Embed Size (px)
Citation preview
ADSA Chronic Care Management Program
Controlling Medicaid costs and improving health outcomes
National Academy For State Health PolicyOctober 5, 2011
1
CHRONIC CAREMANAGEMENT
C Goehring
A Look At The Scope of the Problem:
Making the Case for Chronic Care Management
• “What is right with you is a lot more powerful than what is wrong with you”
•
2C Goehring
Washington State Medicaid Impact
• Five percent of WA Medicaid clients account for 50 percent of the costs.
• They are consumers of LTC
• Are diagnosed with depression and chronic pain.
• Current health care system is focused on acute care and misses working with clients with chronic conditions from developing complications.
3
How did we frame the ADSA Model of Chronic Care Management?
C Goehring
4
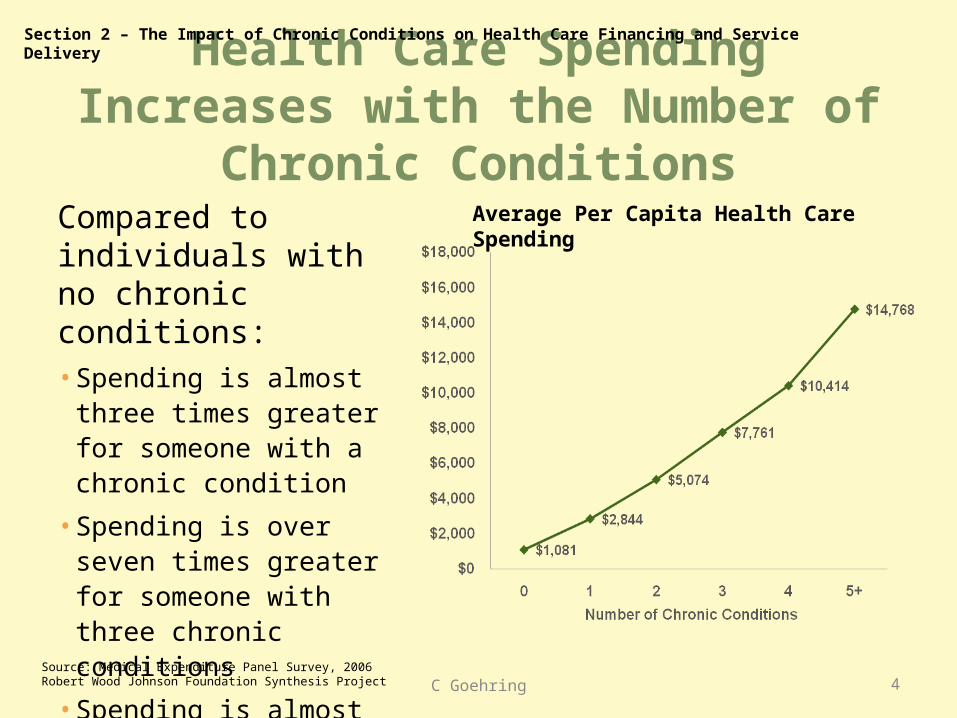
Health Care Spending Increases with the Number of Chronic Conditions
Compared to individuals with no chronic conditions:• Spending is almost three
times greater for someone with a chronic condition
• Spending is over seven times greater for someone with three chronic conditions
• Spending is almost 15 times greater for someone with five or more chronic conditions
