Embed Size (px)
Citation preview
J. Endocrinol. Invest. 27: 67-69, 2004
67
ABSTRACT. Acute adrenal hemorrhage (AAH) isan extremely rare disorder, especially in adults,and may be difficult to diagnose because of itsnonspecific presentation. We report a case ofAAH following a sepsis, resulting in persistant
adrenal insufficiency contrasting with the radio-logic normalisation of the adrenals on comput-ed tomography (CT) scan imaging.(J. Endocrinol. Invest. 27: 67-69, 2004)©2004, Editrice Kurtis
INTRODUCTION
Acute adrenal hemorrhage (AAH) is an extreme-ly rare disorder which can be difficult to diagnosein patients with a severe clinical condition. We re-port a case of AAH following a pulmonary sepsis,resulting in persistant adrenal insufficiency con-trasting with the radiologic normalisation of theadrenals on computed tomography (CT) scanimaging.
CASE REPORT
A 52-yr-old man was admitted to intensive care unitfor severe bilateral pneumonia radiographically char-acterized by bilateral alveolar opacities. He had onlya history of chronic obliterative smoking bronchitisand was otherwise healthy. Despite microbiologicalinvestigations revealing no etiological agent such asmycoplasma pneumoniae, chlamydia, legionella ortuberculosis, the patient was successfully treated withiv levofloxacine. He received no anti-inflammatorydrug, especially no corticosteroid. On the 7th day hecomplained of extreme weakness, associated withabdominal pain, anorexia and vomiting. Confusionand ileus developed and physical examination re-vealed dehydratation, tachycardia (115 bpm) and ablood pressure of 80/40 mmHg. No melanodermiawas noticed. Laboratory tests disclosed a serum sodi-
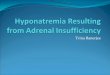
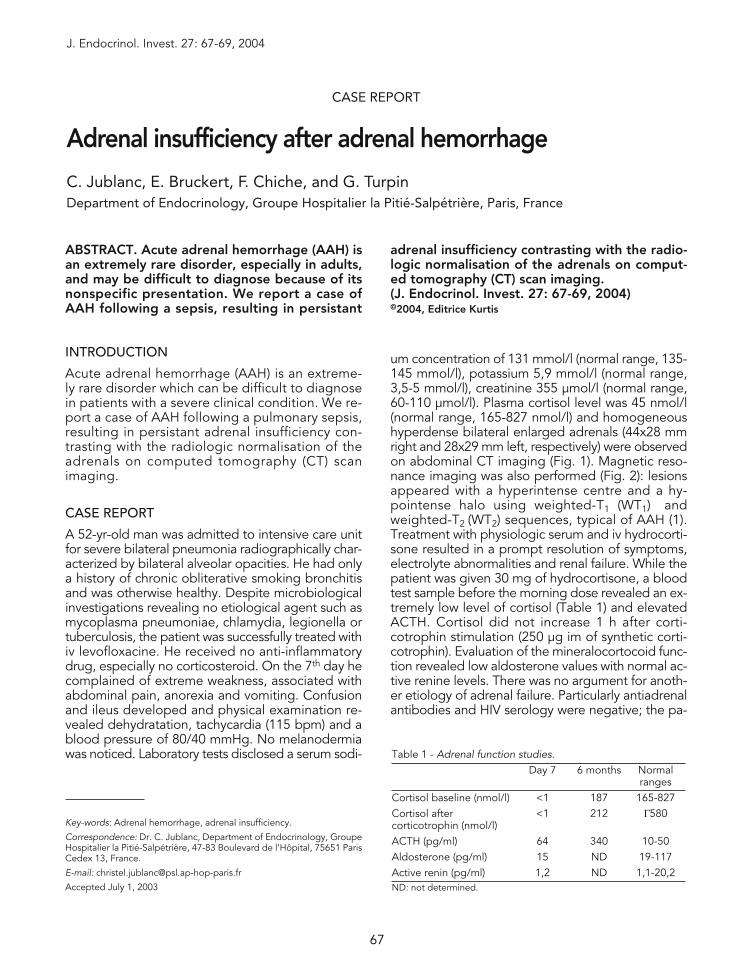
um concentration of 131 mmol/l (normal range, 135-145 mmol/l), potassium 5,9 mmol/l (normal range,3,5-5 mmol/l), creatinine 355 μmol/l (normal range,60-110 μmol/l). Plasma cortisol level was 45 nmol/l(normal range, 165-827 nmol/l) and homogeneoushyperdense bilateral enlarged adrenals (44x28 mmright and 28x29 mm left, respectively) were observedon abdominal CT imaging (Fig. 1). Magnetic reso-nance imaging was also performed (Fig. 