Embed Size (px)
Citation preview

�9/21/2015
�1
Adult Congenital Heart Disease: The New Reality
Kathryn Rouine-Rapp, MD
Professor of Anesthesia
I have nothing to disclose
Disclosures

�9/21/2015
�2
Outline
� Historic perspective
� Our reality
� Common lesions
� Guidelines
� Pathways to expertise
Lorraine Sweeney 1938
� PDA
� First person to survive surgery to correct CHD
� BCH
� Dr. Robert Gros
� 7 yo

�9/21/2015
�3
Eileen Saxon 1944
� TOF� First person to undergo BT(T) shunt � Johns Hopkins� Drs Blalock, Taussig, & Mr Thomas� Age 15 months
“switching arteries sidetracks blood and
oxygen to otherwise starved lungs”

�9/21/2015
�4
Our Reality
� 1-3 million adults USA and CA with CHD� 1.8 million Europe� Survival to adulthood increased from
30% in 1940s to nearly 90% today� More adults vs children with CHD� Median age 40 yrs
�FEBRUARY 23, 2014

�9/21/2015
�5
Our Reality
� >10000 adults with CHD� Increasing fraction of all non-cardiac
surgery� Majority underwent surgery non-
teaching hospitals� Increased morbidity and mortality
� Maxwell et al. Anesthesiology. 2013 Oct;119(4):762-9
Lesion classification
� Complexity classification
� Simple
� Moderate
� Severe
� 20-25% overall severe complexity
� 40% simple or “resolved” post intervention

�9/21/2015
�6
Patient status
� Unoperated� Palliated� Surgical or device correction
� Excellent uncomplicated result� Residual defect� Sequelae

�9/21/2015
�7
Lesions
� Common lesions
� VSD, ASD, PDA
� Pulmonary valve stenosis
� Aortic valve stenosis
� Coarctation of the aorta
� Atrioventricular-septal defects
� TOF
� TGA
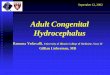
ASDOne of most common defectsFour types
� Secundum (70%) , central IAS, associated MR
� Primum (15-25%), near AV valves, associated cleft MV
� Sinus venosus (10%), associated w anomalous PV
� Unroofed coronary sinus (rare)

�9/21/2015
�8
�http://www.doctortipster.com/wp-content/uploads/2011/07/interatrial-septal-defect2.gif
�https://apps.childrenshospital.org/clinical/mml/viewBLOB.cfm?MEDIA_ID=306

�9/21/2015
�9
Spectrum of severity24 yo male asx athlete, murmur detected, secundum ASD
83 yo male, in OR for CABG, new “incidental” finding on TEE immediately prior to CPB, SV ASD & anomalous RUPV
54 yo female, presented with DOE and new onset atrial fibrillation with RVR, TTE w RVD, L to R ASD flow
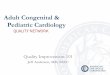
VSD
� Four types� Perimembranous (70%) � Muscular (20%) � Doubly-committed (subarterial)
(5%) � Inlet (5%)

�9/21/2015
�10
�http://206.47.151.137/bcdecker/figures/acs/part11_ch01_fig29.gif
Spectrum of severity
� Large defects = heart failure/sx
� Qp/Qs � pulmonary to systemic flow ratio
� defect size
� SVR and PVR
� PHTN
� Infective endocarditis
� Device closure or surgery

�9/21/2015
�11
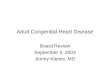
Tetralogy of Fallot
� Most common cyanotic defect � Four lesions
� RVOTO (severity determines cyanosis)
� RVH� VSD (PM)� Overriding aorta
�http://www.heartbirthdefect.com/images/birth-defects/621x440xtetralogy-of-Fallot.jpg.pagespeed.ic.4Xfv8mG3um.jpg

�9/21/2015
�12
Spectrum of severity
� 61yo male for atrial flutter ablation
� Shunt placement
� Shunt revision and PM
� Surgical repair (10yo)
� Proximal LPA hypoplasia
� Aneurysmal RVOT patch, PI
� RV EF 30%
� Decreasing exercise tolerance
� Not a candidate for percutaneous intervention

�9/21/2015
�13
Guidelines
� 2008 ACC/AHA consensus statement
� Adults with CHD : surgical (diagnostic, interventional) procedures that require general anesthesia or conscious sedation in adults with moderate or complex CHD should be performed in a regional adult CHD center with an anesthesiologist familiar with adult CHD patients
Guidelines
� 2008 ACC/AHA consensus statement
� Adult patients with complex or high-risk CHD should be transferred to an adult CHD center for urgent or acute problems
� …and should have a cardiologist consultation prior to procedures

�9/21/2015
�14
Simple lesions
� Unoperated� Isolated mild
aortic or mitral valve lesion
� Isolated ASD� Small isolated VSD� Isolated mild PV
stenosis
� Operated� PDA� Secundum ASD� Sinus venosus
ASD wo residua� VSD wo residua
�Cannesson et al Anesth 2009
Training
� no established curriculum for education
� DiNardo, Baum, Andropoulous: pathways for pediatric cardiac anesthesia fellowships depend on training prior to fellowship AnesthAnalg. 2010 Apr 1;110(4):1121-5
� Inconsistent experience during adult cardiac anesthesia fellowships across USA (personal survey)

�9/21/2015
�15
Closed claim analysis� Factors: adverse events n = 21� 11 (52%) cardiac procedures � 10 (48%) noncardiac procedures� cardiac procedures
� surgical technique (73%) � intraoperative anesthetic care (55%)
� noncardiac cases � postoperative monitoring/care (50%)� CHD (50%) � preoperative assessment or
optimization (40%)�Maxwell BG et al. Congenit Heart Dis. 2015 Jan-Feb;10(1):21-9
Questions to consider
� Status of patient
� Unoperated, palliated, repaired
� Lesion and classification
� Simple, moderate, severe complexity
� Functional status
� NYHA
� Standard of care & experts in your group
� When to say “no”

�9/21/2015
�16
Summary
� Increasing population of adults with CHD who need our care
� Lesion classification
� Specific lesions
� Guidelines
� Training variability
� Reality of local care vs triage
THANK YOU

�9/21/2015
�17

�9/21/2015
�18