Section 2 – The Impact of Chronic Conditions on Health Care Financing and Service Delivery
Average Per Capita Health Care Spending
Source: Medical Expenditure Panel Survey, 2006Robert Wood Johnson Foundation Synthesis Project C Goehring
5
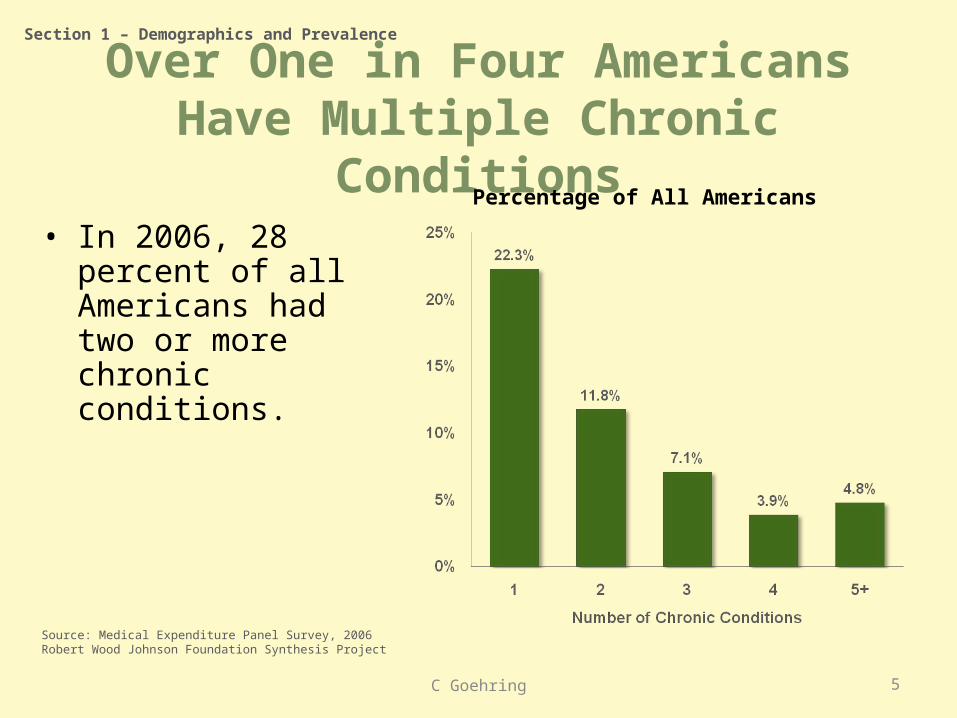
Over One in Four Americans Have Multiple Chronic Conditions
• In 2006, 28 percent of all Americans had two or more chronic conditions.
Section 1 – Demographics and Prevalence
Percentage of All Americans
Source: Medical Expenditure Panel Survey, 2006Robert Wood Johnson Foundation Synthesis Project
C Goehring
6
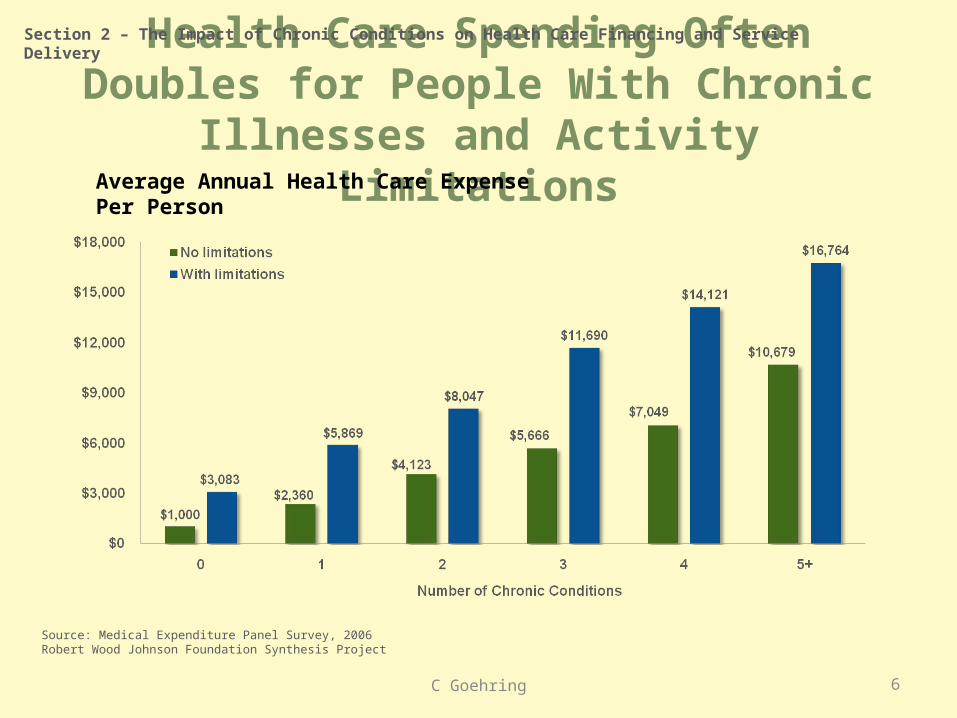
Health Care Spending Often Doubles for People With Chronic Illnesses and Activity Limitations
Section 2 – The Impact of Chronic Conditions on Health Care Financing and Service Delivery
Average Annual Health Care Expense Per Person
Source: Medical Expenditure Panel Survey, 2006Robert Wood Johnson Foundation Synthesis Project
C Goehring
Washington StateAging and Disability Services Administration
Chronic Care Management (CCM)
ADSA Chronic Care Management:• Eligible beneficiaries use home & community-based services and are
at high risk for utilization of medical services.