2): lesionsappeared with a hyperintense centre and a hy-pointense halo using weighted-T1 (WT1) andweighted-T2 (WT2) sequences, typical of AAH (1).Treatment with physiologic serum and iv hydrocorti-sone resulted in a prompt resolution of symptoms,electrolyte abnormalities and renal failure. While thepatient was given 30 mg of hydrocortisone, a bloodtest sample before the morning dose revealed an ex-tremely low level of cortisol (Table 1) and elevatedACTH. Cortisol did not increase 1 h after corti-cotrophin stimulation (250 μg im of synthetic corti-cotrophin). Evaluation of the mineralocortocoid func-tion revealed low aldosterone values with normal ac-tive renine levels. There was no argument for anoth-er etiology of adrenal failure. Particularly antiadrenalantibodies and HIV serology were negative; the pa-
Key-words: Adrenal hemorrhage, adrenal insufficiency.
Correspondence: Dr. C. Jublanc, Department of Endocrinology, GroupeHospitalier la Pitié-Salpétrière, 47-83 Boulevard de l’Hôpital, 75651 ParisCedex 13, France.
E-mail: [email protected]
Accepted July 1, 2003
CASE REPORT
Adrenal insufficiency after adrenal hemorrhage
C. Jublanc, E. Bruckert, F. Chiche, and G. TurpinDepartment of Endocrinology, Groupe Hospitalier la Pitié-Salpétrière, Paris, France
Table 1 - Adrenal function studies.Day 7 6 months Normal
rangesCortisol baseline (nmol/l) <1 187 165-827Cortisol after <1 212 Γ580corticotrophin (nmol/l)ACTH (pg/ml) 64 340 10-50Aldosterone (pg/ml) 15 ND 19-117Active renin (pg/ml) 1,2 ND 1,1-20,2ND: not determined.
Adrenal hemorrhage
68
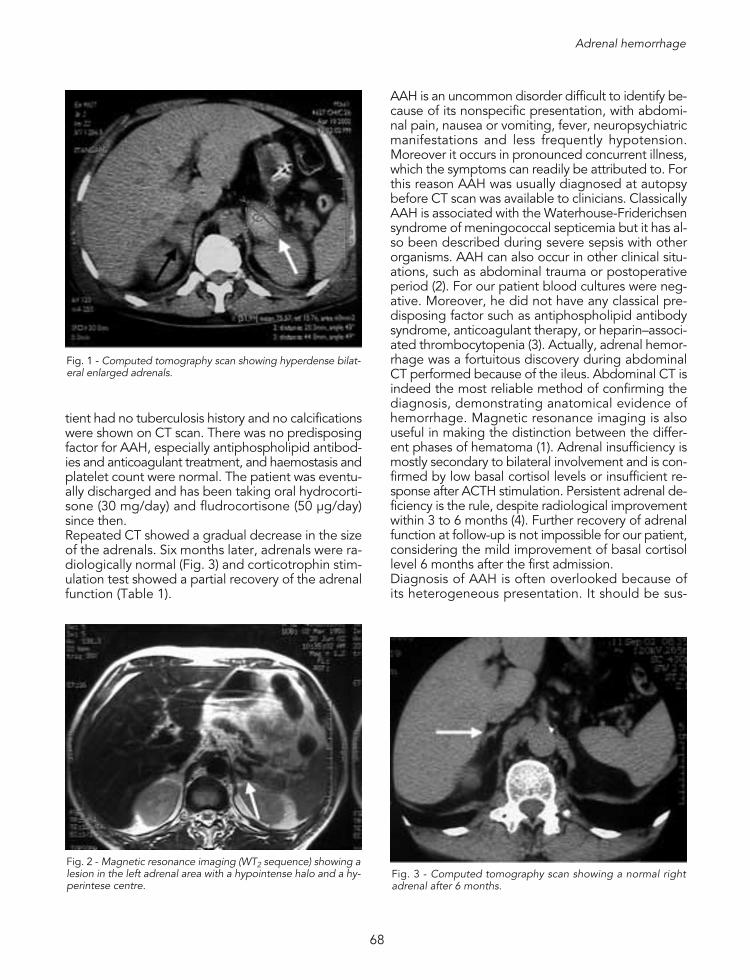
tient had no tuberculosis history and no calcificationswere shown on CT scan. There was no predisposingfactor for AAH, especially antiphospholipid antibod-ies and anticoagulant treatment, and haemostasis andplatelet count were normal. The patient was eventu-ally discharged and has been taking oral hydrocorti-sone (30 mg/day) and fludrocortisone (50 μg/day)since then. Repeated CT showed a gradual decrease in the sizeof the adrenals. Six months later, adrenals were ra-diologically normal (Fig. 3) and corticotrophin stim-ulation test showed a partial recovery of the adrenalfunction (Table 1).
