acute presentations.Hypotention is usually absent except in acute presentations.
» Hyponatremia may occur as a result of water retention.Hyponatremia may occur as a result of water retention.
Clinical features differ from primary in Clinical features differ from primary in that:that:
1.1. Hyperpigmentation does not occur (Because of Hyperpigmentation does not occur (Because of ACTH deficiency).ACTH deficiency).
2.2. Manifestations of mineralocorticoid deficiency are Manifestations of mineralocorticoid deficiency are usually absent (Because Aldosterone secretion by usually absent (Because Aldosterone secretion by Z. G. is usually preserved). Therefore:Z. G. is usually preserved). Therefore:
» Volume depletion, dehydration & hyperkalemia usually absent.Volume depletion, dehydration & hyperkalemia usually absent.
» Hypotention is usually absent except in acute presentations.Hypotention is usually absent except in acute presentations.
» Hyponatremia may occur as a result of water retention.Hyponatremia may occur as a result of water retention.

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyClinical FeaturesClinical Features
Prominent features (due to glucocorticoid Prominent features (due to glucocorticoid deficiency) are nonspecific & include:deficiency) are nonspecific & include:
– Weakness, lethargy & easy fatigabilityWeakness, lethargy & easy fatigability– anorexia, nausea & occasionally vomitinganorexia, nausea & occasionally vomiting– Arthralgias & myalgiasArthralgias & myalgias– HypoglycemiaHypoglycemia– Acute decompensation with severe hypotention or Acute decompensation with severe hypotention or
shock unresponsive to vasopressors.shock unresponsive to vasopressors.
Prominent features (due to glucocorticoid Prominent features (due to glucocorticoid deficiency) are nonspecific & include:deficiency) are nonspecific & include:
– Weakness, lethargy & easy fatigabilityWeakness, lethargy & easy fatigability– anorexia, nausea & occasionally vomitinganorexia, nausea & occasionally vomiting– Arthralgias & myalgiasArthralgias & myalgias– HypoglycemiaHypoglycemia– Acute decompensation with severe hypotention or Acute decompensation with severe hypotention or
shock unresponsive to vasopressors.shock unresponsive to vasopressors.

Secondary Adrenal InsufficiencySecondary Adrenal InsufficiencyAssociated FeaturesAssociated Features
The following additional features may be present:The following additional features may be present:
– History of glucocorticoid therapy or Cushingoid History of glucocorticoid therapy or Cushingoid features. features.
– Features of loss of other pituitary hormones Features of loss of other pituitary hormones (hypogonadism & hypothyroidism).(hypogonadism & hypothyroidism).
– Features of hypersecretion of GH or PRL from Features of hypersecretion of GH or PRL from pituitary adenoma.pituitary adenoma.
– Pressure symptoms from pituitary tumors.Pressure symptoms from pituitary tumors.
The following additional features may be present:The following additional features may be present:
– History of glucocorticoid therapy or Cushingoid History of glucocorticoid therapy or Cushingoid features. features.
– Features of loss of other pituitary hormones Features of loss of other pituitary hormones (hypogonadism & hypothyroidism).(hypogonadism & hypothyroidism).
– Features of hypersecretion of GH or PRL from Features of hypersecretion of GH or PRL from pituitary adenoma.pituitary adenoma.
– Pressure symptoms from pituitary tumors.Pressure symptoms from pituitary tumors.

Diagnosis of Adrenal InsufficiencyDiagnosis of Adrenal Insufficiency
BasalBasal levels of adrenocortical steroids in plasma levels of adrenocortical steroids in plasma or urine may be normal in partial adrenal or urine may be normal in partial adrenal insufficiency. insufficiency.
Tests for adrenocortical Tests for adrenocortical reservereserve are necessary to are necessary to establish the diagnosis.establish the diagnosis.– Rapid ACTH Stimulation TestRapid ACTH Stimulation Test– Plasma ACTH LevelsPlasma ACTH Levels– Metyrapone TestMetyrapone Test– Insulin-induced HypoglycemiaInsulin-induced Hypoglycemia– CRH StimulationCRH Stimulation
BasalBasal levels of adrenocortical steroids in plasma levels of adrenocortical steroids in plasma or urine may be normal in partial adrenal or urine may be normal in partial adrenal insufficiency. insufficiency.
Tests for adrenocortical Tests for adrenocortical reservereserve are necessary to are necessary to establish the diagnosis.establish the diagnosis.– Rapid ACTH Stimulation TestRapid ACTH Stimulation Test– Plasma ACTH LevelsPlasma ACTH Levels– Metyrapone TestMetyrapone Test– Insulin-induced HypoglycemiaInsulin-induced Hypoglycemia– CRH StimulationCRH Stimulation