• Provides interventions for the medical, social, economic, mental health, chemical dependencies, and environmental factors impacting health and health care choices.
• State Plan Amendment Approved 12/2010
7C Goehring
The CCM Intervention• Nurse care manager to client ratio 1:50
• Primarily face to face with telephone support as needed.
• Evidence-based protocols include:• Diabetes management• Pain management• Fall assessment and prevention
planning
• Comprehensive Assessment including Patient Activation Measure (PAM™)
• Client-centered Health Action Plan and Goal Setting Worksheet• Set goals with client according to activation level• Education towards self-management of chronic illness
8C Goehring
• Medication management• Health Action Planning• Coaching for Activation ™
Risk Determinants
High medical cost and risk client determinants
Predictive modeling (PRISM) Past twelve months medical claims, gender and age determine
future medical costs and risk.
Diabetes, cardiovascular disease, mental health and substance abuse (highest diagnosis frequencies).
Pharmacy, inpatient care, and emergency room utilization (highest cost utilization)
Care opportunities identified (avoidable or reducible care)
Risk Score in top 20%
9C Goehring
LTC Risk Determinants
Comprehensive Assessment Resource Evaluation (CARE) LTCrisk criteria (presence of one)
1. Client lives alone
2. High risk moods/behaviors (agitation/irritable)
3. Self health rating is fair or poor
4. Overall self-sufficiency declined in last 90 days
5. Greater than six medications
10C Goehring

Tailored Client Coaching Approach
The client: Is in charge of the care plan;
Sets the pace for change based on perception of need and readiness for change.
The nurse’s role: Encourage client confidence - that their actions can make an impact
on their health and independence
Discuss and offer options and education that allow the client to increase their ability to manage their own care to improve quality of life and/or health outcomes
Ask the client what ideas they have to better manage their health care.
11C Goehring
Health Action Plan• Identify diagnosis affecting health outcomes.
• Identify client identified goals, interventions, and goals.
• Use Goal and Action Planning Worksheet with the client and their identified supports.
• Update with the client at each contact reflecting client; Barriers
Successes
Changing priorities
12C Goehring
Predictive Risk Intelligence System (PRISM)
• Decision support tool designed to support care management interventions for high-risk Medicaid patients Identification of clients most in need of comprehensive care
coordination based on risk scores developed through predictive modeling
Integration of information from medical, social service, behavioral health, and long term care payment and assessment data systems
Intuitive and accessible display of client health and demographic from administrative data sources
• Serves over 200 users with 28 distinct population groups, and continues to evolve to meet changing program needs
C Goehring 13
PRISM ScreensEpisodes Key medical and behavioral health risk areasEligibility Detailed eligibility and demographic data