AAH is an uncommon disorder difficult to identify be-cause of its nonspecific presentation, with abdomi-nal pain, nausea or vomiting, fever, neuropsychiatricmanifestations and less frequently hypotension.Moreover it occurs in pronounced concurrent illness,which the symptoms can readily be attributed to. Forthis reason AAH was usually diagnosed at autopsybefore CT scan was available to clinicians. ClassicallyAAH is associated with the Waterhouse-Friderichsensyndrome of meningococcal septicemia but it has al-so been described during severe sepsis with otherorganisms. AAH can also occur in other clinical situ-ations, such as abdominal trauma or postoperativeperiod (2). For our patient blood cultures were neg-ative. Moreover, he did not have any classical pre-disposing factor such as antiphospholipid antibodysyndrome, anticoagulant therapy, or heparin–associ-ated thrombocytopenia (3). Actually, adrenal hemor-rhage was a fortuitous discovery during abdominalCT performed because of the ileus. Abdominal CT isindeed the most reliable method of confirming thediagnosis, demonstrating anatomical evidence ofhemorrhage. Magnetic resonance imaging is alsouseful in making the distinction between the differ-ent phases of hematoma (1). Adrenal insufficiency ismostly secondary to bilateral involvement and is con-firmed by low basal cortisol levels or insufficient re-sponse after ACTH stimulation. Persistent adrenal de-ficiency is the rule, despite radiological improvementwithin 3 to 6 months (4). Further recovery of adrenalfunction at follow-up is not impossible for our patient,considering the mild improvement of basal cortisollevel 6 months after the first admission.Diagnosis of AAH is often overlooked because ofits heterogeneous presentation. It should be sus-
Fig. 1 - Computed tomography scan showing hyperdense bilat-eral enlarged adrenals.
Fig. 2 - Magnetic resonance imaging (WT2 sequence) showing alesion in the left adrenal area with a hypointense halo and a hy-perintese centre.
Fig. 3 - Computed tomography scan showing a normal rightadrenal after 6 months.

C. Jublanc, E. Bruckert, F. Chiche, et al.
69
pected in patients who are confused, have fever,or who complain of abdominal pain or nausea af-ter surgery, during severe sepsis, or soon after ini-tiation of anticoagulation. In such cases cliniciansshould treat empirically with glucocorticoids (5)while awaiting results for confirmatory tests.
REFERENCES1. Ferreira JG, Borri ML, Menasce S, Ajzen S, Kater CE, Faical
S. Acute adrenal haemorrhage: diagnosis, treatment andfollow-up. Int Urol Nephrol. 1996, 28: 735-41.
2. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage:a 25-year experience at the Mayo Clinic. Mayo Clin Proc.2001, 76: 161-8.
3. Kovacs KA, Lam YM, Pater JL. Bilateral massive adrenalhemorrhage. Assessment of putative risk factors by the case-control method. Medicine (Baltimore) 2001, 80: 45-53.
4. Dahlberg PJ, Goellner MH, Pehling GB. Adrenal insuffi-ciency secondary to adrenal hemorrhage. Two case re-ports and a review of cases confirmed by computed to-mography. Arch Intern Med 1990, 150: 905-9.
5. Rao RH. Bilateral massive adrenal hemorrhage. Med ClinNorth Am 1995, 79: 107-29.