Diagnosis of Adrenal InsufficiencyDiagnosis of Adrenal Insufficiency
Other indirect clues:Other indirect clues:Features of hypersecretion of GH or Features of hypersecretion of GH or
PRL from pituitary adenoma.PRL from pituitary adenoma.Pressure symptoms from pituitary Pressure symptoms from pituitary
tumors.tumors.
Other indirect clues:Other indirect clues:Features of hypersecretion of GH or Features of hypersecretion of GH or
PRL from pituitary adenoma.PRL from pituitary adenoma.Pressure symptoms from pituitary Pressure symptoms from pituitary
tumors.tumors.

Evaluation of Suspected Adrenal InsufficiencyEvaluation of Suspected Adrenal Insufficiency
Rapid ACTH Stimulation TestRapid ACTH Stimulation Test
A.A. Abormal ACTH Stimulation Test: Abormal ACTH Stimulation Test: Adrenocortical insufficiency +ve. Adrenocortical insufficiency +ve. Which type?Which type?
Plasma ACTH level:Plasma ACTH level: Elevated: Elevated: Primary Adrenal Primary Adrenal
Insufficiency +veInsufficiency +ve Normal or Low: Normal or Low: Secondary Adrenal Secondary Adrenal
Insufficiency +veInsufficiency +ve

Evaluation of Suspected Adrenal InsufficiencyEvaluation of Suspected Adrenal Insufficiency
Rapid ACTH Stimulation TestRapid ACTH Stimulation Test
B.B. Normal ACTH Stimulation Test:Normal ACTH Stimulation Test: This excludes Primary Adrenal Insufficiency & This excludes Primary Adrenal Insufficiency &
Adrenal atrophy.Adrenal atrophy. But does not exclude “Decreased ACTH But does not exclude “Decreased ACTH
Reserve”Reserve” Metyrapone TestMetyrapone Test or Insulin-hypoglycemia Testor Insulin-hypoglycemia Test or CRH stimulation Test:or CRH stimulation Test:
Normal: Normal: Exclude Adrenal InsufficiencyExclude Adrenal Insufficiency Abnormal: Abnormal: Secondary Adrenal Secondary Adrenal
Insufficiency +veInsufficiency +ve

Treatment of Adrenal InsufficiencyTreatment of Adrenal InsufficiencyAcute Addisonian CrisisAcute Addisonian Crisis
Glucocorticoid ReplacementGlucocorticoid Replacement– Cortisol (Hyrdocortisone succinate or phosphate) 100 mg Cortisol (Hyrdocortisone succinate or phosphate) 100 mg
every 6 hrs. for 24 hrs.every 6 hrs. for 24 hrs.
– When stable, reduce to 50 mg 6 hrs.When stable, reduce to 50 mg 6 hrs.
– Taper to maintenance therapy by day 4 or 5 & add Taper to maintenance therapy by day 4 or 5 & add mineralocorticoid as required.mineralocorticoid as required.
– If complications persist or occur, maintain or increase the dose If complications persist or occur, maintain or increase the dose to 200-400 mg/d.to 200-400 mg/d.
General or Supportive MeasuresGeneral or Supportive Measures– Correct volume depletion, dehydration, & hypoglycemia with Correct volume depletion, dehydration, & hypoglycemia with
I.V. saline and glucose. I.V. saline and glucose.
– Evaluate and treat infection or other precipitating factors.Evaluate and treat infection or other precipitating factors.
Glucocorticoid ReplacementGlucocorticoid Replacement– Cortisol (Hyrdocortisone succinate or phosphate) 100 mg Cortisol (Hyrdocortisone succinate or phosphate) 100 mg
every 6 hrs. for 24 hrs.every 6 hrs. for 24 hrs.
– When stable, reduce to 50 mg 6 hrs.When stable, reduce to 50 mg 6 hrs.
– Taper to maintenance therapy by day 4 or 5 & add Taper to maintenance therapy by day 4 or 5 & add mineralocorticoid as required.mineralocorticoid as required.
– If complications persist or occur, maintain or increase the dose If complications persist or occur, maintain or increase the dose to 200-400 mg/d.to 200-400 mg/d.
General or Supportive MeasuresGeneral or Supportive Measures– Correct volume depletion, dehydration, & hypoglycemia with Correct volume depletion, dehydration, & hypoglycemia with
I.V. saline and glucose. I.V. saline and glucose.
– Evaluate and treat infection or other precipitating factors.Evaluate and treat infection or other precipitating factors.