Claims All medical claims and encountersOffice Office visits
RX Prescriptions filledIP Inpatient admissionsER Outpatient emergency room visits
LTC Long term care servicesLab Laboratory
Providers Provider list with links to contact informationAOD Alcohol and Drug treatmentMH Mental health services
CARE Long-term care functional assessmentsHRI Health risk indicators
C Goehring14
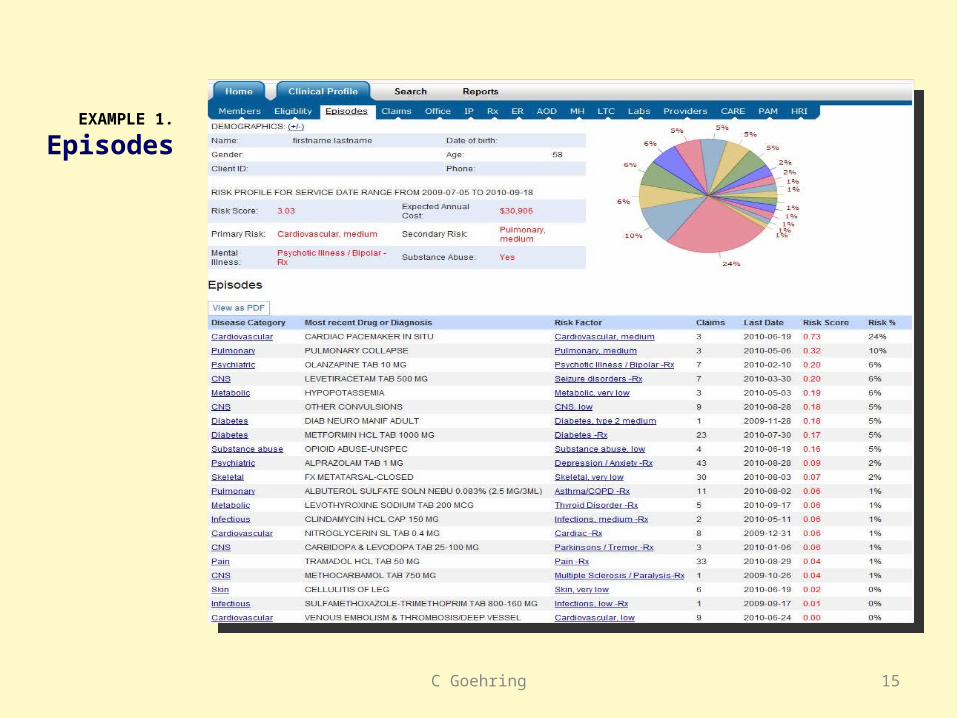
EXAMPLE 1.
Episodes
C Goehring 15
Uses of PRISM
• Medical evidence gathering for determining eligibility for disability-related medical coverage
• Triaging high-risk populations to more efficiently allocate scarce care management resources; for example, stratifying by recent inpatient and emergency department activity
• Identification of child health risk indicators for high-risk children [mental health crisis, substance abuse, ED use, nutrition or feeding problems]
• Identification of behavioral health needs [redacting information where required by state and federal law]
• Medication adherence monitoring C Goehring 16
Uses of PRISM continued
• Identification of other potential barriers to care, Patient’s housing status (e.g., whether they are homeless)
Hearing impairment
Non-English primary language
• Access to treating and prescribing provider contact information for care coordination
• Creation of child health summary reports for foster parents and pediatricians
• A source of regularly updated contact information from the medical eligibility determination process
C Goehring 17
Strengths of PRISM
• “One-stop shopping” for information from administrative data systems across medical, behavioral health and long-term care systems
• An intuitive user interface
• Data refreshed weekly
• The ability to create and share a comprehensive profile of a client
• State-of-the-art prediction of prospective medical costs
• Data on psychosocial risk factors, including behavioral health, homelessness, and functional limitations from care coordination assessments.
C Goehring 18
Limitations of PRISM
• The relationship between traditional measures of medical risk and “impactability” is not well understood
• Many quality measures derived from payment data have limited empirical data to support their relationship to health outcomes in complex populations
• Data quality issues, such as the accuracy of behavioral health diagnoses recorded by medical professionals (e.g., misdiagnosis of bipolar disorder as depression)
• PRISM is not an electronic medical record: lab results and clinical notes are not currently linked into the application
C Goehring 19
Limitations of PRISM
• Potential for incomplete information Lags in processing claims and submitting encounter data
Claims paid through separate coverage like Medicare or private insurance
Services paid out-of-pocket
Redaction of chemical dependency treatment system data where written consent documentation process is not in place
C Goehring 20
Contact Information
Candace (Candy) Goehring RN MN Washington State DSHSAging and Disability Services [email protected]
C Goehring21