Treatment of Adrenal InsufficiencyTreatment of Adrenal InsufficiencyMaintenance TherapyMaintenance Therapy
Life-long replacement therapy with glucocorticoid and Life-long replacement therapy with glucocorticoid and mineralocorticoid.mineralocorticoid.
Preparations:Preparations:– Cortisol (hydrocortisone) tabletsCortisol (hydrocortisone) tablets
» First choiceFirst choice» Maintenance dose: 15-30 mg/d.Maintenance dose: 15-30 mg/d.» Usually, divided into 2 doses (2/3 AM & 1/3 PM)Usually, divided into 2 doses (2/3 AM & 1/3 PM)
– Cortisone acetate (37.5mg/d)Cortisone acetate (37.5mg/d)» Absorbed rapidly from GITAbsorbed rapidly from GIT» converted in the liver to cortisol.converted in the liver to cortisol.
Life-long replacement therapy with glucocorticoid and Life-long replacement therapy with glucocorticoid and mineralocorticoid.mineralocorticoid.
Preparations:Preparations:– Cortisol (hydrocortisone) tabletsCortisol (hydrocortisone) tablets
» First choiceFirst choice» Maintenance dose: 15-30 mg/d.Maintenance dose: 15-30 mg/d.» Usually, divided into 2 doses (2/3 AM & 1/3 PM)Usually, divided into 2 doses (2/3 AM & 1/3 PM)
– Cortisone acetate (37.5mg/d)Cortisone acetate (37.5mg/d)» Absorbed rapidly from GITAbsorbed rapidly from GIT» converted in the liver to cortisol.converted in the liver to cortisol.

Treatment of Adrenal InsufficiencyTreatment of Adrenal InsufficiencyMaintenance TherapyMaintenance Therapy
Preparations:Preparations:Synthetic Steroids Synthetic Steroids
- Prednisone or Prednisolone- Prednisone or Prednisolone5 mg of prednisone tab is equivalent to 20 5 mg of prednisone tab is equivalent to 20 mg of hydrocortisone.mg of hydrocortisone.
-Fludrocortisone (9-alpha fludrocortisol)-Fludrocortisone (9-alpha fludrocortisol)»Used for mineralocorticoid therapyUsed for mineralocorticoid therapy»Usual dose: 0.05-0.1 mg/d PO AMUsual dose: 0.05-0.1 mg/d PO AM
Preparations:Preparations:Synthetic Steroids Synthetic Steroids
- Prednisone or Prednisolone- Prednisone or Prednisolone5 mg of prednisone tab is equivalent to 20 5 mg of prednisone tab is equivalent to 20 mg of hydrocortisone.mg of hydrocortisone.
-Fludrocortisone (9-alpha fludrocortisol)-Fludrocortisone (9-alpha fludrocortisol)»Used for mineralocorticoid therapyUsed for mineralocorticoid therapy»Usual dose: 0.05-0.1 mg/d PO AMUsual dose: 0.05-0.1 mg/d PO AM

Treatment of Primary Adrenal InsufficiencyTreatment of Primary Adrenal Insufficiency
Regimen TherapyRegimen Therapy Cortisol 15-20 mg AM & 10 mg at 4-5 pmCortisol 15-20 mg AM & 10 mg at 4-5 pm Or prednisone 5.0-7.5 mg AMOr prednisone 5.0-7.5 mg AM Fludrocortisone (Fluranif) 0.05 0.1 mg PO AM.Fludrocortisone (Fluranif) 0.05 0.1 mg PO AM. Clinical Follow up:Clinical Follow up:
– Maintenance of normal body weight, BP & Maintenance of normal body weight, BP & electrolytes electrolytes
– Regression of clinical featuresRegression of clinical features Patient education & identification card or Patient education & identification card or
braceletbracelet Increased cortisol dosage during stress.Increased cortisol dosage during stress.
Cortisol 15-20 mg AM & 10 mg at 4-5 pmCortisol 15-20 mg AM & 10 mg at 4-5 pm Or prednisone 5.0-7.5 mg AMOr prednisone 5.0-7.5 mg AM Fludrocortisone (Fluranif) 0.05 0.1 mg PO AM.Fludrocortisone (Fluranif) 0.05 0.1 mg PO AM. Clinical Follow up:Clinical Follow up:
– Maintenance of normal body weight, BP & Maintenance of normal body weight, BP & electrolytes electrolytes
– Regression of clinical featuresRegression of clinical features Patient education & identification card or Patient education & identification card or
braceletbracelet Increased cortisol dosage during stress.Increased cortisol dosage during stress.














![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://img.pdfslide.net/doc/110x75/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)